Embed Size (px)
Citation preview

An Uncommon Cause of Major Lower Gastrointestinal Bleeding Abigail Kopecky, MD1 and Randall E Lee, MD, FACP2,1
1Department of Internal Medicine, University of California, Davis, Sacramento, CA 2Gastroenterology Section, Sacramento VA Medical Center, Mather, CA
CLINICAL COURSE
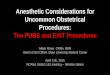
He had no recurrent bleeding. CT chest, abdomen,
and pelvis showed mixed density lesions in the
pelvis and L-spine, but no liver masses.
Chromogranin A was 8 nmol/L (0-5). Surgical
resection confirmed a 2-cm stage T2N0Mx primary
neuroendocrine tumor in the terminal ileum.
Octreotide scan showed no evidence of
metastases.
INITIAL PRESENTATION
HISTORY OF PRESENT ILLNESS:
A 61y.o. man with heavy alcohol use, on aspirin
for atrial fibrillation, presented to the ER with two
days of maroon stools streaked with bright red
blood. Associated postural presyncope. No
nausea, vomiting or abdominal pain.
PAST MEDICALHISTORY:
Two years ago, a routine screening colonoscopy
to the cecum noted hemorrhoids, diverticulosis,
and a 2-cm rectal neuroendocrine tumor,
completely excised on repeat endoscopy. No
follow up since then.
MEDICATIONS:
aspirin, metoprolol, hydrochlorothiazide, lisinopril
FAMILY HISTORY:
No GI or other malignancy.
PHYSICAL EXAM
● Obese male, no distress, hypotensive (BP
88/56, improved to 123/78 after 1L IV NS), HR 71
● Oropharynx was clear
● Abdomen was obese, soft, non-tender
● Maroon guaiac-positive stool on rectal exam
INVESTIGATIVE STUDIES
LABS: CBC showed hemoglobin of 10 g/dL, which was
a drop of 4 g/dL from baseline. Platelet count, INR, and
LFTs were within normal limits.
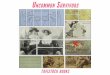
EGD and colonoscopy with ileoscopy within 24 hours
of admission determined the source of the bleeding
was a round, friable, vascular mass in the ileum, less
than 10 cm from the ileocecal valve.
INTRODUCTION
Major lower gastrointestinal bleeding usually is
due to colonic diverticulosis or angioectasia. This
case describes an uncommon cause of significant
bleeding from the small intestine.
DISCUSSION
● Neuroendocrine tumors most commonly occur in
the GI tract, and the most common GI location is
the ileum. Most small bowel NETs initially are
asymptomatic or have vague symptoms and
usually are an incidental endoscopic finding; a
major lower GI bleed is a rare presentation.
● The "carcinoid syndrome" of chronic diarrhea and
flushing was not seen in this case, and is present
only in a minority of cases. It classically is seen
when carcinoid tumors arising from the midgut
have metastasized to the liver, with secretion of
serotonin and other vasoactive substances directly
into systemic circulation.
● While routine screening colonoscopy often does
not examine the ileum, this case illustrates the
critical importance of ileoscopy during colonoscopy
for an initial GI bleed evaluation.
REFERENCES
American Joint Committee on Cancer (AJCC) Staging Manual, 7th Ed, Edge SB, Byrd DR,
Compton CC, et all (Eds), Springer New York 2010.
Goldfinger SE and JR Strosberg, et al. Clinical characteristics of carcinoid tumors. In:
UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA 2012.
Kulke MH, Mayer RJ. Carcinoid tumors. New England Journal of Medicine 1999; 340:858.
Oberg K. Carcinoid Tumors: Current Concepts in Diagnosis and Treatment. The Oncologist
1998; 3:339-345.
Strate LL. Lower GI bleeding: epidemiology and diagnosis. Gastroenterology Clinics of
North America 2005; 34:643.
Ileal mass pre- and post-biopsy.
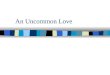
PATHOLOGY
Endoscopic biopsy of the mass showed a well-
differentiated neuroendocrine tumor (NET).
2X 40X