Embed Size (px)
Citation preview

The Opioid Epidemic: Practice, Policy, and
Legislative Overview
Sharon A. Morgan
MSN, RN, NP-C
Senior Policy Advisor
October 21, 2017
IntNSA
2
Objectives• Where are we today and how did we get here?
• Definitions
• Chronic Pain
• Poor Pain Management & Barriers to Effective Care
• National Pain Strategy
• Prescribers as Gatekeepers
• Removing Treatment Barriers
• SUD in Nursing
3
Where Are We Today?
(newea.org)
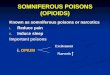
• 91 Americans die every day from an opioid overdose
• At least half of all opioid overdoses involved a prescribed medicine
• Sales of prescription opioids in the U.S. nearly quadrupled from 1999 to 2014, but the overall amount of pain Americans report has not changed
• In 2014, an estimated 1.9 million people had an opioid use disorder related to prescription pain relievers and an estimated 586,000 had an opioid use disorder related to heroin use.
• Men were more likely to die from overdose, but the mortality gap between men and women is closing
• Heroin-related overdose deaths have more than tripled since 2010
(CDC, 2016; SAMSHA, 2015)
4
Heroin Use
5
The Interplay
(newea.org)
6
Definitions
• Use: Taking a substance as prescribed
• Misuse:
• Using a substance for a purpose other than
intended reason
• Taking a substance not prescribed to
oneself
• Abuse: Taking a substance for a pleasant or
euphoric feeling
• Avenues for misuse and abuse
• Crushing, chewing, grinding solids
• Injecting
• Insufflating (nasal)
• Smoking(FDA, 2010; 2016)
ANA Stock Photo

7
Definitions
(newea.org)
• Tolerance: Reduced response to a drug with repeated use
• Physical dependence: Adaptation to a drug that produces symptoms of withdrawal when the drug is stopped
• Addiction: A chronic, relapsing brain disease that is characterized by compulsive drug seeking and use, despite harmful consequences
• Substance Use Disorder: occurs when the recurrent use of alcohol and/or drugs causes significant clinical and functional impairment, such as health problems, disability, and failure to meet major responsibilities at work, school, or home
• Withdrawal: symptoms that occur after long-term use of a drug is reduced or stopped abruptly
• Restlessness
• Muscle and bone pain
• Insomnia
• Diarrhea
• Vomiting
• Cold flashes(CDC, 2016; FDA, 2016)
8
How Did We Get Here• 3400 BC: Sumerians
• Cultivated the opium poppy— “Hul Gil” “Joy Plant”
• Assyrians����Egyptians����Alexander the Great����India����Asia
• 220 AD forward:
• Chinese surgeon Hua To documented use of opium and cannabis
extracts to minimize pain
• Substances used for pleasure and spiritual purposes
• Silk Road: series of interconnected routes that ran from Europe to
China
• 1800’s:
• Morphine extracted from opium
• Opium Wars; US expansion����Chinese labor����opium dens
• Opium marketed freely, best pain treatment option during the
Civil War
• Late 1800's 2/3 of those with opioid addiction were middle and
upper class women, due to over-prescribing the drugs for “female
troubles.”
(Atlantic, nd; BPM, 2014; DEA,nd)
olddesignshop.com
9
How Did We Get Here• Late 19th/early 20th century
• Bayer develops heroin, marketed as cough
elixir—made illegal 1924
• Legislation enacted to curb use of opiates
• 1916: Oxycodone synthesized
• Most clinicians during 20th century acknowledged
addictive risk when using opioids to treat chronic
pain
• Late 20th century
• Oxycodone (Percocet® or Percodan®)
increases in popularity
• 1960’s: Vietnam War�heroin resurgence
• 1970’s: pain is not being controlled
• 1990’s: Oxycontin approved
• Video "I Got My Life Back"
• TJC: “Pain is assessed in all patients”(BPM, 2014; CNN, 2016; TJC, 2016)
deamuseum.org

10
Recipe for Epidemic?
(newea.org)
11
A Growing Epidemic of Pain
• IOM Report, 2011
• Pain is a warning sign
• Subjective, unique
• Complex
• Biological: factors that affect pain tolerance
or thresholds
• Psychological: pain represents something
worse than it does
• Social: response of significant others to the
pain
• Types
• Acute:
• Sudden onset, short duration
• Recurrent: episodic
• Chronic:
• Lasting > several months
• Maladaptive, debilitating(IOM, 2011)
12
Chronic Pain by the Numbers
• 100 million—approximate number of U.S. adults with common chronic pain
conditions
• $560 to 635 billion—conservative estimate of the annual cost of chronic
pain in America
• $99 billion—2008 cost to federal and state governments of medical
expenditures for pain
• 10 to 50 percent of patients with postsurgical pain develop chronic pain
• 2011 survey of U.S. soldiers returned from deployment, 44 percent
reported chronic pain and 15.1 percent reported recent use of opioid pain
relievers(IOM, 2011; JAMA, 2014)

13
Poor Pain Management
(newea.org)
• How Pain Occurs Poorly Understood• The relationship between injury and pain is not
consistent• Location of pain and tissue damage are sometimes
different• Pain can persist long after tissue healing
• Nature of pain and its location can change over time• Individuals respond to a given therapy
• Variable Data Collection• Experience of pain is subjective• Few standardized, validated self-reporting tools
• Varying assessment by location• Meeting a standard vs comprehensive patient
assessment
• Clinician education varies
• Misperceptions about misuse and abuse of opioids• Comprehensive education lacking• Education does not translate to competency
(IOM, 2011)
ANA Stock Photo
14
Barriers to Effective Pain Management
• System-level barriers:
• Clinical services (and research endeavors)
organized along disease-specific lines
• Pain management belongs to everyone and
therefore, belongs to no one
• Clinical (and research) silos prevent cross-
fertilization of ideas and best practices
• Clinician-level barriers:
• Practitioners not well educated current best
practices
• Unable to ID or engage other clinicians skilled
at treating chronic pain(IOM, 2011)
ANA Stock Photo
15
Barriers to Effective Pain Management
• Patient-level barriers:
• Societal stigma
• Is the pain real?
• Drug or disability benefit–seeking behavior?
• Religious or moral judgements
• Popular culture: suck it up; no pain, no gain
• Insurance and third-party payer level barriers
• Payers do not encourage interdisciplinary team care
• Payers frequently limit reimbursement
• CAM therapies not covered(IOM, 2011)

16
National Pain Strategy
(newea.org)
• National effort of public and private organizations to transform how the nation understands and approaches pain management
• Six key areas:
• Population research
• Prevention and care
• Disparities
• Service delivery and payment
• Professional education and training
• Public education and communication
• Specifics:
• Develop metrics to improve the prevention and management of pain
• Support a system of patient-centered integrated pain management practices
• Take steps to reduce barriers to pain care; improve care for vulnerable, stigmatized and underserved populations
• Increase public awareness of pain; increase patient knowledge of treatment options and risks; help develop a better informed health care workforce
(NIH, 2016)
17
Population Research
• 2011 IOM underscored the impact of pain on the health,
productivity, and well-being of the U.S. population
• Core responsibility of public health agencies is assessing
the significance of health problems in the population
• Data collection needs to improve
• Improved data will drive federal and state initiatives
• Objectives:
• Estimate the prevalence of chronic pain and high-
impact chronic pain
• Refine and employ standardized electronic health
care data methods to determine use and costs of care
• Develop a system of metrics to track changes in
prevalence, impact, treatment, and costs(NIH, 2016)
ANA Stock Photo
18
Prevention and Care
• Preventable causes of acute and chronic pain are not
addressed throughout the health care delivery system
• People who have pain do not receive appropriate
assessments or evidence-based care that is coordinated
across providers and personalized
• Poor understanding of the factors that cause pain to
become persistent
• Objectives:
• Articulate the benefits and costs of current
prevention and treatment approaches
Develop nation-wide pain self-management
programs
Develop standardized, consistent, and
comprehensive pain assessments and outcome
measures(NIH, 2016)
arthritis.org

19
Disparities
(newea.org)
• Vulnerable/marginalized populations due to conscious and unconscious biases about higher-risk groups or about pain itself:
• English as a second language
• Race and ethnicity
• Income and education
• Sex and gender identification
• Age group
• Geographic location
• Military veterans
• Cognitive impairments
• Cancer patients
• EOL
• Objectives:
• Reduce bias and its impact on care
• Improve access to high-quality care for vulnerable groups
• Facilitate communication among patients and providers
• Highlight data on the impact of pain on high risk populations(NIH, 2016)
floridahealth.gov
20
Service Delivery and Payment
• Commonly used single-modality treatments often fail as
first-line therapies for chronic pain
• Insurance limitations affect consumer choices of
treatments and their adherence to treatment regimens
• CAM poorly covered, takes time and repeated Rx
• Providers constrained in the time they can spend with
individual patients
• Objectives:
• Define and evaluate integrated, multimodal, and
interdisciplinary pain care
• Enhance evidence for care
• Incentivize payments for quality care based on
integrated, cost-effective, and comprehensive
models(NIH, 2016)
consumerreports.org
21
Professional Education and Training
• IOM report found education key to the needed cultural
transformation to effective pain management
• Most health care professions’ education programs devote
little time to education and training about pain and pain
care
• Preventive approaches are underutilized almost
universally
• Practitioners often experience negative emotions in
caring for people with pain
• Objectives:
• Develop and update core competencies for pain care
education, licensure and certification at the
undergraduate and graduate levels
• Develop a pain education portal that contains a
comprehensive set of materials to enhance curricula(NIH, 2016)
luc.edu

22
Public Education and Communication
(newea.org)
• High-quality, evidence-based communications:
• Increase public awareness of the complexity of chronic pain
• Change cultural attitudes about chronic pain, debunking stereotypes
• Foster coalitions
• Objectives:
• Develop and implement a public awareness campaign about the impact of chronic pain to counter stigma and misperceptions
• Develop and implement an educational campaign encouraging safer medication use, especially opioid use for patients with pain
(NIH, 2016)
23
Prescribers as Gatekeepers
• Interventions to improve safe and appropriate
prescribing must balance the legitimate need for
opioids with the need to curb dangerous practices
• 2016 CDC Guideline for Prescribing Opioids for
Chronic Pain
• Articulation of National Pain Strategy
• Objectives:
• Determine when to initiate or continue
opioids for chronic pain
• Select right dosage, duration, follow-up
and discontinuation
• Assess risk and address harms of opioid
use (CDC, 2016)
ANA Stock Photo
24
Prescription Drug Monitoring Programs

25
Do PDMPs Work
• A PDMP with a mandate
(registration or use) was associated
with a 9 – 10% reduction in
prescriptions for Schedule II opioids
by Medicaid enrollees
• Issues: • PDMPs do not all collect the same
data
• It can be difficult to identify the
correct individual
• Each PDMP has a unique mandate
from the state
• Changing a PDMP to allow a change
in provider access or data sharing
may require the passage of new
legislation
26
The Science of Addiction
(newea.org)
• Drugs change the brain
• Reasons to use
• To feel good
• To feel better
• To do better
• To fit in
• How does addiction occur
• More need to just feel normal
• More needed to feel old high
(NIDA, 2014)
27
The Problem with Tough Love
• Remember, addiction includes compulsive
drug seeking and use, despite harmful
consequences
• Addiction as a chronic disease
• From quick, reactive to slow,
continuous
• Treatment in specific stages of
intervention
• Includes self-management component
• can utilize a wide range of treatments
(including medication) during each
phase(ASAM, nd)

28
Treatment Options
• Treatment Options
• Individual and group counseling
• Inpatient and residential treatment
• Intensive outpatient treatment
• Partial hospital programs
• Case or care management
• Medication
• Recovery support services and 12 Step
• Peer supports
• FDA approved medications available to treat opioid addiction
• Methadone (Dolophine®)
• Naltrexone: Oral (ReVia®, Depade®); ER injectable (Vivitrol®)
• Buprenorphine/naloxone (Suboxone®, Zubsolv®)
• Buprenorphine (Subutex®)(ASAM, nd; SAMSHA, 2016)
thefix.com
29
Removing Treatment Barriers
(newea.org)
• Addiction treatment system
• Separate from mainstream health care
• Built on infrastructure and financing models that treat addiction under an acute care model
• Public and private insurers levy prescribing restrictions against medications to treat opioid addiction
• Medication-Assisted Treatment (MAT)
• With counseling, most effective form of treatment
• Issues:
• A paucity of trained prescribers
• Negative attitudes and misunderstandings about addiction medications held by the public, providers, and patients
• Replacing one addictive medicine with another
• Need for concomitant counseling
(ANA,nd)
drugrehab.org
30
Expanding Treatment Access• Drug Addiction Treatment Act of 2000 (DATA 2000)
• Permits qualified practioners to treat opioid dependency with FDA approved
narcotic medications
• Required training and obtaining a special DEA license
• Patient limits
• Care could not be delegated
• Barriers:
• Inadequate reimbursement by insurance plans
• Detailed training and treatment protocols
• Access to referral agencies
• “Undesirable” clientele
• The Recovery Enhancement for Addiction Treatment Act (TREAT Act, S.1455)
• Revise the definition of a "qualifying practitioner" to include NPs and PAs
• Amend the Controlled Substances Act to increase the number of patients that
a qualifying practitioner can treat from 30�100
• Naloxone
• Immediate reversal of opioid
• Expand access to first responders, family, friends, and caregivers(ANA, nd)

31
SUD in Nursing
• No higher than national average�8-20% combined use/abuse
• Top 4 risks for nurses to develop SUD in the workplace
• Access
• Attitude
• Stress
• Lack of education about SUD
• Signs of SUD
• Job performance
• Personality and mental status changes
• Diversion of drugs
• ANA advocates for comprehensive and consistent access to alternative-to-
discipline programs
• All States, DC, and Territories have some form of Peer Assistance or Chemical
Dependency program(AANA, nd; ANA, nd; NCSBN, 2011)
ANA Stock Photo
32
ANA Opioid Website
http://www.nursingworld.org/MainMenuCategories/W
orkplaceSafety/Healthy-Work-Environment/Opioid-
Epidemic
33
References
(newea.org)
American Association of Nurse Anesthetists. (n.d.) AANA Peer Assistance Resource Directory. Retrieved from http://peerassistance.aana.com/directory.asp?State=All
American Nurses Association. (n.d.) The Opioid Epidemic: Addressing the Growing Drug Overdose Problem. Retrieved from http://nursingworld.org/DocumentVault/Health-Policy/Issue-Briefs/ANA-IssueBrief-Opioid-Epidemic.pdf
ANA. (n.d.) Substance Use Disorder in Nursing. In Work Environment. Retrieved from http://www.nursingworld.org/MainMenuCategories/WorkplaceSafety/Healthy-Work-Environment/Work-Environment/SubstanceUseDisorder
American Society of Addiction Medicine. (n.d.) Treating Opioid Addiction as a Chronic Disease. Retrieved from http://www.asam.org/docs/default-source/advocacy/cmm-fact-sheet---11-07-14.pdf?sfvrsn=0
The Atlantic. (nd). A Brief History of Opioids. Retrieved from http://www.theatlantic.com/sponsored/purdue-health/a-brief-history-of-opioids/184/
Better Pain Management. (2014). History of Opioid Use and Abuse. In Pain & Wellness Evaluation. Retrieved from http://testmypain.com/page5/page10/
Cable News Network. (2016, October 14). Opioid history: From 'wonder drug' to abuse epidemic. Retrieved from http://www.cnn.com/2016/05/12/health/opioid-addiction-history/
Centers for Disease Control. (2016, March 14). Guideline Information for Providers. In Injury Prevention and Control: Opioid Overdose. Retrieved from https://www.cdc.gov/drugoverdose/prescribing/providers.html
CDC. (2016, March 14). Opioid Basics. In Injury Prevention and Control: Opioid Overdose. Retrieved from https://www.cdc.gov/drugoverdose/opioids/index.html
CDC. (2016, June 21). Understanding the Epidemic. In Injury Prevention & Control: Opioid Overdose. Retrieved from https://www.cdc.gov/drugoverdose/epidemic/index.html
Drug Enforcement Administration Museum & Visitors Center. (nd). Opium Poppy: History. In Cannabis, Coca, & Poppy: Nature’s Addictive Plants. Retrieved from: https://www.deamuseum.org/ccp/opium/history.html
Institute of Medicine. (2011). Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Retrieved from https://www.nap.edu/catalog/13172/relieving-pain-in-america-a-blueprint-for-transforming-prevention-care
National Center for Biotechnology Information. (2008, October). Opioids and the Treatment of Chronic Pain: Controversies, Current Status, and Future Directions. In HHS Author Manuscripts. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2711509/#R17
National Council of State Boards of Nursing. (2011). Substance Use Disorder In Nursing. Retrieved from https://www.ncsbn.org/SUDN_11.pdf
National Institute on Drug Abuse. (2014, July). Drug Abuse and Addiction. In Drugs, Brains, and Behavior: The Science of Addiction. Retrieved from https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/drug-abuse-addiction
NIDA. (2015, August). What is withdrawal? How long does it last? In Frequently Asked Questions. Retrieved from https://www.drugabuse.gov/frequently-asked-questions#withdrawal
National Institutes of Health. (2016, March 16). National Pain Strategy. In The Interagency Pain Research Coordinating Committee. Retrieved from https://iprcc.nih.gov/National_Pain_Strategy/NPS_Main.htm
Substance Abuse and Mental Health Services Administration. (2015, October 27). Substance Use Disorders. In Mental and Substance Use Disorders. Retrieved from http://www.samhsa.gov/disorders/substance-use
SAMHSA. (2016, August 9). Treatments for Substance Use Disorders. In Behavioral Health and Treatment Services. Retrieved from http://www.samhsa.gov/treatment/substance-use-disorders
The JAMA Network. (2014, June 30). Research Letter Examines Reports of Chronic Pain, Opioid Use by U.S. Soldiers. In For the Media. Retrieved from http://media.jamanetwork.com/news-item/research-letter-examines-reports-of-chronic-pain-opioid-use-by-u-s-soldiers/
The Joint Commission. (2016, April 16). Joint Commission Statement on Pain Management. In Topic Details. Retrieved from https://www.jointcommission.org/joint_commission_statement_on_pain_management/
U.S. Food and Drug Administration. (2010, July). Combating Misuse and Abuse of Prescription Drugs. In Consumer Health Administration. Retrieved from http://www.fda.gov/downloads/ForConsumers/ConsumerUpdates/UCM220434.pdf
U.S. FDA. (2016, March). General Principles for Evaluating the Abuse Deterrence of Generic Solid Oral Opioid Drug Products Guidance for Industry. Retrieved from http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM492172.pdf