Embed Size (px)
Citation preview
COMPREHENSIVE MANAGEMENT OF
PATIENTS WITH COMPLICATED
INTRA-ABDOMINAL INFECTIONS
STRATEGIES TO OPTIMIZE CLINICAL
OUTCOMES IN PATIENTS WITH CIAIS
Nicholas Namias, MD, MBA, FACS, FCCMUniversity of Miami Miller School of MedicineMiami, Fla.
GUIDELINES FOR ANTIMICROBIAL
TREATMENT OF CIAIS
John E. Mazuski, MD, PhD, FACSWashington University School of MedicineSt. Louis, Mo.
PREVENTING COLLATERAL DAMAGE
IN THE MANAGEMENT OF PATIENTS
WITH CIAIS
Robert G. Sawyer, MD, FACSUniversity of Virginia Health SystemCharlottesville, Va.
This educational activity is sponsored by Cerebrio.
A Supplement to
Supported by an educational grant from Schering-Plough Corporation.

PR E S I D E N T, EL S E V I E R/IMNGAlan J. Imhoff
VI C E PR E S I D E N T, ME D I C A L
ED U C A T I O N
Sylvia H. Reitman, MBA
DI R E C T O R, EL S E V I E R SO C I E T Y
NE W S GR O U P
Mark Branca
PR O G R A M MA N A G E R, ME D I C A L
ED U C A T I O N
Jenny McMahon
GR A P H I C DE S I G N E R
Yenling Liu
PR O D U C T I O N SP E C I A L I S T
Tracy Law
This supplement is based on proceedingsof a symposium held on October 10,2007, in New Orleans, La.
This supplement was produced by themedical education department of Elsevier Society News Group, a divisionof Elsevier/International Medical NewsGroup. Neither the editor of SURGERY
NEWS, the Editorial Advisory Board,the American College of Surgeons, northe reporting staff contributed to itscontent. The opinions expressed in thissupplement are those of the faculty anddo not necessarily reflect the views ofthe American College of Surgeons, thesupporter, or the Publisher.
Copyright © 2008 Elsevier Inc. All rightsreserved. No part of this publication maybe reproduced or transmitted in any form,by any means, without prior written per-mission of the Publisher. Elsevier Inc. willnot assume responsibility for damages,loss, or claims of any kind arising from orrelated to the information contained inthis publication, including any claims re-lated to the products, drugs, or servicesmentioned herein.
Cover photo ©Andres Rodriguez/Fotolia
TABLE OF CONTENTS
Strategies to Optimize Clinical Outcomes in Patients With Complicated Intra-Abdominal Infections .................................................................. 4
Nicholas Namias, MD, MBA, FACS, FCCMChief, Division of BurnsAssociate Professor of SurgeryUniversity of Miami Miller School of MedicineMiami, Fla.
Guidelines for Antimicrobial Treatment of Complicated Intra-Abdominal Infections ................ 6
John E. Mazuski, MD, PhD, FACSAssociate Professor of SurgerySection of Acute and Critical Care SurgeryWashington University School of MedicineSt. Louis, Mo.
Preventing Collateral Damage in the Management of Patients With Complicated Intra-Abdominal Infections ..................................... 9
Robert G. Sawyer, MD, FACSProfessor of Surgery and Public Health SciencesDepartment of SurgeryUniversity of Virginia Health SystemCharlottesville, Va.
CME Evaluation and Post-Test Instructions........... 12
COMPREHENSIVE MANAGEMENT
OF PATIENTS WITH COMPLICATED
INTRA-ABDOMINAL INFECTIONS
TARGET AUDIENCEThis activity is intended for surgeonsand other health care practitionerswho diagnose or treat patients in ahospital setting.
NEEDS ASSESSMENTComplicated intra-abdominal infec-tions (cIAIs) are a major surgical chal-lenge because they are associated withhigh morbidity and mortality. In ad-dition, cIAIs constitute a substantialburden on health care resources be-cause patients with cIAIs not only re-quire a great deal of attention fromsurgeons and other practitioners, butalso often undergo extended stays inthe intensive care unit and the hospi-tal, requiring numerous laboratory,imaging, and surgical procedures. Theultimate treatment goal for individu-als with cIAIs is to avoid mortality dueto the disease process. Optimal man-agement of the patient will also de-crease use of health care resources andshorten the time to recovery. The fun-damental ways to achieve these goalsare through appropriate source control(surgical debridement, drainage, andrepair), carefully selected antimicrobialtherapy, and adjunctive measures to re-store normal physiology.
LEARNING OBJECTIVESAfter completing this program, par-ticipants should be better able to:• Describe surgical, interventional,
metabolic, and resuscitative strate-gies in the management of cIAIs
• Discuss current guidelines for anti-microbial therapy of cIAIs
• Indicate how to incorporate theseprinciples into clinical practice inorder to optimally manage cIAIsand prevent collateral damage
ACCREDITATION STATEMENTThis activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for ContinuingMedical Education (ACCME). Cerebriois accredited by the ACCME to providecontinuing medical education for physicians.
CREDIT DESIGNATIONCerebrio, LLC, designates this educa-tional activity for a maximum of 1.5AMA PRA Category 1 Credit(s)TM.Physicians should only claim creditcommensurate with the extent of theirparticipation in the activity.
FACULTY DISCLOSUREAs an organization accredited by theACCME, Cerebrio, LLC, must ensurebalance, independence, objectivity, andscientific rigor in all its sponsored ed-ucational activities. Individuals in aposition to control the content of aneducational activity must disclose tothe activity audience all relevant fi-nancial relationships with any com-mercial interest. The ACCME defines“relevant financial relationships” asfinancial relationships in any amount,occurring within the past 12 months,including financial relationships of a
spouse or partner, which could createa conflict of interest. Cerebrio, LLC,also encourages authors to identify in-vestigational products or off-label usesof products regulated by the US Foodand Drug Administration.
The following faculty have reportedreal or apparent conflicts of interestthat have been resolved through apeer-review content validation process:
John E. Mazuski, MD, PhD, FACS,discloses that he has served as a paidconsultant to Ortho-McNeil, Inc.,Pfizer Inc., Schering-Plough Corpora-tion, and Wyeth Pharmaceuticals, Inc.He has received research support fromArtisan Pharma, Inc., Ortho BiotechProducts, LP, and Pfizer. Dr Mazuskihas developed educational materialsfor Ortho-McNeil, Schering-Plough,and Wyeth. He has also served as aspeaker for Pfizer, Schering-Plough,and Wyeth.
Nicholas Namias, MD, MBA, FACS,FCCM, discloses that he has served asa paid consultant to AstraZeneca Phar-maceuticals LP, Merck & Co., Inc.,Pfizer, and Schering-Plough. He hasreceived research support from Merckand Ortho-McNeil and has developededucational materials for Schering-Plough. He has also served as a speak-er for AstraZeneca, Merck, and Pfizer.
Robert G. Sawyer, MD, FACS, dis-closes that he has served as a paid con-sultant to Merck, Ortho-McNeil, Pfizer, and Wyeth. He has served as aspeaker for Merck and Ortho-McNeil.
c I A I

Epidemiology and PrognosisComplicated intra-abdominal infections(cIAIs) are a major surgical challenge be-cause they are associated with high mor-bidity and mortality.1 While the treat-ment failure and mortality rates observedin clinical trials are 15% and <5%, re-spectively, they can reach 32% in high-risk patients (who are often excludedfrom these trials).2 The ultimate treat-ment goal is to avoid mortality; in addi-tion, however, every effort should bemade to decrease the use of health care re-sources and shorten the time to recovery.Cases of acute appendicitis, for example,are situations in which proper empirictherapy may result in fewer complicationsand, therefore, reduced mortality.3
Treatment PrinciplesThe fundamental principles associatedwith optimal empiric treatment of cIAIinclude proper initial resuscitation, ap-propriate source control, carefully select-ed antimicrobial therapy, and adjunctivemeasures to restore normal physiology.Achieving stabilization of vital signsthrough circulatory support measures isparamount in the management of pa-tients with cIAIs; ideally, source-controlmeasures should be undertaken after he-modynamic stability is established.Source control is defined as the eradica-tion of the septic focus, which can be per-formed via drainage and/or debridementof purulent materials or necrotic tissues.In addition, antibiotics should be initi-ated as soon as the diagnosis of cIAI ismade or even suspected.1 The Surgical In-fection Society has published guidelinesfor the use of antimicrobial therapy in pa-tients with cIAIs.4 In patients with com-munity-acquired cIAIs, empiric agentsshould have coverage against gram-neg-ative aerobic and anaerobic bacteria with-in the narrowest possible spectrum.1,4
Adding coverage for microbial agentssuch as Enterococcus or Candida is reason-able in higher-risk patients with postop-erative infections.4 Most patients with
cIAIs should be treated with antimicro-bial agents for no more than 5 to 7 daysin an attempt to reduce the risk for pro-moting nosocomial resistant organisms.4
Several agents used as monotherapy haveproved to be as efficacious as combinationtherapy in the management of cIAIs.However, it is still unknown if exposureto a monotherapy is less likely to promoteresistant organisms than is exposure tocombined regimens.
Surgical and Interven-tional ApproachesClinical outcomes for patients with cIAIsmay be influenced by factors such as tim-ing of surgery and the use of various man-agement techniques. In a 6-year prospec-tive study that reviewed data on 451children with a clinical diagnosis of acuteappendicitis, it was found that postponingsurgery for 1 to 6 days because of uncer-tainty of the diagnosis (n=126), as opposedto performing surgery on the day of ad-mission (n=324), had no effect on post-operative morbidity or mortality.5 Thepositive predictive value of “watchful wait-ing” was 97.9%. It is, therefore, possiblethat in cases in which the clinical diagno-sis is in doubt, active observation may notresult in added risk for adverse clinical out-comes.5 In addition, the probability offinding histologically normal appendicespostoperatively might decline according-ly.5 Another management factor related totiming is the method used to close the sur-gical wound. When primary closure (PC)and delayed primary closure (DPC) meth-ods were compared in a prospective, ran-
domized study of 51 patients with dirtyabdominal wounds, both groups weresimilar in measures of cost and length ofstay (LOS) in the hospital; the PC group,however, experienced higher wound in-fection rates.6 Consequently, DPC may bean appropriate option for the managementof dirty abdominal wounds.6
In a retrospective analysis that com-pared laparoscopic appendectomy (LA) in175 patients and open appendectomy(OA) in 69 patients with perforated organgrenous appendicitis, wound infec-tion rates were shown to be significant-ly different.7 Both groups had similar de-mographic characteristics. Although theLA patients had significantly shorter op-erative times, shorter LOS, and lowerrates of wound infection, they did notdemonstrate lower rates of IAI (Table).7
To explore the infectious risks associ-ated with LA, Gupta and colleagues re-viewed the charts of patients who had re-ceived LA during a 7-year period.8 Theoccurrence of infectious complicationswas associated with the presence of gan-grenous appendicitis and with the use ofhigh volumes of irrigation fluid in LA.The significantly higher rate of infectiouscomplications in cases in which high vol-umes of irrigation fluid were used mayhave resulted from either the spreadingof the infection beyond the surgical areabecause of the excess irrigation fluid orthe rough manipulation of the infectedappendix that may occur in such cases.8
Conversely, peritoneal drainage ap-pears to have the same effect on outcomesas does a major operative procedure when
4 Comprehensive Management of Patients With Complicated Intra-Abdominal Infections
STRATEGIES TO OPTIMIZE CLINICAL OUTCOMES IN PATIENTSWITH COMPLICATED INTRA-ABDOMINAL INFECTIONS
NICHOLAS NAMIAS, MD, MBA, FACS, FCCM
TABLE. LAPAROSCOPIC VERSUS OPEN APPENDECTOMY:COMPARISON OF OPERATIVE TIME, LENGTH OF STAY, AND
COMPLICATIONS
LA OA P-ValueAverage operative time 55 min 70 min <0.001Average LOS 5 d 6 d <0.001Wound infection 1 (0.6%) 7 (10%) 0.001IAI 10 (5.7%) 3 (4.3%) 0.473
LOS=length of stay; IAI=intra-abdominal infection.Reproduced with permission from Elsevier.7

performed in preterm infants with per-forated necrotizing enterocolitis (NEC).In a multicenter, randomized trial, 117preterm low-birth-weight infants withNEC were randomly assigned to eitherprimary peritoneal drainage or laparoto-my and bowel resection.9 Three monthslater, the mortality rate in the group thatreceived peritoneal drainage was 34.5%,compared with 35.5% in the laparotomygroup (P=0.92). In addition, the twogroups had a similar mean LOS andcomparable percentages of infants whodepended on total parenteral nutrition(TPN).9
Similarly, in patients with infectedpancreatic necrosis, which is associatedwith high mortality and morbidity rates,the standard approach is surgical de-bridement and drainage through anopen-abdomen technique. However,Echenique et al studied the effects ofpercutaneous catheter-directed debride-ment (another simple interventionaltechnique) on 20 hemodynamically sta-ble patients with the disease over an 8-year period.10 The mortality rate was0%; patients received an average of 17sessions of debridement and stayed inthe intensive care unit for an average of9 days and at home with catheters foroutpatient follow-up for an average of 32days. Based on the results of this study,irrigational debridement can be consid-ered a safe and effective first-line treat-ment option for managing hemody-namically stable patients with infectednecrotizing pancreatitis.10
While evidence exists regarding theuse of alternative surgical and interven-tional techniques to optimize clinical out-comes in certain patients, there are veryfew available data to support the commonpractice of intraoperative peritoneal lavage(IOPL).11 About 97% of surgeons report-ed using IOPL in a postal survey con-ducted in the United Kingdom; volumeand type of fluid administered were amongthe topics of the questionnaire. The re-sponses were widely dispersed among the118 surgeons who returned the question-naires. Only 37% specified the amount offluid used, and the type of fluid variedamong saline, aqueous Betadine®, water,and antibiotic lavage. The results of thissurvey suggest that guidelines are lackingfor the use of IOPL.11
Metabolic ManagementThe timing and method of postoperativefeeding in patients with cIAIs may havean impact on clinical outcomes. In ratmodels, immediate feeding after colon re-section and anastomosis, preceded by ce-cal ligation and puncture (CLP) to inducefecal peritonitis, was associated withhigher anastomotic bursting pressurethan delayed feeding.12 Also, histopatho-logic examination showed more collagendeposition in the early-fed group, whichrepresents enhanced healing, potentiallyreducing the risk of suture dehiscence.Paradoxically, in another animal study inwhich rats with severe intra-abdominalsepsis resulting from CLP received eitherTPN (via a central line) or enteral feed-ing (via a gastrostomy tube), survivalrates were significantly higher in theTPN group.13 Moreover, muscle and he-patic anabolic functions were augment-ed in the TPN group.
Selection of the proper anestheticagent may prevent dysfunction of hepaticand renal physiology after septic peri-tonitis. The use of isoflurane, a volatileanesthetic, was documented to reducemortality in mice that had undergoneCLP. Also, proinflammatory cytokinelevels and renal cortical apoptosis weredecreased in mice receiving isofluranecompared with those receiving pento-barbital anesthesia.14
Resuscitation TechniquesA state of functional hypovolemia and,consequently, hypotension may resultfrom third-space fluid sequestration,which occurs because of paralytic ileuscaused by the infectious process.15 Thissituation needs to be managed in a time-ly manner because of the possibility ofmultisystem failure and death. Therefore,restoration of the intravascular volumevia intravenous (IV) fluid infusion is es-sential. Regular monitoring and themaintenance of normal heart rate andblood pressure help ensure adequate per-fusion and oxygenation of all body tis-sues.1 Additionally, measuring urineoutput is a simple yet very beneficialmeans to determine renal blood flow, in-travascular volume, and physiology ofother organs. An acceptable rate of urineoutput is 0.5 to 1 mL/kg/h.1
Various types of IV fluid were tested
in a study in which fecal peritonitis wasinduced in female sheep. Su et al evalu-ated the difference between Ringer’s lac-tate alone or combined with either al-bumin or hydroxyethyl starch (HES), orgelatin alone.16 Both albumin and HESwere associated with improved strokevolume, cardiac index, and oxygen de-livery (P<0.05); however, the type of flu-id used did not influence survival.
In addition to IV fluids, norepineph-rine (NE) is considered the standard ofcare in cases in which mean arterial pres-sure (MAP) needs to be restored. Levyand colleagues examined the efficacy andhemodynamic effects of NE comparedwith vasopressin (AVP) and L-canavanine(LC) in a rat model of endotoxic shock.17
All agents were able to restore MAP andinhibit endotoxin-induced gut hyper-permeability. Pulmonary hyperperme-ability was reduced by LC and increasedby NE. Only AVP and LC acted to pre-serve glomerular function (P<0.05);however, AVP was more effective in in-creasing renal blood flow.17
Conclusion Patients with cIAIs remain a surgicalchallenge because of high rates of mor-bidity and mortality. The treatmentprinciples for patients with cIAIs are pa-tient stabilization, source control, andproper antimicrobial selection. Impor-tantly, other adjunctive measures canplay an important role in optimizingoutcomes in certain clinical conditions.The practice of active observation is rea-sonable in equivocal cases of acute ap-pendicitis. In cases of contaminated ab-dominal wounds, DPC decreases woundinfection rates compared with PC. Theuse of laparoscopy by experienced sur-geons is safe in patients with cIAIs.Peritoneal drainage and irrigational de-bridement yield good results in cases ofNEC and infected pancreatic necrosis, re-spectively. However, the role of IOPLstill requires further study. Early feedingdoes seem to improve anastomoticstrength, but in cases of severe sepsis, pa-tients should not be fed enterally. Thetypes of anesthetic and pressor agents,and the type of IV fluid infused, mayhave an impact on clinical parameters,but all require further research. ■
Comprehensive Management of Patients With Complicated Intra-Abdominal Infections 5
Continued on page 11

6 Comprehensive Management of Patients With Complicated Intra-Abdominal Infections
GUIDELINES FOR ANTIMICROBIAL TREATMENT OFCOMPLICATED INTRA-ABDOMINAL INFECTIONS
JOHN E. MAZUSKI, MD, PHD, FACS
Definitions and MicrobiologyIntra-abdominal infections (IAIs) are dueto multiplication of pathogenic mi-croorganisms within normally sterile re-gions of the abdomen, such as theperitoneal cavity.1 Complicated intra-abdominal infections (cIAIs) are thosetreated with some type of source control,such as an operative procedure or percu-taneous drainage. Most commonly, IAIspresent clinically as peritonitis or an in-tra-abdominal abscess.2
Peritonitis can be classified as prima-ry, secondary, or tertiary. Primary peri-tonitis (spontaneous bacterial peritoni-tis) is most commonly encountered inpatients with ascites, especially thosewith hepatic cirrhosis. Usually, this typeof peritonitis is managed medically. Sec-ondary peritonitis is a polymicrobial in-fection resulting from disruption of theanatomical integrity of the gastroin-testinal tract or an extension of an in-fection originating in an intra-abdomi-nal structure. The mainstay of therapyfor secondary peritonitis is source con-trol and appropriate antimicrobial ther-apy.3 The most common organisms ob-served are aerobic Enterobacteriaceae,especially Escherichia coli, and obligateanaerobes, such as Bacteroides fragilis.4
Recurrent infections that fail to clear de-spite adequate source control and an-timicrobial therapy are described as ter-tiary peritonitis; this condition isassociated with substantial morbidityand mortality.3,5 The microbial agentsthat cause tertiary peritonitis differ fromthose associated with secondary peri-tonitis, and tend to be resistant to first-line antibiotics. Organisms that may beisolated from patients with tertiary peri-tonitis include resistant gram-negativeorganisms, Candida, enterococci (occa-sionally vancomycin-resistant), and β-lactam–resistant staphylococci.3,5-7
It is important to consider the dis-parate microbial etiologies of commu-nity-acquired and health care–associat-ed IAIs when selecting antimicrobial
therapy.4 Roehrborn and colleagues doc-umented this important difference in aprospective study of 68 patients withcommunity-acquired cIAI and 67 pa-tients with health care–associated cIAIs.The most commonly identified mi-croorganism in patients with commu-nity-acquired cIAIs was E. coli. In pa-tients with postoperative cIAIs, thisorganism was isolated less often, where-as Enterobacter and Pseudomonas were iso-lated more frequently. Enterococci andstaphylococci were also more commonin the patients with health care–associ-ated cIAIs.8
Principles of Antimicrobial TherapySource control is fundamental to themanagement of cIAIs, and should be ac-companied by appropriate resuscitativeefforts to stabilize the patient. Antimi-crobial therapy is used as an adjunct tosource control.5 Except under very lim-ited circumstances, such as treatment ofacute diverticulitis, antimicrobial thera-py alone is not a substitute for source con-trol. The goals of antimicrobial treatmentare to eliminate pathogenic microorgan-isms remaining after source control,thereby reducing the risk of recurrence,and to control microorganisms dissemi-nated during that procedure.9
The choice of empiric therapy is close-ly linked to treatment success. Krobotand colleagues studied the results of ini-tial empiric therapy in 425 patientswith community-acquired cIAIs.10
Based on the susceptibilities of the or-ganisms eventually isolated, the select-ed therapeutic regimen was deemed tobe appropriate or inappropriate. Thestudy found that nearly 80% of patientswho received an appropriate antimicro-bial regimen were successfully treated,whereas 47% of the patients receiving aninappropriate therapy failed initial ther-apy. Infection with resistant gram-neg-ative organisms, particularly E. coli, ac-counted for many of the treatmentfailures. In this study, there was no dif-
ference in mortality between patients re-ceiving appropriate or inappropriatetherapy.10 However, a pronounced effecton mortality was observed in a study of100 patients with postoperative cIAIswho were more severely ill.11 Inadequateempiric therapy, which did not cover allof the organisms eventually isolated, re-sulted in a mortality rate of 50%, where-as patients treated with an adequateregimen had a mortality rate of 26%(relative risk of inadequate therapy, 1.9).
Antimicrobial Therapy forLower-Risk PatientsMany antimicrobial agents are availablefor use in patients with cIAIs. At aminimum, an antimicrobial regimenneeds to be effective against the com-mon aerobic gram-negative and anaer-obic organisms found in these infec-tions. Guidelines developed by theSurgical Infection Society (SIS) and theInfectious Diseases Society of America(IDSA) have recommended various sin-gle-agent and combination regimensfor patients with different levels of dis-ease severity (Table).6,9
One drug combination previously rec-ommended by the SIS for the treatmentof patients with cIAIs is an aminoglyco-side in conjunction with an antianaero-bic agent. However, in addition to beingototoxic and nephrotoxic, aminoglyco-sides have been shown in a meta-analy-sis of prospective, randomized, controlledtrials to be less efficacious than variousother agents such as carbapenems,cephalosporins, and extended-spectrumpenicillin/β-lactamase inhibitor combi-nations.12 As a result, aminoglycoside-based regimens are no longer advocatedas first-line treatments for cIAIs.12 Like-wise, because of the widespread emer-gence of resistant strains of E. coli world-wide, the use of ampicillin/sulbactam hasbeen called into question. Although thisdrug combination had been recom-mended by both the SIS and the IDSAfor the management of cIAIs, a recentstudy found that approximately 45% of

E. coli isolates were resistant to ampi-cillin/sulbactam.13 Moreover, unlikemost other agents, this drug combina-tion was not superior to aminoglycoside-based therapy in the above-mentionedmeta-analysis.12
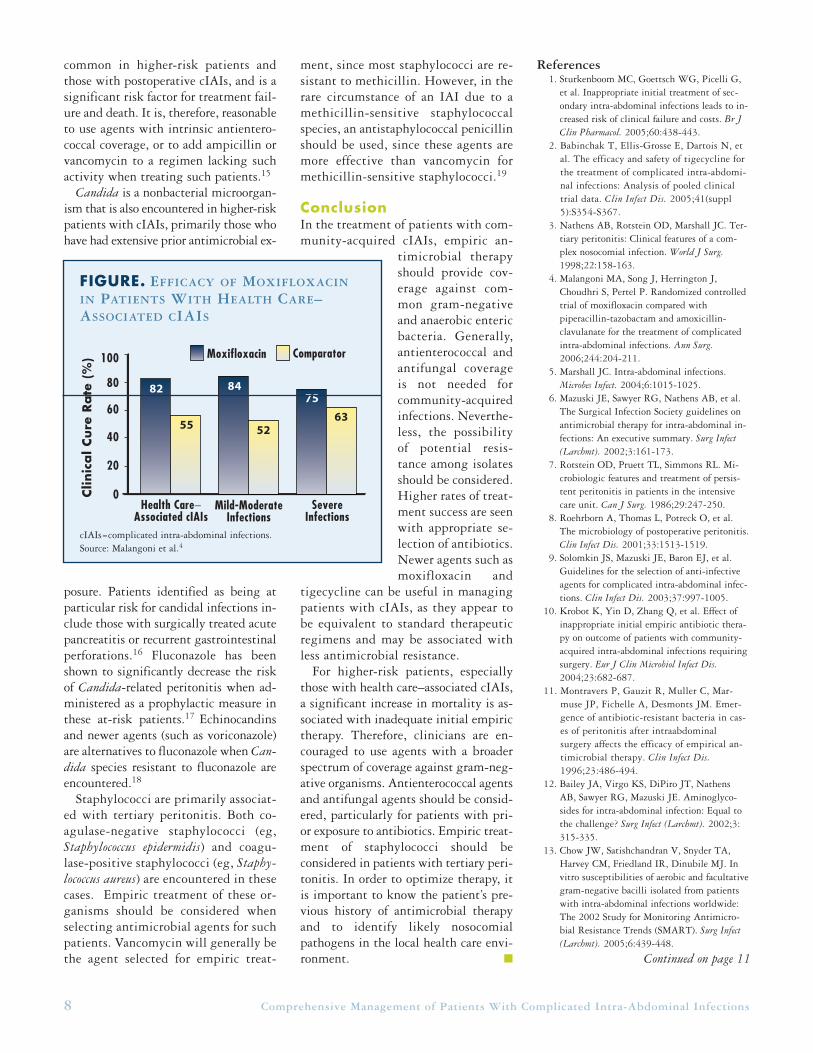
Because of emerging bacterial resis-tance, there is a need for additional an-timicrobial agents for the managementof cIAIs.4 An agent recently approvedby the US Food and Drug Administra-tion (FDA) for cIAIs is moxifloxacin, afluoroquinolone with a broad spectrumof activity against aerobic and anaero-bic bacteria. Moxifloxacin has beenstudied as monotherapy in a prospec-tive, randomized, double-blind, multi-center clinical trial in patients withcIAIs.4 Sequential intravenous (IV) tooral once-daily dosing of moxifloxacinwas shown to be safe, well tolerated(particularly in the elderly), and as ef-
ficacious as a standard multidose regi-men of IV piperacillin/tazobactam fol-lowed by oral amoxicillin/clavulanicacid. The overall clinical cure rate was80% with moxifloxacin compared to78% with the comparator. Moxifloxacintreatment demonstrated significantlyhigher cure rates in patients with healthcare–associated cIAI of varying severi-ty (Figure on page 7) than did thecomparator.4
Tigecycline is another relatively newantimicrobial agent recently approved bythe FDA for the treatment of patientswith cIAIs. Babinchak et al analyzedpooled clinical trial data comparing IVtigecycline administered twice daily for5 to 14 days (after one bolus dose) to IVimipenem/cilastatin given four times perday.2 Their analysis showed that both an-timicrobial regimens were efficaciousand well tolerated in patients with cIAIs.
The clinical cure rates were almost iden-tical in the two groups (86.1% and86.2%, respectively).2
Management of Higher-Risk Patients Because so few antimicrobial clinical tri-als have included higher-risk patientswith cIAIs, data are lacking to supportwell-defined treatment guidelines forthis population. At the present time,most recommendations concerning an-timicrobial therapy for higher-risk pa-tients are based on expert opinion.
Several factors are associated with ahigher risk for treatment failure or deathdue to cIAI. The majority of these fac-tors relate to the patient's underlyingclinical characteristics, such as advancedage, medical comorbidities, hypoalbu-minemia, or poor nutritional status.6
The Acute Physiology and ChronicHealth Evaluation II (APACHE II) score,which reflects the acute physiologic de-rangements produced by an illness aswell as the patient’s age and chronichealth problems, is the most repro-ducible independent predictor of treat-ment failure and death in patients withcIAIs. It represents a useful tool for riskstratification. Many studies have con-cluded that an APACHE II score >10represents serious illness.14
The magnitude of the infection is alsoa marker of higher risk. The patient witha localized infection has a lower risk fortreatment failure than does the patientwith diffuse peritonitis; the former pa-tient also has a much lower risk for sep-ticemia or septic shock.6 In addition, itis important to know a patient’s past his-tory of antimicrobial use and the iden-tity and resistance patterns of likelynosocomial pathogens when choosing anempiric antimicrobial regimen for ahigher-risk patient with cIAI. Empiricantimicrobial agents with extended-spec-trum coverage against gram-negative or-ganisms and anaerobes have been rec-ommended by the SIS and the IDSA foruse in these patients.6
Resistant microorganisms, especiallythose encountered in cases of healthcare–associated cIAI and tertiary peri-tonitis, have been linked to higher treat-ment failure rates and increased mortal-ity.14 Isolation of Enterococcus is more
Comprehensive Management of Patients With Complicated Intra-Abdominal Infections 7
TABLE. AGENTS RECOMMENDED BY THE SIS AND THE
IDSA FOR TREATMENT OF PATIENTS WITH CIAIS
SIS-Recommended SIS-RecommendedSingle-Agent Regimens Combination RegimensAmpicillin/sulbactama Aminoglycosidea (gentamicin, Cefotetanb tobramycin, netilmicin, amikacin)
plus antianaerobe (clindamycin or metronidazole)
Cefoxitinc Cefuroximec plus metronidazoleErtapenemc Third-/fourth-generation Imipenem/cilastatin cephalosporin (cefotaxime,
ceftriaxone, ceftizoxime,b
ceftazidime, cefepime) plus antianaerobe
Meropenem Aztreonam plus clindamycinPiperacillin/tazobactam Ciprofloxacin plus metronidazole Ticarcillin/clavulanic acidc
Mild to Moderate Infections High-Severity InfectionsIDSA-recommended single-agent regimensc
• Ampicillin/sulbactama • Piperacillin/tazobactam• Ticarcillin/clavulanic acid • Imipenem/cilastatin• Ertapenem • Meropenem
IDSA-recommended combination regimensc
• Cefazolin or cefuroxime + • Cefotaxime, ceftriaxone, metronidazole ceftizoxime, ceftazidime, cefepime +
• Ciprofloxacin, levofloxacin, metronidazolemoxifloxacin, gatifloxacinb + • Aztreonam + metronidazolemetronidazole • Ciprofloxacin + metronidazole
aBased on newer data, these agents are no longer recommended as first-line therapy for cIAIs.bThis agent is not currently available in the United States.cRecommended for use in lower-risk patients with community-acquired infections.cIAIs=complicated intra-abdominal infections; SIS=Surgical Infection Society; IDSA=Infectious Diseases Society of America.Reproduced with permission from Mary Ann Liebert, Inc.,6 and the University of Chicago Press.9
common in higher-risk patients andthose with postoperative cIAIs, and is asignificant risk factor for treatment fail-ure and death. It is, therefore, reasonableto use agents with intrinsic antientero-coccal coverage, or to add ampicillin orvancomycin to a regimen lacking suchactivity when treating such patients.15
Candida is a nonbacterial microorgan-ism that is also encountered in higher-riskpatients with cIAIs, primarily those whohave had extensive prior antimicrobial ex-
posure. Patients identified as being atparticular risk for candidal infections in-clude those with surgically treated acutepancreatitis or recurrent gastrointestinalperforations.16 Fluconazole has beenshown to significantly decrease the riskof Candida-related peritonitis when ad-ministered as a prophylactic measure inthese at-risk patients.17 Echinocandinsand newer agents (such as voriconazole)are alternatives to fluconazole when Can-dida species resistant to fluconazole areencountered.18
Staphylococci are primarily associat-ed with tertiary peritonitis. Both co-agulase-negative staphylococci (eg,Staphylococcus epidermidis) and coagu-lase-positive staphylococci (eg, Staphy-lococcus aureus) are encountered in thesecases. Empiric treatment of these or-ganisms should be considered whenselecting antimicrobial agents for suchpatients. Vancomycin will generally bethe agent selected for empiric treat-
ment, since most staphylococci are re-sistant to methicillin. However, in therare circumstance of an IAI due to amethicillin-sensitive staphylococcalspecies, an antistaphylococcal penicillinshould be used, since these agents aremore effective than vancomycin formethicillin-sensitive staphylococci.19
ConclusionIn the treatment of patients with com-munity-acquired cIAIs, empiric an-
timicrobial therapyshould provide cov-erage against com-mon gram-negativeand anaerobic entericbacteria. Generally,antienterococcal andantifungal coverageis not needed forcommunity-acquiredinfections. Neverthe-less, the possibilityof potential resis-tance among isolatesshould be considered.Higher rates of treat-ment success are seenwith appropriate se-lection of antibiotics.Newer agents such asmoxifloxacin and
tigecycline can be useful in managingpatients with cIAIs, as they appear tobe equivalent to standard therapeuticregimens and may be associated withless antimicrobial resistance.
For higher-risk patients, especiallythose with health care–associated cIAIs,a significant increase in mortality is as-sociated with inadequate initial empirictherapy. Therefore, clinicians are en-couraged to use agents with a broaderspectrum of coverage against gram-neg-ative organisms. Antienterococcal agentsand antifungal agents should be consid-ered, particularly for patients with pri-or exposure to antibiotics. Empiric treat-ment of staphylococci should beconsidered in patients with tertiary peri-tonitis. In order to optimize therapy, itis important to know the patient’s pre-vious history of antimicrobial therapyand to identify likely nosocomialpathogens in the local health care envi-ronment. ■
References1. Sturkenboom MC, Goettsch WG, Picelli G,
et al. Inappropriate initial treatment of sec-ondary intra-abdominal infections leads to in-creased risk of clinical failure and costs. Br JClin Pharmacol. 2005;60:438-443.
2. Babinchak T, Ellis-Grosse E, Dartois N, etal. The efficacy and safety of tigecycline forthe treatment of complicated intra-abdomi-nal infections: Analysis of pooled clinicaltrial data. Clin Infect Dis. 2005;41(suppl5):S354-S367.
3. Nathens AB, Rotstein OD, Marshall JC. Ter-tiary peritonitis: Clinical features of a com-plex nosocomial infection. World J Surg.1998;22:158-163.
4. Malangoni MA, Song J, Herrington J,Choudhri S, Pertel P. Randomized controlledtrial of moxifloxacin compared withpiperacillin-tazobactam and amoxicillin-clavulanate for the treatment of complicatedintra-abdominal infections. Ann Surg.2006;244:204-211.
5. Marshall JC. Intra-abdominal infections. Microbes Infect. 2004;6:1015-1025.
6. Mazuski JE, Sawyer RG, Nathens AB, et al.The Surgical Infection Society guidelines onantimicrobial therapy for intra-abdominal in-fections: An executive summary. Surg Infect(Larchmt). 2002;3:161-173.
7. Rotstein OD, Pruett TL, Simmons RL. Mi-crobiologic features and treatment of persis-tent peritonitis in patients in the intensivecare unit. Can J Surg. 1986;29:247-250.
8. Roehrborn A, Thomas L, Potreck O, et al.The microbiology of postoperative peritonitis.Clin Infect Dis. 2001;33:1513-1519.
9. Solomkin JS, Mazuski JE, Baron EJ, et al.Guidelines for the selection of anti-infectiveagents for complicated intra-abdominal infec-tions. Clin Infect Dis. 2003;37:997-1005.
10. Krobot K, Yin D, Zhang Q, et al. Effect ofinappropriate initial empiric antibiotic thera-py on outcome of patients with community-acquired intra-abdominal infections requiringsurgery. Eur J Clin Microbiol Infect Dis.2004;23:682-687.
11. Montravers P, Gauzit R, Muller C, Mar-muse JP, Fichelle A, Desmonts JM. Emer-gence of antibiotic-resistant bacteria in cas-es of peritonitis after intraabdominalsurgery affects the efficacy of empirical an-timicrobial therapy. Clin Infect Dis.1996;23:486-494.
12. Bailey JA, Virgo KS, DiPiro JT, NathensAB, Sawyer RG, Mazuski JE. Aminoglyco-sides for intra-abdominal infection: Equal tothe challenge? Surg Infect (Larchmt). 2002;3:315-335.
13. Chow JW, Satishchandran V, Snyder TA,Harvey CM, Friedland IR, Dinubile MJ. Invitro susceptibilities of aerobic and facultativegram-negative bacilli isolated from patientswith intra-abdominal infections worldwide:The 2002 Study for Monitoring Antimicro-bial Resistance Trends (SMART). Surg Infect(Larchmt). 2005;6:439-448.
8 Comprehensive Management of Patients With Complicated Intra-Abdominal Infections
Continued on page 11
Moxifloxacin Comparator
Health Care−Associated cIAIs
Mild-ModerateInfections
SevereInfections
Clin
ica
l Cure
Ra
te (
%) 100
80
60
40
20
0
82 8475
55 5263
FIGURE. EFFICACY OF MOXIFLOXACIN
IN PATIENTS WITH HEALTH CARE–ASSOCIATED CIAIS
cIAIs=complicated intra-abdominal infections. Source: Malangoni et al.4

DefinitionDespite comprehensive management,treatment success rates in patients withcomplicated intra-abdominal infections(cIAIs) are not reaching desired levels.1,2
The occurrence of unintended damage,injuries, or even death during the man-agement of patients with cIAIs has beentermed “collateral damage” and con-tributes to treatment failure in many cas-es. Noninfectious causes of such types ofcomplications include wound dehiscence,open abdomen, fistula formation, and or-gan failure. Infectious complications canoccur at the primary site of infection, inthe form of persistence or recurrence ofthe original infection, or as a de novo in-fection at a distant anatomic location.
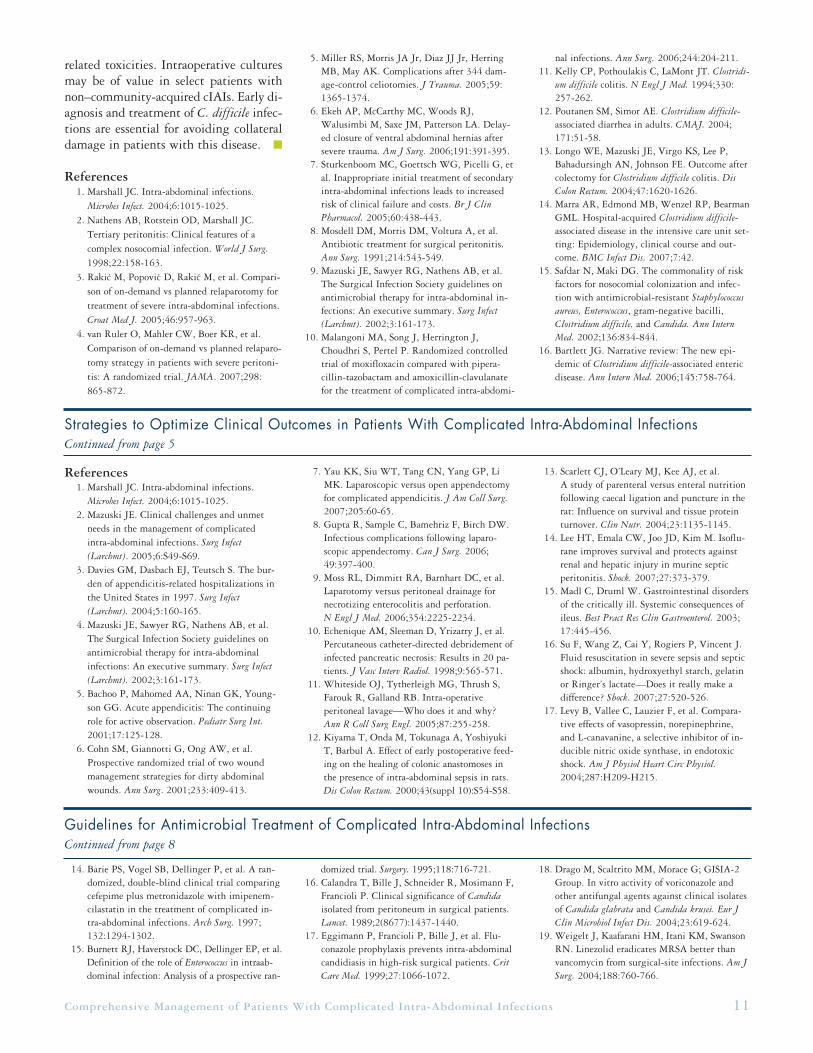
Noninfectious Complications Severely ill patients with cIAIs who un-dergo emergency laparotomies may re-quire relaparotomy aimed at eradicatinga persistent infection.3,4 Of the twomethods for performing relaparotomy,the on-demand method is used only inpatients who are unresponsive to treat-ment or whose condition is deteriorating.In the planned relaparotomy strategy, pa-tients are reevaluated every other day, re-gardless of their clinical condition, byperforming regular inspection, drainage,and peritoneal lavage of the abdominalcavity, until findings of ongoing infec-tion are negative.4 To compare the effi-cacy and safety of the two strategies, vanRuler and colleagues randomized 232patients with a confirmed diagnosis of se-vere secondary peritonitis and an AcutePhysiology and Chronic Health Evalua-tion II (APACHE II) score of >10 to on-demand or planned relaparotomy.4 Therewas no difference in morbidity or mor-tality rates between the two groups (Fig-ure).4 However, the on-demand treat-ment strategy was associated with greaterreductions in consumption of health careresources and shorter median intensive
care unit stays and hospital stays, withconsequently lower medical costs.
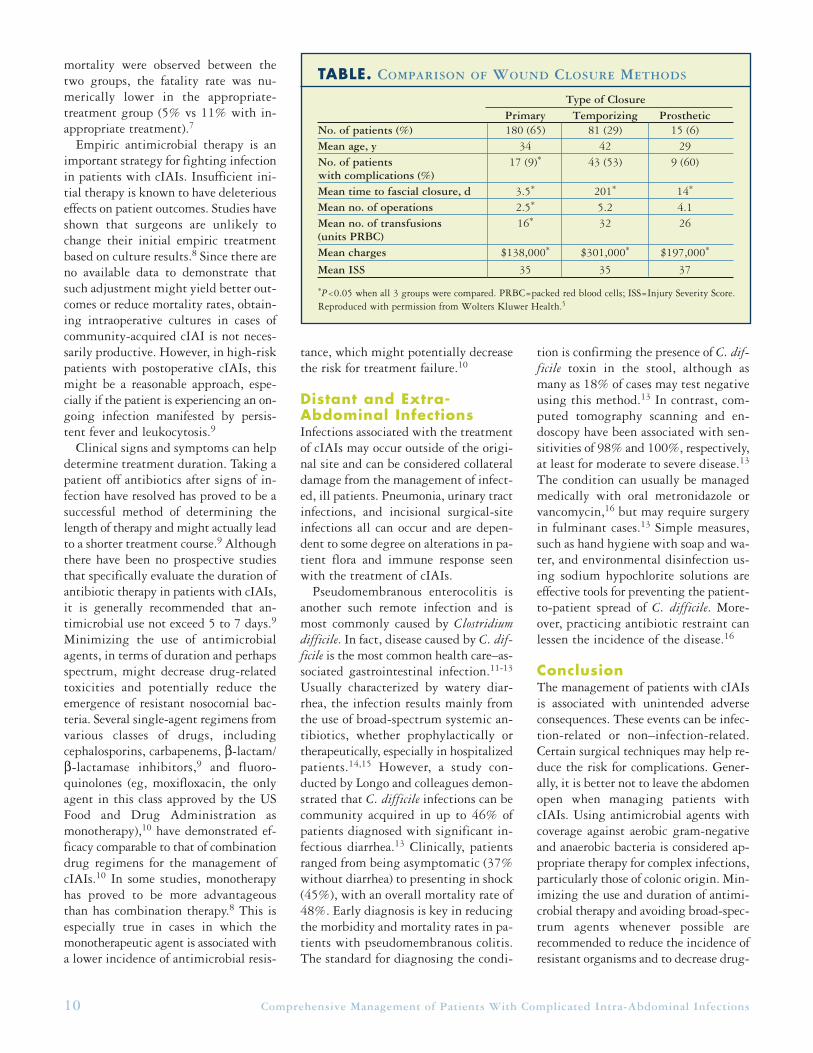
Leaving the abdomen open throughthe process of decompression can be alife-saving technique in patients with ab-dominal compartment syndrome, butsurgeons then have to contend with theassociated high morbidity due to woundcomplications (25%) and the challengeof deciding which wound closure methodto use.5 Miller and associates conducteda retrospective analysis over an 8-year pe-riod of 344 patients with an open ab-domen to evaluate various methods ofwound closure.5 Only 276 patients sur-vived until wound closure and receivedeither primary, temporizing, or pros-thetic closures. The results tended to fa-vor primary closure of the abdomen(Table on page 10).5
In a prospective study, data were col-lected from 84 patients undergoing dam-age-control celiotomies.6 Of the 53 pa-tients who survived, 20 underwentclosure during subsequent hospitaliza-tion (mean time to delayed closure, 193
days). The rate of complications in thatgroup was 45%, including six surgicalsite infections, two enterocutaneous fis-tulae, and two incisional hernias.6
Unresponsiveness or Resistance to TreatmentTreatment failure in patients with cIAIscan be attributed to inadequate sourcecontrol or inadequate antimicrobial cov-erage resulting from insufficient spec-trum, which is potentially due to thepresence of resistant organisms. The ap-propriateness of antibiotic therapy inpatients with cIAIs was the subject of aretrospective study by Sturkenboom andcolleagues that identified 175 patientswho received antimicrobial therapy.7 Ap-propriate treatment, which covered aer-obic gram-negative and anaerobic bac-teria, was administered in approximately84% of patients. Treatment failure rateswere 36% in the group treated inappro-priately versus 14% in the group treat-ed with appropriate therapy (P=0.004).Although no significant differences in
Comprehensive Management of Patients With Complicated Intra-Abdominal Infections 9
PREVENTING COLLATERAL DAMAGE IN THE MANAGEMENT OF PATIENTS WITH COMPLICATED INTRA-ABDOMINAL
INFECTIONS
ROBERT G. SAWYER, MD, FACS
100908070605040302010
00 60 120 180 240 300 360
Surv
iva
l (%
)
Days
On-DemandPlanned Log-rank P=0.33
FIGURE. PLANNED VS ON-DEMAND RELAPAROTOMY
No. at riskOn-Demand 111 88 87 84 83 82 80Planned 112 92 82 80 78 77 72
Source: van Ruler et al, JAMA Aug 22/29, 2007, vol. 298, p. 871. ©2007, American Medical Association. Reproduced with permission.
mortality were observed between thetwo groups, the fatality rate was nu-merically lower in the appropriate-treatment group (5% vs 11% with in-appropriate treatment).7
Empiric antimicrobial therapy is animportant strategy for fighting infectionin patients with cIAIs. Insufficient ini-tial therapy is known to have deleteriouseffects on patient outcomes. Studies haveshown that surgeons are unlikely tochange their initial empiric treatmentbased on culture results.8 Since there areno available data to demonstrate thatsuch adjustment might yield better out-comes or reduce mortality rates, obtain-ing intraoperative cultures in cases ofcommunity-acquired cIAI is not neces-sarily productive. However, in high-riskpatients with postoperative cIAIs, thismight be a reasonable approach, espe-cially if the patient is experiencing an on-going infection manifested by persis-tent fever and leukocytosis.9
Clinical signs and symptoms can helpdetermine treatment duration. Taking apatient off antibiotics after signs of in-fection have resolved has proved to be asuccessful method of determining thelength of therapy and might actually leadto a shorter treatment course.9 Althoughthere have been no prospective studiesthat specifically evaluate the duration ofantibiotic therapy in patients with cIAIs,it is generally recommended that an-timicrobial use not exceed 5 to 7 days.9
Minimizing the use of antimicrobialagents, in terms of duration and perhapsspectrum, might decrease drug-relatedtoxicities and potentially reduce theemergence of resistant nosocomial bac-teria. Several single-agent regimens fromvarious classes of drugs, includingcephalosporins, carbapenems, β-lactam/β-lactamase inhibitors,9 and fluoro-quinolones (eg, moxifloxacin, the onlyagent in this class approved by the USFood and Drug Administration asmonotherapy),10 have demonstrated ef-ficacy comparable to that of combinationdrug regimens for the management ofcIAIs.10 In some studies, monotherapyhas proved to be more advantageousthan has combination therapy.8 This isespecially true in cases in which themonotherapeutic agent is associated witha lower incidence of antimicrobial resis-
tance, which might potentially decreasethe risk for treatment failure.10
Distant and Extra-Abdominal InfectionsInfections associated with the treatmentof cIAIs may occur outside of the origi-nal site and can be considered collateraldamage from the management of infect-ed, ill patients. Pneumonia, urinary tractinfections, and incisional surgical-siteinfections all can occur and are depen-dent to some degree on alterations in pa-tient flora and immune response seenwith the treatment of cIAIs.
Pseudomembranous enterocolitis isanother such remote infection and ismost commonly caused by Clostridiumdifficile. In fact, disease caused by C. dif-ficile is the most common health care–as-sociated gastrointestinal infection.11-13
Usually characterized by watery diar-rhea, the infection results mainly fromthe use of broad-spectrum systemic an-tibiotics, whether prophylactically ortherapeutically, especially in hospitalizedpatients.14,15 However, a study con-ducted by Longo and colleagues demon-strated that C. difficile infections can becommunity acquired in up to 46% ofpatients diagnosed with significant in-fectious diarrhea.13 Clinically, patientsranged from being asymptomatic (37%without diarrhea) to presenting in shock(45%), with an overall mortality rate of48%. Early diagnosis is key in reducingthe morbidity and mortality rates in pa-tients with pseudomembranous colitis.The standard for diagnosing the condi-
tion is confirming the presence of C. dif-ficile toxin in the stool, although asmany as 18% of cases may test negativeusing this method.13 In contrast, com-puted tomography scanning and en-doscopy have been associated with sen-sitivities of 98% and 100%, respectively,at least for moderate to severe disease.13
The condition can usually be managedmedically with oral metronidazole orvancomycin,16 but may require surgeryin fulminant cases.13 Simple measures,such as hand hygiene with soap and wa-ter, and environmental disinfection us-ing sodium hypochlorite solutions areeffective tools for preventing the patient-to-patient spread of C. difficile. More-over, practicing antibiotic restraint canlessen the incidence of the disease.16
ConclusionThe management of patients with cIAIsis associated with unintended adverseconsequences. These events can be infec-tion-related or non–infection-related.Certain surgical techniques may help re-duce the risk for complications. Gener-ally, it is better not to leave the abdomenopen when managing patients withcIAIs. Using antimicrobial agents withcoverage against aerobic gram-negativeand anaerobic bacteria is considered ap-propriate therapy for complex infections,particularly those of colonic origin. Min-imizing the use and duration of antimi-crobial therapy and avoiding broad-spec-trum agents whenever possible arerecommended to reduce the incidence ofresistant organisms and to decrease drug-
10 Comprehensive Management of Patients With Complicated Intra-Abdominal Infections
TABLE. COMPARISON OF WOUND CLOSURE METHODS
Primary Temporizing ProstheticNo. of patients (%) 180 (65) 81 (29) 15 (6)Mean age, y 34 42 29No. of patients 17 (9)* 43 (53) 9 (60)with complications (%)Mean time to fascial closure, d 3.5* 201* 14*
Mean no. of operations 2.5* 5.2 4.1Mean no. of transfusions 16* 32 26(units PRBC)Mean charges $138,000* $301,000* $197,000*
Mean ISS 35 35 37
*P<0.05 when all 3 groups were compared. PRBC=packed red blood cells; ISS=Injury Severity Score.Reproduced with permission from Wolters Kluwer Health.5
Type of Closure
Comprehensive Management of Patients With Complicated Intra-Abdominal Infections 11
References1. Marshall JC. Intra-abdominal infections.
Microbes Infect. 2004;6:1015-1025.2. Mazuski JE. Clinical challenges and unmet
needs in the management of complicated intra-abdominal infections. Surg Infect(Larchmt). 2005;6:S49-S69.
3. Davies GM, Dasbach EJ, Teutsch S. The bur-den of appendicitis-related hospitalizations inthe United States in 1997. Surg Infect(Larchmt). 2004;5:160-165.
4. Mazuski JE, Sawyer RG, Nathens AB, et al.The Surgical Infection Society guidelines onantimicrobial therapy for intra-abdominal infections: An executive summary. Surg Infect(Larchmt). 2002;3:161-173.
5. Bachoo P, Mahomed AA, Ninan GK, Young-son GG. Acute appendicitis: The continuingrole for active observation. Pediatr Surg Int.2001;17:125-128.
6. Cohn SM, Giannotti G, Ong AW, et al.Prospective randomized trial of two woundmanagement strategies for dirty abdominalwounds. Ann Surg. 2001;233:409-413.
7. Yau KK, Siu WT, Tang CN, Yang GP, LiMK. Laparoscopic versus open appendectomyfor complicated appendicitis. J Am Coll Surg.2007;205:60-65.
8. Gupta R, Sample C, Bamehriz F, Birch DW.Infectious complications following laparo-scopic appendectomy. Can J Surg. 2006;49:397-400.
9. Moss RL, Dimmitt RA, Barnhart DC, et al.Laparotomy versus peritoneal drainage fornecrotizing enterocolitis and perforation. N Engl J Med. 2006;354:2225-2234.
10. Echenique AM, Sleeman D, Yrizarry J, et al.Percutaneous catheter-directed debridement ofinfected pancreatic necrosis: Results in 20 pa-tients. J Vasc Interv Radiol. 1998;9:565-571.
11. Whiteside OJ, Tytherleigh MG, Thrush S,Farouk R, Galland RB. Intra-operative peritoneal lavage—Who does it and why? Ann R Coll Surg Engl. 2005;87:255-258.
12. Kiyama T, Onda M, Tokunaga A, YoshiyukiT, Barbul A. Effect of early postoperative feed-ing on the healing of colonic anastomoses inthe presence of intra-abdominal sepsis in rats.Dis Colon Rectum. 2000;43(suppl 10):S54-S58.
13. Scarlett CJ, O’Leary MJ, Kee AJ, et al. A study of parenteral versus enteral nutritionfollowing caecal ligation and puncture in therat: Influence on survival and tissue proteinturnover. Clin Nutr. 2004;23:1135-1145.
14. Lee HT, Emala CW, Joo JD, Kim M. Isoflu-rane improves survival and protects againstrenal and hepatic injury in murine septicperitonitis. Shock. 2007;27:373-379.
15. Madl C, Druml W. Gastrointestinal disordersof the critically ill. Systemic consequences ofileus. Best Pract Res Clin Gastroenterol. 2003;17:445-456.
16. Su F, Wang Z, Cai Y, Rogiers P, Vincent J.Fluid resuscitation in severe sepsis and septicshock: albumin, hydroxyethyl starch, gelatinor Ringer’s lactate—Does it really make adifference? Shock. 2007;27:520-526.
17. Levy B, Vallee C, Lauzier F, et al. Compara-tive effects of vasopressin, norepinephrine,and L-canavanine, a selective inhibitor of in-ducible nitric oxide synthase, in endotoxicshock. Am J Physiol Heart Circ Physiol.2004;287:H209-H215.
14. Barie PS, Vogel SB, Dellinger P, et al. A ran-domized, double-blind clinical trial comparingcefepime plus metronidazole with imipenem-cilastatin in the treatment of complicated in-tra-abdominal infections. Arch Surg. 1997;132:1294-1302.
15. Burnett RJ, Haverstock DC, Dellinger EP, et al.Definition of the role of Enterococcus in intraab-dominal infection: Analysis of a prospective ran-
domized trial. Surgery. 1995;118:716-721.16. Calandra T, Bille J, Schneider R, Mosimann F,
Francioli P. Clinical significance of Candidaisolated from peritoneum in surgical patients.Lancet. 1989;2(8677):1437-1440.
17. Eggimann P, Francioli P, Bille J, et al. Flu-conazole prophylaxis prevents intra-abdominalcandidiasis in high-risk surgical patients. CritCare Med. 1999;27:1066-1072.
18. Drago M, Scaltrito MM, Morace G; GISIA-2Group. In vitro activity of voriconazole andother antifungal agents against clinical isolatesof Candida glabrata and Candida krusei. Eur JClin Microbiol Infect Dis. 2004;23:619-624.
19. Weigelt J, Kaafarani HM, Itani KM, SwansonRN. Linezolid eradicates MRSA better thanvancomycin from surgical-site infections. Am JSurg. 2004;188:760-766.
related toxicities. Intraoperative culturesmay be of value in select patients withnon–community-acquired cIAIs. Early di-agnosis and treatment of C. difficile infec-tions are essential for avoiding collateraldamage in patients with this disease. ■
References1. Marshall JC. Intra-abdominal infections.
Microbes Infect. 2004;6:1015-1025. 2. Nathens AB, Rotstein OD, Marshall JC.
Tertiary peritonitis: Clinical features of a complex nosocomial infection. World J Surg.1998;22:158-163.
3. Rakic M, Popovic D, Rakic M, et al. Compari-son of on-demand vs planned relaparotomy fortreatment of severe intra-abdominal infections.Croat Med J. 2005;46:957-963.
4. van Ruler O, Mahler CW, Boer KR, et al.Comparison of on-demand vs planned relaparo-tomy strategy in patients with severe peritoni-tis: A randomized trial. JAMA. 2007;298:865-872.
5. Miller RS, Morris JA Jr, Diaz JJ Jr, HerringMB, May AK. Complications after 344 dam-age-control celiotomies. J Trauma. 2005;59:1365-1374.
6. Ekeh AP, McCarthy MC, Woods RJ,Walusimbi M, Saxe JM, Patterson LA. Delay-ed closure of ventral abdominal hernias aftersevere trauma. Am J Surg. 2006;191:391-395.
7. Sturkenboom MC, Goettsch WG, Picelli G, etal. Inappropriate initial treatment of secondaryintra-abdominal infections leads to increasedrisk of clinical failure and costs. Br J ClinPharmacol. 2005;60:438-443.
8. Mosdell DM, Morris DM, Voltura A, et al.Antibiotic treatment for surgical peritonitis.Ann Surg. 1991;214:543-549.
9. Mazuski JE, Sawyer RG, Nathens AB, et al.The Surgical Infection Society guidelines onantimicrobial therapy for intra-abdominal in-fections: An executive summary. Surg Infect(Larchmt). 2002;3:161-173.
10. Malangoni MA, Song J, Herrington J,Choudhri S, Pertel P. Randomized controlledtrial of moxifloxacin compared with pipera-cillin-tazobactam and amoxicillin-clavulanatefor the treatment of complicated intra-abdomi-
nal infections. Ann Surg. 2006;244:204-211.11. Kelly CP, Pothoulakis C, LaMont JT. Clostridi-
um difficile colitis. N Engl J Med. 1994;330:257-262.
12. Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ. 2004;171:51-58.
13. Longo WE, Mazuski JE, Virgo KS, Lee P, Bahadursingh AN, Johnson FE. Outcome aftercolectomy for Clostridium difficile colitis. DisColon Rectum. 2004;47:1620-1626.
14. Marra AR, Edmond MB, Wenzel RP, BearmanGML. Hospital-acquired Clostridium difficile-associated disease in the intensive care unit set-ting: Epidemiology, clinical course and out-come. BMC Infect Dis. 2007;7:42.
15. Safdar N, Maki DG. The commonality of riskfactors for nosocomial colonization and infec-tion with antimicrobial-resistant Staphylococcusaureus, Enterococcus, gram-negative bacilli,Clostridium difficile, and Candida. Ann InternMed. 2002;136:834-844.
16. Bartlett JG. Narrative review: The new epi-demic of Clostridium difficile-associated entericdisease. Ann Intern Med. 2006;145:758-764.
Strategies to Optimize Clinical Outcomes in Patients With Complicated Intra-Abdominal InfectionsContinued from page 5
Guidelines for Antimicrobial Treatment of Complicated Intra-Abdominal InfectionsContinued from page 8
′ ′ ′

To obtain CME credit:
1. Review the activity2. Go to http://cmecredit.cerebrio.com
3. Select the activity “Comprehensive Management of Patients With Complicated Intra-Abdominal Infections”
4. Complete the post-test
A score of 70% or higher on the post-test will award physicians with1.5 AMA PRA Category 1 Credit(s)TM.