Embed Size (px)
Citation preview

Anaesthetic Event Anaesthetic Event Database Report April Database Report April
20072007
R. MarcusR. Marcus
Birmingham Children’s Birmingham Children’s HospitalHospital

Incident reporting at BCHIncident reporting at BCH
1569 reports from 5 years1569 reports from 5 years Databased and CategorisedDatabased and Categorised
– ClassificationClassification– SubclassificationSubclassification– Anaesthetic human factorsAnaesthetic human factors
Nomenclature developed from reports Nomenclature developed from reports and previous publicationsand previous publications
715 human factors in 674 715 human factors in 674 reportsreports– 43% of incidents reported43% of incidents reported

Event classificationEvent classification totaltotal preventablepreventable
Airway/RespiratoryAirway/Respiratory 708708 54.8%54.8%
CVSCVS 235235 17.9%17.9%
EquipmentEquipment 217217 72.4%72.4%
OrganizationOrganization 9999 93.9%93.9%
OtherOther 4949 57.1%57.1%
PharmacologyPharmacology 9797 62.9%62.9%
ProcedureProcedure 8888 43.2%43.2%

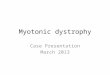
Immediate outcomesImmediate outcomes
42
240
728
519
28
0
100
200
300
400
500
600
700
800
cardiac arrest major change minor change nil other

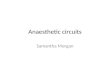
Predicted long term outcomesPredicted long term outcomes
21 5
93 105
1333
0
100
200
300
400
500
600
700
800
death permanent major short minor nil

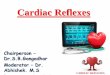
Human factors pie chartHuman factors pie chart
failure to check (iv device)
3%
inad depth GA15%
inattention4%
extubated at wrong time9%
drug slip2%
URTI8%
teaching2%
skill (cvl)4%
skill (la block)2%
skill (iv/ia access)1%
pressure to do0%
skill (airway)3%
other error of judgement
5%
poor choice5%
other1%
lack of care9%
inexperience (may be of trainee)
6%
failure to check (equipment)
6%
failure to check (drug/other)
2%
failure to check (airway)
5%
communication4%
poor pre op prep/assess
4%

Errors of Judgement 303 (42.4%)Errors of Judgement 303 (42.4%)
Inadequate depth of Inadequate depth of anaesthesiaanaesthesia
119 (16.6%)119 (16.6%)
Trachea extubated at wrong Trachea extubated at wrong timetime
61 (8.5%)61 (8.5%)
Anaesthetizing child with Anaesthetizing child with URTIURTI
59 (8.3%)59 (8.3%)
Other error of judgmentOther error of judgment 33 (4.6%)33 (4.6%)
Inadvisable anaesthetic Inadvisable anaesthetic techniquetechnique
31 (4.3%)31 (4.3%)

Failure to Check 105 (14.2%)Failure to Check 105 (14.2%)
EquipmentEquipment 46 (6.4%)46 (6.4%)
Tracheal tubeTracheal tube 28 (3.9%)28 (3.9%)
Intravenous/arterial lineIntravenous/arterial line 23 (3.2%)23 (3.2%)
Drug/otherDrug/other 8 (1.1%)8 (1.1%)

Failures of Skills 72 (10.1%)Failures of Skills 72 (10.1%)
Central venous accessCentral venous access 27 (3.8%)27 (3.8%)
AirwayAirway 17 (2.4%)17 (2.4%)
Local Block/EpiduralLocal Block/Epidural 14 (2%)14 (2%)
Intravenous/arterial lineIntravenous/arterial line 14 (2%)14 (2%)

Lack of careLack of care 65 (9.1%)65 (9.1%)
Inexperience Inexperience (may be of attached (may be of attached trainee)trainee)
51 (7.1%)51 (7.1%)
InattentionInattention 31 (4.3%)31 (4.3%)
Poor pre-operative Poor pre-operative preparation/assessmentpreparation/assessment
31 (4.3%)31 (4.3%)
CommunicationCommunication 25 (3.5%)25 (3.5%)
TeachingTeaching 15 (2.1%)15 (2.1%)
Drug dosage slipDrug dosage slip 12 (1.7%)12 (1.7%)
OtherOther 10 (1.4%)10 (1.4%)
Pressure to do casePressure to do case 2 (0.3%)2 (0.3%)

The 6 most common causative factors in this
study and the AIMS study For ease of comparison the fault of technique category (13%) in the AIMS study has been
included in the errors of judgment to match the classification used in this study.
THIS STUDY AIMS STUDYCAUSATIVE FACTOR % of
incidentsCAUSATIVE FACTOR % of
incidents
Error of judgment 42.4% Error of judgment* 29%
Failure to check 14.2% Failure to check equipment
13%
Technical failure of skill 10.1% Others 13%
Lack of care 9.1% Inattention 12%
Inexperience 7.1% Haste 12%
Inattention 4.3% Inexperience 11%

Yearly incidents reported by each ConsultantYearly incidents reported by each Consultant
0
5
10
15
20
25
30
35

Overall incident typesOverall incident types
Pharmacology6%
Organization7%
Other3%
Equipment15%
CVS16%
Procedure6%
Airway/Respiratory47%

Example of GeneralistExample of Generalist
Other3%
Procedure10%Pharmacology
9%
Organization7%
Equipment10%
CVS14%
Airway/Respiratory47%

Example of Cardiac AnaesthetistExample of Cardiac Anaesthetist
Airway/Respiratory37%
CVS37%
Organization2%
Equipment10%
Other6%
Pharmacology4% Procedure
4%

Example of someone who reports many Problems Example of someone who reports many Problems with organization/equipmentwith organization/equipment
CVS10%
Organization36%
Equipment19%
Airway/Respiratory21%
Procedure6%
Other6%
Pharmacology2%

Overall human factorsOverall human factors
0
10
20
30
40
50
60
70
80
90
100
communication
drug slip
extubated at wrong timefailure to check (airway)
failure to check (drug/other)failure to check (equipment)failure to check (iv device)
inad depth GA
inattention
inexperience (may be of trainee)
lack of care
other
other error of judgement
poor choice
poor pre op prep/assess
pressure to doskill (airway)
skill (cvl)
skill (iv/ia access)
skill (la block)
teaching
URTI

Individual 1Individual 1
0
2
4
6
8
10
12
communication
drug slip
extubated at wrong timefailure to check (airway)
failure to check (drug/other)failure to check (equipment)failure to check (iv device)
inad depth GA
inattention
inexperience (may be of trainee)
lack of care
other
other error of judgement
poor choice
poor pre op prep/assess
pressure to doskill (airway)
skill (cvl)
skill (iv/ia access)
skill (la block)
teaching
URTI

Individual 2Individual 2
0
1
2
3
4
5
6
7
8
9
10
11
12
communication
drug slip
extubated at wrong timefailure to check (airway)
failure to check (drug/other)failure to check (equipment)failure to check (iv device)
inad depth GA
inattention
inexperience (may be of trainee)
lack of care
other
other error of judgement
poor choice
poor pre op prep/assess
pressure to doskill (airway)
skill (cvl)
skill (iv/ia access)
skill (la block)
teaching
URTI

Individual 3Individual 3
0
2
4
6
8
10
12
communication
drug slip
extubated at wrong timefailure to check (airway)
failure to check (drug/other)failure to check (equipment)failure to check (iv device)
inad depth GA
inattention
inexperience (may be of trainee)
lack of care
other
other error of judgement
poor choice
poor pre op prep/assess
pressure to doskill (airway)
skill (cvl)
skill (iv/ia access)
skill (la block)
teaching
URTI

Individual 4Individual 4
0
2
4
6
8
10
12
communication
drug slip
extubated at wrong timefailure to check (airway)
failure to check (drug/other)failure to check (equipment)failure to check (iv device)
inad depth GA
inattention
inexperience (may be of trainee)
lack of care
other
other error of judgement
poor choice
poor pre op prep/assess
pressure to doskill (airway)
skill (cvl)
skill (iv/ia access)
skill (la block)
teaching
URTI

Reporting rates varyReporting rates vary Median 10 (IQR 6.6-15) a yearMedian 10 (IQR 6.6-15) a year Range 0.2 to 35 per yearRange 0.2 to 35 per year What is acceptable range?What is acceptable range?
– Too manyToo many is that anaesthetist unsafe?is that anaesthetist unsafe? or do they under report less?or do they under report less?
– Everyone under reports!Everyone under reports!
– Too fewToo few are they super-safe? are they super-safe? or just avoiding reporting?or just avoiding reporting?
– And hence a risk!And hence a risk! Voluntary reportingVoluntary reporting

Different patterns of reportingDifferent patterns of reporting
We are variableWe are variable– Caseload Caseload
CardiacCardiacLiversLiversNeuroNeuro
– Bees in our bonnets over certain Bees in our bonnets over certain issuesissues
Portex LMAsPortex LMAsCommunicationCommunicationOrganizationOrganization
– NO definite list of triggers for a NO definite list of triggers for a reportreport

Patterns of human errorPatterns of human error
Patterns do vary between Patterns do vary between individualsindividuals– How valid are comparisons?How valid are comparisons?
Reporting habits varyReporting habits varyStill after 5 years small numbers for Still after 5 years small numbers for most individual so percentages can be most individual so percentages can be misleadingmisleading
Overall reporting rates vary, so plain Overall reporting rates vary, so plain numbers can be misleading alsonumbers can be misleading also
– All interpretation of incidents are All interpretation of incidents are by me, so may be wrong by me, so may be wrong

Pros and cons of collecting dataPros and cons of collecting data
PROSPROS– Education of selfEducation of self– Education of othersEducation of others– Evidence for Evidence for revalidationrevalidation
Proof of cooperation Proof of cooperation with reportingwith reporting
Learning from errorsLearning from errors
– Defence if a SUI Defence if a SUI occursoccurs
– PublicationPublication Department profileDepartment profile
CONSCONS– Could be used Could be used against youagainst you
High reporting ratesHigh reporting rates SUISUI Lack of Lack of understanding by understanding by othersothers
– Trial by press?Trial by press? May be disclosable May be disclosable under FOI actunder FOI act
Trust may not Trust may not release individuals release individuals data on a whimdata on a whim

ISSUES & QUESTIONSISSUES & QUESTIONS
Missed some people’s data due to Missed some people’s data due to changeover to electronic versionchangeover to electronic version
Has been retrospective (3+ months or Has been retrospective (3+ months or so), will become more up to date so), will become more up to date with electronic systemwith electronic system
My interpretation…open to questionMy interpretation…open to question Is it useful in its mechanisms of Is it useful in its mechanisms of feedback?feedback?

CONCLUSIONSCONCLUSIONS
– Confidential? Voluntary Confidential? Voluntary – Variable reporting ratesVariable reporting rates– Interpretation by me as to factorsInterpretation by me as to factors– Feedback of overall and individual dataFeedback of overall and individual data– Do act on issues that are raisedDo act on issues that are raised
– PumpsPumps– LMAsLMAs– Drug errorsDrug errors
– How do we ensure that it cannot be How do we ensure that it cannot be misinterpreted by those outside misinterpreted by those outside anaesthesia?anaesthesia?