Embed Size (px)
Citation preview

An Unbiased Lipidomics ApproachIdentifies Early Second TrimesterLipids Predictive of MaternalGlycemic Traits and GestationalDiabetes MellitusDiabetes Care 2016;39:2232–2239 | DOI: 10.2337/dc16-0863
OBJECTIVE
To investigate the relationship between early second trimester serum lipidomicvariation and maternal glycemic traits at 28 weeks and to identify predictive lipidbiomarkers for gestational diabetes mellitus (GDM).
RESEARCH DESIGN AND METHODS
Prospective study of 817 pregnant women (discovery cohort, n = 200; validationcohort, n = 617) who provided an early second trimester serum sample and un-derwent an oral glucose tolerance test (OGTT) at 28 weeks. In the discovery co-hort, lipids were measured using direct infusion mass spectrometry andcorrelated with OGTT results. Variable importance in projection (VIP) scores wereused to identify candidate lipid biomarkers. Candidate biomarkers were mea-sured in the validation cohort using liquid chromatography–mass spectrometryand tested for associations with OGTT results and GDM status.
RESULTS
Early second trimester lipidomic variation was associated with 1-h postload glu-cose levels but not with fasting plasma glucose levels. Of the 13 lipid speciesidentified by VIP scores, 10 had nominally significant associations with postloadglucose levels. In the validation cohort, 5 of these 10 lipids had significant asso-ciations with postload glucose levels that were independent of maternal age andBMI, i.e., TG(51.1), TG(48:1), PC(32:1), PCae(40:3), and PCae(40:4). All except thelast were also associated with maternal GDM status. Together, these four lipidbiomarkers hadmoderate ability to predict GDM (area under curve [AUC] = 0.7160.04, P = 4.853 1027) and improved the prediction of GDM by age and BMI alonefrom AUC 0.69 to AUC 0.74.
CONCLUSIONS
Specific early second trimester lipid biomarkers can predict maternal GDM statusindependent of maternal age and BMI, potentially enhancing risk factor–basedscreening.
1Department of Paediatrics, University of Cam-bridge, Cambridge, U.K.2Medical Research Council Human Nutrition Re-search, Cambridge, U.K.3Medical Research Council Epidemiology Unit,University of Cambridge, Cambridge, U.K.4Wellcome Trust–Medical Research Council Insti-tute of Metabolic Science, Cambridge, U.K.
Corresponding author: David B. Dunger, [email protected].
Received 21 April 2016 and accepted 10 September2016.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc16-0863/-/DC1.
© 2016 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Liangjian Lu,1 Albert Koulman,2
Clive J. Petry,1 Benjamin Jenkins,2
Lee Matthews,2 Ieuan A. Hughes,1
Carlo L. Acerini,1 Ken K. Ong,1,3 and
David B. Dunger1,4
2232 Diabetes Care Volume 39, December 2016
EPIDEM
IOLO
GY/HEA
LTHSERVICES
RESEA
RCH

Gestational diabetes mellitus (GDM) af-fects 9–26% of pregnancies (1). It is clin-ically important because it increases therisk of obstetric complications (e.g., pre-eclampsia and shoulder dystocia), aswell as neonatal complications (e.g., hy-poglycemia and hyperbilirubinemia). Inthe multicenter Hyperglycemia andAdverse Pregnancy Outcome (HAPO)study, a continuous linear relationshipwas shown between maternal glucoselevels at 24–32 weeks of gestation andthe odds of several adverse pregnancyoutcomes, even for glucose levels wellwithin the normal range (2). This hasprovided impetus for the InternationalAssociation of the Diabetes and Preg-nancy Study Groups (IADPSG) to recom-mend universal screening for GDM viathe 75-g oral glucose tolerance test(OGTT)between24and28weeksgestation(3).This recommendation by the IADPSG
has not been uniformly adopted be-cause of various concerns, includingthe implications for service provisionand the large number of normoglycemicwomen who will have to undergo whatcan be an unpleasant and poorly toler-ated test (4). Some countries, such asthe U.K. (4) and Italy (5), perform riskfactor–based screening, with only high-risk individuals undergoing the diag-nostic 75-g OGTTs. Specified risk factorsinclude obesity, previous macrosomicbaby, previous GDM, family history ofdiabetes, and minority ethnic family ori-gin with high prevalence of diabetes. Inthe U.S., the American Diabetes Associa-tion and American Congress of Obstetri-cians and Gynecologists continue toendorse a two-step approach with aninitial universal nonfasted 50-g glu-cose load test at 24–28 weeks of gesta-tion (6).Another recognized limitation of
screening for GDM at 24–28 weeks ofgestation is the delay in detecting casesof GDM that developed in the first orearly second trimesters. By the time ofscreening, significant increased fetal ad-iposity may have developed (4,7,8). Al-though performed in a high-risk ethnicminority population, Agarwal et al. (9)showed that .40% of cases of GDMcould be diagnosed by a 75-g OGTT per-formed before 18 weeks of gestation.These limitations of universal 24- to28-week OGTT support the potentialvalue of predictive early gestational
biomarkers for GDM. The biomarkersthat have been studied include fastingplasma glucose (9) and, more recently,maternal metabolites (10,11), plasmaproteins (12), and microRNA (13) usinghigh-throughput technologies. Althoughthese efforts have not yet informed clin-ical strategies, the results of metabolomicstudies in particular have provided valu-able insights into the pathophysiology ofGDM (11,14).
Variations in lipid profiles have yet tobe comprehensively studied, even thoughchanges in maternal lipid metabolism arewell described from the beginning ofpregnancy (15). In early pregnancy, levelsof plasma lipids, including triglycerides(TGs), phospholipids, and cholesterol, de-crease before steadily increasing fromweek 8 onward (15). The rise in TGs isaccompanied by an increase in VLDL,LDL, and HDL levels (16). Changes in lipidlevels during GDM have also been ob-served, withwomenwho haveGDMhav-ing higher serum TG levels but lower LDLlevels compared with normoglycemicpregnant women (17).
Therefore, we hypothesized that lipi-domic variation in early second trimes-ter maternal serum samples could beassociated with later glucose tolerancemeasured at 28 weeks. Confirmation ofthis hypothesis would enable the iden-tification of candidate lipid biomarkersthat are predictive of GDM, so as toimprove GDM screening and providemechanistic insights into the patho-physiology of GDM.
RESEARCH DESIGN AND METHODS
Recruitment and Sample CollectionThe Cambridge Baby Growth Study(CBGS) is a prospective longitudinalstudy that has been described previously(18–20). Briefly, 2,212 women in earlypregnancy were recruited between2001 and 2009 from ultrasound clinicsat the Rosie Maternal Hospital, Cam-bridge, U.K. Such dating scans are rou-tinely offered to all pregnant womenreceiving antenatal care and are per-formed at 8–14 weeks of gestation.
Shortly after recruitment, at 15.2 60.07 weeks of gestation, a nonfastingvenous blood sample was collected ifwomen consented. After clotting andwithin 2 h of sample collection, thesesamples were centrifuged at 3,000gfor 10 min, and the serum was sepa-rated and stored at 280°C. They were
maintained at 280°C until analysis,with the exception of a single freeze-thaw cycle to prepare the necessary ali-quots for lipid analysis. A total of 1,260serum samples were collected.
All participants were also invited toundergo a standard 75-g OGTT, whichwas performed at 28 weeks of gestationafter an overnight fast. A total of 1,069women underwent the OGTT. Plasmaglucose levels were analyzed by thestandard glucose oxidase method.
Cohort SelectionFor this study, we excluded OGTT partici-pants who 1) were missing fasting or 1-hpostload venous plasmaglucose levelmea-surements (n = 10), 2) subsequently gavebirth to twins (n = 17), or 3) did not providean early second trimester serum sample(n = 219). A very small number of partici-pants (n = 6)were also excluded for variousother reasons (e.g., inadequate remainingserum samples, no paired DNA sample foruse in other studies). This yielded a total of817 women, who were assigned to a dis-covery cohort of 200 women and a valida-tion cohort of 617 women. Women in thediscovery cohort were selected becausethey had data on other genetic or pheno-typic traits, which other ongoing studies inour group were interested in correlatingwith lipidomic variation.
There were two differences in clinicalcharacteristics between the discoveryand validation cohorts. First, 1-h post-load glucose levels were 0.27 mmol/Lhigher in the validation cohort (Table1). This result was of borderline signifi-cance on univariate testing (P = 0.05)and was nonsignificant when multipletesting was accounted for using theBenjamini-Hochberg method (P = 0.175).Importantly, there was no significant dif-ference in the proportion of case patientswith GDM in the two groups. Second,samples were obtained in the validationcohort at a slightly later point in gestation,;0.5 weeks later.
Ethical ApprovalThe study protocol was approved bythe local research ethics committee,Addenbrooke’s Hospital, Cambridge,U.K. Written informed consent was ob-tained from all participants.
Lipid Biomarker AnalysesIn thediscovery cohort, the lipidswerepro-filed by direct infusion mass spectrome-try as described previously (21,22). For
care.diabetesjournals.org Lu and Associates 2233

biomarker validation, we used a liquidchromatography–mass spectrometry (LC-MS) method as described previously (23).
Statistical AnalysisPartial least squares (PLS) regression andPLS-discriminant analysis (DA) were usedto identify associations between lipido-mics variables and OGTT results in thediscovery cohort. Fittedmodelswere con-sidered significant if the value of Q2 (i.e.,R2 of the model as estimated by cross-validation) was positive. The importanceof individual lipid species was quantifiedvia the variable importance in projection(VIP) score and used to identify candidatelipid biomarkers. The VIP score is a widelyusedmethodof variable selection. It takesinto account the amount of Y varianceexplained by the projection and the load-ings of each variable on this projection,while adjusting for the absolute magni-tude of each X variable. As such, two var-iables with identical contributions to theexplanatory power of the model will haveidentical VIP scores, regardless of whichcomponent they have a large influence onor their absolute magnitudes.Standard linear and logistic regression
techniques were used to assess the associ-ation between candidate lipid biomarkersand maternal OGTT results or GDM status.GDMwas defined based on fasting and 1-hpostload glucose levels using IADPSGthresholds (i.e.,$5.1 and 10.0mmol/L, re-spectively). The 2-h postload data wereunavailable for most women and were
omitted fromour casedefinition for unifor-mity. This is acceptable because only 7% ofU.K. women with GDM receive a diagnosisbased on the 2-h measurement alone (1).
Logistic regression was used to com-bine the predictive ability of candidatelipid biomarkers, which was then as-sessed using receiver operating charac-teristic (ROC) plots. Where backwardstepwise selection was used, a signifi-cance threshold of 0.10 for removalwas used. Linear DA was used to ensurethe robustness of these results.
The threshold for statistical significancewas 0.05. For the discovery cohort, uncor-rected P valueswere considered,whereasin the validation cohort P valueswere cor-rected for multiple testing using theBenjamini-Hochberg method. Values inthe text are given as the mean 6 SE,unless otherwise specified. Regressioncoefficients were standardized by thepredictor (i.e., change in response vari-able for each SD increase in thepredictor).
PLS and PLS-DA regressions were per-formed using SIMCA version 14 (MKSUmetrics AB, Umea, Sweden). All otheranalyses were performed using SPSS ver-sion 21 (IBM, Armonk, NY).
RESULTS
Association Between Early SecondTrimester Lipidomic Variation and28-Week Glucose ToleranceAnalysis of the discovery cohort was con-fined to 196 samples because 4 samples
were found to be unsuitable for analy-sis due to hemolysis. In these samples,189 lipid species were detected.
APLSmodelwas constructed toexaminethe extent to which early second trimesterlipidomic variation explained postload ve-nous glucose levels during an OGTT at28 weeks of gestation. The resulting modelyielded one fitted component, which used15% of lipidomic variation (R2X) to explain11% (R2Y) of variation in postload glucoselevels. This was robust to internal cross-validation, yielding a Q2 value of 4%.
Because some lipid species may shownonlinear relationships with postload glu-cose levels, we divided participants intotertiles of OGTT levels and constructed aPLS-DA model to explain membership inthe top tertile. The resulting model alsoyielded a single component, which used15% of lipidomic variation to explain 9%of the variation in top tertilemembership,with a Q2 value of 1.31%.
Similar PLS and PLS-DA models werealso constructed to explore the relation-ship between lipidomic variation and fast-ing plasma glucose levels. However, themodels were overfitted, with the PLS andPLS-DAmodels yieldingQ2 values of23%(R2X = 15%, R2Y = 9%) and 210% (R2X =9%, R2Y = 8%), respectively. Thesemodelswere not used in subsequent analyses.
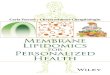
Identification of Lipid Biomarkers ofPostload Plasma Glucose LevelsFrom each of the two models consideringpostload glucose levels, ;10 lipids withthe highest VIP scores were selected,with the exact cut point selected using agraphic method (Fig. 1A and B). The PLSmodel yielded 9 lipid species, and thePLS-DA model yielded 10 lipid species,with 5 lipid species being identified inbothmodels.Oneof the species annotatedas diglyceride-water (DG-H2O[32:0]) waslikely to be an in-source fragment of a dif-ferent lipid species. As in-source fragmentsare artifacts of mass spectrometry, thisspecies was disregarded, leaving a totalof 13 lipid species identified.
The 13 lipid species were regressedagainst postload glucose levels or mem-bership in the top tertile thereof. Toensure that they were not simply surro-gates for known risk factors of GDM,maternal age and prepregnancy BMIwere adjusted for. This resulted in 10 ofthe 13 lipid species having a nominallysignificant association with postload glu-cose levels and/or the top tertile thereof
Table 1—Clinical characteristics of participants in the lipidomics study
Clinicalcharacteristics
AllOGTT
Lipidomicstotal
Discoverycohort
Validationcohort
P value (discoveryvs. validation
cohort)Mean SD Mean SD Mean SD Mean SD
Total participants (n) 1,069 817 200 617
Age (years) 33.39 4.19 33.27 4.11 33.38 3.83 33.22 4.21 0.65
MaternalprepregnancyBMI (kg/m2) 24.10 4.46 24.19 4.48 23.90 4.13 24.30 4.60 0.31
Maternal height (m) 1.66 0.07 1.66 0.07 1.66 0.07 1.66 0.07 0.22
Fasting glucoselevels (mmol/L) 4.33 0.55 4.33 0.49 4.33 0.53 4.32 0.47 0.93
1-h postload glucoselevels (mmol/L) 6.83 1.72 6.77 1.67 6.57 1.59 6.84 1.69 0.05
GDM (%) 9.45 8.20 6.50 8.75 0.38
Gestational age atserum samplecollection (years) 15.2 2.46 15.0 2.02 14.6 1.73 15.1 2.10 0.004
Fasting and postload glucose levels were measured using a standard OGTT at 28 weeks ofpregnancy. GDM was diagnosed based on fasting and 1-h postload venous plasma glucosemeasurements (details in text). Comparisons were performed using Student t test and x2 test forthe proportion of participants with GDM. P values were not corrected for multiple testing.
2234 Early Second Trimester Lipid Biomarkers of GDM Diabetes Care Volume 39, December 2016

(Supplementary Table 1). The two lipidspecies showing the strongest associa-tion with postload glucose levels wereTG(51:1) (0.40 mmol/L per SD increase, P =8.88E-4) and the choline ether phospho-lipid (PCae) PCae(40:3) (20.41 mmol/L
per SD increase, P = 9.73E-4) (Supple-mentary Table 2).
Further examinationof the correlationsamong these 10 lipid species revealedclustering into two large groups (Fig.1C). The first group contained the PCaes,
whereas the second group contained TGsand a phosphatidylcholine (PC).
Validation of Lipid Biomarkers ofPostload Plasma Glucose LevelsThese 10 candidate lipid biomarkers weremeasured in the validation set of 617 sub-jectsusinganLC-MSmethod.Thisprovidedadditional chromatographic information,eliminating any possible artifacts intro-duced by the shotgun approach in the dis-covery set. With this method, we wereunable to detect PCae(44:4) in our sam-ples, suggesting that this putative signalin the discovery set was an artifact, and itwas omitted from further analysis.We alsoomitted 20 samples in which none of theremaining nine lipid species were detect-able, as this was likely indicative of poorsample quality. This left data on the ninecandidate lipid biomarkers in 597 subjectsfor analysis.
Of the nine remaining lipid species, fiveshowed significant associations with post-load glucose levels, even after adjustmentfor maternal age and BMI and correctionfor multiple testing (Table 2). TG(51:1),TG(48:1), and PC(32:1) were positively as-sociated with maternal postload glucoselevels, whereas PCae(40:3) and PCae(40:4)were inversely associated with maternalpostload glucose levels. Logistic regres-sion againstmembership of the top tertileof postload glucose levels did not validateany additional candidate lipid species, nordid adjusting for gestational age at thetime of serum sample collection (datanot shown).
Because fasting and postload glucoselevels have common pathophysiologicaldeterminants andweremoderately corre-lated in our cohort (r = 0.343, P, 0.001),we tested the nine putative lipid bio-markers for an association with fastingglucose levels (data not shown). TG(51:1)and PCae(40:4) showed significant asso-ciations with fasting glucose levels, evenafter adjusting for multiple testing. How-ever, after adjusting for maternal age andBMI, only TG(51:1) remained significant(0.06 mmol/L per SD increase, P = 0.003;Benjamini-Hochberg test, P = 0.02).
Lipid Predictors of GDMOf the 597 subjects in the validation co-hort, 53 met the criteria for GDM. The fivevalidated lipid species were tested for as-sociation with GDM. TG(51:1), TG(48:1),PC(32:1), and PCae(40:4) were signifi-cantly associated with GDM, even after ad-justment for maternal age and maternal
Figure 1—Candidate lipid biomarkers identified from the discovery cohort. A and B: VIP scores ofindividual lipid species in a PLS model mapping early second trimester lipid profiles to latesecond trimester 1-h postload glucose levels. B: VIP scores of individual lipid species in a PLS-DAmodel mapping early second trimester lipid profiles to membership in the top tertile of latesecond trimester 1-h postload glucose levels. C: Correlation between 10 candidate lipid bio-markers taken forward to validation cohort. Underlined lipid species refer to species that hadnominally significant associations with 1-h postload glucose levels (A) or the top tertile thereof(B) and were taken forward to the validation cohort.
care.diabetesjournals.org Lu and Associates 2235

BMI and correction for multiple testing(Fig. 2A). While not reaching significance,PCae(40:3) nonetheless demonstrated astrong trend in the same direction asPCae(40:4) (Benjamini-Hochberg test,P value = 0.07).To assess the combined predictive
ability of these four lipid species, logisticregression was used to calculate the pro-bability of the GDM status of each subjectand the probability scores used to con-struct a ROC curve (Fig. 2B). This yieldeda mean area under the curve (AUC) of0.709 6 0.040 (P = 4.85E-7). Similar re-sults were obtained using linear DA.Of the 597 subjects, 410 (including
37 GDM case patients) had availabledata on maternal age and BMI. This en-abled us to assess the additional predic-tive power conferred by these four lipidbiomarkers over maternal age and BMIalone. In this subgroup, maternal ageand BMI produced a mean AUC of0.6896 0.046 (P = 1.54E-4), and furtherinclusion of the four lipid biomarkers in-creased the AUC to 0.741 6 0.045 (P =1.33E-6) (Fig. 2C). Graphically, the im-provement in AUC was most marked atstringent thresholds (i.e., enhancing thesensitivity at high levels of specificity).For instance, at 91.7% specificity, thesensitivity is 21.6% based on traditionalrisk factors but rose to 48.6% when lipidpredictors were included. In addition,there was some improvement at highlevels of sensitivity, for instance at97.3% sensitivity, where the inclusionof lipid predictors raised specificityfrom 9.9%, based on traditional risk fac-tors alone, to 24.9%.
Finally, we sought to identify the mostparsimonious model from these six po-tential predictive variables. Using a back-ward stepwise selection algorithm, theonly terms left in the model were mater-nal BMI, TG(48:1), and PCae(40:4). Thisyielded a mean AUC of 0.732 6 0.045(P = 3.28E-6),which is similar to themodelincluding all six predictors.
CONCLUSIONS
In this unselected cohort of predominantlyCaucasian pregnant women, using an un-biased lipidomics approach and a preas-signed validation cohort, we show for thefirst time that specific lipid species in thematernal early second trimester lipid pro-file are associated with maternal glycemictraits assessed by standard 75-g oral glu-cose tolerance testing at 28 weeks. Weidentified four lipid biomarkers, TG(51:1),TG(48:1), PC(32:1), and PCae(40:4), thatpredict later onset of GDM, independentofmaternal age andBMI, and could poten-tially enhance the performance of existingrisk factor–based screening approachesused in many countries.
The performance of clinical risk factor–based screening has been examined inmanydifferent populations. A recent study(24) in an Australian population com-pared the performance of the National In-stitute for Health and Care Excellence, theAmerican Diabetes Association, and theAustralasianDiabetes in Pregnancy Societyrisk factor–based screening guidelines,yielding sensitivities of 92%, 100%, and99% and specificities of 32.4%, 3.9%, and13.7%, respectively. This and other studiesreveal limited test performance with the
need for low levels of specificity to achievethe high levels of sensitivity.
The four lipid biomarkers that we iden-tified have moderate predictive perfor-mance, with an estimated AUC of 0.709.This is comparable to other early preg-nancy biomarkers, including conventionalbiomarker fasting levels of plasma glu-cose (estimated AUC = 0.579) (9), HbA1c(AUC in high risk population = 0.67) (25),TGs (AUC = 0.55–0.61), and TG-to-HDLratio (AUC = 0.62) (26), as well as novelbiomarkers, such as second trimester se-rum microRNA (AUC = 0.669) (13). Fur-thermore, the lipid biomarkers that wederivedwere specifically identified topre-dict GDM independent of maternalage and BMI, and thus can enhance thepredictive performance of existing riskfactor–based approaches. Indeed, the in-clusion of the four lipid biomarkers withmaternal age and BMI increased the AUCfrom 0.689 to 0.741.
The enhancement of sensitivity athigh levels of specificity was particularlymarked. Although for the purpose ofpredicting GDM our data on the clinicalperformance of lipid biomarkers mustbe considered very preliminary, lipidbiomarkers may potentially have a rolein identifying high-risk women whoshould undergo an immediate/earlysecond trimester OGTT.
The lipid biomarkers we identifiedcan be divided into two groups. TG(51:1),TG(48:1), and PC(32:1) are associatedwith increased postload glucose levelsand GDM risk and are moderately cor-related. PCae(40:3) and PCae(40:4) areassociated with decreased postload glu-cose levels and/or GDM risk and arestrongly correlated.
The association of TG(51:1), TG(48:1),and PC(32:1) withmaternal glucose levelsis consistent with previous investigationsinto lipidomic changes associated withtype 2 diabetes. TG(48:1) has been impli-cated with type 2 diabetes risk in the Fra-mingham cohort (27), and PC(32:1) levelswere raised in Australian Diabetes, Obe-sity and Lifestyle Study (AusDiab) subjectswith type 2 diabetes (28). These threelipid species are notable for the presenceof a single double bond, which implies thepresence of a monounsaturated fattyacid, predominantly palmitoleate and,to a lesser extent, oleate, on closer in-spection of LC-MS spectra in our analysis.In one study (29), palmitoleate contentwithin circulating phospholipids was
Table 2—Relationship between candidate lipid biomarkers and second trimester1-h postload glucose levels in the validation cohort
Lipid species
Univariate analysis Adjusted for maternal age and BMI
Regressioncoefficient(mmol/L/SD) P value BH P value
Regressioncoefficient(mmol/L/SD) P value BH P value
TG(51:1) 0.18 9.15E-03 0.02 0.18 0.03 0.05
TG(48:1) 0.27 1.00E-04 3.82E-04 0.22 7.40E-03 0.02
TG(50:1) 0.07 0.31 0.40 20.06 0.45 0.50
PC(32:1) 0.33 1.45E-06 1.31E-05 0.21 8.94E-03 0.02
PCae(38:4) 20.06 0.39 0.44 20.15 0.06 0.09
PCae(44:6) 0.02 0.80 0.80 20.03 0.69 0.69
PCae(40:3) 20.26 1.70E-04 3.82E-04 20.24 3.63E-03 0.02
PCae(40:5) 20.16 0.02 0.03 20.14 0.08 0.10
PCae(40:4) 20.27 1.31E-04 3.82E-04 20.29 2.60E-04 2.34E-03
BH, Benjamini-Hochberg corrected. P values in bold type indicate a statistically significant result(P , 0.05).
2236 Early Second Trimester Lipid Biomarkers of GDM Diabetes Care Volume 39, December 2016

found to be associated with increased in-sulin resistance. Because circulatingpalmitoleate is principally synthesized in
the liver in humans, this may reflect he-patic insulin resistance, in line with ourfinding that TG(51:1) is associated with
fasting plasma glucose levels (30). Mech-anistically, palmitoleate and oleate areproduced from palmitate and stearateby the action of steroyl-CoA desaturase1 (SCD1), and SCD1 activity has recentlybeen linked in a large cohort to type 2 di-abetes risk and hepatic steatosis (31). In-deed, SCD12/2 mice display increasedinsulin sensitivity (32).
The association of TG(51:1), primarilycomprising TG(18:1/17:0/16:0) (or posi-tional isomers thereof) in our cohort,withmaternal glucose levels was also sur-prising because odd-chain fatty acids, in-cluding heptadecanoic acid, have beenassociated with reduced risk of type 2 di-abetes (28,33,34). However, our finding isin keeping with results of an untargetedmetabolomic screen using fasted serumsamples from women at 28 weeks of ges-tation who were enrolled in the HAPOstudy (35), in which heptadecanoic acidwas raised in subjects with fasting plasmaglucose levels in the 90th percentile butwith BMI values similar to those of controlsubjects. This may be due to genuine dif-ferences in the pathophysiology of GDMand type 2 diabetes but may also reflectthe fact that the studies of type 2 diabetesmeasured the fatty acid content in phos-pholipids, whereas the latter study (35) ofpregnant womenmeasured free fatty acids.This underscores the advantage of intactlipid studies as opposed to fatty acid pro-filing (30), which is a strength of our study.
The other group of lipid biomarkersidentified, PCae(40:3) and PCae(40:4),were inversely associated with maternalglucose levels. This is consistent with anearlier report from the AusDiab cohort(28) in which ether phospholipid levelswere inversely related to postload glu-cose levels and were reduced in patientswith diabetes. The physiological functionof ether phospholipids remains largelyunknown (36), but they have been impli-cated as physiological ligands of peroxi-some proliferator–activated receptor g(37). Intriguingly, SCD1 is a target of per-oxisome proliferator–activated receptorg, potentially providing a mechanisticlink between low levels of ether phospho-lipids and high levels of palmitoleate- andoleate-containing lipids (32).
The broad overlap between our lipidbiomarkers and those identified in stud-ies of type 2 diabetes may be a result ofthe fact that lipid profiles were derivedfrom samples obtained early in preg-nancy, reflecting the contribution of
Figure 2—Validated lipid biomarkers and GDM prediction within the validation cohort. A: Individualpredictive power of each lipid, independent of maternal age and BMI. *P , 0.05, with Benjamini-Hochberg correction for multiple testing. B: Combined predictive power of four lipid species.C: Enhancement of predictive power of conventional risk factors.
care.diabetesjournals.org Lu and Associates 2237

preexisting insulin resistance to thedevelopment of GDM. Indeed, it will beideal to obtain a sample before concep-tion as well as one obtained during preg-nancy to identify lipid biomarkers thatreflect the pathophysiological contribu-tion of pregnancy itself. Nevertheless,this explanation of our findings is madeless likely by the fact that genome-wideassociation studies have revealed abroadly shared genetic architecture be-tween GDM and type 2 diabetes andmetabolomic studies from later in preg-nancy, including one using samples from28 weeks of gestation, have shown over-lapping metabolic signatures betweenGDM and type 2 diabetes (11,14,35).There are several limitations to our
study. First, although we validated ourcandidate lipid biomarkers using a pre-defined subset, these biomarkers havenot been externally validated, for exam-ple in ethnic populations at high risk.Second, our study was not designed todemonstrate the superiority of a lipidbiomarker–based and risk factor–basedapproach compared with a risk factor–based screening alone. Thus, we lackeddata on other conventional risk factors(e.g., family history of diabetes and per-sonal history of GDM). For similar reasons,we also lacked data on other traditionalbiochemical risk factors, such as HbA1c,TGs, and HDL cholesterol, and are thus un-able to directly compare the performanceof the lipid biomarkers to these alterna-tives within this study. Third, because weselected only 13 lipids from the 189 lipidsmeasured for univariate analysis,wemighthave been overly conservative in our ap-proach. Finally, because serumsamples forlipidomic analysis were obtained in thenonfasting state without controlling formeal time and meal content, this wouldhave added additional lipidomic variabilitythat was not related to variation in OGTTresults at 28 weeks of gestation, thus re-ducing study power. However, this addi-tional variability might be small comparedwith existing intersubject and intrasubjectvariation (38). Our reanalysis of data fromBegum et al. (38) suggests that variance ispartitioned among intersubject differ-ences, intrasubject differences not due tomeal time, and the effect of meal time intheproportion62%,31%,and7%, althoughthe population that they studied was lessheterogeneous than that in the CBGS.In summary, we report for the first time
an association between maternal early
second trimester lipid species and glycemictraits at 28 weeks of gestation, as assessedby a standard OGTT. We further show thatfour lipid biomarkers, TG(51:1), TG(48:1),PC(32:1), and PCae(40:4), are able to pre-dict maternal GDM status independent ofmaternal age and BMI and have the poten-tial to improve the performance of clinicalrisk factor–based screening. The lipid bio-markers identified also revealed markedsimilarities between the pathophysiologyof GDM and that of type 2 diabetes (14).In particular, we highlight the establishedrole of monounsaturated fatty acids (espe-cially palmitoleate) and the emerging roleof ether phospholipids, as well as the po-tential pathological role of odd-chain fattyacids, which might indicate a divergence inthe pathophysiologies of GDM and type 2diabetes.
Acknowledgments. The authors thank DianneWingate, Rachel Seear, Katrin Mooslehner, andRadkaPlatte(UniversityofCambridge,Cambridge,U.K.) for excellent laboratory assistance. The au-thors also thank the families who participated inthis study; the research nurses, including SuzanneSmith, Ann-Marie Wardell, and Karen Forbes(University of Cambridge, Cambridge, U.K.), fortheir important contributions; colleagues at theAddenbrooke’s Wellcome Trust Clinical ResearchFacility; and the midwives at the Rosie MaternityHospital for data collection.Funding. This part of theCambridgeBabyGrowthStudy was funded by Wellbeing of Women (grantRG1644) and Diabetes UK (grant 11/0004241). Thelipidomics assays were supported by the MedicalResearch Council (UD99999906) and CambridgeLipidomics Biomarker Research Initiative (grantG0800783). Core funding was also obtainedthrough the Medical Research Council (grants7500001180 and UD99999906), European UnionFramework 5 (grant QLK4-1999-01422), WorldCancer Research Fund (2004/03), MothercareFoundation (grant RG54608), and the NewlifeFoundation for Disabled Children (grant 07/20).There has also been support from National Insti-tute for Health Research Cambridge BiomedicalResearch Centre.Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.Author Contributions. L.L. designed the study,interpreted and analyzed the data, and drafted andedited the manuscript. A.K. designed the study,collected and interpreted the data, and edited themanuscript. C.J.P. and D.B.D. designed the study,interpreted the data, and edited the manuscript.B.J. and L.M. collected the data. I.A.H., C.L.A., andK.K.O. contributed to discussion and reviewed themanuscript. L.L. and D.B.D. are the guarantors ofthisworkand,assuch,hadfullaccess toall thedatainthestudyandtakeresponsibility for the integrityof the data and the accuracy of the data analysis.
References1. Sacks DA, Hadden DR, Maresh M, et al.;HAPO Study Cooperative Research Group.
Frequency of gestational diabetes mellitus atcollaborating centers based on IADPSG consen-sus panel-recommended criteria: the Hypergly-cemia and Adverse Pregnancy Outcome (HAPO)Study. Diabetes Care 2012;35:526–5282. Metzger BE, Lowe LP, Dyer AR, et al.; HAPOStudy Cooperative Research Group. Hyperglyce-mia and adverse pregnancy outcomes. N Engl JMed 2008;358:1991–20023. Metzger BE, Gabbe SG, Persson B, et al.; In-ternationalAssociation ofDiabetes andPregnancyStudy Groups Consensus Panel. International as-sociation of diabetes and pregnancy study groupsrecommendations on the diagnosis and classifica-tion of hyperglycemia in pregnancy.Diabetes Care2010;33:676–6824. National Collaborating Centre for Women’sand Children’s Health. Diabetes in Pregnancy:Management of Diabetes and Its Complicationsfrom Preconception to the Postnatal Period.London, RCOG Press, 20155. Lacaria E, Lencioni C, Russo L, et al. Selectivescreening for GDM in Italy: application and ef-fectiveness of National Guidelines. J Matern Fe-tal Neonatal Med 2015;28:1842–18446. American Diabetes Association. Classifica-tion anddiagnosis of diabetes. Sec. 2. In StandardsofMedical Care inDiabetesd2015. Diabetes Care2015;38(Suppl. 1):S8–S167. Schaefer-Graf UM, Kjos SL, Kilavuz O, et al.Determinants of fetal growth at different pe-riods of pregnancies complicated by gestationaldiabetesmellitus or impaired glucose tolerance.Diabetes Care 2003;26:193–1988. Riskin-Mashiah S, Younes G, Damti A,Auslender R. First-trimester fasting hyperglyce-mia and adverse pregnancy outcomes. DiabetesCare 2009;32:1639–16439. Agarwal MM, Dhatt GS, Punnose J, Zayed R.Gestational diabetes: fasting and postprandial glu-cose as first prenatal screening tests in a high-riskpopulation. J Reprod Med 2007;52:299–30510. Sachse D, Sletner L, Mørkrid K, et al. Meta-bolic changes in urine during and after preg-nancy in a large, multiethnic population-basedcohort study of gestational diabetes. PLoS One2012;7:e5239911. Lowe WL Jr, Karban J. Genetics, genomicsand metabolomics: new insights into maternalmetabolism during pregnancy. Diabet Med2014;31:254–26212. Zhao C,Wang F,Wang P, DingH, Huang X, ShiZ. Early second-trimester plasma protein profilingusing multiplexed isobaric tandem mass tag(TMT) labeling predicts gestational diabetes mel-litus. Acta Diabetol 2015;52:1103–111213. Zhao C, Dong J, Jiang T, et al. Early second-trimester serum miRNA profiling predicts gesta-tional diabetes mellitus. PLoS One 2011;6:e2392514. Angueira AR, Ludvik AE, Reddy TE, WicksteedB, Lowe WL Jr, Layden BT. New insights into ges-tational glucose metabolism: lessons learnedfrom 21st century approaches. Diabetes 2015;64:327–33415. Butte NF. Carbohydrate and lipid metabo-lism in pregnancy: normal compared with ges-tational diabetes mellitus. Am J Clin Nutr 2000;71(Suppl.):1256S–1261S16. Di Cianni G, Miccoli R, Volpe L, Lencioni C,Del Prato S. Intermediate metabolism in normalpregnancy and in gestational diabetes. DiabetesMetab Res Rev 2003;19:259–270
2238 Early Second Trimester Lipid Biomarkers of GDM Diabetes Care Volume 39, December 2016

17. Koukkou E, Watts GF, Lowy C. Serum lipid,lipoprotein and apolipoprotein changes ingestational diabetes mellitus: a cross-sectionaland prospective study. J Clin Pathol 1996;49:634–63718. Petry CJ, Seear RV, Wingate DL, et al. Ma-ternally transmitted foetal H19 variants and as-sociations with birth weight. Hum Genet 2011;130:663–67019. Petry CJ, Seear RV, Wingate DL, et al. Asso-ciations between paternally transmitted fetalIGF2 variants and maternal circulating glucoseconcentrations in pregnancy. Diabetes 2011;60:3090–309620. Prentice P, Acerini CL, Eleftheriou A, HughesIA, Ong KK, Dunger DB. Cohort profile: the Cam-bridge Baby Growth Study (CBGS). Int J Epide-miol 2016;45:35.a-g21. Koulman A, Prentice P, Wong MCY, et al.The development and validation of a fast androbust dried blood spot based lipid profilingmethod to study infant metabolism. Metabolo-mics 2014;10:1018–102522. Eiden M, Koulman A, Hatunic M, et al.Mechanistic insights revealed by lipid profilingin monogenic insulin resistance syndromes. Ge-nome Med 2015;7:6323. Koulman A, Woffendin G, NarayanaVK, Welchman H, Crone C, Volmer DA. High-resolution extracted ion chromatography, anew tool for metabolomics and lipidomicsusing a second-generation orbitrap massspectrometer. Rapid Commun Mass Spectrom2009;23:1411–141824. Teh WT, Teede HJ, Paul E, Harrison CL,Wallace EM, Allan C. Risk factors for gesta-tional diabetes mellitus: implications for the
application of screening guidelines. Aust N Z JObstet Gynaecol 2011;51:26–3025. Amylidi S, Mosimann B, Stettler C, FiedlerGM, Surbek D, Raio L. First-trimester glycosy-lated hemoglobin in women at high risk for ges-tational diabetes. Acta Obstet Gynecol Scand2016;95:93–9726. Wang C, Zhu W, Wei Y, Su R, Feng H, Lin L,et al. The predictive effects of early pregnancylipid profiles and fasting glucose on the risk ofgestational diabetes mellitus stratified bybody mass index. J Diabetes Res 2016;2016:301356727. Rhee EP, Cheng S, Larson MG, et al. Lipidprofiling identifies a triacylglycerol signature ofinsulin resistance and improves diabetes pre-diction in humans. J Clin Invest 2011;121:1402–141128. Meikle PJ, Wong G, Barlow CK, et al. Plasmalipid profiling shows similar associations withprediabetes and type 2 diabetes. PLoS One2013;8:e7434129. Mozaffarian D, Cao H, King IB, et al. Circu-lating palmitoleic acid and risk of metabolic ab-normalities and new-onset diabetes. Am J ClinNutr 2010;92:1350–135830. Roberts LD, Koulman A, Griffin JL. Towardsmetabolic biomarkers of insulin resistance andtype 2 diabetes: progress from the metabolome.Lancet Diabetes Endocrinol 2014;2:65–7531. Jacobs S, Schiller K, Jansen EHJM, Boeing H,Schulze MB, Kroger J. Evaluation of various bio-markers as potential mediators of the associationbetween D5 desaturase, D6 desaturase, andstearoyl-CoA desaturase activity and incidenttype 2 diabetes in the European Prospective
Investigation into Cancer and Nutrition-PotsdamStudy. Am J Clin Nutr 2015;102:155–16432. Paton CM, Ntambi JM. Biochemical andphysiological function of stearoyl-CoA desaturase.Am J Physiol Endocrinol Metab 2009;297:E28–E3733. Forouhi NG, Koulman A, Sharp SJ, et al. Dif-ferences in the prospective association betweenindividual plasma phospholipid saturated fattyacids and incident type 2 diabetes: the EPIC-InterAct case-cohort study. Lancet Diabetes Endo-crinol 2014;2:810–81834. Jenkins B, West JA, Koulman A. A review ofodd-chain fatty acid metabolism and the role ofpentadecanoic Acid (c15:0) and heptadecanoicAcid (c17:0) in health and disease. Molecules2015;20:2425–244435. Scholtens DM, Muehlbauer MJ, Daya NR,et al.; HAPO Study Cooperative ResearchGroup. Metabolomics reveals broad-scale met-abolic perturbations in hyperglycemic mothersduring pregnancy. Diabetes Care 2014;37:158–16636. Lodhi IJ, Semenkovich CF. Peroxisomes: anexus for lipid metabolism and cellular signal-ing. Cell Metab 2014;19:380–39237. Lodhi IJ, Yin L, Jensen-Urstad APL, et al. Inhib-iting adipose tissue lipogenesis reprograms ther-mogenesis and PPARg activation to decreasediet-induced obesity. Cell Metab 2012;16:189–20138. Begum H, Li B, Shui G, et al. Discoveringand validating between-subject variations inplasma lipids in healthy subjects. Sci Rep2016;6:19139
care.diabetesjournals.org Lu and Associates 2239