-
7/27/2019 Anatomy of Tracheostomy
1/4
Related Questions:
Anatomy of tracheostomy, cricothyrotomy... Describe the anatomy
of the larynx. What is the nerve supply? Candidates must be able to
demonstrate their knowledge of practical invasive
procedures, with an understanding of the principles and hazards
involved.
Emergency airway management including tracheostomy Describe the
technique of percutaneous tracheostomy, including all the
relevant
anatomy. What are the complications?
Anatomy of the larynx
The larynx is a valve separating the trachea from the upper
aerodigestive tract. It is
primarily thought of as an organ of communication but it is also
an important regulator of
respiration, and is necessary for an effective cough or valsalva
manoeuvre, and prevents
aspiration during swallowing.
Skeleton
Hyoid bone - attachment to epiglottis and strap muscles. Thyroid
cartilage - anterior attachment of vocal folds. Posterior
articulation with cricoid
cartilage.
Cricoid cartilage - complete ring. Articulates with thyroid and
arytenoid cartilages. Arytenoids - two cartilages which glide along
the posterior cricoid and attach to
posterior ends of vocal folds.
-
7/27/2019 Anatomy of Tracheostomy
2/4
Divisions
Supraglottis - usually covered with respiratory epithelium
containing mucous glands. Epiglottis - leaf-shaped mucosal-covered
cartilage, which projects over larynx. Aryepiglottic folds - extend
from the lateral epiglottis to the arytenoids. False vocal cords -
mucosal folds superior to the true glottis. Separated from true
vocal folds by the ventricle.
Ventricle - mucosal-lined sac, variable in size, which separates
the supraglottis fromthe glottis.
Glottis - the true vocal folds attach to the thyroid cartilage
at the anteriorcommissure. The posterior commissure is mobile, as
the vocal folds attach to the
arytenoids. Motion of the arytenoids affects abduction or
adduction of the larynx. The
bulk of the vocal fold is made up of muscle covered by mucosa.
The free edge is
characterised by stratified squamous epithelium. The vocal folds
abduct for inspiration
and adduct for phonation, cough and valsalva.
Subglottis - below the vocal folds, extending to the inferior
border of the cricoidcartilage.
Innervation
Branches of the vagus nerve. Superior laryngeal nerve -
sensation of the glottis and supraglottis. Motor fibres to
the cricothyroid muscle, which tenses the vocal folds. This
nerve leaves the vagus high
in the neck.
Recurrent laryngeal nerve - sensation of the subglottis, and
motor fibres to intrinsicmuscles of the larynx. This nerve branches
from the vagus in the mediastinum, thenturns back up into the neck.
On the right, it travels inferior to the subclavian artery,
and on the left, the aorta.
-
7/27/2019 Anatomy of Tracheostomy
3/4
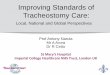
Equipment: The percutaneous tracheostomy set illustrated is
manufactured by Portex,
although other sets are available. It consists of a
Seldinger-type needle and wire, over which
a guide and then a single one-step dilator is passed. In
addition to the equipment given, one
also needs :
Sterile field and cleaning fluid
Lubricating jelly
Local anaesthetic with adrenaline
Tracheal dilator
Fibreoptic laryngoscope/bronchoscope
Catheter mount to accept scope
Intravenous anaesthesia
One-step percutaneous tracheostomy kit
Airway management
Although inhalation anaesthesia is possible, a total intravenous
technique provides
much smoother anaesthesia and better conditions for performing
the bronchoscopy and
tracheostomy. A combined propofol and opioid technique is a
favoured option. Full monitoring
is instituted, and ventilatory parameters altered during the
bronchoscopy to maintain
adequate oxygenation and end-tidal CO2 levels.
Following induction of anaesthesia, the patient is prepped and
draped. The bronchoscope is
passed through a tracheal tube and the anatomy of the airway
visualised. The aim of the
fibreoptic scope is to ensure correct initial placement of the
introducer needle, in the midline
and through the second or third tracheal rings. Subsequent to
this, it will monitor dilation of
the trachea, and ensure that the introducer does not remain in
the trachea.
Landmarks
Although not necessary for the procedure, information from
bronchoscopy is very useful and it should always be used
when
learning the technique.
The patient is positioned with the neck extended, with an
intravenous
fluid bag between the shoulder blades and the head in a head
ring.
This brings as much of the trachea as possible into the
neck.
The larynx and cricoid cartilage with the intervening
cricothyroid
membrane are identified. From the cricoid, moving caudally,
the
tracheal rings are identified. The tracheostomy should ideally
pass
between the second and third tracheal rings, although a space
one
higher or lower may be employed. Placing the airway higher, next
tothe cricoid, can cause tracheal erosion and long-term
problems.
http://www.frca.co.uk/article.aspx?articleid=243http://www.frca.co.uk/article.aspx?articleid=243
-
7/27/2019 Anatomy of Tracheostomy
4/4
Technique: Seldinger method
Local anaesthetic with adrenaline is infiltrated subcutaneously,
and a 1 cm incision made
horizontally with a scalpel. Keeping in the midline at all
times, the introducer needle and
syringe are advanced, at 45 degrees to the skin, until air is
aspirated from the trachea.
The guide wire is passed through the needle, then the small
dilator (green) is passed. This is
then removed and the white introducer passed into the trachea.
The guidewire is removed.
Now only the white introducer is left in the trachea. Over this
the tracheal dilator(s) (blue)
are passed in order, gradually dilating the incision to
accommodate the appropriately sized
tracheostomy tube. Plenty of lubricating jelly is applied to
each dilator, and they are passed
down the tract with a twisting motion. Only moderate downward
force is applied. If the dilator
does not pass easily, return to the previous smaller dilator and
ensure that it passes freely
and easily. Often, it is the skin that impedes progress, and the
incision has to be slightly
widened with the scalpel. The portex kit consists of a one-step
dilatation.
Each size of tracheostomy tube has a corresponding dilator size
(see the manufacturers'
instructions), and this should pass freely and easily into the
trachea before attempting to
insert the tracheostomy tube. Once the tracheostomy will easily
accept the final dilator, the
tracheostomy tube (cuff already checked) is loaded onto the
dilator one size lower. The
tracheal tube is wathdrawn, under direct vision, into the
larynx, and the tracheostomy tube is
passed over the introducer into the trachea. Once again, undue
force should not be
necessary. Use plenty of jelly and, if required, return to the
previous dilator.
The use of the tracheal dilator instruments is rarely necessary,
and may be hazardous.
However, if the introducer is inadvertently pulled out of the
trachea, or some other mishap
occurs, they may be useful in relocating the tract for
replacement.
With the tracheostomy tube in place, the tracheal tube is
removed and the ventilator isconnected to the tracheostomy. The
chest is auscultated for adequate ventilation and the
ventilator checked for appropriate tidal volumes and airway
pressures. The tube is secured
with tapes or ties.
References
1. Elective percutaneous dilatational tracheostomy. A new simple
bedside procedure;preliminary report. Ciaglia P, Firsching R,
Syniec C.Chest 1985; 87: 715-19.
2. Percutaneous endoscopic tracheostomy. Paul A et al.Ann Thorac
Surg 1989; 47: 314-15.
3. Percutaneous dilatational tracheostomy. Results and long-term
follow-up [seecomments]. Ciaglia P, Graniero KD.Chest 1992; 101:
464-7.
http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=3996056http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=3996056http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=1735273http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=1735273http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=1735273http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=1735273http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=2919922http://http/www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=3996056