Embed Size (px)
Citation preview

Anatomy, Embryology, and Physiology of the LiverDr. Nicholas Smith
Liverpool Hospital
2014

Historical Developments
• “Now, why is the stomach surrounded by the liver? Is it in order that the liver may warm it and it may in turn warm the food? This is indeed the very reason why it is closely clasped by the lobes of the liver, as if by fingers." -- Galen, ca. 200 A.D.

• 1887: First liver resection performed by Carl Lengenbeck• 1908: J Hogarth Pringle ‘Pringle maneovre’• 1911: Walter Wendell Right Hemihepatectomy• 1952: Jean Louis Lortat-Jacob Extended Right
Hemihepatectomy• World War I and II• “At present, liver resections are based upon the precise
knowledge of the natural lines of division of the liver which define the anatomical surgery of the liver”
Henri Bismuth

• Ton That Tung 1936• Claude Couinaud 1957• Le Foie: Études anatomiques et chirurgicales (The
Liver: Anatomic and Surgical Studies 1957)-Claude Couinaud (1922–2008)

Anatomy of the Liver
- Largest gland in the body 1500g- Lies in the RUQ under the rib cage- Right border: 5th rib-ribs 7-11 right midaxillary line- Left border: left 5th intercostal space 8cm from midline- Inferior border along the right costal margin and crosses
the midline between the costal margins beneath the xiphisternum

• 2 surfaces• Superior/diaphragmatic: convex, moulded to shape
beneath diaphragm, subphrenic space usually potential• Inferior/visceral surface: contains the hilum/porta hepatis,
GB fossa, contact impregnations with esophagus/duodenum/right colon/right kidney/right adrenal gland
• Suphepatic space/Morrison’s pouch

• Falciform ligament-- Inferior edge contains ligamentum teres and remains of
left umbilical vein- Connects abdominal wall to the liver from umbilicus to
liver surface- Continues posteriorly as ligamentum venosum- Contained in umbilical fissure and fissure for ligamentum
venosum

• Glisson’s capsule• Ligaments:• Falciform ligamantsplits at umbilical fissure to upper leaf
of right coronary ligament and left triangular ligament• Right apex of the upper leaf of the right coronary ligament is
the right triangular ligamentcontinues medially as the lower leaf the right coronary ligament
• Bare area between upper and lower leafs of right coronary ligament contains IVC and is in contact with diaphragm

• Continues to the left at ligamentum venosum• Forms posterior layer of lesser omentum at porta hepatis• Anterior layer of lesser omentum returns and completes
liver circle at left triangular ligament• Lesser omentum= hepatoduodenal and hepatogastric
ligaments

• Ligaments help stabilize the liver, but there division at surgery for mobilization does not allow liver to be displaced
• Liver is held in place by hepatic vein connections to IVC


• Liver is morphologically divided into a large right lobe and a smaller left lobe by the falciform ligament
• Viewed from the inferior side an ‘H’ is formed:- Right anterior limb=GB- Right posterior limb=IVC- Left anterior limb=falciform ligament- Left posterior limb=ligamentum venosum

• Between the right anterior and posterior lobes is the quadrate lobe
• Between the left anterior and posterior lobes is the caudate lobe



• Cournaud in 1957 proved the liver was divided by its arterial/portal venous/biliary ductal system into functional right and left lobes
• Increased anatomical knowledge allowed for precise resectional surgery on the liver

• Plane of division lies along Cantlie’s line• GB fossa anteriorly to IVC posteriorly• Quadrate lobe becomes part of left hemiliver instead of
right hemiliver• Each lobe of liver divided into 2 sectors• Right hemiliver divided into right anterior sector and
right posterior sector• Left hemiliver divided into left lateral sector and left
medial sector

• Vertical division of sectors by fissures which contain the hepatic veins
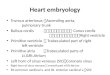
• Segment I is autonomous, posterior, receives supply from right and left hepatic arteries, right and left hepatic ducts, and has its own venous drainage to IVC
• Segment II (left lateral sector)• Left fissure containing left hepatic vein seperates
segment II from segments III(left lateral sector)

• Falciform ligament and umbilical fissure separate segments III from segment IV (left medial sector)
• Segment IV (quadrate lobe) divided superiorly segment IVa and inferiorly segment IVb (note Japanese use different classification)
• Median fissure divides right and left hemilivers (segment IV from segments V and VIII-left anterior sector)
• Median fissure contains middle hepatic vein

• Horizontal plane of right portal vein divides left anterior and posterior sectors into respective superior and inferior segments-total 4
• Right fissure divides segments V and VIII (right anterior sector) from segmens VI and VII (right posterior sector)
• Right fissure contains right heptic vein

• Total of 8 segments• 4 in each hemiliver
• With exception of caudate lobe (segment I) each liver independently receives its own arterial/portal venous/biliary supply without mixing
• Venous drainage shows a degree of mixing of both halves of the liver due middle hepatic vein





• Portal triad- Hepatic artery, portal vein, hepatic (biliary) duct- Enters the liver at the edge of lesser omentum and into
the porta hepatis- Hepatic artery is anteromedial, hepatic duct is
anterlateral, portal vein is posterior- Pringle maneovre

• At porta hepatic the portal triad divides into right and left• Further sectoral divisions• Further segmental divisions

• Hepatic artery:- Coeliac artery common hepatic artery hepatic artery
proper right and left hepatic arteries- Supplies 30% of hepatic blood supply- Oxygenated blood systemic circulation- Cystic artery to GB comes off right hepatic artery

• Portal vein- Formed by the confluence of the SMV and the splenic
vein behind the neck of the pancreas- Ascends in the porta hepatic and divides into right and
left branches- Carries nutrient-rich venous blood from the portal
circulation of the gut

• Hepatic ducts- Travel in opposite direction to hepatic artery and portal
vein- Segmental ducts sectoral ducts right and left hepatic
ducts common hepatic duct, joined by cystic duct common bile duct enters posteromedially into second portion of duodenum and joined by main pancreatic duct system
- Carries bile to GB and duodenum

• Hepatic veins• 3 of them drain into IVC• Segment I has own venous drainage• Short extrehepatic course to IVC• Left and middle hepatic veins coalesce in 20% of cases• Possible accessory hepatic veins, esp. right draining veins


• Aberrant anatomy• Definitions replaced vs. accessory• 25% people have an aberrant anatomy

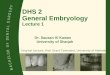
Aberrant Right Hepatic Artery• Arises from SMA, runs left to right along posterior border of bile duct• May supply a segment, section, (R) hemiliver or the whole liver• Significance = Division during biliary surgery Devascularisation liver• May also occur as an accessory (R) HA (ie normal R.HA also present)
Aberrant Left Hepatic Artery• Arises from the Left Gastric Artery & passes in lesser omentum to liver• May supply a segment, section, (R) hemiliver or the whole liver• Significance: Division of L. Gastric Artery during gastrectomy Devasc.• May also occur as an accessory (L) HA (ie normal L.HA also present)
Aberrant Hepatic Artery• Arises directly from aorta

Aberrant Right Hepatic Artery (5)• CHA - 75%• SMA – 15%• Gastroduodenal – 6%• R. Gastric – 3%• Aorta 1%• When not arising from CHA, arises from aorta or it’s right-sided branches
Aberrant Left hepatic Artery (5)• CHA – 80%• L. Gastric - 15%• Gastroduodenal – 2%• Splenic – 2%• Aorta – 1%• When not arising from CHA, arises from aorta ot it’s left-sided branches

• Aberrant biliary anatomy• RP and RA from common R 57%• · RP from bifurcation 16%• · RA from bifurcation 12%• · RP from LH 5%• · RA from LH 4%• · Absent LH 3%• · RP from cystic 2%


• Lymphatic drainage of the liver• 1/3-1/2 of total lymph is produced in the liver• Kupffer cells• Liver periportal lymph nodes perihepatic artery
retroduodenal lymph nodes coeliac nodes• Bare area nodes drain into diaphragmatic nodes
posterior mediastinal lymph nodes

• Radiological sectioning of the liver• Remember that Cournaud used the caudad view as his
reference, and the segments are numbered counterclockwise around the IVC as the arrondisements of Paris

• Nervous supply:- Symphathetic autonomic supply via coeliac nerves- Parasympathetic autonomic supply via anterior (hepatic)
branch of left (anterior) Vagas nerve



• Surgical Nomenclature

• Right lobectomy: from between falciform ligament and GB to the right, taking GB, preserving right hepatic vein +- middle hepatic vein
• Right extended lobectomy (right trisegmentectomy): above and segment IV
• Left lobectomy: left lobe +- GB with preservation of right hepatic vein +- middle hepatic vein

• IHPBA 2000 Brisbane Terminology• Hemihepatectomies, sectionectomies, segmentectomies




• Embryology of the liver• Ventral outgrowth of the foregut at 3/40 gestation forms
the hepatic diverticulum• Cranial part becomes the septum transversum• The cranial part of septum transversum becomes
peritoneal/pericardial division and diaphragm• Caudal part of septum transversum becomes ventral
mesogastrium

• Liver parenchyma develops from ventral mesogastrium• Vitilline veins invade from septum transversum forming
anastomoses-eventually forming hepatic veins• Proliferating hepatocytes from ventral mesogastrium
invaded by sinusoidal vessels draining into vitilline veins

• Original hepatic diverticular endoderm forms biliary ductal system
• Blind diverticulum of the ductal system becomes the cystic duct and GB
• In utero, maternal blood from the left umbilical vein in the ligamentes teres bypasses the liver by passing to the hepatic vein/IVC through the ductus venosus
• At birth, the ductus venosis becomes the ligamentum venosus

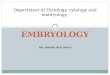
Histology of Hepatocytes



Physiology of the Liver
• Huge topic!• Carbohydrate metabolism:- Glycogenesis (glucose under action of glucokinase
converted to glucose-6-phosphate)glycogen synthaseglycogen (augmented by actions of insulin)
- Glycogenoylsis: glycogen converted to ready glucose via glycogen phosphorylase and augmented by glucagon

- gluconeogenesis: conversion of lactate, glycerol, amino acids into glucose

• Protein and amino acid synthesis, regulation, destruction

• Lipid Metabolism- Cholesterol synthesis from Acetyl CoA via HMG-CoA
Reductase- Lipogenesis (production of TAG)- Production of lipoproteins

• Formation of Bile
-breakdown of heme to biliverdin to bilirubin
-conjugated with glucuronic acid by UDP-glucuryltransferase
-formation of bile salts from cholesterol
-secretion of bile along bile caniliculi to hepatic ducts
(Note that cholestasis injures zone I, bile caniliculi lined by ALP), hence increase ALP

• Production of ALL coagulation factors, protein C, protein S, antithrombin III
• Until week 32 gestation, main organ of hematopoisis • Insulin-like growth factor I• Thrombopoitin

• Detoxification, first pass metabolism, breakdown of drugs, toxins, hormones in the smooth endoplasmic reticulum
• Urea cycle• Storage of vitamins and other minerals• Production of albumin• Production of hormone binding proteins• Production of angiotensinogen