Embed Size (px)
Citation preview
An Update on Carotid Artery PTASAn Update on Carotid Artery PTASContemporary Results, Trends, and ChallengesContemporary Results, Trends, and Challenges
Matthew S. Edwards, M.D.Matthew S. Edwards, M.D.Assistant Professor of Surgery Assistant Professor of Surgery
Wake Forest University School of Wake Forest University School of MedicineMedicine
Winston-Salem, North CarolinaWinston-Salem, North Carolina
SAVS Postgraduate Course January 2006
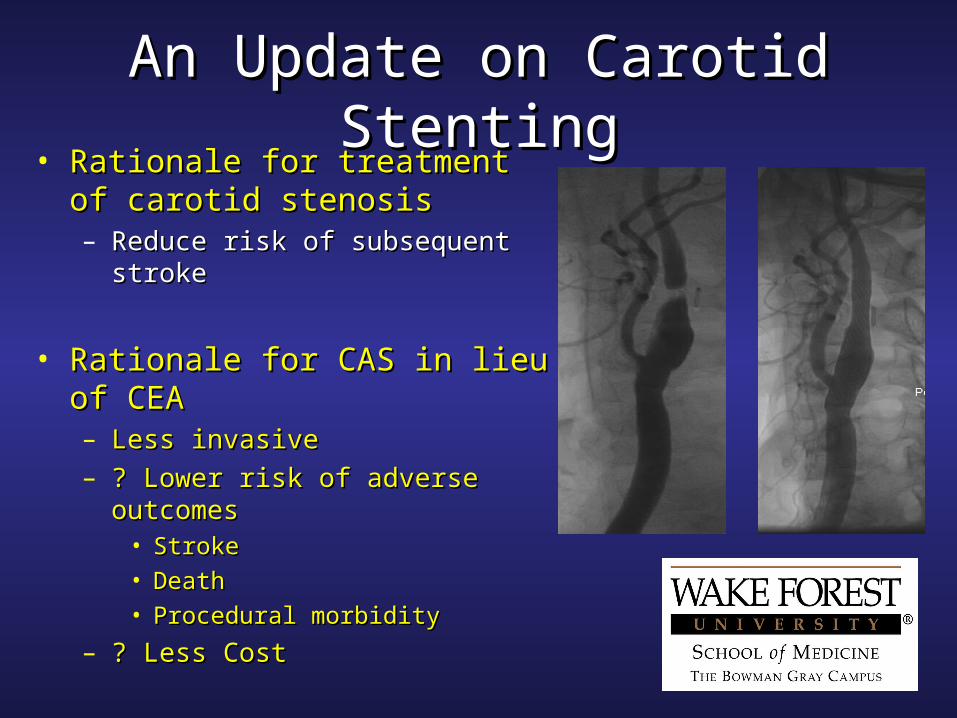
An Update on Carotid StentingAn Update on Carotid Stenting• Rationale for treatment of carotid Rationale for treatment of carotid
stenosisstenosis– Reduce risk of subsequent strokeReduce risk of subsequent stroke
• Rationale for CAS in lieu of CEARationale for CAS in lieu of CEA– Less invasiveLess invasive– ? Lower risk of adverse outcomes? Lower risk of adverse outcomes
• StrokeStroke
• DeathDeath
• Procedural morbidityProcedural morbidity
– ? Less Cost? Less Cost
Biller et al, Circulation 1998
An Update on Carotid StentingAn Update on Carotid Stenting• American Heart Association GuidelinesAmerican Heart Association Guidelines
– Asymptomatic PatientsAsymptomatic Patients• For treatment of 60% or greater stenosisFor treatment of 60% or greater stenosis
– Perioperative stroke/death must be less than 3%Perioperative stroke/death must be less than 3%
– Symptomatic PatientsSymptomatic Patients• For treatment of 50% or greater stenosisFor treatment of 50% or greater stenosis
– Perioperative stroke/death must be less than 6%Perioperative stroke/death must be less than 6%
– No proven indications beyond these thresholdsNo proven indications beyond these thresholds
An Update on Carotid StentingAn Update on Carotid Stenting
• Update on Contemporary DataUpdate on Contemporary Data– Clinical TrialsClinical Trials– Recent CREST ResultsRecent CREST Results– Cochrane ReviewCochrane Review
• Update on Contemporary TrendsUpdate on Contemporary Trends– Embolic ProtectionEmbolic Protection
• Update on Contemporary ChallengesUpdate on Contemporary Challenges– CredentialingCredentialing– Program establishmentProgram establishment
An Update on Carotid StentingAn Update on Carotid Stenting
Contemporary Trial Results
An Update on Carotid StentingAn Update on Carotid Stenting
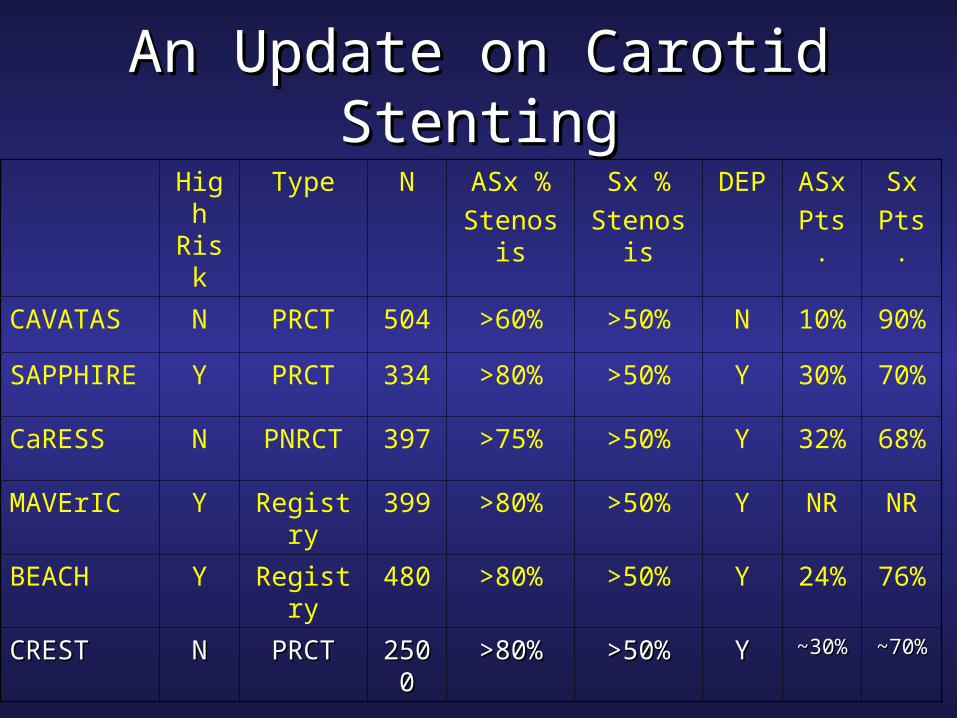
High Risk
Type N ASx %
Stenosis
Sx %
Stenosis
DEP ASx
Pts.
Sx
Pts.
CAVATAS N PRCT 504 >60% >50% N 10% 90%
SAPPHIRE Y PRCT 334 >80% >50% Y 30% 70%
CaRESS N PNRCT 397 >75% >50% Y 32% 68%
MAVErIC Y Registry 399 >80% >50% Y NR NR
BEACH Y Registry 480 >80% >50% Y 24% 76%
CRESTCREST NN PRCTPRCT 25002500 >80%>80% >50%>50% YY ~30%~30% ~70%~70%
An Update on Carotid StentingAn Update on Carotid Stenting
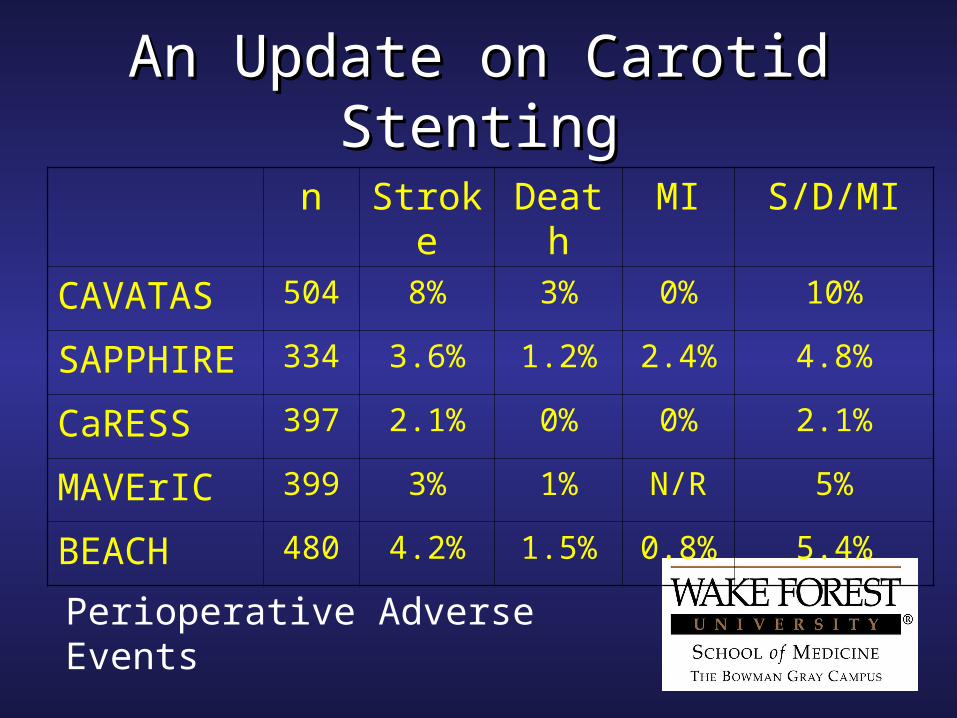
n Stroke Death MI S/D/MI
CAVATAS 504 8% 3% 0% 10%
SAPPHIRE 334 3.6% 1.2% 2.4% 4.8%
CaRESS 397 2.1% 0% 0% 2.1%
MAVErIC 399 3% 1% N/R 5%
BEACH 480 4.2% 1.5% 0.8% 5.4%
Perioperative Adverse Events
An Update on Carotid StentingAn Update on Carotid Stenting
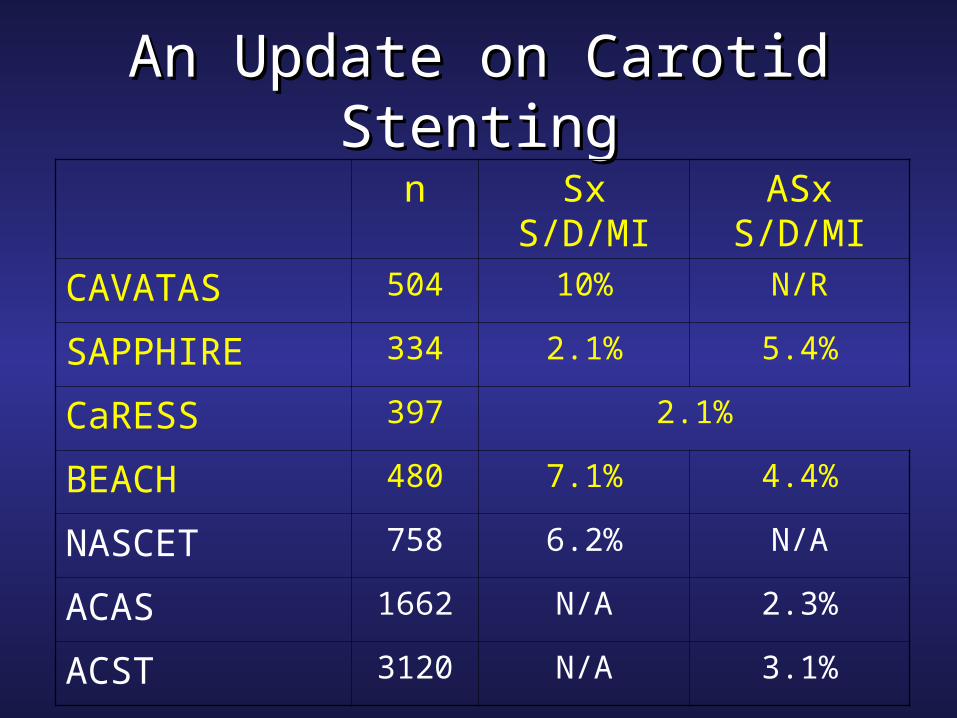
n Sx S/D/MI ASx S/D/MI
CAVATAS 504 10% N/R
SAPPHIRE 334 2.1% 5.4%
CaRESS 397 2.1%
BEACH 480 7.1% 4.4%
NASCET 758 6.2% N/A
ACAS 1662 N/A 2.3%
ACST 3120 N/A 3.1%
An Update on Carotid StentingAn Update on Carotid Stenting
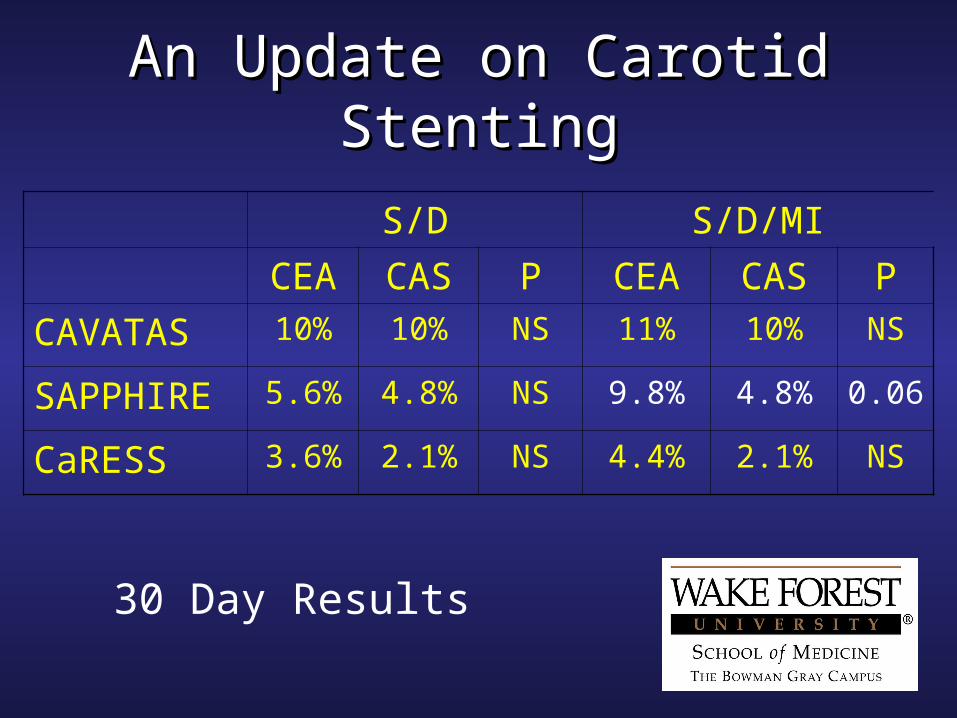
S/D S/D/MI
CEA CAS P CEA CAS P
CAVATAS 10% 10% NS 11% 10% NS
SAPPHIRE 5.6% 4.8% NS 9.8% 4.8% 0.06
CaRESS 3.6% 2.1% NS 4.4% 2.1% NS
30 Day Results

An Update on Carotid StentingAn Update on Carotid Stenting
S/D S/D/MI
CEA CAS P CEA CAS P
CAVATAS* 14.3% 14.2% NS N/R N/R N/A
SAPPHIRE 8.4% 5.5% NS 20.1% 12.2% 0.05
CaRESS 13.6% 10% NS 14.3% 10.9% NS
One (*Three) Year Results
Hobson et al, Journal of Vascular Surgery 2004
An Update on Carotid StentingAn Update on Carotid Stenting
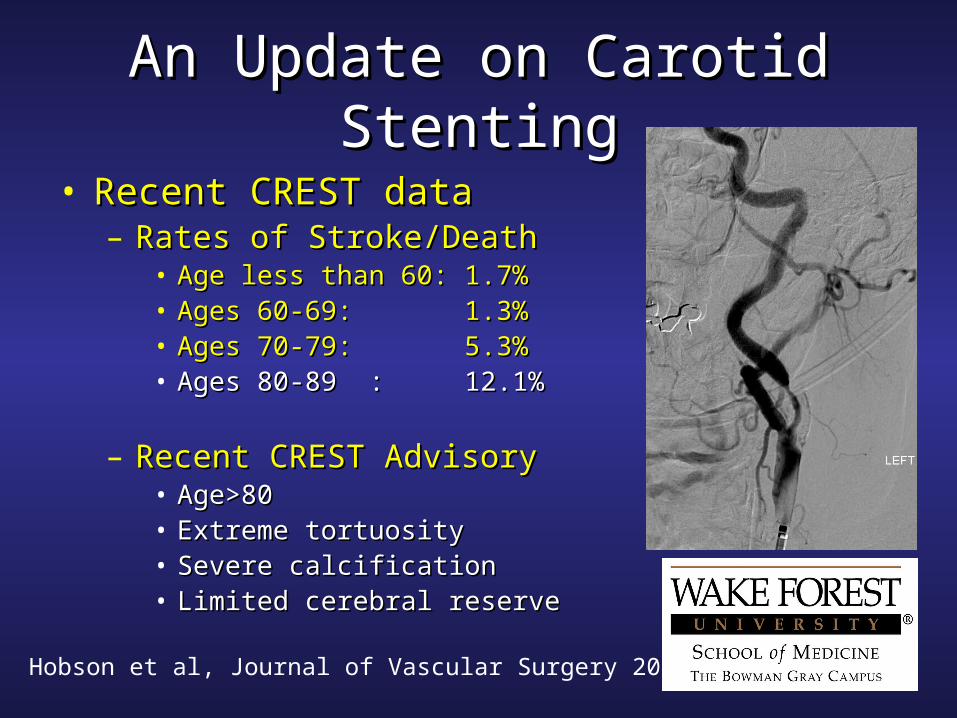
• Recent CREST data Recent CREST data – Rates of Stroke/DeathRates of Stroke/Death
• Age less than 60:Age less than 60: 1.7%1.7%• Ages 60-69:Ages 60-69: 1.3%1.3%• Ages 70-79:Ages 70-79: 5.3%5.3%• Ages 80-89Ages 80-89 :: 12.1%12.1%
– Recent CREST AdvisoryRecent CREST Advisory• Age>80Age>80• Extreme tortuosityExtreme tortuosity• Severe calcificationSevere calcification• Limited cerebral reserveLimited cerebral reserve
Coward et al, Stroke 2005
An Update on Carotid StentingAn Update on Carotid Stenting• Cochrane ReviewCochrane Review
– Essentially a meta-analysisEssentially a meta-analysis– Extensively used by Insurers and Health Plan Extensively used by Insurers and Health Plan
Managers in defining benefitsManagers in defining benefits– ConclusionsConclusions
• Insufficient evidence to recommend change in Insufficient evidence to recommend change in current practice of CEA as treatment of choicecurrent practice of CEA as treatment of choice
• CAS should only be offered as part of ongoing CAS should only be offered as part of ongoing randomized trials of CEA randomized trials of CEA vv CAS CAS
An Update on Carotid StentingAn Update on Carotid Stenting
Contemporary Trends and Controversies
An Update on Carotid StentingAn Update on Carotid Stenting
• Embolic ProtectionEmbolic Protection– Are emboli really a problem?Are emboli really a problem?– DEP devicesDEP devices
• Which is better?Which is better?– AnticoagulationAnticoagulation
• Heparin v BivalirudinHeparin v Bivalirudin• Antiplatelet agentsAntiplatelet agents
An Update on Carotid StentingAn Update on Carotid Stenting• Emboli- Are they really a problem?Emboli- Are they really a problem?
– Reasonable results in CAS without DEP but Reasonable results in CAS without DEP but CAVATAS strongly weighs in favor of useCAVATAS strongly weighs in favor of use
– Bibl, Neurology 2005Bibl, Neurology 2005
– Large volume of work demonstrating debris & Large volume of work demonstrating debris & infarctsinfarcts• Debris captured in 70-95% of casesDebris captured in 70-95% of cases
– Reimers et al, Am J Cardiol 2005; Hammer et al, JVS Reimers et al, Am J Cardiol 2005; Hammer et al, JVS 20052005
• 30-40% of CAS procedures demonstrate infarcts30-40% of CAS procedures demonstrate infarcts– Cosottini et al, Stroke 2005; Hammer et al, JVS 2005Cosottini et al, Stroke 2005; Hammer et al, JVS 2005
• Over half of infarcts ‘inconsistent’Over half of infarcts ‘inconsistent’
An Update on Carotid StentingAn Update on Carotid Stenting
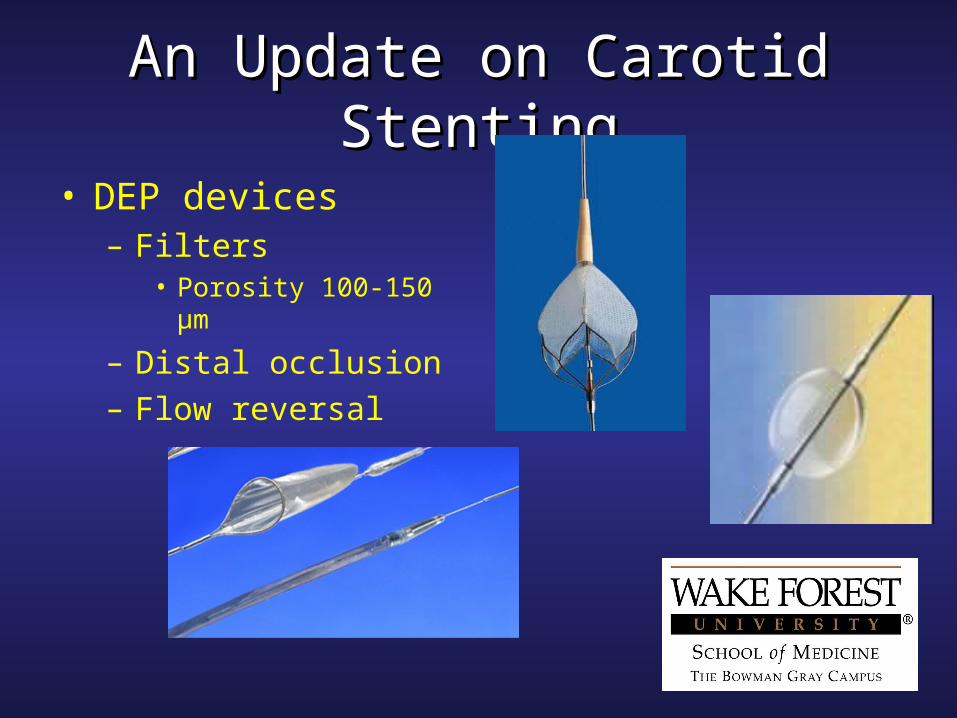
• DEP devices– Filters
• Porosity 100-150 µm
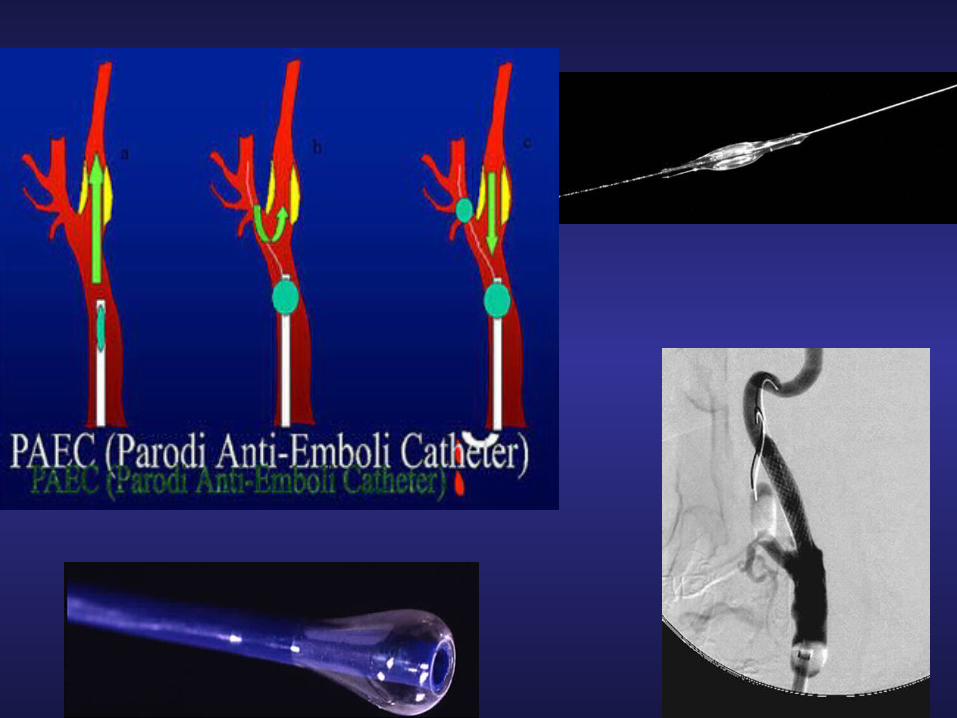
– Distal occlusion– Flow reversal
An Update on Carotid StentingAn Update on Carotid Stenting
• DEP use in CASDEP use in CAS– Accepted despite lack of level I evidenceAccepted despite lack of level I evidence– No controlled data demonstrating superior No controlled data demonstrating superior
efficacy of any particular designefficacy of any particular design– Several reviews suggest equivalent efficacy Several reviews suggest equivalent efficacy
for filters and distal occlusion DEPfor filters and distal occlusion DEP– Zahn et al, J Am Coll Cardiol 2005; Zahn et al, J Am Coll Cardiol 2005; – Arjomand et al J Am Coll Cardiol 2005Arjomand et al J Am Coll Cardiol 2005
An Update on Carotid StentingAn Update on Carotid Stenting
• Embolic Protection- Medical AdjunctsEmbolic Protection- Medical Adjuncts– Aspirin and clopidogrel accepted adjunctsAspirin and clopidogrel accepted adjuncts
• Use required in CRESTUse required in CREST• Most use 3-7 days prior Most use 3-7 days prior • Continue for at least 28 days postContinue for at least 28 days post• ASA lifetimeASA lifetime
– Glycoprotein IIbIIIa inhibitors Glycoprotein IIbIIIa inhibitors • Less efficacious than DEPLess efficacious than DEP• Higher risk of adverse outcomeHigher risk of adverse outcome
» Chan et al, Am J Cardiol 2005Chan et al, Am J Cardiol 2005
An Update on Carotid StentingAn Update on Carotid Stenting
Credentialing and Program Necessities
An Update on Carotid StentingAn Update on Carotid Stenting
Credentialing
An Update on Carotid StentingAn Update on Carotid Stenting
• CredentialingCredentialing– Highly politicized and contentiousHighly politicized and contentious– Two main sets of ‘consensus’ documentsTwo main sets of ‘consensus’ documents
• SVS/SCAI/SVMBSVS/SCAI/SVMB• ASITN/ASN/SIR/AAN/AANS/CNSASITN/ASN/SIR/AAN/AANS/CNS
– Local decisions still made at hospital levelLocal decisions still made at hospital level– Major pointsMajor points
• Cognitive SkillsCognitive Skills• Technical SkillsTechnical Skills• Clinical SkillsClinical Skills
Creager MA, Vascular Medicine 2004; Clinical Competence Statement, Vascular Medicine 2005
• SCAI/SVMB/SVS Cognitive RequirementsSCAI/SVMB/SVS Cognitive Requirements– Pathophysiology of carotid artery disease and strokePathophysiology of carotid artery disease and stroke– Clinical manifestations of strokeClinical manifestations of stroke– Natural history of carotid artery diseaseNatural history of carotid artery disease– Associated pathologyAssociated pathology– Diagnosis of stroke and carotid artery diseaseDiagnosis of stroke and carotid artery disease– Angiographic anatomyAngiographic anatomy– Alternative treatment optionsAlternative treatment options– Case selectionCase selection– Role of post procedure f/u and surveillanceRole of post procedure f/u and surveillance
Creager MA, Vascular Medicine 2004; Clinical Competence Statement, Vascular Medicine 2005.
• SCAI/SVMB/SVS Technical RequirementsSCAI/SVMB/SVS Technical Requirements– Expertise with antiplatelet therapy and procedural Expertise with antiplatelet therapy and procedural
anticoagulationanticoagulation– Angiographic skillsAngiographic skills– Interventional skillsInterventional skills– Recognition and management of procedural complicationsRecognition and management of procedural complications
• Cerebrovascular eventsCerebrovascular events• Cardiovascular eventsCardiovascular events• Vascular access eventsVascular access events
– Management of vascular accessManagement of vascular access
Creager MA, Vascular Medicine 2004; Clinical Competence Statement, Vascular Medicine 2005; Connors JJ, JVIR 2004.
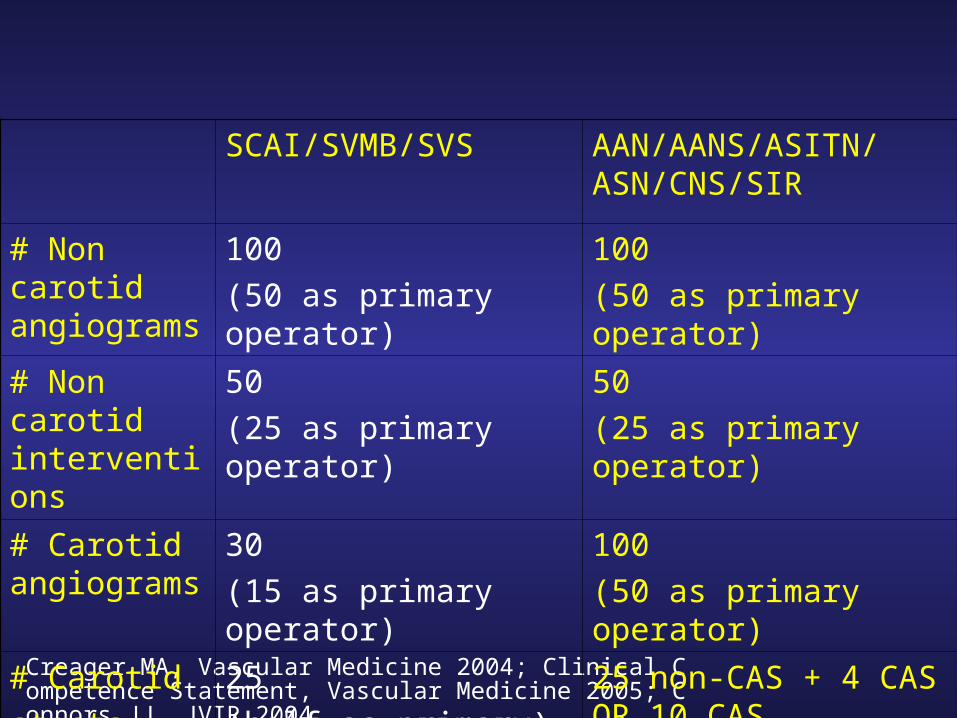
SCAI/SVMB/SVS AAN/AANS/ASITN/ASN/CNS/SIR
# Non carotid angiograms
100
(50 as primary operator)
100
(50 as primary operator)
# Non carotid interventions
50
(25 as primary operator)
50
(25 as primary operator)
# Carotid angiograms
30
(15 as primary operator)
100
(50 as primary operator)
# Carotid
stents
25
(half as primary)
25 non-CAS + 4 CAS OR 10 CAS
Creager MA, Vascular Medicine 2004; Clinical Competence Statement, Vascular Medicine 2005.
• Clinical SkillsClinical Skills– Determine the patient’s risk/benefit for the procedureDetermine the patient’s risk/benefit for the procedure– Outpatient responsibilitiesOutpatient responsibilities
• Medication managementMedication management• CounselingCounseling
– Inpatient responsibilitiesInpatient responsibilities– Coordination of post-stent surveillance and clinical Coordination of post-stent surveillance and clinical
outpatient follow-upoutpatient follow-up
An Update on Carotid StentingAn Update on Carotid Stenting
Program Necessities
CMS Manual System. Transmittal 531. April 2005.
An Update on Carotid StentingAn Update on Carotid Stenting
• Current Medicare CoverageCurrent Medicare Coverage– Patients at ‘high-risk’ for CEA and Patients at ‘high-risk’ for CEA and ≥70% ≥70%
carotid stenosis with symptomscarotid stenosis with symptoms– As part of Category B IDE clinical trials or As part of Category B IDE clinical trials or
post-approval trialspost-approval trials• 50% or greater carotid stenosis with symptoms50% or greater carotid stenosis with symptoms• 80% or greater carotid stenosis without symptoms 80% or greater carotid stenosis without symptoms
CMS Manual System. Transmittal 531. April 2005.
An Update on Carotid StentingAn Update on Carotid Stenting
• High risk for CEA defined as High risk for CEA defined as – Class III/IV CHFClass III/IV CHF– LVEF <30%LVEF <30%– Unstable anginaUnstable angina– Contralateral carotid occlusionContralateral carotid occlusion– Recent MIRecent MI– Previous CEA with recurrent stenosisPrevious CEA with recurrent stenosis– Prior neck radiationPrior neck radiation– COPDCOPD– Contralateral laryngeal nerve palsyContralateral laryngeal nerve palsy
CMS Manual System. Transmittal 531. April 2005.
An Update on Carotid StentingAn Update on Carotid Stenting
• Facility requirementsFacility requirements– High quality x-ray imagingHigh quality x-ray imaging– In-suite advanced physiologic monitoringIn-suite advanced physiologic monitoring– Emergency management equipment and Emergency management equipment and
personnelpersonnel– Clearly delineated program for granting privilegesClearly delineated program for granting privileges– Maintenance of data registry with at least biannual Maintenance of data registry with at least biannual
reviewsreviews– CMS certificationCMS certification
CMS Manual System. Transmittal 531. April 2005.
An Update on Carotid StentingAn Update on Carotid Stenting
• CMS certificationCMS certification– FDA approved site for prior IDE trialsFDA approved site for prior IDE trials
• SAPPHIRE, ARCHER, BEACHSAPPHIRE, ARCHER, BEACH
– FDA approved site for ongoing IDE trialsFDA approved site for ongoing IDE trials• CRESTCREST
– FDA approved site for post-approval studies FDA approved site for post-approval studies
CMS Manual System. Transmittal 531. April 2005.
An Update on Carotid StentingAn Update on Carotid Stenting• CMS certification (cont’d)CMS certification (cont’d)
– Written affidavit to CMS containingWritten affidavit to CMS containing• Facility name and addressFacility name and address• Facility Medicare provider numberFacility Medicare provider number• Point of contact and contact infoPoint of contact and contact info• Mechanism of data collection for CAS proceduresMechanism of data collection for CAS procedures
– http://www.vascularweb.org/http://www.vascularweb.org/_CONTRIBUTION_PAGES/Practice_Issues/_CONTRIBUTION_PAGES/Practice_Issues/Vascular_Registry/Carotid_Registry.htmlVascular_Registry/Carotid_Registry.html
• Signature of senior facility administrative official Signature of senior facility administrative official
?