Embed Size (px)
Citation preview

Anemia With Erythropoietin DeficiencyOccurs Early in Diabetic NephropathyDEBORAH R. BOSMAN, MBBS
1
ANDREA S. WINKLER, MBBS1
JOANNE T. MARSDEN, PHD2
IAIN C. MACDOUGALL, MD3
PETER J. WATKINS, MD1
OBJECTIVE — The normochromic normocytic anemia of erythropoietin (EPO) deficiency isrecognized in advanced renal failure but not in early renal disease. The aim of this study was todetermine whether anemia with EPO deficiency is found in type 1 diabetic patients with diabeticnephropathy in the absence of advanced renal failure and to compare them with patients withnondiabetic renal disease of similar severity.
RESEARCH DESIGN AND METHODS — A total of 27 type 1 diabetic patients withdiabetic nephropathy (DN), defined as having persistent proteinuria (mean 1,086 mg/day [CI120–5,190]), a serum creatinine #180 mmol/l, and retinopathy, were compared with 26 non-diabetic patients with glomerulonephritis (GN) and persistent proteinuria (1,874 mg/day [349–5,005]). The Hb concentration, red cell indexes, and serum EPO levels were measured, and othercauses for the anemia were excluded. The EPO values were compared with a normal referencerange obtained from nondiabetic patients with a microcytic anemia. The DN patients were testedfor signs of diabetic peripheral and autonomic neuropathy.
RESULTS — We found that 13 of the 27 DN patients were anemic (Hb 10.6 6 0.9 g/dl) inmarked contrast to none of the GN patients (Hb 13.7 6 1.4 g/dl, P , 0.005). In the DN group,serum EPO concentrations failed to increase in response to anemia compared with the responseseen in patients with microcytic anemia. Thus, the anemia of the DN group was associated withEPO deficiency. The anemic DN patients showed evidence of more severe proteinuria anddiabetic neuropathy than the nonanemic DN patients.
CONCLUSIONS — Anemia associated with EPO deficiency can occur early in DN before theonset of advanced renal failure, but does not normally occur in nondiabetic renal disease ofsimilar severity. The pathogenesis requires elucidation.
Diabetes Care 24:495–499, 2001
E rythropoietin (EPO), a 30.4-kDa gly-coprotein, is produced mainly by theperitubular fibroblasts of the renal
cortex in adult life (1). The actions of EPOinclude stimulation of erythroid progeni-tor cells and differentiation of normo-blasts to increase the red cell mass inresponse to tissue hypoxia precipitated byanemia, hemorrhage, or altitude (1–3).
An anemia with EPO deficiency hasrecently been described in some type 1
diabetic patients with severe symptomaticdiabetic autonomic neuropathy (4,5).EPO release is thought to be modulatedby the splanchnic innervation of the kid-neys because renal denervation in animalmodels leads to a loss of EPO productionin response to hypoxic stimuli (6–8). Ithas been postulated that EPO deficiencyin these patients may be caused at least inpart by efferent sympathetic denervationof the kidney leading to the loss of appro-
priate EPO production (5), and there issome clinical and experimental evidencethat this may be the case (6–11). How-ever, all of these autonomic neuropathypatients also had evidence of diabeticnephropathy (DN) with persistent pro-teinuria, although some had only mi-croalbuminuria. Because the lesion ofDN may involve not only the glomerulibut also the renal interstitial area (12), itis possible that the EPO deficiency ofthese patients results from damage to theEPO-producing fibroblasts and is not aconsequence of the neuropathy itself.
The aim of this study was to deter-mine whether an EPO-deficient anemiaexists in patients with DN without severerenal function impairment and to com-pare them with a group of patients withnondiabetic renal disease of comparableseverity.
RESEARCH DESIGN ANDMETHODS — Patients were recruitedfrom the King’s Diabetes Center and therenal clinic at King’s College Hospital,London. The study was approved by thelocal ethics committee, and all patientsgave their informed consent. We identi-fied 27 consecutive type 1 diabetic pa-tients aged ,60 years with persistentproteinuria and retinopathy. Persistentproteinuria was defined as positive (11 ormore) Albustix readings for .1 year. Pa-tients with a serum creatinine level of.180 mmol/l were excluded. A diagnosisof DN was assumed because all of the pa-tients showed evidence of diabetic reti-nopathy. We also recruited 26 patientsaged ,60 years with glomerulonephritis(GN) if there was evidence of proteinuria(more than one positive Albustix reading)and a serum creatinine level #180mmol/l. Causes of GN confirmed by renalbiopsy included IgA nephropathy (6),minimal change nephropathy (1), focalsegmental glomerulosclerosis (2), mesan-giocapillary GN (1), secondary interstitialnephritis (1), IgA-negative mesangiopro-liferative GN (4), and membranous GN(7). Patients with vasculitic causes forGN, such as systemic lupus erythemato-sis, and those with concomitant diabeteswere excluded.
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1King’s Diabetes Centre, the 2Department of Biochemistry, and the 3Department of Renal Medicine,King’s College Hospital, London, U.K.
Address correspondence and reprint requests to Dr. Peter J. Watkins, King’s Diabetes Centre, King’sCollege Hospital, Denmark Hill, London SE5 9RS, U.K. E-mail: [email protected].
Received for publication 31 July 2000 and accepted in revised form 10 November 2000.Abbreviations: DN, diabetic nephropathy; EPO, erythropoietin; GN, glomerulonephritis; PH, postural
hypotension.A table elsewhere in this issue shows conventional and Systeme International (SI) units and conversion
factors for many substances.
P a t h o p h y s i o l o g y / C o m p l i c a t i o n sO R I G I N A L A R T I C L E
DIABETES CARE, VOLUME 24, NUMBER 3, MARCH 2001 495

MethodsThe patients with DN were assessed for allsymptoms and signs of diabetic complica-tions, including diabetic peripheral andautonomic neuropathy. Autonomicsymptoms, as defined by Guy et al. (13),including postural hypotension (PH),diabetic diarrhea, gastroparesis, bladderparesis, and gustatory sweating, were re-corded. All of the diabetic patients wereexamined for evidence of neuropathy andunderwent a battery of peripheral nerveand cardiovascular autonomic functiontests. All patients were screened for ane-mia (defined as an Hb level #11.5 g/dl forwomen and 12.0 g/dl for men), and thosewith identified causes (e.g., ferritin, B12,folate deficiencies, thyroid dysfunction,and hemoglobinopathies) were excluded.Serum creatinine, liver function tests, al-bumin, and lipid profiles were recorded.Serum EPO levels were measured in allthe DN patients and in most of the GN
patients. The serum EPO levels of the ane-mic subjects were compared with valuesobtained from the control group (nondi-abetic patients with and without micro-cytic anemia[s]).
EPO assayEPO was measured using an enzyme-linked immunosorbent assay based onthe double-antibody sandwich method(Quantikine IVD; R & D Systems, Minne-apolis, MN). The within-assay precisionwas 3.1% (n 5 30, mean 16.2 IU/l), andthe between-assay coefficient of variationwas 6.5% (n 5 20, mean 10.6 IU/l). Thelaboratory normal range of EPO for non-anemic subjects is 3.3–16.6 IU/l. A smalldiurnal variation in EPO production hasbeen recognized; therefore, all EPO mea-surements were recorded in the middayor early afternoon (14).
Peripheral nerve and cardiovascularautonomic function testsPeripheral nerve tests. These includedassessment using the 10-g Semmes-Wein-stein monofilament at five points on thesole of the foot and scoring the number ofpoints perceived, vibration perception atthe grand hallux using a biosthesiometer(Biomedical Instruments, Newbury, OH),and thermal threshold assessment usingthe Thermotest (RDG Medical, Croydon,U.K.) at the lateral aspect of the foot. Thevalues were compared with publishednormal ranges (15).Cardiovascular autonomic functiontests. These included heart rate variationon deep breathing, Valsalva maneuver(only performed when proliferative reti-nopathy was not present because of theincreased risk of retinal hemorrhage), andheart rate change on standing. Standardmethods were used (16). Postural hypo-tension was defined as a systolic bloodpressure drop of $20 mmHg (17).
Statistical analysisNormal distribution of parameters was as-sessed using diagnostic plots, and whereno departure from normality was demon-strated, group differences in Hb and otherbaseline parameters were compared usingthe t tests for independent samples. Val-ues were expressed as means 6 SD. Thedata for serum creatinine, proteinuria,and serum EPO were expressed as the me-dian (range). These data were comparedusing the Mann-Whitney U test for non-parametric values. The relationship of
Table 1—Clinical and biochemical characteristics of the two groups
DN GN
n 27 26Sex (M:F) 10:17 16:10Age (years) 41 6 9 44 6 12Proteinuria (mg/day) 1,086 (120–5,190) 1,874 (349–5,005)Creatinine (mmol/l) 96 (63–160) 93 (49–180)Retinopathy (proliferative:background) 25:2 —Use of ACE/angiotensin II inhibitors 22 21Number of anemic patients 13 0
Data are n, means 6 SD, or mean (range).
Table 2—Hematological characteristics of the different patient groups
DN(anemic)
DN(nonanemic) GN
n 13 14 26Sex (M:F) 2:11 8:6 16:10Age (years) 41.3 6 11.2 41.1 6 5.1 45.0 6 11.9Diabetes duration (years) 25 6 12 30 6 9 —HbA1c (%) 11.3 6 2.1 10.5 6 2.1 —Hb (g/dl) 10.6 6 0.9 (8.7–12.0)† 13.7 6 1.1 (11.8–15.1)† 13.7 6 1.4 (11.6–16.3)EPO (IU/l) 8.1 (2.5–19.0) 8.5 (2.5–17.5) 8.5 (2.5–17.0)Mean corpuscular volume (fl) 87.3 6 5.8 88.5 6 4.3 89.4 6 4.0Mean corpuscular Hb (pg) 28.7 6 1.8 29.8 6 1.7 29.4 6 2.0B12 (pmol/l) 410.6 6 137.9 — —Folate (nmol/l) 18.1 6 7.0 — —Ferritin (ng/ml) 70.3 6 52.9 — —Proteinuria (mg/day) 2,536 (130–5,190)‡ 579 (120–2,876)‡ 1,874 (349–5,005)Creatinine (mmol/l) 110 (63–160) 88 (64–133) 93 (49–180)
Data are n, means 6 SD, means 6 SD (range), or median (range). *Our published data used here as reference data (5). †P , 0.0001; ‡P 5 0.01.
Erythropoietin deficiency in diabetic nephropathy
496 DIABETES CARE, VOLUME 24, NUMBER 3, MARCH 2001

EPO with Hb was expressed by regressionof the natural logarithm of EPO (lnEPO)on Hb of the DN group compared withthe control group. The predictive powerof the model was measured by percentagevariance of lnEPO explained by variationin Hb and group membership. We per-formed t tests to determine whether theregression lines differed (in slope and in-tercept) and whether the individualslopes differed from zero. Significancewas defined as P , 0.05.
RESULTS — We identified 27 patientswith type 1 diabetes and nephropathy. Allof the patients had proteinuria (1,086mg/day, range 120 –5,190), but nonewere in severe renal failure (creatinine 96mmol/l, 63–160). The 26 patients withGN had similar levels of renal function interms of proteinuria (1,874 mg/day, 349–5,005) and creatinine (93 mmol/l, 49–180). Proteinuria exceeded 3.5 g/day inonly two of the DN patients and four ofthe GN subjects, but none had a low se-rum albumin. There was no significantdifference between the characteristics ofthe two groups (Table 1).
Of the diabetic patients with DN, 13were found to be anemic (Hb 10.6 6 0.9g/dl). The anemia was normochromic andnormocytic, as evidenced by a normalmean corpuscular volume and mean cor-puscular Hb (87.3 6 5.8 fl and 28.7 61.8 pg, respectively). There was no evi-dence of any hematinic deficiencies suchas iron, B12, or folate to explain the ane-mia. In marked contrast, none of the 26
patients with GN were found to be anemic(Hb 13.7 6 1.4 g/dl); therefore, by impli-cation, they were not EPO deficient, de-spite having the same severity of renaldisease and use of ACE inhibition. Of the26 GN patients, 17 had serum EPO levelsof 8.5 IU/l (2.5–17.0), which is in the nor-mal range for nonanemic subjects. SerumEPO levels were not measured in nine ofthe GN patients because of logistical
problems in outlying clinics. The hema-tological characteristics of the groups areshown in Table 2.
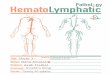
The serum EPO levels in the anemicDN patients were found to be inappropri-ately low compared with the results froma control group of iron-deficient anemicsubjects (5). In comparing the regressionlines for the whole DN group with thoseof the nonanemic and anemic controlgroup, we found a difference in the slopeof lnEPO in relation to Hb (t 5 25.359,df 5 62, P , 0.001) when allowing non-parallel regression lines in the model. Themodel was able to explain r2 5 72.7% ofthe variation in lnEPO. There was no ev-idence at the 5% level of an EPO responseto falling Hb in the DN group (t 520.522, P 5 0.604, 95% CI for the slope0.166–0.098). In contrast, in the controlgroup, lnEPO increased by 0.46 for a fallof 1 g/dl in Hb (P 5 0.001; 95% CI forslope [20.55 to 20.36]) (5). Thus, in thecontrol group, the serum EPO levels roseappropriately with a decreasing Hb,whereas there was no appropriate rise inEPO with decreasing Hb concentrationsin the DN group (Fig. 1).
The DN groups were reviewed to de-termine whether there were any addi-tional factors to explain the anemia. Therewas no difference in age, duration of dia-
Figure 1—Relationship between the natural logarithm of serum EPO and Hb concentrations in 26of 27 DN patients (l) compared with nonanemic and microcytic anemic control subjects (V)(one nonanemic DN patient not shown because serum EPO value not available). The best fittingregression lines are illustrated with solid and dotted lines, which are significantly different in bothslope and intercept (P , 0.001). The dotted line shows the normal relationship of lnEPO to Hb inthe control subjects, with a significant rise in EPO with decreasing Hb. This relationship is notfound in the DN group.
Table 2—Continued
Nondiabetic(anemic)*
Nondiabetic(nonanemic)* Normal values
14 18 —4:10 3:15 —
46.7 6 15.3 41.1 6 10.8 —— — —— — 3.8–6.4
9.3 6 1.3 (6.9–11.6) 13.5 6 0.8 (12.0–14.8) 11.5–15.557.7 (29.2–195.8) 6.6 (2.5–12.9) 3.3–16.6
69.9 6 4.8 91.7 6 2.8 79–9621.3 6 2.2 31.1 6 1.5 27–32
— — 165–835— — 7.0–28.1— — 10–200— — ,30
68 (59–148) 97 (51–108) 45–120
Bosman and Associates
DIABETES CARE, VOLUME 24, NUMBER 3, MARCH 2001 497

betes, or glycemic control between theanemic and nonanemic patients. TheHbA1c was high in many of the patientswith DN, indicating the protracted poorcontrol of these patients. There was a fe-male preponderance in the anemic group(2 males vs. 11 females), but this was notevident in the nonanemic DN subjects (8males vs. 6 females) The small differencesin serum creatinine did not reach statisti-cal significance (110 mmol/l [63–160] vs.88 mmol/l [64–133]). There was no dif-ference in the use of ACE inhibitors be-tween the groups (9 of 13 vs. 13 of 14).However, the anemic group had worseproteinuria (2,536 mg/day [130–5,190]vs. 579 mg/day [120–2,876]) than thenonanemic group (P 5 0.01).
Both groups of diabetic patients hadevidence of peripheral and autonomicneuropathy (Table 3), although none ofthe patients had symptomatic disease.Nerve function is known to deterioratewith age. The mean age of both groups issimilar, and thus the results of the neu-ropathy assessments of both groups canbe compared. There was evidence of im-paired vibration perception and monofil-ament perception in both groups,indicating impaired large-fiber function.Strikingly, the anemic group had evi-dence of more severely impaired thermalperception (P 5 0.04). Both groupsshowed evidence of cardiac autonomicdysfunction with impaired heart rate vari-ation (parasympathetic dysfunction). Al-though both groups showed impairedheart rate increase on standing (sympa-thetic dysfunction), this was worse in theanemic group (P 5 0.028). The anemicgroup had evidence of some postural hy-potension, which was more severe than inthe nonanemic group (P 5 0.003). Thisdid not reach the severity classified asclinically relevant (17); however, it didsuggest more severe sympathetic dys-
function in the anemic group comparedwith the nonanemic group.
CONCLUSIONS — We have shownthat some type 1 diabetic patients withDN but without severe renal function im-pairment are anemic (normochromic andnormocytic) and that this is associatedwith a relative EPO deficiency. This is insharp contrast to the nondiabetic patientswith a similar degree of renal damage(similar levels of proteinuria and creati-nine), who did not develop anemia at thesame stage of the disease. This anemia ofearly DN has long been suspected by cli-nicians but not documented. We cannotexplain the apparent female preponder-ance; all of these subjects had a normo-chromic normocytic blood profile with anormal serum ferritin level, thus exclud-ing iron deficiency. Given the remote pos-sibility that the anemia may have hadsome other cause in these female patients,our study still shows that they are EPOdeficient. Thus, EPO deficiency appearsto occur early in diabetic renal disease.
The anemia of chronic renal failureis not normally observed until the glo-merular filtration rate drops to ,20 – 40ml/min, which is equivalent to a serumcreatinine of greater than ;177 mmol/l(18,19). The mechanisms that may con-tribute to this anemia include shortenedred cell survival, decreased EPO produc-tion, blood loss because of defective plate-let function, and impaired erythropoiesissecondary to inhibitors or toxic metabo-lites (20). The major explanation, how-ever, is a relative EPO deficiency resultingfrom an inability of the renal fibroblasts toproduce EPO to maintain the red cellmass in response to tissue hypoxia. As therenal function deteriorates, the anemiabecomes more marked. The anemia char-acteristically responds to exogenous EPOadministration in the form of recombi-
nant human EPO in the presence of ade-quate iron replacement (21–23).
Anemia and EPO deficiency are notusually seen during the early stages of re-nal disease, and they did not occur in thenondiabetic patients with GN describedin this study. The exception to this is thenephrotic syndrome, where it is specu-lated that EPO deficiency results from theseverity of proteinuria, leading to reducedEPO production and an excessive loss ofEPO in the urine (24–26). None of thepatients in this study had nephrotic syn-drome.
In some patients, ACE inhibitors maycause a small decrease in serum EPO lev-els with a nonsignificant reduction in Hb(mean 0.27 g/dl) (28). ACE inhibitorswere used in the majority of patients inboth groups; however, it is unlikely thattheir use can therefore account for theanemia in the diabetic patients, and 4 ofthe 13 anemic DN patients were not usingACE inhibitors.
EPO deficiency and anemia can arisein a number of chronic diseases, includ-ing HIV and rheumatoid disease (2,27).Thus, other possible explanations for thefailure of adequate EPO production inearly DN include cytokine inhibition ofEPO production or a failure of the oxy-gen-sensing mechanism, which triggersthe production of EPO synthesis. Cyto-kine inhibition of the EPO receptor hasbeen proposed as an explanation for theanemia with EPO deficiency that resultsfrom rheumatoid disease and other auto-immune diseases. One plausible explana-tion for inappropriately low EPO in renaldisease (based on in vitro work in hepa-toma cells) is immunomodulatory cyto-kine inhibition of EPO formation (29).Type 1 diabetes is closely associated withother autoimmune diseases in which cy-tokine release might be elevated.
In conclusion, EPO-deficient anemiacan be observed prematurely in patientswith type 1 diabetes and DN before theonset of advanced renal failure and in theabsence of nephrotic syndrome. This is incontrast to other renal diseases of similarseverity in which anemia is not normallyfound. The mechanisms for the failure ofappropriate EPO production have notbeen characterized, but a contributingfactor may be renal denervation second-ary to diabetic autonomic neuropathy inthe presence of damaged EPO-producingfibroblasts in the renal cortex.
Table 3—Results of peripheral and autonomic nerve function tests
Abnormalvalues
DNanemic
DNnonanemic P
Vibration perception $15 33.4 6 17.9 22.1 6 13.6 —Monofilament ,5/5 2 6 2 4 6 1 —Thermal thresholds (°C) .10 23.3 6 7.3 16.9 6 7.6 0.04Heart rate variation (beats/min) ,10 6.0 6 5.7 6.6 6 4.1 —Heart rate increase on standing ,12 6.0 6 5.7 10.9 6 3.6 0.028Systolic blood pressure drop (mmHg) .20 13.0 6 9.2 2.2 6 3.8 0.003
Data are means 6 SD. Abnormal values according to Purewal et al. (15).
Erythropoietin deficiency in diabetic nephropathy
498 DIABETES CARE, VOLUME 24, NUMBER 3, MARCH 2001

Acknowledgments— This study was sup-ported by a grant from the British DiabeticAssociation.
The authors are grateful to Sabina Landau,Department of Biostatistics and Computing,Institute of Psychiatry, Decrespigny Park, Lon-don, for statistical advice.
References1. Schuster SJ, Koury ST, Bohrer M, Sal-
ceda S, Caro J: Cellular sites of extrare-nal and renal erythropoietin productionin anemic rats. Br J Haematol 81:153–159, 1992
2. Jelkmann W, Metzen E: Erythropoietin inthe control of red cell production (Re-view). Anat Anz 178:391–403, 1996
3. Bachmann S, Le Hir M, Eckhardt KU: Co-localisation of erythropoietin mRNA andecto-59-nucleotidase immunoreactivity inperitubular cells of rat renal cortex indi-cates that fibroblasts produce erythropoi-etin. J Histochem Cytochem 41:335–341,1993
4. Ricerca BM, Todaro L, Caputo S, Cotro-neo P, Damiani P, Manto A, Pitocco D,Storti S, Ghirlanda G: Blunted erythropoi-etin response to anemia in type 1 diabeticpatients (Letter). Diabetes Care 22:647,1999
5. Winkler AS, Marsden J, Chaudhuri KR,Hambley H, Watkins PJ: Erythropoietindepletion and anemia in diabetes melli-tus. Diabet Med 16:813–819, 1999
6. Beynon G: The influence of the auto-nomic nervous system in the control ofthe erythropoietin secretion in the hy-poxic rat. J Physiol 266:347–360, 1977
7. Spannhake EWM, Fisher JW: Partial inhi-bition of hypoxia-induced erythropoietinproduction by cholinergic blockade in thedog. Proc Soc Exp Biol Med 156:19–23,1977
8. Takaku F, Hirasima K, Okinaka S: Effectsof the bilateral section of the splanchnicnerve in erythropoiesis. Nature 191:500–501, 1961
9. Biaggioni I, Robertson D, Krantz S, JonesM, Haile V: The anemia of primary auto-nomic failure and its reversal with eryth-ropoietin. Ann Intern Med 121:181–186,1994
10. Fink GD, Fisher JW: Stimulation of eryth-ropoiesis by b adrenergic agonists. II.Mechanisms of action. J Pharmacol ExpTher 202:199–208, 1977
11. Zivny J, Ostadal B, Neuwirt J, PrtochazkaJ, Pelouch V: Effect of b adrenergic block-ing agents on erythropoiesis in rats.J Pharmacol Exp Ther 226:222–225, 1983
12. Fioretto P, Mauer M, Brocco E, Velussi M,Frigato F, Muollo B, Sambataro M, Abat-erusso C, Baggio B, Crepaldi G, NosadiniR: Patterns of renal injury in NIDDM pa-tients with microalbuminuria. Diabetolo-gia 39:1569–1576, 1996
13. Guy RJC, Richards F, Edmonds ME,Watkins PJ: Diabetic autonomic retinop-athy and iritis: an association suggestingan immunological cause. Br Med J 189:343–345, 1984
14. Cotes PM, Brozovic B: Diurnal variation ofserum immunoreactive erythropoietin ina normal subject. Clin Endocrinol (Oxf) 17:419–422, 1982
15. Purewal TS, Edmonds ME, Watkins PJ:Clinical assessment of neuropathy, vascu-lar disease and the leg in diabetes. In Di-abetes Forum V: Research Methodologies inHuman Diabetes. Pt. 2. Mogensen CE,Standl E, de Gruyter W, Eds. 1995, p.247–287
16. Ewing DJ: Analysis of heart rate variabilityand other noninvasive tests with specialreference to diabetes mellitus. In Auto-nomic Failure: A Textbook of Clinical Disor-ders of the Autonomic System. Bannister R,Mathias CJ, Eds. Oxford, U.K., OxfordUniversity Press, 1992, p. 312–333
17. Robertson D, Low PA, Polinsky RJ: Amer-ican Autonomic Society and the AmericanAcademy of Neurology: consensus state-ment on the definition of orthostatic hy-potension, pure autonomic failure andmultiple system atrophy. In Primer on theAutonomic Nervous System. 1st ed. San Di-ego, CA, Academic Press, 1996, p. 334–336
18. Chandra M, Clemons GK, McVicar MI:Relation of serum erythropoietin levels torenal excretory function: evidence forlowered set point for erythropoietin pro-duction in chronic renal failure. J Pediatr113:1015–1021, 1988
19. Ratke HW, Claussner A, Erbes PM,Scheuermann EH, Scheppe W, Koch KM:Serum erythropoietin concentration inchronic renal failure: relationship to de-gree of anemia and excretory renal func-tion. Blood 54:877–884, 1979
20. Eschbach JW, Adamson JW: Modern as-pects of the pathophysiology of renal ane-mia (Review). Contrib Nephrol 66:63–70,1988
21. Bayes B, Serra A, Junca J, Lauzurica R:Successful treatment of anemia of ne-phrotic syndrome with recombinanterythropoietin. Nephrol Dial Transplant13:1894–1895, 1998
22. Gansevoort RT, Vaziri ND, de Jong PE:Treatment of anemia of nephrotic syn-drome with recombinant erythropoietin.Am J Kidney Dis 28:274–277, 1996
23. Ishimitsu T, Ono H, Sugiyama M,Asakawa H, Oka K, Numabe A, Abe M,Matsoka H, Yagi S: Successful erythro-poietin treatment for severe anemia innephrotic syndrome without renal dys-function. Nephron 74:607–610, 1996
24. Kaysen G: Nonrenal complications of thenephrotic syndrome. Annu Rev Med 45:201–210, 1994
25. Vaziri ND: Endocrinological conse-quences of the nephrotic syndrome. Am JNephrol 13:360–364, 1993
26. Vaziri ND, Kaupke CJ, Barton CH,Gonzales E: Plasma concentration and theurinary excretion of erythropoietin inadult nephrotic syndrome. Am J Med 92:35–40, 1992
27. Means RT, Krantz SB: Progress in under-standing the pathogenesis of the anemiaof chronic disease. Blood 80:1639–1647,1992
28. Pratt MC, Lewis-Barnard NJ, Walker RJ,Bailey RR, Shand BI, Livesey J: Effect ofangiotensin converting enzyme inhibitorson erythropoietin concentrations inhealthy volunteers. Br J Clin Pharmacol 34:363–365, 1992
29. Eckardt KU: Erythropoietin: oxygen-de-pendent control of erythropoiesis and itsfailure in renal disease: seminars in renalphysiology (Review). Nephron 67:7–23,1994
Bosman and Associates
DIABETES CARE, VOLUME 24, NUMBER 3, MARCH 2001 499