Anatomy & Physiology of the Vitreous & the Vitreoretinal
Interface
The vitreous gel is a transparent extracellular matrix that
fills the cavity behind the lens of the eye. It occupies an average
volume of 4.4 ml in adulthood. It is surrounded by and attached to
the retina and lens of the eye.[1]It is a virtually acellular,
highly hydrated extracellular gel matrix, composed of approximately
99% water.[15]The transparent nature of the vitreous makes it
challenging to study its structure and anatomy.
The gel structure is maintained by a dilute network of thin,
unbranched collagen fibrils that are mixed (heterotopic) in
composition, comprising collagen types II, V/XI and IX in a molar
ratio of 75:10:15, respectively. Collagen type V/XI forms the core
of the fibrils, with type II surrounding the core and type IX on
the outside of the fibril. The spaces between these collagen
fibrils are mostly filled by glycosaminoglycans (GAGs), mainly
hyaluronan.[15]Opticin has been found to coat the collagen fibers
and, by binding to different GAGs, may play a role in maintaining
the gel structure of the vitreous and also in adhesion at the
vitreoretinal interface.[1517]Chondroitin sulfate, another GAG
linked to type IX collagen, was found to play a role in bridging
adjacent collagen fibrils and at the same time spacing them apart
to minimize light scattering and maintain vitreous
transparency.[18]The vitreoretinal interface is an adhesive sheet
that facilitates the connection of the posterior vitreous cortex of
the vitreous body to the internal limiting membrane of the
retina.[6]The vitreoretinal interface consists of matrix proteins
including laminin, fibronectin and collagen IV,[18,19]and it is
thought that these may act as an extracellular matrix 'glue'.[6]It
is not completely understood how the vitreous and retina interact.
The vitreous is known to be most firmly attached at places where
the internal limiting membrane is thinnest, that is, the vitreous
base, optic disc and macula, and over retinal blood vessels.[1]At
the base area, the vitreous and the retina are connected by
vitreous collagen fibers passing though the internal limiting
membrane and intertwining with retinal collagen.[20]The collagen
fibrils of the posterior vitreous cortex are indirectly attached to
the internal limiting membrane, and hence to the retina via laminin
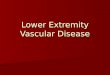
and fibronectin,[21]as shown in Figure 1. The attachment between
the vitreous and the macula is called the vitreomacular
interface.
(Enlarge Image)Figure 2.
Protein bonds in the vitreomacular interface.
Starting in the fourth decade of life, the vitreous body
witnesses a significant decrease in gel volume with a concomitant
increase in the liquid volume. Derangement of the normal
association between hyaluronan and collagen results in the
simultaneous aggregation of collagen fibrils into bundles of
parallel fibrils seen as large fibers and the formation of large
pockets of liquid vitreous recognized clinically as 'lacunae'. By
8090 years of age, more than half of the vitreous is
liquid.[22]With aging, weakening of the adhesion between the
posterior vitreous cortex and the internal limiting membrane
occurs, probably due to biochemical alterations in the
vitreoretinal interface.[23,24]One component of the extracellular
matrix of the vitreoretinal interface, galactose
(1,3)-N-acetylglucosamine, is no longer present in
adults.[25]Several studies demonstrated that an intact
vitreoretinal interface has been found in patients less than 60
years of age, despite extensive vitreous liquefaction.[1]After the
age of 60 years, weakening of the posterior vitreous
cortex/internal limiting membrane adhesion at the posterior pole
occurs, allowing liquid vitreous to enter the retrocortical space.
Volume displacement from the central vitreous to the preretinal
space causes the observed collapse of the vitreous body,[6]usually
leading to posterior vitreous detachment.
References
1. Johnson MW. Posterior vitreous detachment: evolution and
complications of its early stages.Am. J. Ophthalmol.149(3),
371382(2010).
2. Krebs I, Brannath W, Glittenberg C, Zeiler F, Sebag J, Binder
S. Posterior vitreomacular adhesion: a potential risk factor for
exudative age-related macular degeneration?Am. J.
Ophthalmol.144(5), 741746(2007).
Provides an association between vitreomacular adhesion and wet
age-related macular degeneration.
3. Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular
traction syndrome.Am. J. Ophthalmol.119(1), 5561(1995).
Provides important natural history of the disease data.
4. Sonmez K, Capone A Jr, Trese MT, Williams GA. Vitreomacular
traction syndrome: impact of anatomical configuration on anatomical
and visual outcomes.Retina (Philadelphia, PA)28(9),
12071214(2008).
5. Melberg NS, Williams DF, Balles MWet al.Vitrectomy for
vitreomacular traction syndrome with macular detachment.Retina
(Philadelphia, PA)15(3), 192197(1995).
6. Sebag J. Molecular biology of pharmacologic
vitreolysis.Trans. Am. Ophthalmol. Soc.103, 473494(2005).
7. Guillaubey A, Malvitte L, Lafontaine POet al.Incidence of
retinal detachment after macular surgery: a retrospective study of
634 cases.Br. J. Ophthalmol.91(10), 13271330(2007).
8. Ramkissoon YD, Aslam SA, Shah SP, Wong SC, Sullivan PM. Risk
of iatrogenic peripheral retinal breaks in 20-G pars plana
vitrectomy.Ophthalmology117(9), 18251830(2010).
9. Rizzo S, Belting C, Genovesi-Ebert F, di Bartolo E. Incidence
of retinal detachment after small-incision, sutureless pars plana
vitrectomy compared with conventional 20-gauge vitrectomy in
macular hole and epiretinal membrane surgery.Retina (Philadelphia,
PA)30(7), 10651071(2010).
10. Recchia FM, Scott IU, Brown GC, Brown MM, Ho AC, Ip MS.
Small-gauge pars plana vitrectomy: a report by the American Academy
of Ophthalmology.Ophthalmology117(9), 18511857(2010).
11. Cheng L, Azen SP, El-Bradey MHet al.Duration of vitrectomy
and postoperative cataract in the vitrectomy for macular hole
study.Am. J. Ophthalmol.132(6), 881887(2001).
12. Banker AS, Freeman WR, Kim JW, Munguia D, Azen SP.
Vision-threatening complications of surgery for full-thickness
macular holes. Vitrectomy for Macular Hole Study
Group.Ophthalmology104(9), 14421452; discussion 1452(1997).
Provides important natural history of disease data, as well as
data on vitrectomy complications.
13. Freeman WR, Azen SP, Kim JW, el-Haig W, Mishell DR 3rd,
Bailey I; The Vitrectomy for Treatment of Macular Hole Study Group.
Vitrectomy for the treatment of full-thickness stage 3 or 4 macular
holes. Results of a multicentered randomized clinical trial.Arch.
Ophthalmol.115(1), 1121(1997).
Provides important natural history of disease data, as well as
data on vitrectomy complications.
14. Sebag J. Pharmacologic vitreolysis.Retina18(1),
13(1998).
Introduces the concept of pharmacological vitreolysis.
15. Bishop PN. Structural macromolecules and supramolecular
organisation of the vitreous gel.Prog. Retin. Eye Res.19(3),
323344(2000).
16. Reardon AJ, Le Goff M, Briggs MDet al.Identification in
vitreous and molecular cloning of opticin, a novel member of the
family of leucine-rich repeat proteins of the extracellular
matrix.J. Biol. Chem.275(3), 21232129(2000).
17. Hindson VJ, Gallagher JT, Halfter W, Bishop PN. Opticin
binds to heparan and chondroitin sulfate proteoglycans.Invest.
Ophthalmol. Vis. Sci.46(12), 44174423(2005).
18. Scott JE, Chen Y, Brass A. Secondary and tertiary structures
involving chondroitin and chondroitin sulphates in solution,
investigated by rotary shadowing/electron microscopy and computer
simulation.Eur. J. Biochem.209(2), 675680(1992).
19. Le Goff MM, Bishop PN. Adult vitreous structure and
postnatal changes.Eye22(10), 12141222(2008).
20. Wang J, McLeod D, Henson DB, Bishop PN. Age-dependent
changes in the basal retinovitreous adhesion.Invest. Ophthalmol.
Vis. Sci.44(5), 17931800(2003).
21. Matsumoto B, Blanks JC, Ryan SJ. Topographic variations in
the rabbit and primate internal limiting membrane.Invest.
Ophthalmol. Vis. Sci.25(1), 7182(1984).
22. Bishop PN, Holmes DF, Kadler KE, McLeod D, Bos KJ.
Age-related changes on the surface of vitreous collagen
fibrils.Invest. Ophthalmol. Vis. Sci.45(4), 10411046(2004).
23. Larsson L, Osterlin S. Posterior vitreous detachment. A
combined clinical and physiochemical study.Graefes Arch. Clin. Exp.
Ophthalmol.223(2), 9295(1985).
24. Vaughan-Thomas A, Gilbert SJ, Duance VC. Elevated levels of
proteolytic enzymes in the aging human vitreous.Invest. Ophthalmol.
Vis. Sci.41(11), 32993304(2000).
25. Russell SR, Shepherd JD, Hageman GS. Distribution of
glycoconjugates in the human retinal internal limiting
membrane.Invest. Ophthalmol. Vis. Sci.32(7), 19861995(1991).
26. Sebag J. Anomalous posterior vitreous detachment: a unifying
concept in vitreo-retinal disease.Graefes Arch. Clin. Exp.
Ophthalmol.242(8), 690698(2004).
27. Smiddy WE, Green WR, Michels RG, de la Cruz Z.
Ultrastructural studies of vitreomacular traction syndrome.Am. J.
Ophthalmol.107(2), 177185(1989).
28. Shinoda K, Hirakata A, Hida Tet al.Ultrastructural and
immunohistochemical findings in five patients with vitreomacular
traction syndrome.Retina20(3), 289293(2000).
29. Wu PC, Chen YJ, Chen YHet al.Factors associated with
foveoschisis and foveal detachment without macular hole in high
myopia.Eye23(2), 356361(2009).
30. Shechtman DL, Dunbar MT. The expanding spectrum of
vitreomacular traction.Optometry80(12), 681687(2009).
31. Ito Y, Terasaki H, Suzuki Tet al.Mapping posterior vitreous
detachment by optical coherence tomography in eyes with idiopathic
macular hole.Am. J. Ophthalmol.135(3), 351355(2003).
32. Huang D, Swanson EA, Lin CPet al.Optical coherence
tomography.Science254(5035), 11781181(1991).
The first time that the concept of optical coherence tomography
was published.
33. Chang LK, Fine HF, Spaide RF, Koizumi H, Grossniklaus HE.
Ultrastructural correlation of spectral-domain optical coherence
tomographic findings in vitreomacular traction syndrome.Am. J.
Ophthalmol.146(1), 121127(2008).
34. van Velthoven ME, Faber DJ, Verbraak FD, van Leeuwen TG, de
Smet MD. Recent developments in optical coherence tomography for
imaging the retina.Prog. Retin. Eye Res.26(1), 5777(2007).
35. Do DV, Cho M, Nguyen QDet al.The impact of optical coherence
tomography on surgical decision making in epiretinal membrane and
vitreomacular traction.Trans. Am. Ophthalmol. Soc.104,
161166(2006).
36. Gallemore RP, Jumper JM, McCuen BW 2nd, Jaffe GJ, Postel EA,
Toth CA. Diagnosis of vitreoretinal adhesions in macular disease
with optical coherence tomography.Retina20(2), 115120(2000).
37. Sayegh RG, Georgopoulos M, Geitzenauer W, Simader C, Kiss C,
Schmidt-Erfurth U. High-resolution optical coherence tomography
after surgery for vitreomacular traction: a 2-year
follow-up.Ophthalmology117(10), 20102017(2010).
38. Tammewar AM, Bartsch DU, Kozak Iet al.Imaging vitreomacular
interface abnormalities in the coronal plane by simultaneous
combined scanning laser and optical coherence tomography.Br. J.
Ophthalmol.93(3), 366372(2009).
39. Chew EY, Sperduto RD, Hiller Ret al.Clinical course of
macular holes: the Eye Disease CaseControl Study.Arch.
Ophthalmol.117(2), 242246(1999).
40. Morgan CM, Schatz H. Idiopathic macular holes.Am. J.
Ophthalmol.99(4), 437444(1985).
41. Kim JE, Mantravadi AV, Hur EY, Covert DJ. Short-term
intraocular pressure changes immediately after intravitreal
injections of anti-vascular endothelial growth factor agents.Am. J.
Ophthalmol.146(6), 930934(2008).
42. Akiba J, Yoshida A, Trempe CL. Risk of developing a macular
hole.Arch. Ophthalmol.108(8), 10881090(1990).
43. Ezra E. Idiopathic full thickness macular hole: natural
history and pathogenesis.Br. J. Ophthalmol.85(1), 102108(2001).
44. Thompson JT, Sjaarda RN, Lansing MB. The results of vitreous
surgery for chronic macular holes.Retina17(6), 493501(1997).
45. Gaucher D, Haouchine B, Tadayoni Ret al.Long-term follow-up
of high myopic foveoschisis: natural course and surgical
outcome.Am. J. Ophthalmol.143(3), 455462(2007).
46. Nasrallah FP, Jalkh AE, Van Coppenolle Fet al.The role of
the vitreous in diabetic macular edema.Ophthalmology95(10),
13351339(1988).
47. Avunduk AM, Cetinkaya K, Kapicioglu Z, Kaya C. The effect of
posterior vitreous detachment on the prognosis of branch retinal
vein occlusion.Acta Ophthalmol. Scand.75(4), 441442(1997).
48. Haller JA, Qin H, Apte RSet al.; Diabetic Retinopathy
Clinical Research Network Writing Committee. Vitrectomy outcomes in
eyes with diabetic macular edema and vitreomacular
traction.Ophthalmology117(6), 10871093.e3(2010).
49. Mojana F, Cheng L, Bartsch DUet al.The role of abnormal
vitreomacular adhesion in age-related macular degeneration:
spectral optical coherence tomography and surgical results.Am. J.
Ophthalmol.146(2), 218227(2008).
50. Robison CD, Krebs I, Binder Set al.Vitreomacular adhesion in
active and endstage age-related macular degeneration.Am. J.
Ophthalmol.148, 7982(2009).
51. Uchino E, Uemura A, Ohba N. Initial stages of posterior
vitreous detachment in healthy eyes of older persons evaluated by
optical coherence tomography.Arch. Ophthalmol.119(10),
14751479(2001).
52. Panozzo G, Mercanti A. Optical coherence tomography findings
in myopic traction maculopathy.Arch. Ophthalmol.122(10),
14551460(2004).
53. The Eye Disease CaseControl Study Group. Risk factors for
idiopathic macular holes: the Eye Disease CaseControl Study
Group.Am. J. Ophthalmol.118, 754761(1994).
54. McCannel CA, Ensminger JL, Diehl NN, Hodge DN.
Population-based incidence of macular holes.Ophthalmology116(7),
13661369(2009).
55. Huang LL, Levinson DH, Levine JP, Mian U, Tsui I. Optical
coherence tomography findings in idiopathic macular holes.J.
Ophthalmol.2011, 928205 (2011).
56. Krebs I, Brannath W, Glittenberg Cet al.Posterior
vitreomacular adhesion: a potential risk factor for exudative
age-related macular degeneration?Am. J. Ophthalmol.144,
741746(2007).
57. Lee SJ, Lee CS, Koh HJ. Posterior vitreomacular adhesion and
risk of exudative age-related macular degeneration: paired eye
study.Am. J. Ophthalmol.147(4), 621626(2009).
58. Robison CD, Krebs I, Binder Set al.Vitreomacular adhesion in
active and end-stage age-related macular degeneration.Am. J.
Ophthalmol.148(1), 7982(2009).
59. Mojana F, Cheng L, Bartsch DUet al.The role of abnormal
vitreomacular adhesion in age-related macular degeneration:
spectral optical coherence tomography and surgical results.Am. J.
Ophthalmol.146, 218227(2008).
60. Sebag J. Pharmacologic vitreolysis premise and promise of
the first decade.Retina29(7), 871874(2009).
61. Hageman GS, Russell SR. Chondroitinase-mediated disinsertion
of the primate vitreous body.Invest. Ophthalmol. Vis. Sci.35,
1260(1994).
62. Staubach F, Nober V, Janknecht P. Enzyme-assisted vitrectomy
in enucleated pig eyes: a comparison of hyaluronidase,
chondroitinase, and plasmin.Curr. Eye Res.29, 261268(2004).
63. Hermel M, Schrage NF. Efficacy of plasmin enzymes and
chondroitinase ABC in creating posterior vitreous separation in the
pig: a masked, placebo-controlledin vivostudy.Graefes Arch. Clin.
Exp. Ophthalmol.245(3), 399406(2007).
64. O'Neill R, Shea M. The effects of bacterial collagenase in
rabbit vitreous.Can. J. Ophthalmol.8(2), 366370(1973).
65. Moorhead LC, Radtke N. Enzyme-assisted vitrectomy with
bacterial collagenase. Pilot human studies.Retina5(2),
98100(1985).
66. Takahashi K, Nakagawa M, Ninomiya Het al.Enzyme-assisted
vitrectomy with collagenase.Jpn. J. Clin. Ophthalmol.47,
802803(1993).
67. Stenn KS, Link R, Moellmann G, Madri J, Kuklinska E.
Dispase, a neutral protease from Bacillus polymyxa, is a powerful
fibronectinase and type IV collagenase.J. Invest. Dermatol.93(2),
287290(1989).
68. Oliveira LB, Tatebayashi M, Mahmoud TH, Blackmon SM, Wong F,
McCuen BW 2nd. Dispase facilitates posterior vitreous detachment
during vitrectomy in young pigs.Retina21(4), 324331(2001).
69. Tezel TH, Del Priore LV, Kaplan HJ. Posterior vitreous
detachment with dispase.Retina18(1), 715(1998).
70. Jorge R, Oyamaguchi EK, Cardillo JA, Gobbi A, Laicine EM,
Haddad A. Intravitreal injection of dispase causes retinal
hemorrhages in rabbit and human eyes.Curr. Eye Res.26(2),
107112(2003).
71. Zhu D, Chen H, Xu X. Effects of intravitreal dispase on
vitreoretinal interface in rabbits.Curr. Eye Res.31(11),
935946(2006).
72. Wang F, Wang Z, Sun X, Wang F, Xu X, Zhang X. Safety and
efficacy of dispase and plasmin in pharmacologic
vitreolysis.Invest. Ophthalmol. Vis. Sci.45(9), 32863290(2004).
73. Kaplan HJ, Tezel TH, Del Priore LV. Purification of the
active constituents of dispase for vitreopharmacolysis.Invest.
Ophthalmol. Vis. Sci.46, E-abstract 5454 (2005).
74. Narayanan R, Kuppermann BD. Hyaluronidase for pharmacologic
vitreolysis.Dev. Ophthalmol.44, 2025(2009).
75. Gottlieb JL, Antoszyk AN, Hatchell DL, Saloupis P. The
safety of intravitreal hyaluronidase. A clinical and histologic
study.Invest. Ophthalmol. Vis. Sci.31(11), 23452352(1990).
76. Kuppermann BD, Thomas EL, de Smet MD, Grillone LR; Vitrase
for Vitreous Hemorrhage Study Groups. Pooled efficacy results from
two multinational randomized controlled clinical trials of a single
intravitreous injection of highly purified ovine hyaluronidase
(Vitrase) for the management of vitreous hemorrhage.Am. J.
Ophthalmol.140(4), 573584(2005).
77. Kuppermann BD, Thomas EL, de Smet MD, Grillone LR; Vitrase
for Vitreous Hemorrhage Study Groups. Safety results of two Phase
III trials of an intravitreous injection of highly purified ovine
hyaluronidase (Vitrase) for the management of vitreous
hemorrhage.Am. J. Ophthalmol.140(4), 585597(2005).
78. Wang ZL, Zhang X, Xu X, Sun XD, Wang F. PVD following
plasmin but not hyaluronidase: implications for combination
pharmacologic vitreolysis therapy.Retina25(1), 3843(2005).
79. Hikichi T, Kado M, Yoshida A. Intravitreal injection of
hyaluronidase cannot induce posterior vitreous detachment in the
rabbit.Retina20(2), 195198(2000).
80. Sumi H, Hamada H, Nakanishi K, Hiratani H. Enhancement of
the fibrinolytic activity in plasma by oral administration of
nattokinase.Acta Haematol.84(3), 139143(1990).
81. Urano T, Ihara H, Umemura Ket al.The profibrinolytic enzyme
subtilisin NAT purified fromBacillus subtiliscleaves and
inactivates plasminogen activator inhibitor type 1.J. Biol.
Chem.276(27), 2469024696(2001).
82. Takano A, Hirata A, Ogasawara Ket al.Posterior vitreous
detachment induced by nattokinase (subtilisin NAT): a novel enzyme
for pharmacologic vitreolysis.Invest. Ophthalmol. Vis. Sci.47(5),
20752079(2006).
83. Liotta LA, Goldfarb RH, Brundage R, Siegal GP, Terranova V,
Garbisa S. Effect of plasminogen activator (urokinase), plasmin,
and thrombin on glycoprotein and collagenous components of basement
membrane.Cancer Res.41(11 Pt 1), 46294636(1981).
84. Uemura A, Nakamura M, Kachi Set al.Effect of plasmin on
laminin and fibronectin during plasmin-assisted vitrectomy.Arch.
Ophthalmol.123(2), 209213(2005).
85. Li X, Shi X, Fan J. Posterior vitreous detachment with
plasmin in the isolated human eye.Graefes Arch. Clin. Exp.
Ophthalmol.240(1), 5662(2002).
86. Takano A, Hirata A, Inomata Yet al.Intravitreal plasmin
injection activates endogenous matrix metalloproteinase-2 in rabbit
and human vitreous.Am. J. Ophthalmol.140(4), 654660(2005).
87. Verstraeten TC, Chapman C, Hartzer M, Winkler BS, Trese MT,
Williams GA. Pharmacologic induction of posterior vitreous
detachment in the rabbit.Arch. Ophthalmol.111(6), 849854(1993).
88. Hikichi T, Yanagiya N, Kado M, Akiba J, Yoshida A. Posterior
vitreous detachment induced by injection of plasmin and sulfur
hexafluoride in the rabbit vitreous.Retina19(1), 5558(1999).
89. Gandorfer A, Putz E, Welge-Lssen U, Grterich M, Ulbig M,
Kampik A. Ultrastructure of the vitreoretinal interface following
plasmin assisted vitrectomy.Br. J. Ophthalmol.85(1), 610(2001).
90. Gandorfer A, Priglinger S, Schebitz Ket al.Vitreoretinal
morphology of plasmin-treated human eyes.Am. J. Ophthalmol.133(1),
156159(2002).
91. Margherio AR, Margherio RR, Hartzer M, Trese MT, Williams
GA, Ferrone PJ. Plasmin enzyme-assisted vitrectomy in traumatic
pediatric macular holes.Ophthalmology105(9), 16171620(1998).
92. Wu WC, Drenser KA, Trese MT, Williams GA, Capone A.
Pediatric traumatic macular hole: results of autologous plasmin
enzyme-assisted vitrectomy.Am. J. Ophthalmol.144(5),
668672(2007).
93. Tsukahara Y, Honda S, Imai Het al.Autologous
plasmin-assisted vitrectomy for stage 5 retinopathy of prematurity:
a preliminary trial.Am. J. Ophthalmol.144(1), 139141(2007).
94. Wu WC, Drenser KA, Lai M, Capone A, Trese MT. Plasmin
enzyme-assisted vitrectomy for primary and reoperated eyes with
stage 5 retinopathy of prematurity.Retina (Philadelphia, PA)28(3
Suppl.), S75S80(2008).
95. Trese MT, Williams GA, Hartzer MK. A new approach to stage 3
macular holes.Ophthalmology107(8), 16071611(2000).
96. Sakuma T, Tanaka M, Inoue M, Mizota A, Souri M, Ichinose A.
Efficacy of autologous plasmin for idiopathic macular hole
surgery.Eur. J. Ophthalmol.15(6), 787794(2005).
97. Azzolini C, D'Angelo A, Maestranzi Get al.Intrasurgical
plasmin enzyme in diabetic macular edema.Am. J. Ophthalmol.138(4),
560566(2004).
98. Sakuma T, Tanaka M, Inoue J, Mizota A, Souri M, Ichinose A.
Use of autologous plasmin during vitrectomy for diabetic
maculopathy.Eur. J. Ophthalmol.16(1), 138140(2006).
99. Hirata A, Takano A, Inomata Y, Yonemura N, Sagara N,
Tanihara H. Plasmin-assisted vitrectomy for management of
proliferative membrane in proliferative diabetic retinopathy: a
pilot study.Retina27(8), 10741078(2007).
100. Udaondo P, Daz-Llopis M, Garca-Delpech S, Salom D, Romero
FJ. Intravitreal plasmin without vitrectomy for macular edema
secondary to branch retinal vein occlusion.Arch. Ophthalmol.129(3),
283287(2011).
101. Kamei M, Estafanous M, Lewis H. Tissue plasminogen
activator in the treatment of vitreoretinal diseases.Semin.
Ophthalmol.15(1), 4450(2000).
102. Hesse L, Nebeling B, Schroeder B, Heller G, Kroll P.
Induction of posterior vitreous detachment in rabbits by
intravitreal injection of tissue plasminogen activator following
cryopexy.Exp. Eye Res.70(1), 3139(2000).
103. Hesse L, Chofflet J, Kroll P. Tissue plasminogen activator
as a biochemical adjuvant in vitrectomy for proliferative diabetic
vitreoretinopathy.Ger. J. Ophthalmol.4(6), 323327(1995).
104. Le Mer Y, Korobelnik JF, Morel C, Ullern M, Berrod JP.
TPA-assisted vitrectomy for proliferative diabetic retinopathy:
results of a double-masked, multicenter trial.Retina19(5),
378382(1999).
105. Gandorfer A, Rohleder M, Sethi Cet al.Posterior vitreous
detachment induced by microplasmin.Invest. Ophthalmol. Vis.
Sci.45(2), 641647(2004).
106. Gad Elkareem AM, Willekens B, Vanhove M, Noppen B, Stassen
JM, de Smet MD. Characterization of a stabilized form of
microplasmin for the induction of posterior vitreous
detachment.Curr. Eye Res.35(10), 909915(2010).
107. Sakuma T, Tanaka M, Mizota A, Inoue J, Pakola S. Safety
ofin vivopharmacologic vitreolysis with recombinant microplasmin in
rabbit eyes.Invest. Ophthalmol. Vis. Sci.46(9), 32953299(2005).
108. de Smet MD, Valmaggia C, Zarranz-Ventura J, Willekens B.
Microplasmin:ex vivocharacterization of its activity in porcine
vitreous.Invest. Ophthalmol. Vis. Sci.50(2), 814819(2009).
109. de Smet MD, Gandorfer A, Stalmans Pet al.Microplasmin
intravitreal administration in patients with vitreomacular traction
scheduled for vitrectomy: the MIVI I trial.Ophthalmology116(7),
13491355(2009).
110. Stalmans P, Delaey C, de Smet MD, van Dijkman E, Pakola S.
Intravitreal injection of microplasmin for treatment of
vitreomacular adhesion: results of a prospective, randomized,
sham-controlled Phase II trial (the MIVI-IIT trial).Retina30(7),
11221127(2010).
111. Benz MS, Packo KH, Gonzalez Vet al.A placebo-controlled
trial of microplasmin intravitreous injection to facilitate
posterior vitreous detachment before
vitrectomy.Ophthalmology117(4), 791797(2010).
112. Girach A, Kozma-Wiebe P, Pakola S. Ocriplasmin as treatment
for symptomatic vitreomacular adhesion: Phase III trial results.
Presented at:Knowledge for Growth 2012. Gent, Belgium, 24 May
2012.
113. Zhi-Liang W, Wo-Dong S, Min L, Xiao-Ping B, Jin J.
Pharmacologic vitreolysis with plasmin and hyaluronidase in
diabetic rats.Retina29(2), 269274(2009).
Websites
201. Vitrectomy, St Luke's Cataract and Laser Institute.
www.stlukeseye.com/surgical/vitrectomy.html (Accessed 25 February
2012)
202. IDC-9-CM Tabular Addenda.
www.cdc.gov/nchs/data/icd9/ICD-9-CM%20TABULARADDENDAfy12.pdf
(Accessed 12 January 2012)
203. Medscape. Oh KT, Hughes BM, Atebara NH, Drouilhet JH.
Macular hole.
http://emedicine.medscape.com/article/1224320-overview#a0199
(Accessed 19 January 2012)
Papers of special note have been highlighted as:
of interest
of considerable interest
Expert Review of OphthalmologyVitreomacular Interface
Diseases
Pathophysiology, Diagnosis and Future Treatment Options
Aniz Girach, Steve Pakola
DisclosuresExpert Rev Ophthalmol.2012;7(4):311-323.
http://www.medscape.com/viewarticle/772188_3 PrintAnatomi &
Fisiologi Vitreous & yang vitreoretinal Antarmuka
Vitreous gel adalah matriks ekstraseluler transparan yang
mengisi rongga di belakang lensa mata. Ini menempati volume
rata-rata dari 4,4 ml di masa dewasa. Hal ini dikelilingi oleh dan
melekat pada retina dan lensa mata. [1] Ini adalah hampir
acellular, sangat terhidrasi matriks ekstraseluler gel, terdiri
dari sekitar 99% air. [15] transparan sifat vitreous membuatnya
menantang untuk mempelajari struktur dan anatomi.
Struktur gel dikelola oleh jaringan encer tipis, fibril kolagen
bercabang yang dicampur (heterotopic) dalam komposisi, terdiri dari
kolagen tipe II, V / XI dan IX dalam rasio molar 75:10:15,
masing-masing. Kolagen tipe V / XI membentuk inti dari fibril,
dengan tipe II sekitar inti dan tipe IX di luar urat saraf. Ruang
antara fibril kolagen sebagian besar diisi oleh glycosaminoglycans
(GAG), terutama Hyaluronan. [15] Opticin telah ditemukan untuk
melapisi serat kolagen dan, dengan mengikat GAG yang berbeda,
mungkin memainkan peran dalam mempertahankan struktur gel vitreous
dan juga dalam adhesi pada antarmuka vitreoretinal. [15-17]
Chondroitin sulfat, GAG lain terkait dengan mengetik kolagen IX,
ditemukan untuk memainkan peran dalam menjembatani fibril kolagen
yang berdekatan dan pada jarak waktu yang sama mereka terpisah
untuk meminimalkan hamburan cahaya dan memelihara transparansi
vitreous. [18] antarmuka vitreoretinal adalah lembar perekat yang
memfasilitasi sambungan dari vitreous korteks posterior vitreous
body pada membran membatasi internal retina. [6] Antarmuka
vitreoretinal terdiri dari protein matriks termasuk laminin,
fibronektin dan kolagen IV, [18,19] dan diperkirakan bahwa dapat
bertindak sebagai 'lem' matriks ekstraselular. [6]
Hal ini tidak sepenuhnya dipahami bagaimana vitreous dan retina
berinteraksi. Vitreous diketahui paling melekat erat di tempat di
mana membran batas yang tertipis, yaitu, basis vitreous, disk optik
dan makula, dan lebih dari pembuluh darah retina. [1] Di daerah
basis, vitreous dan retina dihubungkan oleh serat kolagen vitreous
lewat meskipun internal membatasi membran dan terjalinnya dengan
kolagen retina. [20] fibril kolagen dari vitreous korteks posterior
secara tidak langsung melekat pada membran batas, dan karenanya ke
retina melalui laminin dan fibronektin, [21 ] seperti yang
ditunjukkan pada Gambar 1. Lampiran antara vitreous dan makula
disebut antarmuka vitreomacular.
(Perbesar Gambar)
Gambar 2.
Obligasi protein dalam antarmuka vitreomacular.
Dimulai pada dekade keempat kehidupan, saksi vitreous body
penurunan yang signifikan dalam volume gel dengan seiring
bertambahnya volume cairan. Kekacauan asosiasi normal antara
Hyaluronan dan hasil kolagen dalam agregasi simultan fibril kolagen
ke dalam bundel fibril paralel dilihat sebagai serat besar dan
pembentukan kantong besar vitreous cair diakui secara klinis
sebagai 'kekosongan'. Dengan 80-90 tahun, lebih dari setengah dari
vitreous cair. [22]
Dengan penuaan, melemahnya adhesi antara korteks posterior
vitreous dan membran batas terjadi, mungkin karena perubahan
biokimia dalam antarmuka vitreoretinal [23,24] Salah satu komponen
dari matriks ekstraseluler dari antarmuka vitreoretinal, galaktosa
(1,. 3)-N-asetilglukosamin, tidak lagi hadir pada orang dewasa.
[25] Beberapa penelitian menunjukkan bahwa antarmuka vitreoretinal
utuh telah ditemukan pada pasien kurang dari 60 tahun, meskipun
pencairan vitreous yang luas. [1] Setelah usia 60 tahun, melemahnya
vitreous posterior korteks / internal yang membatasi adhesi membran
pada kutub posterior terjadi, sehingga vitreous cairan masuk ke
ruang retrocortical. Volume perpindahan dari vitreous pusat ke
ruang preretinal menyebabkan runtuhnya diamati dari tubuh vitreous,
[6] biasanya mengarah ke posterior vitreous detachment.