Embed Size (px)
Citation preview

1
2
3
4
5 Q1
67
89
1 1
12131415
1617 Q2181920212223
2 4
49
50
51
52
53
54
55
56
57
58
European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
Contents lists available at SciVerse ScienceDirect
European Journal of Pharmaceutics and Biopharmaceutics
journal homepage: www.elsevier .com/locate /e jpb
Research paper
Analysis of the enhanced oral bioavailability of fenofibrate lipid formulationsin fasted humans using an in vitro–in silico–in vivo approach
Yang Fei a, Edmund S. Kostewicz a, Ming-Thau Sheu b, Jennifer B. Dressman a,⇑a Institute of Pharmaceutical Technology, Goethe University, Frankfurt am Main, Germanyb School of Pharmacy, College of Pharmacy, Taipei Medical University, Taipei, Taiwan
a r t i c l e i n f o a b s t r a c t
252627282930313233343536
Article history:Received 6 November 2012Accepted in revised form 2 March 2013Available online xxxx
Keywords:FenofibrateLipid-based formulationBiorelevant dissolution testsPermeabilityOral absorptionComputational simulation
3738394041424344454647
0939-6411/$ - see front matter � 2013 Published byhttp://dx.doi.org/10.1016/j.ejpb.2013.03.001
⇑ Corresponding author. Institute of Pharmaceuticasity, Max-von-Laue-Str. 9, 60438 Frankfurt am Main29680; fax: +49 69 798 29724.
E-mail addresses: [email protected] (Y. Fei),de (E.S. Kostewicz), [email protected] (M.-T. Shfurt.de (J.B. Dressman).
Please cite this article in press as: Y. Fei et al.,in vitro–in silico–in vivo approach, Eur. J. Pharm
Lipid-based formulations have established a significant role in the formulation of poorly soluble drugs fororal administration. In order to better understand their potential advantages over solid oral dosage forms,we studied the solubility and dissolution/precipitation characteristics of three self-microemulsifyingdrug delivery system (SMEDDS) formulations and one suspension of micronized fenofibrate in lipidexcipients, for which pharmacokinetic studies had already been reported in the open literature. Thein vitro dispersion/dissolution studies were carried out in biorelevant media using USP II apparatus. Thesewere followed up by in silico simulations using STELLA� software, in which not only dispersion/dissolu-tion, but also the precipitation and re-dissolution of fenofibrate was taken into account. While unformu-lated drug exhibited poor solubility (0.22 lg/mL in FaSSGF and 4.31 lg/mL in FaSSIF-V2(PO4)) anddissolved less than 2% in dissolution tests, the solubility of fenofibrate in the presence of the lipid excip-ients increased dramatically (e.g., to 65.44 lg/mL in the presence of the Myritol 318/TPGS/Tween 80SMEDDS) and there was an attendant increase in the dissolution (over 80% from capsules containingthe Myritol 318/TPGS/Tween 80 SMEDDS and about 20% from the dispersion of fenofibrate in lipid excip-ients). For the four lipid-based fenofibrate formulations studied, combining in vitro data in biorelevantmedia with in silico simulation resulted in accurate prediction of the in vivo human plasma profiles.The point estimates of Cmax and AUC ratio calculated from the in silico and in vivo plasma profiles fellwithin the 0.8–1.25 range for the SMEDDS solution and capsule formulations, suggesting an accurate sim-ulation of the in vivo profiles. This similarity was confirmed by calculation of the respective f2 factors.Sensitivity analysis of the simulation profiles revealed that the SMEDDS formulations had virtuallyremoved any dependency of absorption on the dissolution rate in the small intestine, whereas for the dis-persion in lipid excipients, this barrier remained. Such results pave the way to optimizing the perfor-mance of oral lipid-based formulations via an in vitro–in silico–in vivo approach.
� 2013 Published by Elsevier B.V.
48
59
60
61
62
63
64
65
66
67
68
1. Introduction
Many new compounds in drug development have poor aqueoussolubility and slow dissolution rate characteristics, which oftenlimit their oral bioavailability [1]. Common solid formulationapproaches to overcome these difficulties include, for example, saltformation, reduction in drug particle size by micronizing or nano-sizing technology, morphology modification, and complex forma-tion with cyclodextrins. However, lipid formulation techniquesmay be sometimes more appropriate, especially when the com-
69
70
71
72
73
74
75
Elsevier B.V.
l Technology, Goethe Univer-, Germany. Tel.: +49 69 798
[email protected]), [email protected]
Analysis of the enhanced oral b. Biopharm. (2013), http://dx.d
pound shows extremely high lipophilicity as well as a pronouncedfood effect. Several types of lipid-based drug delivery systems suchas emulsions, suspensions, oil solutions, or self-microemulsifyingdrug delivery systems (SMEDDSs) are available [2]. Lipid formula-tion is able to overcome the food effect for certain drugs, and thereare numerous examples where lipid formulations have signifi-cantly enhanced the absorption of poorly soluble drugs underfasting conditions [3].
The ‘‘lipid formulation classification system’’ was first describedby Pouton in 2000 [4]. Since then, many studies regarding develop-ment of lipid-based formulations, including some with fenofibrate[5–7], have been published. Such studies have mainly focused onoptimization of the formulation by varying the composition andproportion of various excipients with the help of phase diagramsand using dispersion tests for their assessment [5–9]. Up tillnow, however, few if any attempts have been made to simulatethe plasma concentration of the drug based on in vitro data.
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
2 Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
In the cases where in vivo pharmacokinetics are available, PBPKmodeling has been successfully applied to simulate the plasmaprofile for solid dosage formulations of various drugs or drug can-didates, such as tablets of cimetidine, fenofibrate, ‘‘Compound A’’ (ab3-adrenergic receptor agonist in development), nelfinavir, and dil-tiazem [10–15].
Recently, Sheu et al. [16,17] examined the behavior of various li-pid-based formulations of fenofibrate, a widely used cholesterollowering agent, in healthy human volunteers. One formulationwas a SMEDDS (Type IIIA-MC, medium-chain lipids) administeredas an oral solution on one occasion and as a capsule formulationon another occasion. A second SMEDDS formulation, with Tween20 substituting for Tween 80, was also administered as a capsule.The fourth formulation was a suspension of fenofibrate in a lipid-based excipient mix. In the current study, the solubility anddissolution characteristics of fenofibrate for these oral lipid-basedformulations were examined in biorelevant media simulating thefasting stomach and intestine. Then, the absorption behavior ofthese lipid-based formulations was simulated using the commercialsoftware program STELLA� by combining the in vitro dissolutionbehavior of the formulations with gastrointestinal parameters forthe fasted state and the essential post-absorptive PK parameters(which were obtained from the literature [18–20] and throughdeconvolution of the observed in vivo data). The goal of this workwas to examine the role of dispersion and dissolution of the lipid-based formulations in the absorption of fenofibrate and thus helpto identify the key determinants of absorption from lipid formula-tions containing this drug. This in turn should point the way to beststrategies for optimizing lipid-based formulations which consistmostly of surfactant excipients.
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
2. Materials and methods
2.1. Chemicals and materials
Fenofibrate drug substance (lot BCBB4253), TPGS (D-a-tocophe-ryl polyethylene glycol 1000 succinate, lot BCBG6651V), and Tween80 (polysorbates, lot MKBD3974) were purchased from Sigma–Al-drich Chemie GmbH, Steinheim, Germany. Myritol 318 (C8/C10 tri-glycerides, lot CE71900007) was purchased from Cognis GmbH,Düsseldorf, Germany. Tween 20 (polysorbates, lot 0000340418)was purchased from Wilton Site Redcar, Cleveland, UK. Egg phos-phatidylcholine (Lipoid E PC�, 99.1% pure, lot 108015-1/42) waskindly donated by Lipoid GmbH, Ludwigshafen, Germany. Sodiumtaurocholate (NaTC, >97% pure, lot 2011040152) was purchasedfrom Prodotti Chimici Alimentari SpA, Basaluzzo, Italy. Pepsin (Ph.Eur., 0.51 U/mg, lot 1241256), 37% hydrochloric acid (conc. HCl),and 85% orthophosphoric acid (H3PO4) were obtained from FlukaChemie AG, Buchs, Switzerland. Sodium hydroxide solution (0.1 NNaOH) and hydrochloric acid solution (0.1 N HCl) were purchasedfrom VWR International GmbH, Darmstadt, Germany. Acetonitrile,dichloromethane, sodium chloride, sodium dihydrogen phosphatemonohydrate, and sodium hydroxide pellets were all of analyticalgrade and purchased from Merck KGaA, Darmstadt, Germany.Whatman� PTFE filters with 0.45 lm pore size were purchased fromWhatman GmbH, Dassel, Germany.
189
190
191
192
193
194
195
196
197
2.2. Preparation of fenofibrate lipid formulations
The composition of the different fenofibrate lipid formulations (3SMEDDSs and 1 micronized dispersion system (MDS)) used for dis-solution and solubility tests have been described previously [16] andare summarized in Table 1. The SMEDDSs (E5(80) and E5(20) formu-lations) comprised of 25% medium-chain triglyceride oil (Myritol318), 60% surfactant mixture consisting of TPGS (D-a-tocopheryl
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
polyethylene glycol 1000 succinate) and polysorbates (Tween 80or Tween 20) at ratios of 1:4, and 5% MilliQ-water. To prepare thedifferent formulations, each of the excipients was directly weighedinto a glass flask and heated to 80 �C under stirring for approxi-mately 10 min to obtain a homogeneous melt. Ten percentage offenofibrate was then dissolved in the melt. Once fully dissolved,the SMEDDS was allowed to cool down to ambient temperature,and 500 mg aliquots were then manually transferred to size 1 trans-parent hard gelatin capsules. The MDS formulation comprised 20%fenofibrate, which had been pre-sieved through a 40 lm analyticalsieve (likely resulting in a similar, but slightly different particle sizedistribution than what was administered in the in vivo study, inwhich a particle size ‘‘smaller than 37 lm’’ was used), dispersed ina mixture of 27.5% Myritol 318, 9.5% TPGS, 38% Tween 20, and 5%MilliQ-water. Owing to the high percentage of API in the MDS for-mulation, fenofibrate was mostly suspended in this formulation.To keep the dose strength the same as the SMEDDSs (equivalent to50 mg in each capsule), 250 mg of the MDS suspension was manu-ally transferred to size 3 transparent hard gelatin capsules. As thedose of fenofibrate in the formulation administered to humanswas 54 mg (Section 2.7), the slight dose difference between thein vitro and in vivo tests was taken into account when performingthe simulations.
2.3. Media preparation
To simulate preprandial conditions in the stomach, Fasted StateSimulated Gastric Fluid was prepared as previously described[21–23], but with the pH adjusted to 2 (FaSSGF pH 2). To simulateconditions in the preprandial intestine, a modified version ofFasted State Simulated Intestinal Fluid containing phosphate bufferand 0.5 mM Lecithin (FaSSIF-V2(PO4)) was used. These media werechosen to be consistent with the transfer model experiments [24]that had been planned to investigate precipitation from the formu-lations. However, as precipitation was shown not to occur in thetransfer model for the formulations studied, these results are notfurther discussed in this work. Table 2 summarizes the composi-tions of the simulated gastric and intestinal media used in thisstudy.
2.4. Solubility of fenofibrate in biorelevant dissolution media in thepresence of formulation excipients
The change in solubility of fenofibrate due to the presence of thelipid-based excipients was examined in FaSSGF pH 2 and FaSSIF-V2(PO4) using the shake-flask method (n = 3). To replicate the ratioof volume of excipients to volume of medium used in the dissolu-tion studies (in which 50 mg of API in 0.5 mL of lipid vehicle wasintroduced as a solution in a capsule or as a dispersion in a capsuleto 250 mL of FaSSGF pH 2 or to 500 mL of FaSSIF-V2(PO4)), thevolumes for the solubility study were scaled down proportionally.Using a pipette, 10 lL of each freshly prepared fenofibrate lipid for-mulation (according to Section 2.2) was added to a vial containingeither 5 mL pre-warmed FaSSGF pH 2 or 10 mL pre-warmed FaS-SIF-V2(PO4). The sample vials were closed using screw caps andvortexed for 5 s to ensure a fine dispersion. Subsequently, the sam-ples were gently shaken on an orbital shaker which was incubatedin a 37 �C oven for 24 h. Thereafter, the dispersions were filtered(0.45 lm PTFE membrane filters, Whatman, Germany), and theconcentration of fenofibrate in the resulting filtrate was analyzedby HPLC (Section 2.6). The concentration of dissolved fenofibrateafter 24 h was less than the concentration initially generated byadding the formulation to the medium, indicating that the solubil-ity of fenofibrate is exceeded in the experiment. As a check, theexperiment was repeated on a larger scale, and after 24 h, a furtheramount of fenofibrate powder was added to the medium. There
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
Table 1Composition of the fenofibrate lipid formulationsa.
Dose 50 mg E5(80) solution E5(80) capsule E5(20) capsule MDS capsule
Fenofibrate (%) 10 10 10 20 (micronized)b
Myritol 318 (%) 25 25 25 27.5TPGS (%) 12 12 12 9.5Tween 20 (%) / / 48 38Tween 80 (%) 48 48 / /H2O (%) 5 5 5 5
a This table was summarized from the literature [16].b The fenofibrate was pre-sieved through a 40 lm analytical sieve.
Table 2Composition of the gastric and intestinal media.
FaSSGF pH 2 FaSSIF-V2(PO4)
CompositionSodium taurocholate (mM) 0.08 3Lecithin (mM) 0.02 0.5Pepsin (mg mL�1) 0.1 –Sodium chloride (mM) 34.2 62.6Hydrochloric acid (mM) 12.6 –Monobasic sodium phosphate (mM) – 28.6Sodium hydroxide (mM) – 8.7
Characteristic parameterpH 2.0 6.5Osmolality (mOsm kg�1) 120 ± 2.5 180 ± 10Buffer capacity (mmol L�1 DpH�1) – 12
Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx 3
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
was no change in the concentration of dissolved fenofibrate afterthe further addition of fenofibrate, confirming that the equilibriumsolubility had been reached. As a control experiment, the solubilityof fenofibrate drug powder in the absence of the lipid excipientswas evaluated according to the same protocol in the two media.
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
2.5. Dissolution studies
The dissolution characteristics of each lipid formulation werealso examined in FaSSGF pH 2 and FaSSIF-V2(PO4). In gastric med-ia, the dissolution studies were performed using 250 mL of mediain a USP II mini-paddle apparatus, while in intestinal media, thestudies were performed in an USP II apparatus in 500 mL of media.The mini-paddle apparatus is based on a USP paddle setup butscaled down geometrically with respect to dimensions [25]. An Er-weka Dissolution-Tester DT 600 (Erweka, Heusenstamm, Ger-many) was used. The experiments were carried out at 37 �Cusing a paddle speed of 75 rpm. Introduction of lipid formulationinto the dissolution medium was as follows: the E5(80) solutionformulation (500 mg lipid blend) was placed into the dissolutionmedia under stirring using a 1000 lL pipette. For the capsule for-mulations, the required amount of the E5(80), E5(20), and MDS li-pid blends was filled into hard gelatine capsules and sealed 1 daybefore the dissolution tests (see details in Section 2.2). Before man-ual placement into the dissolution vessels, a helix wire sinker wasslipped over to the capsule shell to prevent floating of the capsule.Samples were periodically (5, 10, 15, 20, 30, 45, 60, 90, 120, 180,and 240 min) withdrawn from the gastric (2.5 mL) and intestinal(5 mL) media. After each sample withdrawal, the volume was re-placed with an equivalent volume of blank fresh dissolution mediapre-warmed to 37 �C. Once withdrawn, the samples were immedi-ately filtered (0.45 lm PTFE membrane). The first 1 mL from sam-ples of gastric media and the first 2 mL from samples of intestinalmedia were discarded, and the rest of the filtrate was collected into10 mL glass tubes and immediately diluted with 80% acetonitrileand subsequently assayed by HPLC (Section 2.6). All dissolutionswere carried out in triplicate. Dissolution profiles were generated,
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
and the initial dissolution rate of fenofibrate was calculated usingdata points from the first hour of the profiles (see Section 2.8.1).Where, it occurred, precipitation was also taken into consideration(see Section 2.8.2).
2.6. Quantitative analysis of fenofibrate by HPLC
The concentration of fenofibrate from samples of the solubilityand dissolution tests was measured by high performance liquidchromatography (HPLC). The HPLC system comprised of aLaChrom� L-7110 pump, a LaChrom� L-7200 autosampler, aLiChroCART� Purospher RP-18e 5 lm, 125 � 4 mm column (Merck,Darmstadt, Germany), a LaChrom� L-7400 UV–Vis-Detector (MerckHitachi, Darmstadt, Germany), and EZ-Chrom Elite™ Version 2.8Data System Software� (Biochrom Ltd., Cambridge, UK). The mobilephase consisted of 80% acetonitrile and 20% MilliQ-water (v/v, pH ofthe mobile phase mixture was adjusted to 2.5 by orthophosphoricacid). The UV detector wavelength was set at 254 nm, the injectionvolume was 20 lL, and the flow rate maintained at 0.85 mL/min. Allanalysis was performed under ambient temperature. Using theseoperating conditions, fenofibrate typically eluted at 4.5 min.
2.7. In vivo evaluation of lipid formulations
The plasma concentration profiles of fenofibric acid after oraladministration of 54 mg fenofibrate lipid formulations (1 oral solu-tion, 2 SMEDDS capsules and 1 MDS capsule) were obtained fromthe literature [16]. Briefly, twelve healthy male Taiwanese volun-teers aged between 24 and 29 years participated in the clinicalstudy after signing an informed consent agreement of ethics. A par-tial crossover design was used, where each formulation wasadministered to a group of four subjects. After an overnight fastof at least 10 h, each subject was administered either the respec-tive capsule formulation together with 240 mL of water, or the oralsolution formulation of 0.5 mL lipid vehicle, which was pre-dis-solved in 240 mL of water. After administration of the dosageforms, subjects remained fasted for 4 h. For the hour prior toadministration and 2 h after, no water was permitted. Thereafter,subjects were given free access to water. Lunch and dinner wasserved by Taipei Medical University Hospital at 4 and 10 h afterdose administration, respectively.
The post-absorptive PK parameters of fenofibric acid were cal-culated from the in vivo plasma concentration profiles, using Win-Nonlin� Professional Edition 5.2.1 software (Pharsight Corporation,Mountain View, CA, USA). Since there are no published intravenousPK data for fenofibrate, the post-absorptive disposition parametersneeded for the simulations were calculated according to plasmaconcentration data for the oral solution. The plasma concentrationswere fitted to a two-compartment model using WinNonlin� 5.2.1,with first order micro rate constants and no lag time (model 11).The resulting constants obtained for the oral solution which in-cluded k10 (elimination rate constant), k12 (rate constant from cen-tral to periphery compartment), and k21 (rate constant from
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302303
305305
306
308308
309
311311
312
314314
315
317317
318
320320
321
323323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
4 Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
periphery to central compartment) were then used to simulate theplasma profiles for all the fenofibrate lipid formulations in thefasted state. The V/F value (volume of distribution corrected forthe fraction absorbed) from the oral solution was also calculated.
2.8. Model setup and PBPK simulation of fenofibric acid plasma profiles
Using STELLA� 9.1.3 (Cognitus Ltd., North Yorkshire, UK), thefenofibric acid plasma concentration versus time profiles weresimulated by incorporating the experimental solubility and disso-lution results for the different lipid formulations. Although fenofi-brate was used in the in vitro dissolution and solubility tests,fenofibric acid was used in describing all the plasma concentrationprofiles both in vivo and in silico, since in vivo fenofibrate is rapidlyand completely hydrolyzed within the gut wall, liver and by plas-ma esterase to its active metabolite fenofibric acid [5,26]. Fig. 1shows the model map for the STELLA�-based simulations.
Eqs. )((1)–(7) describe drug flux within each compartment ofthe STELLA� model (Fig. 1). Eqs. (1) and (2) represent conditionsof the gastric lumen; Eqs. (3) and (4) represent conditions of theintestinal lumen; Eq. (5) represents the pathway for the coadmin-istered water volume; and Eqs. (6) and (7) represent the plasmaand periphery tissue compartments, respectively.
dXDOðtÞdt
¼ �JDSðtÞ � kGEXDOðtÞ ð1Þ
dXDSðtÞdt
¼ JDSðtÞ � kGEXDSðtÞ ð2Þ
338339
340
341
342
343344
346346
347
348
349
350
351
352
353
354
Fig. 1. Stella� model map used to simulate the plasma profiles of the fenofibratelipid-based formulations (shown without precipitation and re-dissolution ele-ments). stom, stomach; si, small intestine; vfluid, volume of coadministered fluid;vfge, time factor of gastric emptying of the fluid volume; I lumen, intestinal lumen;plasma con, plasma concentration; vcf, volume of distribution including factor forbioavailability. (For interpretation of the references to color in this figure legend,the reader is referred to the web version of this article.)
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
dXFIðtÞdt
¼ kGEXDOðtÞ � JDIðtÞ ð3Þ
dXILðtÞdt
¼ JDIðtÞ þ kGEXDSðtÞ � kaXILðtÞ ð4Þ
dVFðtÞdt
¼ �kGEVFðtÞ ð5Þ
dXPLðtÞdt
¼ kaXILðtÞ þ k21XPEðtÞ � ðk12 þ k10ÞXPLðtÞ ð6Þ
dXPEðtÞdt
¼ k12XPLðtÞ � k21XPEðtÞ ð7Þ
In the above equations, XDO(t) describes the time evolution for theorally administered formulated drug dose in the stomach, mg; XDS(-t) describes the time evolution for the dissolved drug mass in thestomach, mg; XFI(t) describes the time evolution for the formulateddrug mass in the small intestine, mg; XIL(t) describes the time evo-lution for the dissolved drug mass in the intestinal lumen, mg; XPL(t)describes the time evolution for the absorbed drug mass in the plas-ma, mg; XPE(t) describes the time evolution for the absorbed drugmass in the periphery tissue, mg; JDS(t) represents the dissolutionrate for the formulated drug content in the stomach, mg h�1; JDI(t)represents the dissolution rate for the formulated drug content inthe small intestine, mg h�1; kGE is a first order kinetic rate constantfor gastric emptying, h�1; ka is the absorption rate constant fromthe small intestinal lumen to plasma compartment, h�1; and VF(t)describes the time evolution for the coadministered water volumein the stomach, mL.
2.8.1. Calculation of the dissolution parametersTo describe the dissolution behavior of the different lipid for-
mulations in the PBPK model, the Noyes–Whitney theory was uti-lized, as shown in the following equation [18]:
dWt
dt¼ z
VW2=3ðXs �WtÞ ¼ zW2=3ðCs � CtÞ ð8Þ
In this case, the amount of drug (Wt) dissolved at time t is describedby the following parameters: z value, an apparent parameter fordescribing the initial drug dissolution rate from the lipid formula-tion which can be calculated using the in vitro dissolution data,mL mg�2/3 h�1; V, the dissolution medium volume, mL; W, the massof drug remaining to be dissolved, mg; Xs, the amount of drug thatsaturates the dissolution medium, mg; Cs, the drug solubility in thedissolution medium, mg mL�1 and Ct, the concentration of dissolved
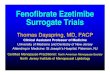
Fig. 2. Solubility data (n = 3) of fenofibrate in diluted lipid-based formulations(E5(80), E5(20), and MDS) and the unformulated drug substance in FaSSGF pH 2 andFaSSIF-V2(PO4). (For interpretation of the references to color in this figure legend,the reader is referred to the web version of this article.)
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393394
396396
397
398
399
400
401
402
403
404
405
406
Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx 5
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
drug at time t (h), mg mL�1. Similar to a previously describedapproach [11], the assumptions in this model include: (i) there isno absorption of drug from the stomach; (ii) gastric emptying intothe small intestine of the dispersed drug formulation and coadmin-istered water can occur simultaneously; (iii) the average first ordergastric emptying rate constant (kGE) is 2.8 h�1 [18,23]; (iv) limita-tions to the drug permeation processes can be simulated by incor-porating a compartment to reflect the unstirred water layer and/or penetration into the mucosa. Further assumptions, specific to thiscase, were that (v) all absorbed fenofibrate is completely convertedand appears in blood as fenofibric acid [11,27] and (vi) the volumeof coadministered water is 240 mL [16]. Sensitivity analyses of theSTELLA� model generated were carried out by varying various phys-iological or measured parameters (zstomach, zintestine, Cs,stomach, Cs,intestine,ka, and kGE) from one-fifth to five times of the nominal referencevalue, to examine their impact on the simulated plasma profiles.
407
408
409
410
411
412
413414
416416
417
418
419
420
421
422
423
424
425
426427
429429
2.8.2. Calculation of precipitation parametersIt has been hypothesized that lipid formulations that consist
mainly of surfactants may lose their solvent capacity when dilutedby GI-fluids and exposed to physical agitation in GI-tract, leadingthe metastable phase system to undergo phase separation andcause precipitation of the API [7]. For the lipid formulations in thisstudy, the solubilization capacity of fenofibrate in gastric andintestinal media was significantly enhanced by the excipients,leading to a high degree of supersaturation in comparison withthe solubility of pure fenofibrate in the same media. FormulationsE5(80) solution and E5(80) capsule showed no tendency to precip-itate after dissolving. By contrast, for the E5(20) formulation, someprecipitation in the gastric and small intestinal media was detectedanalytically, so precipitation and re-dissolution were taken intoconsideration in the STELLA� model for this formulation. A zero or-der precipitation rate constant was calculated from the in vitro dis-solution curve using data points taken after 90 min for thisformulation (see Fig. 3). The rate of drug precipitation was calcu-lated using Eq. (9), where Pt is the amount of drug precipitated attime t (h), mg; and k0 is a zero order rate constant of the precipita-tion process, mg h�1. The re-dissolution rate of the precipitate was
Fig. 3. Dissolution profiles (n = 3) of four fenofibrate lipid formulations: E5(80) solution,pH 2 (A) and in 500 mL of FaSSIF-V2(PO4) (B). The horizontal lines depict the mean eformulations in each respective media. (For interpretation of the references to color in t
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
assumed to be the same as the initial dissolution rate of the puredrug substance in each of the media.
dPt
dt¼ �k0 ð9Þ
2.8.3. Fenofibrate permeability and intestinal absorptionAlthough fenofibrate is often assumed to be a BCS Class II drug,
it has been recently shown for nanosized formulations of fenofi-brate that membrane uptake may also partially play a limiting role[11]. This may also be the case for lipid formulations from whichdispersion/dissolution is rapid. Therefore, a permeability restric-tion was incorporated in the STELLA� model for the PK simulations.A Caco-2 permeability coefficient for fenofibrate was estimatedusing data obtained from the literature by in vitro permeabilitytests [28–30]. In these experiments, a U-shaped chamber dividedinto two parts by fixing the Caco-2 monolayer in between wasused. Following the addition of drug to the donor chamber understirring, samples were periodically taken from both chambers con-taining buffer solutions simulating conditions on both the apicaland basal sides of the intestinal membrane. For this setup, theapparent Caco-2 permeability (PCaco-2, cm s�1) was calculatedaccording to the following equation [31]:
PCaco-2 ¼dQdt� 1
A � C0ð10Þ
where dQ/dt is the permeation rate with the amount of drug repre-sented in fraction (%), s�1; C0 is the initial concentration in the do-nor chamber with the amount of drug represented in fraction (%),mL�1; and A is the surface area of the mono layer, cm2.
Since drug diffusion through the unstirred water layer (UWL)adjacent to the intestinal epithelial membrane might also limit theintestinal permeation of highly permeable drugs [32], we comparedthe permeation rate through the UWL (PUWL) and the permeationrate through Caco-2 cells (PCaco-2). Eq. (11) was used to calculatethe permeation coefficient through the UWL [32]:
ðPUWLÞMW ¼ 10� 10�4 � 180MW
� �1=3
ð11Þ
E5(80) capsule, E5(20) capsule and MDS capsule of 50 mg dose in 250 mL of FaSSGFquilibrium solubility (n = 3) of fenofibrate in the diluted E5(80), E5(20) and MDShis figure legend, the reader is referred to the web version of this article.)
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

430
431
432
433
434
435
436
437
438
439
440441
443443
444
445446
448448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464465
467467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
6 Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
where (PUWL)MW is the UWL permeability calculated using themolecular weight (MW) of the drug, cm s�1. In Eq. (11), glucose isincluded as the reference compound as it is assumed that glucosepermeation across the human intestine is completely limited by dif-fusion through the UWL and is therefore often used for calculatingUWL permeability of various compounds. The values 10 � 10�4 and180 represent the human UWL permeability value (cm s�1) and themolecular weight of glucose, respectively [32].
The effective permeability coefficient (Peff, cm s�1) accounts forcontributions of both the Caco-2 cell permeability and the UWL, asgiven in Eq. (12):
1Peff¼ 1
PCaco�2þ 1
PUWLð12Þ
The flux of drug from the intestinal tract into the blood circulationwas calculated using Eq. (13):
dMt
dt¼ ka �Mt ¼ 3600 � Peff � S �
Mt
Vð13Þ
As shown by Eq. (13) [33], the amount of drug (Mt, mg) permeatedfrom the intestinal tract into the blood circulation at time t (h) wascalculated using the Peff value calculated from Eq. (12); the availableintestinal surface area for absorption (S), which was assumed to be800 cm2 [19]; and the intestinal fluid volume (V), which was as-sumed to be 105 ± 72 mL in the fasted state [20]. This equationwas then used to calculate the absorption rate constant, and the va-lue was compared with the one used in previous simulations offenofibrate plasma profiles [11].
2.9. Comparison of simulated and reported plasma concentrationprofiles
A model-independent approach using the similarity factor (f2)was applied for comparing the observed and simulated plasmaconcentration profiles obtained under fasting conditions. The fol-lowing equation was used to calculate the f2 value for the plasmacurves in this study:
f2 ¼ 50 log 1
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi0:0001þ 1
n
Xn
t¼1
ðRt � TtÞ2s," #
ð14Þ
where T is the relative fraction of in silico plasma drug concentrationcompared to the Cmax value at time t, R is the relative fraction of ob-served plasma drug concentration compared to the Cmax value attime t, and n is the number of sampling time points. The f2-valuecan range between 0 and 100, a value above 50 indicates that thedifference between the two plasma profiles is less than 10% andare therefore assumed to be similar to each other [34,35].
535
536
537
538
539
540
Table 3Summary of z values of fenofibrate lipid formulations in biorelevant media.
z/V-valuea (mg�2/3 h�1) FaSSGF pH 2 FaSSIF-V2(PO4)
E5(80) solution 9.4565 ± 4.2330 7.5276 ± 1.1784E5(80) capsule 0.5248 ± 0.1361 0.2595 ± 0.0815E5(20) capsule 0.2724 ± 0.0398 0.2036 ± 0.0463MDS capsule 0.3835 ± 0.0892 0.2453 ± 0.0330Pure drug 0.0741 ± 0.0114 0.0232 ± 0.0039
a Value corrected for in vivo dose (54 mg), and calculated from the in vitro dis-solution data (n = 3).
3. Results and discussion
3.1. Solubility of fenofibrate lipid formulations in biorelevant media
The measured solubility of fenofibrate in FaSSGF pH 2 and FaS-SIF-V2(PO4) from the lipid-based formulations is shown in Fig. 2.The influence of the lipid formulation components on solubilizationis illustrated by comparison with the solubility of unformulatedfenofibrate powder in the fasted state media (0.22 ± 0.01 lg/mL inFaSSGF [11] and 4.31 ± 0.23 lg/mL in FaSSIF-V2(PO4)). As can beseen from the figure, the solubility of fenofibrate in physiologicallyrelevant dilutions of the formulations is significantly greater thanthat of the pure drug in both media (horizontal dash lines, Fig. 2).Through lipid-based formulation, the solubility of fenofibrate hasbeen increased by about 15-fold in FaSSIF-V2(PO4) and up to 650-fold in FaSSGF pH 2.
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
As shown in Fig. 2, the measured solubility of fenofibrate in gas-tric media was as follows: 142.01 ± 10.65 lg/mL from the E5(80)formulation, for E5(20), it was 93.25 ± 3.33 lg/mL and for MDS46.01 ± 2.30 lg/mL. In intestinal media, the respective values wereas follows: E5(80) 65.44 ± 2.61 lg/mL, E5(20) 32.74 ± 1.50 lg/mLand MDS 17.22 ± 0.57 lg/mL. The rank order of solubility was thesame in both media: E5(80) > E5(20) > MDS. This trend can be ex-plained by the lipid formulation classification system [36] (i.e., theSMEDDS of E5(80) is expected to be more resistant to dilution andthus more likely to maintain the solubilization capacity of fenofi-brate than the E5(20) lipid formulation, since Tween 80(HLB = 15, [17]) which is used in E5(80) is more lipophilic thanTween 20 (HLB = 16.7, [17]) which is used in the E5(20) formula-tion). The data also show that the solubility of fenofibrate undergastric conditions is slightly higher than under intestinal condi-tions when applying the various formulations, despite the fact thatfenofibrate is a neutral compound. This trend is due to the differentratios of formulation versus medium applied for the solubility testsin FaSSGF pH 2 and FaSSIF-V2(PO4) (see Section 2.4). Since the dilu-tion of excipients by the medium in the solubility tests in FaSSIF-V2(PO4) is double that compared with FaSSGF pH 2, they will exertless influence on fenofibrate solubility.
3.2. Dissolution of fenofibrate lipid formulations and the pure drug inbiorelevant media
The dissolution experiments were carried out over 4 h, and thistime reflects the transit time through the small intestine [14,37].For comparison purposes, a sample from the gastric media was alsotaken at 4 h, even though the residence time would typically not bethis long in the fasted stomach. The dissolution profiles of the dif-ferent fenofibrate formulations and pure drug in the simulated gas-tric and intestinal media are shown in Fig. 3A and B. Forcomparison purpose, the solubility values (for fenofibrate in therespective formulation) are also shown in these profiles as horizon-tal lines.
As expected, in each of the media, the unformulated drug pow-der dissolved only very slowly, with only 0.07% released after60 min in FaSSGF pH 2 and 1.7% after 90 min in FaSSIF-V2(PO4).In contrast, the E5(80) solution showed very rapid dissolution inboth media, with the maximum dissolution of just over 80% occur-ring after approximately 10 min. This suggests that the E5(80) lipidformulation was able to sustain the dispersion and dissolution fol-lowing dilution in the media over 4 h. The E5(80) and E5(20) cap-sule formulations reached their maximum percent dissolution(60–80%) somewhat more slowly, after approximately 1 h. Thesedifferences between the oral solution and the capsule formulationsare also reflected by the significantly greater z value for the solu-tion compared to the lipid filled capsules (Table 3, Section 3.3.1).Although the MDS formulation showed a faster rate of dissolutionin the FaSSGF pH 2 media than in FaSSIF-V2(PO4), the maximumpercent released in both media was just under 20%. These valuescorrespond closely to the solubility of fenofibrate (from the MDSformulation) in the two media.
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
652
653
Table 4Summary of calculated mean values of human post-absorptive parameters offenofibric acid using individual in vivo plasma concentration profiles following oraladministration of the E5(80) solution in fasted state using WinNonlin� software.
Subject A B C D Meana ±SD
k12 (h�1) 0.705 0.512 0.392 0.312 0.480 ± 0.171k21 (h�1) 0.284 0.330 0.231 0.171 0.254 ± 0.069k10 (h�1) 0.078 0.223 0.093 0.103 0.124 ± 0.066V/F (mL) 4817.0 5516.7 6551.8 5978.4 5716.0 ± 733.8Cl/F (mL h�1) 377.9 1228.0 606.6 616.5 707.2 ± 364.3
a The arithmetic mean values of the four individuals (subject A, B, C and D) areincorporated to the STELLA� model to simulate the mean plasma profiles followingtreatment of various fenofibrate lipid formulations.
Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx 7
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
As expected from the solubilities, the percent dissolution wasmuch higher from the E5(20) and E5(80) capsule formulationscompared to unformulated fenofibrate. Both achieved a supersatu-ration in FaSSGF pH 2 as well as in FaSSIF-V2(PO4) even comparedto the fenofibrate solubility in the presence of the excipients. TheE5(20) capsules achieved concentrations almost doubling the solu-bility in the presence of excipients, but then began to precipitateafter approximately 90 min. For the E5(80) capsules, the supersat-uration was less extensive, but the concentrations were sustainedover the 4 h period.
It is clear from the results that the composition of the lipidexcipients, the ratio of drug to lipid excipients and the dosage formpresentation all influence the dissolution profile of fenofibrate.First, the E5(80) capsule, in which Tween 80 is used, and theE5(20) capsule, in which Tween 20 is incorporated, differ in theirability to create and maintain drug supersaturation in the simu-lated GI-fluids. Second, comparing the dissolution of MDS capsulewith E5(20) capsule, a drug load in excess of the fenofibrate solu-bility in these excipients leads to reduced drug release, and third, itis clear that the oral solution dissolves much faster than the cap-sule releases fenofibrate from the E5(80) formulation.
3.3. Simulation of fenofibric acid plasma profiles followingadministration of lipid formulations
3.3.1. z value estimationThe initial dissolution rates (z values) were calculated from the
initial data points (up to 60 min) of the in vitro dissolution curves,according to the Noyes–Whitney theory (see Eq. (8)), and the val-ues are summarized in Table 3.
As anticipated, the z value for the E5(80) solution was greaterthan for the capsule formulations, reflecting the faster initial disso-lution rate from this formulation. Similarly, the z values for the li-pid formulations are much greater than those calculated for thedrug powder.
3.3.2. Permeability estimationSince the simulated plasma profile of micronized fenofibrate
tablets had been successfully predicted without considering per-meability restriction [11], the rate limiting step for oral adminis-tration of the micronized solid dosage forms was assumed to bedissolution rather than uptake rate through intestinal mucosa.However, since fenofibrate dissolves much faster from lipid formu-lations than from tablets, the initial dissolution rate might be com-parable to its permeation rate in this case. As a result, we assumedfor the modeling that permeability restrictions should be ac-counted for when simulating plasma profiles for the fenofibrate li-pid formulations.
Using the in vitro Caco-2 data for fenofibrate from the literature[29,30] and Eq. (10), the human permeability coefficient of fenofi-brate was calculated to be 2.76 � 10�5 cm/s (PCaco-2). This of courseis only an approximation, since it is a mean value calculated fromthe in vitro data of different fenofibrate formulations (n = 5) fromUssing chamber experiments [29,30]. Those formulations wereimmediate release (IR) fenofibrate dosage forms based either uponsolid dispersion techniques using hydrophilic polymer (Melt-Dose�), or upon nanoparticulate tablet technology (Tricor�)[29,30]. As they were all IR dosage forms, we assume the maximumdissolved concentration in the donor chamber in vitro was veryquickly reached and maintained throughout the permeation testfor 120 min. Therefore, the C0 in Eq. (10) was approximated to beconstant, allowing integration of Eq. (10).
The calculated permeability coefficient of fenofibrate throughthe unstirred water layer (PUWL) using Eq. (11) was 7.93 �10�4 cm/s. The PUWL is thus approximately 30 times higher thanthe PCaco-2. This suggests that fenofibrate permeation through the
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
unstirred water layer of the gut wall is much faster than permeationthrough the enterocytes. Consequently, the permeation through theenterocytes should be the primary rate limiting step to uptake oncefenofibrate is in solution. In fact, we accounted for both steps usingEq. (12), resulting in an overall effective permeability (Peff) of2.66 � 10�5 cm/s.
Applying the calculated Peff ((2.66 ± 0.48) � 10�5 cm/s, n = 5), S(800 cm2 [19]), and V (105 ± 72 mL [20]) parameters in Eq. (13),we arrive at an absorption rate constant, ka, value of 0.730 h�1,which is a little lower than the overall ka we used for our simula-tions (1.00 h�1 [11]). As these values are also in good agreementwith the ka value (0.830 ± 0.241 h�1, n = 4) obtained using Win-Nonlin� software to deconvolute the in vivo plasma profiles, thiscalculation of the absorption rate constant from the effective per-meability data seems like a promising approach to bridge the gapbetween the in vitro and in vivo permeation behavior of drugs foruse in the in silico models.
3.3.3. Simulated plasma profiles of fenofibric acid using STELLA�
softwareTo predict the human plasma profile of fenofibric acid after
administration of the lipid formulations, in silico PBPK simulationusing STELLA� software was performed. For each of the formula-tions, the plasma concentration of fenofibric acid was simulatedusing the in vitro solubility and dissolution data as the inputparameters for the model. Simulated profiles were then comparedto those observed in vivo.
The post-absorptive parameters required for the STELLA� basedmodel were calculated using the plasma profiles following oraladministration of the E5(80) solution from four individuals (sub-ject A, B, C, and D) using WinNonlin� software. The parametersare listed in Table 4. As a commonly used approach suggested byCardot and Davit [38], the arithmetic mean values of respectiveindividual parameters were derived, and these data were incorpo-rated to STELLA� as input human PK parameters to simulate themean plasma profiles for the lipid formulations. This approxima-tion is based upon the assumption that the mean dispositionparameters for subject A, B, C, and D are very close to the meandrug disposition parameters of all twelve subjects who partici-pated in the study.
Fig. 4A shows the simulated and observed fenofibric acid plas-ma concentration profiles for the E5(80) solution at a dose strengthof 54 mg in the fasted state. Since precipitation of dissolved mate-rial was not observed for the E5(80) solution during the 4 h tests inboth the gastric and the intestinal media, the structure of the mod-el omitting precipitation and re-dissolution (as shown in Fig. 1)was used to simulate the E5(80) solution. As shown in Fig. 4A,the simulated plasma profile (solid line) of the E5(80) solution fitsthe mean observed data (symbols with error bars) very well,although that the Tmax value was slightly overestimated, and theplasma concentration after 12 h was slightly underestimated
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
Fig. 4. Simulated and observed (both individual and mean, n = 4) fenofibric acid plasma concentration profiles for the different fenofibrate lipid formulations at a dosestrength of 54 mg in the fasted state: (A) E5(80) solution, (B) E5(80) capsule, (C) E5(20) capsule and (D) MDS capsule. In silico data are shown with solid lines, in vivo meandata are shown by symbols with error bars, and in vivo individual data are depicted as dashed lines and symbols. (For interpretation of the references to color in this figurelegend, the reader is referred to the web version of this article.)
8 Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
compare to the in vivo profile. With respect to the in vivo data, itshould be noted that all four individual plasma profiles of E5(80)solution (dash lines and symbols) showed high consistency in Tmax,but the Cmax values were variable. Larger variability in the data wasobserved after 5 h, reflecting differences among the individual sub-jects with respect to elimination of fenofibrate (see Table 4).
In Fig. 4B, the simulated and observed fenofibric acid plasmaconcentration profiles of the E5(80) capsule at a dose strength of54 mg are shown. The model used to simulate the plasma concen-trations was identical to that used for the E5(80) solution. Asshown in Fig. 4B, the simulated plasma profile (solid line) of theE5(80) capsule is in good agreement but slightly lower than themean observed data out to 12 h. Although the simulated profileslightly overestimates the observed data after 12 h, the overall dif-ference between the in silico and in vivo profiles is minimal, andthis is also evident by the corresponding f2 value and ratio of thePK parameters (Table 5). Since the in vivo study was carried outin parallel rather than as a full crossover study design, the plasmaprofiles are not directly comparable among different lipid formula-tions. Even so, from the plasma profile comparison between E5(80)solution and E5(80) capsule, it seems that there is a delay in plas-ma peak (from comparison of the Tmax value) and less completeabsorption (from comparison of the AUC) of fenofibric acid fromthe E5(80) capsule. Thus, the differences observed in the dissolu-tion tests (Fig. 3) are quantitatively expressed in the simulatedplasma profiles (Fig. 4). Comparing Fig. 4A and B, it is clear thatthe presentation of the formulation (pre-diluted in a glass of watervs. administration as a capsule with a glass of water) has a stronginfluence on behavior in the GI-tract and hence on the plasmaprofile.
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
Fig. 4C shows the simulated and observed fenofibric acid plas-ma concentration profiles for the E5(20) capsule. Since fenofibratewas observed to precipitate in the in vitro dissolution profiles,additional compartments to accommodate the precipitation andre-dissolution kinetics in both the stomach and the small intestinewere included in the original STELLA� model map (modified modelmap not shown). The precipitation rate was calculated from thedissolution profiles in either FaSSGF pH 2 or FaSSIF-V2(PO4) usingtime points after 90 min and fitting the data to zero order kinetics(see Section 2.8.2). The in vitro precipitation rate constants werecalculated to be 3.426 mg h�1 in stomach and 0.777 mg h�1 insmall intestine, respectively. Additionally, to account for any re-dissolution of the precipitate, which could then be absorbed, there-dissolution rate was assumed to be identical to the initial disso-lution rate of the pure drug substance in each of the respectivemedia. For re-dissolution, the z values (Table 3) were therefore cal-culated from the dissolution profiles of unformulated drug (Fig. 3).Apart from the addition of the precipitation and re-dissolutionsteps, the STELLA� model used for the simulation of the E5(20)plasma profile was identical to that used for E5(80) formulation.As shown in Fig. 4C, the simulated plasma profile (solid line) forE5(20) capsule correlated well with the mean observed data (sym-bols with error bars) over the initial 12 h. Calculation of the overallf2 value between the in silico and in vivo profiles (f2 = 74.40, Table5) also suggests a very high degree of similarity (e.g., <10% differ-ence). Removing the precipitation and re-dissolution processesfrom the STELLA� model still resulted a similar profile, with an f2
value of 59.29 (indicating less than a 10% difference in the profiles)but was not as close to the observed profile as when these pro-cesses were taken into account. Still, this result indicates that
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

714
715
716
717
718
719
720
721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
781
782
Table 5Comparison of in silico and in vivo pharmacokinetic parameters after treatment of different fenofibrate lipid formulations at 54 mg dose strength.
Pharmacokinetic parameters E5(80) solution E5(80) capsule E5(20) capsule MDS capsule
AUC0-inf (lg mL�1 h)In silico 70.51 53.66 56.75 33.31In vivoa 78.31b 51.66 52.66 44.52Ratioc 0.90 1.04 1.08 0.75
Cmax (mg mL�1)In silico 3.92 2.95 2.31 1.57In vivoa 4.29b 3.21 2.62 1.90Ratioc 0.91 0.92 0.88 0.83
Tmax (h)In silico 1.90 2.35 4.25 3.40In vivoa 1.25b 2.00 3.00 3.25Ratioc 1.52 1.18 1.42 1.05
f2 52.78 66.28 74.40 41.37
a Mean values for in vivo data (n = 4), from the literature [16].b Mean values for in vivo data (n = 4), from the literature [17].c Ratio: PK parameter (in silico)/PK parameter (in vivo).
Fig. 5. Simulated and observed plasma fenofibric acid concentration profiles for thelipid formulations (three SMEDDSs and one MDS, n = 4). In silico data are shown bysolid lines, and in vivo mean data are depicted by symbols with error bars. (Forinterpretation of the references to color in this figure legend, the reader is referredto the web version of this article.)
Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx 9
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
precipitation does not pose an important limitation to fenofibrateabsorption for the SMEDDS studied. In Fig. 4C, it can be seen thatthe in vivo Tmax values of the individual subjects were highly vari-able. Compared with the E5(80) formulation, E5(20) dissolved andabsorbed slower, which may account for the higher variation ofTmax values in the E5(20) formulation. The differences in the PKbehavior between the E5(80) and E5(20) formulations are mostlikely a net result from differences in drug dissolution (see Table3), solubilization capacity (see Fig. 2), and precipitation properties(see Fig. 3).
Fig. 4D shows the simulated and observed fenofibric acid plas-ma concentration profiles for the MDS capsule. The model setupwas identical to that used for the E5(80) solution, in which drugprecipitation was not taken into account. As shown in Fig. 4D,the model underestimated the in vivo plasma profile somewhat.This most likely arises from the fact that the particle size of fenof-ibrate in the MDS formulation used for the in vitro dissolution andsolubility tests (<40 lm) was slightly larger than that used for thein vivo human PK studies (<37 lm). In fact, since the particle sizesused in the in vitro and in vivo studies are outside the limit of 1–10 lm, neither can really be considered micronized. Since in theMDS formulation, fenofibrate is mostly present as solid drug parti-cles suspended in the lipid blends, it is not surprising that both theobserved and the simulated AUC and Cmax values of plasma profilesfor the MDS capsule are much lower than those for the other lipidformulations examined (see Fig. 5) and suggest incomplete absorp-tion of fenofibric acid. However, since the in vivo data of four indi-vidual plasma profiles for MDS capsule showed similar AUC andTmax values (dash lines and symbols, Fig. 4D), the absorption ap-peared to be rather consistent.
An overview of the simulated and observed plasma fenofibricacid concentration for each of the lipid formulations (3 SMEDDSsand 1 MDS) is shown in Fig. 5. As can be clearly seen, each lipid for-mulation behaves differently, with the highest plasma levels ob-served for the E5(80) solution and the lowest for the MDS capsule.The simulated plasma profiles of each of the formulations were inaccordance with the in vivo data, suggesting that the in vitro–in sil-ico–in vivo (IVISIV) approach is useful for the prediction of plasmafenofibric acid concentration from lipid-based formulations.
The simulated and observed fenofibric acid PK parameters foreach of the lipid formulations are summarized in Table 5. The sim-ulated profiles for the lipid formulations were compared to thein vivo data using the point estimate ratios for both AUC0-inf andCmax. The in silico and in vivo profiles can be considered ‘‘equiva-lent’’ when the 90% confidence intervals around the point estimateratios for the simulated plasma profile fall in the 0.8–1.25 range of
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
the in vivo profile [39]. Applying this criterion, simulated profilesfor all of the lipid formulations except the MDS capsule (whichshowed an AUC0-inf ratio of 0.75, probably due to the particle sizedifference from the in vitro and in vivo experiments) can be consid-ered equivalent to their observed profiles. Similarly, the f2 valueswere greater than 50 for all of the formulations except the MDScapsule (41.37).
3.3.4. Sensitivity analysis of the model parameters for simulation of thefenofibric acid plasma profiles
In order to better understand which factors drive the pharmaco-kinetics from these formulations of fenofibrate, sensitivity analyseswere conducted on the following parameters: dissolution rate inthe stomach (zstomach), dissolution rate in the small intestine (zintes-
tine), solubility in the gastric fluid (Cs,stomach), solubility in the intes-tinal fluid (Cs,intestine), absorption rate (ka), and gastric emptying rate(kGE). Results of the analysis are summarized in Table 6. Based onthe sensitivity analysis, the oral pharmacokinetics of the lipid for-mulation is controlled not only by both dissolution and permeabil-ity in the small intestine, but also by the solubilization capacity ofthe lipid formulation for fenofibrate after dilution in the intestinalfluids. Across the formulations, the effects of dissolution rate andsolubility in small intestine on the plasma profile are increasinglyimportant in the following rank order: E5(80) solution < E5(80)
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
809
810
811
812
813
814
815
816
817
818
Table 6Summary of sensitivity analysis for the variable parameters used in the STELLA� model.
Parameter Range of values tested Impact of a change in the parametersa
E5(80) solution E5(80) capsule E5(20) capsule MDS capsule
Dissolution rate in stomach Fb=0.2–5 Negligible Negligible Negligible NegligibleDissolution rate in small intestine F = 0.2–5 Negligible Moderate Significant SignificantSolubility in gastric fluid F = 0.5–2 Negligible Negligible Negligible NegligibleSolubility in intestinal fluid F = 0.5–2 Negligible Marginal Moderate ModerateAbsorption rate F = 0.2–5 Significant Significant Significant SignificantGastric emptying rate F = 0.5–3 Negligible Negligible Negligible Negligible
a The impact of a change in the parameter was defined according to the index of either Cmax ratio or AUC ratio between the simulated and the reference profiles as follows:negligible: within 0.9–1.1, marginal: within 0.8–1.2, moderate: within 0.7–1.3, significant: outside 0.7–1.3.
b F: Factor applied to the reference input value used in the simulations.
Fig. 7. Effect of dissolution rate in small intestine (zintestine) on simulated plasmaprofiles of MDS capsule. zintestine was varied from one-fifth to five times of thereference value. In silico data are given by solid lines, while in vivo mean data aredepicted by symbols with error bars (insert map: effect of absorption rate (ka value)on simulated plasma profiles of MDS capsule). (For interpretation of the referencesto color in this figure legend, the reader is referred to the web version of thisarticle.)
10 Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
capsule < E5(20) capsule < MDS capsule. The slower in vitro releaseproperties of the E5(80) capsule, E5(20) capsule, and MDS capsulerelative to the E5(80) solution appear to be the major driving forcefor this trend.
Additionally, the hypothesis that fenofibrate lipid formulationperformance might be influenced by permeation as well as dissolu-tion (Section 3.3.2, the first paragraph) was confirmed by thesensitivity of the plasma profile to both parameters. Changingthe absorption rate had a noticeable effect on the simulation foreach of the formulations, suggesting that while fenofibrate hasbeen classified as a BCS class II compound, the plasma profile ofits lipid-based formulations is more sensitive to the permeationprocess than to changes in dissolution and solubility in the intes-tine. To illustrate how the relative importance of these two param-eters varies with formulation, we refer to Fig. 6, which shows thesensitivity of the plasma profile for the E5(80) solution to absorp-tion rate, and Fig. 7, which shows the sensitivity of the plasma pro-file of the MDS capsule to dissolution rate in the small intestine.For the E5(80) solution, a change of absorption rate (ka value) bya factor of 0.2–5 times of the reference value resulted in a 2.7-foldvariation in Cmax value in the in silico plasma profiles (Fig. 6), whilea change in the intestinal dissolution rate (zintestine) by a factor of0.2–5 resulted in no variation in the in silico plasma profiles(Fig. 6 insert). For the MDS capsule, by contrast, variations in Cmax
value in the in silico plasma profiles resulted when either the dis-solution rate in the small intestine (result in a 2.2-fold change inCmax, see Fig. 7) or the absorption rate (result in a 1.8-fold changein Cmax, see Fig. 7 insert) was varied over a range of 0.2–5 times thereference value. This difference between formulations arises
819
820
821
822
823
824
825
826
827
828
829
830
Fig. 6. Effect of absorption rate (ka value) on simulated plasma profiles of E5(80)solution. ka was varied from one-fifth to five times of the reference value. In silicodata are shown by solid lines, while in vivo mean data are depicted by symbols witherror bars (insert map: effect of dissolution rate in small intestine (zintestine) onsimulated plasma profiles of E5(80) solution). (For interpretation of the referencesto color in this figure legend, the reader is referred to the web version of thisarticle.)
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
because the dissolution and solubility limitations have, to a largeextent, been removed by the E5(80) formulation but not for theMDS formulation.
Further, sensitivity analysis revealed that the plasma profilesfor these lipid formulations are not likely to be effected by differ-ences in the dissolution rate in stomach, the solubility in gastricfluid, or changes in the gastric emptying rate.
A full sensitivity analysis for the respective parameters on the insilico plasma profiles for each formulation was conducted, and allresults are summarized in Table 6. For parameters where the sen-sitivity analysis revealed that the Cmax ratio between the simulatedand the reference plasma profiles fell within the range 0.9–1.1, theeffect of that parameter on the simulated plasma profile is given as‘‘negligible’’ in Table 6.
Interestingly, it was not necessary to consider digestion of theformulation in order to simulate the oral performance of these for-mulations. This is likely due to their composition: mostly surfac-tant with a comparatively modest fraction of medium-chainglycerides.
831
832
833
834
835
836
837
838
4. Conclusions
Biorelevant solubility and dissolution testing under fasting con-ditions of four lipid-based formulations indicated greatly enhancedsolubilization and dissolution properties of fenofibrate comparedto traditional solid dosage forms [11]. By incorporating the dissolu-tion data with the PBPK model using STELLA� software, humanplasma fenofibric acid concentration profiles were accurately pre-dicted for an oral solution and two capsule dosage forms, while the
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001

839
840
841
842
843
844
845
846
847
848
849
850
851
852
853
854
855
856
857
858
859
860
861
862
863
864
865
866
867
868
869870871872873874875876877878879880881882883884885886887888889890891892893894895896897898899900901902903904905906907908909
910911912913914915916917918919920921922923924925926927928929930931932933934935936937938939940941942943944945946947948949950951952953954955956957958959960961962963964965966967968969970971972973974975976977978979980981982983984985986987988989990991992993994
Y. Fei et al. / European Journal of Pharmaceutics and Biopharmaceutics xxx (2013) xxx–xxx 11
EJPB 11350 No. of Pages 11, Model 5G
16 March 2013
fourth formulation was generally well predicted (considering thatit was not possible to completely reproduce the particle size distri-bution of the suspension that had been administered in the phar-macokinetic study). Detailed sensitivity analysis providedevidence that the absorption of fenofibrate from the lipid-basedformulations was highly dependent on the ability of the excipientsto enhance fenofibrate solubility and dissolution from the formula-tion under intestinal conditions and on the permeation rate offenofibrate in the small intestine. By contrast, the plasma profileseems not be dependent upon the dissolution performance in thestomach or on the gastric emptying rate. For these Type IIIA-MCand Type IIIB-MC lipid-based dosage forms, it was not necessaryto consider digestion to predict the in vivo differences inperformance.
Based on these results, it appears that the in vitro–in silico–in vivo approach may provide a useful tool for identifying and com-paring limitations to oral absorption for lipid-based formulationsand for optimizing lipid formulation development of poorly solubledrugs.
Acknowledgements
The authors would like to acknowledge the China ScholarshipCouncil (CSC) for its financial support of Yang Fei during hisPh.D. study at Goethe University Frankfurt. The authors would alsolike to express their thanks to Mr. Atsushi Kambayashi and Ms.Ying-Chen Chen for their kind assistance with model setup and de-tailed information about the pharmacokinetic studies, respectively.Some results from this work were presented at the 8th worldmeeting of Pharmaceutics, Biopharmaceutics and Pharmaceuticaltechnology (PBP), March 19 to 22, 2012, Istanbul, Turkey.
References
[1] C. Leuner, J.B. Dressman, Improving drug solubility for oral delivery using soliddispersions, Eur. J. Pharm. Biopharm. 50 (2000) 47–60.
[2] S.F. Han, T.T. Yao, X.X. Zhang, L. Gan, C. Zhu, H.Z. Yu, Y. Gan, Lipid-basedformulations to enhance oral bioavailability of the poorly water-soluble druganethol trithione: effects of lipid composition and formulation, Int. J. Pharm.379 (2009) 18–24.
[3] A.J. Humberstone, W.N. Charman, Lipid-based vehicles for the oral delivery ofpoorly water soluble drugs, Adv. Drug Deliv. Rev. 25 (1997) 103–128.
[4] C.W. Pouton, Lipid formulation for oral administration of drugs: non-emulsifying, self-emulsifying and ‘self-microemulsifying’ drug deliverysystems, Eur. J. Pharm. Sci. 11 (2000) 93–98.
[5] L. Hu, H. Wu, F. Niu, C. Yan, X. Yang, Y. Jia, Design of fenofibrate microemulsionfor improved bioavailability, Int. J. Pharm. 420 (2011) 251–255.
[6] P. Ratanabanangkoon, H. Guzman, O. Almarsson, D. Berkovitz, S. Tokarcyzk,A.B. Straughn, H. Chen, A high-throughput approach towards a novelformulation of fenofibrate in omega-3 oil, Eur. J. Pharm. Sci. 33 (2008) 351–360.
[7] K. Mohsin, M.A. Long, C.W. Pouton, Design of lipid-based formulations for oraladministration of poorly water-soluble drugs: precipitation of drug afterdispersion of formulations in aqueous solution, J. Pharm. Sci. 98 (2009) 3582–3595.
[8] H.D. Williams, P. Sassene, K. Kleberg, J.C. Bakala-N’Goma, M. Calderone, V.Jannin, A. Igonin, A. Partheil, D. Marchaud, E. Jule, J. Vertommen, M. Maio, R.Blundell, H. Benameur, F. Carriere, A. Mullertz, C.J.H. Porter, C.W. Pouton,Toward the establishment of standardized in vitro tests for lipid-basedformulations, part 1: method parameterization and comparison of in vitrodigestion profiles across a range of representative formulations, J. Pharm. Sci.101 (2012) 3360–3380.
[9] M.U. Anby, H.D. Williams, M. McIntosh, H. Benameur, G.A. Edwards, C.W.Pouton, C.J.H. Porter, Lipid digestion as a trigger for supersaturation evaluationof the impact of supersaturation stabilization on the in vitro and in vivoperformance of self-emulsifying drug delivery systems, Mol. Pharm. 9 (2012)2063–2079.
[10] J.B. Dressman, K. Thelen, E. Jantratid, Towards quantitative prediction of oraldrug absorption, Clin. Pharmacokinet. 47 (2008) 655–667.
[11] D. Juenemann, E. Jantratid, C. Wagner, C. Reppas, M. Vertzoni, J.B. Dressman,Biorelevant in vitro dissolution testing of products containing micronized ornanosized fenofibrate with a view to predicting plasma profiles, Eur. J. Pharm.Biopharm. 77 (2011) 257–264.
[12] D. Juenemann, J. Dressman, Analytical methods for dissolution testing ofnanosized drugs, J. Pharm. Pharmacol. 64 (2012) 931–943.
995
Please cite this article in press as: Y. Fei et al., Analysis of the enhanced oral bin vitro–in silico–in vivo approach, Eur. J. Pharm. Biopharm. (2013), http://dx.d
[13] C. Wagner, E. Jantratid, F. Kesisoglou, M. Vertzoni, C. Reppas, J.B. Dressman,Predicting the oral absorption of a poorly soluble, poorly permeable weak baseusing biorelevant dissolution and transfer model tests coupled with aphysiologically based pharmacokinetic model, Eur. J. Pharm. Biopharm. 82(2012) 127–138.
[14] Y. Shono, E. Jantratid, J.B. Dressman, Precipitation in the small intestine mayplay a more important role in the in vivo performance of poorly soluble weakbases in the fasted state: case example nelfinavir, Eur. J. Pharm. Biopharm. 79(2011) 349–356.
[15] M.D. Muria, G. Lamberti, G. Titomanlio, Physiologically basedpharmacokinetics: a simple, all purpose model, Ind. Eng. Chem. Res. 49(2010) 2969–2978.
[16] J.D. Wei, H.O. Ho, C.H. Chen, W.T. Ke, E.T.H. Chen, M.T. Sheu, Characterisation offenofibrate dissolution delivered by a self-microemulsifying drug-deliverysystem, J. Pharm. Pharmacol. 62 (2010) 1685–1696.
[17] Y.M. Lin, J.Y. Wu, Y.C. Chen, Y.D. Su, W.T. Ke, H.O. Ho, M.T. Sheu, In situformation of nanocrystals from a self-microemulsifying drug delivery systemto enhance oral bioavailability of fenofibrate, Int. J. Nanomed. 6 (2011) 2445–2457.
[18] E. Nicolaides, M. Symillides, J.B. Dressman, C. Reppas, Biorelevant dissolutiontesting to predict the plasma profile of lipophilic drugs after oraladministration, Pharm. Res. 18 (2001) 380–388.
[19] L.X. Yu, An integrated model for determining causes of poor oral drugabsorption, Pharm. Res. 16 (1999) 1883–1887.
[20] C. Schiller, C.P. Frohlich, T. Giessmann, W. Siegmund, H. Monnikes, N. Hosten,W. Weitschies, Intestinal fluid volumes and transit of dosage forms as assessedby magnetic resonance imaging, Aliment. Pharmacol. Ther. 22 (2005) 971–979.
[21] E. Jantratid, N. Janssen, C. Reppas, J.B. Dressman, Dissolution media simulatingconditions in the proximal human gastrointestinal tract: an update, Pharm.Res. 25 (2008) 1663–1676.
[22] E. Galia, E. Nicolaides, D. Horter, R. Lobenberg, C. Reppas, J.B. Dressman,Evaluation of various dissolution media for predicting in vivo performance ofclass I and II drugs, Pharm. Res. 15 (1998) 698–705.
[23] M. Vertzoni, J. Dressman, J. Butler, J. Hempenstall, C. Reppas, Simulation offasting gastric conditions and its importance for the in vivo dissolution oflipophilic compounds, Eur. J. Pharm. Biopharm. 60 (2005) 413–417.
[24] E.S. Kostewicz, M. Wunderlich, U. Brauns, R. Becker, T. Bock, J.B. Dressman,Predicting the precipitation of poorly soluble weak bases upon entry in thesmall intestine, J. Pharm. Pharmacol. 56 (2004) 43–51.
[25] S. Klein, The mini paddle apparatus-a useful tool in the early developmentalstage? Experiences with immediate-release dosage forms, Dissol. Technol. 13(4) (2006) 6–11.
[26] J. Najib, Fenofibrate in the treatment of dyslipidemia: a review of the data asthey relate to the new suprabioavailable tablet formulation, Clin. Ther. 24(2002) 2022–2050.
[27] A. Hanafy, H. Spahn-Langguth, G. Vergnault, P. Grenier, M. Tubic Grozdanis, T.Lenhardt, P. Langguth, Pharmacokinetic evaluation of oral fenofibratenanosuspensions and SLN in comparison to conventional suspensions ofmicronized drug, Adv. Drug Deliv. Rev. 59 (2007) 419–426.
[28] M. Kataoka, Y. Masaoka, Y. Yamazaki, T. Sakane, H. Sezaki, S. Yamashita, In vitrosystem to evaluate oral absorption of poorly water-soluble drugs:simultaneous analysis on dissolution and permeation of drugs, Pharm. Res.20 (2003) 1674–1680.
[29] P. Buch, P. Languth, M. Kataoka, S. Yamashita, IVIVC in oral absorption forfenofibrate immediate release tablets using a dissolution/permeation system,J. Pharm. Sci. 98 (2009) 2001–2009.
[30] P. Buch, P. Holm, J.Q. Thomassen, D. Scherer, R. Branscheid, U. Kolb, P.Langguth, IVIVC for fenofibrate immediate release tablets using solubility andpermeability as in vitro predictors for pharmacokinetics, J. Pharm. Sci. 99(2009) 4427–4436.
[31] P. Artursson, J. Karlsson, Correlation between oral drug absorption in humansand apparent drug permeability coefficients in human intestinal epithelial(Caco-2) cells, Biochem. Biophys. Res. Commun. 175 (1991) 880–885.
[32] R. Takano, K. Sugano, A. Higashida, Y. Hayashi, M. Machida, Y. Aso, S.Yamashita, Oral absorption of poorly water-soluble drugs: computersimulation of fraction absorbed in humans from a miniscale dissolution test,Pharm. Res. 23 (2006) 1144–1156.
[33] G.M. Grass, Simulation models to predict oral drug absorption from in vitrodata, Adv. Drug Deliv. Rev. 23 (1997) 199–219.
[34] J. Dressman, J. Kraemer, Pharmaceutical Dissolution Testing, Taylor & FrancisGroup, Boca Raton, USA, 2005.
[35] T. O’Hara, A. Dunne, J. Butler, J. Devane, A review of methods used to comparedissolution profile data, Pharm. Sci. Technol. Today 1 (1998) 214–223.
[36] C.W. Pouton, Formulation of poorly water-soluble drugs for oraladministration: physicochemical and physiological issues and the lipidformulation classification system, Eur. J. Pharm. Sci. 29 (2006) 278–287.
[37] V.H. Sunesen, R. Vedelsdal, H.G. Kristensen, L. Christrup, A. Mullertz, Effect ofliquid volume and food intake on the absolute bioavailability of danazol, apoorly soluble drug, Eur. J. Pharm. Sci. 24 (2005) 297–303.
[38] J.M. Cardot, B.M. Davit, In vitro–in vivo correlations: tricks and traps, AAPS J. 14(2012) 491–499.
[39] EMEA, Guideline on the Investigation of Bioequivalence, CPMP/EWP/QWP/1401/98, 2010. <http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/01/WC500070039.pdf.
ioavailability of fenofibrate lipid formulations in fasted humans using anoi.org/10.1016/j.ejpb.2013.03.001