Embed Size (px)
Citation preview

Slide 1
Anatomy and Biomechanics Anatomy and Biomechanics of the ACLof the ACL
Current Influences on (my) Current Influences on (my) Surgical TechniqueSurgical Technique
Thomas H. Myers MDThomas H. Myers MD
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2 EpidemiologyEpidemiology
1 In 3000 Americans will sustain ACL 1 In 3000 Americans will sustain ACL rupture this yearrupture this year1 in 1750 Americans aged 15y 1 in 1750 Americans aged 15y –– 45y will 45y will sustain ACL rupture this yearsustain ACL rupture this year95,000 injuries per year in United States95,000 injuries per year in United States60,000 60,000 –– 75,000 ligament reconstructions75,000 ligament reconstructionsAverage cost per reconstruction is approx. Average cost per reconstruction is approx. $17,000$17,000Financial impact close to 1 billion dollarsFinancial impact close to 1 billion dollars
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4 EpidemiologyEpidemiology
Cost of treating longCost of treating long--term complications of term complications of postpost--traumatic DJD has not been traumatic DJD has not been determined determined Average number of visits to Average number of visits to orthopaedicorthopaedicsurgeons up 28% over the last 20 years surgeons up 28% over the last 20 years (11.3 (11.3 –– 14.5 visits per 100 people)14.5 visits per 100 people)Current emphasis on health and fitnessCurrent emphasis on health and fitnessIncidence and prevalence likely to Incidence and prevalence likely to continue to increasecontinue to increase
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5
DO WE TRULY UNDERSTAND DO WE TRULY UNDERSTAND THE ANATOMY AND THE ANATOMY AND
BIOMECHANICS OF THE ACL?BIOMECHANICS OF THE ACL?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6
(5-6 mm from posterior wall of femur)
AnatomyAnatomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
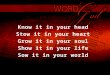
Slide 7 AnatomyAnatomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8 Anterior Cruciate LigamentAnterior Cruciate Ligament
FemurFemurThe ACL insertsThe ACL inserts
inferiorly to the roof ofinferiorly to the roof ofthe intercondylar the intercondylar
notchnotch
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
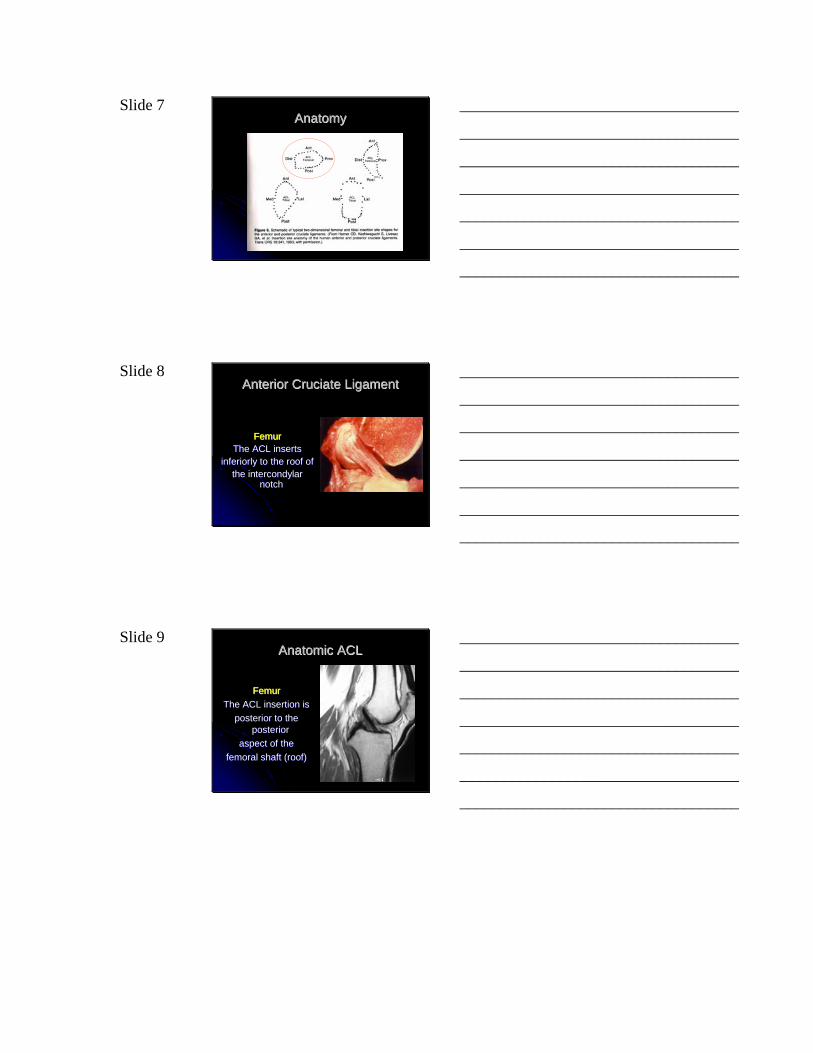
Slide 9 Anatomic ACLAnatomic ACL
FemurFemurThe ACL insertion is The ACL insertion is
posterior to the posterior to the posterior posterior
aspect of theaspect of thefemoral shaft (roof)femoral shaft (roof)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10
TibiaTibia
The ACL insertion is The ACL insertion is
In the anterior 1/3 of In the anterior 1/3 of the tibia adjacent to the tibia adjacent to
the anterior horn of the the anterior horn of the lateral meniscuslateral meniscus
AnteriorAnterior CruciateCruciate LigamentLigament
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11
Initially we failed in our attempts to Initially we failed in our attempts to repair ruptures of this ligament repair ruptures of this ligament
primarily. Now we have turned to primarily. Now we have turned to methods of ligament reconstruction.methods of ligament reconstruction.
HistoryHistory
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12
What is now the current What is now the current accepted surgical technique for accepted surgical technique for
ACL reconstruction?ACL reconstruction?
HistoryHistory
Controversial (ie There is none!)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 13
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
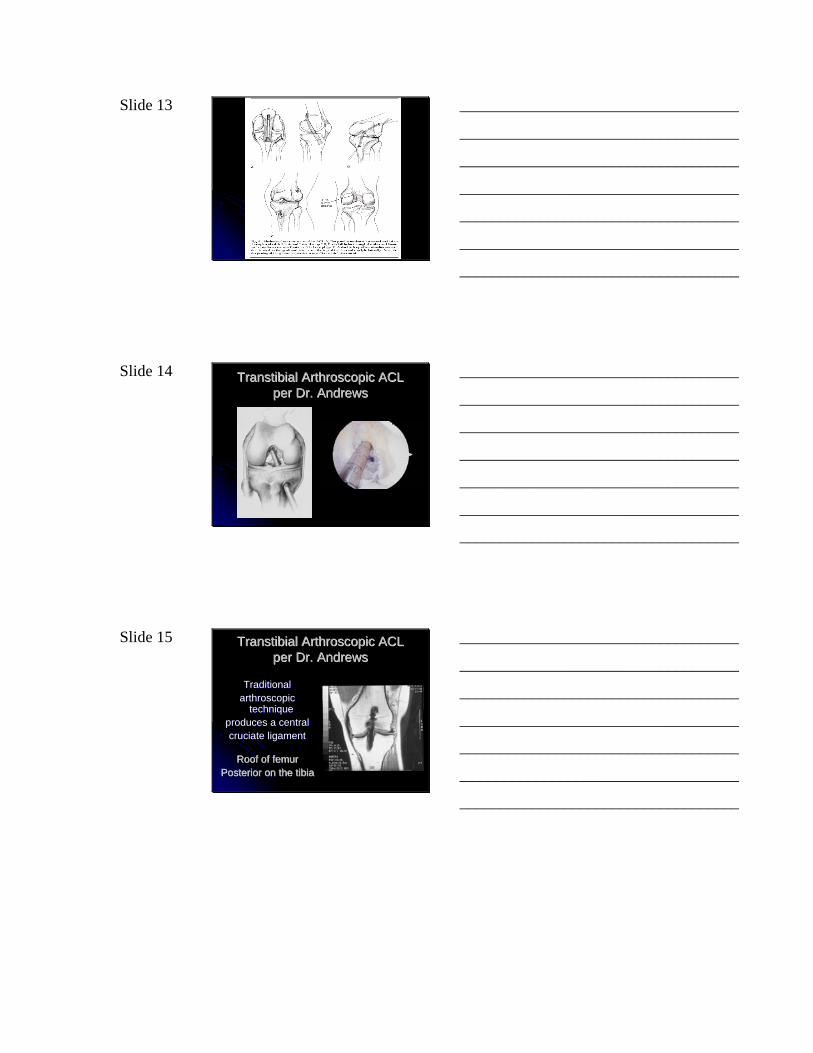
Slide 14 Transtibial ArthroscopicTranstibial Arthroscopic ACL ACL per Dr. Andrewsper Dr. Andrews
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15 Transtibial ArthroscopicTranstibial Arthroscopic ACL ACL per Dr. Andrewsper Dr. Andrews
TraditionalTraditionalarthroscopicarthroscopic
technique technique produces a centralproduces a centralcruciate ligamentcruciate ligament
Roof of femurRoof of femurPosterior on the tibiaPosterior on the tibia
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 16 Location of ACL Femoral Location of ACL Femoral TunnelTunnel
For 20 years,For 20 years,the recommended the recommended
femoral tunnel femoral tunnel placement was placement was
posteriorposteriorand superiorand superior
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17
Placement of Placement of femoral tunnel on femoral tunnel on
the roof of the the roof of the intracondylar intracondylar notch notch
(11:00 or 1:00) (11:00 or 1:00) predisposes to predisposes to
notch impingement notch impingement and possible early and possible early
graft failuregraft failure
Transtibial ArthroscopicTranstibial Arthroscopic ACL ACL per Dr. Andrewsper Dr. Andrews
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18 Location of ACL Femoral Location of ACL Femoral TunnelTunnel
Can we use a Can we use a transtibialtranstibial drilling drilling technique and move the tunnel technique and move the tunnel
down the wall of the down the wall of the intracondylarintracondylarnotch (10:00 or 2:00) closer to the notch (10:00 or 2:00) closer to the
antatomicantatomic position of the ACL position of the ACL footprint?footprint?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 19 Transtibial ArthroscopicTranstibial Arthroscopic ACL ACL per Dr. Andrewsper Dr. Andrews
It is difficult to It is difficult to move tunnel down move tunnel down the side wall due the side wall due to limited degrees to limited degrees of freedom with of freedom with drill bit in drill bit in tibial tibial
tunneltunnel
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21 Femoral Insertion Site forFemoral Insertion Site forTranstibialTranstibial ACLACL
A 10 mm reamerA 10 mm reamerangled 30º makesangled 30º makes
an 11.5 mm entrance holean 11.5 mm entrance hole
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 22 Femoral Insertion Site for Femoral Insertion Site for TranstibialTranstibial ACLACL
Neither anatomically orNeither anatomically orbiomechanically correct!biomechanically correct!
William ClancyWilliam Clancy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23 Dr. Clancy’s Anatomic Dr. Clancy’s Anatomic Endoscopic Endoscopic TechniqueTechnique
Lateral femoral tunnel Lateral femoral tunnel not made through the not made through the tibial tunneltibial tunnel
Made through the Made through the medial parapatellar medial parapatellar portalportal
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
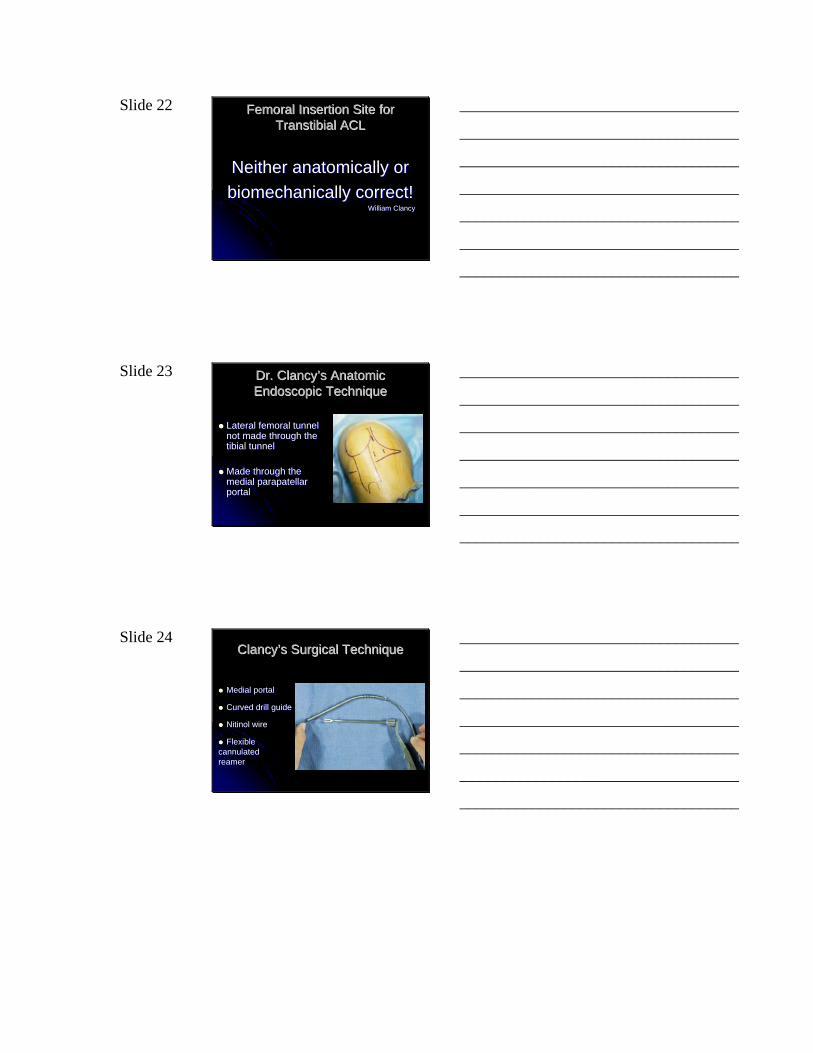
Slide 24 Clancy’s Surgical TechniqueClancy’s Surgical Technique
Medial portalMedial portal
Curved drill guideCurved drill guide
Nitinol wireNitinol wire
Flexible Flexible cannulated cannulated reamerreamer
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25 Clancy’s TechniqueClancy’s Technique
Requires flexible reamersRequires flexible reamersMedial portals Medial portals Reams 7mm diameter tunnel and requires Reams 7mm diameter tunnel and requires curetting to enlarge tunnel curetting to enlarge tunnel anteriorlyanteriorlyFemoral tunnel size and orientation limited Femoral tunnel size and orientation limited by risk of back wall compromiseby risk of back wall compromiseTechnically difficult and time consuming Technically difficult and time consuming for inexperienced surgeonsfor inexperienced surgeonsNot possible with certain femoral Not possible with certain femoral morphologymorphology
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26 Anatomic ACLAnatomic ACL
Anatomic placement of the graft Anatomic placement of the graft on the tibia and the femuron the tibia and the femur
can be achieved can be achieved most of the most of the time time ---- William ClancyWilliam Clancy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27
Allows femoral tunnel positionAllows femoral tunnel positionfurther down on wall (10:00)further down on wall (10:00)
Requires flexible reamers andRequires flexible reamers andcuretting of tunnel (7mm max)curetting of tunnel (7mm max)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 28
Produces aProduces a
Horizontal graftHorizontal graft
Controls rotationControls rotation
No notch impingementNo notch impingement
Rarely necessitates a Rarely necessitates a notchplastynotchplasty
Produces aProduces a
More vertical graftMore vertical graftTried and TrueTried and TrueFaster and EasierFaster and EasierDoes not require special Does not require special instrumentationinstrumentationDoes not limit graft tunnel sizeDoes not limit graft tunnel sizeMinimal risk of back wall Minimal risk of back wall “blowout”“blowout”
Anatomic Anatomic Endoscopic Endoscopic
ACLACLClancyClancy
TranstibialTranstibialACLACL
AndrewsAndrews
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29 Failed ACL ReconstructionFailed ACL Reconstruction
Reported longReported long--term success rates between 75% term success rates between 75% and 95%and 95%Recurrent knee instability and graft failure Recurrent knee instability and graft failure requiring revision surgery in 8%requiring revision surgery in 8%Technical errors most common cause of failure Technical errors most common cause of failure (77% of revision cases in 1 series)(77% of revision cases in 1 series)70% 70% -- 80% of technical errors are due to 80% of technical errors are due to malpositioned tunnelsmalpositioned tunnelsMost common error is improper positioning of Most common error is improper positioning of the femoral tunnelthe femoral tunnelAnterior and superiorAnterior and superior
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
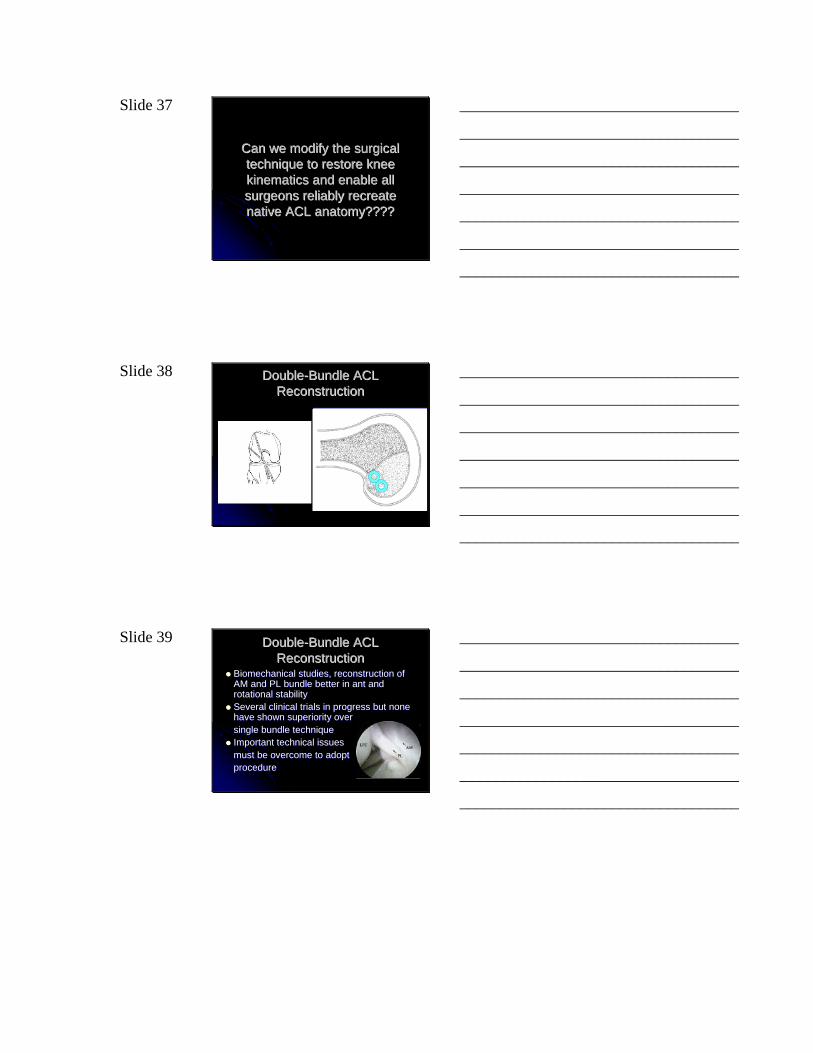
Slide 30
GetelmanGetelman MH and MH and Friedman MJ, Friedman MJ, JAAOS 1999.JAAOS 1999.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 31
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32 BiomechanicsBiomechanics
Distinction exists between clinical stability Distinction exists between clinical stability and normal kinematicsand normal kinematicsSideSide--toto--side difference in anterior laxity of side difference in anterior laxity of 2 2 -- 5mm considered stable reconstructed 5mm considered stable reconstructed knee (also pivotknee (also pivot--shift?)shift?)May correlate with pts return to level of May correlate with pts return to level of activity and reported incidences of giving activity and reported incidences of giving waywayOverall kinematics of reconstructed knee Overall kinematics of reconstructed knee are not the same as uninvolved kneeare not the same as uninvolved knee
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33 BiomechanicsBiomechanics
Reconstructed knee is probably Reconstructed knee is probably susceptible to DJDsusceptible to DJDInitiated and propagated by abnormal joint Initiated and propagated by abnormal joint motionsmotionsFocus of evaluation of ACL reconstruction Focus of evaluation of ACL reconstruction has been on restraint of anterior has been on restraint of anterior translation only (not coupled translation only (not coupled translation/rotation)translation/rotation)Only single degreeOnly single degree--ofof--freedom test freedom test ((LachmanLachman) )
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 34 BiomechanicsBiomechanics
“Perhaps the true goal of the surgical “Perhaps the true goal of the surgical treatment of ACL deficiency should be the treatment of ACL deficiency should be the complete restoration of normal kinematics complete restoration of normal kinematics and not simply the restoration of and not simply the restoration of “stability”…“stability”…
Smith, BA; Smith, BA; LivesayLivesay, GA; and , GA; and Woo, SLWoo, SL--Y in “The Anterior Y in “The Anterior CruciateCruciate Ligament”. Ligament”. Clinics inClinics inSports Medicine, Sports Medicine, Oct. 1993.Oct. 1993.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35 BiomechanicsBiomechanics
“…more anatomic reconstruction of the anterior “…more anatomic reconstruction of the anterior cruciatecruciate ligament, which restores the morphligament, which restores the morph--ologyology of the intact anterior of the intact anterior cruciatecruciate ligament, ligament, might be necessary to improve the response to might be necessary to improve the response to rotational loads. Potential solutions include rotational loads. Potential solutions include more lateral placement of the graft or a doublemore lateral placement of the graft or a double--bundle reconstruction.bundle reconstruction.
Woo, SLWoo, SL--Y et al. in “The Effectiveness of Y et al. in “The Effectiveness of Reconstruction of the Anterior Reconstruction of the Anterior Cruciate Cruciate Ligament with Hamstrings and Patellar Ligament with Hamstrings and Patellar Tendon”, JBJS, 84Tendon”, JBJS, 84--A,6, June, 2002, 907A,6, June, 2002, 907--14.14.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36
20th Century20th CenturyFunctional stabilityFunctional stability
21st Century21st CenturyBiomechanical stabilityBiomechanical stability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 37
Can we modify the surgical Can we modify the surgical technique to restore knee technique to restore knee kinematics and enable all kinematics and enable all surgeons reliably recreate surgeons reliably recreate native ACL anatomy????native ACL anatomy????
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38 DoubleDouble--Bundle ACL Bundle ACL ReconstructionReconstruction
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39 DoubleDouble--Bundle ACL Bundle ACL ReconstructionReconstruction
Biomechanical studies, reconstruction of Biomechanical studies, reconstruction of AM and PL bundle better in ant and AM and PL bundle better in ant and rotational stabilityrotational stabilitySeveral clinical trials in progress but none Several clinical trials in progress but none have shown superiority overhave shown superiority oversingle bundle techniquesingle bundle techniqueImportant technical issuesImportant technical issuesmust be overcome to adoptmust be overcome to adoptprocedureprocedure
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 40 Technical Hurdles Technical Hurdles -- TibiaTibia
Average AP length of Average AP length of tibial tibial footprint is 14mm footprint is 14mm (range 9 to 18mm)(range 9 to 18mm)Natural center of AM and PL bundles are only Natural center of AM and PL bundles are only 5mm apart5mm apart“Experts” recommend “Experts” recommend 2mm bone bridge 2mm bone bridge between tunnelsbetween tunnelsTibial Tibial footprint is generally footprint is generally too narrow to place 2 too narrow to place 2 separate bone tunnels separate bone tunnels in the ML directionin the ML direction
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41 Technical Hurdles Technical Hurdles -- TibiaTibia
Original Original sagittal sagittal coursescoursesof both footprints need to of both footprints need to be changed in order to placebe changed in order to place2 bone tunnels2 bone tunnels
In order to reproduce DBIn order to reproduce DB tibialtibialanatomy tunnels must be less anatomy tunnels must be less than 5 or 6mm and than 5 or 6mm and communicatecommunicate
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42 Technical Hurdles Technical Hurdles -- TibiaTibia
Tibia footprint smaller Tibia footprint smaller than 10 mm wide and than 10 mm wide and 14mm long renders 14mm long renders separate bone tunnel separate bone tunnel placement impossibleplacement impossibleBasically…Basically…NOT ENOUGH ROOM NOT ENOUGH ROOM for 2 tunnelsfor 2 tunnels
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 43
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45 Technical Hurdles Technical Hurdles -- FemurFemur
Average AP length of femoral footprint is Average AP length of femoral footprint is 11mm and 11mm and proxprox/distal length is 18mm/distal length is 18mmDrilling transDrilling trans--tibial tibial tunnel places AM tunnel places AM footprint superior on sidefootprint superior on side--wallwall“Experts” recommend 2mm bridge “Experts” recommend 2mm bridge between tunnels and tunnel between tunnels and tunnel divergancediverganceAM tunnel must be cheated anterior and AM tunnel must be cheated anterior and superior to avoid tunnel superior to avoid tunnel converganceconvergance
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 46 Technical Hurdles Technical Hurdles -- FemurFemur
Due to limitations in tunnel Due to limitations in tunnel angles footprints less than angles footprints less than 18mm in 18mm in proxprox/dist diameter /dist diameter render anatomic placement of render anatomic placement of femoral tunnels impossiblefemoral tunnels impossibleBasically…Basically…With standard graft sizes With standard graft sizes there’s NOT ENOUGH ROOM there’s NOT ENOUGH ROOM for 2 femoral tunnels without for 2 femoral tunnels without converganceconvergance
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 49
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 50
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 51
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
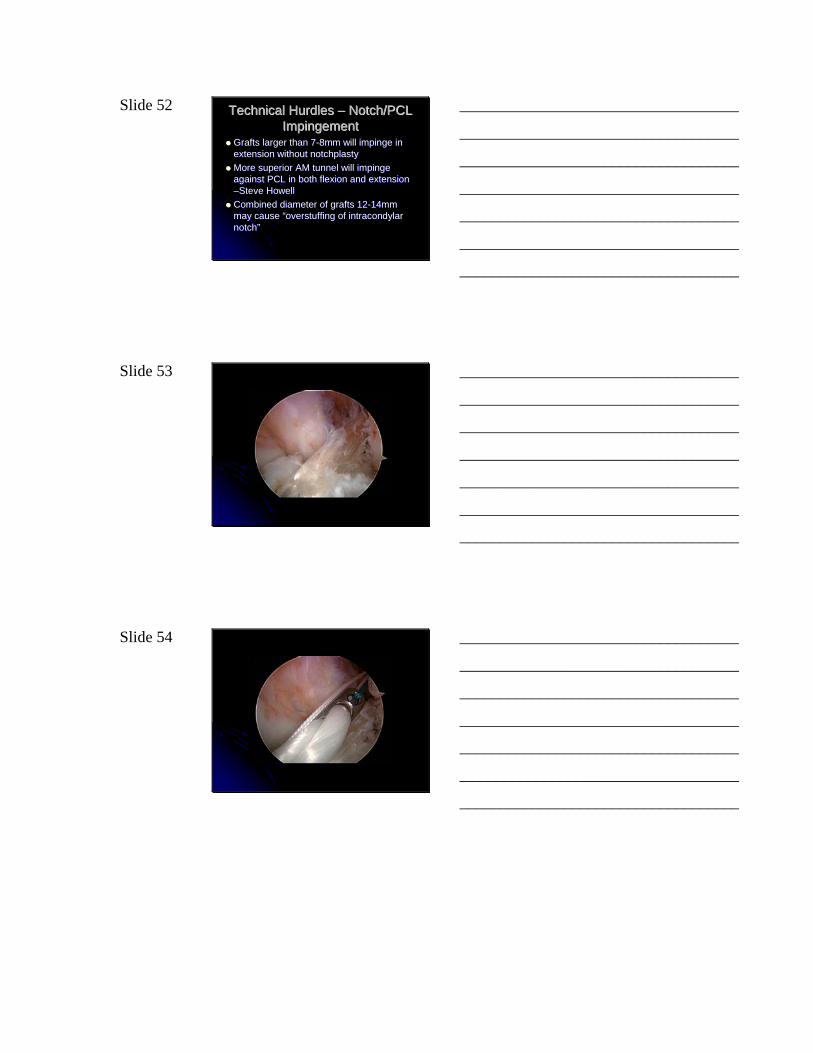
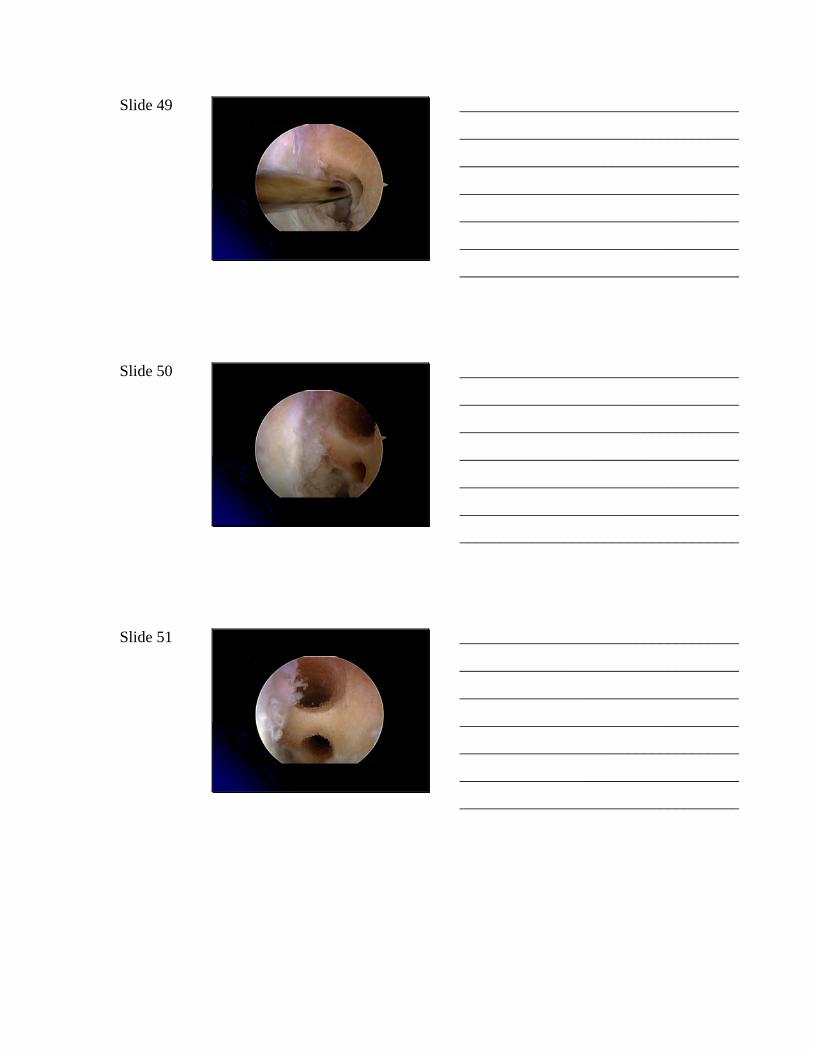
Slide 52 Technical Hurdles Technical Hurdles –– Notch/PCL Notch/PCL ImpingementImpingement
Grafts larger than 7Grafts larger than 7--8mm will impinge in 8mm will impinge in extension without extension without notchplastynotchplastyMore superior AM tunnel will impinge More superior AM tunnel will impinge against PCL in both flexion and extension against PCL in both flexion and extension ––Steve HowellSteve HowellCombined diameter of grafts 12Combined diameter of grafts 12--14mm 14mm may cause “overstuffing of may cause “overstuffing of intracondylar intracondylar notch”notch”
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 53
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 54
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 55
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 56
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 57
161219.bmp 162916.bmp
162924.bmp
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 58
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
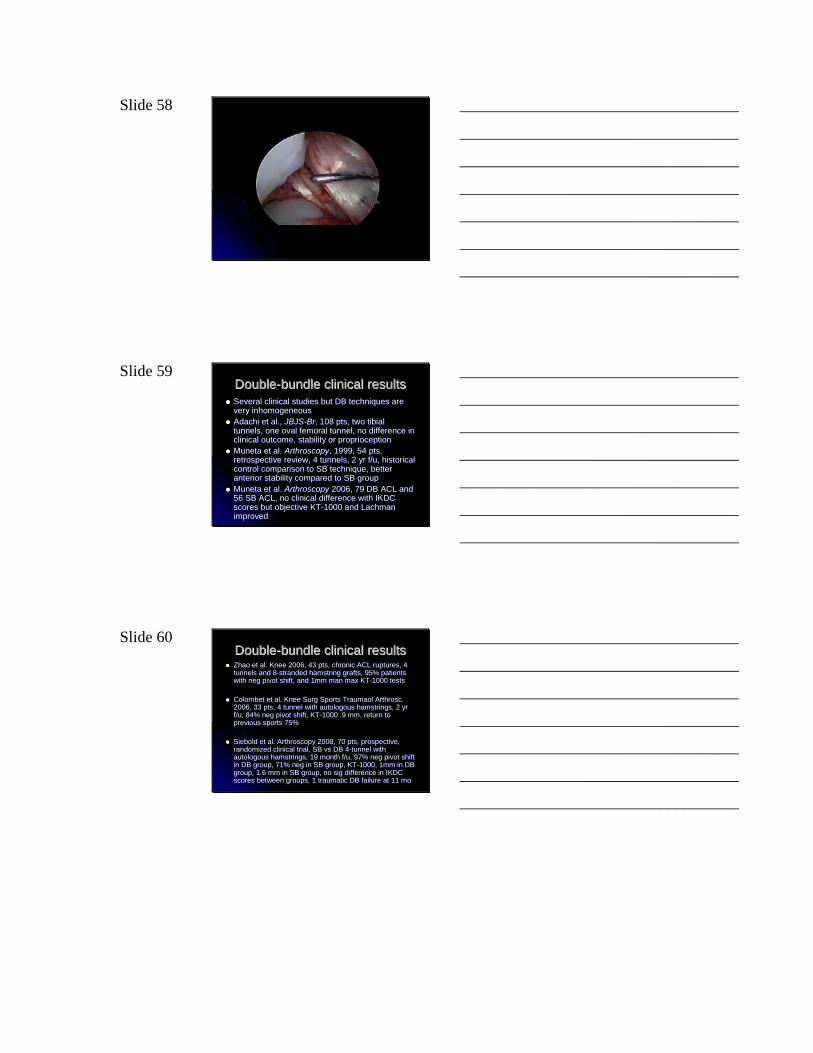
Slide 59 DoubleDouble--bundle clinical results bundle clinical results Several clinical studies but DB techniques are Several clinical studies but DB techniques are very inhomogeneousvery inhomogeneousAdachi et al., Adachi et al., JBJSJBJS--BrBr, 108 pts, two , 108 pts, two tibial tibial tunnels, one oval femoral tunnel, no difference in tunnels, one oval femoral tunnel, no difference in clinical outcome, stability or clinical outcome, stability or proprioceptionproprioceptionMuneta Muneta et al. et al. ArthroscopyArthroscopy, 1999, 54 pts, , 1999, 54 pts, retrospective review, 4 tunnels, 2 yr f/u, historical retrospective review, 4 tunnels, 2 yr f/u, historical control comparison to SB technique, better control comparison to SB technique, better anterior stability compared to SB groupanterior stability compared to SB groupMuneta Muneta et al. et al. ArthroscopyArthroscopy 2006, 79 DB ACL and 2006, 79 DB ACL and 56 SB ACL, no clinical difference with IKDC 56 SB ACL, no clinical difference with IKDC scores but objective KTscores but objective KT--1000 and 1000 and Lachman Lachman improvedimproved
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 60 DoubleDouble--bundle clinical resultsbundle clinical resultsZhao Zhao et al. Knee 2006, 43 pts, chronic ACL ruptures, 4 et al. Knee 2006, 43 pts, chronic ACL ruptures, 4 tunnels and 8tunnels and 8--stranded hamstring grafts, 95% patients stranded hamstring grafts, 95% patients with with neg neg pivot shift, and 1mm man max KTpivot shift, and 1mm man max KT--1000 tests1000 tests
ColombetColombet et al. Knee et al. Knee Surg Surg Sports Sports Traumaol ArthroscTraumaol Arthrosc. . 2006, 33 pts, 4 tunnel with 2006, 33 pts, 4 tunnel with autologous autologous hamstrings, 2 yr hamstrings, 2 yr f/u, 84% f/u, 84% neg neg pivot shift, KTpivot shift, KT--1000 .9 mm, return to 1000 .9 mm, return to previous sports 75%previous sports 75%
SieboldSiebold et al. Arthroscopy 2008, 70 pts, prospective, et al. Arthroscopy 2008, 70 pts, prospective, randomized clinical trial, SB randomized clinical trial, SB vs vs DB 4DB 4--tunnel with tunnel with autologous autologous hamstrings, 19 month f/u, 97% hamstrings, 19 month f/u, 97% neg neg pivot shift pivot shift in DB group, 71% in DB group, 71% neg neg in SB group, KTin SB group, KT--1000, 1mm in DB 1000, 1mm in DB group, 1.6 mm in SB group, no group, 1.6 mm in SB group, no sig sig difference in IKDC difference in IKDC scores between groups, 1 traumatic DB failure at 11 moscores between groups, 1 traumatic DB failure at 11 mo
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 61 Technical Hurdles Technical Hurdles -- FailureFailure
Failure of DB grafts is possible due to notch Failure of DB grafts is possible due to notch impingement (impingement (cyclops cyclops lesion)lesion)Revision difficult due to bone loss, risk of Revision difficult due to bone loss, risk of back wall compromiseback wall compromiseTunnel Tunnel osteolysis osteolysis may result in loss of may result in loss of adequate bone bridge between tunnelsadequate bone bridge between tunnelsLikely require bone grafting and standard Likely require bone grafting and standard revision ACL reconstruction (2 separate revision ACL reconstruction (2 separate procedures)procedures)Revise to single tunnel ACL reconstruction?Revise to single tunnel ACL reconstruction?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 62
Notch Impingement Dr. Andrews SB Notch Impingement Dr. Andrews SB -- 20032003
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
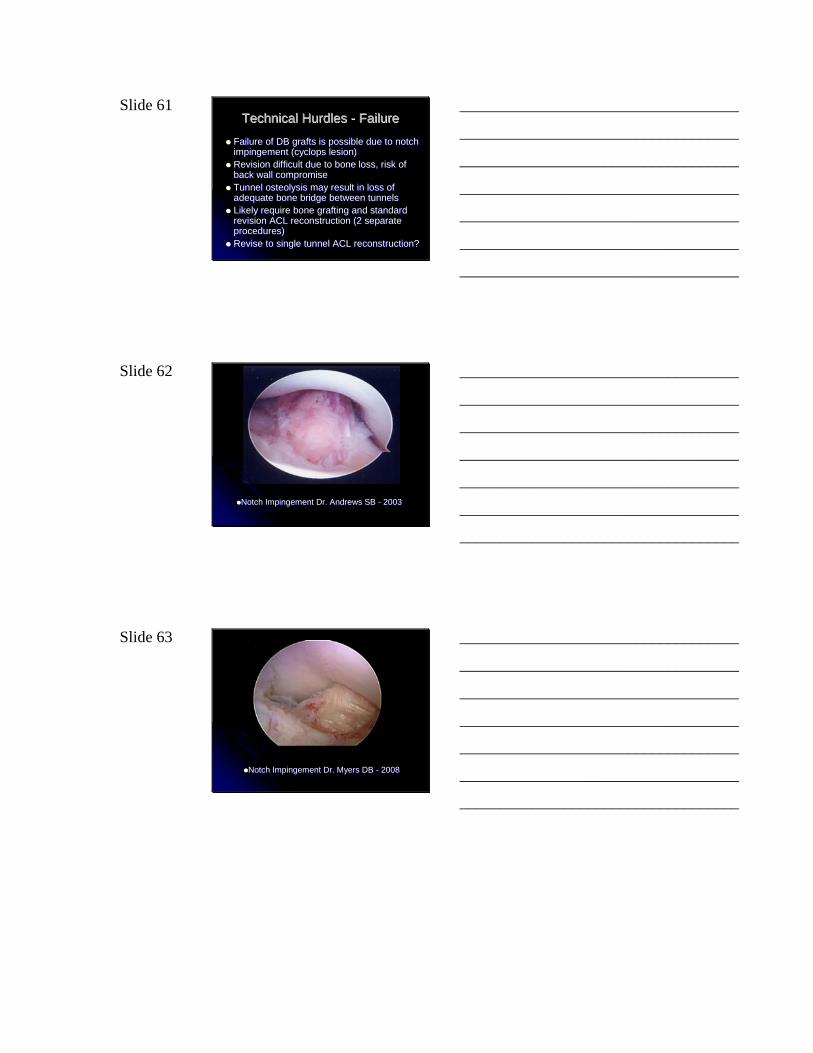
Slide 63
Notch Impingement Dr. Myers DB Notch Impingement Dr. Myers DB -- 20082008
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 64 Is this new DoubleIs this new Double--Bundle Bundle
technique the way of the future?technique the way of the future?
ANDAND
Are we really improving onAre we really improving onrelatively good clinical results or relatively good clinical results or
decreasing the risk of postdecreasing the risk of post--traumatic traumatic osteoarthritisosteoarthritis??
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 65
We’ll see…We’ll see…
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 66 THANK YOU!THANK YOU!
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________