-
8/6/2019 Anaesthetics Booklet
1/23
Coliste na hOllscoile Corcaigh
University College Cork
MED3/GM2 CLERKSHIP
IN
ANAESTHESIA & INTENSIVE CARE MEDICINE
AT
UNIVERSITY COLLEGE CORK MEDICAL SCHOOL
2010/11
1
-
8/6/2019 Anaesthetics Booklet
2/23
DEPARTMENT OF ANAESTHESIA & INTENSIVE CARE
MEDICINE
Med3/GM2 Medical Students
Module CP3002
Background
The anaesthetic/ICU component of module CP3002 will comprise two
elements.
TERM 1
During Term 1 (Sept. to Dec.) it is proposed that students will
attend the Operating
Theatres of either Cork University Hospital, South
Infirmary/Victoria University
Hospital, Bon Secours Hospital or Mercy University Hospital on
Tuesday,
Wednesday and Thursday mornings over a two week period. This is
designed to
complement the intensive course on clinical skills offered
during September.
Since this module is timed to occur at the introduction to the
clinical curriculum, it is
appropriate and timely to expose students to the basics of
clinical and practical skills,
BLS (Basic Life Support) and Resuscitation. Teaching of the
theoretical concepts can
be followed by the demonstration and practice of skills in the
Clinical Skills
Laboratory. Here students can develop and practise skills in a
non-clinical
environment. The theoretical knowledge will then be reinforced
and the clinical
skills demonstrated and applied in a clinical setting during the
three weeks in the
hospital component of the module.
2
-
8/6/2019 Anaesthetics Booklet
3/23
Because the work of anaesthetists straddles a number of clinical
areas in a hospital
setting eg perioperative care, intensive care, acute and chronic
pain management it is
hoped that students will be exposed to some or all of these
areas during the two week
component of the clerkship.
------------------------
TERM 2
In Term 2, students will attend the Department of
Anaesthesia/Intensive Care of a
designated Acute Teaching hospital for one full week attachment.
This will
comprise one of a four week surgical clinical attachment.
During that week students will be exposed to:
a) Further small group teaching in a theatre setting.
b) Principles/practice of preoperative Anaesthetic Evaluation of
patients.
c) Patient care in post operative recovery room.
d) Have two tutorials (airway management, resuscitation).
-------------------------
Educational Objectives
3
-
8/6/2019 Anaesthetics Booklet
4/23
1 To enable the student to understand the roles of the
anaesthetist within
a hospital setting.
2 To enable the student to learn how to assess a patient for
anaesthesia
and surgery.
3 To enable students to gain a basic understanding of induction,
maintenance
and emergence from anaesthesia, including intraoperative
monitoring and
post operative care.
4 To allow students to observe and understand the principles of
fluid and
electrolyte management intra and post operatively.
5 To enable students to observe and understand the principles of
pain
assessment and management.
6 To learn the principles and practice of Cardiopulmonary
Resuscitation.
7 To learn the theory and gain practical experience in airway
management,
bag and mask ventilation, LMA insertion, ETT intubation and IV
access.
4
-
8/6/2019 Anaesthetics Booklet
5/23
Clerkship Content
The content of this clerkship can be divided into three
areas:
1 Theory
2 Demonstration and practice of clinical and practical
skills.
3 Assessment/Evaluation
Theory
Theoretical concepts will be taught both at tutorial sessions
(at least two during the
three week hospital attendance) and on a one to one level in the
Operating
Theatres.
Clinical /Practical Skills
Clinical skills such as history taking, preoperative patient
assessment, patient
examination, interpretation of ECGs and Chest Xrays will be
demonstrated and
discussed.
Practical Skills
CPR, airway management, bag/mask ventilation, intravenous
access, LMA/ETT
insertion will be demonstrated and practised.
Management of specific situations
e.g. Choking
Drowning
Smoke inhalation
Burns
Electrocution
Drug overdose
Severe haemorrhage
Multiple InjuriesHead/Spinal Injuries.
5
-
8/6/2019 Anaesthetics Booklet
6/23
Assessment/Evaluation
In keeping with other clinical rotations anaesthesia assessment
will be a part of
written/skill based assessment at end of year examinations
(EMQ/OSCE).
Students are required to submit an essay following completion of
clerkship
(which accounts for 30% of anaesthesia clerkship marks). See
Gaffney Prize,
page 22.
Students will be asked to give an anonymous evaluation of the
Anaesthesia clerkship
at the end of Term 2 attachment.
Recommended Reading:
How To Survive In Anaesthesia. Neville Robinson and George Hall,
2nd Edition.
6
-
8/6/2019 Anaesthetics Booklet
7/23
Core Topics
Below are listed a number of core topics under various headings.
These are simply
guidelines for both students and teachers. It allows teachers to
cover what we regard
as important areas in this clerkship and it allows students to
ensure that different
topics are covered on different days in Theatre/ICU. It also
gives students headings
underwhich questions may be asked of their teachers.
Knowledge and understanding:
Roles of anaesthetist
Patient assessment
Induction, maintenance, emergence
Post operative care
Monitoring
Fluid management
Electrolytes
ICU ABGs, shock, CCF, respiratory failure, ventilation
Anaphylaxis
Clinical Skills:
Pre-operative assessment
History taking
Examination CVS, respiratory, head and neck
CXR
ECG
7
-
8/6/2019 Anaesthetics Booklet
8/23
Technical Skills:
CPR
I.V. insertion
B-V-M ventilation
(LMA, ET tube insertion)
Attitudes
Standards of care
Vigilance
Appropriate behaviour to staff and patients
Problem Solving:
Simple anaesthetic plan
Management of clinical scenarios e.g. hypoxia, hypotension
etc.
----------------------
8
-
8/6/2019 Anaesthetics Booklet
9/23
FOR CUH STUDENTS ONLY
Theatre Assignments
Students Numbered 1 12
Week 1 of Term 1
Th.1/1a Th. 2 Th.3 Th.4 Th. 5 Th.6 Th.7 Th.8 Th. 9
Tuesday 1/12 2/11 3 5/6 7 8 9 10 4
Wednesday 10 5 8/9 1/2 4 6/7 3 12 11
Thursday 4/7 12/6 10 9/4 3/11 5 8 2 1
Week 2 of Term 1
Tuesday 5/6 8/9 7 3/10 1 2 4 11 12
Wednesday 3 10 5/6 7/8 2 11 12/4 1 9
Thursday 8/9 1/4 11 10 5/12 9 6/7 3 2
FOR CUH STUDENTS ONLY
Theatre Assignments
Term 2
9
-
8/6/2019 Anaesthetics Booklet
10/23
-
8/6/2019 Anaesthetics Booklet
11/23
Manual ventilation (facemask/airway)
LMA Insertion
ETT Insertion
IV Insertion
Other e.g. Arterial Line
MED 111 ANAESTHESIA AND INTENSIVE CARE CLERKSHIP
COURSE EVALUATION FORM
Please rate the content of each of the core topics listed below
as inadequate, adequate
or good by ticking the appropriate box.
Core Topic Inadequate Adequate Good
ResuscitationAirway Management
Perioperative Patient Monitoring
Applied Pharmacology
Applied Physiology
Procedural Skills
Please rate the importance and relevance to practice of each of
the core topics
listed below as very important, fairly important or not
important by ticking the
appropriate box.
Core Topic Very Fairly Important Not Important
11
-
8/6/2019 Anaesthetics Booklet
12/23
Important
Resuscitation
Airway Management
Perioperative Patient Monitoring
Applied Pharmacology
Applied PhysiologyIntensive Care Medicine
Procedural Skills
Any other comments
ERC Guidelines for Resuscitation 2005
Summary
Main changes in adult basic life support
The decision to start CPR is made if a victim is unresponsive
and notbreathing normally.
Rescuers should be taught to place their hands on the centre of
thechest, rather than to spend more time using the rib margin
method.
Each rescue breath is given over 1 sec rather than 2 sec.
The ratio of compressions to ventilations is 30:2 for all adult
victims ofcardiac arrest. This same ratio should also be used for
children whenattended by a lay rescuer.
For an adult victim, the 2 initial rescue breaths are omitted,
with 30compressions being given immediately after cardiac arrest
isestablished.
Main changes in automated external defibrillation
Public access defibrillation (PAD) programmes are recommended
forlocations where the expected use of an AED for witnessed
cardiacarrest exceeds once in two years.
A single defibrillatory shock (at least 150J biphasic or
360Jmonophasic) is delivered, immediately followed by two minutes
of
uninterrupted CPR, without a check for termination of VF or a
check forsigns of life or a pulse.
Main changes in adult advanced life supportCPR before
defibrillation
In out-of-hospital cardiac arrest attended, but unwitnessed,
byhealthcare professionals equipped with manual defibrillators,
give CPRfor 2 min (i.e. about 5 cycles at 30:2) before
defibrillation.
Do not delay defibrillation if an out-of-hospital arrest is
witnessed by ahealthcare professional.
Do not delay defibrillation for in-hospital cardiac arrest.
Defibrillation strategy
12
-
8/6/2019 Anaesthetics Booklet
13/23
-
8/6/2019 Anaesthetics Booklet
14/23
Unconscious adult patients, with spontaneous circulation, after
out-of-hospital VF cardiac arrest should be cooled to 32-34C for
12-24 h.
Mild hypothermia may also benefit unconscious adult patients,
withspontaneous circulation, after out-of-hospital cardiac arrest
from a non-shockable rhythm or after cardiac arrest in
hospital.
Main changes in paediatric life support
Paediatric basic life support
Lay rescuers or lone rescuers witnessing or attending
paediatriccardiac arrest will use a ratio of 30 compressions to 2
ventilations.They will start with 5 rescue breaths and continue
with the 30:2 ratio astaught in adult BLS.
Two or more rescuers with a duty to respond will use the 15:2
ratio in achild up to the onset of puberty. It is inappropriate and
unnecessary to
establish the onset of puberty formally; if the rescuer believes
thevictim to be a child then they should use the paediatric
guidelines.
In an infant (less than 1 year) the compression technique
remains thesame: two-finger compression for single rescuers and
two-thumbencircling technique for two or more rescuers. Above one
year of age,there is no division between one- or two-hand
technique. The one ortwo hands technique may be used according to
rescuer preference.
AED may be used in children above one year of age. Attenuators
of theelectrical output are recommended between 1 and 8 years of
age.
For foreign body airway obstruction relief, in an unconscious
child orinfant, attempt five rescue breaths and in the absence of
response,proceed to chest compressions without further assessment
of thecirculation.
Paediatric advanced life support
The Layngeal Mask Airway is an acceptable initial airway device
forproviders experienced in its use. In hospital, a cuffed tracheal
tube maybe useful in certain circumstances, e.g. in cases of poor
lungcompliance, high airway resistance or large glottic air
leak.The cuffinflation pressure should be monitored regularly and
must remain
below 20 cm H2O .
14
-
8/6/2019 Anaesthetics Booklet
15/23
Hyperventilation is harmful during cardiac arrest. The ideal
tidal volumeshould achieve modest chest wall rise.
When using a manual defibrillator, a dose of 4 J kg-1 (biphasic
ormonophasic waveform) should be used for the first and
subsequentshocks.
Asystole, pulseless electrical activity (PEA)
Adrenaline IV or IO should be given at the dose of 10 mcg kg-1
andrepeated every 3-5min. If no vascular access is available and
atracheal tube is in-situ, adrenaline may be given at the dose of
100mcg kg-1 via this route until IV/IO access is obtained
Defibrillation strategy
Ventricular fibrillation/pulseless ventricular tachycardia
(VF/VT) shouldbe treated with a single shock, followed by immediate
resumption of
CPR (15 compressions to 2 ventilations). Do not reassess the
rhythmor feel for a pulse. After 2 min of CPR, check the rhythm and
giveanother shock (if indicated).
Give adrenaline 10 mcg kg-1 IV if VF/VT persists after a second
shock.
Repeat adrenaline every 3-5 min thereafter if VF/VT
persists.
Temperature control
After cardiac arrest, treat fever aggressively.
A child who regains a spontaneous circulation but remains
comatoseafter cardiac arrest may benefit from being cooled to a
coretemperature of 32-34C for 12-24 h. After a period of mild
hypothermia,
the child should be rewarmed slowly at 0.25-0.5C h-1.
Resuscitation of the newborn
Protect the newborm from heat loss. Premature babies should
becovered with plastic wrapping on head and body (apart from the
face),without drying the baby beforehand. The baby so covered
should thenbe placed under radiant heat
Ventilation: an initial inflation for 2-3 seconds must be given
for the firstfew breaths to help lung expansion
Trachal route for adrenaline is not recommended. If the tracheal
route
must be used, a dose of 100 mcg kg-1 must be used. Suctioning
meconium from the babys nose and mouth before delivery
of the babys chest (intrapartum suctioning) is not useful and no
longerrecommended.
Standard resuscitation in delivery room should be made with
100%oxygen. However lower concentrations are acceptable.
15
-
8/6/2019 Anaesthetics Booklet
16/23
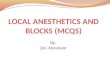
Figure 2.1 Adult basic life support algorithm.
16
-
8/6/2019 Anaesthetics Booklet
17/23
Figure 2.20 Algorithm for use of an automated external
defibrillator.
17
-
8/6/2019 Anaesthetics Booklet
18/23
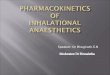
Figure 4.1 Algorithm for the treatment of in-hospital cardiac
arrest.
18
-
8/6/2019 Anaesthetics Booklet
19/23
Figure 4.2 Advanced life support cardiac arrest algorithm.
19
-
8/6/2019 Anaesthetics Booklet
20/23
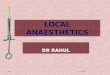
Figure 6.1 Paediatric basic life support algorithm.
20
-
8/6/2019 Anaesthetics Booklet
21/23
THE GAFFNEY PRIZE
An undergraduate prize in Anaesthesia and Intensive Care
Medicine has been
established in honour of Dr. Desmond Gaffney, former Chairman,
Department of
Anaesthesia, Cork University Hospital. A prize of 1000.00 will
be awarded
annually for the best essay (1500 2000 words) on a topic
relevant to the practice
of anaesthesia and/or intensive care medicine from registered
medical undergraduates
at UCC. Submission of essays is mandatory for all Med3/GM2
students. The
successful applicant will be invited to present on the subject
of their
essay at the following South of Ireland Anaesthetists
Association Annual Scientific
Meeting.
The subject matter of the essay will relate to the clinical
practice of Anaesthesia or
Intensive Care Medicine. Basic physiological or pharmacological
topics can be
discussed, but only in so far as they relate to clinical
practice. Candidates are
encouraged to select topics which are current and/or
controversial. Submissions,
which include the application of new information (either
recently published or
collected by the submitting student) or original ideas to
well-established problems, are
encouraged.
Marks will be awarded according to the following criteria:
Content (50%),
Presentation (20%), Originality (15%), Clinical Significance
(15%). Students should
note that Originality may mean the presentation of an argument
in favour or against
a proposed idea OR the presentation of original data collected
by the submitting
student. Marks will also be awarded for attempts to demonstrate
an understanding
of a topic rather than a recycling or assembly of previously
published material.
21
-
8/6/2019 Anaesthetics Booklet
22/23
White A4 paper should be used with margins of at least 2.5 cms
(1 inch), double-
spacing should be used throughout. All pages should be numbered
consecutively,
beginning with the title page.
The title page should not include the authors name. A maximum of
20 references are
permitted. The essay should be accompanied by a cover letter
stating the title of the
article and the name, address, telephone number, student number
and medical class
year of the author.
---------------
N.B. Students to submit their essays within four weeks of
completion of their
Anaesthetic clerkship.
Essays to be submitted to the designated Gaffney Essay
assignment
box in the Assessment area of Blackboard. (CP3002 / GM2004)
22
-
8/6/2019 Anaesthetics Booklet
23/23
NOTES: