-
The anatomy, investigationsand management of adultbrachial
plexus injuriesJonathan Gregory
Alex Cowey
Matthew Jones
Simon Pickard
David Ford
AbstractBrachial plexus injuries have increased in numbers since
the turn of the
twentieth century in line with the increased use of motorcycles.
Advances
in microsurgical and tissue transfer techniques have seen the
management
of such injuries change dramatically during this time period. As
a result,
surgery for plexus injuries is now considered a legitimate
option. Such
injuries require extensive medical input in a multidisciplinary
environment.
All patients should be thoroughly investigated to establish the
exact extent
was confined to exploration in order to determine prognosis,
onic, as this significantly affects both management and
prog-
PERIPHERAL NERVEof the injury andmanaged on an individual basis.
The options available are
conservative or surgical. Conservative options include
physiotherapy,
orthotics and pain control. Surgical reconstruction of the
plexus may
involve neurolysis, nerve grafting, nerve transfer and late
peripheral recon-
struction including arthrodesis, tendon transfers, free muscle
transfers and
amputation. Despite many advances in the field, injuries still
result in
considerable disability and loss of working days.
Keywords anatomy; brachial plexus; management; nerve injury;
neurophysiology
Jonathan Gregory BSc MB ChB FRCS (TO) Specialist Registrar
Trauma andOrthopaedics, Robert Jones and Agnes Hunt Orthopaedic
& District
General Hospital, Shropshire, UK.
Alex Cowey MB ChB FRCS (TO) Specialist Registrar Trauma
andOrthopaedics, Robert Jones and Agnes Hunt Orthopaedic &
District
General Hospital, Shropshire, UK.
Matthew Jones MB ChB MRCP Clinical Research Fellow and
Specialist
Registrar in Neurology, University of Manchester, Wolfson
Molecular
imaging Centre, Manchester, UK.
Simon Pickard MB ChB FRCS FRCS(Orth) Consultant Orthopaedic
Surgeon
and Specialist in Hand, Upper limb and Nerve Injury Surgery,
Nerve
Injury Unit, The Robert Jones and Agnes Hunt Orthopaedic &
District
General Hospital, Shropshire, UK.
David Ford MB ChB FRCS FRCS(Orth) Consultant Orthopaedic Surgeon
and
Specialist in Hand, Upper limb and Nerve Injury Surgery, Nerve
Injury
Unit, The Robert Jones and Agnes Hunt Orthopaedic & District
General
Hospital, Shropshire, UK.ORTHOPAEDICS AND TRAUMA 23:6 420nosis,
and this may require supplementary tests such as
electrophysiological or radiological investigations.
Concurrent
severe injuries occur in up to 80% of patients, and the
attending
clinician must be alert to this. Commonly associated
injuries
include dislocated shoulders, fractures of the proximal
humerus,
clavicle, scapula and cervical spine, in addition to major
upper
limb vascular injuries (subclavian or axillary artery).
These
injuries require management in their own right but can also
provide vital clues to the extent and nature of the
plexopathy.
A lesion can be classified using a variety of systems, which
often differentiate between upper plexus and lower plexus
injuries. Lefferts classification system6 based on aetiology
and
level of the injury is commonly used (Table 1), but it must
be
remembered that lesions may occur at more then one level.
Following a full evaluation the management plan should be
tailored to an individual patients needs and a time scale set
out,
with consideration given to both conservative measures and
secondary reanimation of the limb.more complex interventions
being associated with poor
results.1e4 The extent of this belief is highlighted by
Seddons
comments in 1961 The results of reconstructive operations
have
been so disappointing that we believe that this type of
treatment
should be abandoned.5 Towards the end of the 20th century
advances in microsurgical techniques and tissue transfer
proce-
dures have improved the functional outcome of these
injuries.
However, many of these patients still require extensive
medical
input and a multidisciplinary approach to their care.
Assessment
A full assessment to establish the aetiology, and clearly
define
the level and severity of the injury must be performed. It
is
important to ascertain whether the lesion is pre- or post
gangli-Introduction
Brachial plexus injuries range from transient nerve
dysfunction
to a completely flail upper limb associated with
life-threatening
injuries. Significant injuries lead to physical disability in
addition
to psychological and financial hardship. The management of
such cases is complicated by concurrent injuries that may
delay
or cloud the neurological assessment. In addition to this,
anatomical variations within the brachial plexus make these
injuries a considerable challenge to clinicians responsible
for
their care.
Traumatic lesions are most commonly the result of motor-
cycle accidents and typically affect young men.1e3 Lesions
can
also occur following penetrating or sports related injuries,
falls,
industrial accidents, radiation therapy and iatrogenic
causes
(first rib resection, shoulder surgery, interventional
radiology).
The most common mechanism is a traction injury to the nerves
secondary to forceful separation of the neck from the
shoulder.1
History
Brachial plexus reconstruction began in earnest in the mid
20th
century with work by Barnes, Brooks, Bonney, Seddon and
Leffert and later Narakas. Despite their work the role of
surgery 2009 Elsevier Ltd. All rights reserved.
-
Anatomy of the brachial plexus
The anatomy of the brachial plexus demonstrates a large
degree of variability, both between individuals and between
the left and right limbs of the same individual.7 Most
commonly the brachial plexus is formed by the confluence of
the ventral rami of the spinal nerve roots from C5 to T1.
Common variations include contributions to the plexus by
the C4 nerve root (described as a pre-fixed plexus) or the
T2
nerve root (a post-fixed plexus). The 5 roots normally
contributing to the plexus merge into 3 trunks, each of
which
Two anatomical triangles contain the proximal plexus. The
interscalene triangle is formed between the anterior and
middle
scalene muscles superiorly and the first rib inferiorly and
contains the roots of the plexus. The posterior triangle of
the
neck contains the trunks of the plexus and is formed by the
sternocleidomastoid muscle anteriorly, trapezius laterally
and
the clavicle inferiorly.
Dorsal (sensory) and ventral (motor) rootlets arise from the
spinal cord and merge to form a root as they pass through
the vertebral foramen. Just prior to the formation of the root
the
sensory rootlet enlarges in diameter forming the dorsal root
ganglia (DRG). The DRG contains the cell bodies of the
sensory
nerves (motor nerve cell bodies are within the spinal cord).
An
injury proximal to the DRG is described as pre-ganglionic.
This
may be avulsion of the rootlets from the spinal cord or an
injury,
which is still intradural, but just proximal to the DRG. The
rootlets have no connective tissue or meningeal covering as
they
originate from the spinal cord; this contributes to their
suscep-
tibility to avulsion from the cord. The roots have a
protective
layer formed by the dura and are able to move freely within
the
foramen. As the C4, C5, C6 and C7 roots emerge from the
foramen they are tethered to the transverse processes of
their
respective vertebrae. C8 and T1 are not tethered in this
way,
which leads to a higher incidence of root avulsion from the
spinal
cord being seen at these levels compared to the upper
plexus.
The roots enter the scalene triangle, being found between
anterior and middle scalene muscles. The first terminal nerves
to
Leffert classification of brachial plexus injuries
I Open
II Closed IIa Supraclavicular
Preganglionic e nerve root avulsion
Postganglionic e traction injuries
IIb Infraclavicular
IIc Combined
III Radiotherapy induced
IV Obstetric IVa Upper root (Erbs palsy)
IVb Lower root (Klumpkes palsy)
IVc Mixed
Table 1
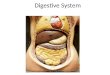
PERIPHERAL NERVEsplits into anterior and posterior divisions.
The divisions
become 3 cords which give rise to the terminal branches
(Figure 1).Figure 1 Diagrammatic representation of the Brachial
Plexus.
ORTHOPAEDICS AND TRAUMA 23:6 421arise from the plexus do so at
this level. The C5 root has 3
branches at this point: contributions to the phrenic, long
thoracic
and dorsal scapular nerves. The roots descend and move
laterally
into the posterior triangle of the neck. 2009 Elsevier Ltd. All
rights reserved.
-
Terminal branches of the roots, trunks and cords of the brachial
plexus
Nerve Origin from plexus Root value Muscle/area innervated
Phrenic Root C345 Ipsilateral hemidiaphragm
Dorsal scapular Root C5 Rhomboids
Long thoracic Root C567 Serratus anterior
Subclavius Upper trunk C56 Subclavius
Suprascapular Upper trunk C56 Supraspinatus, infraspinatus
Lateral pectoral Lateral cord C56 Clavicular and sternocostal
heads
Pectoralis major, Pectoralis minor
Medial pectoral Medial cord C678 Sternocostal head Pectoralis
major,
Pectoralis minor
Medial brachial cutaneous Medial cord Medial arm above the
elbow
Medial antebrachial cutaneous Medial cord Medial forearm
Upper subscapular Posterior cord C567 Subscapularis
Thoracodorsal Posterior cord C678 Latissimus dorsi
Lower subscapular Posterior cord C567 Subscapularis, Teres
Major
Table 2
PERIPHERAL NERVEThe C5 and C6 roots combine to form the upper
trunk of the
plexus. The point atwhich they become confluent is knownas
Erbs
point.TheC7rootbecomes themiddle trunkand theC8andT1roots
merge into the lower trunk. If, on clinical examination, the
rhom-
boids (dorsal scapular nerve) and serratus anterior (long
thoracic
nerve) are functional the lesion must be distal to Erbs
point.
The trunks divide to form anterior and posterior divisions,
which are located behind the clavicle. The upper trunk gives
off
the nerve to subclavius and the suprascapular nerve,
supplying
supraspinatus and infraspinatus, prior to forming its 2
divisions.
There are no branches given off by the divisions of the
brachial plexus. The posterior divisions all combine to form
the
posterior cord located behind the axillary artery. The
anterior
divisions of the upper and middle trunks form the lateral
cord,
lateral to the axillary artery, and the anterior division of the
lower
trunk forms the medial cord, medial to the axillary artery.
Thereare terminal branches arising from all of the cords. The
lateral
Dorsal rootganglion
A
C-spine
Posterior
B
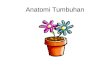
Figure 2 Preganglionic and Postganglionic nerve lesions.
ORTHOPAEDICS AND TRAUMA 23:6 422cord gives off the lateral
pectoral nerve to pectoralis major. The
posterior and medial cords each give rise to 3 terminal
branches.
The posterior cord forms the upper subscapular,
thoracodorsal
and lower subscapular nerves. The medial cord gives rise to
the
medial pectoral nerve, the medial brachial cutaneous nerve
and
the medial antebrachial cutaneous nerve.
The terminal branches of the plexus arise from the cords.
The
posterior cord terminates as the axillary and radial nerves.
The lateral cord contributes to the median nerve and forms
the
musculocutaneous nerve. The medial cord forms the ulnar
nerve
and contributes to the median nerve (Table 2).
Clinical clues to the anatomical location of pathology
When considering the level of an injury to the brachial
plexus
injury, the most important step is determining whether a
lesion
affects the roots and is therefore pre-ganglionic (proximal to
thedorsal root ganglion) or post ganglionic (Figure 2).
Stretch
RupturePOSTGANGLIONIC
Avulsion
PREGANGLIONIC
2009 Elsevier Ltd. All rights reserved.
-
nerve. This has finger-like projections called filopodia,
which
explore the microenvironment. The axon grows and contracts
by
the addition and removal of actin polypeptides. The
filopodia
guide the growing axon towards the distal stump and its
Bynger
bands. It responds to four classes of substances;
neurotrophic
factors, neurite promoting factors, matrix forming precursors
and
metabolic factors.
Pathological changes also occur in the target organs for the
nerve. When their motor supply is lost, muscle cells reduce
in
volume leading to atrophy and interstitial fibrosis.
Denervation
hypersensitivity is produced by an increase in the number of
motor endplates. The muscle then responds to smaller amounts
of acetylcholine than is normally effective, which is detected
as
fibrillations on electromyography (EMG) and clinically may
produce fasciculation. Motor endplates start to be lost
irretriev-
ably after 3 months. Sensory end organs such as Meissner
corpuscles also degenerate, although over a less clearly
defined
time scale than muscle. These end organ changes are the
factor
PERIPHERAL NERVEThere are clinical clues that indicate that an
injury has
occurred in the vicinity of the DRG. If the rhomboids or
serratus
anterior are weak then pre-ganglionic injury should be sus-
pected, as the dorsal scapular and long thoracic nerves arise
at
the proximal ends of their roots. In a non-acute situation
fasi-
culations may be seen in the paraspinal muscles. These are
not
supplied by the plexus but from the dorsal rami, which arise
from
the spinal nerves as they exit the intervertebral foramen.
The T1 root is in close proximity to the T1 sympathetic
ganglion. The inference is that if the T1 sympathetic ganglion
is
injured then it is probable that the T1 root will also have
been
injured. Injury to the T1 sympathetic ganglion will produce
a Horners syndrome of the ipsilateral eye. The 4 components
of
Horners syndrome are; meiosis (unopposed parasympathetic
function), mild ptosis (weakness of Mullers muscle which
assists levator palpebrae superioris), enopthalmos and
facial
anhydrosis.
Classification of peripheral nerve injury
Myelinated peripheral nerve fibres are surrounded by Schwann
cells. Each nerve fibre and its accompanying Schwann cell
are
surrounded by loose vascular tissue called endoneurium.
Bundles of nerve fibers are grouped together into fascicles.
Each
fascicle is covered in a layer of collagen called the
perineurium.
Most nerves consist of numerous fascicles, which are held
together by loose collagenous tissue, which is condensed
peripherally into a strong outer layer; the epineurium.
Seddons classification of nerve injury is widely used and
describes nerve injuries as neurapraxia, axonotmesis and
neu-
rotmesis.8 Neurapraxia is due to a physiological dysfunction
leading to a blockade of nerve conduction. The axon of the
nerve
fibre remains in continuity, without any degeneration of the
nerve distal to the site of injury. There may be a local area
of
myelin damage that is repaired by the Schwann cells9 and
normal
conduction is restored. Axonotmesis describes loss of axonal
continuity of individual nerve fibres but the perineurium is
preserved. Neurotmesis is the most severe injury where all
the
connective tissue elements and axons of the peripheral nerve
are
disrupted.
The category of axonotmesis is very broad and contains
a variety of nerve injuries that have very different
outcomes.
Therefore Seddonss classification was refined by
Sunderland.10
Sunderlands classification is based upon 5 groups. The benefit
of
Sunderlands classification is that it subdivides axonotmesis in
to
injuries that recovery very well (type 2) from those that
have
a poor outcome, (type 4) (Table 3).
The classification systems of Sunderland and Seddon can only
be applied retrospectively or at the time of surgical
exploration.
Birch and Bonney developed a classification system based
upon
neurophysiological testing.11 They defined injuries as those
producing a conduction block and those without a conduction
block with the hope of producing a more clinically useful
clas-
sification system.
Pathophysiology of nerve regeneration
Axonotmesis and neurotmesis involve axonal damage, which
leads to pathological changes along the entire nerve, from
the
nerve distal to the injury up to the cell body.12,13 There
isORTHOPAEDICS AND TRAUMA 23:6 423swelling of the cell body and the
nucleus moves to the periphery
of the cell body. Approximately 10% of the cell bodies may
undergo apoptosis. The rough endoplasmic reticulum changes,
with dispersal of the Nissl granules, which are usually
involved
in neurotransmitter production, in a process called
chromatol-
ysis. These changes occur as the cell switches its synthetic
output
from neurotransmitters to the structural proteins required
for
nerve repair. There is increased synthesis of mRNA, actin,
tubulin and growth factors. The axon proximal to the injury
undergoes retrograde degeneration to the node of Ranvier
prox-
imal to the zone of injury. The nerve stump distal to the point
of
injury undergoes Wallerian degeneration after 48 to 96
hours.
There is demyelination and axonal degeneration. Schwann
cells
proliferate and act to phagocytose the degenerating nerve in
a calcium dependent process. Macrophages rapidly invade the
distal nerve stump removing debris14 and secreting
neurotrophic
factors to commence repair. The neurobiology of nerve repair
has
been discussed in a recent Current Orthopaedics article.15
Once Wallerian degeneration is complete the Schwann cells
begin to align themselves along their basal laminae. This leads
to
the formation of columns of Schwann cells called Bynger
bands.
These columns provide a structural framework for
regeneration.
A growth cone emerges from the proximal end of the divided
Comparison of the Seddon and Sunderland classifi-cation of
peripheral nerve injury
Sunderland
classification
Seddons
classification
Histology
1 Neurapraxia Physiological not
anatomical disruption
2 Axonotmesis Endoneurium and
perineurium intact
3 Axonotmesis Intact Perineurium
4 Axonotmesis Intact Epineurium
5 Neurotmesis All layers disrupted
Table 3 2009 Elsevier Ltd. All rights reserved.
-
that limits the time available for nerve repair. If the
recovering
nerve does not reach the end effectors within approximately
18
months following injury then little functional improvement
will
occur.
In addition to the type of nerve injury other factors
determine
prognosis (Table 4).
Investigations
The aim of investigations is to localise the level of the
brachial
plexus lesion and determine the prognosis for spontaneous
recovery. Knowledge of these two features determines the
subsequent patient management.
Radiological
During the initial assessment of the patient, plain films of
the
clavicle and cervical spine may identify bony injuries and
raise
the clinical suspicion for a brachial plexus injury e.g.
displaced
fracture of the transverse process of the cervical spine,
fracture of
the 1st and 2nd ribs. The complexity of the anatomical
structure
of the plexus, combined with the number of air/fluid/fat
inter-
Histamine test
Now rarely performed, it was of use in differentiating pre-
ganglionic from post ganglionic lesions. A drop of histamine
is
placed on the skin and the skin is scratched through the
hista-
mine. When the nerve is intact a triple response will occur
(vasodilatation, wheal formation and a flare response). The
histamine causes vasodilatation. The wheal is localised
tissue
swelling due to increased capillary permeability secondary
to
histamine and substance P. The flare is a mottled reddening
around the area of skin injury due to mechanical stimulation
of
nociceptive nerve endings and C fibres. This leads to
antidromic
conduction in axon branches, which then release substance P,
which causes vasodilatation and histamine release from mast
cells in the surrounding tissues. When there is nerve
disruption
proximal to the DRG there will be a normal response in an area
of
skin that is anaesthetic. If the nerve is injured distal to the
DRG
there will be vasodilatation and wheal formation in an
anaes-
thetic area of skin but no flare response will occur as this is
an
axon-mediated response requiring a functioning axon in
conti-
nuity with its cell body.
s are
o se
ion
Poorer outcome if arterial injury
reb
ette
lly
rog
m
eco
bro
s. E
PERIPHERAL NERVEAge of patient Better outcome in younger
patients. Ce
changes in sensory input.
Type of nerve Purely motor or sensory nerves have b
reach an end organ that they can usefu
superficial radial nerve.
Level of injury Supraclavicular injuries have a poorer p
prognosis.
Pain Patients who have persistent pain for 6
prognosis with regard to neurological r
Time interval injury to surgery If surgery is delayed for months
then fi
Patient factors Other medical co-morbidities, infection
Table 4Traction poorer than sharp divisfaces (due to its
proximity to the lungs and vasculature struc-
tures) make interpretation of brachial plexus imaging
difficult.
The main role of imaging in traumatic brachial plexus
injuries
is to differentiate root avulsions from more distal injuries.
Roots
are approximately 1 mm thick and, until recently, the
conven-
tional slice thickness of CT and MR imaging was greater than
this. Improvements in hardware and scanning sequences mean
that useful information can now be obtained.
MR scanning is useful in the investigation of non-traumatic
lesions because of the wide variety of pathology that may be
responsible for non-traumatic brachial plexus dysfunction;
infil-
trating tumours, compressive tumours, radiation injury,
idio-
pathic brachial neuritis and vasculitic/granulomatous
conditions
may all result in a brachial plexopathy. Oedema on a T2
weighted scan indicates the zone of injury and if it is within
or
around the plexus it implies injury if the clinical
situation
correlates with a plexus injury.
Factors affecting outcome of peripheral nerve injury
Factor Effect
Mechanism of injury High energy poorer prognosis related
tORTHOPAEDICS AND TRAUMA 23:6 424verity of injury.
ral cortex plasticity allows adaption to new sizes of motor
units and
r functional recovery than mixed nerves (growth cones more
likely to
supply). Some pure nerves do poorly for unknown reasons eg
nosis than infraclavicular injuries. Upper trunk lesions have
the best
onths after a brachial plexus injury have a poorer
very.
sis and degeneration of end organs make for a poorer outcome
ffect of smoking unknown but thought to be detrimental.stimulus
arrive. The period during which the Na channelBasic
electrophysiology
Action potentials (AP) are transient changes in axon
membrane
potential, which are conducted over considerable distances
without any change in amplitude. Neurons have a negative
resting membrane potential - their internal charge is
negative
relative to the surrounding environment. This is due to the
rela-
tive levels of K, Na and Cl across the membrane. The
restingmembrane potential for neurons is approximately70 mV.Whena
neuron is stimulated above its threshold for activation there
is
a rapid influx of Na, which causes depolarisation. Themembrane
potential usually reaches approximately 30 mVbefore the Na channels
are inactivated. Voltage sensitiveK channels open and release
potassium into the surroundingenvironment and Cl channels allow
chloride into the cell tore-establish the negative membrane
potential of 70 mV. Thesodium channels are then capable of
reactivation should another 2009 Elsevier Ltd. All rights
reserved.
-
ed to
Changes in conduction velocity and amplitude can be used to
help
differentiate between types of nerve injury andmay
indicatewhether
demyelination or axonal damage or both has occurred (Figure
4).
5
10
15
20
mV
NormalVelocity
Reduced
ixed
Demylinat
ing
PERIPHERAL NERVEobtain greater reproducibility of results. The
response of the
distal motor unit is usually recorded by a surface electrode
placed on the skin overlying the belly of the target muscle.
Needle electrodes are occasionally required if there has
been
profound muscle wasting. The recording from the muscle is
called the motor action potential (MAP) or the compound
muscle AP (CMAP). The CMAP represents a summation of the
voltage responses from individual muscle fibre action
potentials.
The time from the stimulus being applied and the appearance
of
the MAP is called the distal motor latency. This period of time
is
a composite of the time taken for nerve excitation, conduction
of
the AP, Acetylcholine release at the NMJ and generation ofhave
an effect on the amplitude of the motor potential. T
a supra-maximal stimulus. A supra-maximal stimulus is usclosed
as the cell repolarises is called the refractory period, as the
cell is unable to respond in this period to standard
stimuli.
At any time only a small area of the axon is depolarised as
the
AP passes along it. The flow of the AP is unidirectional, as
the
area the AP has passed through will enter a refractory period
and
reversal of the direction of flow is thereby prevented.
AP velocity is increased by increasing nerve fibre size, as
in
these circumstances there are more ions within the cell to
carry
the current. Myelination means that depolarisation is limited
to
the nodes of Ranvier. This reduces the number of
depolarisations
required to travel the length of the nerve (salutatory
conduction).
Nerve conduction studies (NCS)
Motor studies (Figure 3): An electrical stimulus is applied to
the
skin directly over a nerve. The electrical stimulus intensity
is
gradually increased until a further increase in stimulus does
not
his is
5 10 15 20 25 30 35 40 45 50
m/s
Figure 3 CMAP recording - biphasic, large amplitude and long
duration ofthe potential.a post synaptic muscle potential to
trigger the muscle response.
To calculate conduction velocity the nerve must be stimulated
at
2 points along its course with the MAP being measured by the
same muscle electrode. To remove the effect of the distal
apparatus the conduction velocity is then calculated.
The normal conduction velocity in the upper limbs is between
45 and 60 m/s, whilst in the lower limb it is between 40 and
55
Conduction Velocitym=s Distance bproxima
ORTHOPAEDICS AND TRAUMA 23:6 425m/s but absolute values vary
between patients and with different
recording apparatus. Intra-examiner variability is low but
there
can be considerable inter-observer variability of sensory
and
motor amplitudes.16 For this reason serial studies should be
performed by the same neurophysiologist.
The amplitude of the CMAP relates to the number of working
muscle fibres in the muscle sampled. The conduction velocity
is
proportional to the nerve diameter. Conduction velocity is
lower
in unmyelinated axons and axons which have undergone
demylination. Motor and sensory conduction velocity
decreases
with age; 0.4e1.7 m/s per decade after 20 years of age for
motor
and 2e4 m/s for sensory.17
After the CMAP has been recorded there may be observed the
appearance of a small F wave. This is a rebound phenomenon.
The
nerve has been stimulated somewhere along its length
therefore
the AP can move proximally and distally (unlike under normal
circumstances where the AP begins either proximally or
distally).
The AP therefore passes up the nerve to the motoneurone cell
body
and then comes back down the nerve, eventually reaching the
recording electrode after the CMAP. F waves are a sensitive
marker
of nerve pathology and are useful when the lesion is very
proximal
and not therefore easily accessible by routine NCS
techniques.
Reduced
Amplitu
de
M
Axonal
Figure 4 Differentiating types of nerve lesions using changes in
conduc-tion velocity and amplitude.Sensory studies (Figure 5): A
sensory nerve is stimulated distally
and the response is recorded proximally. The proximal
response
is called the Sensory Nerve Action Potential (SNAP). In the
upper
limb sensory nerves are often stimulated by the use of a
ring
electrode placed on a digit served by the nerve of interest
e.g.
middle finger for median nerve. SNAPs are much smaller than
CMAPs e in the micro-volt range. The conduction velocity and
etween the 2 sites of nerve stimulus
l latencyms distal latencyms
2009 Elsevier Ltd. All rights reserved.
-
erve
denervation changes are localized to deltoid, triceps and
extensor
digitorum communis a posterior cord lesion should suspected.
EMG is able to differentiate myopathic from neuropathic
causes of muscle weakness. EMG can also identify the first
signs of recovery after nerve injury. As the regenerating
motor
axons start reforming motor units they initially conduct at
a slower velocity, leading to low amplitude complex poly-
phasic waveforms being recorded from the muscle. These are
called nascent potentials and are an early sign of
reinnerva-
tion. Nascent potentials are the only way to differentiate
temporary from permanent denervation. As recovery
continues the waveforms become greater in amplitude and
have a simpler waveform. When reinnervation is complete the
EMG will still not be completely normal, as the size of the
1
10
20
30
40
2 3 4 5 6 7 8 9 10
uv
m/s
Figure 5 SNAP recording - triphasic, small amplitude and short
duration of
potential.
PERIPHERAL NERVEroots or anterior horn cell diseases. They are
caused by hyper-
sensitivity to acetylcholine as receptor numbers are
up-regulated
to compensate for the reduced/lost innervation. The
acetylcho-
line receptors are also found outside the confines of the
previous
neuromuscular junction spreading across the whole muscle
surface. Fasciculations may be seen; these represent
spontaneous
discharges. They develop approximately 7e14 days after
dener-
vation. Muscles are sampled by EMG to map the distribution
of
denervation changes. This information can then be interpreted
to
allow localization of a brachial plexus lesion. For example
ifproduce complex discharges. Spontaneous discharges are a
of partial or complete denervation, compression of spinal
namplitude can be calculated. The amplitude of the SNAP gives
an
indication of the number of functioning axons. It is also
affected
by the synchrony of the AP arriving at the recording site e i.e.
AP
arriving over a prolonged period will cause reduced peak
SNAP
amplitude. Demylination will lead to a small SNAP as the AP
will
have greater temporal spread. Axonal degeneration will lead
to
an absent SNAP. Age does have an effect on the SNAP.
For further information regarding the technical aspects of
nerve conduction studies the following reference is
suggested.17
Electromyography (EMG)
A needle is placed into a muscle to record the activity of
motor
units at rest and on muscle contraction. The needle records
from
a radius of approximately 1 mm around the needle. The number
of motor units in this field will vary between muscles.
A normal muscle will not have any spontaneous activity. A
sub-maximal contraction will allow individual motor unit
potentials to be identified and a maximal contraction will
signSummary of neurophysiological findings for the
categoriNeurophysiological differentiation between axonotmesis
and
Neurapraxia
Conduction velocity Normal in most cases
CMAP Amplitude Normal/Reduced
SNAP Amplitude Reduced
Spontaneous Activity on EMG Absent
Table 5
ORTHOPAEDICS AND TRAUMA 23:6 426motor units will be larger than
prior to injury. To compensate
for this the firing pattern of each motor unit will be
different,
usually with increased firing rates to try and maintain
force
production.
For further information regarding the technical aspects of
electromyography the following reference is suggested.18
The neurophysiologic findings seen in nerve injuries are
shown in Table 5.
Neurophysiological assessment of the brachial plexus
Neurophysiology can confirm the diagnosis of a brachial
plexus
injury. It can localise the site of the lesion, attempt to
quantify the
degree of axonal loss and identify if recovery is occurring.
Initial
NCS should be performed 3e4 weeks after injury, as Wallerian
degeneration will have been completed. Denervation changes
maybe seen in 10e14 days but can take up to 40 days to
appear.
Proximal muscles are affected prior to distal muscles. When
denervation changes occur in the cervical paraspinal
muscles,
rhomboids or serratus anterior it implies the lesion is proximal
to
the brachial plexus. Motor responses are affected before
sensory
responses when measured on NCS .16 The CMAP will be reduced
in amplitude, reflecting the loss of axons if an injury of
greater
severity than neurapraxia/Sunderland 1 has been sustained.
The SNAP can indicate if a lesion is pre- or post-ganglionic.
If
a SNAP is present the lesion is proximal to the sensory
nerve
bodies in the DRG. If the SNAP is absent or reduced the lesion
is
distal to the DRG. The number of intact axons dictates the
amplitude of the SNAP. One limitation is that a SNAP may be
absent due to a post-ganglionic injury but there may also be
a coexistent injury at the pre-ganglionic level.
es of peripheral nerve injury as defined by Seddon.neurotmesis
can be challenging
Axonotmesis Neurotmesis
Normal/slight reduction Absent
Reduced Absent
Reduced Absent
Maybe present Present 2009 Elsevier Ltd. All rights
reserved.
-
artefact when recording NAPs.
PERIPHERAL NERVEIf no NAP is recordable across a lesion then
grafting is per-
formed if the proximal nerve root is in continuity. The
presence
of a NAP across a lesion indicates either preserved axons or
that
recovering axons have now traversed the lesion. If the nerves
are
judged to be functional neurolysis rather than grafting may
be
appropriate.
Somato-sensory evoked potentials (SSEP) and cortical evoked
potentials have also been used for intraoperative monitoring.
If
an SSEP is present then there is contact between the
peripheral
sensory nerve and the CNS suggesting that the DRG is
intact.19
Management of open injuries
Open injuries are not common and range from minor
penetrating
wounds to complex major blast injuries with near amputation
of
the upper limb. These injuries are usually caused by sharp
penetrating implements or missiles, resulting in a neurotmesis.
In
this situation, with sharp division of the nerve(s), primary
exploration and repair in the acute setting should be attempted
if
the patients other injuries allow. It is not unusual however
for
additional injuries to the major vessels or thoracic viscera
to
preclude immediate exploration and in these cases repair must
be
delayed. If a cursory plexus inspection and tagging of the
injured
nerves is possible during the management of concurrent
injuries
the opportunity should be taken.
If there is a delay between the initial injury and
presentation
to the clinician responsible for the management of the
brachial
plexus injury, then all wounds and other injuries should be
left
to stabilise before considering any further surgical
intervention.
The opportunity may be taken to perform EMG during this
period at 3e4 weeks, aiming for exploration and repair at
4e6
weeks. Due to the delay, in these cases primary nerve repair
may not be possible because of nerve retraction or following
the
resection of neuromatous stumps, necessitating the need for
nerve grafting. Neurolysis of scarred nerve ends may also
beThere is a lot of overlapping innervation of the paraspinal
muscles. One root injury may cause fibrillation potentials
in
more than one paraspinal level. Therefore the number of
para-
spinal fibrillations cannot tell you how many root injuries
there
are, only that at least one root injury is present. However if
no
paraspinal fibrillations are recorded then it is possible to say
that
no root injuries have occurred.
Nascent potentials on EMG and reduced fibrillations can
point
to nerve recovery long before clinical recovery is apparent.
Nascent potentials indicate that nerve fibres have reached
the
muscles and established motor end-plate connections. However
EMG recovery does not always equate to useful clinical
recovery.
Some centres use intra-operative nerve conduction studies.
The nerves of the plexus are stimulated across their damaged
areas to identify whether there are functional axons. These
are
NAPs e nerve action potentials. They measure activity in
sensory
and motor fibres in mixed nerves along the length of nerve
tested
with no distal organ effect being measured. The nerve is
stimu-
lated directly with an electrode and the recording is
performed
with a hook or forceps type electrode at least 4 cm away from
the
stimulating electrode. Four cm of separation between the
stim-
ulating and recording electrodes is essential to produce
reliable
recording of NAPs intra-operatively. There is a lot of
stimulusORTHOPAEDICS AND TRAUMA 23:6 427Non-surgical management
The goals are to maintain passive motion, to strengthen
those
muscles that remain functional, to protect anaesthetic skin
areas
and to control pain. Physiotherapy plays an important role
in
maintaining passive motion as well as strengthening muscles.
A
home programme of physiotherapy should run alongside struc-
tured departmental sessions, to maximise the functional
outcome
of the limb. Functional splinting will complement
physiotherapy.
Chronic oedema can develop secondary to dependent posi-
tioning, loss of vascular tone due to sympathetic nerve
dener-
vation and concurrent soft tissue injury to the limb.
Elevation,
bracing and compression garments can all be used to reduce
the
oedema that, if ignored, can lead to stiffness, particularly in
the
hand.
The mainstay of the management of anaesthetic skin is
education, and the program is essentially the same as for
diabetic
neuropathy with patients avoiding extreme temperatures and
inspecting the insensate area daily.
The management of pain can be difficult and significant pain
is more common with total plexus injuries than partial,
particu-
larly with root avulsions. Pain, in addition to being very
dis-
tressing, can also compromise rehabilitation, and its control
is
paramount. Restoration of function, both of the limb and the
patient, including the return to employment, is often the
most
effective form of pain control. The use of pharmacological
agents
is vital, but dependency and side effects must be taken into
account. Non-steroidal anti-inflammatories and opioids
insti-
gated at the time of injury may become ineffective with
time,
particularly in relation to neuropathic pain. In these cases
there isthese injuries.required in these cases. In one of the
biggest series in the
literature of stab wounds to the plexus Dunkerton reported
good
results with early exploration, with a better prognosis
associated
with C5/C6 lesions.20
Open injuries secondary to low-velocity missiles (gunshot
wounds), do not warrant early exploration. This is because
the
resultant injuries are mostly neurapraxic.21 It must be
added,
though, that as technology advances more powerful weapons
are
being produced leading to an increase in severe stretch
injuries
(lesions in continuity) to the plexus. If there is no
associated
vascular or thoracic injury, conservative management with
local
wound care is advocated. If no recovery is seen by 3 months
exploration with repair/grafting is indicated. Kline reported
on
a large series of civilian gunshot wounds in the era of low-
velocity weapons and found the best surgical outcomes were
associated with upper trunk and lateral and posterior cord
injuries.
Management of closed injuries
In the absence of any open wounds and life-threatening
injuries
surgery is not traditionally the first line of treatment. The
initial
management is observation, pain control and physiotherapy.
Electromyography is performed at 3e4 weeks and a myelogram
or magnetic resonance imaging at 6e8 weeks if a neurological
deficit persists. If function fails to return, or if initial
neurological
recovery ceases, then surgical exploration is justified at 3 to
6
months, although there is no uniformly accepted algorithm for
2009 Elsevier Ltd. All rights reserved.
-
h the
in of
PERIPHERAL NERVEa role for carefully titrated doses of
anti-epileptics (gabapentin
and carbamazipine) or tricyclic anti-depressant (amitriptyline).
It
should be noted, though, that only one third of patients
report
significant pain relief with these medications.22 Other
modalities
including counseling, biofeedback, hypnosis, acupuncture and
transcutaneous nerve stimulation have all been used with
mixed
results. Severe cases of intractable pain, which do not respond
to
the above non-surgical measures, can be considered for
dorsal
root entry zone (DREZ) ablation, described by Nashold23 or
the
use of implantable dorsal root stimulators. Pain control should
be
managed by a multi-disciplinary team and customised to the
character of the pain and to the patient. Access to a pain
clinic is
an important adjunct.
Surgical management
Considerable advances have been made since the early 1900s,
when attempts at surgical repair and neurolysis proved
almost
futile. Modern microsurgical techniques have led to improved
results, but as of yet no definitive management algorithm
has
been constructed and uniformly accepted. There are several
general statements concerning surgical intervention of
closed
injuries that can be made:
1. Patients who have complete loss of C5, C6 and C7 root
functions have the most to gain
2. Nerve grafting of the upper roots is often possible as
rupture,
not avulsion, is the usual mechanism of injury.
3. Grafting C8 and T1 is often not an option, as at this
level
avulsion injuries are likely to have occured. If grafting is
possible it is only likely to provide protective sensation
and
no meaningful motor recovery. This is because muscle
atrophy occurs prior to reinnervation of the finger flexors
and intrinsics due to the considerable distance the regen-
erated nerves have to travel.
4. In a child any complete lesion regardless of level should
be
repaired and grafted if possible.
5. Across the literature, timing of surgery most commonly
occurs between 3e6 months.
Surgical approach to the brachial plexus
The plexus can be exposed in its entirety or partially,
depending
on the procedure being performed and the extent of the
injury.
The patient is positioned for primary exposure allowing for
intra-
operative adjustment. Any potential nerve grafts and
transfer
sites and must also be readily accessible (intercostals or
sural
nerve, for example).
Under general anaesthesia, with the use of a short acting
muscle relaxant for intubation to allow for intra-operative
nerve
stimulation, the patient is placed in the semi-recumbent
beach
chair position with the neck slightly extended and turned to
the
contralateral shoulder. The arm is prepared so that it can
be
moved intra-operatively to aid dissection.
The surface markings for exploration of the supraclavicular
plexus are the posterior border of sternocleidomastoid and a
line
just superior and parallel to the clavicle. The skin and
superficial
fascia are incised and subplatysmal flaps are raised to
improve
exposure. Deep to the platysma are the external jugular
vein,
which is retracted medially, and the cervical plexus, which
should be preserved where possible to prevent
neuromaORTHOPAEDICS AND TRAUMA 23:6 428the vertebral artery lies
close, as does the lung pleura.
Clavicular osteotomy can be performed to increase exposure,
facilitating closure by preparing a pre-contoured plate and
pre-
drilling the lateral screws. The clavicle should be divided
via
a low energy osteotomy at an oblique angle.
The infraclavicular plexus is exposed through the delto-
pectoral groove (Figure 6aef). To expose the entire plexus
the
supraclavicular and infraclavicular approaches are linked
over
the lateral clavicle. The cephalic vein is preserved and
mobilised
laterally with the deltoid. The delto-pectoral interval is
developed
and the clavicular attachments of pectoralis major and
deltoid
may be partially released to optimise exposure. Distal
exposure
requires the release of the humeral attachment of pectoralis
major. Pectoralis minor is divided close to its insertion onto
the
coracoid (a stay suture is placed in the tendon) to expose a
fat
pad which is swept aside bringing the cords of the brachial
plexus into view. The lateral cord is the most readily
identifiable
and deep to this is the axillary artery which requires
mobilisation
and protection. The medial and posterior cords are identified
in
relation to the artery. The cords can be traced both distally,
to
identify the branches, and proximally, to locate the
divisions.
Surgical options
A variety of surgical strategies exist to improve function and
the
choice used will depend on the extent and location of the
injury.
A clear surgical plan with realistic expectations of the
outcome
should be discussed with the patient. Surgical options
available
include:
Neurolysis
Lesions in continuity, with external compression or scarring,
can
be treated with neurolysis. For these procedures to be
successful
the fascicular pattern and endoneural tissue must be preserved.
If
there is concern or doubt over the integrity of the fascicle
pattern,
resection of the segment and grafting is preferred.
Nerve grafting
This forms the basis of modern post-ganglionic plexus
surgery.
Anatomical reconstruction, with connection of the proximal
and
distal stumps is attempted. The limiting factors in
reconstruction
tend to be the length of the gap that requires grafting and
the
availability of a sufficient nerve graft. Therefore, priority is
given
to 1, restoration of elbow flexion, 2, restoration of
shoulder
abduction, and 3, restoration of sensation on the medial
borderligated if necessary. To access the lower trunk the subcl
vasculature is mobilised and retracted with care as the
origsubclavian vein anteriorly and the subclavian artery
posteriorly.
For proximal foraminal exposure scalenius anterior is
divided.
The upper trunk is located by tracing the C5 and C6 roots
distally,
the middle trunk being found both deeper and medial to this.
Access may be limited by the transverse cervical artery, which
is
avianthe lateral edge of the muscle. The lower roots can be
visua
distally by retraction of scalenius anterior, taking care
witformation. Omohyoid muscle, which signals the transition
from
superficial to deep dissection, is divided and the
supraclavicular
fat pad is swept away from the operative site. Below the fat pad
is
the transverse cervical artery with Erbs point deep to this.
The phrenic nerve is identified, closely applied to scalenus
anterior, and is followed proximally to identify the root of C5
at
lised 2009 Elsevier Ltd. All rights reserved.
-
PERIPHERAL NERVEof the forearm. The commonly used donor sensory
nerves for
grafting are, sural, saphenous, medial brachial and
antebrachial
cutaneous and superficial radial nerves. Vascularised nerve
grafts24 have added another possibility and the most
commonly
used is the ulnar nerve. In these cases the ulnar nerve should
be
split into minor units roughly the size of the sural nerve
before
grafting, in order to increase chances of success.25
Nerve transfer (Neurotization)
Neurotization is used more often in pre-ganglionic lesions.
Nerve
fibres from one nerve are transferred to a denervated nerve,
in
order to neurotize the nerve. Motor nerves have to be used
as
donors to restore motor function and sensory nerves to
restore
sensory function. Classically this technique involves
sacrificing
Intra-operative photographs demonstrating exposure of the
terminal bran
Figure 6
ORTHOPAEDICS AND TRAUMA 23:6 429the function of the axon donor,
but new end-to-side26 techniques
mean this is not necessarily the case. From a surgical point
of
view it must also be considered whether the donor nerve can
be
transferred without tension. Table 6 shows the donor nerves
commonly used for transfers.
Some surgeons prefer to use intraplexus donors suggesting
they give better results, due to the greater number of axons
compared with extraplexus donors, therefore increasing the
chances of successful neurotization27. Despite this
viewpoint,
some extraplexus donors give consistently good results in
clinical
practice; the intercostals when used for shoulder and elbow
function are reported to give up to 70% good to excellent
results.27 The accessory nerve, according to published studies,
is
also a reliable donor.27
ches of the brachial plexus.
2009 Elsevier Ltd. All rights reserved.
-
work has emerged on human subjects. Despite this, to date,
this surgical option has not reached the stage where it
warrants
re is
unlikely to be any substantial gain in function from
shoulder
PERIPHERAL NERVEinclusion in the standard surgical
armamentarium.
As with all peripheral nerve injuries, a considerable number
of factors influence the results of surgery to the brachial
plexus.
As a result, firm statements regarding the prognosis of
surgery
are difficult to justify. The literature indicates overall
that
younger patients do better, as do upper plexus injuries.
This
almost certainly reflects the fact that in upper lesions the
target
organs are much closer to the plexus, making regeneration
more
likely. Terzis27 in a series of over two hundred surgically
managed plexus injuries reported good to excellent results
in
75% of suprascapular nerve reconstructions, 40% of biceps
reconstructions, 30% of triceps reconstructions, 35% finger
flexion reconstructions and 15% of finger extension
reconstruc-
tions. Restoration of hand function secondary to a lower
plexus
injury remains the most difficult area to address, but with
aggressive management, according to Terzis, it is not out of
the
question.
Late reconstruction
In cases where spontaneous recovery has not occurred, or
when
surgical intervention has failed to yield any functional
benefit,
then late reconstructive options should be considered. In
suchRepair of avulsed spinal nerve roots has been attempted by
many, with Bonney and Jamieson reporting on a case in 1979.
Both Jamieson and Carlstedt have published experimental work
on animal models with some functional success28,29 and
early30,31
Donor nerves used for transfer
Donor nerve for transfer Described
Intercostal (to Musculocutaneous) Seddon 1961
Ipisilateral Cervical Plexus Brunelli 1980
Contralateral Lateral Pectoral Gibert 1992
Accessory Bonnel 1984
Hypoglossal Narakas 1984
Phrenic Zhen 1989
Contra lateral C7 Chen 1991
Ulnar nerve to Musculocutaneous Oberlin 1997
Table 6cases there needs to be conclusive evidence that
neurological
recovery is unlikely, or sufficient time has elapsed without
functional improvement following the injury. Many of the
tech-
niques used in reconstruction have been adapted from use in
poliomyelitis and peripheral nerve injuries. It must be
acknowl-
edged, however, that in poliomyelitis there is no loss of
sensation
and thus in plexus injuries the functional benefits from
motor
improvement maybe less. The primary procedures in peripheral
reconstruction are arthrodesis and tendon transfers, with
the
newer technique of free muscle transfers becoming an option.
There is also a limited place for amputation.
Numerous procedures have been described to improve the
function of the upper limb and, as previously stated, it is
important to assess each individual patient carefully and to
determine from which procedures they are likely to derive
the
f the
ORTHOPAEDICS AND TRAUMA 23:6 430paralysis and donor muscles
available. Thus, no precise
management algorithm can be constructed, although Alnot in
199633 outlined his surgical approach to shoulder muscle
palsies
(Table 7).sion as to which is used will depend on the exact
nature oarthrodesis.
Integrity of the acromioclavicular, sternoclavicular
andscapulothoracic joints should be considered. Stiffness of
these
joints may limit the success of arthrodesis and it is also
important to ensure the acromioclavicular joint is not
incor-
porated into the arthrodesis
With advances in bone fixation, especially rigid compression
plating, the need for prolonged postoperative immobilisation
is
no longer required. The most common position for arthrodesis
is
20 of abduction, 30 of flexion and 30 internal
rotation.Excessive abduction must be avoided, as it leads to
chronic
fatigue around the shoulder girdle. This position should
give
a strong and functional shoulder to feed and address
personal
hygiene with an average movement of 60 of abduction andflexion32
being possible via the scapulothoracic articulation.
Shoulder arthrodesis gives predictable results and can
improve
the function of the limb considerably. The strength and
move-
ment is greater than is achieved with muscle transfers, but
does
depend on the scapulothoracic muscles. It should be born in
mind when combining shoulder arthrodesis with other distal
procedures, that following the arthrodesis it can be difficult
to
position the arm and thus the distal procedures may be more
easily performed first.
Tendon transfers to the shoulder
In cases where only partial paralysis of the shoulder has
occurred
arthrodesismaynot be necessary and tendon transfers are
sufficient
to restore function. Many transfers have been described
including:
Trapezius to deltoid insertion on the humerus
(Batemanprocedure)
Latissimus dorsi and teres major to the posterolateralhumerus
(LEpiscopo) to improve external rotation
Anterior advancement of the posterior portion of deltoid
toreplace non-functioning anterior segment.
Transfer of the long head of triceps to the acromionThere are
many other described transfers and the final deci- Good distal
function of the arm is needed for the procedube worthwhile. If the
hand is completely paralysed themost benefit. In essence,
peripheral reconstruction is aimed at
restoring shoulder stability, with or without movement, in
addition to restoring elbow flexion and hand function.
Shoulder arthrodesis
The role of shoulder arthrodesis is two-fold. Firstly, in
total
plexus palsies, by stabilising the shoulder it enables the
surgeon
to concentrate all available nerve grafts and transfers,
which
maybe limited, on restoring elbow and hand function.
Secondly,
in upper plexus palsies, it may be of benefit in unstable
shoulders
(painful, subluxing or dislocating) where attempts to
stabilise
have failed or where it is not appropriate to undertake such
procedures in the first place. Certain aspects are worth
consid-
ering when planning shoulder arthrodesis:
Good scapulothoracic muscle function is vitalre to 2009 Elsevier
Ltd. All rights reserved.
-
ce in
PERIPHERAL NERVE Sternocleidomastoid - rarely used due to web
appearanTendon transfers to restore elbow flexion
Elbow flexion plays a vital role in upper limb function and
its
restoration can significantly improve a patients functional
outcome. Depending on the level of the lesion and the degree
of
successful reinnervation different reconstructive procedures
are
available. Once again the final decision depends on the
precise
functional deficit and on available donor muscles. When
consid-
eringwhich transfer to use,muscle excursion, alignment,
cosmesis
and pre-existing range of movement must be considered. The
aim
of surgery is to restore good strength through a functional
range of
30 to 130without excessive pronation. The commondonors usedin
transfers to restore elbow flexion are:
Proximal advancement of the common origin of the
forearmflexor-pronator muscles (Steindler) - historically most
popular, but can be weak and can lead to flexion
contractures
and excessive pronation.
Latissimus dorsi - good power and excursion but
frequentlydenervated along with elbow flexors and thus
unavailable.
Pectoralis major (Clarke) - requires stable or
arthrodesedshoulder to establish correct tension
Pectoralis minor - stable or arthrodesed shoulder Triceps - good
strength, excursion and cosmesis but loss of
extension is a high price to pay.Table 7Alnots surgical approach
to shoulder muscle palsies
Deltoid muscle palsy only Trapezius to deltoid (Bateman)
or
Long head triceps to Acromion
Deltoid & Infraspinatus palsy Derotation osteotomy of
humeral
shaft for external rotation
Deltoid, Infraspinatus &
Supraspinatus
Stabilisation shoulder with long
head of biceps
Derotation osteotomy
Shoulder arthrodesis
Trapezius transferneck and the occasional need to preposition
the head to
achieve elbow flexion.
Tendon transfers to restore hand function
This is a very difficult area to address and there are no
simple
solutions. In essence the tendon transfers available are
those
commonly used for isolated peripheral nerve injuries and to
cover them exhaustively is beyond the scope of this review.
The
most notable difference is that often the donor muscles used
in
isolated median, ulnar and radial nerve palsies are not
neces-
sarily available or expendable in a brachial plexus lesion, due
to
the more global effect they have on hand function. As with
all
tendon transfers, consideration must be given to the
potential
gains from the procedure and also the functional loses that
will
occur. Ultimately the treating clinician must assess and
discuss
with the patient the available options including risks and
benefits
and come to a mutual conclusion as to what is the best
management plan. hilst
ORTHOPAEDICS AND TRAUMA 23:6 431Unfortunately brachial plexus
injuries are becoming increas
common and they result in a very significant disability, wFree
muscle transfers
Free muscle transfers are a feasible option in reconstruction
of
elbow flexion and prehensile reconstruction of the hand.34,35
In
order for these transfers to function it is necessary for the
prox-
imal joints to be stable. Thus in reconstruction of elbow
flexion
function is compromised if the shoulder is not stable, and
this
must be addressed either at the same time or before the free
muscle transfer. When addressing finger function, stability of
the
elbow and wrist is mandatory. In addition to proximal joint
stability the presence of an antagonistic muscle greatly
influences
functional outcome. The weight of the limb and the effects
of
gravity to a certain extent act as antagonists, but this is
often not
enough, and thus when addressing finger flexion in the
absence
of active extension, splinting may be required. Double free
muscle transfers may deal with this potential problem.35 The
donor muscles commonly used are latissimus dorsi, gracilis
and
rectus femoris. Consideration must be given to donor muscle
blood supply, length, volume and shape. Latissimus dorsi and
rectus femoris are mainly used for restoration of elbow
flexion
whereas gracilis due to its shape and amplitude of contraction
is
the preferred donor for wrist and finger function.
Orthotics
The role of orthotics should not be forgotten in brachial
plexus
injuries, in both the non-surgically and surgically managed
cases.
They can be used to immobilise, stabilise, and support a joint
in
a desired position, protect weak muscles from overstretch,
prevent contractures and support structures following
surgical
repair. They can be used instead of, or alongside, late
recon-
struction to enhance the function of the limb. A static orthosis
is
primarily intended to stabilise joints or place the limb in a
posi-
tion of function. Dynamic orthoses are often more complex
and
intended to more than simply stabilise a joint. Multiple
dynamic
orthoses are available including shoulder, elbow, wrist and
hand
orthotics. The exact orthoses used will depend on the
functional
deficit and needs of the patient as assessed by a trained
orthotist.
Consideration must be given to ease of use, wear and
application
as well as the risks of skin problems, particularly with
anaes-
thetic skin. Despite some patients finding orthotics
undesirable,
they can be a very useful adjunct to management.
Amputation
With theadventof themodern techniques inbrachial plexus
injuries
discussed above there has been a significant shift away from
amputation. This has occurred to the extent that Tervis in
1999
claimed Amputation has no place in the modern treatment of
traumatic plexopathies.With that considered, in some
caseswhere
reconstruction has failed and the patient is left with a flail
useless
arm, struggles with the weight of it and fails to properly care
for the
anaesthetic skin, amputation is a viable option. The amputation
can
be at any level, depending on the needs of the patient and
maybe
combined with shoulder arthrodesis. Amputation is not an
appro-
priate option for those who request it for neurological pain
relief.
Summary
ingly 2009 Elsevier Ltd. All rights reserved.
-
occurring in young individuals, usually of working age.
Conser-
vative management helps control pain and maintain movement
and function. Recent technical advances, however, have
signifi-
cantly increased the role of early surgery employing
neurolysis,
nerve grafting and nerve transfer. Functionmay also be helped
by,
or in combinationwith, shoulder arthrodesis and a range of
tendon
transfers to capitalise on any remaining functioning muscle
units.
The care of patients with plexus injuries is complex and
requires
a multiskilled, multidisciplinary approach for the best results.
A
19 Hetreed MA, Howard LA, Birch R. Evaluation of sensory
evoked
potentials recorded from nerve roots to the cervical epidural
space
during brachial plexus surgery. In: Jones SJ, Boyd S, Hetree
M,
Smith NJ, eds. Handbook of spinal cord monitoring.
Dordrecht:
Kluwer Academic Publishers, 1994. p. 171e8.
20 Dunkerton MC, Boome RS. Stab wounds involving the
brachial
plexus. J Bone Joint Surg 1988; 70B: 566e70.
21 Kline Dg. Civilian gunshot wounds to the brachial plexus. J
Neurosurg
1989; 70: 166e74.
22 Leffert RD. Brachial plexus injuries in the adult. In: Norris
TR, ed.
PERIPHERAL NERVEREFERENCES
1 Barnes R. Traction injuries of the brachial plexus in adults.
J Bone
Joint Surg 1949; 31B: 10e6.
2 Bonney G. Prognosis in traction lesions of the brachial
plexus. J Bone
Joint Surg 1959; 41B: 4e35.
3 Leffert RD, Seddon H. Infraclavicular brachial plexus
injuries. J Bone
Joint Surg 1965; 49B: 9e22.
4 Narakas A. Surgical treatment of traction injuries of the
brachial
plexus. Clin Orthop 1978; 133: 71e90.
5 Yeoman PM, Seddon HJ. Brachial plexus injuries: treatment of
the flail
arm. J Bone Joint Surg 1961; 43B: 493e500.
6 Leffert RD. Brachial plexus injuries. N Engl J Med 1974; 291:
1059e67.
7 Kerr A. Brachial plexus of nerves in man. the variations in
its
formation and branches. Am J Anat 1918; 23: 285.
8 Seddon HJ. Three types of nerve injury. Brain 1943; 66:
238e88.
9 DeVries GH. Schwann cell proliferation. In: Dyck PJ, Thomas
PK,
Griffin JW, et al., eds. Peripheral neuropathy. Philadelphia:
WB
Saunders, 1993. p. 290e8.
10 Sunderland S. A classification of peripheral nerve injuries
producing
loss of function. Brain 1951; 74: 491e516.
11 Birch R, Bonney G, Wynn Parry CB. Surgical disorders of the
periph-
eral nerves. Edinburgh: Churchill Livingstone, 1998.
12 Lieberman AR. The axonal reaction. a review of the principal
features of
perikaryal responses to axon injury. Int Rev Neurobiol 1971; 14:
49e124.
13 Price DL, Porter K. The response of ventral horn neurns to
axonal
transaction. J Cell Biol 1972; 53: 24e37.
14 Stoll G, Griffin JW, Li CY, Trapp BD. Wallerian degeneration
in the
peripheral nervous system: participation of both schwann cells
and
macrophages in myelin degredation. J Neurocytol 1989; 18:
671e83.
15 Dahlin LB. Nerve Injuries. Curr Orthop 2008; 22: 9e16.
16 Chaudhry V, Cornblath DR, Mellits ED, et al. Inter and intra
examiner
reliability of nerve conduction measurements in normal subjects.
Ann
Neurol 1991; 30: 841e3.
17 Mallik A, I Weir A. Nerve conduction studies: essentials and
pitfalls in
practice. J Neurol Neurosurg Psychiatry 2005; 76(Suppl. II):
ii23e31.
18 Mills KR. The Basics of electromyography. J Neurol
Neurosurg
Psychiatry 2005; 76(Suppl. II): ii32e5.ORTHOPAEDICS AND TRAUMA
23:6 432Orthopaedic knowledge update: shoulder and elbow 2. J Am
Acad
Orthop Surg 2002: 394.
23 Nashold BS. Current status of the DREZ operations. J
Neurosurg
1984; 15: 942e4.
24 Taylor GI, Ham FJ. The free vascularized nerve graft: a
further
experimental and clinical application of microvascular
techniques.
Plast Reconstr Surg 1976; 57: 413e26.
25 Eberhard D, Millesi H. Split nerve grafting. J Reconstr
Microsurg 1994;
12: 71e6.
26 Viterbo F, Trindale JC, Hoshino K, Mazzoni A. Two
end-to-side
neurorhaphies and nerve graft with removal of the epineural
sheath:
experimental study in rats. Br J Plast Surg 1994; 47: 75e80.
27 Terzis JK, Vekris MD, Soucacos PN. Outcomes of brachial
plexus
reconstruction in 204 patients with devastating paralysis.
Plast
Reconstr Surg 1999; 104: 1221e40.
28 Jamieson A, Earnes RA. Reimplantation of avulsed brachial
plexus
roots: an experimental study on dogs. Int J Microsurg 1980;
2:
75e80.
29 Carlstedt T, Grane P, Hallin RG. Return of function after
spinal cord
implantation of avulsed spinal nerve roots. Lancet 1995;
346:
1323e5.
30 Carlstedt T, Anand P, Hallin R. Spinal nerve root repair and
reim-
plantation of avulsed ventral roots into the spinal cord after
brachial
plexus injury. J Neurosurg 2000; 2(Suppl): 237.
31 Fournier H, Mercier P, Menei P. Repair of avulsed ventral
nerve roots
by direct ventral intraspinal implantation after brachial plexus
injury.
Hand Clin 2005; 21: 109.
32 Rouholamin E, Wootton R, Jamieson AM. Arthrodesis of the
shoulder
following brachial plexus injury. Injury 1991; 22: 271e4.
33 Alnot JY. Brachial plexus palsies: palliative surgery. In:
J-Y and
Narnkas A, eds. Traumatic brachial plexus injuries.
Expansion
Scientifique Francaise: Paris 218e220.
34 Doi K, Sakai K, Fuchigami Y, Kawai S. Reconstruction of
irreparable
brachial plexus injuries with reinnervated free-muscle
transfer.
J Neurosurg 1996; 85: 174e7.
35 Doi K, Sakai K, Kuwata N, et al. Double-muscle technique
for
reconstruction of prehension after complete avulsion of
brachial
plexus. J Hand Surg Am 1995; 20: 408e14. 2009 Elsevier Ltd. All
rights reserved.
The anatomy, investigations and management of adult brachial
plexus injuriesIntroductionHistoryAssessmentAnatomy of the brachial
plexusClinical clues to the anatomical location of
pathologyClassification of peripheral nerve injuryPathophysiology
of nerve regenerationInvestigationsRadiologicalHistamine testBasic
electrophysiologyNerve conduction studies (NCS)Electromyography
(EMG)
Neurophysiological assessment of the brachial plexusManagement
of open injuriesManagement of closed injuriesNon-surgical
management
Surgical managementSurgical approach to the brachial
plexusSurgical optionsNeurolysisNerve graftingNerve transfer
(Neurotization)
Late reconstructionShoulder arthrodesisTendon transfers to the
shoulderTendon transfers to restore elbow flexionTendon transfers
to restore hand functionFree muscle transfers
OrthoticsAmputationSummaryReferences