Embed Size (px)
Citation preview

Analysis of Out-of-Pocket Expenditures in the Philippines
Valerie Gilbert Ulep and Nina Ashley dela Cruz
Supervising Research Specialist and Research Analyst Philippine Institute for Development Studies
July 1, 2014

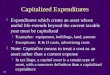
Objectives of the Study
• Determine the patterns of OOP over time • Dissect the different sources of OOP • Estimate the following:
– PhilHealth Support Value – Utilization rates and other related indicators
• Estimate the burden of payments and impoverishment due to OOP.
• Inequities in health financing (not included in the presentation)

Data Sources
• Family Income and Expenditure Surveys (2000 to 2012)
• Annual Poverty Indicators Survey (2011) • Hospital Statistical Reports (2011) • Claims data of PhilHealth (results not
included)

Out of Pocket: importance • Highly catastrophic; impoverishing • Signals ineffective and inefficient healthcare
system • Higher risk of forgoing care, delayed health
seeking and non-compliance • The goal is not to totally eliminate OOP:
– Tame the rapid growth – Decrease it to rational levels
• The ‘realistic’ goal is to reduce OOP by less than 50% (by 2016) by increasing the share of social insurance.

OOP expenditures “any direct outlay by households to health practitioners and suppliers of pharmaceuticals, therapeutic appliances, and other goods and services whose primary intent is to contribute to the restoration or enhancement of the health status of individuals or population groups”

Total Health Expenditures
Government (national &
local)
Social insurance
Private sources Others
OOP
Private insurance
HMOs
Private establishments

- 50,000
100,000 150,000 200,000 250,000 300,000 350,000 400,000 450,000 500,000
in m
illio
n Ph
P
Total health expenditure, Philippines, 1991-2011
current constant
THE is growing in a fast rate!! Is the growth rational?

-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2009 2010 2011
Sources of health expenditures, Philippines 1994-2011
Government Social insurance Out-of-pocket Private insurance + HMO
6.3%
8.5%
9.5%
Note: in constant terms using 2006 CPI Source of raw data: NSCB 2006
OOP outpacing other sources of financing….
3.9%

0.38 0.35 0.36 0.37 0.35 0.36 0.38 0.39 0.39 0.41 0.35
0.30 0.31 0.29 0.26 0.23 0.26 0.26 0.27 0.27
0.05 0.06 0.06 0.06
0.05 0.05 0.05 0.04 0.05 0.07 0.08
0.09 0.09 0.09 0.10
0.09 0.09 0.08 0.09 0.09
0.47 0.49 0.47 0.47 0.50 0.48 0.46 0.46 0.43 0.40 0.45 0.49 0.47 0.49 0.53 0.57 0.54 0.53 0.53 0.53
0.04 0.04 0.04 0.04 0.04 0.04 0.04 0.05 0.06 0.06 0.06 0.06 0.07 0.06 0.07 0.07 0.07 0.07 0.07 0.07 0.05 0.06 0.06 0.06 0.07 0.07 0.06 0.06 0.06 0.06 0.06 0.06 0.06 0.06 0.05 0.05 0.04 0.05 0.05 0.04
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
19911992199319941995199619971998199920002001200220032004200520062007200920102011
Sources of health expenditures, Philippines, 1991-2011
Government Social insurance Out-of-pocket
Source of raw data: NSCB
More than 50 percent of the THE are accounted to OOP…

OOP across ASEAN…..
34.1 40.4
49.3
85.1
22.5
31.0
75.5
33.3
55.2
13.0
49.9
55.7 39.7
14.8
56.9
60.4 13.7 55.9 35.4 80.7
16.0 4.0 11.0 0.2 20.7 8.6 10.9 10.7 9.4 6.4
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Indonesia Viet Nam LaoPeople's
DemocraticRepublic
BruneiDarussalam
Cambodia Singapore Thailand Philippines Malaysia Myanmar
Share of financing, ASEAN countries, 2011
Government OOP other private

Year Current Constant (2006)
Q1 Q2 Q3 Q4 Q5 National Q1 Q2 Q3 Q4 Q5 National
2000 301 624 1,114 2,210 7,084 2,267 416 862 1,539 3,053 9,785 3,131
2003 388 843 1,452 2,708 7,528 2,582 445 967 1,665 3,106 8,633 2,961
2006 506 1,083 2,054 3,807 13,516 4,193 506 1,083 2,054 3,807 13,516 4,193
2009 635 1,312 2,426 4,892 15,138 4,880 547 1,131 2,091 4,217 13,050 4,207
2012 1,379 2,424 3,850 8,240 19,283 7,035 1,075 1,889 3,001 6,422 15,029 5,483
AGR* 46% 21%
Average OOP health expenditure is increasing both in nominal and constant terms…
Increasing OOP=increasing demand for care Source: analysis of various rounds of FIES surveys

Medicines account for more than half of the out of pocket expenditures.The poorest spend less on inpatient and outpatient care services relative to their total OOP health expenditures. This suggests heavy reliance on medicines in lieu of actual visit to a health facility…
Components Quintile 1 Quintile 5 National
ave exp Share ave exp Share ave exp Share
Medical products 514.6 59% 10,189.6 46% 3,415.1 49%
Pharma products 329.7 64% 6,597.6 65% 2,191.9 64%
Nutritionals 148.5 29% 2,934.3 29% 997.7 29%
Other medical prep 20.1 4% 304.7 3% 107.8 3%
Other medical products 11.9 2% 129.2 1% 48.9 1%
Therapeutic appliance 4.4 1% 223.8 2% 68.8 2%
Outpatient services 113.7 13% 3,876.2 17% 1,101.0 16%
Medical services 86.9 76% 3,224.2 83% 917.8 83%
Dental services 3.3 3% 366.0 9% 89.5 8%
Paramedical services 23.5 21% 286.1 7% 93.7 9%
Inpatient services 242.2 28% 8,271.0 37% 2,519.0 36%
Public 179.7 74% 1,104.4 13% 664.1 26%
Private 62.4 26% 7,166.6 87% 1,854.9 74% Source: analysis of various rounds of FIES surveys

2.7% 3.0% 2.4% 2.6% 3.9% 5.5% 6.5% 5.2% 5.4% 6.9% 9.8% 11.2% 9.8% 9.9%
10.9%
19.5% 21.0%
18.2% 20.1% 23.4%
62.5% 58.3% 64.4% 62.1%
54.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2000 2003 2006 2009 2012
Share of OOP health expenditure by quintile groups, Philippines, 2000-2012
Q1 Q2 Q3 Q4 Q5
Healthcare overutilization and underutilization among the richer and poorer segments remain to be a problem. The lack of effective policy and regulatory instruments (direct and indirect) that control health expenditure in richer segments may not lead to decrease in the total value of OOP.
Source: analysis of various rounds of FIES surveys

Burden of OOP payments is rising….
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
Q1 Q2 Q3 Q4 Q1 Philippines
Share of OOP to capacity to pay, 2000 to 2012
2000 2003 2006 2009 2012Source: analysis of various rounds of FIES surveys

Higher number (percentage) of HH experiencing catastrophe due to OOP payments..
0.4
0.6 0.6
0.9
1.1
0.7
0.4
0.6
0.8 0.8
1.0
0.7
0.4
0.9
1.1 1.2
1.8
1.1
0.5
0.9 1.1
1.6
2.0
1.2
0.8
1.3
1.6 1.6
2.3
1.5
0.0
0.5
1.0
1.5
2.0
2.5
Q1 Q2 Q3 Q4 Q5 Philippines
perc
ent
Prevalence of HH that experienced catastrophe due to OOP
2000 2003 2006 2009 2012
If burden of payments [OOP/income], exceeds a specified threshold. World Health Organization researchers use 40 percent as threshold when “capacity to pay” (roughly, total expenditure minus food) is used as the denominator (Xu, 2005)
Source: analysis of various rounds of FIES surveys

Increasing number (and percentage) of impoverished HH due to OOP..
indicators 2000 2003 2006 2009 2012
headcount pre-OOP 23.1% 19.2% 19.8% 18.4% 19.4%
headcount post-OOP 23.7% 19.9% 20.6% 19.2% 20.4%
% of impoverished HH 0.6% 0.7% 0.9% 0.8% 1.0%
poverty gap before OOP 231.8 191.8 222.0 240.6 282.1
poverty gap after OOP 239.1 199.4 232.7 252.6 299.7
difference 7.2 7.5 10.7 12.0 17.5
Source: analysis of various rounds of FIES surveys

Why OOP is continuously growing?
• Are we covering everyone? • Are the people utilizing their benefits?
Especially the poor? • Is PHIC doing enough to increase the
support value? • Is PHIC doing enough to control
healthcare cost?

1.1% 1.5% 2.3% 2.8%
4.6%
2.3%
18.3% 17.6% 16.6% 16.6%
16.7%
17.3%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5 Philippines
Benefit utilization and demand for care, 2011
ill and availed PHIC did not avail but got sick
Low benefit utilization vis-a-vis demand for care…
Source: authors’ calculation using APIS 2011

Why significant number of patients are not covered with PhilHealth? And why private hospitals are more efficient in admitting PhilHealth patients?
65.9%
29.6%
44.7% 49.0% 57.5%
30.9%
70.1%
54.2% 49.8% 40.1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Private DOH retained Local Government Others Total
patient discharges, PHIC status, 2011
PHIC non-PHIC
Source: authors’ calculation of 2011 HSR

Why government hospitals are still saturated with non-PHIC ‘charity’ cases?
44.6%
20.3% 18.2%
31.1% 34.5%
11.9%
6.9% 15.6%
11.0% 12.9%
39.9%
23.9% 20.0%
24.7%
32.1%
3.7%
48.9% 46.2%
33.3%
20.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Private DOH-retained LGU hospitals Others Total
Distribution of admissions, by type of patients, 2011
Paying PHIC Indigent PHIC Paying non-PHIC Charity non-PHIC
Source: authors’ calculation of 2011 HSR; number of hospitals: 963

Low support value of PhilHealth…
53.8%
42.7% 44.2% 39.3%
32.9%
41.4%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
PHIC Support value, by socio-economic status, 2011
Source: authors’ calculation using APIS 2011
Significance (chi-square): p:0.000 (significant)
44.7%
41.1%
39.0%
40.0%
41.0%
42.0%
43.0%
44.0%
45.0%
46.0%
CCT non-CCT
PHIC Support Value, by CCT membership, 2011
Significance (chi-square): p:0.000 (significant)

Are we covering the most vulnerable age groups?
41.1%
43.9%
40.7% 41.0% 40.5%
39.2%
37.1%
32.0%
34.0%
36.0%
38.0%
40.0%
42.0%
44.0%
46.0%
less than 5 6-20 years old 21-30 years old 31-40 years old 41-50 years old 51-60 years old 61 and above
Support value of PHIC, by age group, 2011
Significance (chi-square): p:0.01 (significant) Source: authors’ calculation using APIS 2011

Why there is regional variation in SV?
45.2%
34.3%
48.9%
27.8%
41.7%
49.6%
22.3%
50.3%
41.4%
57.1%
34.4%
44.9% 41.3%
92.6%
54.7%
42.5%
24.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Support value of PHIC, by region, 2011
Significance (chi-square): p:0.000 (significant) Source: authors’ calculation using APIS 2011

.
Source: authors’ calculation using APIS 2011
Highly variable and dispersed value of reimbursements.. PHIC reimbursements by quintile, 2011

Key Findings • OOP continue to rise despite the enormous
programmatic and policy reforms in the health financing system.
• The growth in OOP is outpacing other key financial sources like social insurance and government spending.
• Healthcare demand is increasing as manifested by the increasing average household OOP health expenditures (both in nominal and constant terms). The growth is notable in all SES groups.
• Drugs continue to be the major source of OOP expenditure.

Key Findings
• The prevalence of catastrophic payments and incidence of impoverishment due to OOP are increasing.
• There is a compelling evidence of underutilization and overutilization of healthcare services and goods.

Key Findings
• The support value of PHIC is less than 50 percent. Highly variable across SES, regions, age groups.
• The support value of vulnerable groups are low.
• Significant portion of patients in hospitals are not PHIC members. Private hospitals are more efficient in admitting patients with PHIC.