Embed Size (px)
Citation preview
An Update on Herpes Zoster
HZ Burden and the Rationale for
Vaccination
Ian D.R. Landells, MD, FRCPC
Clinical Associate Professor
Memorial University
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may
be reproduced, copied, stored, or transmitted in
any form or by any means – graphic, electronic,
or mechanical, including photocopying,
recording, or information storage and retrieval
systems without prior written permission of Sea
Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker
or participant’s statements, materials, acts or
omissions.
Learning Objectives
• Discuss the pathogenesis & clinical consequences of
pain caused by herpes zoster (HZ)
• Answer questions from patients and their families
about the efficacy and safety of the HZ vaccine
• Identify patients in whom HZ vaccination should be
considered, based on recent clinical and
epidemiological studies
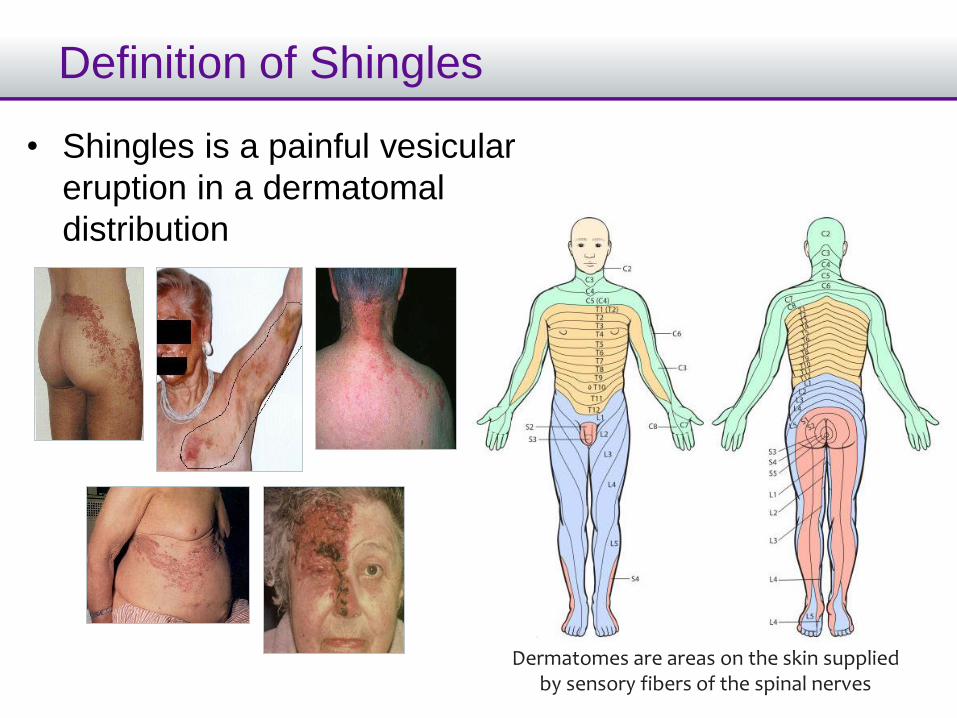
Definition of Shingles
• Shingles is a painful vesicular
eruption in a dermatomal
distribution
Dermatomes are areas on the skin supplied by sensory fibers of the spinal nerves
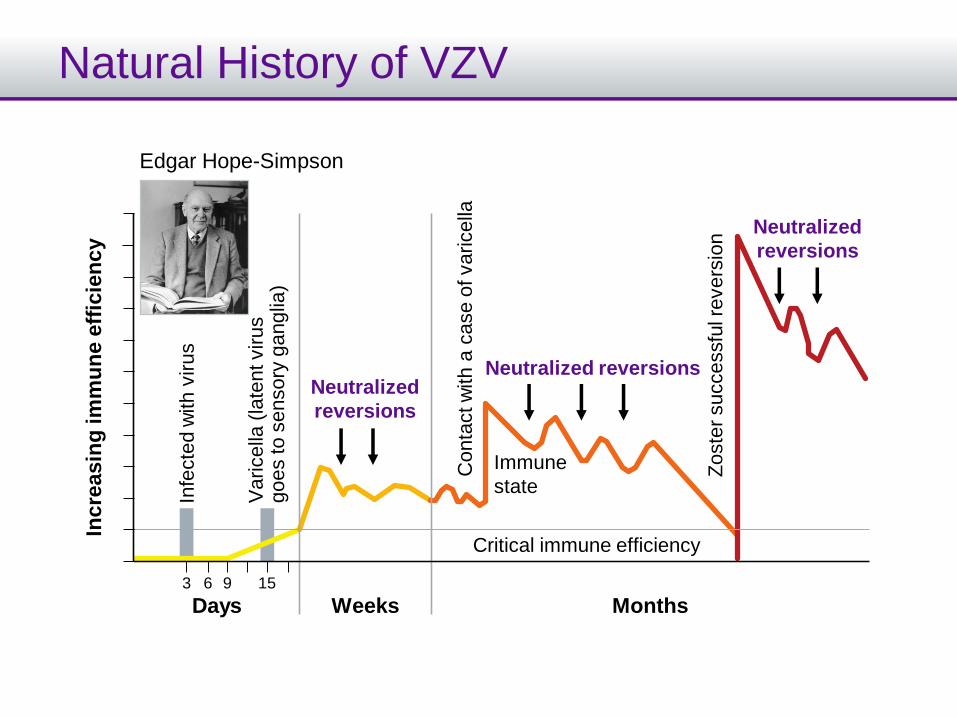
Natural History of VZVIn
cre
asin
g im
mu
ne
eff
icie
nc
y
Days
Edgar Hope-Simpson
3 1596
Weeks Months
Critical immune efficiency
Neutralized reversionsNeutralized
reversions
Neutralized
reversions
Immune
stateC
onta
ct w
ith a
case o
f varicella
Zoste
r successfu
l revers
ion
Infe
cte
d w
ith
viru
s
Varicella
(la
tent virus
go
es to
se
nso
ry g
ang
lia)
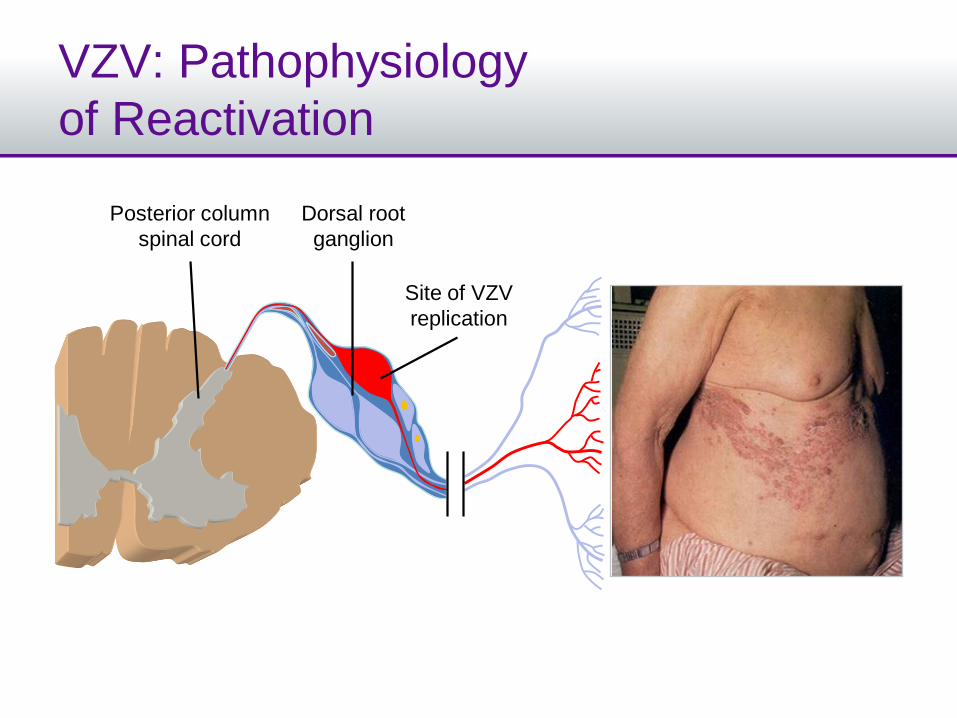
VZV: Pathophysiology
of Reactivation
Posterior column
spinal cord
Dorsal root
ganglion
Site of VZV
replication
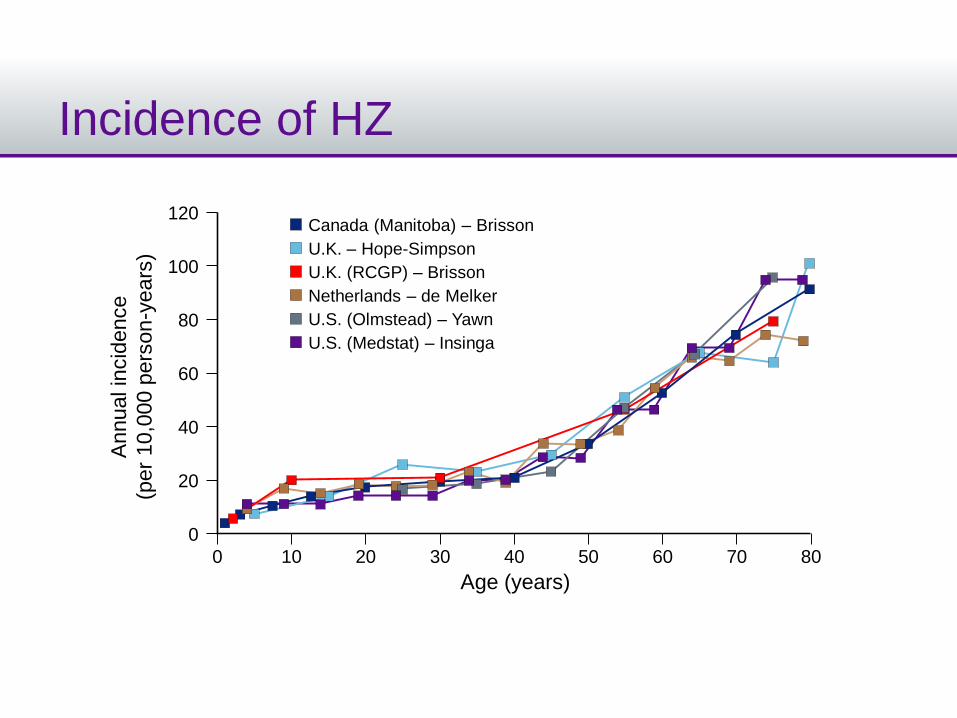
Incidence of HZA
nnual in
cid
ence
(per
10,0
00 p
ers
on
-ye
ars
)
80
0
40
120
60
20
100
0
Age (years)
10 20 30 40 50 60 70 80
Canada (Manitoba) – Brisson
U.K. – Hope-Simpson
U.K. (RCGP) – Brisson
Netherlands – de Melker
U.S. (Olmstead) – Yawn
U.S. (Medstat) – Insinga
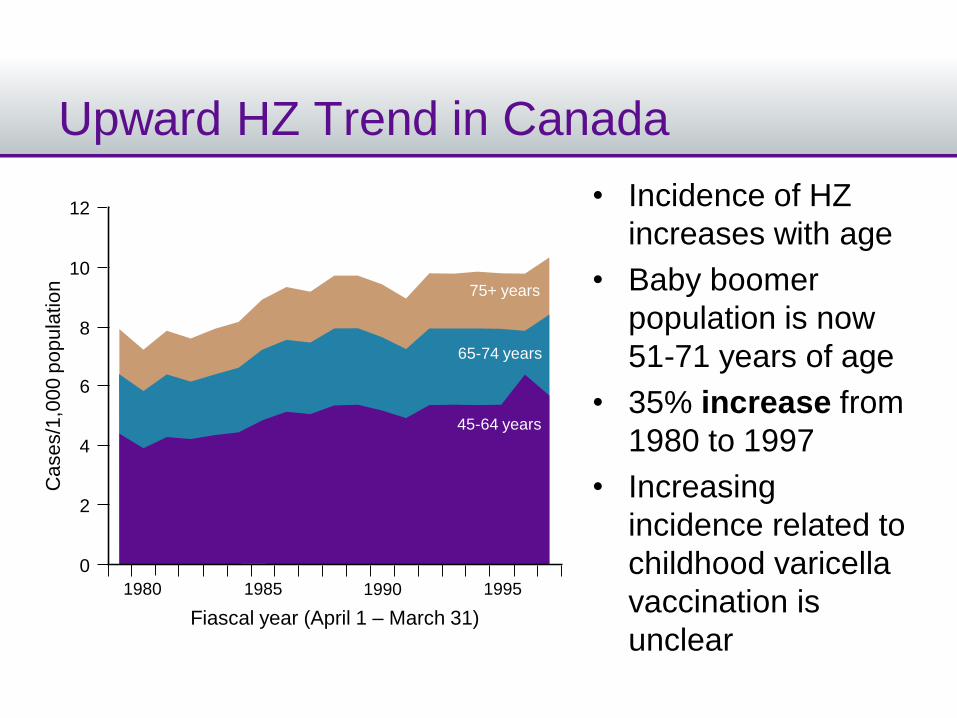
Upward HZ Trend in Canada
12
10
Cases/1
,000 p
opula
tion
Fiascal year (April 1 – March 31)
75+ years
65-74 years
45-64 years
8
0
4
6
2
• Incidence of HZ
increases with age
• Baby boomer
population is now
51-71 years of age
• 35% increase from
1980 to 1997
• Increasing
incidence related to
childhood varicella
vaccination is
unclear
1980 1985 1990 1995
HZ Burden and Complications
• 1 out of 3 Canadians will experience an episode
of HZ in their lifetime
– 1 out of 2 for those aged 85 years and older
• Complications can severely affect the patient’s
quality of life
PHN (10-22%)
Ocular complications
Scarring
Super infections
Stroke
ACUTE
HZ PAIN• loss of work
• low quality of life
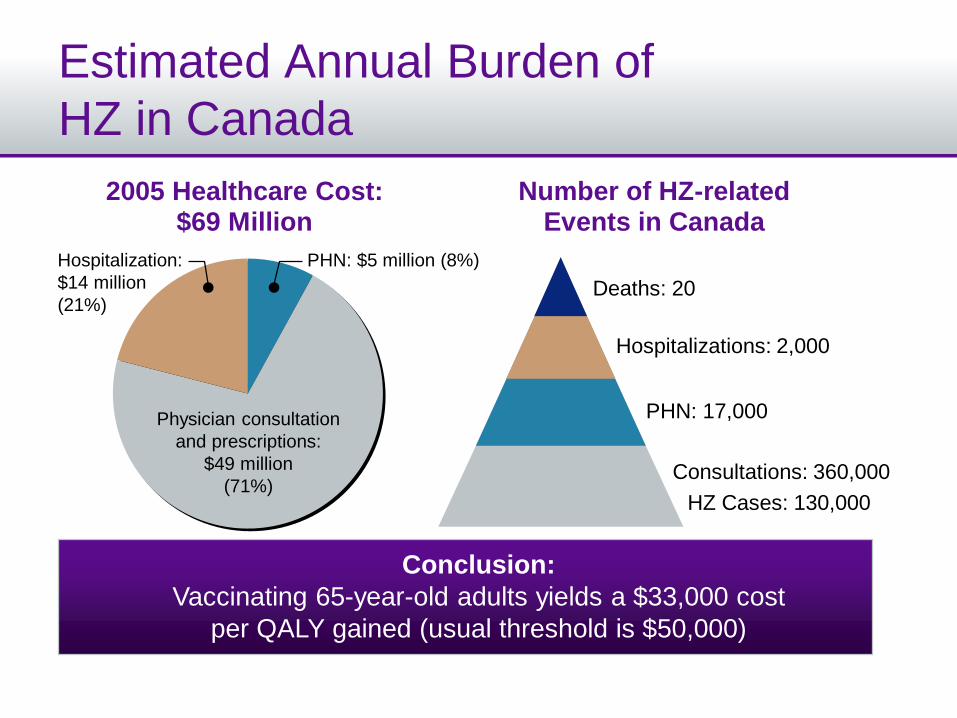
Estimated Annual Burden of
HZ in Canada
2005 Healthcare Cost: $69 Million
Number of HZ-related Events in Canada
Conclusion:
Vaccinating 65-year-old adults yields a $33,000 cost
per QALY gained (usual threshold is $50,000)
HZ Cases: 130,000
Consultations: 360,000
Hospitalizations: 2,000
Deaths: 20
PHN: 17,000Physician consultation
and prescriptions:
$49 million
(71%)
PHN: $5 million (8%)Hospitalization:
$14 million
(21%)
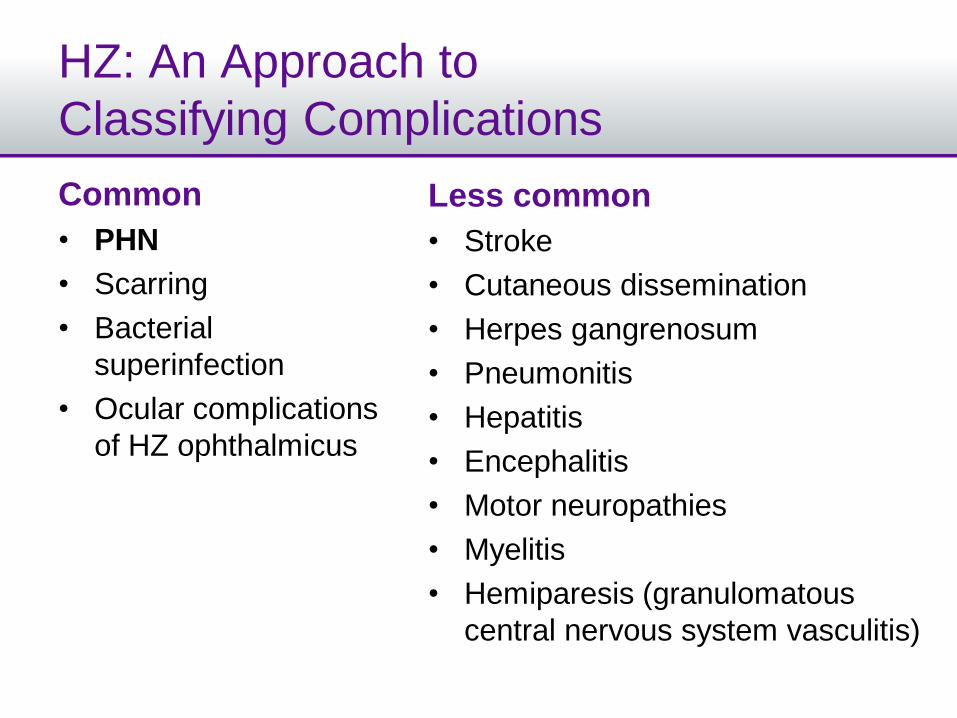
HZ: An Approach to
Classifying Complications
Common
• PHN
• Scarring
• Bacterial
superinfection
• Ocular complications
of HZ ophthalmicus
Less common
• Stroke
• Cutaneous dissemination
• Herpes gangrenosum
• Pneumonitis
• Hepatitis
• Encephalitis
• Motor neuropathies
• Myelitis
• Hemiparesis (granulomatous
central nervous system vasculitis)
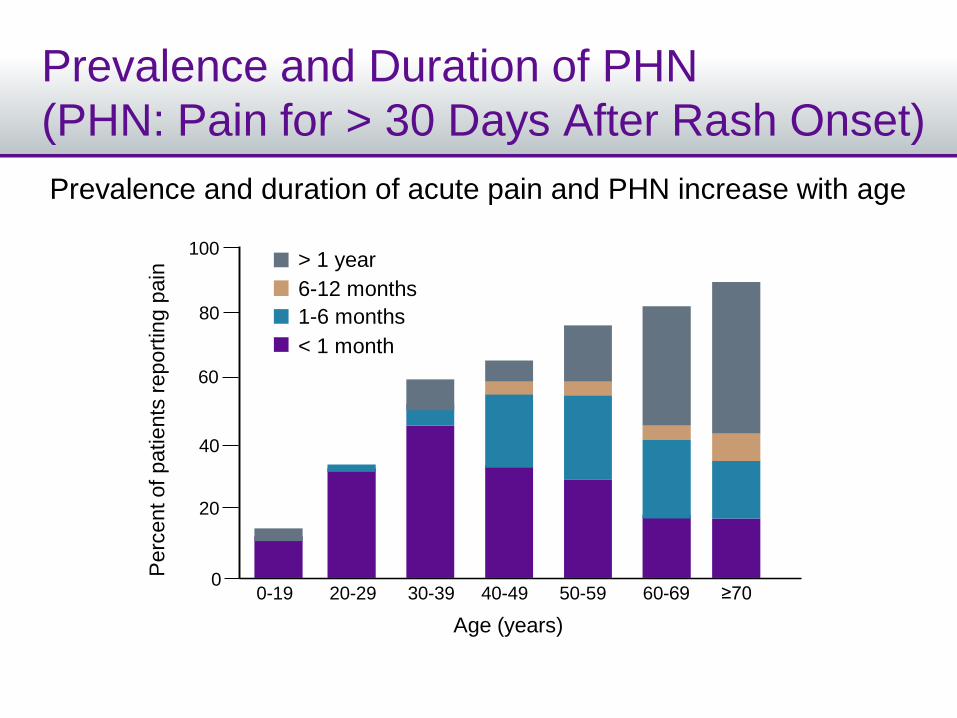
Prevalence and Duration of PHN
(PHN: Pain for > 30 Days After Rash Onset)
Prevalence and duration of acute pain and PHN increase with age
0-19 20-29 30-39 40-49 50-59 60-69 ≥70
Age (years)
100
80
60
40
20
0
Perc
ent of
patie
nts
report
ing p
ain
> 1 year
6-12 months
1-6 months
< 1 month
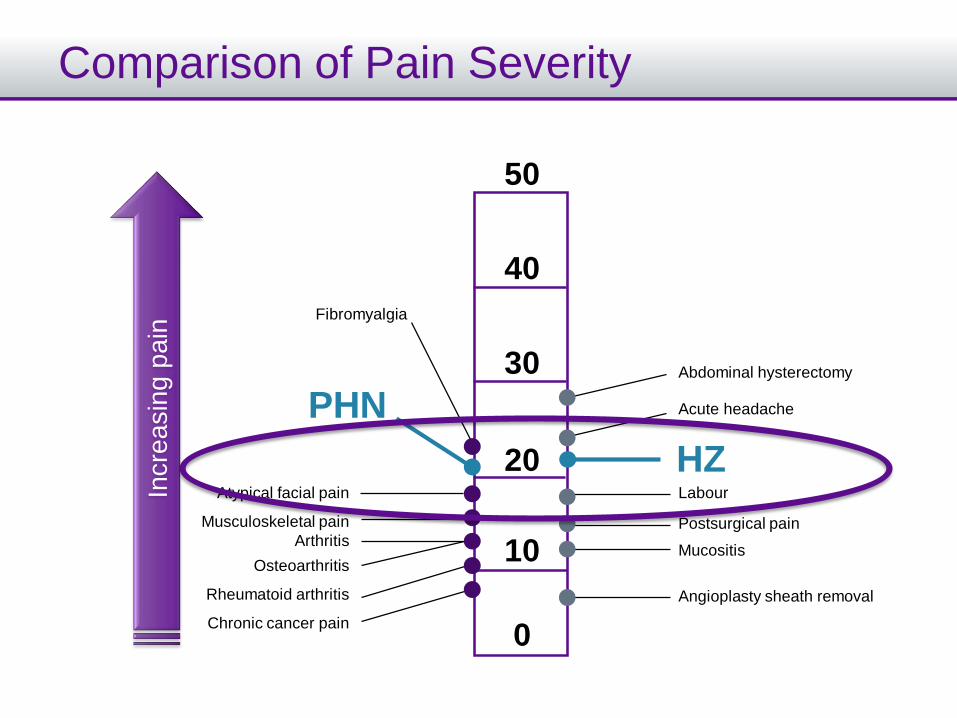
Comparison of Pain Severity
HZ
PHN
50
40
30
20
10
0
Fibromyalgia
Atypical facial pain
Musculoskeletal pain
Arthritis
Osteoarthritis
Rheumatoid arthritis
Chronic cancer pain
Abdominal hysterectomy
Acute headache
Labour
Postsurgical pain
Mucositis
Angioplasty sheath removal
Incre
asin
g p
ain
Risk Factors for Developing PHN
Increased likelihood
• Age over 50 years
• Female
• Severity of prodrome
• Severe or disseminated rash > 1 dermatome
• Severe pain at presentation (visual analogue scale > 5)
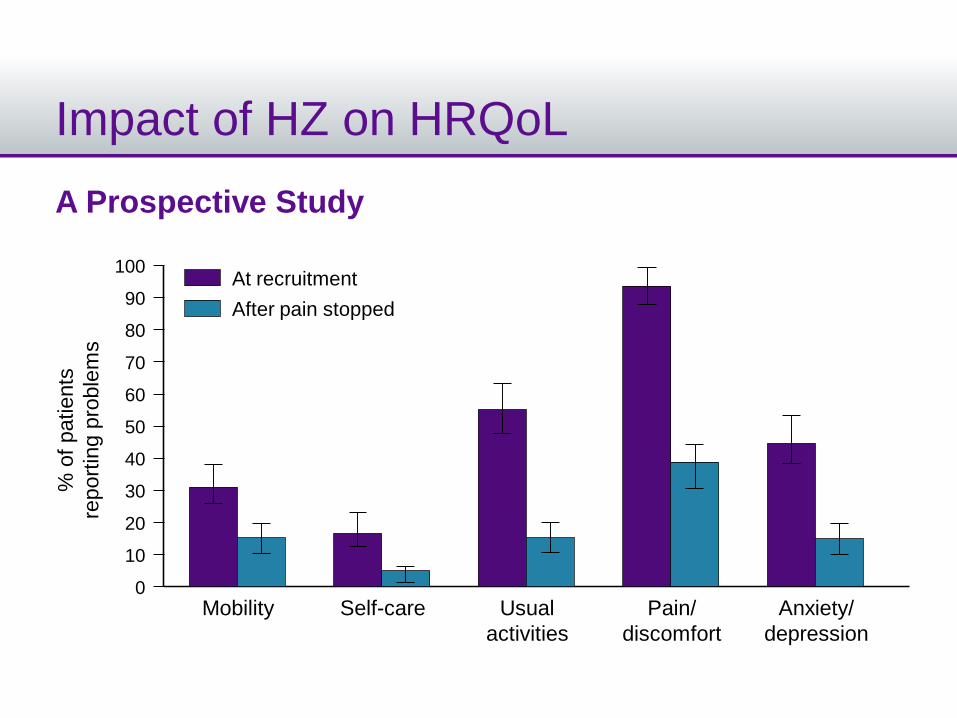
Impact of HZ on HRQoL
A Prospective Study
% o
f patie
nts
report
ing p
roble
ms
80
0
60
40
20
100At recruitment
70
50
30
10
90
Mobility Self-care Usual
activities
Pain/
discomfort
Anxiety/
depression
After pain stopped
% o
f patie
nts
report
ing p
roble
ms
80
0
60
40
20
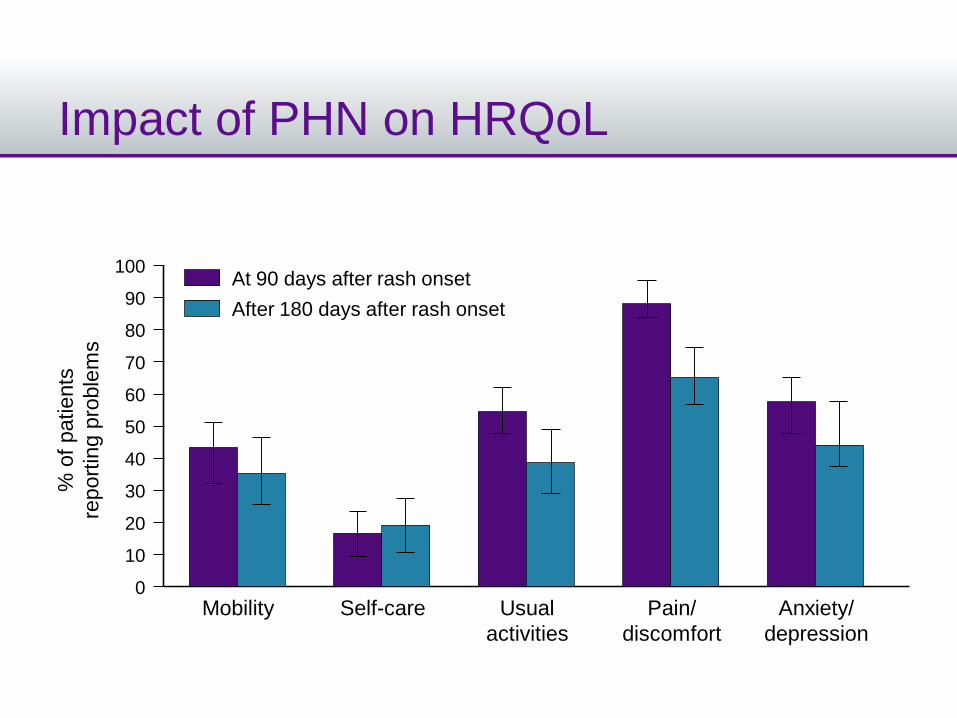
100At 90 days after rash onset
70
50
30
10
90
Mobility Self-care Usual
activities
Pain/
discomfort
Anxiety/
depression
After 180 days after rash onset
Impact of PHN on HRQoL
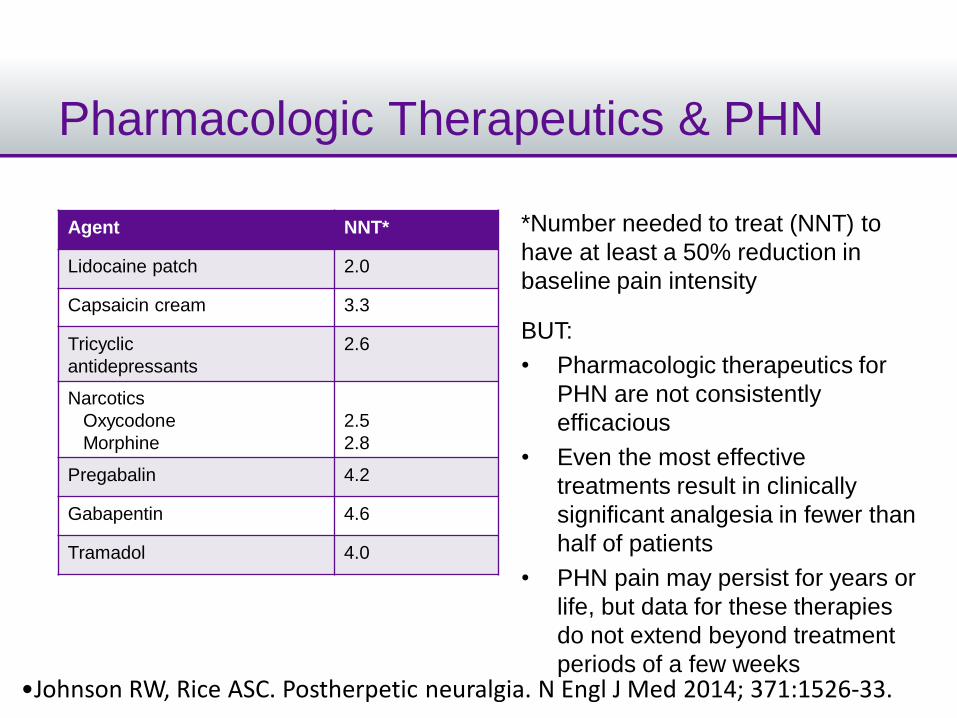
Pharmacologic Therapeutics & PHN
Agent NNT*
Lidocaine patch 2.0
Capsaicin cream 3.3
Tricyclic
antidepressants
2.6
Narcotics
Oxycodone
Morphine
2.5
2.8
Pregabalin 4.2
Gabapentin 4.6
Tramadol 4.0
•Johnson RW, Rice ASC. Postherpetic neuralgia. N Engl J Med 2014; 371:1526-33.
*Number needed to treat (NNT) to
have at least a 50% reduction in
baseline pain intensity
BUT:
• Pharmacologic therapeutics for
PHN are not consistently
efficacious
• Even the most effective
treatments result in clinically
significant analgesia in fewer than
half of patients
• PHN pain may persist for years or
life, but data for these therapies
do not extend beyond treatment
periods of a few weeks
Antivirals for Preventing PHN?
•Chen N, Li Q, Yang J, et al. Antiviral treatment for preventing postherpeticneuralgia. Cochrane Database of Systematic Reviews 2014; 2:CD006866.
• Must be given during time of rash (within 72 hours of
HZ onset in studies)
• In 6 RCTs with 1,211 eligible subjects:
– No significant difference between aciclovir and control
groups for PHN incidence
• 4 months after HZ rash onset: RR 0.75; 95% CI 0.51-1.11
• 6 months after HZ rash onset: RR 1.05; 95% CI 0.87-1.27
– No significant reduction in PHN incidence with famciclovir
vs. placebo
• Further research needed to investigate famciclovir and
other new antivirals for preventing PHN
The Shingles Prevention Study (SPS)
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS: Study Design
• RCT: double-blind, placebo-controlled
• Subjects:– 38,546 subjects enrolled, ≥ 60 years of age
– History of chickenpox or U.S. resident ≥ 30 years
• Excluded– Immunocompromised
• One dose of live-attenuated vaccine or placebo
• 93% of HZ cases confirmed to be VZV by PCR
• Primary endpoint: Burden of Illness Score = severity-by-duration over 182 days after rash onset
• PHN: pain with severity ≥ 3 out of 10 max, present at ≥ 90 days after rash onset
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
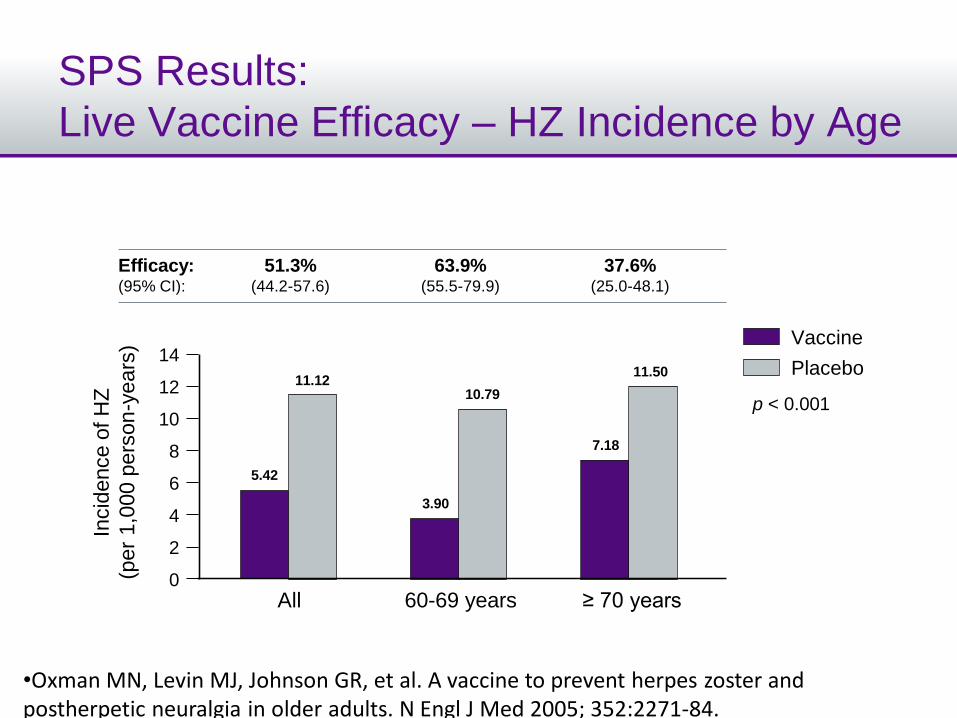
SPS Results:
Live Vaccine Efficacy – HZ Incidence by AgeIn
cid
ence o
f H
Z
(per
1,0
00 p
ers
on
-years
)
0
12
8
4
14
10
6
2
All 60-69 years ≥ 70 years
11.12
5.42
10.79
3.90
11.50
7.18
p < 0.001
Efficacy:(95% CI):
51.3% (44.2-57.6)
63.9% (55.5-79.9)
37.6% (25.0-48.1)
Vaccine
Placebo
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
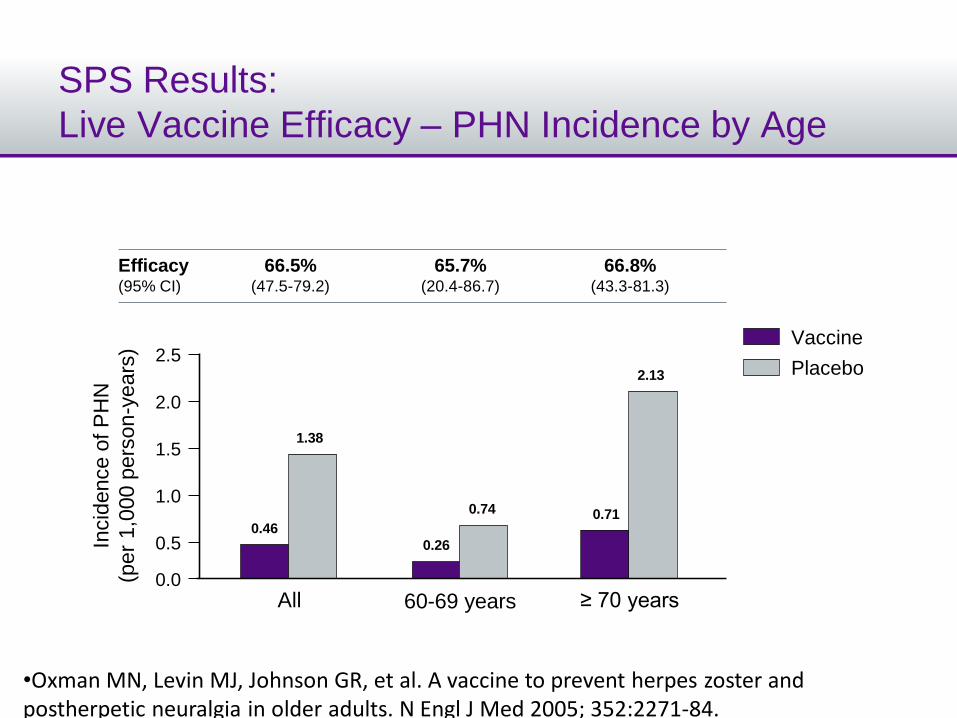
SPS Results:
Live Vaccine Efficacy – PHN Incidence by AgeIn
cid
ence o
f P
HN
(per
1,0
00 p
ers
on
-years
)
0.0
2.0
1.0
2.5
1.5
0.5
All 60-69 years ≥ 70 years
1.38
0.46
0.74
0.26
2.13
0.71
Efficacy(95% CI)
66.5% (47.5-79.2)
65.7% (20.4-86.7)
66.8% (43.3-81.3)
Vaccine
Placebo
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
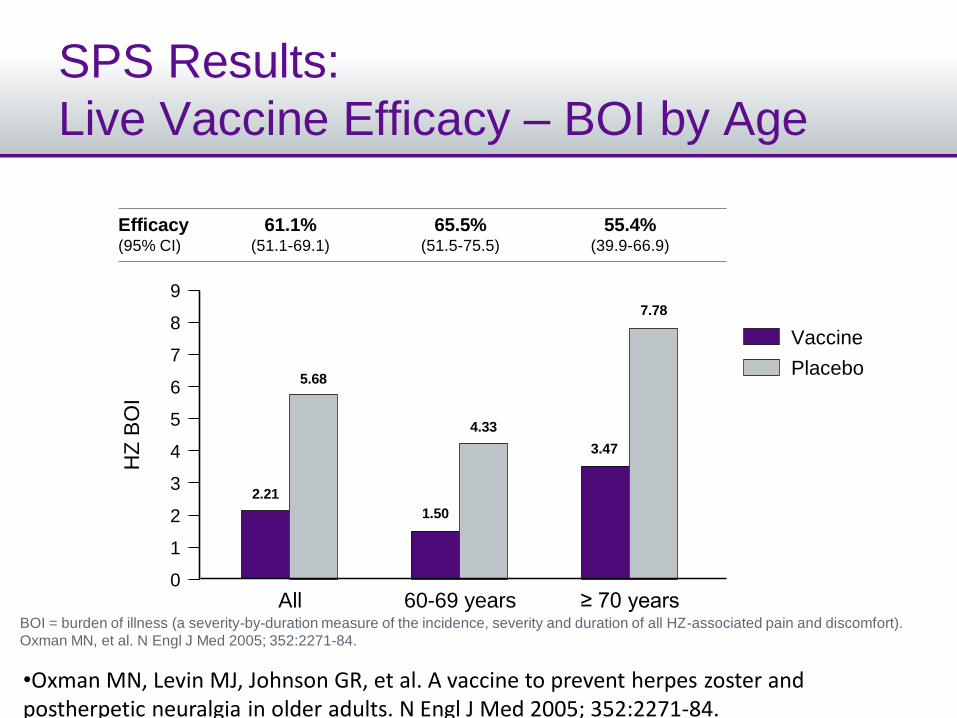
SPS Results:
Live Vaccine Efficacy – BOI by Age
BOI = burden of illness (a severity-by-duration measure of the incidence, severity and duration of all HZ-associated pain and discomfort).
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Efficacy(95% CI)
Vaccine
9
Placebo
61.1% (51.1-69.1)
All
65.5% (51.5-75.5)
60-69 years
55.4% (39.9-66.9)
≥ 70 years
HZ
BO
I
8
0
6
4
2
7
5
3
1
5.68
2.21
4.33
1.50
7.78
3.47
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
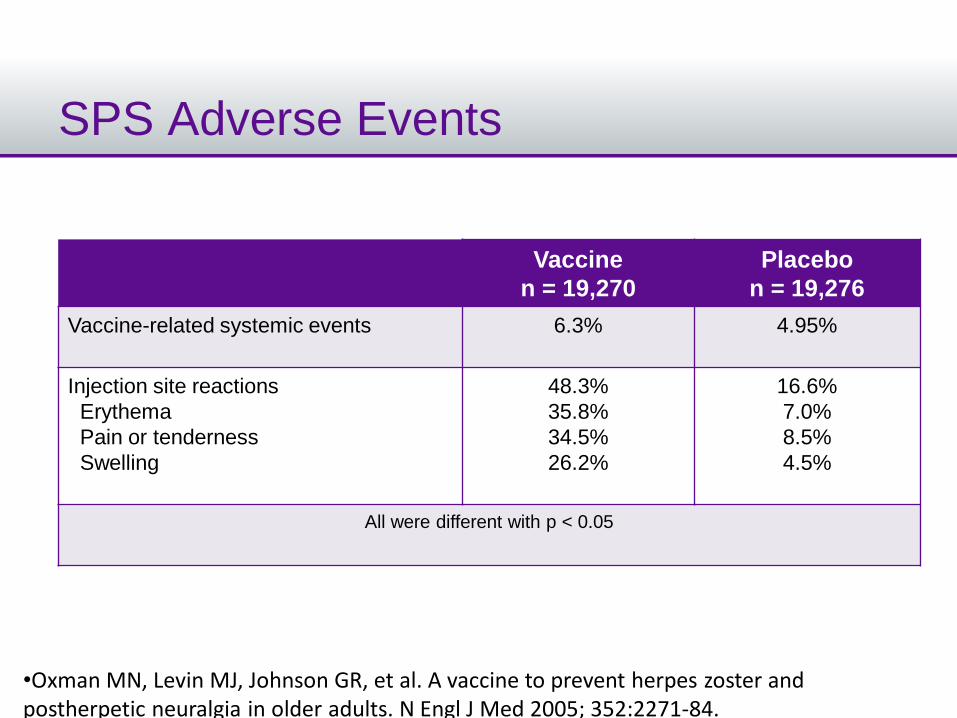
SPS Adverse Events
Vaccine
n = 19,270
Placebo
n = 19,276
Vaccine-related systemic events 6.3% 4.95%
Injection site reactions
Erythema
Pain or tenderness
Swelling
48.3%
35.8%
34.5%
26.2%
16.6%
7.0%
8.5%
4.5%
All were different with p < 0.05
•Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
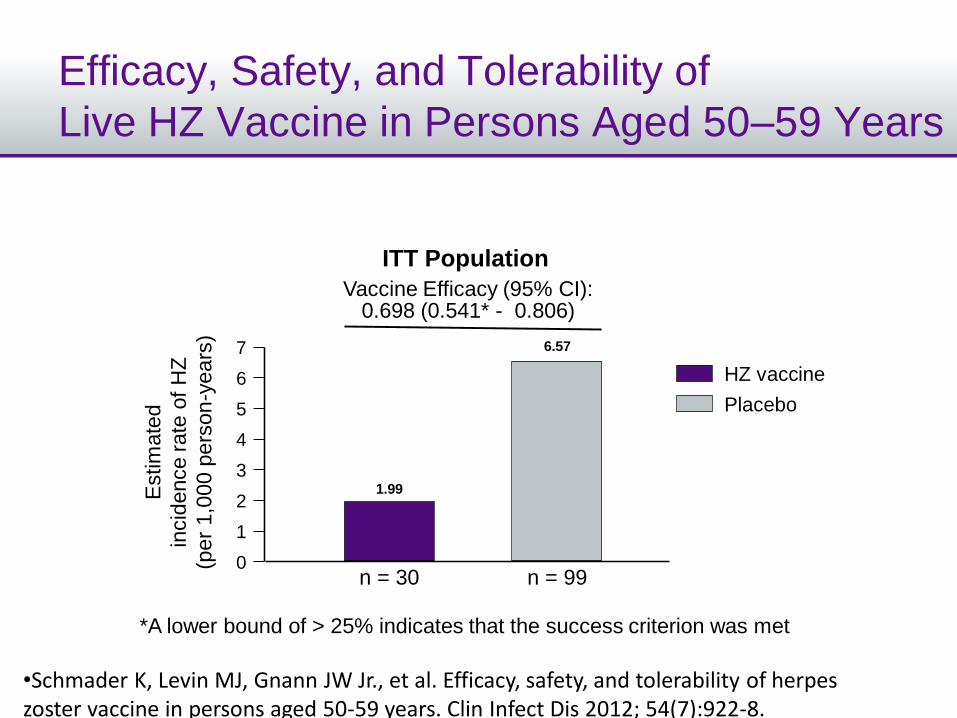
Efficacy, Safety, and Tolerability of
Live HZ Vaccine in Persons Aged 50–59 Years
HZ vaccine
Placebo
Estim
ate
d
incid
ence r
ate
of
HZ
(per
1,0
00 p
ers
on
-years
)
0
6
4
2
7
5
3
1
1.99
6.57
n = 30 n = 99
ITT Population
Vaccine Efficacy (95% CI): 0.698 (0.541* - 0.806)
*A lower bound of > 25% indicates that the success criterion was met
•Schmader K, Levin MJ, Gnann JW Jr., et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50-59 years. Clin Infect Dis 2012; 54(7):922-8.
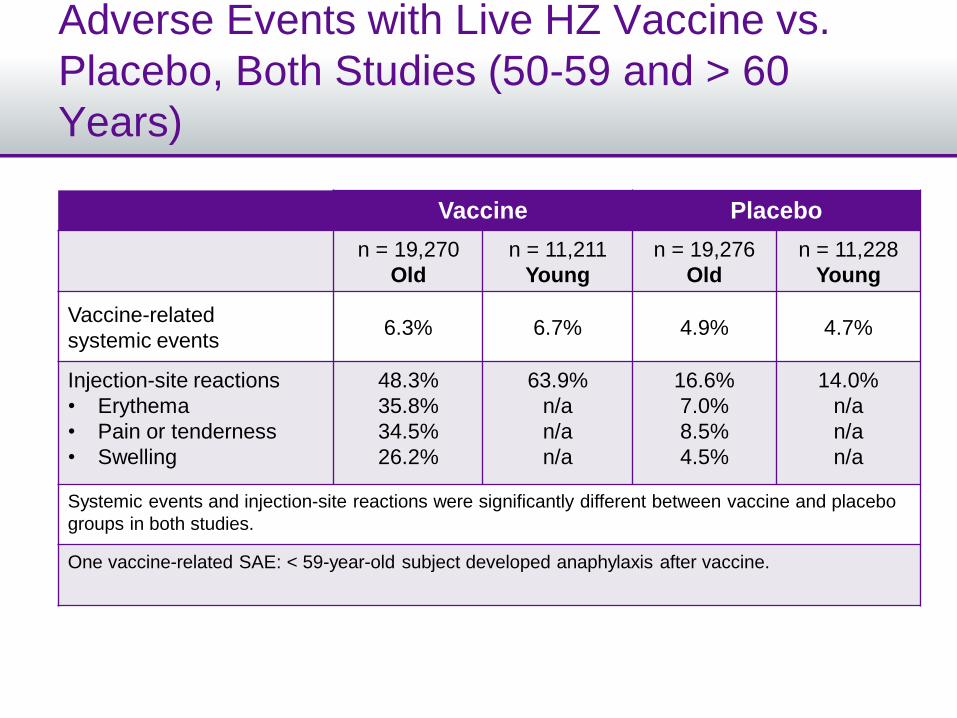
Adverse Events with Live HZ Vaccine vs.
Placebo, Both Studies (50-59 and > 60
Years)
Vaccine Placebo
n = 19,270
Old
n = 11,211
Young
n = 19,276
Old
n = 11,228
Young
Vaccine-related
systemic events6.3% 6.7% 4.9% 4.7%
Injection-site reactions
• Erythema
• Pain or tenderness
• Swelling
48.3%
35.8%
34.5%
26.2%
63.9%
n/a
n/a
n/a
16.6%
7.0%
8.5%
4.5%
14.0%
n/a
n/a
n/a
Systemic events and injection-site reactions were significantly different between vaccine and placebo
groups in both studies.
One vaccine-related SAE: < 59-year-old subject developed anaphylaxis after vaccine.
Conclusions
• Immunization with Live HZ vaccine reduced:
– The PHN Burden of Illness score by 66% (aged
60-69 years) and 55% (aged ≥ 70 years)
– The incidence of HZ by 64% and 37% in the two
age cohorts
– The incidence of PHN by 66% and 67% in the
two age cohorts
• HZ vaccine was well tolerated and was not
accompanied by an increased risk of AEs
Live HZ Vaccine Duration of Protection
• HZ vaccine (1 dose) reduces the
risk of HZ for at least 8 years in
immunocompetent adults1
• No booster dose is currently
recommended2
1. Morrison VA, et al. Clin Infect Dis 2014; [epub ahead of print].2. National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
NACI Recommendations – Live HZ
Vaccine
Immunization with Live HZ vaccine for
immunocompetent adults:
• Vaccine is recommended for adults ≥ 60 years of age
• Vaccine may be used in adults 50-59 years of age
• Vaccine may be administered to individuals ≥ 50 years old with
a prior history of HZ. Based on expert opinion, it is
recommended that the vaccine be given at least one year
following the last episode of HZ
– Annual recurrence rate in immunocompetent adults has varied
across studies/methods:
• Yawn et al 2011: 5.7% recurrence rate over 8 years (and 12% in
immunocompromised adults)
See supplementary slides for more detailed NACI recommendations.National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
NACI Recommendations – Live HZ
Vaccine (cont’d)
Immunization with HZ vaccine for
immunosuppressed adults:
• Individuals on low-dose immunosuppressive therapy
– It is reasonable to consider HZ vaccine in patients on lower doses of
immunosuppressive agents: prednisone < 20 mg/day; methotrexate
≤ 0.4 mg/kg/week, azathioprine ≤ 3.0 mg/kg/day; 6-mercaptopurine ≤
1.5 mg/kg/day
• Individuals on anti-TNF biologics
– HZ vaccine may be used; on a case-by-case basis after review with
an expert in immunodeficiency
See supplementary slides for more detailed NACI recommendations.National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Updated NACI Recommendations:
Live HZ Vaccine Recommended Use –
Administration with Other Vaccines
Recommendation Comments
• PneumovaxTM23 may be
administered concomitantly
with HZ vaccine at a different
body injection site
• NACI recommendation
A, good.
• This is a change from the
previous NACI
recommendation.
National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Updated NACI RecommendationsLive HZ Vaccine Recommended Use –Immunosuppressed Patients (cont’d)
Group Recommendation Comments
Individuals on anti-TNF
biologics
• May be used
• NACI
recommendation
B, fair.
On a case-by-case basis
after review with an
expert in
immunodeficiency
National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Adjuvanted subunit vaccine:
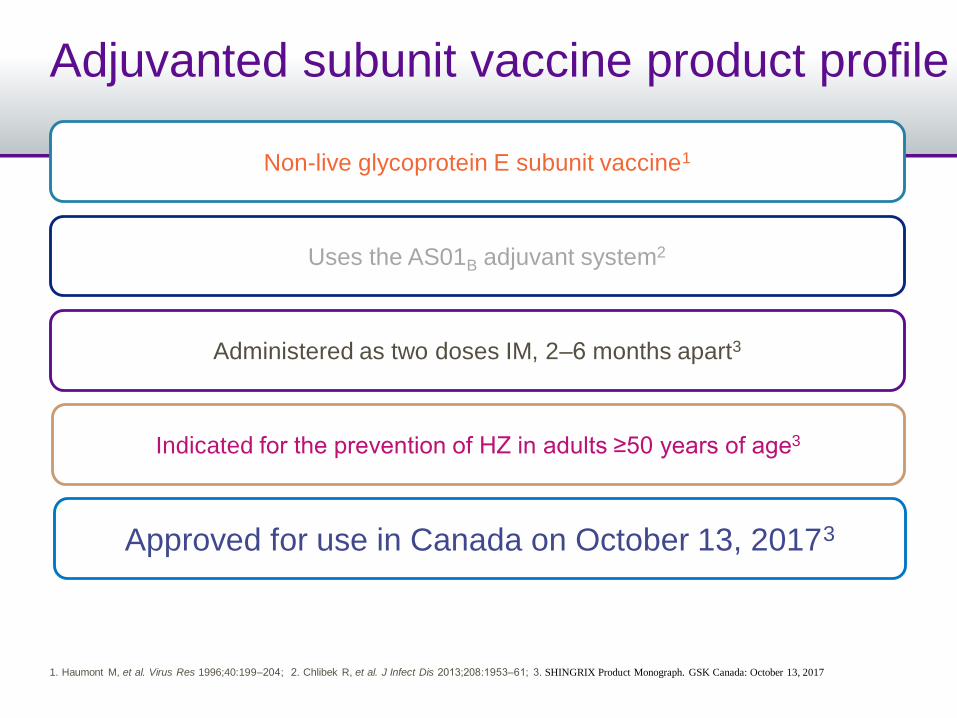
Adjuvanted subunit vaccine product profile
Administered as two doses IM, 2‒6 months apart3
Indicated for the prevention of HZ in adults ≥50 years of age3
Non-live glycoprotein E subunit vaccine1
– Uses the AS01B adjuvant system2
Approved for use in Canada on October 13, 20173
1. Haumont M, et al. Virus Res 1996;40:199‒204; 2. Chlibek R, et al. J Infect Dis 2013;208:1953‒61; 3. SHINGRIX Product Monograph. GSK Canada: October 13, 2017
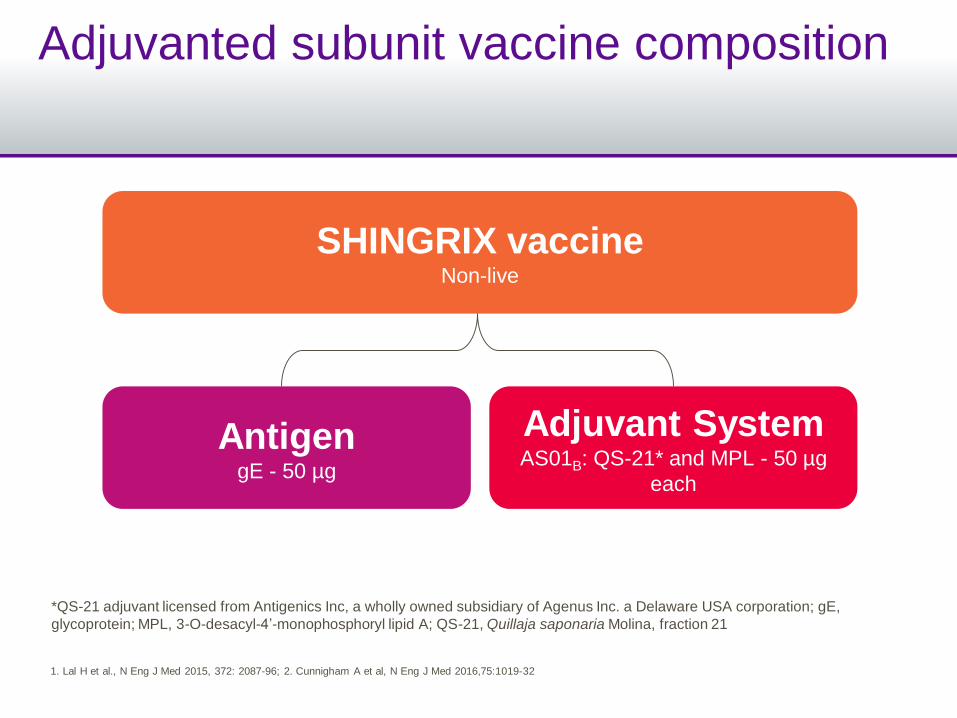
Adjuvanted subunit vaccine composition
SHINGRIX vaccineNon-live
Adjuvant SystemAS01B: QS-21* and MPL - 50 µg
each
AntigengE - 50 µg
*QS-21 adjuvant licensed from Antigenics Inc, a wholly owned subsidiary of Agenus Inc. a Delaware USA corporation; gE,
glycoprotein; MPL, 3-O-desacyl-4’-monophosphoryl lipid A; QS-21, Quillaja saponaria Molina, fraction 21
1. Lal H et al., N Eng J Med 2015, 372: 2087-96; 2. Cunnigham A et al, N Eng J Med 2016,75:1019-32
Adjuvanted subunit vaccine pivotal phase III program: ZOE-50 and ZOE-701,2
New England Journal of Medicine, 2015, 2016
1.Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
PHN, postherpetic neuralgia; VE, vaccine efficacy
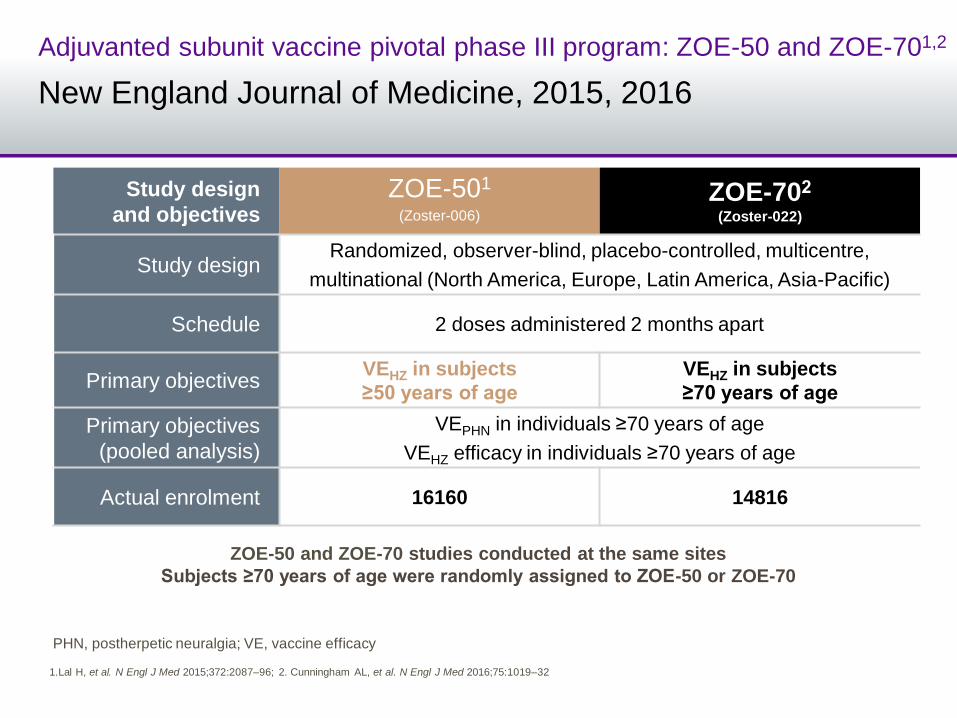
Adjuvanted subunit vaccine pivotal phase III program: ZOE-50 and ZOE-701,2
New England Journal of Medicine, 2015, 2016
ZOE-50 and ZOE-70 studies conducted at the same sites
Subjects ≥70 years of age were randomly assigned to ZOE-50 or ZOE-70
Study design
and objectivesZOE-501
(Zoster-006)
ZOE-702
(Zoster-022)
Study designRandomized, observer-blind, placebo-controlled, multicentre,
multinational (North America, Europe, Latin America, Asia-Pacific)
Schedule 2 doses administered 2 months apart
Primary objectivesVEHZ in subjects
≥50 years of age
VEHZ in subjects
≥70 years of age
Primary objectives
(pooled analysis)
VEPHN in individuals ≥70 years of age
VEHZ efficacy in individuals ≥70 years of age
Actual enrolment 16160 14816
1.Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
PHN, postherpetic neuralgia; VE, vaccine efficacy
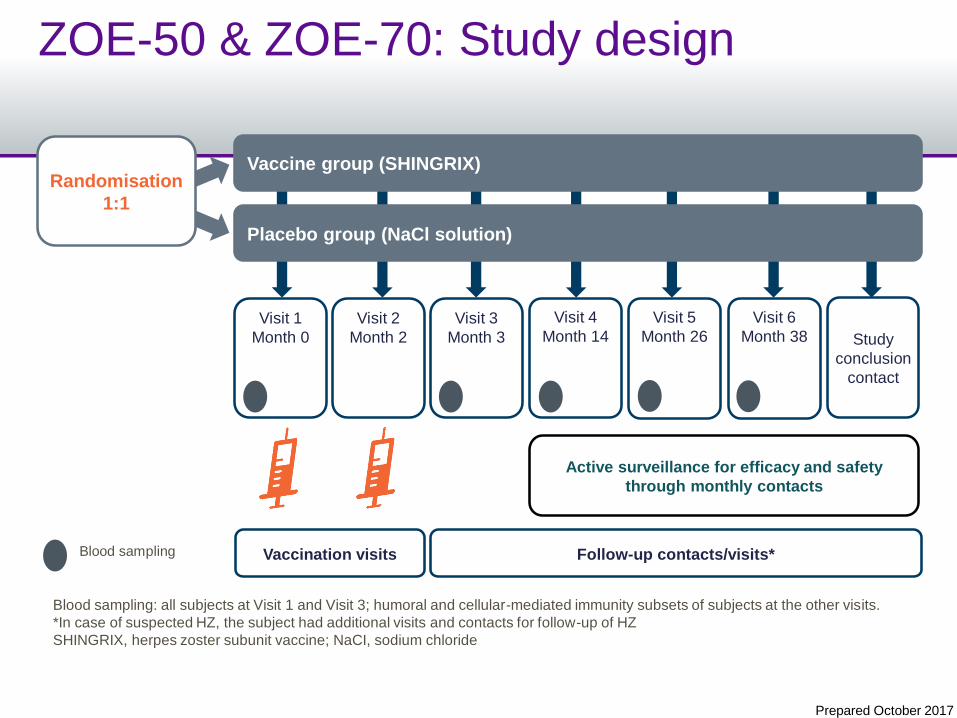
ZOE-50 & ZOE-70: Study design
Randomisation
1:1
Visit 1
Month 0
Visit 2
Month 2
Visit 3
Month 3 Study
conclusion
contact
Placebo group (NaCl solution)
Vaccine group (SHINGRIX)
Vaccination visits Follow-up contacts/visits*
Active surveillance for efficacy and safety
through monthly contacts
Visit 6
Month 38
Visit 5
Month 26
Visit 4
Month 14
Blood sampling
Blood sampling: all subjects at Visit 1 and Visit 3; humoral and cellular-mediated immunity subsets of subjects at the other visits.
*In case of suspected HZ, the subject had additional visits and contacts for follow-up of HZ
SHINGRIX, herpes zoster subunit vaccine; NaCI, sodium chloride
Prepared October 2017
Adjuvanted subunit vaccine
Efficacy
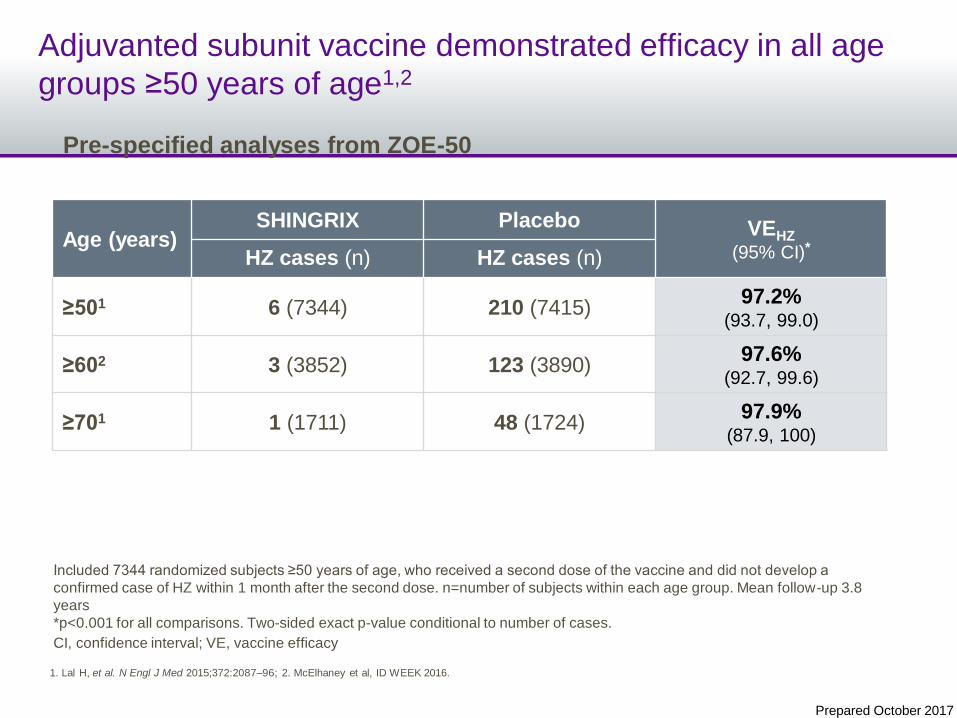
Adjuvanted subunit vaccine demonstrated efficacy in all age
groups ≥50 years of age1,2
Age (years)SHINGRIX Placebo VEHZ
(95% CI)*HZ cases (n) HZ cases (n)
≥501 6 (7344) 210 (7415)97.2%
(93.7, 99.0)
≥602 3 (3852) 123 (3890)97.6%
(92.7, 99.6)
≥701 1 (1711) 48 (1724)97.9%
(87.9, 100)
Included 7344 randomized subjects ≥50 years of age, who received a second dose of the vaccine and did not develop a
confirmed case of HZ within 1 month after the second dose. n=number of subjects within each age group. Mean follow-up 3.8
years
*p<0.001 for all comparisons. Two-sided exact p-value conditional to number of cases.
CI, confidence interval; VE, vaccine efficacy
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. McElhaney et al, ID WEEK 2016.
Pre-specified analyses from ZOE-50
Prepared October 2017
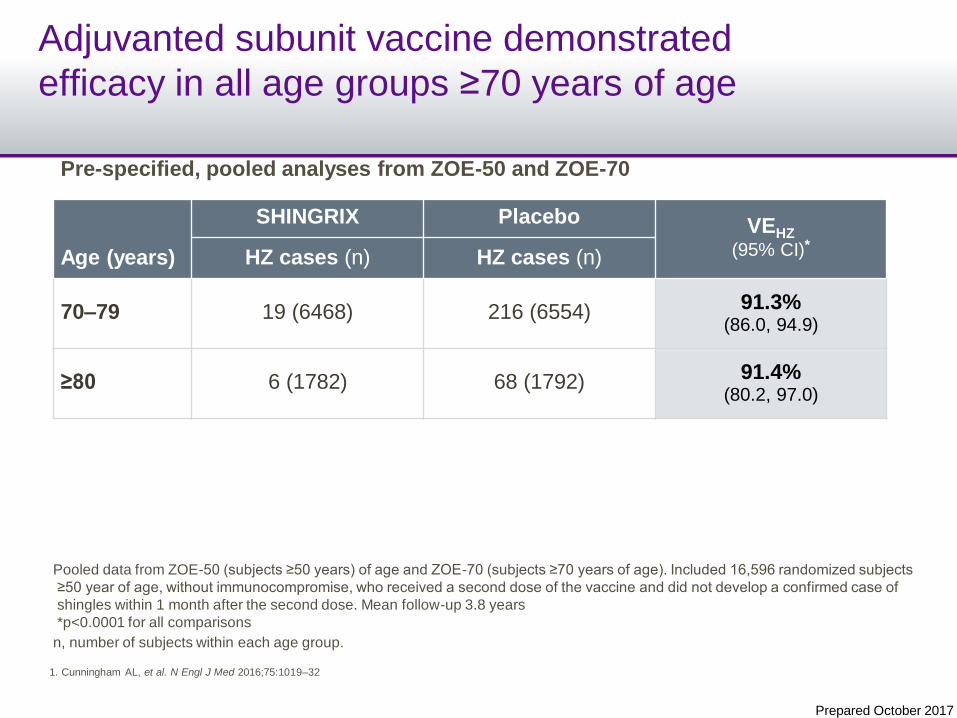
Adjuvanted subunit vaccine demonstrated
efficacy in all age groups ≥70 years of age
Age (years)
SHINGRIX Placebo VEHZ
(95% CI)*HZ cases (n) HZ cases (n)
70‒79 19 (6468) 216 (6554) 91.3%(86.0, 94.9)
≥80 6 (1782) 68 (1792) 91.4%(80.2, 97.0)
Pooled data from ZOE-50 (subjects ≥50 years) of age and ZOE-70 (subjects ≥70 years of age). Included 16,596 randomized subjects
≥50 year of age, without immunocompromise, who received a second dose of the vaccine and did not develop a confirmed case of
shingles within 1 month after the second dose. Mean follow-up 3.8 years
*p<0.0001 for all comparisons
n, number of subjects within each age group.
1. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Pre-specified, pooled analyses from ZOE-50 and ZOE-70
Prepared October 2017
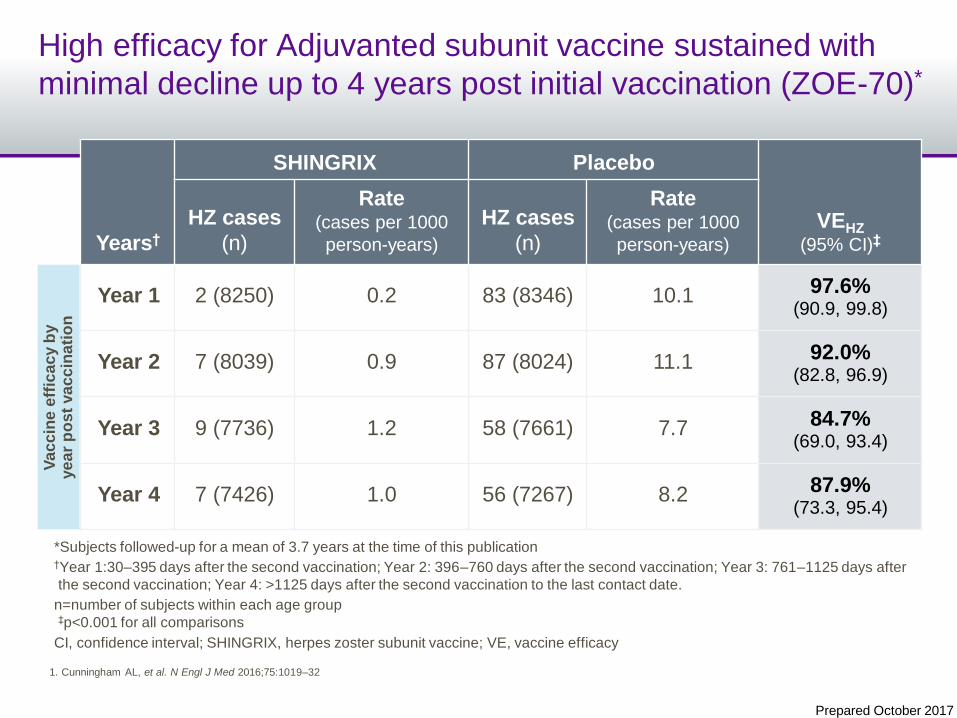
High efficacy for Adjuvanted subunit vaccine sustained with
minimal decline up to 4 years post initial vaccination (ZOE-70)*
Years†
SHINGRIX Placebo
VEHZ
(95% CI)‡HZ cases
(n)
Rate(cases per 1000
person-years)
HZ cases
(n)
Rate(cases per 1000
person-years)
Year 1 2 (8250) 0.2 83 (8346) 10.1 97.6%(90.9, 99.8)
Year 2 7 (8039) 0.9 87 (8024) 11.1 92.0%(82.8, 96.9)
Year 3 9 (7736) 1.2 58 (7661) 7.7 84.7%(69.0, 93.4)
Year 4 7 (7426) 1.0 56 (7267) 8.2 87.9%(73.3, 95.4)
Va
cc
ine
eff
ica
cy b
y
ye
ar
po
st
va
cc
ina
tio
n
*Subjects followed-up for a mean of 3.7 years at the time of this publication†Year 1:30‒395 days after the second vaccination; Year 2: 396‒760 days after the second vaccination; Year 3: 761‒1125 days after
the second vaccination; Year 4: >1125 days after the second vaccination to the last contact date.
n=number of subjects within each age group‡p<0.001 for all comparisons
CI, confidence interval; SHINGRIX, herpes zoster subunit vaccine; VE, vaccine efficacy
1. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Prepared October 2017
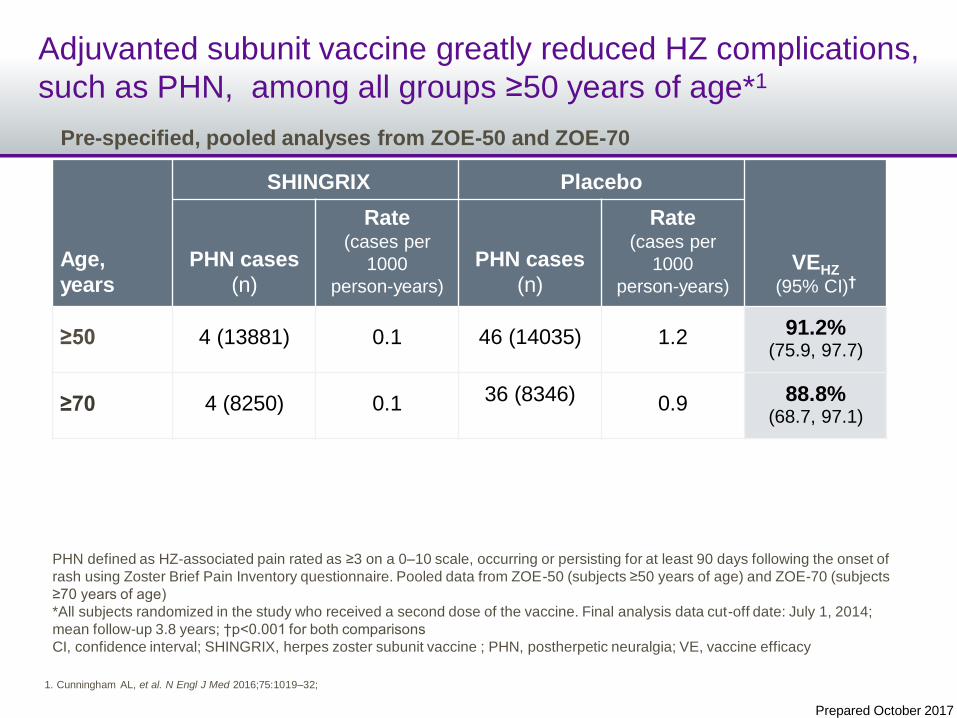
Adjuvanted subunit vaccine greatly reduced HZ complications,
such as PHN, among all groups ≥50 years of age*1
PHN defined as HZ-associated pain rated as ≥3 on a 0‒10 scale, occurring or persisting for at least 90 days following the onset of
rash using Zoster Brief Pain Inventory questionnaire. Pooled data from ZOE-50 (subjects ≥50 years of age) and ZOE-70 (subjects
≥70 years of age)
*All subjects randomized in the study who received a second dose of the vaccine. Final analysis data cut-off date: July 1, 2014;
mean follow-up 3.8 years; †p<0.001 for both comparisons
CI, confidence interval; SHINGRIX, herpes zoster subunit vaccine ; PHN, postherpetic neuralgia; VE, vaccine efficacy
Pre-specified, pooled analyses from ZOE-50 and ZOE-70
1. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32;
Age,
years
SHINGRIX Placebo
VEHZ
(95% CI)†PHN cases
(n)
Rate(cases per
1000
person-years)
PHN cases
(n)
Rate(cases per
1000
person-years)
≥50 4 (13881) 0.1 46 (14035) 1.2 91.2%(75.9, 97.7)
≥70 4 (8250) 0.1 36 (8346) 0.9 88.8%(68.7, 97.1)
Prepared October 2017
Summary: Adjuvanted subunit vaccine efficacyConsistent efficacy across all ages groups ≥50 years of age
High efficacy regardless of age in all ≥50 years old (>90%)1,2
High efficacy sustained with minimal decline up to 4 years post initial vaccination2*
HZ complications, such as PHN, were greatly reduced in all ≥50 years of age2
– z
– z
*Subjects have been followed for a mean of 3.7 years
YOA, years of age
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Prepared October 2017
Adjuvanted subunit vaccine
Safety
Prepared October 2017
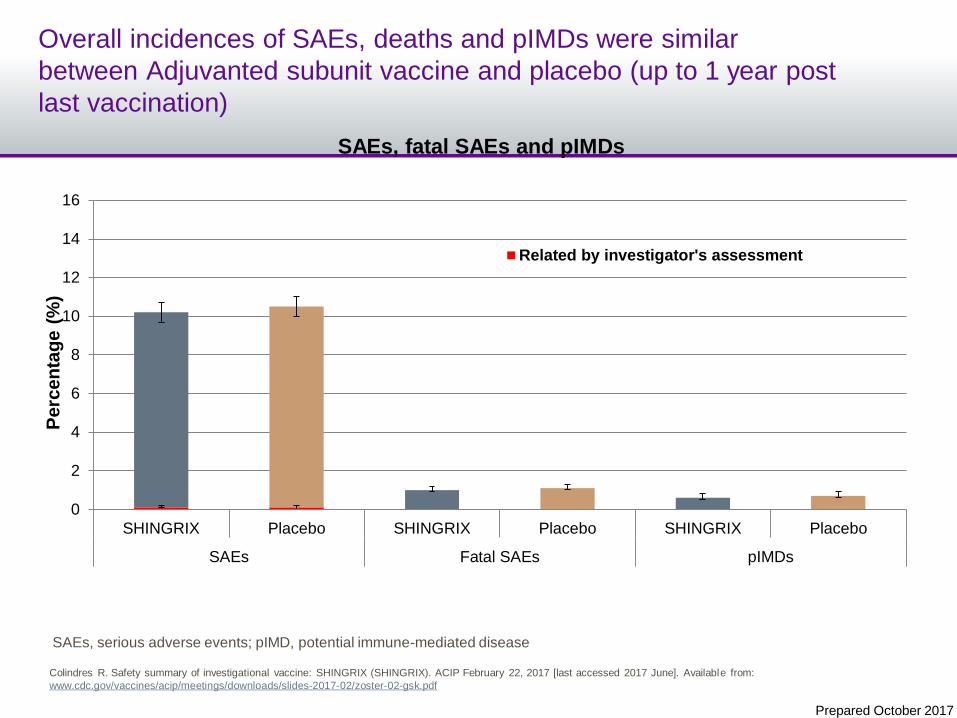
Overall incidences of SAEs, deaths and pIMDs were similar
between Adjuvanted subunit vaccine and placebo (up to 1 year post
last vaccination)
0
2
4
6
8
10
12
14
16
SHINGRIX Placebo SHINGRIX Placebo SHINGRIX Placebo
SAEs Fatal SAEs pIMDs
Perc
en
tag
e (
%)
SAEs, fatal SAEs and pIMDs
Related by investigator's assessment
SAEs, serious adverse events; pIMD, potential immune-mediated disease
Colindres R. Safety summary of investigational vaccine: SHINGRIX (SHINGRIX). ACIP February 22, 2017 [last accessed 2017 June]. Available from:
www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf
Prepared October 2017
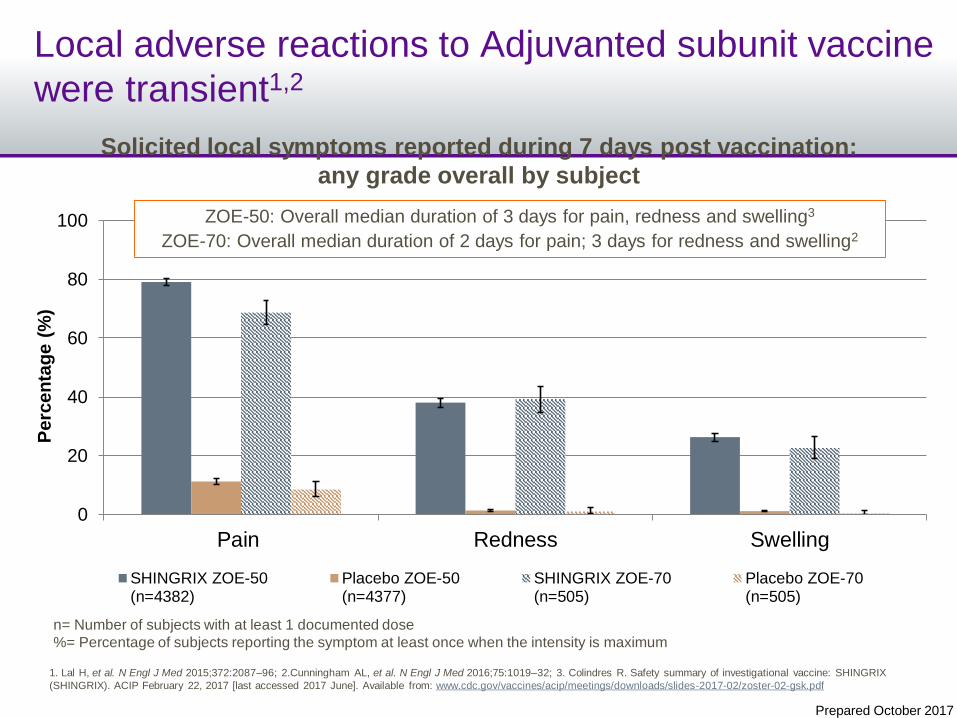
Local adverse reactions to Adjuvanted subunit vaccine
were transient1,2
Solicited local symptoms reported during 7 days post vaccination:
any grade overall by subject
0
20
40
60
80
100
Pain Redness Swelling
SHINGRIX ZOE-50(n=4382)
Placebo ZOE-50(n=4377)
SHINGRIX ZOE-70(n=505)
Placebo ZOE-70(n=505)
ZOE-50: Overall median duration of 3 days for pain, redness and swelling3
ZOE-70: Overall median duration of 2 days for pain; 3 days for redness and swelling2
Perc
en
tag
e (
%)
n= Number of subjects with at least 1 documented dose
%= Percentage of subjects reporting the symptom at least once when the intensity is maximum
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX
(SHINGRIX). ACIP February 22, 2017 [last accessed 2017 June]. Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf
Prepared October 2017
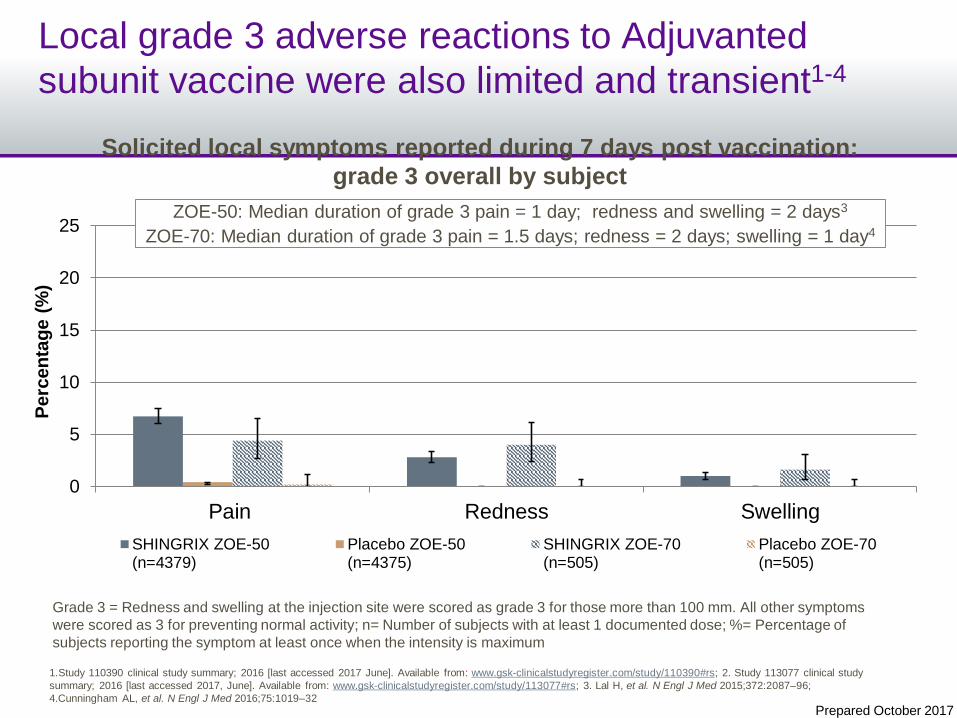
Local grade 3 adverse reactions to Adjuvanted
subunit vaccine were also limited and transient1-4
0
5
10
15
20
25
Pain Redness Swelling
SHINGRIX ZOE-50(n=4379)
Placebo ZOE-50(n=4375)
SHINGRIX ZOE-70(n=505)
Placebo ZOE-70(n=505)
Solicited local symptoms reported during 7 days post vaccination:
grade 3 overall by subject
ZOE-50: Median duration of grade 3 pain = 1 day; redness and swelling = 2 days3
ZOE-70: Median duration of grade 3 pain = 1.5 days; redness = 2 days; swelling = 1 day4
Perc
en
tag
e (
%)
Grade 3 = Redness and swelling at the injection site were scored as grade 3 for those more than 100 mm. All other symptoms
were scored as 3 for preventing normal activity; n= Number of subjects with at least 1 documented dose; %= Percentage of
subjects reporting the symptom at least once when the intensity is maximum
1.Study 110390 clinical study summary; 2016 [last accessed 2017 June]. Available from: www.gsk-clinicalstudyregister.com/study/110390#rs; 2. Study 113077 clinical study
summary; 2016 [last accessed 2017, June]. Available from: www.gsk-clinicalstudyregister.com/study/113077#rs; 3. Lal H, et al. N Engl J Med 2015;372:2087‒96;
4.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Prepared October 2017
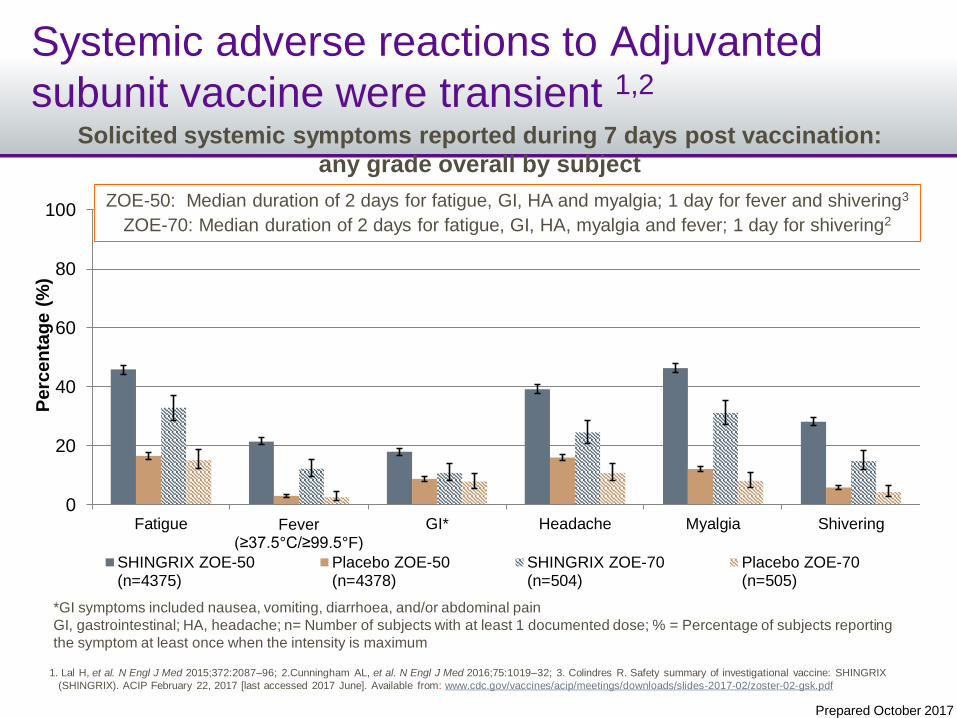
Systemic adverse reactions to Adjuvanted
subunit vaccine were transient 1,2
0
20
40
60
80
100
Fatigue Fever (≥37.5°C/≥99.5°F)
GI* Headache Myalgia Shivering
SHINGRIX ZOE-50(n=4375)
Placebo ZOE-50(n=4378)
SHINGRIX ZOE-70(n=504)
Placebo ZOE-70(n=505)
Solicited systemic symptoms reported during 7 days post vaccination:
any grade overall by subject
Perc
en
tag
e (
%)
ZOE-50: Median duration of 2 days for fatigue, GI, HA and myalgia; 1 day for fever and shivering3
ZOE-70: Median duration of 2 days for fatigue, GI, HA, myalgia and fever; 1 day for shivering2
*GI symptoms included nausea, vomiting, diarrhoea, and/or abdominal pain
GI, gastrointestinal; HA, headache; n= Number of subjects with at least 1 documented dose; % = Percentage of subjects reporting
the symptom at least once when the intensity is maximum
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX
(SHINGRIX). ACIP February 22, 2017 [last accessed 2017 June]. Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf
Prepared October 2017
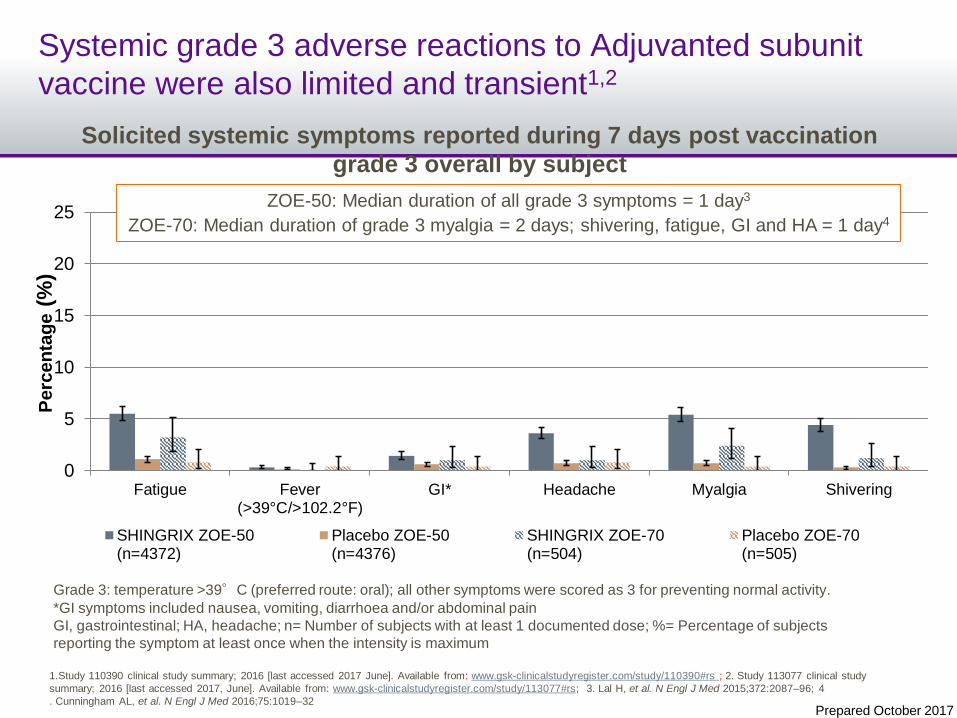
Systemic grade 3 adverse reactions to Adjuvanted subunit
vaccine were also limited and transient1,2
0
5
10
15
20
25
Fatigue Fever(>39°C/>102.2°F)
GI* Headache Myalgia Shivering
SHINGRIX ZOE-50(n=4372)
Placebo ZOE-50(n=4376)
SHINGRIX ZOE-70(n=504)
Placebo ZOE-70(n=505)
Perc
en
tag
e(%
)
ZOE-50: Median duration of all grade 3 symptoms = 1 day3
ZOE-70: Median duration of grade 3 myalgia = 2 days; shivering, fatigue, GI and HA = 1 day4
Grade 3: temperature >39°C (preferred route: oral); all other symptoms were scored as 3 for preventing normal activity.
*GI symptoms included nausea, vomiting, diarrhoea and/or abdominal pain
GI, gastrointestinal; HA, headache; n= Number of subjects with at least 1 documented dose; %= Percentage of subjects
reporting the symptom at least once when the intensity is maximum
1.Study 110390 clinical study summary; 2016 [last accessed 2017 June]. Available from: www.gsk-clinicalstudyregister.com/study/110390#rs ; 2. Study 113077 clinical study
summary; 2016 [last accessed 2017, June]. Available from: www.gsk-clinicalstudyregister.com/study/113077#rs; 3. Lal H, et al. N Engl J Med 2015;372:2087‒96; 4
. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Solicited systemic symptoms reported during 7 days post vaccination
grade 3 overall by subject
Prepared October 2017
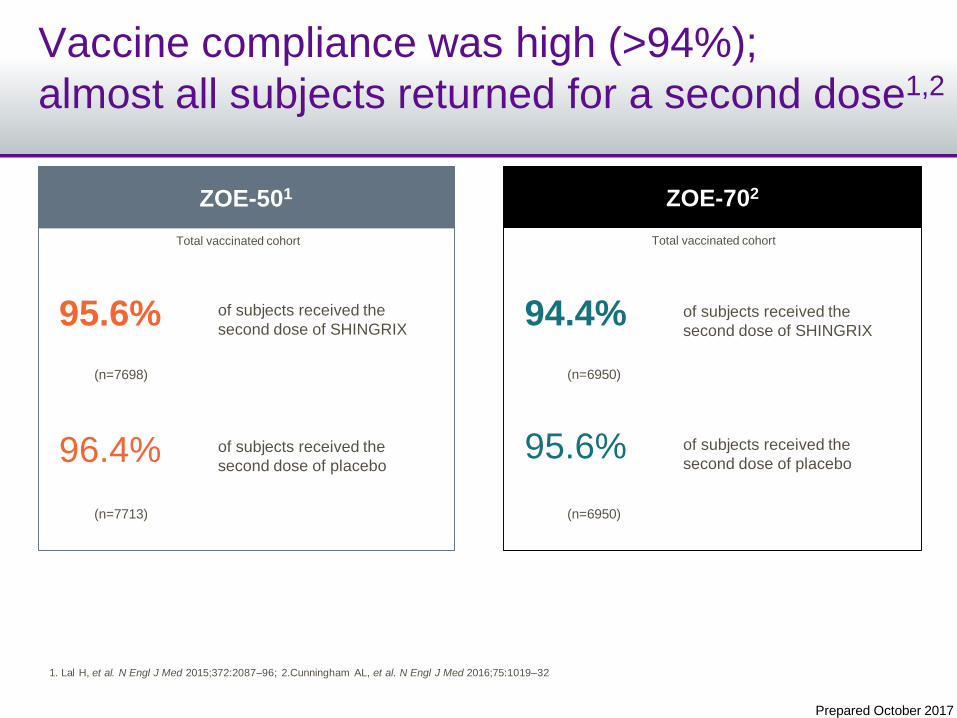
Vaccine compliance was high (>94%);
almost all subjects returned for a second dose1,2
N = 7698
ZOE-501
of subjects received the
second dose of SHINGRIX95.6%
of subjects received the
second dose of placebo96.4%
Total vaccinated cohort
(n=7698)
(n=7713)
ZOE-702
of subjects received the
second dose of SHINGRIX94.4%
of subjects received the
second dose of placebo95.6%
Total vaccinated cohort
(n=6950)
(n=6950)
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
Prepared October 2017
Summary: safety and adverse reactionsBased on available data, the benefit: risk profile for
Adjuvanted subunit vaccine is favourable
Safety data from the SHINGRIX clinical program has not detected any safety
signals, and the benefit of SHINGRIX outweighs the risk1
Overall incidences of SAEs, deaths and pIMDS were similar between SHINGRIX and
placebo (no imbalances overall or within any time frame)1
The most frequently reported symptom was pain at the injection site; myalgia,
fatigue and headache were the most frequently reported general symptoms2,3
The majority of reactions, both local and systemic, were mild to moderate in intensity
and of short duration (1‒3 days)2,3
– z
–z
–z
Vaccine compliance with 2 doses was high (>94%)2,3
–z
1. Colindres R. Safety summary of investigational vaccine: SHINGRIX (HZ/su). ACIP February 22, 2017 [last accessed 2017 June]. Available from:
www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf ; 2. Lal H, et al. N Engl J Med 2015;372:2087‒96; 3.Cunningham AL, et al. N Engl J Med
2016;75:1019‒32
Prepared October 2017
1.Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX (HZ/su). ACIP February 22, 2017 [last accessed 2017 June].
Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf ; 4. Study 113077 clinical study summary; 2016 [last accessed 2017, June]. Available from: www.gsk-
clinicalstudyregister.com/study/113077#rs; 5. Study 110390 clinical study summary; 2016 [last accessed 2017 June]. Available from: www.gsk-clinicalstudyregister.com/study/110390#rs
Summary: efficacy and safety in pivotal Phase III programAdjuvanted subunit vaccine provided efficacy across all age groups ≥50 years of age with an
acceptable safety and tolerability profile
>90% efficacy shown in all age groups ‒from 50 to over 80 years of age
(pooled data from 2 pivotal phase 3 trials)1,2
There was no significant decline in efficacy during an ongoing follow-up period
(mean 3.8 years),2 and immunogenicity was maintained for at least 9 years3
SHINGRIX eliminated almost all occurrences of PHN 2,4
Adverse reactions were mostly transient and of mild-to-moderate intensity, with a
median duration of 3 days2,3,4,5
– z
– z
– z
Efficacy
Adverse Reactions
– z
Prepared October 2017
Is HZ a Risk Factor for Stroke?
HZ as a Risk Factor for Stroke
• There are 5 studies demonstrating an increased
risk of stroke following an episode of HZ (see
following slides)
• Greatest risk is in the first 2 weeks
– Risk Ratio 1.31 - 2.27
• Risk increases with cases of HZ ophthalmicus
– Risk Ratio = 4.29
Stroke: Theoretical Mechanisms
“VZV is the only human virus that has been proven
to replicate in cerebral arteries and produce stroke”
Thrombosis,
occlusions,
infarctions,
aneurysms,
hemorrhage
Viral infection
Damages and
weakens cerebral
artery walls
Nagel M, et al. Clin Infect Dis 2014; 58(11):1504-6.Sreenivasan N, et al. PLoS ONE 2013; 8(7):e69156.
Rationale for HZ Vaccination
• Inform your patients
• Should be an incentive for you to offer vaccine
• Should be an incentive for patient to accept
Acute Zoster Pain• Loss of work
• Reduced quality of life
This should be
enough
• PHN• Ocular complications
• Scarring
• Super infections
Stroke
Emerging Risk Factors for HZ:
Chronic Obstructive Pulmonary
Disease (COPD)
COPD as a Risk Factor for HZ
• 4 studies assessing the risk of HZ in
patients with COPD
– 1 study showed little to no risk of HZ:
OR = 1.05 (0.96-1.14)
– 3 studies showed a significant increase in
risk of HZ in patients with COPD: risk
increase ranges from 1.32 to 1.85
Risk-based Approach: COPD
COPD should be a trigger/opportunity for you
to offer vaccination:
– Patient is at higher risk
– Quick discussion for you
– Patient more likely to accept because they
understand their condition and how it makes
them prone to complications
Emerging Risk Factors for HZ:
Diabetes
Diabetes as a Risk Factor for HZ
• 6 studies demonstrated that diabetes is a risk factor for HZ
– Risk ranges from 1.17 to 3.30
• 1 study showed risk associated with type 1 (OR = 1.27) but
not type 2 (OR = 1.01) diabetes
– However, “The lack of effect found with type 2 diabetes must be
interpreted cautiously, as negative confounding by ethnic group is
possible”
• The type 2 diabetes population may have included South Asian patients,
known to be at lower risk of HZ and higher risk of diabetes
Risk-based Approach: Diabetes
• Diabetes should be a trigger/opportunity for
you to offer vaccination:
– Patient is at higher risk
– Quick discussion for you because they
understand their condition and how it makes
them prone to complications
Emerging Risk Factors for HZ:
Statin Use
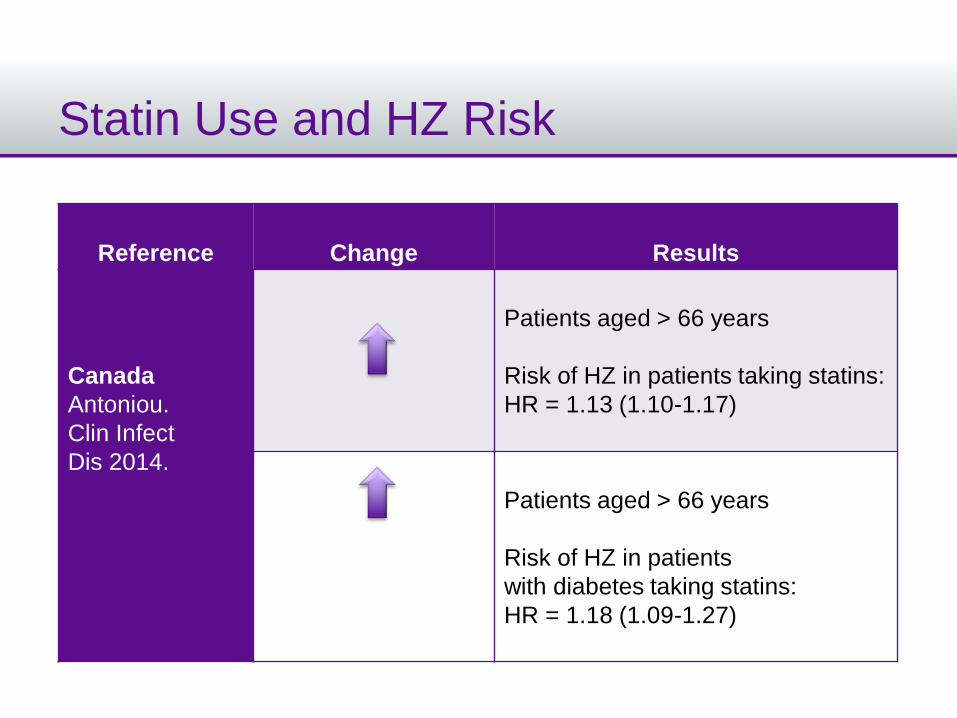
Statin Use and HZ Risk
Reference Change Results
Canada
Antoniou.
Clin Infect
Dis 2014.
Patients aged > 66 years
Risk of HZ in patients taking statins:
HR = 1.13 (1.10-1.17)
Patients aged > 66 years
Risk of HZ in patients
with diabetes taking statins:
HR = 1.18 (1.09-1.27)
Take-home Messages
• Every visit is a vaccine opportunity
• HZ vaccination should be offered to all patients older than
50 years
• However, a risk-based approach would be an excellent
start
– You have the skill
– They deserve to know
– They value your recommendation
• Immunization is your best medicine
Thank You
• Any Questions?