Embed Size (px)
Citation preview

ANATOMY
© 2005 The Medicine Publishing Company Ltd217ANAESTHESIA AND INTENSIVE CARE MEDICINE 6:7
Pharynx
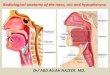
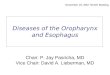
The pharynx, a muscular tube about 14 cm long, extends from the skull base to the level of the sixth cervical vertebra, where it becomes the oesophagus. It lies behind the nose, mouth and larynx and communicates with each; it is divided into the naso-, oro- and laryngopharynx (Figure 1). Posteriorly it lies on the pre-vertebral fascia and muscles; laterally, from above downwards, it is related, to the auditory tube, the styloid process and its muscles, the carotid sheath and its contents, and the thyroid gland. Its walls have mucous, submucous and muscular coats. The mucous coat is continuous with those of the nose, auditory tube, oral cavity, larynx and oesophagus; in the nasopharynx it is lined with respiratory epithelium, and elsewhere with stratified squamous epithelium. The muscular coat comprises the superior, middle and inferior constrictor muscles, blending with and reinforced by salpingo-, stylo- and palatopharyngeus muscles. Each constrictor fans out from its anterior attachment and passes posteriorly around the pharynx to join its opposite fellow in a fibrous midline raphe, which extends from the occipital bone to the oesophagus. The pairs of muscles overlap; the inferior lies outside the middle, which is outside the superior constrictor. All pharyngeal muscles are concerned in swallowing and are supplied by the vagus and cranial accessory nerves via the pha-ryngeal plexus, apart from stylopharyngeus, which is supplied directly by the glossopharyngeal nerve.
NasopharynxThe nasopharynx lies behind the two posterior nasal openings (choanae) above the soft palate, which, during swallowing, con-tract to cut off the nasopharynx from the oropharynx. On each lateral wall are the openings of the auditory tube. Posteriorly, a small aggregation of lymphoid tissue, the nasopharyngeal tonsils (adenoids), is present. The nasopharynx is limited superiorly by the base of the skull; below it communicates with the oropharynx through the pharyngeal isthmus, a constriction that can be closed by the mobile soft palate. The nasopharynx is readily inspected by a mirror passed to the back of the tongue.
OropharynxThe oropharynx extends down to the upper border of the epiglot-tis, where it is continuous with the laryngopharynx. Anteriorly it communicates through the faucial isthmus or fauces with the oral cavity. Below the isthmus is the tongue, partly in the pharynx and partly in the oral cavity. In the lateral wall of the isthmus there are two vertical folds of mucous membrane, the anterior and posterior arches of the fauces, formed by palatoglossus and palatopharyngeus (Figure 2). The palatine tonsil, more commonly known as the ‘tonsil’, lies between them.
Lymphatic drainageThe nasopharynx drains to the retropharyngeal nodes, the remain-der of the pharynx to the deep cervical nodes. Aggregations of lymph tissue surround the upper part of the pharynx: the palatine tonsil below the soft palate, the lingual tonsil in the posterior tongue, the tubal tonsil around the opening of the auditory tube and the nasopharyngeal tonsil (adenoids) in the roof and posterior wall of the nasopharynx. The adenoids and tubal tonsils of young children are prone to infection and enlargement, and the resultant swelling may cause blockage of the auditory (Eustachian) tube. This results in infection of the middle ear (otitis media) and is often the cause of mouth-breathing and nasal speech. Surgical removal of tonsils and adenoids must occasionally be performed to improve hearing and poor behaviour caused by ‘glue ear’.
Palatine tonsilThe tonsil (palatine tonsil) is a body of lymph tissue in the fossa on the lateral wall of the fauces, oval in shape, with upper and lower poles. Its size varies, but it is always larger in children. A well-marked supratonsillar cleft lies between the upper pole and the upper wall of the fossa. The deep surface of the tonsil is attached to a fibrous capsule, which separates it from the superior constrictor muscle and facial artery. The tonsil’s blood vessels
Anatomy of the naso- and oropharynxJohn Craven
John Craven was formerly Consultant Surgeon at York District Hospital,
York, UK. He is past chairman of the primary examiners of the Royal
College of Surgeons of England.
1
Sagittal view showing parts of the pharynx
Nasal cavity
Hard palate
Tongue
Epiglottis
Trachea
Nasal part
Oral part
Laryngeal part
Opening of auditory tube
Soft palate
Pharynx

ANATOMY
© 2005 The Medicine Publishing Company Ltd218ANAESTHESIA AND INTENSIVE CARE MEDICINE 6:7
enter it inferiorly. Anteriorly lies the palatoglossal arch, posteriorly the palatopharyngeal arch. Above it is the soft palate and below it is the tongue.
Blood supply is from the tonsillar branches of the facial, lingual and ascending pharyngeal arteries. The veins drain to the pha-ryngeal venous plexus.
Lymphatic drainage is to the deep cervical chain, particularly the jugulodigastric node. Infection of the palatine tonsils is common in children. The gland is seen to be swollen and its surface marked by exudates of pus. Pain is often referred to the ear (referred otalgia) via the glossopharyngeal nerve, which lies in the tonsil-lar bed, and swallowing is difficult because of the pain. Rarely it may develop into peritonsillar abscess (quinsy), which requires surgical intervention.
Auditory tubeThe auditory (Eustachian) tube passes from the lateral pharyngeal wall at the level of the soft palate to the middle ear. It is about 4 cm long and directed upwards, backwards and laterally. The lateral third lies within the temporal bone; the remainder is largely carti-laginous and completed by fibrous tissue. The pharyngeal branch of the maxillary nerve supplies it. Its lymph vessels drain to the retropharyngeal nodes. The tube passes between the middle ear and nasopharynx and serves to equalize the pressure on the two sides of the tympanic membrane. In children, the tube is wider and more horizontal, and thus infection is more likely to spread from the nasopharynx to the slower-draining middle ear.
FURTHER READINGAbrahams P, Craven J, Lumley J. Illustrated clinical anatomy. London:
Hodder Arnold, 2005.
2
Pillars of the fauces
UvulaHard palate
Soft palate
Palatinetonsil
Tongue
Posterior wall of oropharynx
Palatopharyngeal arch
Palatoglossal arch
Anterior view of the larynx
C3
Vertebral levels
C4
C6
T2/3
Hyoid
Carotid bifurcation
Thyroid notch
Thyroid cartilage
Cricoid cartilage
Isthmus of thyroid
Suprasternal notch