Embed Size (px)
Citation preview

Anesthetic Management of the Elderly Patient
Raymond C. Roy, PhD, MDRaymond C. Roy, PhD, MD
Professor & Chair of AnesthesiologyProfessor & Chair of Anesthesiology
Wake Forest University Health SciencesWake Forest University Health Sciences
Winston-Salem, NC, USA 27157-1009Winston-Salem, NC, USA 27157-1009
http://www.wfubmc.edu/anesthesiaEducation: Annual Meeting – American Society of Anesthesiologists

Hayflick’s View of AgingHayflick’s View of Aging
““Because modern humans, unlike feral Because modern humans, unlike feral animals, have learned how to escape animals, have learned how to escape death long after reproductive success, we death long after reproductive success, we have revealed a process that, have revealed a process that, teleologically, was never intended for us teleologically, was never intended for us
to experience.”to experience.”

# Older Americans# Older Americans
20002000 20302030
> 65 yrs> 65 yrs 12.4%12.4% 19.6%19.6%
35 mil35 mil 71 mil71 mil
> 80 yrs> 80 yrs 9.3 mil9.3 mil 19.5 mil19.5 mil


The Oldest…..The Oldest…..
• MANMAN 120 yrs120 yrs
• WOMANWOMAN 122 122 – Guinness Book of RecordsGuinness Book of Records
• GENERAL ANESTHETICGENERAL ANESTHETIC 113 113 – Br J AnaesthBr J Anaesth 2000; 84:260 2000; 84:260

Life Expectancy at birth Life Expectancy at birth USA - 1997USA - 1997
WOMENWOMEN CaucasianCaucasian 79.9 yrs79.9 yrs
African-AmericanAfrican-American 74.774.7
MENMEN CaucasianCaucasian 74.374.3
African-AmericanAfrican-American 67.267.2

Life Expectancy, Life Span, Life Expectancy, Life Span, & Maximum Length of Life& Maximum Length of Life
• Maximum Length of LifeMaximum Length of Life > 120 yrs> 120 yrs
• Life SpanLife Span 85-10085-100
– Natural death (no trauma or disease)Natural death (no trauma or disease)
• Life Expectancy (USA)Life Expectancy (USA) 67-8067-80
– Premature death (trauma, disease)Premature death (trauma, disease)

Oldest Surgical Patient?Oldest Surgical Patient?Oliver. Oliver. Br J AnaesthBr J Anaesth 2000; 84:260 2000; 84:260
• Woman, 113 yrs, femoral fractureWoman, 113 yrs, femoral fracture
• General anesthesiaGeneral anesthesia
• CVP, no arterial-lineCVP, no arterial-line
• Extubation in ICU after 5hExtubation in ICU after 5h
• Hospital discharge POD 23Hospital discharge POD 23

# Anesthetics per 100 Population?# Anesthetics per 100 Population?Clergue. Clergue. AnesthesiologyAnesthesiology 1999; 91:1509 (France) 1999; 91:1509 (France)
Ages (yrs)Ages (yrs) MenMen WomenWomen
35 – 4435 – 44 8.98.9 13.213.2
55 - 6455 - 64 17.717.7 14.614.6
75 - 8475 - 84 30.230.2 23.623.6

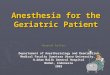
Vascular Surgery – Mortality vs AgeVascular Surgery – Mortality vs AgeFleisher. Fleisher. Anesth AnalgAnesth Analg 1999; 89:849 1999; 89:849
0%
5%
10%
15%
20%
25%
<65 66-70 71-75 76-80 81-85 >85 yrs
aorticinfrainquinal

Perioperative Complication Perioperative Complication Rates in Medicare PatientsRates in Medicare Patients
• Intermediate Risk Surgery - 42%Intermediate Risk Surgery - 42%– Silber, Silber, AnesthesiologyAnesthesiology 2000; 93:152 2000; 93:152
– 217,440 general & orthopedic surgery217,440 general & orthopedic surgery
• Low Risk Surgery - 3%Low Risk Surgery - 3%– Schein, Schein, N Engl J MedN Engl J Med 2000; 342:168 2000; 342:168
– 18,901 cataract surgery18,901 cataract surgery

Age & Perioperative OutcomeAge & Perioperative Outcome
• With advancing ageWith advancing age
– More surgeryMore surgery
– Morbidity increasesMorbidity increases
– Mortality increasesMortality increases
• Cause - disease vs age ?Cause - disease vs age ?
– Disease > age when < 85 yrsDisease > age when < 85 yrs
– Age may = disease when > 85 yrsAge may = disease when > 85 yrs
– Increase ASA PS when > 85 yrsIncrease ASA PS when > 85 yrs

Preoperative ConsiderationsPreoperative Considerations
• Preoperative AssessmentPreoperative Assessment
– No routine preoperative testingNo routine preoperative testing
– Statin myopathic syndromesStatin myopathic syndromes
– Diastolic dysfunctionDiastolic dysfunction
• Diabetes MellitusDiabetes Mellitus
– Tighter glucose control with insulinTighter glucose control with insulin
– Stop oral hypoglycemic agentsStop oral hypoglycemic agents

Why Obtain Preoperative Tests?Why Obtain Preoperative Tests?
• Screening – NO with one exceptionScreening – NO with one exception
– Urinalysis if hip surgery or acutely illUrinalysis if hip surgery or acutely ill
– Cook & Rooke, Cook & Rooke, Anesth AnalgAnesth Analg 2003; 96:1823 2003; 96:1823
• Treatment effectiveness - YESTreatment effectiveness - YES
• Baseline – MAYBE, but overusedBaseline – MAYBE, but overused
• Risk Assessment - YESRisk Assessment - YES

Value of Preoperative Testing Value of Preoperative Testing Before Low Risk SurgeryBefore Low Risk SurgerySchein. Schein. N Engl J MedN Engl J Med 2000; 342:168 2000; 342:168
Rate/100 Untested Tested
Medical Event: Intraop 1.87 1.94
Postop .92 .94
Unplanned Hospitalization .34 .29
Death .02 .01
Total 3.13 3.13

Value of Preoperative Testing Value of Preoperative Testing Before Low Risk SurgeryBefore Low Risk Surgery Schein. Schein. N Engl J MedN Engl J Med 2000; 342:168 2000; 342:168
““Tests should be ordered only when the Tests should be ordered only when the history or a finding on a physical history or a finding on a physical examination would have indicated the examination would have indicated the need for the test need for the test even if surgery had even if surgery had not been planned.not been planned.””

Intermediate Risk Noncardiac Intermediate Risk Noncardiac Surgery (Mortality > 1%, < 5%)Surgery (Mortality > 1%, < 5%)
CAROTIDCAROTID
HEAD & NECKHEAD & NECK
INTRAPERITONEALINTRAPERITONEAL
INTRATHORACICINTRATHORACIC
ORTHOPEDICORTHOPEDIC
PROSTATEPROSTATE

Preoperative Tests - Prevalence of Preoperative Tests - Prevalence of Abnormal ResultsAbnormal Results544 consecutive intermediate risk non-cardiac surgical 544 consecutive intermediate risk non-cardiac surgical patients > 69 yrs - Dzankic. patients > 69 yrs - Dzankic. Anesth AnalgAnesth Analg 2001; 93:301 2001; 93:301
Creatinine > 1.5 mg/dL 12%Creatinine > 1.5 mg/dL 12%
Hemoglobin < 10 mg/dL 10%Hemoglobin < 10 mg/dL 10%
Glucose > 200 mg/dL 7%Glucose > 200 mg/dL 7%
KK++ < 3.5 mEq/L 5% < 3.5 mEq/L 5%
KK++ > 5.0 mEq/L 4% > 5.0 mEq/L 4%
Platelets < 115,000/ml 2%Platelets < 115,000/ml 2%

Outcomes of Patients with No Outcomes of Patients with No Laboratory Assessment for Laboratory Assessment for Intermediate Risk SurgeryIntermediate Risk Surgery
N = 1,044N = 1,044 Narr. Narr. Mayo Clin ProcMayo Clin Proc 1997; 72:505 1997; 72:505
““Patients … assessed by history and Patients … assessed by history and physical examination … safely physical examination … safely undergo … operation undergo … operation with tests drawn with tests drawn only as indicated intraoperatively and only as indicated intraoperatively and postoperativelypostoperatively.”.”

Is ROUTINE Preoperative Is ROUTINE Preoperative Testing Indicated?Testing Indicated?
NO (my opinion), IFNO (my opinion), IF
– FOLLOWED BY PRIMARY CARE MDFOLLOWED BY PRIMARY CARE MD
– RELIABLE SYSTEM TO OBTAIN H & PRELIABLE SYSTEM TO OBTAIN H & P
– NO “RED FLAGS” IN H & PNO “RED FLAGS” IN H & P
– MODERATE FUNCTIONAL STATUS + MODERATE FUNCTIONAL STATUS + INTERMEDIATE RISK SURGERY INTERMEDIATE RISK SURGERY OR OR
POOR BUT STABLE FUNCTIONAL STATUS + POOR BUT STABLE FUNCTIONAL STATUS + LOW RISK SURGERYLOW RISK SURGERY

No Non-invasive or Invasive No Non-invasive or Invasive Cardiac Testing for Intermediate Cardiac Testing for Intermediate Risk SurgeryRisk Surgery
MODERATE FUNCTIONAL CAPACITY + MODERATE FUNCTIONAL CAPACITY + INTERMEDIATE CLINICAL PREDICTORSINTERMEDIATE CLINICAL PREDICTORS
OROR
POOR FUNCTIONAL CAPACITY + MINOR POOR FUNCTIONAL CAPACITY + MINOR CLINICAL PREDICTORSCLINICAL PREDICTORS
J Am Coll CardiolJ Am Coll Cardiol 1996; 27:910 1996; 27:910

INTERMEDIATE INTERMEDIATE CLINICAL PREDICTORSCLINICAL PREDICTORS
MILD STABLE ANGINAMILD STABLE ANGINA
PRIOR MIPRIOR MI
COMPENSATED CHFCOMPENSATED CHF
PRIOR CHFPRIOR CHF
DIABETES MELLITUSDIABETES MELLITUS

FUNCTIONAL CAPACITYFUNCTIONAL CAPACITY
MET= metabolic equivalent OMET= metabolic equivalent O22 consumption of 70 kg, 40 yr old consumption of 70 kg, 40 yr old man in resting stateman in resting state
> 7 METs - excellent> 7 METs - excellent
4-7 METs - moderate4-7 METs - moderate
< 4 METs - poor< 4 METs - poor– JJ Am Coll Cardiol 1996; 27:910-48Am Coll Cardiol 1996; 27:910-48

Estimated Energy Requirements Estimated Energy Requirements for Activities of Daily Living - 1for Activities of Daily Living - 1
1 MET -------------------------> 4 METs1 MET -------------------------> 4 METs
– eat, dress, use toileteat, dress, use toilet
– walk indoors around housewalk indoors around house
– walk 1-2 blocks on level groundwalk 1-2 blocks on level ground
– light house worklight house work

Estimated Energy Requirements Estimated Energy Requirements for Activities of Daily Living - 2for Activities of Daily Living - 2
4 METs -------------------> 10 METs4 METs -------------------> 10 METs
– climb flight of stairs, walk up a hillclimb flight of stairs, walk up a hill
– walk briskly on level groundwalk briskly on level ground
– run a short distancerun a short distance
– do heavy house workdo heavy house work
– golf, bowling, dancing, doubles tennisgolf, bowling, dancing, doubles tennis

Most Difficult ROUTINE Most Difficult ROUTINE Preoperative Tests to Justify Preoperative Tests to Justify
• Chest X-rayChest X-ray
• PT and aPTT (if no heparin or warfarin)PT and aPTT (if no heparin or warfarin)
• Liver Function TestsLiver Function Tests

4 Statin Myopathic Syndromes4 Statin Myopathic SyndromesThompson. Thompson. JAMAJAMA 2003; 289:1681 2003; 289:1681
• STATIN MYOPATHYSTATIN MYOPATHY
– Any muscle complaint with onset Any muscle complaint with onset coincident with start of statin therapycoincident with start of statin therapy
• MYALGIA with normal CKMYALGIA with normal CK
• MYOSITIS with elevated CKMYOSITIS with elevated CK
• RHABDOMYOLYSISRHABDOMYOLYSIS

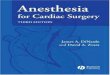
% of Older Patients with % of Older Patients with Diastolic DysfunctionDiastolic Dysfunction
0
10
20
30
40
50
60
45-54 55-64 65-74 75 orgreat er
MildModerat eSevere

Diabetes Mellitus – 8.7% of Diabetes Mellitus – 8.7% of ElderlyElderly
• Ischemic heart diseaseIschemic heart disease
• Problems with all oral hypoglycemic agentsProblems with all oral hypoglycemic agents
• More infections – pulmonary, woundMore infections – pulmonary, wound
• Decreased pulmonary functionDecreased pulmonary function
• Decreased response to hypoxiaDecreased response to hypoxia
• Prolonged response to vecuroniumProlonged response to vecuronium

Problems with Oral Problems with Oral Hypoglycemic AgentsHypoglycemic AgentsGu. Gu. AnesthesiologyAnesthesiology 2003; 98:1359 2003; 98:1359
• Sulfonylureas – myocardial ischemiaSulfonylureas – myocardial ischemia
– Interfere with K-ATP channelsInterfere with K-ATP channels
– Prevent ischemic preconditioningPrevent ischemic preconditioning
– Eliminate ECG benefit of warm-upEliminate ECG benefit of warm-up
– Eliminate functional benefit of warm-upEliminate functional benefit of warm-up
– Worsen dipyridamole-induced ischemiaWorsen dipyridamole-induced ischemia
• Metformin – lactic acidosisMetformin – lactic acidosis

Diabetes Mellitus – Tight Diabetes Mellitus – Tight Control of GlucoseControl of Glucose Gu. Gu. AnesthesiologyAnesthesiology 2003; 98:1359 2003; 98:1359
• Insulin infusions to maintain glucose:Insulin infusions to maintain glucose:– 80-150 mg/dl intraoperatively80-150 mg/dl intraoperatively
– 80-110 mg/dl postoperatively80-110 mg/dl postoperatively
• Reduce ICU mortality by 40%Reduce ICU mortality by 40%
• Improve outcome from acute MIImprove outcome from acute MI
• Decrease infectionsDecrease infections

Beta-adrenergic Blocking Beta-adrenergic Blocking Agents – Perioperative Agents – Perioperative AdministrationAdministration• Reduces myocardial ischemiaReduces myocardial ischemia
• Reduces myocardial infarctionReduces myocardial infarction
• Secondary Secondary ObservationsObservations– Zaugg. Zaugg. AnesthesiologyAnesthesiology 1999; 91:1674 1999; 91:1674
– Decrease anesthetic administrationDecrease anesthetic administration
– Enable faster emergenceEnable faster emergence
– Decrease post-op analgesic requirementDecrease post-op analgesic requirement

Perioperative Myocardial Perioperative Myocardial IschemiaIschemiaWallace. Wallace. AnesthesiologyAnesthesiology 1998; 88:7 1998; 88:7
MYOCARDIAL MYOCARDIAL ISCHEMIAISCHEMIA
ATENOLOLATENOLOL
(N = 99)(N = 99)
PLACEBOPLACEBO
(N = 101)(N = 101)
POD 0 - 2POD 0 - 2 1717 34*34*
* p = 0.008* p = 0.008
POD 0 - 7POD 0 - 7 2424 39**39**
**p = 0.029**p = 0.029

Perioperative Beta-Blockade - Perioperative Beta-Blockade - Therapeutic Target Therapeutic Target Auerbach. Auerbach. JAMAJAMA 2002; 287:1435 2002; 287:1435
• HEART RATE 55 – 65 bpmHEART RATE 55 – 65 bpm
• SYSTOLIC SYSTOLIC >100 mm Hg >100 mm Hg
• Before, during, and after surgeryBefore, during, and after surgery

Actual Practice versus Evidenced-Actual Practice versus Evidenced-based Beta-blockade – “Wrong” based Beta-blockade – “Wrong” Answers from ABA Oral ExamineesAnswers from ABA Oral Examinees
• DID NOT ADD IN PREOP CLINICDID NOT ADD IN PREOP CLINIC
• USED HR 80 AS TARGET INTRAOPUSED HR 80 AS TARGET INTRAOP
• DID NOT ORDER POSTOP (7 days)DID NOT ORDER POSTOP (7 days)
• ASSUMED ESMOLOL-BOLUS = LONG-ASSUMED ESMOLOL-BOLUS = LONG-ACTING PRE-, INTRA-, POSTOPACTING PRE-, INTRA-, POSTOP
(REACTIVE vs PROPHYLACTIC)(REACTIVE vs PROPHYLACTIC)

General AnesthesiaGeneral Anesthesia
• Anesthetic depthAnesthetic depth
• Neuromuscular blocking agentsNeuromuscular blocking agents
• Diastolic pressureDiastolic pressure
• Transfusion triggerTransfusion trigger
• Regional vs general anesthesiaRegional vs general anesthesia

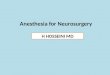
MAC & AgeMAC & AgeNickalls. Nickalls. Br J AnaesthBr J Anaesth 2003; 91:170 2003; 91:170
0123456789
I sof lurane Sevoflurane Desflurane
1 yr40 yr80 yr

Nitrous Oxide MAC & AgeNitrous Oxide MAC & AgeNickalls. Nickalls. Br J AnaesthBr J Anaesth 2003; 91:170 2003; 91:170
020406080
100120140
Nit rous Ox ide
1 yr40 yr80 yr

End-tidal Isoflurane to Provide End-tidal Isoflurane to Provide MAC with N2O in 80 Year OldsMAC with N2O in 80 Year OldsNickalls. Nickalls. Br J AnaesthBr J Anaesth 2003; 2003; 91:170 91:170
0
0.2
0.4
0.6
0.8
1
I sof lurane
0% N2O50% N2O67% N2O

Most of Us Overdose ElderlyMost of Us Overdose Elderly
• Gas monitorsGas monitors
– Assume patient is 40 yrs oldAssume patient is 40 yrs old
– Do not know what other drugs givenDo not know what other drugs given
– Do not know opioids & epidurals lower MACDo not know opioids & epidurals lower MAC
– Underestimate brain concentration on emergenceUnderestimate brain concentration on emergence
• BIS Index 55-60 with beta-blockers better than BIS Index 55-60 with beta-blockers better than BIS Index 35-45BIS Index 35-45

End-tidal Concentrations Under-End-tidal Concentrations Under-estimate Brain Concentrations estimate Brain Concentrations During Emergence from IsofluraneDuring Emergence from IsofluraneLockhart. Lockhart. AnesthesiologyAnesthesiology 1991; 74:575 1991; 74:575
0
0.1
0.2
0.3
0.40.5
0.6
0.7
0-6 13-18 25-30 m in
End-t idal concrat ioCerebral conc rat io

PROPOFOL INDUCTIONS IN 25 – PROPOFOL INDUCTIONS IN 25 – 81 YR-OLDS81 YR-OLDSSchnider. Anesthesiology 1999; 90:1502Schnider. Anesthesiology 1999; 90:1502
• Propofol: 2 mg/kg < 65 yrs; 1 mg/kg > 65 yrs Propofol: 2 mg/kg < 65 yrs; 1 mg/kg > 65 yrs
• Injection time 13-24 sInjection time 13-24 s
• Loss of consciousnessLoss of consciousness– Young = old = 40 sYoung = old = 40 s
• Return of consciousnessReturn of consciousness– 30 yrs – 5 min, 75 yrs – 10 min30 yrs – 5 min, 75 yrs – 10 min

PROPOFOL INDUCTIONS PROPOFOL INDUCTIONS 20 20 – 84 YRS– 84 YRSKazama. Anesthesiology 1999; 90:1517Kazama. Anesthesiology 1999; 90:1517
HALF-TIME FOR NADIR IN BPHALF-TIME FOR NADIR IN BP
20 – 29 yrs 20 – 29 yrs 5.7 min 5.7 min
70 – 85 yrs70 – 85 yrs 10.2 min10.2 min

PROPOFOL INDUCTIONS PROPOFOL INDUCTIONS > > 65 YRS65 YRSHabib. Br J Anaesth 2002; 88:430Habib. Br J Anaesth 2002; 88:430
Glycopyrrolate, propofol 1 mg/kg, and Glycopyrrolate, propofol 1 mg/kg, and either alfentanil 10 either alfentanil 10 μμg/kg or remifentanil g/kg or remifentanil 0.5 0.5 μμg/kg + 0.1 g/kg + 0.1 μμg/kg/ming/kg/min
SBP: < 100 mmHg 50%, < 80 mmHg 8%SBP: < 100 mmHg 50%, < 80 mmHg 8%

RECOMMENDED PROPOFOL DOSE RECOMMENDED PROPOFOL DOSE FOR INDUCTION IF > 65 yrs oldFOR INDUCTION IF > 65 yrs old
IF BOLUS (< 30 s)IF BOLUS (< 30 s)
No concurrent drugs 1.0-1.5 mg/kgNo concurrent drugs 1.0-1.5 mg/kg
Concurrent drugs 0.5-1.0 mg/kgConcurrent drugs 0.5-1.0 mg/kg
HYPOTENSIONHYPOTENSION
Continues for 10 min after injectionContinues for 10 min after injection
Fentanyl peak 6-8 min, midazolam peak 5 minFentanyl peak 6-8 min, midazolam peak 5 min
PREFER SLOWER INJECTION (1 min)PREFER SLOWER INJECTION (1 min)
Less hypotension if slow with < 1.0 mg/kgLess hypotension if slow with < 1.0 mg/kg

Elderly Take Longer to Emerge Elderly Take Longer to Emerge Than Younger PatientsThan Younger Patients
• Lower MACawake and higher pain thresholdLower MACawake and higher pain threshold
• Hypothermia more likelyHypothermia more likely
• Emergence hypertension treated as light anesthesiaEmergence hypertension treated as light anesthesia
• Reluctance to turn off vaporizerReluctance to turn off vaporizer
• Longer durations of action for drugs in elderlyLonger durations of action for drugs in elderly
• Relative drug overdosesRelative drug overdoses
• Synergistic drug interactionsSynergistic drug interactions

Neuromuscular Blocking Agents Neuromuscular Blocking Agents in the Elderly - 1in the Elderly - 1
• Same initial dose as in youngerSame initial dose as in younger
• Longer onset times withLonger onset times with::
– Advanced ageAdvanced age
– Vecuronium vs rocuroniumVecuronium vs rocuronium• Tullock. Tullock. Anesth AnalgAnesth Analg 1990; 70:86 1990; 70:86
– EsmololEsmolol• Szmuk. Szmuk. Anesth AnalgAnesth Analg 2000; 90:1217 2000; 90:1217]]

Onset Time (sec) Increases with Onset Time (sec) Increases with Advancing AgeAdvancing Age Koscielniak-Nelson. Koscielniak-Nelson. AnesthesiologyAnesthesiology 1993; 79:229 1993; 79:229
0
50
100
150
200
250
300
3-10 yrs 20-40 60-80
succinylcholine 1mg/ kgvecuronium 0.1mg/ kg

Neuromuscular Blocking Agents Neuromuscular Blocking Agents in the Elderly - 2in the Elderly - 2
• Longer duration (except cisatracurium)Longer duration (except cisatracurium)
– Advanced ageAdvanced age
– Intraoperative hypothermia (34.7Intraoperative hypothermia (34.7oo C) C)
– Diabetes mellitus (8.7% of elderly) Diabetes mellitus (8.7% of elderly)
– Obesity – dosing mg/kgObesity – dosing mg/kg

Obesity in Older MenObesity in Older Men% with BMI > 29.2% with BMI > 29.2Flegal. Flegal. JAMAJAMA 2002; 288:1723 2002; 288:1723
05
10152025303540
60-69 70-79 80+ yrs
19902000

Obesity in Older WomenObesity in Older Women% with BMI > 29.2% with BMI > 29.2Flegal. Flegal. JAMAJAMA 2002; 288:1723 2002; 288:1723
05
1015202530354045
60-69 70-79 80+ yrs
19902000

Times to Reappearance of T1, T2, T3, Times to Reappearance of T1, T2, T3, & T4 after Vecuronium 0.1 mg/kg in & T4 after Vecuronium 0.1 mg/kg in Patients with Diabetes MellitusPatients with Diabetes MellitusSaito. Saito. Br J AnaesthBr J Anaesth 2003; 90:480 2003; 90:480
0
10
20
30
40
5060
70
T1 T2 T3 T4
No DMDM

Effect of Hypothermia on Time-to-Effect of Hypothermia on Time-to-25%-Recovery from Vecuronium 0.1 25%-Recovery from Vecuronium 0.1 mg/kgmg/kg Caldwell. Caldwell. AnesthesiologyAnesthesiology 2000; 92: 84 2000; 92: 84
0
10
20
30
40
50
60
70
34 35 36 37 38 C
Time (min)

Rocuronium > Vecuronium > Rocuronium > Vecuronium > Pancuronium (My Practice)Pancuronium (My Practice)
Fastest onsetFastest onset
Shortest durationShortest duration
Least inter-patient variabilityLeast inter-patient variability
Easiest to reverseEasiest to reverse
Shortest PACU length of stayShortest PACU length of stay
Fewest post-op pulmonary complicationsFewest post-op pulmonary complications
[Cisatracurium > rocuronium if renal insufficiency][Cisatracurium > rocuronium if renal insufficiency]

Transfusion Trigger for ElderlyTransfusion Trigger for ElderlyHgb 10 g/dl or Hct 0.30Hgb 10 g/dl or Hct 0.30
• Ischemic Heart DiseaseIschemic Heart Disease– Especially if reversible ischemia, unstable Especially if reversible ischemia, unstable
angina, recent infarction or dysfunctionangina, recent infarction or dysfunction
• Pulmonary DiseasePulmonary Disease– Intra-thoracic or intra-abdominal surgeryIntra-thoracic or intra-abdominal surgery
• Leukocyte-reducedLeukocyte-reduced
• Walsh, McClelland, Walsh, McClelland, Br J AnaesthBr J Anaesth 2003; 719 2003; 719

Minimum Diastolic PressureMinimum Diastolic PressurePauca Abstract ASA 2003Pauca Abstract ASA 2003
• When treating systolic pressure (SP), pay When treating systolic pressure (SP), pay attention to diastolic pressure (DP)attention to diastolic pressure (DP)
• To maintain coronary perfusion, keepTo maintain coronary perfusion, keep
– DP at least 2/3DP at least 2/3rdrd SP SP
– DP greater than Pulse PressureDP greater than Pulse Pressure
– DP at least 60 mmHgDP at least 60 mmHg

Regional vs General Regional vs General Anesthesia – Mortality & Anesthesia – Mortality & MorbidityMorbidity
REGIONAL = GENERALREGIONAL = GENERAL
• BP, HR tightly controlled in studiesBP, HR tightly controlled in studies
• More interventions to control BP, HR in More interventions to control BP, HR in general anesthesia groupgeneral anesthesia group
REGIONAL < GENERALREGIONAL < GENERAL
• ““Real world” , BP, HR not tightly controlledReal world” , BP, HR not tightly controlled
• Included combined regional-general in Included combined regional-general in regional groupregional group
• Rogers et al. Rogers et al. Br Med JBr Med J 2000;321:1493 2000;321:1493

Postoperative ConsiderationsPostoperative Considerations
• Postoperative AnalgesiaPostoperative Analgesia
• Postoperative DeliriumPostoperative Delirium

Postoperative Titration of Postoperative Titration of Intravenous Morphine in Elderly Intravenous Morphine in Elderly Patients Patients Abrun. Abrun. AnesthesiologyAnesthesiology 2002; 96:17 2002; 96:17
• Bolus q 5 min to VAS = 30 (max 100)Bolus q 5 min to VAS = 30 (max 100)
– 2 mg if <60 kg; 3 mg if > 60 kg2 mg if <60 kg; 3 mg if > 60 kg
• Total mg/kg dose: young = oldTotal mg/kg dose: young = old
– Young (< 70, mean 45) vs Old (> 70, mean 76)Young (< 70, mean 45) vs Old (> 70, mean 76)
• Morbidity – young = oldMorbidity – young = old
– adverse opioid effects, sedation, stopped adverse opioid effects, sedation, stopped titrationstitrations

Age is not an Impediment to Age is not an Impediment to Effective Use of PCA Effective Use of PCA Gagliese. Gagliese. AnesthesiologyAnesthesiology 2000; 93:601 2000; 93:601
• Initial Dose for Pain Relief:Initial Dose for Pain Relief:
– young = oldyoung = old
• Total Dose:Total Dose:
– old < youngold < young

Postoperative Delirium in 5-50%Postoperative Delirium in 5-50%That Appears on POD’s 1-3That Appears on POD’s 1-3Cook. Cook. Anesth AnalgAnesth Analg 2003; 96:1823 2003; 96:1823
• Cellular proteins altered by potent inhaled agentsCellular proteins altered by potent inhaled agents
• Central cholinergic insufficiency, MicroemboliCentral cholinergic insufficiency, Microemboli
• Preexisting subclinical dementia, HypoxiaPreexisting subclinical dementia, Hypoxia
• Fever, Infection (UTI, sinusitis, pneumonia)Fever, Infection (UTI, sinusitis, pneumonia)
• Electrolyte abnormalities, Anemia, PainElectrolyte abnormalities, Anemia, Pain
• Sleep deprivation, Unfamiliar environmentSleep deprivation, Unfamiliar environment

Ten Ways to Improve Ten Ways to Improve Anesthesia in Older PatientsAnesthesia in Older Patients
1.1. H & P > Pre-op Testing > CXR, PT, PTTH & P > Pre-op Testing > CXR, PT, PTT
2.2. Beta-blockers pre-. intra-, post-opBeta-blockers pre-. intra-, post-op
3.3. Timely antibiotic administrationTimely antibiotic administration
4.4. Lower doses of inhaled & iv agentsLower doses of inhaled & iv agents
5.5. Rocuronium or cisatracuriumRocuronium or cisatracurium

Ten Ways to Improve Ten Ways to Improve Anesthesia in Older PatientsAnesthesia in Older Patients
6. Higher F6. Higher F IIOO22 intra-, post-op intra-, post-op
7. Transfusion trigger – Hct .307. Transfusion trigger – Hct .30
8. Diastolic pressure 60 mmHg8. Diastolic pressure 60 mmHg
9. Blood glucose - periop 80-150 mg/dl9. Blood glucose - periop 80-150 mg/dl
10. Reduce post-op opioid requirements10. Reduce post-op opioid requirements