Embed Size (px)
Citation preview

11/12/2012
1
1
AnaphylaxisScreening
and Protection Program
Development and Support
This webinar was developed by the American
Pharmacists Association and supported by an independent educational grant from
Mylan Specialty L. P.
Speakers and Disclosures
Philip Johnston, PharmDProfessor and Dean
Belmont University College of Pharmacy
Elisa Greene, PharmDAssistant Professor, Pharmacy PracticeBelmont University College of Pharmacy
The speakers and APhA’s education staff declares no conflicts of interest or financial interests in any product or service mentioned in this activity, including grants, employment, gifts, stockholdings, and honoraria. For complete staff disclosures, please see the Education and Accreditation Information section at www.pharmacist.com.

11/12/2012
2
Accreditation Information
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education (CPE). This activity, Anaphylaxis Screening and Protection is approved for 1.5 hours of CPE credit (0.15 CEUs). The ACPE Universal Activity Number assigned by the accredited provider is 0202-0000-12-255-L04-P for pharmacist and 0202-0000-12-255-L04-T for technicians.
To obtain CPE credit for this activity, participants will be requires to actively participate in the entire webinar and complete an online evaluation and assessment located at www.pharmacist/com/live-activities by November 27, 2012. Instructions and an attendance code will be provided at the completion of the webinar.
Target audience: Pharmacist and Technicians
ACPE Activity Type: Knowledge-based
Learning Level: 2
Initial Release Date: November 13, 2012
Recall the pathophysiology, clinical presentation, and treatment of anaphylaxis.
Identify factors that increase a person’s risk of experiencing anaphylaxis as well as factors that increase the severity of anaphylaxis.
Outline a comprehensive strategy for preventing and treating episodes of anaphylaxis in the community setting.
Explain the appropriate use of epinephrine auto-injectors and identify errors commonly made by patients.
Prepare an emergency action plan for an individual patient at risk of anaphylaxis and counsel the patient on implementing the plan.
Learning Objectives for Pharmacists
Define the term “anaphylaxis,” list common symptoms, and identify key elements of anaphylaxis treatment.
Name factors that increase a person’s risk of experiencing anaphylaxis as well as factors that increase the severity of anaphylaxis.
Describe the elements of a comprehensive strategy for preventing and treating episodes of anaphylaxis in the community setting.
Explain the appropriate use of epinephrine auto-injectors and identify errors commonly made by patients.
Summarize the usual components of an emergency action plan for an individual patient at risk of anaphylaxis.
Learning Objectives for Technicians

11/12/2012
3
Only 1 does of epinephrine should be used to reverse a severe allergic reaction or anaphylaxis event?
True
False
When should an epinephrine autoinjector be replaced?
a.If it was obtained more than 6 months ago.
b.If it will expire before the patient can return to the pharmacy for a replacement.
c.After it has expired.
d.It does not need to be replaced unless it has been used.
Side effects of epinephrine include:
a.Palpitations and difficulty breathing
b.Dizziness and lightheadedness
c.Leg weakness
d.Nausea

11/12/2012
4
Roy Petrey is a 32-year-old male with a history of allergic reactions
Through trial and error, he has eliminated multiple possible causes, such as dust, grass, and animal dander
The most recent incident included complete body rash, facial swelling, and bronchospasm
Introduction to Patient Case
Definition◦ “A severe and sometimes fatal allergic reaction that is
characterized by hives, itching, respiratory difficulty, and shock; this condition requires immediate medical attention”◦ “A severe, life-threatening, generalized or systemic
hypersensitivity reaction that is characterized by rapidly developing life-threatening airway and/or breathing and/or circulation problems usually associated with skin and mucosal changes”
Anaphylaxis Overview
Highly likely when any one of the following 3 criteria are fulfilled:
◦ 1. Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissue, or both (e.g., generalized hives, pruritus or flushing, swollen lips-tongue-uvula) AND AT LEAST ONE OF THE FOLLOWING A. Respiratory compromise
B. Reduced Blood Pressure or symptoms of end-organ dysfunction
Clinical Criteria for Diagnosis of Anaphylaxis

11/12/2012
5
◦2. Two or more of the following that occur rapidly after exposure to a likely allergen for that patient (minutes to several hours): A. Involvement of the skin-mucosal tissue
B. Respiratory compromise
C. Reduced BP or associated symptoms
D. Persistent gastrointestinal symptoms
Clinical Criteria for Diagnosis of Anaphylaxis
◦3. Reduced blood pressure after exposure to known allergen for that patient (minutes to several hours): A. Infants and children: low systolic blood pressure (age specific)
or >30% decrease in systolic blood pressure
B. Adults: systolic blood pressure of <90 mm Hg or >30% decrease from that person’s baseline
Clinical Criteria for Diagnosis of Anaphylaxis
Overall incidence◦ Estimates range widely◦ Up to 49.8 per 100,000 person years◦ Up to 10.5-70 per 100,000 person years in those <19
years
Compare to colorectal cancer◦ 52.7 per 100,000 person years (males)◦ 39.7 per 100,000 person years (females)
Anaphylaxis Incidence

11/12/2012
6
Admissions rate for anaphylactic shock◦ 3.8 cases per 100,000 hospital admissions
Emergency room visits◦ 71% of patients present to ED or urgent care ◦ Of these, only 11% required hospitalization
Inpatients◦ 1 in 3,000 inpatients in US has an anaphylactic reaction
Anaphylaxis Statistics
Ages ◦ Peak occurrence: 15-55 years◦ Mean age 29 years, highest rates in <20 years
Gender◦ 56% female
Epinephrine prescriptions ◦ More in men if <15 years◦ More in women if >15 years
Anaphylaxis Statistics
Season◦ Peak: July-Sept (stings)
Geographic region◦ More in North/East vs South/West
Deaths ◦ 1,443-1,503 deaths per year (0.002%)
Anaphylaxis Statistics

11/12/2012
7
Anaphylaxis: IgE mediated ◦ First exposure: sensitization◦ Subsequent exposure: release of inflammatory mediators
(e.g., histamine, cytokines)
Anaphylactoid: Non-IgE mediated ◦ May occur after first exposure
Pathophysiology
Note: Distinction not recommended because presentation and treatment are identical
Most commonly peanuts, milk, eggs, tree nuts, shellfish, soy, fish, wheat, sesame seed
Usually immediate although may be delayed or return
Common Triggers: Food
Antibiotics◦ Penicillin most common medication cause
NSAIDs or ASA◦ 2nd most common◦ May be med specific
Other medications◦ Radio contrast media◦ IV anesthetics◦ Opioid analgesics◦ Omalizumab All patients should have epinephrine Rx
Common Triggers: Medications

11/12/2012
8
Insect venom◦ Most commonly Hymenoptera order – honeybees,
bumblebees, sweat bees, yellow jackets, hornets, wasps, ants
Latex
Exercise
Idiopathic
Autoimmune
Other Common Triggers
Food 33.2%
Insect sting 18.5%
Medication 13.7%
Contrast 0.5%
Other known 9 %
Unknown 25.1%
Incidence
Typical ◦ Exposure to trigger May not be identified
◦ Rapid onset of symptoms◦ Resolves within minutes to hours Spontaneous or with medical attention
Less likely◦ Delayed onset◦ Prolonged duration◦ Biphasic reaction
Clinical Presentation
May vary between people
and between episodes!
May vary between people
and between episodes!

11/12/2012
9
Most frequently encountered signs/symptoms◦ Mucocutaneous 94%◦ Respiratory 88%◦ Gastrointestinal 22%◦ Cardiovascular 21%
Early signs/symptoms◦ Flushing◦ Urticaria
Clinical Presentation
Recurrence after remission of initial symptoms ◦ Maximum incidence 20%◦ Variable severity◦ Difficult to predict◦ May require second dose
Increased likelihood with:◦ Delay in epinephrine ◦ Inadequate epinephrine◦ Need for large amounts of epinephrine
Biphasic Reactions
Mucocutaneous Respiratory Cardiovascular Gastrointestinal Other
Pruritis Congestion Hypotension Nausea Weakness
Flushing Sneezing Vascular collapse Vomiting Dizziness
Angioedema Bronchospasm Shock Abdominal cramps
Urticaria Upper respiratory obstruction•Dyspnea•Stridor•Wheezing•Throat tightness•Aphonia
Arrest Diarrhea
Arrhythmias
Syncope or pre-syncope
Chest pain
Increased vascular permeability

11/12/2012
10
◦ Diffuse urticaria 51.2%◦ Local angioedema 48.8%◦ Dyspnea 48.8%◦ Pruritis 48.3%◦ Throat tightness/fullness 39.8%◦ Flushing 38.4%◦ Tachycardia 35.6%◦ Wheezing/bronchospasm 26.5%◦ Emesis 18.0%◦ Local urticaria 17.1%
Most Common Symptoms
Dyspnea/difficulty breathing 48.8%
Intra-oral angioedema 15.6%
Hypotension 12.3%
Oro/hypo-pharyngeal edema 10.9%
Arrhythmia 6.6%
Syncope 6.6%
Diffuse angioedema 6.2%
Cyanosis 5.2%
Laryngeal edema 4.3%
Shock 1.0%
Severe Symptoms
RP has determined that his most recent allergic reaction was actually anaphylaxis◦ Skin testing has revealed an allergy to beef protein
RP has been educating himself about trigger avoidance but is worried and fearful about future episodes of anaphylaxis
RP calls and asks if you can talk him through what might happen if he needs to be treated again
The Case of Mr. Petrey

11/12/2012
11
First line therapy◦ Epinephrine first and always!
Management of Acute Anaphylaxis
http://www.epipen.com/about-epipen [Accessed 08/31/2012]http://www.auvi-q.com/ [Accessed 09/13/12]
Second-line therapy◦ Antihistamines Symptomatic for urticaria, angioedema and pruritis May use H1 + H2
◦ Systemic corticosteroids May prevent protracted or biphasic reaction
Management of Acute Anaphylaxis
Sample Regimen:
Diphenhydramine 25-50 mg
Ranitidine 300 mg
Methylprednisolone 1-2 mg/kg
*or equivalents
Third-line therapy◦ Bronchodilators◦ Supportive measures Oxygen Fluid resuscitation Vasopressors Glucagon
Positioning ◦ Remain recumbent (unless vomiting/SOB prevents)◦ Legs elevated
It is not recommended to induce vomiting
Management of Acute Anaphylaxis

11/12/2012
12
Observe patient after initial event ◦ Recommended: 8 hours ◦ Longer if more severe◦ Caution in patients with reactive airway disease More fatalities
At discharge◦ Prescription: epinephrine auto-injector ◦ Education: avoidance if trigger known◦ Follow-up: notify PCP/refer to allergist
Management of Acute Anaphylaxis
That was awful—am I ever going to have to do it again?
You really want me to give myself a shot?
The Case of Mr. Petrey
Access◦ Epinephrine auto-injector is not available◦ Not prescribed◦ Not on their person◦ Not able to use epinephrine auto-injector◦ Regulatory restrictions (schools, day care. etc.)
Fear◦ Needle◦ Adverse effects
Denial◦ Recognition of reaction◦ Severity of reaction
Behavioral Barriers

11/12/2012
13
“I had plenty of auto-injectors available, but that time the symptoms were different…it wasn’t until we got into the car (that) I suddenly thought, ‘no, this is the same thing.’”
“I thought I was having an asthma attack; I thought if I had anaphylactic shock I would be throwing up, because that’s what I did when I was little.”
“I didn’t realize that I could use it if I was just going into the reaction. You don’t know if you should take it now or wait until it develops and see how it goes. Are you bad enough to use it, that’s the big issue…”
Behavioral Barriers
Self-education◦ Food labels “May contain”
◦ Eating out◦ Travel
Vigilance
Parental role◦ Educating child on trigger avoidance◦ Reinforcement ◦ Gradual hand over of responsibility/management to
adolescent
Overcoming Barriers
Psychosocial Impact
“I think if you have experienced an anaphylactic shock and you know what it’s like. Very, very frightening…the second time he had an anaphylactic reaction he hardly ate for 6 months.”
—Parent of child with anaphylaxis

11/12/2012
14
“Quite a lot of my friends go and kiss boys and things and it’s kind of awkward for me because I’ll have to kind of ask have you eaten nuts. And you can’t really do that in a club…”
Psychosocial Impact
After discussing treatment of acute anaphylaxis, RP feels reassured and is confident he can overcome any of the barriers he is facing
He asks if he is at high risk for experiencing a future episode—if so, is there anything he can do to prevent it?
The Case of Mr. Petrey
Previous episode: greatest predictor of future event ◦ Within 10 years:◦ Median 395 days◦ Range 7 days to 13 years later
Atopic history: present in 54%-60% of patients◦ i.e. Asthma, allergic rhinitis, atopic dermatitis, hives ◦ More likely if food-induced or idiopathic
Identifying Patients at Risk

11/12/2012
15
Patient age
Concomitant disease states◦ Asthma◦ Allergies to anaphylaxis-causing substances◦ Heart Disease
Medications◦ Beta blockers, alpha blockers (block epinephrine activity)◦ ACE inhibitors, ARBs (may interfere with endogenous
compensatory responses)
Identifying Patients with Increased Severity
Identify and avoid patient-specific triggers
Manage relevant comorbidities
Assess benefits, risks of concurrent meds
Assess need for prophylactic therapy◦ Trigger not identified or not avoidable◦ Consider: H1 and/or H2 antagonist Leukotriene modifier Corticosteroids
Consider immunomodulation ◦ Venom-induced anaphylaxis
Preventing Anaphylaxis
ACE inhibitors
ARBs
Beta blockers
Alpha blockers
Cocaine
Amphetamines
Tricyclic antidepressants
Monoamine oxidase inhibitors
Epinephrine Drug Interactions

11/12/2012
16
Has RP eliminated all possible allergens to protect himself from future episodes of anaphylaxis?
What education does RP require to be prepared for the future?◦ Hint: He has never used an epinephrine auto-injector
What are the elements of a complete emergency plan?
The Case of Mr. Petrey
Also known as adrenaline
Mechanism of action◦ Alpha and beta adrenergic agonist
Therapeutic effects ◦ Vasoconstriction◦ Bronchodilation◦ Decreased mucosal edema◦ Decreased release of mast calls, basophils, tryptase,
histamine◦ Increased myocardial output and contractility
Autoinjectable Epinephrine
Adverse effects◦ Anxiety◦ Tremor◦ Headache◦ Difficulty breathing◦ Palpitations (could be drug or disease)
Contraindications◦ None!
Autoinjectable Epinephrine

11/12/2012
17
Delivery systems◦ EpiPen◦ Auvi-Q◦ No longer marketed: Twinject, Adrenaclick
Available in 0.15 mg or 0.3 mg doses◦ Weight-based dosing: If 10-25 kg: give 0.15 mg If >25 kg: give 0.3 mg
Route of administration: intramuscular
Autoinjectable Epinephrine
Site of administration: anterior lateral thigh◦ Inject through clothing
May repeat every 5-15 minutes
If in doubt, administer!
13% required >2 doses
Autoinjectable Epinephrine
Both doses are available as auto-injections◦ EpiPen – Yes Auvi-Q – Yes
Needle left exposed after auto-injection◦ EpiPen – Yes Auvi-Q – No
Second dose can be saved and used later◦ EpiPen – Yes Auvi-Q - Yes
Trainer device is included◦ EpiPen – Yes Auvi-Q - Yes
Autoinjectable Epinephrine Comparison

11/12/2012
18
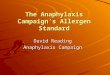
[NOTE
Autoinjector Administration Technique
1
2
3
4
Common adverse effects◦ Anxiety◦ Tremors◦ Pallor◦ Tachycardia
10 seconds may feel like eternity
Should feel improvement within 5-10 minutes
What to Expect After Administration
You receive a call from an EMT en route to the emergency room with RP, who appears to be having an acute cyanotic episode◦ The EMT has found the pharmacy telephone number on a
prescription for a metered dose inhaler in RP’s hand
The EMT asks you what other medications RP is getting and if you have a history that would help them manage RP
On questioning you find that they do not know of RP’s history of anaphylaxis!
The Case of Mr. Petrey

11/12/2012
19
The EMT determines that RP has already self administered an epinephrine auto-injector
Based on patient reaction and vital signs, the EMT administers an additional dose (0.3mg) of epinephrine en route to the nearest ED
RP is given supportive treatment and kept for observation, but makes a full recovery
The Case of Mr. Petrey
RP arrives in your pharmacy and asks for you by name
He shakes your hand and thanks you for “saving his life” during his recent ambulance ride
You assure him that you are happy to assist and that keeping all of his records in one pharmacy helped his chances of having a complete medication history available for the EMT
RP states that he will always keep his emergency action plan on his person, and needs to acquire an emergency ID bracelet
The Case of Mr. Petrey
Emergency action plan ◦ Information necessary for urgent care◦ Instructions for family, others
Emergency preparedness◦ Medical alert bracelet◦ Vigilance and education
Emergency Action Plan

11/12/2012
20
Practice Improvements◦ Keep all brands of epinephrine necessary for your
clientele◦ Keep emergency plan forms for patient education◦ Offer patients a method of purchasing a medical
emergency identification◦ Consider collaborative drug therapy management
agreement with allergist of primary care physician◦ Administer epinephrine and call 911 in patient presenting
with anaphylaxis
Tips for Pharmacists
Educate!◦ patients, parents, teachers, and others 46% of people contacted friend or family member first when
they had severe reactions Counsel on secondary treatments and preventive measures,
as necessary Teach proper use, storage and administration of epinephrine Review product insert/instructions with patients Avoid excessive heat or cold Remind about intramuscular injection Replace if submersed in water Inspect regularly for changes in color or clarity
Tips for Pharmacists
Alleviate patient fears◦ Provide necessary, patient specific information◦ Assure them this is a manageable situation◦ Address psychosocial barriers
Help resolve access barriers◦ Physician collaboration for initial prescription◦ Second prescription for keeping at school or work◦ Prescription renewal/expiration reminders
Tips for Pharmacists

11/12/2012
21
Provide support◦ Offer to help complete the patient emergency plan Suggest who should be informed and trained
◦ Give the patient your contact information for follow up information with a copy for his/her primary care provider◦ Call the patient if an incident has occurred recently◦ Keep specialist contact information available
Tips for Pharmacists
◦ Educate close contacts◦ Check expiration date on epinephrine◦ Know and avoid triggers◦ Recognize symptoms◦ Carry self-injectable epinephrine at all times◦ Use epinephrine early and correctly◦ Seek medical care after epinephrine use
Patient Steps for Successful Management
Only 1 does of epinephrine should be used to reverse a severe allergic reaction or anaphylaxis event?
True
False

11/12/2012
22
When should an epinephrine autoinjector be replaced?
a.If it was obtained more than 6 months ago.
b.If it will expire before the patient can return to the pharmacy for a replacement.
c.After it has expired.
d.It does not need to be replaced unless it has been used.
Side effects of epinephrine include:
a.Palpitations and difficulty breathing
b.Dizziness and lightheadedness
c.Leg weakness
d.Nausea
For more information: ◦ EpiPen: www.myepipen.com
◦ The American College of Allergy, Asthma, and Immunology: http://www.acaai.org/allergist/allergies/Anaphylaxis/Pages/anaphylaxis-patient-tip-sheet.aspx
◦ The Food Allergy and Anaphylaxis Network: http://www.foodallergy.org/section/education◦ http://www.foodallergy.org/section/support-groups
Additional Resources

11/12/2012
23
References Akeson N, Worth A. Sheikh A. The psychosocial impact of anaphylaxis on young people and their parents. Clin Exp
Allergy. 2007; 37:1213-20.
Bohlke K, Davis RL, DeStefano F, Marcy SM, Braun MM, Thompson RS, et al. Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization. J Allergy Clin Immunol. 2004;113:536-42.
Bothnar BS, Lichtenstein LM. Anaphylaxis. NEJM 1991; 324: 1785-90.
Camargo CA, Clark S, Kaplan MS, Lieberman P, Wood RA. Regional differences in EpiPen prescriptions in the United States: The potential role of Vitamin D. J Allergy Clin Immunol 2007;120:131-6.
Campbell RL, Luke A, Weaver AL, St. Sauver JL, Bergstralh EJ, et. al. Prescriptions for selfinjectable epinephrine and follow-up referral in emergency department patients presenting with anaphylaxis. Ann Allergy Asthma Immunol. 2008;101:631-6.
CDC Glossary, www2a.cdc.gov/nip/isd/ycts/mod1/scripts/glossary.asp?item=anaphylaxis accessed: August 29, 2012.
Choo K and Sheikh A. Action plans for the long-term management of anaphylaxis: systematic review of effectiveness. Clinical and Experimental Allergy. 37;1090-1094
Decker WW, Campbell RL, Manivanna V, Luke A, St Sauver JL, Weaver A, et. Al. The etiology and incidence of anaphylaxis in Rochester, Minnesota: A report from the Rochester Epidemiology Project. J Allergy Clin Immunol. 2008;122:1161-5.
Eigenmann PA, Dayer Pastore F, Zamora SA. An Internet-based survey of anaphylactic reactions to foods. Allergy 2001; 56:540-3.
Gallagher M, Worth A, Cunningham-Burley S, Sheikh A. Epinephrine auto-injector use in adolescents at risk of anaphylaxis: a qualitative study in Scotland, UK. Clin Exp Allergy 2011; (41): 869-77.
Gupta R, Sheikh A, Strachan DP, and Anderson HR. Time trends in allergic disorders in the UK.Thorax 2007; 62: 91-6.
Gupta R, Sheikh A, Strachan DP, and Anderson HR. Burden of allergic disease in the UK: secondary analyses of national databases. Clin Exp Allergy 2004;34:520-6.
Johann-Liang R, Josephs S, and Dreskin SC. Analysis of anaphylaxis cases after vaccination: 10-year review from the national vaccine injury compensation program. Ann Allergy Asthma Immunol. 2011.
Johannes CB, Ziyadeh N, Seeger, Tucker E, Reiter, and Faich G. Incidence of Allergic Reactions Associated with Antibacterial Usei in a Large, Managed Care Organisation. Drug Safety. 2007; 30 (8): 705-13.
Kelso JM. A second dose of epinephrine for anaphylaxis: How often needed and how to carry. J Allergy Clin Immunol. ;17(2): 464-5.
Kemp SF, Lockey RF, Simos FER. Epinephrine: the drug of choice for anaphylaxis. A statement of the World Allergy Organization. Allergy; 2008: 63;1061-70.
Lieberman P. Biphasic anaphylactic reactions. Ann Allergy Asthma Immunol. 2005; 95:217-26.
Lieberman P, Decker W, Camargo CA, O’Connor R, Oppenheimer J, Simons FE. SAFE: a multidisciplinary approach to anaphylaxis education in the emergency department. Ann Allergy Asthma Immunol. 2007;98:519-23.
Lieberman P, Nicklas RA, Oppenheimer J, Kemp SF, Lang D. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol 2010; 126:477-80.
Manivannan V, Campbell RL, Bellolio MR, Stead LG, Li JTC, Decker WW. Factors associated with repeated use of epinephrine for the treatment of anaphylaxis. Ann Allergy Asthma Immunol. 2009;103:395-400.
Muelleman RL, Tran TP. Chapter 113: Allergy, hypersensitivity, and anaphylaxis. In: Rosen’s emergency medicine: concepts and clinical practice. 5th ed. St Lousi (MO): Mosby, INC., 2002.
Neugut AI, Ghatak AT, Miller RL. Anaphylaxis in the United States: An Investigation Into Its Epidemiology. Arch Intern Med. 2001; 161:15-21.
References
Pumphrey R. Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol 2004;4:285-
90. Resuscitation Council (2008) Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers.
Available at: www.resus.org.uk/pages/reaction.pdf. Accessed: August 24,2012.
Sampson HA, Munoz-Furlong A, Campbell RL, Adkinson NF, Bock SA, Branum A, et. al. Second symposium on the definition and management of anaphylaxis: Summary report - Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117:391-7.
Sheikh A and Alves B. Age, sex, geographical and socio-economic variations in admissions for anaphylaxis: analysis of four years of English hospital data. Clinical and Experimental Allergy. 2001; 31: 157106.
Sheikh A, Shehata YA, Brown SGA, Simons FER. Adrenaline (epinephrine) for the treatment of anaphylaxis with and without shock (Review). The Cochrane Library 2012; 4: 1-16.
Simons FER, Peterson S, Black CD. Epinephrine dispensing patterns for an out of hospital population: A novel approach to studying the epidemiology of anaphylaxis. J Allergy Clin Immunol 2002;110:647-51.
Stumpf JL, Shehab N, Patel AC. Safety of Angeiotensin-Converting EnzymeInhibitors in Patients with Insect Venom Allergies. Ann Pharmacother 2006;40:699-703.
Walker S, Sheikh A. Managing anaphylaxis: effective emergency and long-term care are necessary. Clin Exp Allergy 2003; 33:1015-18.
References

11/12/2012
24
Go to www.pharmacist/com/live-activities and under the Live Activities list, select the Claim Credit link for: Anaphylaxis Screening and Protection
You will need to enter your pharmacist.com username and password.
Select “Add to Cart” or “Enroll Now” from the left navigation and successfully complete the Assessment (use Attendance Code provided during the webinar), Learning Evaluation and Activity Evaluation/ You will need to provide your NABP e-profile ID number to access your Statement of Credit.
Please visit www.pharmacist.com/cpe-monitor for any questions regarding your NABP e-profile ID number. Note that it may take up to 3 hours for your NABP e-profile ID number to become activated.
The filing deadline for this CPE activity is Tuesday, November 27, 2012. No credit will be issued after this date.
If you have any questions or require additional information to claim your credit, please contact Marcia Tomaselli, Senior Manager, Education Department at the American Pharmacists Association by calling 202-429-4125 or e-mailing [email protected].
How to Obtain Your CPE Credit