Embed Size (px)
Citation preview

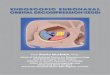
Anatomic comparison of the endonasal and transpetrosal approaches for interpeduncular fossa access
Kenichi Oyama1,3, Daniel M Prevedello1, Leo F.S. Ditzel Filho1, Jun Muto1Ramazan Gun2, Edward E Kerr1, Bradley A Otto2, Ricardo L Carrau2
Department of Neurological Surgery1 and Otolaryngology-Head & Neck Surgery2The Ohio State University Wexner Medical Center
Department of Neurosurgery 3, Teikyo University School of Medicine, Tokyo, Japan
IntroducVon)&)ObjecVves)
• The%interpeduncular%cistern%(IPC),%including%the%retrochiasma:c%area,%is%one%of%the%most%challenging%regions%to%approach%surgically.%
• The%endoscopic%endonasal%approach%(EEA)%with%pituitary%transposi:on%and%the%transpetrosal%approach%(TPA)%provide%ideal%exposure%with%a%caudalCcranial%view.%%%
• We%compared%the%EEA%and%TPA%to%clarify%the%limita:ons%and%advantages%of%these%approaches%for%the%removal%of%retrochiasma:c%craniopharyngiomas.%%
Material)&)Methods)
• Four%fresh%cadaver%heads%were%studied.%%%• An%EEA%transdorsum%sellae%with%pituitary%transposi:on%was%
performed%to%expose%the%IPC.%%• A%TPA%was%performed%bilaterally%combining%a%retrolabyrinthine%
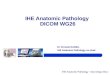
presigmoid%and%a%subtemporal%transtentorium%approach.%%%• “Water%balloon%tumors”%(WBT)%(Fig.1))were%placed%(volume%0.5%ml%
and%1%ml)%in%the%IPC%to%compare%their%visualiza:on%by%the%two%approaches.%%%
• The%distance%between%cranial%nerve%III%(CN%III)%and%the%posterior%communica:ng%artery%(PcomA),%and%between%CN%III%and%the%edge%of%the%tentorium,%were%measured%through%a%TPA%to%determine%the%width%of%surgical%corridors%using%0C%6%ml%WBT%in%the%IPC%(Fig.2A)).%%
%
%Fig.1)“Water)Balloon)Tumor”)
A%water%balloon%(green),%represen:ng%a%cys:c%tumor,%is%connected%by%a%kinkCresistant%tube%with%a%roller%clamp%to%a%syringe%for%the%infusion%of%water%(0%C%>%10%ml)%into%the%balloon.%%The%photograph%shows%a%5Cml%“water%balloon%tumor”.�
Results)
• Both%approaches%provided%sufficient%exposure%of%the%IPC.%%%• With%a%WBT%in%the%IPC,%the%EEA%yielded%a%good%visualiza:on%of%both%
CNs%III%and%the%Pcom%A%(Fig.3A,C)).%%• %The%visualiza:on%of%anatomical%structures%on%the%contralateral%side%
was%impaired%when%we%used%the%TPA%rela:ve%to%the%EEA%(Fig.3B,D)).%%%• The%surgical%corridor%to%the%IPC%via%the%TPA%was%narrow%when%the%
WBT%volume%was%small,%and%its%width%increased%as%the%volume%of%the%WBT%increased%(Fig.2B,4)).�
%
%
Fig.2))Visibility)of)IPC)harboring)0.5M)&)1Mml)WBT)
0.5 ml-WBT� 1 ml-WBT�A. View%via%the%endoscopic%endonasal%approach%with%pituitary%transposi:on%(EEAPT)%
with%a%0.5Cml%“water%balloon%tumor”%(WBT)%in%the%interpeduncular%cistern%(IPC).%%There%is%good%visualiza:on%of%both%cranial%nerve%III%(CN%III)%and%the%posterior%communica:ng%artery%(PcomA)%with%the%0°C%(upper),%30°C%(lower%leQ),%and%70°%endoscope%(lower%right).%
B. %View%via%the%transpetrosal%approach%(TPA)%on%both%sides%of%the%specimen.%%The%IPC%harbored%a%0.5Cml%WBT.%The%visualiza:on%of%anatomical%structures%in%the%contralateral%side%was%obstructed.%%This%specimen%has%a%hypoplas:c%PcomA%on%the%leQ%(Lt.)%and%a%fetalCtype%PcomA%on%the%right%(Rt.).%%The%surgical%corridor%to%the%WBT%is%wider%on%the%leQ%side.%%
C. View%via%the%EEAPT.%%The%IPC%harbored%a%1Cml%WBT.%%Although%visualiza:on%of%both%CN%III%and%the%PcomA%was%partly%obstructed%when%we%used%the%0°%endoscope%(upper%leQ),%gentle%medial%mobiliza:on%of%the%WBT%facilitated%good%visualiza:on%of%both%structures%(upper%right).%%With%the%30°C%(lower%leQ)%and%70°%endoscope%(lower%right),%both%structures%were%readily%observed%below%without%WBT%mobiliza:on.�
D. View%via%the%TPA%on%both%sides%of%the%specimen.%%The%IPC%harbored%a%1Cml%WBT.%The%WBT%completely%obstructed%visualiza:on%of%the%structures%on%the%contralateral%side.%This%specimen%has%a%hypoplas:c%PcomA%on%the%leQ%(Lt.)%and%a%fetal%type%PcomA%on%the%right%(Rt.).%%The%surgical%corridor%to%the%WBT%is%wider%on%the%leQ%side.�
A. Using%WBT%of%different%volumes,%we%measured%the%maximum%distance%between%CN%III%and%the%PcomA%(leQ),%and%between%CN%III%and%the%edge%of%the%tentorium%(right)%to%show%the%width%of%surgical%corridor%to%the%IPC%when%the%TPA%was%used.%%
B. View%via%the%transnpetrosal%approach%(TPA)%on%the%right%side.%%The%interpeduncular%cistern%(IPC)%harbored%“water%balloon%tumors”%(WBT)%of%different%volumes.%%The%possible%surgical%corridor%between%cranial%nerve%III%(CN%III)%and%the%posterior%communica:ng%artery%(PcomA),%and%between%CN%III%and%the%tentorium%was%narrow%when%the%WBT%was%small%and%gradually%increased%as%the%volume%of%WBT%increased.�
Fig.3&Width&of&the&Surgical&Corridor&with&the&TPA&
Discussions)
• While%both%approaches%are%valid%surgical%op:ons%for%retrochiasma:c%pathology,%the)EEA%transdorsum%sellae%provides%a%direct%and%wide%exposure%of%the%IPC%with%negligible%neurovascular%manipula:on.%%%
• Although%the%TPA%also%allows%direct%access%to%the%IPC%without%pituitary%manipula:on,%the%surgical%corridor%is%narrow%due%to%the%surrounding%neurovascular%structures%with%poor%contralateral%visibility.%%%
• On%the%other%hand,%for%large%or%giant%tumors%in%the%IPC,%the%spaces%between%neurovascular%structures%are%widened,%and%the%TPA%becomes%an%excep:onal%route%whereas%the%EEA%may%have%limited%freedom%of%movement%in%the%lateral%extension.%%
Fig.4&Width&of&the&Surgical&Corridor&with&the&TPA&
All#data#were#expressed#as#the#mean±SD.#*P#<#0.05#vs.#0#mL,#paired#t#test#with#Bonferroni#correc@on#for#mul@ple#comparisons#
Conclusions)
• Both%the%EEA%and%TPA%seem%to%be%considerable%good%surgical%approaches%to%the%interpeduncular%fossa.%%
• The%EEA%provides%a%midline%surgical%corridor%to%the%tumor%in%the%IPC%without%traversing%neurovascular%structures.%
• We%suggest%the%TPA%in%pa:ents%with%large%or%giant%tumors%because%the%space%between%neurovascular%structures%is%narrow.%%
• Further%clinical%experience%must%be%collected%to%clarify%the%advantages%and%limita:ons%of%these%approaches%to%the%IPC%in%the%clinical%secngs.%%
%
Comparison)of)TPA)&)EEA))Pros)&)Cons)