Embed Size (px)
Citation preview

An Overview of the Health of Our PopulationCapital Health, 2013
Understanding Communities Unit Public Health Services
Lead Author: Holly D’Angelo-Scott, PhD
May 2014
Part 2

3.2.2 FRUIT AND VEGETABLE CONSUMPTION AND OBESITY
However, the relationship between social deprivation and being overweight or obese here is not significant (Figure 16).
One possible risk factor that may contribute to over-weight or obesity is the consumption of fruit and vegetablesin amounts less than the recommended guidelines. We didnot find a significant association between fruit and vegetableconsumption less than the recommended guidelines andBMI categories of overweight or obese (OR = 1.11, 95% CI0.90 – 1.37). However, when looking at BMI categoriesof overweight and obese separately, participants who reported meeting or above the recommended guidelines for fruit and vegetable consumption are 25%less likely to be obese when compared to participantswho were below the guidelines (OR = 0.75, 95% CI 0.56- 0.98).
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results47
Note. The 20% least deprived category was used as the reference category (odds ratio = 1), with all other categories of deprivation being compared to the referencecategory. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The odds of Having a Body Mass Index of Overweight or Obese Based on Social Deprivation, AdultsAged 18 and Over, Capital Health, 2009/10 (n = 1720)
Figure 16
Odds
Ratio
2.5
2
1.5
1
0.5
0
Material Deprivation Index
1 2 3 4 5
When exploring the association between deprivation and fruit and vegetable consumption, a significant relationship wasfound. As shown in Figure 17, individuals residing in the areas with the highest total deprivation are the most likelyto report fruit and vegetable consumption that did not meet the recommended guidelines (OR = 1.79, 95% CI 1.13– 2.83). When looking at the separate components of total deprivation, material and social, significant variations in fruit andvegetable consumption were not found. Although the result was not statistically significant, it is worth noting that the oddsof fruit and vegetable consumption below the recommended guidelines is the highest among people residing inareas with the highest material deprivation (OR = 1.35, 95% 1.00 – 1.83).

Based on the findings, individuals with higher total deprivation and higher material deprivation are more likely to be belowthe recommended guidelines for fruit and vegetable consumption, and those who are below the recommended guidelinesare more likely to be obese. Researchers have suggested that food security may be a factor linking deprivation and fruit andvegetable consumption (Slater, Green, Sevenhuysen, O'Neil, & Edginton,2009; Franklin, Jones, Love, Puckett, Macklin, &White - Means, 2012). We were unable to explore this relationship due to limitations in our data. However, the availability offood was examined in this report.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results48
Note. The asterisk indicates a significant association between category of total deprivation and the odds of consuming less than the recommended guidelines forfruit and vegetable consumption. The 20% least deprived category was used as the reference category (odds ratio = 1), with all other categories of deprivationbeing compared to the reference category. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Consuming Less Than the Recommended Guidelines for Fruit and Vegetable ConsumptionBased on Total Deprivation Among Adults Aged 18 and Over, Capital Health, 2009/10 (n = 1737)
Figure 17
Odds
Ratio
2
1.5
1
0.5
0
Total Deprivation Index
1 2 3 4 5*
The following maps depict the density of fast food and grocery locations in Capital Health communities (refer to Figure 18). While no technical analysis was performed, thefollowing observations were made. When looking at the density of fast food and grocery locations in communitieswithin Capital Health(refer to Figure 18 and Table 28), it canbe seen that the majority of the communities have a lowdensity of grocery locations and fast food locations. Thehighest density of grocery locations was found in Hubbardsand Moser River while the highest density of fast food locations was found in Halifax Citadel. It is important to notethat Halifax Citadel has a total deprivation score of 4 (20 to40% most deprived).
Density of Grocery Locations and Fast Food Locations per 100,000 Population by CommunityTable 28
CommunityDensity Grocery Locations per 100,000 Population
Armdale – Northwest Arm, Beaver Bank, Brooklyn, Clayton Park, Cole Harbour,Dartmouth East, Dartmouth South, Eastern Passage, Enfield, Fall River, Falmouth,Hammonds Plains, Hantsport, Herring Cove, Kempt Shore, Lake Echo, Lantz,Lawrencetown, Mount Uniacke, Newport Corner, Peggy’s Cove, Porter’s Lake, Preston, St. Margaret’s Bay, Sackville North, Sackville South, Sheet Harbour, Spryfield, Summerville, Tantallon, Terrance Bay, Three Mile Plains, Timberlea, Windsor, Windsor Forks
Low Density 0.0 – 45.5

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results49
CommunityDensity Fast Food Locations per 100,000 Population
Armdale – Northwest Arm, Beaver Bank, Brooklyn, Chezzetcook, Cole Harbour,Eastern Passage, Enfield, Fall River, Falmouth, Hammonds Plains, Jeddore, LakeEcho, Lantz, Lawrencetown, Middle Musquodoboit, Moser River, Mount Uniacke,Newport Corner, Peggy’s Cove, Preston, Prospect, St. Margaret’s Bay, SackvilleNorth, Sambro, Sheet Harbour, Ship Harbour, Smiths Corner, Spryfield, Tantallon,Terrence Bay, Timberlea, Upper Musquodoboit
Bedford, Clayton Park, Dartmouth East, Fairview, Hantsport, Hatchet Lake, Hubbards, Sackville South, Spryfield, Windsor Forks
Low Density 0.0 - 84.7
84.8 - 169.5
169.6 - 254.3
254.4 - 339.0
339.1 - 423.8High Density Halifax Citadel
Dartmouth South, Hacketts Cove, Halifax Chebucto, Waverly
Dartmouth North, Halifax Needham, Musquodoboit Harbour, Windsor
Medium Density
CommunityDensity Grocery Locations per 100,000 Population
Bedford, Dartmouth North, Fairview, Halifax Chebucto, Halifax Citadel, Jeddore,Middle Musquodoboit, Prospect, Sambro, Ship Harbour, Upper MusquodoboitLow Density
45.6 – 91.1
91.2 – 136.7
136.8 – 182.2
182.3 - 227.8High Density Hubbards, Moser River
Hacketts Cove, Hatchet Lake
Chezzetcook, Halifax Needham, Musquodoboit HarbourMedium Density
Density of Fast Food Locations and Grocery Store Locations per 100,000 Population by Community Figure 18 A
Total Deprivation
1 (20% least deprived)
2
3
4
5 (20% most deprived)
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.1
DATA Sources:
1) M. Terashima, PhD, Dalhousie Univ., 2011Health Geomatics Laboratory
2) Sara Kirk, PhD, Dalhousie Univ., 2011
August 31, 2014
No Score
Fast Food Location Rate
0.00 - 22.60
2.61 - 65.57
65.58 - 117.42
117.43 - 180.10
189.11 - 423.77

3.2.1 PHYSICAL ACTIVITY AND OBESITY
Overweight and obesity are multifactoral conditions. Therehas been observed links between physical activity level andBMI status. Literature points to those who have increasedlevels of physical activity having lower chances of beingoverweight or obese (Harrington & Elliott, 2009; Kruger,Ham, & Prohaska, 2009). This was found when exploringthe data.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results50
Density of Fast Food Locations and Grocery Store Locations per 100,000 Population by Community Figure 18 B
Note. Grocery store locations included bakeries, markets, mixed services (e.g., video and grocery), specialty stores, and grocery chains. The locations for thegrocery stores and the fast food sites were provided by Dr. S. Kirk, Dalhousie University (2011).
Individuals in this population health status report who reportbeing inactive are more likely to be overweight or obesewhen compared to those who are active or moderately active(OR = 1.70, 95% CI 1.39 – 2.09). Although individuals residing in areas with the highest total deprivation are morelikely to report being physically inactive (OR = 1.23, 95%0.93 – 1.65) when compared to those residing in areas ofthe least total deprivation, the association is not statisticallysignificant (refer to Figure 19).
The classification of physical activity as active, moder-ately active and inactive is based on an index of averagedaily activity over past 3 months.Active ≥ 3.0 kcal/kg/dayModerately active = 1.5 – 2.9 kcal/kg/dayInactive < 1.5 kcal/kg/day
Total Deprivation
1 (20% least deprived)
2
3
4
5 (20% most deprived)
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.2
DATA Sources:
1) M. Terashima, PhD, Dalhousie Univ., 2011Health Geomatics Laboratory
2) Sara Kirk, PhD, Dalhousie Univ., 2011
August 31, 2014
No Score
Grocery Store Locations
1.00 - 12.40
12.41 - 40.00
40.01 - 70.83
70.84 - 118.62
118.63 - 227.79
(Per 100,000 Population)

Similarly, significant relationships were not found with material or social deprivation and physical activity.As shown in Figure20, there appeared to be a positive trend with increased odds of being physically inactive with both increasing material and social deprivation, however, neither relationship was significant.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results51
Note. The 20% least deprived category was used as the reference category (odds ratio =1), with all other categories of deprivation being compared to the referencecategory. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Being Physically Inactive Based on Total Deprivation Among Adults Aged 18 and Over,Capital Health, 2009/10 (n = 1814)
Figure 19
Odds
Ratio
2
1.5
1
0.5
0
Total Deprivation Index
1 2 3 4 5
Note. The 20% least deprived category was used as the reference category (odds ratio =1), with all other categories of deprivation being compared to the referencecategory. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Being Physically Inactive Based on Material and Social Deprivation Among Adults Aged18 and Over, Capital Health, 2009/10 (n = 1814)
Figure 20
Odds
Ratio
2
1.5
1
0.5
0
Deprivation Category
1 2 3 4 5
Material Deprivation Social Deprivation
The presence of parks and trails in communities, and theirfeatures, was analyzed as part of this population health status report. Figure 21 shows a concentration of parks andpark feature locations as well as trails in the urban areaswhen compared to the rural areas. It is interesting to notethat we also found an increase of self-reported overweightand obesity in Eastern Shore – Musquodoboit, a rural area,when compared to Halifax Peninsula, an urban area. Thisfinding reflects the results of other studies which have

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results52
suggested that in addition to a higher consumption of fat due to cultural eating patterns and reduced access to healthfulfood (Befort, Nazir, & Perri, 2012); the built environment, including the presence of parks and trails, may also be a contributingfactor (Sallis, Floyd, Rodriguez, & Saelens, 2012).
Parks, Park Features and Trails in Halifax Regional Municipality (Excludes West Hants). Figure 21
The data were obtained from HalifaxOpenData (2013).
Total Deprivation
1 (20% least deprived)
2
3
4
5 (20% most deprived)
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.1
DATA:
1) CIHI, 20062) Halifax Open Data
July 29, 2013
Missing Values
Parks/Park Features
Parks
Park Features
Total Deprivation
1 (20% least deprived)
2
3
4
5 (20% most deprived)
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.1
DATA Source:
1) M. Terashima, PhD., Dalhousie UniversityHealth GeomaticsLaboratory
August 26, 2014
Missing Values
Trails
Trails

SUMMARY
When exploring overweight and obesity in Capital Health,there was a variation in BMI between the Community HealthBoards. Total and material deprivation was significantly associated with overweight and obesity, such that with increasing deprivation, there was an increase in the odds ofbeing overweight or obese. We found significant associations between being overweight or obese and sex; fruit and vegetable consumption; and physical activity. Fruit and vegetable consumption was also associated with depriva-tion. Although rigorous analyses of community factors werenot done, we found that the highest density of grocery storeswas in Hubbards and Moser River while the highest densityof fast food locations was found in Halifax Citadel. Finally, alower concentration of parks and park feature locations aswell as trails was found in rural areas when compared tothe urban areas.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results53
3.3 ALCOHOL AND CAPITAL HEALTH
• Heavy drinking was more likely among individuals residing in areas with higher total and material deprivation
• Heavy drinking was associated with not being satisfied with life
• Males were more likely to engage in heavy drinking
• Those who reported heavy drinking were more likely to be daily or occasional smokers. Daily or occasional
smoking was more likely among residents residing in areas with higher total and material deprivation
In this report we examined the relationship of heavy drinkingmeasures and total deprivation as well as material and social deprivation. As well, individual and community riskfactors were explored to better understand the picture of alcohol use in our communities. Similar to obesity, a conceptual diagram was created to describe the many factors associated with heavy drinking was created (refer toFigure 22). Material and social deprivation are the under-lying conditions for both the individual and community factors and represent the determinants of health. It is important to note that the conceptual diagram for heavydrinking is not complete as there are many factors that contribute to an increased risk of heavy drinking. The variables captured in the conceptual diagram are some of the factors that were considered in this population health report.The following sections discuss variables which were significantly associated with heavy alcohol drinking. Appendix A providesa summary of the association between heavy alcohol drinking and all of the considered factors.

In accordance with the 2009 CCHS results, 27.9% of therespondents reported having 5 or more drinks on one occasion, at least once a month in the previous year with7.1% having 5 or more drinks at least once a week. Whencomparing Community Health Boards, having 5 or moredrinks on one occasion at least once a month was reportedmore often by those residing in West Hants (58.6%) andleast often by those residing in Southeastern Dartmouth(refers to Figure 23). We also found that males are morelikely to report heavy drinking when compared to females(OR = 2.57, 95% CI 1.91 – 3.45).
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results54
Conceptual Diagram for Alcohol Use. Figure 22
Note. This diagram does not capture all factors that have been associated with alcohol use.
ALCOHOL USE
AVERAGE CONSUMPTION
AVAILABILITY OF ALCOHOL
Alcohol RelatedIncidents
Opinions Effects of Alcohol
Opinions of Alcohol UseOutside the Home
Opinions of Alcohol CostOpinions
SellingOpinions
Allocations ofRevenue
Opinions Purchasing
Opinions AlcoholPolicy
Opinions, Price & Availability
Material Deprivation
Material Deprivation
High BloodPressure
CardiovascularDisease
Diabetes Prevalence
RespiratoryDisease
Cancer
MENTALHEALTH
SMOKING
Drinking Population
Density of Alcohol Outlets
Alcohol Paid Advertising
Age of AlcoholDrinking Initiation
Perceived Safe Drinking Levels
Consequences of Use
Participation in Addiction PreventiveTreatment Services
Drinking &Social Usage
Drinking Situations
Participation inIWK Choices
Alcohol Comsumption
During Pregnancy
Alcohol Related Violence
Physical Education
Alcohol Related Injury
Medical Costs
Drinking and Driving
Policing Costs

Studies have shown that deprivation has an influence on the drinking habits of individuals, that is, with increasing deprivation,there appears to be an increased likelihood of heavy drinking (Batty, Lewars, Emslie, Benzeval, & Hunt, 2008; Baumann etal., 2007). This was found when exploring total deprivation and heavy drinking in CDHA. When looking at the percentages ofadults who reported heavy drinking by the five quintiles of total deprivation, those residing in areas with the lowest deprivationare the least likely to report having 5 or more drinks on occasion at least once a month or more. Individuals residing inareas with the highest total deprivation are the most likely to report having 5 or more drinks on occasion at leastonce a month or more (refer to Figure 24).
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results55
3.3.1 DEPRIVATION AND ALCOHOL
Note. Individuals who reported never drinking, didn’t know or had missing data (n = 1581) were excluded.
Note. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
Percent of Adults Who Reported Having 5 or More Drinks on One Occasion at Least Once a Monthby Community Health Board, Aged 15 and Over, Capital Health, 2009/10 (n = 1238)
Figure 23
100.0%
80.0%
60.0%
40.0%
20.0%
0.0%
Community Health Board
53.0% 54.6% 44.8% 50.9% 54.8% 53.8% 58.6%
Chebucto West(n = 185)
Cobequid(n = 183)
Dartmouth(n = 183)
ES/Musquodoboit(n = 167)
Halifax Peninsula(n = 186)
SE Dartmouth(n = 194)
West Hants(n = 140)
5 or More Drinks per Occasion at Least Once a Month 5 or More Drinks per Occasion Less Than Once a Month
5 or More Drinks on One Occasion Once a Month or More 5 or More Drinks on One Occasion Less Than Once a Month
Percent of Adults With Self-Reported Drinking by Total Deprivation, Aged 15 and Over, CapitalHealth, 2009/10 (n = 794)
Figure 24
Drinking
Status
100.0%
80.0%
60.0%
40.0%
20.0%
0.0%
Total Deprivation Index
42.0% 50.3% 54.1% 52.9% 55.1%
1 2 3 4 5

Figure 26 summarizes the percentage of adults who report heavy drinking by the categories of material deprivation. Similarto the findings of other studies, there appears to be relationship between deprivation and heavy drinking, with the highestpercentage of adults who report heavy drinking residing in areas of both lower and higher deprivation.
Further analysis of the likelihood of heavy drinking and total deprivation suggests that an increased likelihood of heavy drinkingis significantly associated with total deprivation (refer to Figure 25). In fact, the odds of being a heavy drinker appear to begreatest among those with the highest total deprivation when compared to those with the least deprivation. The odds ofheavy drinking are 1.68 times greater among individuals residing in areas with the highest total deprivation (95%CI 1.09 - 2.59).
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results56
Note. The asterisk indicates a significant association between category of total deprivation and the odds of heavy drinking. The 20% least deprived category wasused as the reference category, with all other categories of deprivation being compared to the reference category. The total deprivation ranges from 20% leastdeprived (1) to 20% most deprived (5).
The Odds of Heavy Drinking Based on Total Deprivation, Persons Aged 15 and Over, Capital Health, 2009/10 (n = 794)
Figure 25
Odds
Ratio of H
eavy Drin
king
3
2.5
2
1.5
1
0.5
0
Total Deprivation Index
1 2 3 4* 5*
Note. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
5 or More Drinks on One Occasion Once a Month or More 5 or More Drinks on One Occasion Less Than Once a Month
Percent of Adults With Self-Reported Drinking by Material Deprivation, Aged 15 and Over, CapitalHealth, 2009/10 (n = 794)
Figure 26
Drinking
Status
100.0%
80.0%
60.0%
40.0%
20.0%
0.0%
Material Deprivation Index
42.3% 57.4% 49.0% 45.0% 58.1%
1 2 3 4 5

While there appeared to be a relationship between materialdeprivation and heavy drinking, it was important to determine if the relationship was significant. The results ofthe analyses suggest that there is a significant relationshipbetween material deprivation and heavy drinking (refer toFigure 27). When compared to those residing in areaswith the lowest deprivation, the odds of heavy drinkingare 1.89 times higher among those in areas with thehighest material deprivation (95% CI 1.23 – 2.90). A sig-nificant association is also seen between heavy drinking anda lower material deprivation. The odds of heavy drinkingare 1.84 times greater (95% CI 1.14 – 2.96) amongthose residing in areas with category 2 of the materialdeprivation index when compared to those in the areaswith the least material deprivation.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results57
Note. The asterisk indicates a significant association between category of material deprivation and the odds of heavy drinking. The 20% least deprived categorywas used as the reference category, with all other categories of deprivation being compared to the reference category. The total deprivation ranges from 20% leastdeprived (1) to 20% most deprived (5).
The Odds of Heavy Drinking Based on Material Deprivation, Persons Aged 15 and Over, CapitalHealth, 2009/10 (n = 794)
Figure 27
Odds
Ratio of H
eavy Drin
king
3
2.5
2
1.5
1
0.5
0
Material Deprivation Index
1 2* 3 4 5*
When looking at social deprivation and drinking, the percent of adults who report drinking 5 or more drinks at least once permonth was highest among those residing in areas with average to high social deprivation. Further analysis show the odds ofheavy drinking increasing with increasing social deprivation; however, the association was not significant.
In addition to deprivation and individual factors, there is evidence that community factors can influence the likelihood of heavydrinking and the problems associated with heavy drinking. Based on a number of studies, communities with a high densityof alcohol outlets are more likely to have higher rates of violence, drinking and driving, motor vehicle related pedestrianinjuries; child abuse and neglect; and alcohol related deaths (Campbell et al., 2009; Stockwell et al., 2011; Task Force onCommunity Preventive Services, 2009). There are 61 establishments in Capital Health where alcohol can be purchased; notethis excludes establishments with alcohol making kits for purchase and licensed restaurants and bars (refer to Figure 29).The Halifax Peninsula Community Health Board has the greatest number of establishments for alcohol purchase (n = 19,31.1%) while Southeastern Dartmouth has the fewest number of establishments (n = 2, 3.3%).

Figure 29 shows the spatial distribution of liquor stores by total deprivation. In a recent systematic review conducted byPopova, Giesbrecht, Bekmuradov, and Patra (2009), it was found that higher alcohol outlet density tends to be associatedwith higher rates of damage, harm or problems including alcohol-related pedestrian collisions, self-reported injuries, and alcohol-related vehicle accidents.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results58
Note. This includes Nova Scotia Liquor Commission facilities, breweries and specialty stores and excludes “make your own” and licensed restaurants and bars.
Number of Establishments for Alcohol Purchase by Community Health BoardFigure 28
20181614121086420
Community Health Board
Halifax Peninsula Cobequid Dartmouth Chebucto West Eastern Shore West Hants SE Dartmouth
Numbe
r of L
ocations
for
Alco
hol P
urch
ases
Liquor Stores and Agencies by DeprivationFigure 29
Total Deprivation
1 (20% least deprived)
2
3
4
5 (20% most deprived)
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.1
DATA:
1) CIHI, 2006July 29, 2013
Missing Values
NSLC Stores & Agencies
Locations

SUMMARY
As shown in Table 29, the highest liquor store density was found in Eastern Shore – Musquodoboit, followed byHalifax Peninsula. For the period of 2006 – 2011, the annualaverage sales in each Community Health Board ranged from 8 million to 62.5 million dollars, with the highest sales per capita in Halifax Peninsula. It is important to notethe annual average sales and the sales per capita do notnecessarily reflect the sales to the population residing in aparticular Community Health Board.
In this population health report, we found significant relationships between heavy drinking and deprivation (total and material).Consideration of community factors identified that the highest density of liquor stores per 100,000 population was in EasternShore – Musquodoboit with the highest sales per capita in Halifax Peninsula.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results59
3.4 MENTAL HEALTH AND CAPITAL HEALTH
Liquor Store Density per 100,000 Population and Sales per Person, by Community Health Board,2006 - 2011
Table 29
Halifax Peninsula 10 13.9 $62,542,768 $870
Cobequid 8 9.6 $45,176,939 $541
Dartmouth 5 7.4 $39,581,954 $582
Chebucto West 5 5.9 $31,932,644 $378
Eastern Shore – Musquodoboit 4 18.6 $10,527,132 $491
Hants West 1 4.6 $8,086,551 $374
Southeastern Dartmouth 2 4.7 $15,805,013 $372
Sales per CapitaNumber of Liquor Storesper 100,000 Population
Number of Liquor Stores Average Annual Sales*
• Self-rated negative mental health was associated with reporting daily life as stressful, being physically inactive,being neither or unsatisfied with life, and having a mood disorder.
• Those who reported negative mental health were more likely to report negative physical health. Negative physical health was more likely among individuals residing in areas with higher material and social deprivation.
• Those who reported negative mental health were more likely to report negative oral health. Negative oral health was more likely among individuals residing in areas with higher material and social deprivation.
• Those who reported negative mental health were more likely to be daily or occasional smokers. Daily or occasional smoking was more likely among residents residing in areas with higher total and material deprivation.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results60
• A weak sense of belonging was more likely among those who reported negative mental health. A weak sense of belonging was more likely among individuals residing in areas with higher material deprivation.
• Self-rated negative mental health was associated with a BMI of obese. Being obese was more likely among individuals residing in areas with higher material deprivation.
There are many factors that may be associated with an increased likelihood of poor mental health. Similar to obesity and alcohol use, a conceptual diagram depicting the many factors associated with mental health was created (refer toFigure 30). Material and social deprivation are the underlyingconditions for both the individual and community factors and represent the determinants of health. It is important tonote that the conceptual diagram for mental health is notcomplete as there are many factors that contribute to an increased risk of poor mental health. The variables capturedin the conceptual diagram are some of the factors that wereconsidered in this population health report. The followingsections discuss variables which were significantly associated with mental health; however, Appendix A provides a summary of the association between mental health and all ofthe considered factors, as well as the associations of the considered factors and life satisfaction and mood disorders.
Conceptual Diagram for Mental HealthFigure 30
Note. This diagram does not capture all factors associated with mental health.
aterial Deprivation
Drug Use
Mental Health
Alcohol Consumption
High Blood Pressure
Access to Mental HealthProfessionals
Access to Youth Health
Centres
Self-Rated Illness
Mood Disorders
LifeSatisfaction
Self-RatedMental Health
Gambling
Prescription Drugs Illicit Drugs
Cancer
Diabetes Prevalence
CardiovascularDisease
RespiratoryDisease
Smoking
Social Support
Sense of CommunityBelonging
PerceivedSafety of
Neighbourhood
Violent Crime
Social Deprivation
MaterialDeprivation
IncomeRental HousingAffordability
Education
Employment
Living Alone
Single Parent
Separated, Widowed or Divorced

3.4.1 DEPRIVATION AND MENTAL HEALTH
In accordance with the 2009 CCHS results, 5.8% of the respondents reported having poor (negative) mental health. Stratificationby Community Health Board (refer to Figure 31) suggests a higher percentage of respondents residing in the Halifax Peninsulareporting negative mental health (7.0 %) while residents of Cobequid are the least likely to report having negative mental health (4.2%).
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results61
100.0%90.0%80.0%70.0%60.0%50.0%40.0%30.0%20.0%10.0%0.0%
Positive Mental Health Negative Mental Health
Percen
tage
of P
artic
ipan
ts (%
)
Percen
tage
of P
artic
ipan
ts (%
)
Chebucto West Cobequid Dartmouth ES/Musquodoboit Halifax Peninsula SE Dartmouth West Hants
Community Health Board
Self-Rated Mental Health by Community Health Board, Capital Health, CCHS 2009/10 Figure 31
8.0%
6.0%
4.0%
2.0%
0.0%
The sample size was 2815 for self-rated mental health, 2811 for life satisfaction and 2810 for mood disorder.
Based on the results of the Canadian Community Health Survey (CCHS), conducted in Capital Health in 2009/10,there appears to be an inverse u-shaped relationship between self-rated negative mental health and total deprivation. As shown in Table 30, those residing in areas with the least (category 1) and greatest (category 5)total deprivation are less likely to report negative mental health when compared to those in the other categories oftotal deprivation.
Self-Rated Mental Health Among Adults Aged 15 and Over, by Total Deprivation, Capital Health, 2009/10.Table 30
Note. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
1 324 (95.0) 17 (5.0)
2 288 (93.8) 19 (6.2)
3 239 (93.7) 16 (6.3)
4 492 (93.7) 33 (6.3)
5 443 (95.1) 23 (3.9)
Positive, n (%)Total Deprivation Index Category Negative, n (%)
Self-Rated Mental Health (n = 1894)

The odds of reporting negative health was lowest among those residing with the lowest and highest deprivation (refer toFigure 32); however, the relationship between mental health and total deprivation was not significant.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results62
Note. The 20% least deprived category was used as the reference category, with all other categories of deprivation being compared to the reference category. Thetotal deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Reporting Negative Mental Health Based on Total Deprivation Among Adults Aged 15and Over, Capital Health, 2009/10
Figure 32
Odds
Ratio of S
elf-Re
ported
Neg
ative
Men
tal H
ealth
3
2.5
2
1.5
1
0.5
0
Total Deprivation Index
1 2 3 4 5
An analysis of the two separate components of the total deprivation index, material deprivation and social depriva-tion, was conducted to explore the impact of each of thecomponents on mental health. When considering materialdeprivation as a separate influencing component, the proportion of participants who reported negative mentalhealth is highest among those who were least materially deprived (refer to Table 31). However, these differences arenot statistically significant.
Self- Rated Mental Health, Among Adults Aged 15 and Over, by Material Deprivation, Capital Health,2009/10.
Table 31
Note. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
1 274 (92.9) 21 (7.1)
2 285 (94.4) 17 (5.6)
3 268 (94.0) 17 (6.0)
4 408 (94.9) 22 (5.1)
5 549 (94.5) 32 (5.5)
Positive, n (%)Material Deprivation Index Category Negative, n (%)
Self-Rated Mental Health (n = 1894)

Nevertheless, compared to those residing in areas with the least material deprivation, the odds of reporting negative mentalhealth were lower in all other categories of material deprivation (refer to Figure 33). This finding suggests that there may bea potential protective link between self-reported negative mental health and material deprivation; however, this associationrequires further investigation.
Next, the association between social deprivation and self-rated negative mental health was considered. Strong social tieshave been thought to be preventative against negative mental health (Kawachi & Berkman, 2001). Again, there appears tobe more individuals reporting negative mental health in all categories of social deprivation when compared to the leastdeprived category (refer to Table 32).
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results63
Note. The 20% least deprived category was used as the reference category, with all other categories of deprivation being compared to the reference category. Thetotal deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Reporting Negative Mental Health Based on Material Deprivation Among Adults Aged15 and Over, Capital Health, 2009/10
Figure 33
Odds
Ratio of S
elf-Re
ported
Ne
gativ
e Men
tal H
ealth
1.8
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Material Deprivation Index
1 2 3 4 5
Self-Rated Mental Health, Among Adults Aged 15 and Over, by Social Deprivation, Capital Health,2009/10
Table 32
Note. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
1 276 (95.8) 12 (4.2)
2 410 (92.6) 33 (7.4)
3 393 (94.7) 22 (5.3)
4 270 (93.8) 18 (6.2)
5 436 (94.6) 25 (5.4)
Positive, n (%)Social Deprivation Index Category Negative, n (%)
Self-Rated Mental Health (n = 1894)

3.4.2 OTHER FACTORS ASSOCIATED WITH MENTAL HEALTH
In addition to deprivation, there are other factors that may impact mental health and were considered in this population healthstatus report.
As shown in Figure 34, there was no statistically significant association when comparing those residing in areas with thelowest social deprivation to those with higher deprivation with respect to self-rated mental health.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results64
Note. The 20% least deprived category was used as the reference category (odds ratio = 1), with all other categories of deprivation being compared to the referencecategory. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Reporting Negative Mental Health Based on Social Deprivation Among Adults Aged 15and Over, Capital Health, 2009/10 (n = 1503)
Figure 34
Odds
Ratio of R
eportin
g Ne
gativ
e Men
tal H
ealth
4
3.5
3
2.5
2
1.5
1
0.5
0
Social Deprivation Index
1 2 3 4 5
We found individuals who report negative mental healthare more likely to report daily life is stressful (OR =2.38, 95% CI 1.48 – 3.83). However, stress in daily life wasnot associated with deprivation; as deprivation increased(total, material or social), there was not an associated in-creased likelihood in daily stress.
Sense of belonging in a community may also influence mental health. Having a strong sense of belonging to one’scommunity has been shown to be linked to positive mentalhealth (Carpiano & Hystad, 2011; German & Latkin, 2012;Hystad & Carpiano, 2012; Kitchen, Williams, & Chowhan,2012; Williams & Kitchen, 2012). Sense of belonging toone’s community has been shown to increase with thelength of stay one has had in the community (Schellenberg,2004). Sense of belonging has also been shown to increasewith increasing income (Carpiano & Hystad, 2011).

Significant associations were found between negative mental health and sense of belonging. Individuals who report negative mental health are more likely to have a weak sense of belonging (OR = 2.14, 95% CI 1.44 –3.16). When looking at deprivation and sense of belonging,an association between total deprivation and a weak senseof belonging was not found. The odds of reporting a weaksense of belonging are similar among all total deprivationcategories. However, a weak association was found between material deprivation and sense of belonging. As shown in Figure 35, the greatest odds of having aweak sense of belonging were not in those in areas ofthe greatest material deprivation but in category 4 (20to 40% most deprived).
A significant association between social deprivation andsense of belonging was not found, however, the relationshipbetween social deprivation and sense of belonging appearedto the reverse of what was found for material deprivation(refer to Figure 35, A-B). That is, those in areas of the highest and lowest social deprivation are more likely to have a weak sense of belonging when compared to thosein the middle categories of social deprivation. The competinginfluences of material and social deprivation may explain theabsence of an overall association between total deprivationand sense of belonging.)
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results65
Note. The asterisk indicates a significant association between category of material deprivation or social deprivation and the odds of reporting a weak sense of belonging. The 20% least deprived category was used as the reference category (odds ratio = 1), with all other categories of deprivation being compared to thereference category. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Reporting a Weak Sense of Belonging Based on Material and Social Deprivation, AdultsAged 15 and Over, Capital Health, 2009/10
Figure 35-A
Odds
Ratio of W
eak Se
nse
of Belon
ging
2.5
2
1.5
1
0.5
0
Material Deprivation Index
1 2 3 4* 5

In the CCHS (Capital Health, 2009/10), participants were asked about issues in their communities.Table 33 summarizes the responses to a series of statements about communities. Of the nine community issues that were explored, loss of respect (by young people) for elders and vandalism or theft were perceived as the two most serious issues in communities. When exploring the relationship between each of the community issues and self-rated negative mental healthfor the purposes of this report, it was found that for the majority of the issues did not appear to have a statistically significantrelationship with mental health.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results66
The 20% least deprived category was used as the reference category (odds ratio = 1), with all other categories of deprivation being compared to the reference category. The total deprivation ranges from 20% least deprived (1) to 20% most deprived (5).
The Odds of Reporting a Weak Sense of Belonging Based on Material and Social Deprivation, AdultsAged 15 and Over, Capital Health, 2009/10
Figure 35-B
Odds
Ratio of W
eak Se
nse
of Belon
ging
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Social Deprivation Index
1 2 3 4 5
Perception of the Severity of Community Issues, Capital Health 2009/10Table 33
Loss of Respect by Young People Towards 370 (33.3) 742 (66.7)the Elders, n = 1112
Vandalism or Theft, n = 1097 363 (33.1) 734 (66.9)
Illegal Drug Use, n = 1066 447 (41.9) 619 (58.1)
Alcohol Abuse, n = 1043 477 (45.7) 566 (54.3)
Public Fights or Disturbances, n = 1100 675 (61.4) 425 (38.6)
Negligence of Children by Their Parents, 646 (64.1) 362 (35.9)n = 1008
Physical or Verbal Violence Between Husband (64.0) 336 (36.0)and Wife, n = 932 596
Suicide Among the Young, n = 980 673 (68.7) 307 (31.3)
Sexual Abuse of Children, n = 929 647 (69.6) 282 (30.4)
Not at All Serious or Not Too Serious, n (%)Community Issues Somewhat Serious or Very Serious, n (%)

Community crime may have an impact on bothphysical and mental health, as it influences thelevel of social connectedness one has with theircommunity (Public Health Agency of Canada,2008). A closer look at selected crimes reportedin Capital Health (excluding West Hants) during theperiod of 2008 to 2012 identifies that the mostfrequently reported crimes were theft under$5000, mischief, assaults, break and enters, andtraffic offences (refer to Figure 36). When exploringthe trends in the crimes, the frequency of theftsunder and over $5000 increased in 2012 as wellas traffic offences when compared to previousyears. All of the other crime category frequenciesdecreased in 2012 when compared to previousyears.
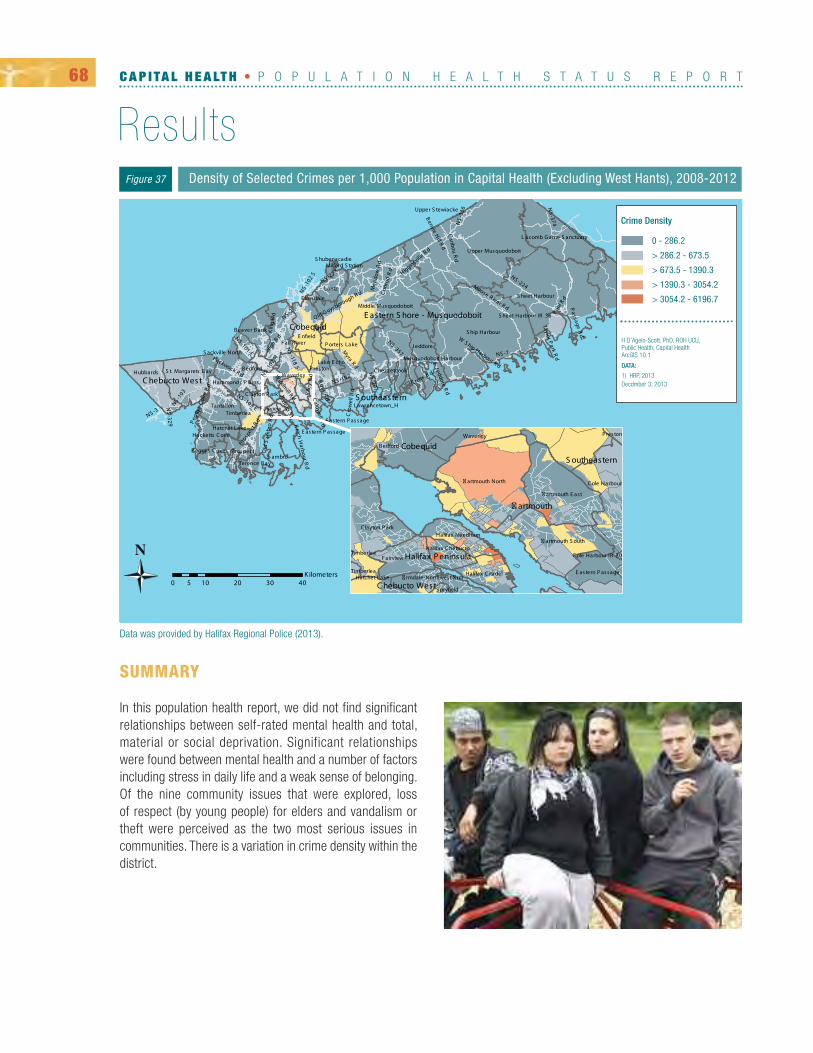
Further exploration of the density of the selected crime categories by dissemination area was conducted to determine if therewere variations in the density of crime by geography. As shown in Figure 37, the density of crime per 1,000 population ishigher in certain dissemination areas of the Halifax Regional Municipality. The densities ranged from 0 to 6197 crimes per1,000 population. As the crime density was based on crime location as the numerator and residential population as the denominator, the density will be influenced by the influx of individuals to areas with liquor establishments and restaurants.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results67
2008
Trend in Selected Crime Categories in Capital Health (Excluding West Hants), 2008 to 2012Figure 36
2009 2010 2011 2012
Theft – Under $5000
Mischief
Assaults
Break & Enter (Home/Business/Other)
Traffic Offences
Posession/Trafficking of Stolen Goods
Fraud/Identity Theft
Drug Possession/Trafficking/Production/Import
Impaired Operation of a Vehicle/Boat
Theft – Over $5000
Youth Complaint/Crime
Arson
Homicide/Attempted Homicide
10000 30002000 4000 5000 6000 7000 8000 9000
Number of Reported Crimes
SUMMARY
In this population health report, we did not find significantrelationships between self-rated mental health and total,material or social deprivation. Significant relationships were found between mental health and a number of factorsincluding stress in daily life and a weak sense of belonging.Of the nine community issues that were explored, loss of respect (by young people) for elders and vandalism ortheft were perceived as the two most serious issues in communities. There is a variation in crime density within thedistrict.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Results68
Density of Selected Crimes per 1,000 Population in Capital Health (Excluding West Hants), 2008-2012Figure 37
Data was provided by Halifax Regional Police (2013).
0 - 286.2
> 286.2 - 673.5
> 673.5 - 1390.3
> 1390.3 - 3054.2
> 3054.2 - 6196.7
H D’Agelo-Scott, PhD, ROH UCU, Public Health, Capital Health ArcGIS 10.1
DATA:
1) HRP, 2013Decdmber 3, 2013
Crime Density

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Results69

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T70

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Discussion71

The underlying premise for this population health status report was to demonstrate that geography matters, as within thegeography of communities, people experience a combination of risk factors, community factors and levels of relative deprivation that ultimately influence health outcomes. It is with this in mind that this population health status report exploredthe associations between these geographically based components and three health outcomes: obesity, alcohol, and mental health.
While there are a number of deprivation indices being used in Canada (Ontario Marginalization Index, the INSPQ [Institut national du santé publique du Quebec] Deprivation Index, and the Vancouver Area Neighbourhood Deprivation Index [VANDIX]),the INSPQ deprivation index was used for this report as it was readily available through CIHI. The INSPQ deprivation indexhas been used in other studies (Canadian Population Health Initiative & CIHI, 2009; CIHI, 2010a; CIHI, 2010b) and so the reliability and validity of the index is well established in Canadian public health circles Although the different indices may bebased on different socioeconomic variables, the intent of all of the indices is to enable a measure of socioeconomic statusthat can be used to define health status patterns within a population. By having such a measure, inequalities in health andsocial well-being between population groups or between geographical areas can be better understood (Region of Peel, 2011).This is particularly important for public health practice, as in order to locate the most vulnerable groups, an awareness of thevariations in deprivation is necessary (Pampalon, Hamel, Gamache, Philibert, Raymond, & Simpson, 2012).
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Discussion72
The INSPQ deprivation index allows for separation of the two components, material and social deprivation, to assessthe independent impact of each component. An interesting finding in this report has been the rather consistent finding that higher material deprivation is not necessarily associated with higher social deprivation. For example,the rural Community Health Boards are the least sociallydeprived while being the most materially deprived. We havedemonstrated separate influences from each component in both outcomes and risk factors analyses. This finding suggests that there is value in exploring material and socialdeprivation independently from total deprivation in analysesof health outcomes.
Another interesting finding in this report has been the differences in the deprivation values for communities as compared to the smaller dissemination areas of which the communities are composed. For most communities, even those of lowerdeprivation, we found pockets of higher deprivation within them, which represent opportunities for targeted interventions.This was true for both material and social deprivation, and reinforces our hypothesis that when information is available at thelowest possible levels of geography, it may shift understanding of the health outcome, its distribution, and its root causes.
This report found associations between deprivation and obesity, and deprivation and heavy alcohol drinking. No clear association was found between mental health and deprivation when using self-reported mental health as a proxy measurefor mental health. Deprivation was significantly associated with obesity with individuals residing in areas with higher totaldeprivation more likely to be overweight or obese. When looking at material and social deprivation, increasing material deprivation was linked to increased odds of being overweight or obese but not social deprivation. The link between deprivationand being overweight or obese may be associated with reduced availability of fresh foods and fitness amenities in areas ofhigher deprivation. It may be that individuals residing in areas of higher material deprivation have limited resources to buyfood. Fruit and vegetable consumption is commonly used as a measure for healthy eating, however, the relationship betweenbeing overweight or obese and fruit and vegetable consumption is less clear with varying conclusions from studies (Giskes,Van Lenthe, Avendano-Pabon, & Brug, 2011; Heo et al., 2011; Ledoux, Hingle, & Baranowski, 2011; Vioque, Weinbrenner,Castelló, Asensio, & Garcia de la Hera, 2008).

Studies have suggested that access to food may be a priority for reducing obesity (Lopez, 2007). We did not systematicallyanalyze the density of grocery store locations as a risk factor for obesity in this population health status report; however,when considering the communities within Capital Health, we did find the highest density of grocery locations was in Hubbardsand Moser River. It was also found that many communities had few or no grocery store locations. There is some evidencethat lower consumption of fruits and vegetables among lower socioeconomic groups may be due to an increased likelihoodof fast food and take-out consumption (Glantz, Basil, Maibach, Goldberg, & Snyder, 1998; Pereira, et al., 2005). Similarly toour analysis of grocery stores, systematic analyses of fast food density was not done in this population health status report,however, we found the high density of fast food locations to be in Halifax Citadel, a community with a total deprivation indexof 4 (20 to 40% most deprived). Although the association between food security and obesity could not be analyzed for thispopulation health status report, there is a growing body of literature that supports the link between obesity, food security anddeprivation. The issue of food security as a potential risk factor for obesity requires further exploration at a community level.
The physical activity guidelines for adults aged 18 to 64 years recommend at least 150 minutes of moderate to vigourousintensity aerobic physical activity per week in periods of 10 minutes or more, and muscle and bone strengthening activitiesat least 2 days per week. In the sample population used in this report, over 40% of Capital Health residents reported beingphysically inactive. A significant association was found between being overweight or obese and being physically inactive.While a significant association was not found between deprivation and physical activity, studies have reported a relationshipwhen considering the built environment (Black & Macinko, 2008; Black & Macinko, 2010; Duranceau & Bergeron, 2013).The built environment can be defined as all of the buildings, spaces and products, including our homes, schools, workplaces,parks, business centres, and roads. As succinctly stated by Lopez (2007), “Where one lives may affect obesity status”.Analyses for obesity by fitness amenities were not included in this population health report. However, the geographic distribution of parks and park features and trails suggests a concentration of those features in urban areas.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Discussion73
In Capital Health, individuals who reported fruit and vegetable consumption at or above the recommended guidelines had decreased odds of being obese. Literaturesuggests an association between socioeconomic status andfruit and vegetable consumption with lower socioeconomicgroups less likely to consume fruits and vegetables in theirdiets (Dubowitz et al., 2008; Giskes, Avendano, Brug, &Kunst, 2010). We found an association between total deprivation and fruit and vegetable consumption below therecommended guidelines. This link may be due to the presence of “food deserts” in communities, where individuals experience a lack of readily available produce, or“food swamps” , where individuals experience a high con-centration of unhealthy fast, processed and packaged foods (Dubowitz, Ghosh – Dastidar, Steiner, Escarce, & Collins, 2013;Jones, Terashima, & Rainham, 2009; Robitaille, Bergeron, & Lasnier, 2010). Some researchers have stated that the presenceof food deserts in low socioeconomic areas is a contributing factor to lower fruit and vegetable consumption and hence, obesity. While definitions may vary about what exactly constitutes a food desert (Jiao, Moudon, Ulmer, Hurvitz, & Drewnowski,2012), many define a food desert as a disadvantaged geographical area with relatively poor access to health and affordablefood. The examination of food deserts and their interplay with communities’ ability to access healthy food has been a newarea of research over the last few years, aided by the use of geographical mapping techniques to assist with the analysis.There is a current lack of quality, comprehensive research in the Canadian context linking food deserts and their existencein low socioeconomic areas. Further research is needed to determine the existence and strength of this link.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Discussion74
Similar to obesity, an association between heavy drinkingand deprivation was found. Alcohol use impacts our culture,economy, politics, health status and relationships. In HalifaxRegional Municipality, there were over 1000 arrests madefor impaired driving of a vehicle or a boat in 2012 (HalifaxRegional Police, 2013). The Nova Scotia alcohol strategy,‘Changing the Culture of Alcohol Use in Nova Scotia’ reported an average of 3,100 hospital admissions(42,000 hospital days) in Nova Scotia that can be attributedto alcohol, with 230 alcohol-related deaths occurring annually (Department of Health Promotion and Protection,2007). Other undesirable outcomes linked to alcohol includephysical and sexual assaults, family and intimate partner violence, and numerous chronic diseases (CDC, 2011). In this report, we describe patterns of alcohol consumption that revealtrends towards harmful behaviours. In 2011, 19.0% of Canadians reported having 5 or more drinks on one occasion, at leastonce a month in the previous year (Statistics Canada, 2013g). In Nova Scotia, 20.3% reported having 5 or more drinks, whilein Capital Health, 20.4% reported having 5 or more drinks. Interestingly, the daily consumption of alcohol in Capital Healthand Nova Scotia was less than the daily consumption among Canadians. While daily drinking may be less likely here, regularheavy drinking is more likely.
We found that with increasing total deprivation, heavy drinking was more likely. While social deprivation was not linked toheavy drinking, material deprivation was. We found that individuals in the highest material deprivation and the 20 to 40%least deprived categories were more likely to participate in heavy drinking. The findings of a number of studies have shownthat lower socioeconomic status is associated with an increased likelihood of heavy drinking (Batty et al., 2008; Baumann etal., 2007; Matheson, White, Moineddin, Dunn, & Glazier, 2012) and increased harmful impacts from heavy alcohol consumption (Batty et al., 2008; Cerdá, Johnson-Lawrence, & Galea, 2011; Erskine, Maheswaran, Pearson, & Gleeson,2010). Similar to our findings for material deprivation and heavy alcohol use, a U-shaped pattern has been found in the literature. In addition to the influence of deprivation and risk factors on heavy drinking, community factors must also be considered. Based on a number of studies, communities with a high density of alcohol outlets are more likely to have higherrates of violence, drinking and driving, motor vehicle related pedestrian injuries; child abuse and neglect; and alcohol-relateddeaths (Campbell et al., 2009; Stockwell et al., 2011; Task Force on Community Preventive Services, 2009). Ahern, Margerison-Zilko, Hubbard, and Galea (2013) reported an increased prevalence in binge drinking with increased alcoholoutlet density. Detailed analyses of alcohol outlet density with respect to heavy drinking were not conducted in this populationhealth status report. However, we did find the highest liquor store density was in Eastern Shore – Musquodoboit, followed byHalifax Peninsula. The highest sales per capita were in Halifax Peninsula.
Mental health has been defined as “a state of well-being in which the individual realizes his or her own abilities, can copewith the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community.”(WHO, 2011b) Positive mental health is increasingly being linked with positive overall health with some arguing that it is impossible to separate mental health from physical health (Prince et al., 2007). One’s mental health status is influenced bya variety of determinants throughout their life span including biological, social, and economical determinants (CIHI, 2009). Inaddition to the physical and emotional consequences of mental illness, mental illness also poses huge economic burden onour society. It is estimated that direct cost of mental illness in Canada is around $43.3 billion and the indirect costs are estimated at $6.3 billion (Risk Analytica, 2011). It is projected that mental illness will be the leading cause of disability inhigh income countries by 2030 (Mathers & Loncar, 2006).

LIMITATIONS
In our population health status report, we have found that more Nova Scotians report fair or poor mental health when comparedto the rest of Canada. This percentage is even higher for people who live within the Capital Health boundaries. In this healthreport and contrary to other studies (CIHI, 2008; Stafford & Marmot, 2003), we found self-rated negative mental health wasnot associated with deprivation. It is possible that our finding is due to the choice of self-rated mental health as the variableof study; other variables may have yielded a different result. Stress in daily life was significantly higher among those withself-rated mental health, which may be due to a heightened reaction to daily stressors which results in a heightened likelihoodof reporting anxiety and depressive disorders (Charles, Piazza, Mogle, Sliwinski, & Almeida, 2013). However, we did not finda relationship between stress in daily life and deprivation. This finding is contrary to the literature which suggests high levelsof stress among those with adverse social and material living conditions, which may lead to an increased vulnerability forchronic diseases (Mikkonen & Raphael, 2010).
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Discussion75
The correlation between sense of belonging and mentalhealth has been suggested by a number of studies. Whilethe concept of belonging is difficult to quantify, a strongsense of belonging has been associated with better self-reported health (Kitchen, P., Williams, A., & Chowhan, J.(2012). In our report, we found that individuals with a weak sense of belonging were more likely to report negativemental health. We found a relationship between sense of belonging and material deprivation. Those residing in the20 to 40% most materially deprived areas were more likelyto report a weak sense of belonging. Further exploration is needed to fully understand this relationship. Communityfactors have been shown to have a potential impact on mental health. The occurrence of negative life events and high rates of violent crime have been linked to depression (Kim,2008; Stafford, Chandola, & Marmot, 2007). When looking at crime rates for Capital Health, while there appears to be adownward trend in the number of crimes, there were areas with higher density of the crime categories selected for this population health status report.
Overall for the three outcomes we explored, we were able find variation by geography and deprivation. Our report, while byno means conclusive, certainly points to deprivation as influencing health status in a number of ways, including through influencing the community conditions and individual risk factors from which poor health outcomes arise.
One of the most significant limitations with this population health status report is that it is cross-sectional using data fromone point in time. While cross-sectional studies are used to explore associations between outcomes and risk factors, includingdeprivation, there is no indication of when the exposure to the risk factor occurred – before, during or after the onset of theoutcome. As such, causality cannot be inferred. For example, while an association was found between heavy drinking andmaterial deprivation, it is unknown if material deprivation caused heavy drinking or heavy drinking caused material deprivation.Cross-sectional studies indicate the possible existence of associations to promote discussion and further investigation throughresearch.
It is important to recognize that there are a number of limitations associated with deprivation indices. One limitation is theuse of area-based deprivation measures as opposed to individual-level data may not reflect the factors that lead to some individuals being healthier than others (Bell & Hayes, 2012). All deprived people may not live in deprived areas and all people

living in deprived areas may not be deprived. As well, the INSPQ does not consider all social determinants of health such asethnicity and immigration. As indices typically use postal codes for the assignment of individuals to deprivation area by dissemination area, there may be errors as postal codes and dissemination areas may not match, particularly in rural areas.Since the development of the INSPQ Deprivation Index, it has been used extensively in Quebec and throughout Canada to explore geographic variations in deprivation, inequalities in population health status, and service use according to deprivation(Pampalon et al., 2012). One of the noted advantages of the index is its use in identifying significant inequalities in healthstatus and health service use. However, the index has been criticized for misrepresenting in particular social deprivation byusing measures that may no longer accurately describe “at risk” populations. For example – lone parenthood and singlestatus in some circumstances may not necessarily denote vulnerability as they may have in the past. The index has also beencriticized for its use of the term “deprivation”, which many public health practitioners feel misrepresents the resiliency heldin many communities that would score low in index. In this technical report we have chosen to use the word “deprivation”simply for the sake of consistency with the original INSPQ methodologies. Other language to describe the concept will besought for further (publically-oriented) knowledge translation products.
Use of secondary data sources, such as the CCHS data, has a number of advantages including a reduction in time neededto collect primary data, the sample size, the representativeness of the data, and a reduction of recall bias (Sorensen, Sabroe,& Olsen, 1996). However, there are disadvantages associated with the use of secondary data. As the data collection methodology and selection and quality of the data are not controlled by the user, the validation of the data may pose a problem(Sorensen, Sabroe, & Olsen, 1996). However, other studies have used survey data such as the CCHS to evaluate the healthof the population (Caron & Liu, 2011; Gariepy et al., 2010a; Khaled, Bulloch, Exner, & Patten, 2009; Lorant, Croux, Weich,Deliege, Mackenbach, & Ansseau, 2007; Romans, Cohen, & Forte., 2011; Satyanarayana, Enns, Cox, & Sareen, 2009). Futurereporting projects from Capital Health will examine the feasibility of de novo data collection as part of the process.
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Discussion76
Reporting bias in a number of the factors used to explorehealth outcomes may have occurred. Self-reported heightand weight are frequently biased, resulting in mis-classification of the BMI category. There is evidence to suggest that the BMI categories may actually be higher. Arecent study conducted by Shields, Gorber, and Tremblay(2008) found height was over-reported, particularly amongthose who were the shortest, and weight was under-reported, particularly among those who were overweight or obese, in the 2005 CCHS. The researchers reported theestimated prevalence of obesity when using measured datawas 7% higher than the prevalence based on self-reporteddata. Stigmatization associated with negative mental health and disclosing a mood disorder may have resulted in underreporting as well. The use of self-rated mental healthmay not have accurately measured mental health. CIHI (2009) found when comparing self-rated mental health and life satisfaction, areas with high self-rated mental health were not necessarily the areas with high life satisfaction. Studies indicatethat mental health can be characterized by one’s maturity, emotional and social intelligence and resilience as well as subjectivewell-being (Rissanen et al., 2011). While there are clinical tools and assessment instruments to evaluate one’s mental healthstatus, subjective measures such as self-report on well-being have been used to evaluate one’s mental health (Bellis et al.,2012; Gariepy et al., 2010b; Koivumaa-Honkanen, Kaprio, Honkanen, Viinamäki, & Koskenvuo, 2004; Koivumaa-Honkanen,Kaprio, Korhonen, Honkanen, Heillila, & Koskenvuo, 2012; Rissanen et al., 2011; Schmitz, Lesage, & Wang, 2009).

OUR LESSONS LEARNED REGARDING OUR FIRST POPULATION HEALTH STATUSREPORT
For this population health status report, a framework was developed to explore three topics, obesity, alcohol, and mentalhealth. At first glance, the framework appears to be simple – the linking of a health outcome to deprivation, and then to riskfactors and community factors, and then finally linking the deprivation to the significant risk factors and community factors.The selection of topics was based on priority issues for Nova Scotia and our Community Health Board partners. It is possiblethat a review of existing data for each topic for Capital Health to determine if these issues were disproportionately representedin the district may have suggested other issues requiring more immediate attention. Regardless of the topics for a populationhealth status report, consideration of the availability of data at the level of geography desired for analysis is necessary.
The most significant challenge found in this reporting effort was the lack of available data at the dissemination level and/orcommunity level. The only data available for the health outcomes at the dissemination data were from CCHS. While the samplesize for 2009/10 was larger than other survey years, the CCHS data were intended to represent CHBs and not communities.As a result, not all communities were represented by the CCHS data, and so meaningful analyses by community could notbe conducted. As well, for some variables, such as food security, the sample size was too small for analyses.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Discussion77
The three topics of focus for the population health status report are complex with many possible associated factors,and as such, we did not capture all of the factors due to datalimitations. Data sources for other factors were not readilyavailable to Public Health and limited the ability to presenta more complete assessment of the health outcomes. Thelack of available identifiable data at low levels of geographyis a concern as it will impede the development of future population health status reports.
While a technical document is often a product of population health status reporting, there was recognition that additionalproducts would be required for knowledge translation and dissemination of the report. We underestimated the time and resources needed to produce a population health status report, particularly a report that is based on a multi-level frameworksuch as this one. While we established a timeline early in the process, completion dates were regularly modified due to sourcingof updated data, conflicting priorities, and departure of key staff members. A key difference in this report as compared tothose produced by other Canadian cities is that this report, being our first report, was not designed to create recommendationsfor policy. Rather, at this stage, we wished to test the feasibility of producing a population health status report. It is our hopethat future reports would start to frame policy recommendations based on the report findings.
The knowledge, experience, and insight of the National Collaborating Centres for the Determinants of Health (NCCDH) andthe Learning Circle members greatly contributed to the development of this population health status report. Consultation withkey partners, including our Community Health Board members, Capital Health Mental Health and Addictions, Capital HealthPrimary Care, and Dalhousie University, throughout the process was important as it increased awareness of the reportand allowed for feedback through the process.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T78

As stated by Pampalon, et al. (2012), the material and social deprivation index is a “marker of social inequalities in health”(p. 521) which can be used to monitor social inequalities over time and space. In this population health status report, we have shown that there are variances in health status by deprivation within Capital Health, between CHBs, between communities and within communities. These associations suggest a need to consider the underlying factors which impacthealth when determining action and establishing policies intended to address health inequities.
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Conclusion79
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T80

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
References81
Ahern, J., Margerison-Zilko, C., Hubbard, A., & Galea, S. (2013).Alcohol outlets and binge drinking in urban neighborhoods:the implications of nonlinearity for intervention and policy.American Journal of Public Health, 103 (4), e81-7.
Association of Public Health Epidemiologists in Ontario.(2012). Core indicators. Retrieved from http://www.apheo.ca/index.php?pid=55
Batty, G.D., Lewars, H., Emslie, C., Benzeval, M. & Hunt, K.(2008). Problem drinking and exceeding guidelines for 'sensible' alcohol consumption in Scottish men: associationswith life course socioeconomic disadvantage in a population-based cohort study. BMC Public Health 8(302). doi: 10.1186/1471-2458-8-302.
Baumann, M., Spitz, E., Guillemin, F., Ravaud, J-F., Choquet,M., Falissard, B. Lorhandicap Group. (2007). Associations ofsocial and material deprivation with tobacco, alcohol andpsychotropic drug use, and gender: A population – basedstudy. Retrieved from http://www.ij-healthgeographics.com/content/6/1/50. doi: 10.1186/1476-072X-6-50
Befort, C.A., Nazir, N., & Perri, M.G. (2012). Prevalence ofobesity among adults from rural and urban areas of theUnited States: Findings from NHANES (2005 - 2008). Journalof Rural Health, 28(4): 392-97. doi: 10.1111/j.1748-0361.2012.00411.x
Bell, N. & Hayes, M.V. (2012). The Vancouver Area neighbourhood deprivation index (VANDIX): A census-basedtool for assessing small-area variations in health status.Canadian Journal of Public Health, 103 (8 Suppl. 2): S28-32.
Bellis, M. A., Lowey, H., Hughes, K., Deacon, L., Stansfield, J.,& Perkins, C. (2012). Variations in risk and protective factorsfor life satisfaction and mental wellbeing with deprivation: Across-sectional study. BMC Public Health, 12(492).doi:10.1186/1471-2458-12-492
Black, J.L., & Macinko, J. (2008). Neighborhoods and obesity.Nutrition Reviews, 66(1), 2-20.
Black, J.L., & Macinko, J. (2010). The changing distributionand determinants of obesity in the neighborhoods of NewYork City, 2003-2007. American Journal of Epidemiology,171(7), 765-75.
Brownstone, D. & Golob, T.F. (2009). The impact of residentialdensity on vehicle usage and energy consumption. Journal ofUrban Economics, 65; 91-98.
Campbell, C.A., Hahn, R.A., Elder, R., Chattopadhyay, S.,Brewer, R., Fielding, J. Task Force on Community PreventiveServices. (2009). The effectiveness of limiting alcohol outletdensity as a means of reducing excessive alcohol consumption and alcohol-related harms. American Journal ofPreventive Medicine 37(6), 556-69.
Campiano, R.M. & Hystad, P.W. (2011). Sense of communitybelonging in health surveys: what social capital is it measuring? Health & Place, 17(2), 606-17.
Canadian Institute for Health Information. (n.d.) Variables. Retrieved from http://www.cihi.ca/cihi-ext-portal/xls/internet/cphi_cma_depindex_excel_en
Canadian Institute for Health Information. (2008). ReducingGaps in Health: A Focus on Scocio-Economic Status in UrbanCanada. Retrieved from https://secure.cihi.ca/free_prod-ucts/Reducing_Gaps_in_Health_Report_EN_081009.pdf
Canadian Institute for Health Information. (2009). Exploringpositive mental health. Retrieved from http://www.cpa.ca/cp-asite/userfiles/Documents/Practice_Page/positive_mh_en.pdf
Canadian Institute for Health Information. (2010a). Data brief:Exploring urban environments and inequalities in health, Halifax census metropolitan area. Retrieved fromhttp://www.cihi.ca/ CIHI-ext-portal/pdf/internet/PDF_DATA-BRIEF_HALIFAX_EN
Canadian Institute for Health Information. (2010b). Hospitalization disparities by socio-economic status formales and females. Retrieved from https://secure.cihi.ca/free_products/disparities_in_hospitalization_by_sex2010_e.pdf
Canadian Population Health Initiative & Canadian Institute forHealth Information. (2009). Proceedings from: The INSPQDeprivation Index for Health in Canada: Applications for Research, Policy and Practice. Retrieved from https://secure.cihi.ca/free_products/DepIndexProceedingsReportENGFinal.pdf
Caron, J., & Liu, A. (2011). Factors associated with psycho-logical distress in the Canadian population: a comparison oflow-income and non low-income sub-groups. CommunityMental Health Journal, 47(3), 318–30. doi:10.1007/s10597-010-9306-4
Carpiano, R. & Hystad, P. (2011). Sense of community belonging in health surveys: What social capital is it measuring? Health and Place, 17(2): 606-17.
Centers for Disease Control and Prevention. (2011). Excessive alcohol use: Addressing a leading risk for death,chronic disease, and injury at a glance 2011. Retrieved fromhttp://www.cdc.gov/chronicdisease/resources/publications/aag/alcohol.htm
Cerdá, M., Johnson-Lawrence, V.D., & Galea, S. (2011). Lifetime income patterns and colcohol consumption: investigating the association between long- and short-termincome trajectories and drinking. Social Science and Medicine, 73(8), 1178-85.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
References82
Charles, S.T., Piazza, J.R., Mogle, J., Sliwinski, M.J., &Almeida, D.M. (2013). The wear and tear of daily stressors onmental health. Psychological Science, 24(5): 733-41. Abstract retrieved from http://pss.sagepub.com/content/24/5/733
Chen, Y., Jiang, Y., & Mao, Y. (2009). Association betweenobesity and depression in Canadians. Journal of Women’sHealth (2002), 18(10), 1687–92. doi:10.1089/jwh.2008.1175
Clean Air Partnership. (2010). Benchmarking Active Transportation in Canadian Cities. Retrieved fromhttp://www.cleanairpartnership.org.
Clifton, K.J. & Dill, J. (2005). Women’s travel behavior andland use: Will new styles of neighborhoods lead to morewomen walking? Transportation Research Board: 89–99.
Cohen, S., Gottlieb, B.H., & Underwood, L.G. (2000). Socialrelationships and health. In S. Cohen, L.G. Underwood, & B.H.Gottlieb (Eds.), Social support measurement and intervention.New York: Oxford University Press.
Commission on Social Determinants of Health (2008). Closingthe gap in a generation: health equity through action on thesocial determinants of health. Final Report of the Commissionon Social Determinants of Health. Geneva, World Health Organization. Retrieved from http://www.who.int/social_determinants/thecommission/finalreport/en/index.html
Department of Health Promotion and Protection. (2007). Analcohol strategy to prevent and reduce the burden of alcohol-related harm in Nova Scotia. Retrieved from http://www.gov.ns.ca/ohp/publications/alcohol_strategy.pdf
Department of Health and Wellness. (2012). Together we can:The plan to improve mental health and addictions care forNova Scotians. Halifax, NS: Government of Nova Scotia.
Dubowitz, T., Ghosh-Dastidar, M.B., Steiner, E., Escarce, J.J., & Collins, R.L. (2013). Are our actions aligned with ourevidence? The skinny on changing the landscape of obesity.Obesity, 21(3): 419-20.
Dubowitz, T., Heron, M., Bird, C.E., Lurie, N., Finch, B.K., Basturto-Davila, R., Hale, L., & Escarce, J.J. (2008). Neighborhood socioeconomic status and fruit and vegetableintake among whites, blacks, and Mexican Americans in theUnited States, The American Journal of Clinical Nutrition,87(6): 1883-91.
Duranceau, A., & Bergeron, P. (2013). Built environment andphysical activity among young people. Québec, PQ: InstitutNational de Santé Publique du Québec.
Elani, H.W., Harper, S., Allison, P.J., Bedos, C. & Kaufman,J.S. (2012). Socio-economic inequalities and oral health inCanada and the United States. Journal of Dental Research,91(9), 865-70.
Erskine, S., Maheswaran, R., Pearson, T., & Gleeson, D.(2010). Socioeconomic deprivation, urban-rural location andalcohol-related mortality in England and Wales. BMC PublicHealth, 10(99). doi: 10.1186/1471-2458-10-99.
Franklin, B., Jones, A., Love, D., Puckett, S., Macklin, J., &White-Means, S. (2012). Exploring mediators of food insecurity and obesity: A review of recent literature. Journalof Community Health, 37(1), 253-264.
Friedli, L. (2009). Mental health, resilience and inequalities.Retrieved from http://www.euro.who.int/__data/ assets/pdf_file/0012/100821/E92227.pdf
Gadalla, T. M. (2009). Association of obesity with mood andanxiety disorders in the adult general population. Chronic Diseases in Canada, 30(1), 29–36.
Gamache, P., Pampalon, R., & Hamel, D. (2010). Methodolog-ical guide: The material and social deprivation index: a summary. Québec, PQ: Institut National de Santé Publique duQuébec.
Gariepy, G., Wang, J., Lesage, A., & Schmitz, N. (2010a). Theinteraction of obesity and psychological distress on disability.Social Psychiatry and Psychiatric Epidemiology, 45(5), 531–40. doi:10.1007/s00127-009-0090-9
Gariepy, G., Wang, J., Lesage, A., & Schmitz, N. (2010b). Thelongitudinal association from obesity to depression: Resultsfrom the 12-year national population health survey. Obesity,18(5), 1033-1038.
Gauvin, L, Riva, M, Barnett, T, Richard, L, Craig, C.L., Spivock,M. Gagne, S. (2008). Association between neighbourhood active living potential and walking. American Journal of Epidemiology, 167(8): 944-53.
German, D. & Latkin, C.A. (2012). Social stability and health:exploring multidimensional social disadvantage. Journal ofUrban Health 89(1), 19-35.
Giskes, K., Avendano, M., Brug, J., & Kunst, A. (2010). A systematic review of studies on socioeconomic inequalities indietary intakes associated with weight gain and overweight/obesity conducted among European adults. Obesity Reviews,11(6), 413-429.
Giskes, K., van Lenthe, F., Avendano-Pabon, M., & Brug, J.(2011). A systematic review of environmental factors andobesogenic dietary intakes among adults: are we gettingcloser to understanding obesogenic environments? ObesityReviews, 12(5).

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
References83
Glanz, K., Basil, M., Maibach, E., Goldberg, J., & Snyder, D. (1998). Why Americans eat what they do: taste, nutrition,cost, convenience, and weight control concerns as influenceson food consumption. Journal of the American Dietetic Association, 98(10): 1118-26.
Government of Nova Scotia. (2013). Nova Scotia CommunityCounts. Retrieved from: http://www.novascotia.ca/finance/communitycounts/geogpage.asp
Grant, B.F., Hasin, D.S., Chou, S.P., Stinson, F.S., & Dawson,D.A. (2004). Nicotine dependence and psychiatric disordersin the United States: Results from the National EpidemiologicSurvey on Alcohol and Related Conditions. Archives of General Psychiatry 61:1107–1115.
Guh, D. P., Zhang, W., Bansback, N., Amarsi, Z., Birmingham,C. L., & Anis, A. H. (2009). The incidence of co-morbiditiesrelated to obesity and overweight: A systematic review andmeta-analysis. BMC Public Health, 9(88).
Halifax Regional Police. (2013). Halifax Regional Municipalitycrime data, 2007-2012 [Data file]. Halifax, NS: Halifax Regional Police.
Harrington, D. W., & Elliott, S. J. (2009). Weighing the importance of neighbourhood: A multilevel exploration of thedeterminants of overweight and obesity. Social Science &Medicine, 68(4), 593-600.
Heo, M., Kim, R. S., Wylie-Rosett, J., Allison, D. B., Heymsfield,S. B., & Faith, M. S. (2011). Inverse association between fruitand vegetable intake and BMI even after controlling for demographic, socioeconomic and lifestyle factors. ObesityFacts, 4(6), 449-455.
Hess P, Moudon A, Snyder M, Stanilov K. Site Design andPedestrian Travel. Transportation Research Record: Journal ofthe Transportation Research Board. 1999 Jan 1; 1674(-1):9-19.
Hystad, P. & Carpiano, R.M. (2012). Sense of community-belonging and health-behaviour change in Canada. Journal ofEpidemiology and Community Health, 66(3), 277-83.
Jiao, J., Moudon, A.V., Ulmer, J., Hurvitz, P.M. & Drewnowski,A. (2012). How to identify food deserts: measuring physicaland economic access to supermarkets in King County, Washington. American Journal of Public Health, 102(10),e32-9.
Jones, J., Terashima, M., & Rainham, D. (2009). Fast foodand deprivation in Nova Scotia. Canadian Journal of PublicHealth, 100(1): 32-5.
Kawachi, I, & Berkman, L.F. (2001). Social ties and mentalhealth. Journal of Urban Health, 78(3): 458-67. Retrievedfrom http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3455910/
Kessler, R.C. (1982). A disaggregation of the relationship between socio-economic status and psychological distress.American Sociological Review, 46, 752-64.
Khaled, S. M., Bulloch, A., Exner, D. V, & Patten, S. B. (2009).Cigarette smoking, stages of change, and major depressionin the Canadian population. Canadian Journal of Psychiatry.Revue Canadienne de Psychiatrie, 54(3), 204–8.
Khokhar, W. A., Clifton, A., Jones, H., & Tosh, G. (2011). Oralhealth advice for people with serious mental illness. TheCochrane Database of Systematic Reviews, (11), CD008802.doi:10.1002/14651858.CD008802.pub2
Kim, D. (2008). Blues from the neighborhood? Neighborhoodcharacteristics and depression. Epidemiologic Reviews, 30,101–17. doi:10.1093/epirev/mxn009
King, A. (2012). Oral health - more than just cavities. A reportby Ontario's Chief Medical Officer of Health. Retrieved fromhttp://www.health.gov.on.ca/en/common/ministry/publications/reports/oral_health/oral_health.pdf
Kitchen, P., Williams, A., & Chowhan, J. (2012). Sense ofcommunity belonging and health in Canada: A regional analysis. Abstract retrieved from http://link.springer.com/article/10.1007%2Fs11205-011-9830-9. doi: 10.1007/s11205-011-9830-9.
Koivumaa-Honkanen, H., Kaprio, J., Honkanen, R., Viinamäki,H., & Koskenvuo, M. (2004). Life satisfaction and depressionin a 15-year follow-up of healthy adults. Social Psychiatryand Psychiatric Epidemiology, 39(12), 994–9. doi:10.1007/s00127-004-0833-6
Koivumaa-Honkanen, H., Kaprio, J., Korhonen, T., Honkanen,R. J., Heikkilä, K., & Koskenvuo, M. (2012). Self-reported lifesatisfaction and alcohol use: a 15-year follow-up of healthyadult twins. Alcohol and Alcoholism, 47(2), 160–8.doi:10.1093/alcalc/agr151
Kruger, J., Ham, S. A., & Prohaska, T. R. (2009). Behavioralrisk factors associated with overweight and obesity amongolder adults: The 2005 national health interview survey. Preventing Chronic Disease, 6(1).
Ledoux, T.A., Hingle, M.D., & Baranowski, T. (2011). Relation-ship of fruit and vegetable intake with adiposity: a systematicreview. Obesity Reviews, 12(5).
Lopez, R. P. (2007). Neighborhood risk factors for obesity.Obesity, 15(8), 2111-2119.
Lorant, V., Croux, C., Weich, S., Deliège, D., Mackenbach, J.,& Ansseau, M. (2007). Depression and socio-economic riskfactors: 7-year longitudinal population study. The British Journal of Psychiatry: The Journal of Mental Science, 190,293–8. doi:10.1192/bjp.bp.105.020040

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
References84
Lu, X.Y. (2007). The leptin hypothesis of depression: a potential link between mood disorders and obesity? CurrentOpinion in Pharmacology 7(6), 648-52.
Mathers, C.D., & Loncar, D. (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLoSMedicine, 3(11), e442.
Matheson, F.I., Moineddin, R., & Glazier, R.H. (2008). Theweight of place: A multilevel analysis of gender, neighborhoodmaterial deprivation, and body mass index among Canadianadults. Social Science and Medicine, 66(3), 675-90.
Matheson, F.I., White, H.L., Moineddin, R., Dunn, J.R., &Glazier, R.H. (2012). Drinking in context: the influence of gender and neighborhood deprivation on alcohol consumption.Journal of Epidemiology and Community Health, 66(6), e4.
McKinney, C.M., Chartier, K.G., Caetano, R., & Harris, T.R.(2012). Alcohol availability and neighborhood poverty andtheir relationship to binge drinking and related problemsamong drinkers in committed relationships. Journal of Interpersonal Violence, 27(13), 2703-27.
McLaren, L. (2007). Socioeconomic status and obesity. Epidemiologic Reviews, 29, 29-48.
Mikkonen, J., & Raphael, D. (2010). Social determinants ofhealth: The Canadian facts. Retrieved from http://ywca-canada.ca/data/research_docs/00000131.pdf
National Obesity Observatory. (2011). Obesity and mentalhealth. Retrieved from http://www.noo.org.uk/uploads/doc/vid_10266_Obesity%20and%20mental%20health_FINAL_070311_MG.pdf
Nova Scotia Public Health. (2010). Moving forward: A commitment to Public Health's future. Retrieved fromhttp://www.gov.ns.ca/hpp/yourmove/yourmove-movingforward.pdf
Orpana, H.M., Berthelot, J., Kaplan, M.S., Feeny, D.H., McFarland, B., & Ross, N.A. (2010). BMI and mortality: Results from a national longitudinal study of Canadian adults.Obesity. 18:214–218.
Pampalon, R., Hamel, D., Gamache, P., Philibert, M.D., Raymond, G., & Simpson, A. (2012). An area-based materialand social deprivation index for Public Health in Quebec andCanada. Canadian Journal of Public Health, 103 (8 Suppl. 2):S17–22.
Pampalon, R., & Raymond, G. (2000). A deprivation index forhealth and welfare planning in Quebec. Chronic Diseases inCanada, 21(3), 104 – 113.
Pan-American Health Organization. (1999). Methodologicalsummaries: Measuring inequity in health. EpidemiologicalBulletin, 20(1). Retrieved from http://www.paho.org/english/sha/be991cov.htm
Paul, L.A., Grubaugh, A.L., Frueh, B.C., Ellis, C., & Egede, L.E.(2011). Associations between binge and heavy drinking andhealth behaviors in a nationally representative sample. Retrieved from https://canvas.brown.edu/courses/350909/files/20953022/download?.doi: 10.1016/j.addbeh.2011.07.034.
Pereira, M.A., Kartashov, A.I., Ebbeling, C.B., Van Horn, L., Slattery, M.L., Jacobs, D.R. Jr., & Ludwig, D.S. (2005).Fast-food habits, weight gain, and insulin resistance (theCARDIA study): 15-year prospective analysis. Lancet365(9453), 36-42.
Pereira, G., Wood, L., Foster, S., & Haggar, F. (2013). Accessto alcohol outlets, alcohol consumption and mental health.PLoS One, 8(1), e53461.
Popova, S., Giesbrecht, N., Bekmuradov, D., & Patra, J.(2009). Hours and days of sale and density of alcohol outlets:Impacts on alcohol consumption and damage: A systematicreview. Alcohol & Alcoholism, 44(5): 500-16.
Prince, M., Patel, V., Saxena, S., Mak, M., Maselko, J.,Phillips, M.R., & Rahman, A. (2007). No health without mentalhealth. Lancet, 370(9590), 859-77.
Public Health Agency of Canada. (2008). The Chief PublicHealth Officer’s report on the state of public health inCanada, 2008. Ottawa, ON: Government of Canada.
Public Health Agency of Canada & Canadian Institute ofHealth Information. (2011). Obesity in Canada, Retrieved fromhttp://www.phac-aspc.gc.ca/hp-ps/hl-mvs/oic-oac/assets/pdf/oic-oac-eng.pdf
Public Health Agency of Canada. (2012). Chronic Disease Infobase Data Cubes. Retrieved from http://66.240.150.17/cubes/data-cubes-eng.html
Ravaghi, V., Quiñonez, C., & Allison, P.J. (2013). The magnitude of oral health inequalities in Canada: findings ofthe Canadian health measures survey. Community Dentistryand Oral Epidemiology. doi: 10.1111/cdoe.12043.
Region of Peel. (2008). A Picture of Health: A ComprehensiveReport on Health in Peel. Retrieved from http://www.peelregion.ca/health/health-status-report/chsr/pdfs/entire-report.pdf
Region of Peel. (2011). Health in Peel: Determinants and Disparities. Brampton, ON: Region of Peel. Retrieved fromhttps://www.peelregion.ca/health/health-status-report/determinants/pdf/MOH-0036_Determinants_final.pdf

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
References85
Reproductive Care Program of Nova Scotia. (2012). NovaScotia ATLEE Perinatal Database. Halifax, NS: ReproductiveCare Program of Nova Scotia.
Risk Analytica. (2011). The Life and Economic Impact ofMajor Mental Illness in Canada. Retrieved fromhttps://www.google.ca/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CDgQFjAA&url=http%3A%2F%2Fwww.mentalhealthcommission.ca%2FEnglish%2Fsystem%2Ffiles%2Fprivate%2Fdocument%2FMHCC_Report_Base_Case_FINAL_ENG_0.pdf&ei=wyBlUpC5Mvaw4AOwzoG4Bg&usg=AFQjC-NHR1_CZL3usErIU0oAfSwe94iefWg&sig2=yaLazbDydYFo-ZALnGTdwA&bvm=bv.54934254,d.dmg
Rissanen, T., Viinamäki, H., Honkalampi, K., Lehto, S. M., Hintikka, J., Saharinen, T., & Koivumaa-Honkanen, H. (2011).Long term life dissatisfaction and subsequent major depressive disorder and poor mental health. BMC Psychiatry,11(140). doi:10.1186/1471-244X-11-140
Roberts, R.E., Deleger, S., Strawbridge, W.J., & Kaplan, G.A.(2003). Prospective association between obesity and depression: evidence from the Alameda County Study. International Journal of Obesity and Related Metabolic Disorders 27(4), 514-21.
Robitaille, E., Bergeron, P., & Lasnier, B. (2010). Geographicalanalysis of the accessibility of fast-food restaurants and convenience stores around public schools in Québec.Québec, PQ: Institut National de Santé Publique du Québec.
Romans, S., Cohen, M., & Forte, T. (2011). Rates of depressionand anxiety in urban and rural Canada. Social Psychiatry andPsychiatric Epidemiology, 46(7), 567–75. doi:10.1007/s00127-010-0222-2
Saelens, B.E., Sallis, J.F., Frank, L.D. (2003). Environmentalcorrelates of walking and cycling: Findings from the Transportation, Urban Design and Planning Literatures. Annals of Behavioural Medicine, 25(2): 80-91.
Sallis, J.F., Floyd, M.F>, Rodriguez, D.A., & Saelens, B.E.(2012). Role of built environments in physical activity, obesity,and cardiovascular disease. Circulation, 125: 729-37. doi:10.1161/CIRCULATIONAHA.110.969022
Satyanarayana, S., Enns, M. W., Cox, B. J., & Sareen, J.(2009). Prevalence and correlates of chronic depression inthe canadian community health survey: mental health andwell-being. Canadian Journal of Psychiatry, 54(6), 389–98.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19527559
Schellenberg, G. (2004). General Social Survey on Social En-gagement, Cycle 17: An Overview of Findings (Catalogue no.89-598-XIE). Ottawa, ON: Statistics Canada.
Schmitz, N., Lesage, A., & Wang, J. (2009). Should psychological distress screening in the community accountfor self-perceived health status? Canadian Journal of Psychiatry, 54(8), 526–33. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19726005
Shields, M., Gorber, S. C., & Tremblay, M. S. (2008). Estimates of obesity based on self-report versus direct measures. Health Reports/Statistics Canada, Canadian Centre for Health Information, 19(2), 61-76.
Slater, J., Green, C., Sevenhuysen, G., O’Neil, J., & Edginton,B. (2009). Socio-demographic and geographic analysis ofoverweight and obesity in Canadian adults using the Canadian Community Health Survey (2005). Chronic Diseasesin Canada, 30(1), 4–15. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/20031083
Stafford, M., Chandola, T., & Marmot, M. (2007). Associationbetween fear of crime and mental health and physical functioning. American journal of public health, 97(11), 2076–81. doi:10.2105/AJPH.2006.097154
Stafford, M., & Marmot, M. (2003). Neighbourhood deprivation and health: does it affect us all equally? International Journal of Epidemiology, 32(3), 357-66.
Statistics Canada. (2007). East Hants, Nova Scotia, 2006Community Profiles. (Statistics Canada Catalogue no. 92-591-XWE). Ottawa, ON: Statistics Canada.
Statistics Canada. (2008). Health Indicators (StatisticsCanada Catalogue no. 82-221-XIE). Ottawa, ON: StatisticsCanada.
Statistics Canada (2010a). Birth-related indicators, by sex,three-year average, Canada, provinces, territories, censusmetropolitan areas and metropolitan influence zones(CANSIM Table no.: 102-4304) [Data file]. Retrieved fromhttp://www5.statcan.gc.ca/cansim/a26?Lang=eng&retr-Lang=eng&id=1024304&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada (2010b). Birth-related indicators, by sex,three-year average, Canada, provinces, territories, health regions and peer groups (CANSIM Table no.: 102-4303)[Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1024303&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada (2010c). Infant and perinatal mortality, bysex, three-year average, Canada, provinces, territories,health regions and peer groups (CANSIM Table no.: 102-4305) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1024305&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
References86
Statistics Canada. (2011a). Census indicator profile, Canada,provinces, territories, health regions and peer groups (CANSIM Table no.:109-0300) [Data file]. Retrieved fromhttp://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1090300&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada. (2011b). Mortality and potential years oflife lost, by selected causes of death and sex, three-year average, Canada, provinces, territories, health regions andpeer groups (CANSIM table no.: 102-4309) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1024309&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada. (2012a). Cancer incidence, by selectedsites of cancer and sex, three-year average, Canada,provinces, territories and health regions (CANSIM Table no.:103-0404) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=1030404&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada (2012b). Canada’s rural population since1851: Population and dwelling counts, 2011 Census. Retrieved from http://www5.statcan.gc.ca/access_acces/alternative_alternatif.action?t=98-310-XWE2011003&k=61&l =eng&loc=http://www12.statcan.gc.ca/census-recensement/2011/as-sa/98-310-x/98-310-x2011003_2-eng.pdf
Statistics Canada. (2012c). Census dictionary (StatisticsCanada Catalogue no. 98-301-XWE). Ottawa, ON: StatisticsCanada.
Statistics Canada. (2012d). Estimates of population, by agegroup and sex for July 1, Canada, provinces and territories(CANSIM Table no.: 051-0001) [Data file]. Retrieved fromhttp://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=0510001&paSer=&pattern=&stByVal=1&p1=1&p2=37&tabMode=dataTable&csid=
Statistics Canada. (2012e). Health-adjusted life expectancy,at birth and at age 65, by sex and income, Canada andprovinces (CANSIM Table no.: 102-0122) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=1020122&paSer=&pattern=&stByVal=1&p1=1&p2=37&tabMode=dataTable&csid=
Statistics Canada. (2012f). Life expectancy, at birth and atage 65, by sex, three-year average, Canada, provinces, territories, health regions and peer group (CANSIM Table no.:102-4307) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1024307&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada. (2012g). Potential years of life lost, by selected causes of death (ICD-10) and sex, population aged0 to 74, Canada, provinces and territories (CANSIM Tableno.: 102-0110) [Data file]. Retrieved from http://www5.statcan. gc.ca/ cansim/a26?lang=eng&retrLang=eng&id=1020110&paSer=&pattern=&stByVal=1&p1=1&p2=31&tabMode=dataTable&csid=
Statistics Canada. (2012h). The Daily: Canada’s populationestimates: Age and sex, July 1, 2012. Retrieved fromhttp://www.statcan.gc.ca/daily-quotidien/120927/dq120927b-eng.htm
Statistics Canada. (2013a). 2006 census of the population.Retrieved from http://www12.statcan.gc.ca/census-recensement/2006/index-eng.cfm
Statistics Canada. (2013b). 2011 census of the population.Retrieved from http://www12.statcan.gc.ca/census-recensement/index-eng.cfm
Statistics Canada (2013c). Canadians in context – Perceptionsand life satisfaction. Retrieved from http://www4.hrsdc.gc.ca/[email protected]?iid=39#M_4
Statistics Canada. (2013d). Crude birth rate, age-specific andtotal fertility rates (live births), Canada, provinces and territories (CANSIM Table no.: 102-4505) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a05?lang=eng&id=1024505
Statistics Canada. (2013e). Definitions, data sources andmethods: Variables and definitions. Retrieved fromhttp://www.statcan.gc.ca/concepts/definitions/index-eng.htm
Statistics Canada. (2013f). Dependency ratio, by age groupfor July 1st, Canada, provinces, territories, health regionsand peer groups (CANSIM Table no.: 109-5326) [Data file].Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1095326&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada. (2013g). Health indicator profile, annualestimates, by age group and sex, Canada, provinces, territories, health regions and peer groups (CANSIM Tableno.: 105-0501) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=1050501&paSer=&pattern=&stByVal=1&p1=1&p2=31&tabMode=dataTable&csid=
Statistics Canada (2013h). Health indicator profile, two-yearperiod estimates, by age group and sex, Canada, provinces,territories, census metropolitan areas and influence zones(CANSIM Table no.: 105-0592) [Data file]. Retrieved fromhttp://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=1050592&paSer=&pattern=&stByVal=1&p1=1&p2=31&tabMode=dataTable&csid=

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
References87
Statistics Canada. (2013i). Health indicator profile, two yearperiod estimates, by age group and sex, Canada, provinces,territories, health regions and peer groups (CANSIM Tableno.: 105-0502) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?Lang=eng&retrLang=eng&id=1050502&paSer=&pattern=&stByVal=1&p1=1&p2=-1&tabMode=dataTable&csid=
Statistics Canada. (2013j). Health profile (Statistics CanadaCatalogue no. 82-228-XWE). Ottawa, ON: Statistics Canada.
Statistics Canada. (2013k). Overweight and obese adults(self-reported), 2012. Retrieved fromhttp://www.statcan.gc.ca/pub/82-625-x/2013001/article/11840-eng.htm
Statistics Canada. (2013l). Unemployment rate, Canada,provinces, health regions and peer groups (CANSIM Tableno.: 109-5324) [Data file]. Retrieved from http://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=1095324&pattern=109-5324..109-5326&tabMode=dataTable&srchLan=-1&p1=-1&p2=31
Stockwell, T., Zhao, J., Macdonald, S., Vallance, K., Gruenewald, P., Ponicki, W…Treno, A. (2011). Impact of alcohol-related mortality of a rapid rise in the density of private liquor outlets in British Columbia: a local area multi-level analysis. Addiction, 106(4), 768-76.
Task Force on Community Preventive Services. (2009). Preventing Excessive Alcohol Consumption. Retrieved fromhttp://www.thecommunityguide.org/alcohol/index.html
Terashima, M. (2011). Geographical Epidemiology of Healthand Deprivation: a Population-Based, Spatio-Temporal Analysis of Health and Social Inequality in Nova Scotia,Canada. (Doctoral Dissertation). Retrieved from DalhousieRepository. http://hdl.handle.net/10222/13496
Teychenne, M., Ball, K., & Salmon, J. (2008). Physical activityand likelihood of depression in adults: A review. Abstract retrieved from http://www.ncbi.nlm.nih.gov/pubmed/18289655?dopt=Abstract&holding=f1000,f1000m,isisrc.Doi: 10.1016/j.ypmed.2008.01.009
The National Advisory Committee on SARS and Public Health.Learning from SARS: renewal of Public Health in Canada. Ottawa: Health Canada; 2003.
Toronto Public Health (2012). Road to health: Improving walk-ing and cycling in Toronto. Retrieved from http://www.google.ca/ url? sa=t&rct=j&q=&esrc=s&frm=1&source=web&cd=1&ved=0CCkQFjAA&url=http%3A%2F%2Fwww.toronto.ca%2Fhealth%2Fhphe%2Fpdf%2Froadtohealth.pdf&ei=HjWeUo_FCIGNtAaFqYGgAQ&usg=AFQjCNF-OTquORS56JqroLZ2QuhMJUzp_g&sig2=bvJdFPms2yyW3YyYmF4-YA&bvm=bv.57155469,d.Yms
Turcotte, M. (2008). The city/suburb contrast: How can wemeasure it? Retrieved from http://www.statcan.gc.ca/pub/11-008-x/2008001/article/10459-eng.htm#15.
University of Victoria. (2012). ASHG201: Spatial Epidemiology,Lecture 1. Retrieved from https://www.uvcs.uvic.ca/aspnet/Profile/Courses/
Van Berkel, J., Proper, K.I., van Dam, A., Boot, C.R.L.,Bongers, P.M., & van der Beek, A.J. (2013). An exploratorystudy of associations of physical activity with mental healthand work engagement. Retrieved from http://www.biomedcentral.com/1471-2458/13/558. doi: 10.1186/1471-2458-13-558.
Vanasse, A., Courteau, J., Lesage, A., Fleury, M.J., Gregoire,J.P., Moisan, J. Bergeron, C. (2012). Health inequities inmood disorders based on material and social deprivaiton indwelling sectors. Canadian Journal of Psychiatry, 57(12):772-81.
Vioque, J., Weinbrenner, T., Castello, A., Asensio, L., & Garciade la Hera, M. (2008). Intake of fruits and vegetables in relation to 10-year weight gain among Spanish adults. Obesity, 16(3): 664-70.
Wang, F. Orpana, H.M., Morrison, H., de Groh, M., Dai, S., &Luo, W. (2012). Long-term association between leisure-timephysical activity and changes in happiness: Analysis of theprospective National Population Health Survey. Abstract retrieved from http://aje.oxfordjournals.org/content/176/12/1095.abstract. doi: 10.1093/aje/kws199
Warburton, D.E., Charlesworth, S., Ivey, A., Nettlefold, L., &Bredin, S.S. (2010), A systematic review of the evidence forCanada’s Physical Activity Guidelines for Adults. The International Journal of Behavioral Nutrition and Physical Activity, 7(39). doi:10.1186/1479-5868-7-39.
Williams, A. & Kitchen, P. (2012). Sense of Place and Healthin Hamilton, Ontario: A Case Study. Social Indicators Research, 108(2), 257-76.
World Health Organization. (2011a). Indicator and measure-ment registry (version 1.7.0). Retrieved from http://apps.who.int/gho/ indicatorregistry/App_Main/view_indicator.aspx?iid=1
World Health Organization. (2011b), Mental health: a state ofwell-being. Retrieved from http://www.who.int/features/factfiles/mental_health/en.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T88

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendices89
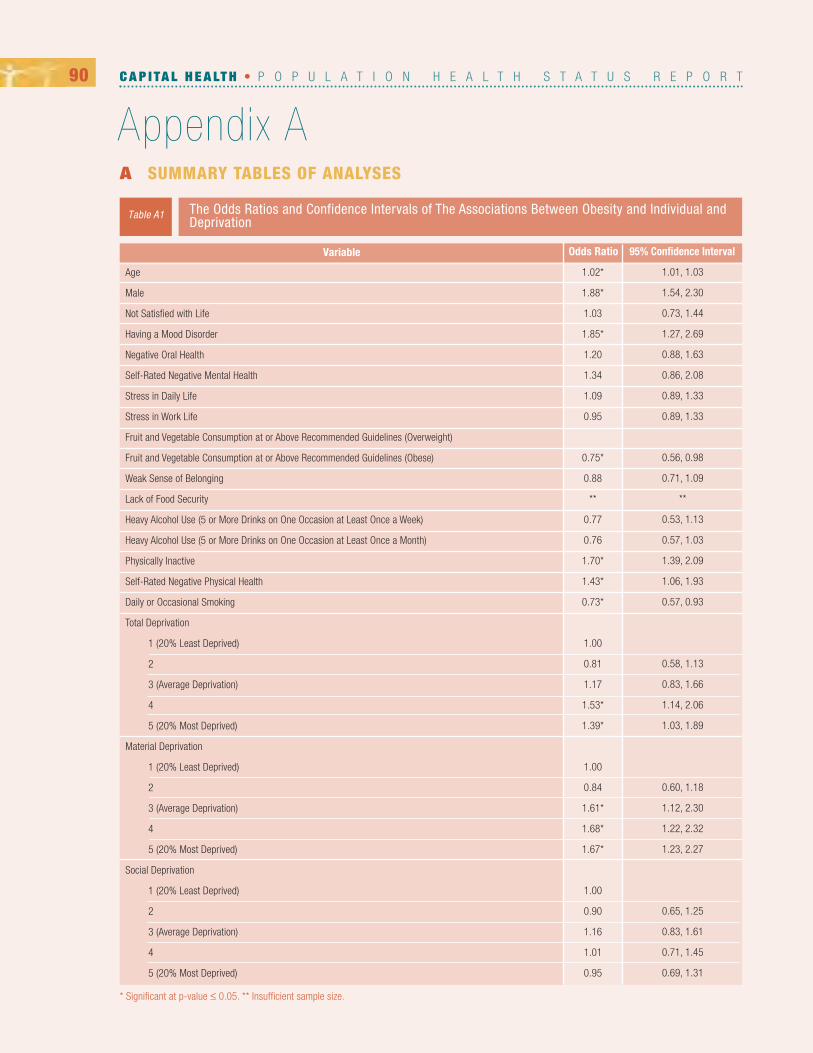
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix A90
The Odds Ratios and Confidence Intervals of The Associations Between Obesity and Individual andDeprivation
Table A1
Variable
Age
Male
Not Satisfied with Life
Having a Mood Disorder
Negative Oral Health
Self-Rated Negative Mental Health
Stress in Daily Life
Stress in Work Life
Fruit and Vegetable Consumption at or Above Recommended Guidelines (Overweight)
Fruit and Vegetable Consumption at or Above Recommended Guidelines (Obese)
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Week)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Physically Inactive
Self-Rated Negative Physical Health
Daily or Occasional Smoking
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
1.02*
1.88*
1.03
1.85*
1.20
1.34
1.09
0.95
0.75*
0.88
**
0.77
0.76
1.70*
1.43*
0.73*
1.00
0.81
1.17
1.53*
1.39*
1.00
0.84
1.61*
1.68*
1.67*
1.00
0.90
1.16
1.01
0.95
1.01, 1.03
1.54, 2.30
0.73, 1.44
1.27, 2.69
0.88, 1.63
0.86, 2.08
0.89, 1.33
0.89, 1.33
0.56, 0.98
0.71, 1.09
**
0.53, 1.13
0.57, 1.03
1.39, 2.09
1.06, 1.93
0.57, 0.93
0.58, 1.13
0.83, 1.66
1.14, 2.06
1.03, 1.89
0.60, 1.18
1.12, 2.30
1.22, 2.32
1.23, 2.27
0.65, 1.25
0.83, 1.61
0.71, 1.45
0.69, 1.31
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.
A SUMMARY TABLES OF ANALYSES

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix A91
The Odds Ratios and Confidence Intervals of the Associations Between Heavy Drinking and Individual Variables and Deprivation
Table A2
Variable
Age
Male
Not Satisfied with Life
Having a Mood Disorder
Negative Oral Health
Self-Rated Negative Mental Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight
BMI of Obese
Weak Sense of Belonging
Lack of Food Security
Physically Inactive
Self-Rated Negative Physical Health
Daily or Occasional Smoking
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
0.99
2.57*
1.82*
0.89
1.31
1.78
0.87
0.72
0.82
0.67*
0.87
**
0.93
1.42
2.91*
1.00
1.39
1.61
1.55*
1.68*
1.00
1.84*
1.31
1.11
1.89*
1.00
1.13
0.83
1.28
1.36
0.98, 1.00
1.91, 3.45
1.14, 2.90
0.54, 1.45
0.84, 2.04
0.98, 3.25
0.65, 1.17
0.51, 1.01
0.59, 1.14
0.46, 0.99
0.65, 1.17
**
0.70, 1.23
0.86, 2.34
2.10, 4.03
0.89, 2.19
0.98, 2.62
1.03, 2.35
1.09, 2.59
1.14, 2.96
0.81, 2.09
0.70, 1.75
1.23, 2.90
0.77, 1.64
0.55, 1.23
0.85, 1.92
0.94, 1.97
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix A92
The Odds Ratios and Confidence Intervals for the Associations Between Self-Rated Negative MentalHealth and Individual Variables and Deprivation
Table A3
Variable
Age
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight
BMI of Obese
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Week)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Self-Rated Negative Physical Health
Physical Inactivity
Neither or Not Satisfied with Life
Have a Mood Disorder
Daily or Occasional Smoking
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
1.00
1.00
3.71*
2.38*
1.56
0.99
1.87*
2.14*
**
1.58
1.78
7.48*
1.85*
15.73*
13.45*
3.48*
1.00
1.24
1.25
1.27
0.99
1.00
0.81
0.82
0.73
0.78
1.00
1.78
1.22
1.44
1.26
0.99, 1.01
0.68, 1.47
2.41, 5.72
1.48, 3.83
0.84, 2.92
0.59, 1.65
1.14, 3.08
1.44, 3.16
**
0.80, 3.13
0.98, 3.25
5.00, 11.19
1.25, 2.74
10.33, 23.98
8.87, 20.39
2.34, 5.18
0.63, 2.41
0.62, 2.51
0.70, 2.31
0.52, 1.87
0.42, 1.57
0.42, 1.60
0.39, 1.35
0.44, 1.38
0.91, 3.47
0.60, 2.48
0.68, 3.03
0.63, 2.53
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix A93
The Odds Ratios and Confidence Intervals for the Associations Between Having a Mood Disorderand Individual Variables and Deprivation
Table A4
Variable
Age
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight
BMI of Obese
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Week)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Self-Rated Negative Physical Health
Daily or Occasional Smoking
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
0.99*
1.72*
2.56*
2.52*
1.19
1.27
2.79*
2.00*
**
0.84
0.89
0.76
3.27*
2.40*
1.00
1.03
1.06
0.74
0.98
1.00
0.88
1.01
0.73
0.87
1.00
0.74
0.70
0.83
0.80
0.98, 0.99
1.26, 2.35
1.76, 3.72
1.73, 3.65
0.77, 1.82
0.83, 1.96
1.84, 4.22
1.47, 2.74
**
0.42, 1.66
0.54, 1.45
0.57, 1.03
2.31, 4.64
1.73, 3.33
0.62, 1.70
0.62, 1.79
0.46, 1.18
0.62, 1.55
0.52, 1.50
0.60, 1.70
0.44, 1.21
0.55, 1.38
0.46, 1.19
0.43, 1.15
0.49, 1.40
0.50, 1.28
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.
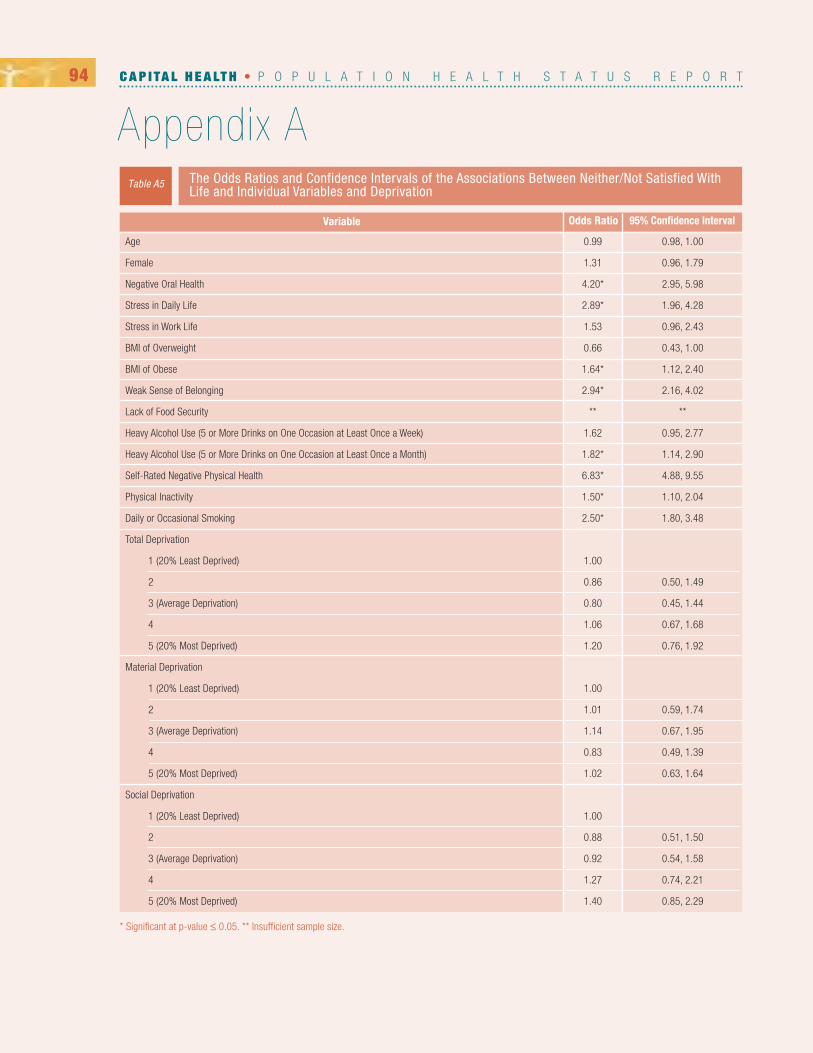
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix A94
The Odds Ratios and Confidence Intervals of the Associations Between Neither/Not Satisfied WithLife and Individual Variables and Deprivation
Table A5
Variable
Age
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight
BMI of Obese
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Week)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Self-Rated Negative Physical Health
Physical Inactivity
Daily or Occasional Smoking
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
0.99
1.31
4.20*
2.89*
1.53
0.66
1.64*
2.94*
**
1.62
1.82*
6.83*
1.50*
2.50*
1.00
0.86
0.80
1.06
1.20
1.00
1.01
1.14
0.83
1.02
1.00
0.88
0.92
1.27
1.40
0.98, 1.00
0.96, 1.79
2.95, 5.98
1.96, 4.28
0.96, 2.43
0.43, 1.00
1.12, 2.40
2.16, 4.02
**
0.95, 2.77
1.14, 2.90
4.88, 9.55
1.10, 2.04
1.80, 3.48
0.50, 1.49
0.45, 1.44
0.67, 1.68
0.76, 1.92
0.59, 1.74
0.67, 1.95
0.49, 1.39
0.63, 1.64
0.51, 1.50
0.54, 1.58
0.74, 2.21
0.85, 2.29
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix A95
The Odds Ratios and Confidence Intervals for the Associations Between Self-Rated Negative MentalHealth and Individual Variables and Deprivation
Table A6
Variable
Age
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight
BMI of Obese
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Week)
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Self-Rated Negative Physical Health
Physical Inactivity
Daily or Occasional Smoking
Being Neither or Unsatisfied with Life
Having a Mood Disorder
Total Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Material Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
Social Deprivation
1 (20% Least Deprived)
2
3 (Average Deprivation)
4
5 (20% Most Deprived)
1.00
1.00
3.71*
2.38*
1.56
0.99
1.87*
2.14*
**1.58
1.78
7.48*
1.85*
3.48*
15.71
13.42
1.00
1.24
1.25
1.27
0.99
1.00
0.81
0.82
0.73
0.78
1.00
1.78
1.22
1.44
1.26
0.99, 1.01
0.68, 1.47
2.41, 5.72
1.48, 3.83
0.84, 2.92
0.59, 1.65
1.14, 3.08
1.44, 3.16
**
0.80, 3.13
0.98, 3.25
5.00, 11.19
1.25, 2.74
2.34, 5.18
10.32, 23.96
8.93, 20.37
0.63, 2.41
0.62, 2.51
0.70, 2.31
0.52, 1.87
0.42, 1.57
0.42, 1.60
0.39, 1.35
0.44, 1.38
0.91, 3.47
0.60, 2.48
0.68, 3.03
0.63, 2.53
95% Confidence IntervalOdds Ratio
* Significant at p-value ≤ 0.05. ** Insufficient sample size.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix A96
The Odds Ratios and Confidence Intervals of the Associations Between Total Deprivation andIndividual Variables
Table A7
Variable
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight (Reference Category Normal/Underweight)
BMI of Obese (Reference Category Normal/Underweight)
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Fruit and Vegetable Consumption Below the Recommended Guidelines
Self-Rated Negative Mental Health
Having a Mood Disorder
Not Satisfied with Life
Self-Rated Negative Physical Health
Physically Inactive
Daily or Occasional Smoking
1(20% LeastDeprived) 2 3 (Average
Deprivation) 4 5 (20% Most Deprived)
* Significant at p-value ≤ 0.05. ** Insufficient sample size.
0.99 (0.75, 1.31)
2.17* (1.36, 3.45)
0.97 (0.73, 1.30)
1.07 (0.74, 1.55)
1.00
1.00
0.98 (0.72, 1.34)
**
1.68* (1.09, 2.59)
1.37* (1.02, 184)
0.99 (0.52, 1.87)
0.98 (0.62, 1.55)
1.20 (0.76, 1.92)
2.36* (1.50, 3.69)
1.18 (0.89, 1.57)
1.63* (1.13, 2.33)
0.95 (0.72, 1.25)
1.88* (1.18, 2.98)
1.06 (0.80, 1.41)
0.95 (0.67, 1.35)
1.18 (0.86, 1.61)
1.01 (0.72, 1.41)
0.98 (0.72, 1.32)
**
1.55* (1.03, 2.35)
0.97 (0.73, 1.29)
1.27 (0.70, 2.31)
0.74 (0.46, 1.18)
1.06 (0.67, 1.68)
1.84 (1.17, 2.89)
0.97 (0.74, 1.28)
1.42 (0.99, 2.03)
1.03 (0.75, 1.43)
1.27 (0.72, 2.23)
0.83 (0.59, 1.15)
1.28 (0.83, 1.96)
0.91 (0.62, 1.33)
0.76 (0.50, 1.15)
1.06 (0.75, 1.51)
**
1.61(0.98, 2.66)
1.25 (0.88, 1.76)
1.25 (0.62, 2.51)
1.06 (0.62, 1.79)
0.80 (0.45, 1.44)
1.79 (1.06, 3.01)
0.84 (0.60, 1.16)
1.25 (0.82, 1.92)
1.12 (0.82, 1.52)
1.13 (0.65, 1.97)
1.16 (0.84, 1.60)
1.10 (0.74, 1.64)
0.71 (0.50, 1.02)
0.42* (0.28, 0.64)
1.03 (0.74, 1.45)
**
1.39 (0.89, 2.19)
1.15 (0.83, 1.59)
1.24 (0.63, 2.41)
1.03 (0.62, 1.70)
0.86 (0.50, 1.49)
1.09 (0.64, 1.88)
0.85 (0.62, 1.17)
1.15 (0.76, 1.74)
1.00
1.00
1.00
1.00
0.80 (0.57, 1.12)
0.62* (0.43, 0.91)
1.00
**
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
Total Deprivation Category

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix A97
The Odds Ratios and Confidence Intervals of the Associations Between Material Deprivation and Individual Variables
Table A8
Variable
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight (Reference Category Normal/Underweight)
BMI of Obese (Reference Category Normal/Underweight)
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Fruit and Vegetable Consumption Below the Recommended Guidelines
Self-Rated Negative Mental Health
Having a Mood Disorder
Not Satisfied with Life
Self-Rated Negative Physical Health
Physically Inactive
Daily or Occasional Smoking
1(20% LeastDeprived) 2 3 (Average
Deprivation) 4 5 (20% Most Deprived)
* Significant at p-value ≤ 0.05. ** Insufficient sample size.
0.92 (0.69, 1.22)
2.17* (1.32, 3.56)
0.94 (0.70, 1.26)
0.85 (0.58, 1.25)
1.00
1.00
1.00 (0.73, 1.38)
**
1.89* (1.23, 2.90)
1.31 (0.98, 1.76)
0.78 (0.44, 1.38)
0.87 (0.55, 1.38)
1.02 (0.63, 1.64)
1.83* (1.19, 2.81)
1.18 (0.89, 1.57)
1.72* (1.19, 2.48)
1.06 (0.79, 1.43)
2.03* (1.21, 3.41)
0.91 (0.67, 1.24)
0.67* (0.45, 0.99)
1.00 (0.73, 1.37)
1.01 (0.72, 1.42)
1.44* (1.04, 2.00)
**
1.11 (0.70, 1.75)
1.21 (0.89, 1.65)
0.73 (0.39, 1.35)
0.73 (0.44, 1.21)
0.83 (0.49, 1.39)
1.42 (0.90, 2.25)
1.09 (0.80, 1.47)
1.17 (0.78, 1.74)
0.91 (0.66, 1.26)
1.46 (0.82, 2.61)
0.94 (0.67, 1.32)
0.86 (0.55, 1.33)
0.95 (0.67, 1.36)
0.97 (0.66, 1.43)
1.35 (0.94, 1.93)
**
1.31 (0.81, 2.09)
1.17 (0.83, 1.64)
0.82 (0.42, 1.60)
1.01 (0.60, 1.70)
1.14 (0.67, 1.95)
0.93 (0.54, 1.60)
0.93 (0.67, 1.30)
1.43 (0.94, 2.19)
1.37 (0.99, 1.89)
1.59 (0.90, 2.79)
1.03 (0.74, 1.44)
0.77 (0.50, 1.18)
0.51* (0.36, 0.71)
0.49* (0.34, 0.72)
1.32 (0.93, 1.88)
**
1.84* (1.14, 2.96)
1.20 (0.93, 1.82)
0.81 (0.42, 1.57)
0.88 (0.52, 1.50)
1.01 (0.59, 1.74)
0.95 (0.56, 1.62)
0.95 (0.69, 1.32)
1.22 (0.80, 1.87)
1.00
1.00
1.00
1.00
0.70* (0.50, 0.98)
0.45* (0.30, 0.68)
1.00
**
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
Material Deprivation
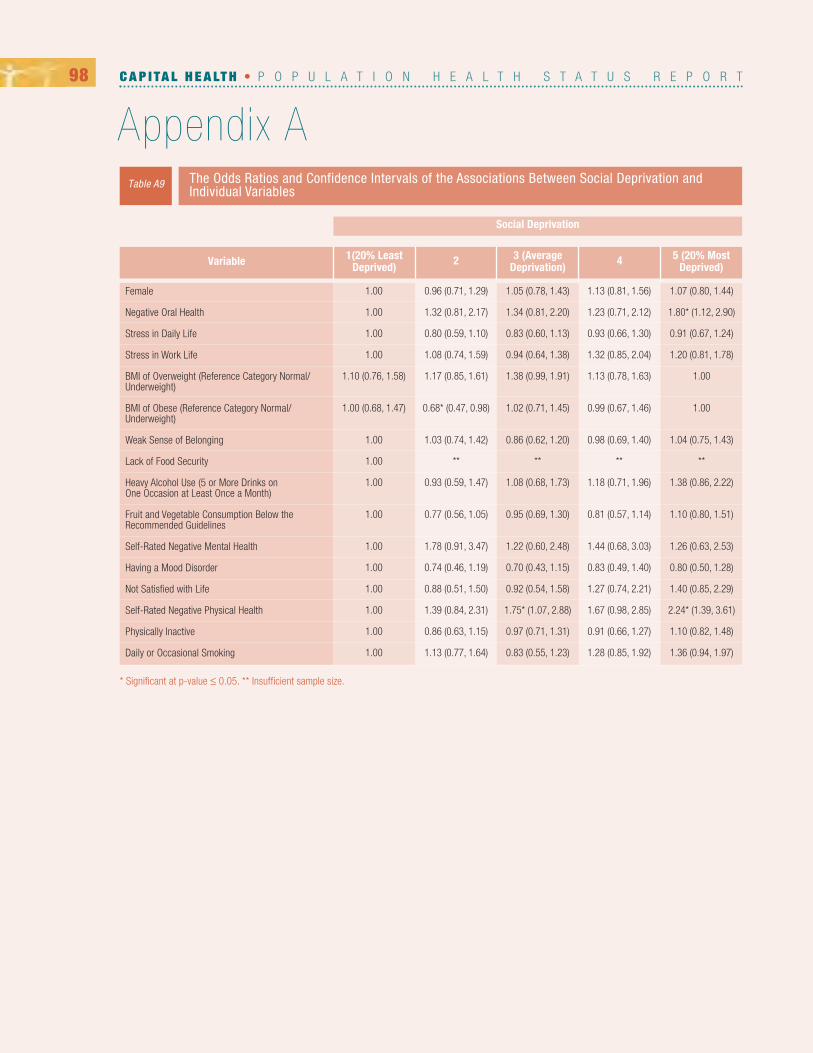
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix A98
The Odds Ratios and Confidence Intervals of the Associations Between Social Deprivation and Individual Variables
Table A9
Variable
Female
Negative Oral Health
Stress in Daily Life
Stress in Work Life
BMI of Overweight (Reference Category Normal/Underweight)
BMI of Obese (Reference Category Normal/Underweight)
Weak Sense of Belonging
Lack of Food Security
Heavy Alcohol Use (5 or More Drinks on One Occasion at Least Once a Month)
Fruit and Vegetable Consumption Below the Recommended Guidelines
Self-Rated Negative Mental Health
Having a Mood Disorder
Not Satisfied with Life
Self-Rated Negative Physical Health
Physically Inactive
Daily or Occasional Smoking
1(20% LeastDeprived) 2 3 (Average
Deprivation) 4 5 (20% Most Deprived)
* Significant at p-value ≤ 0.05. ** Insufficient sample size.
1.07 (0.80, 1.44)
1.80* (1.12, 2.90)
0.91 (0.67, 1.24)
1.20 (0.81, 1.78)
1.00
1.00
1.04 (0.75, 1.43)
**
1.38 (0.86, 2.22)
1.10 (0.80, 1.51)
1.26 (0.63, 2.53)
0.80 (0.50, 1.28)
1.40 (0.85, 2.29)
2.24* (1.39, 3.61)
1.10 (0.82, 1.48)
1.36 (0.94, 1.97)
1.13 (0.81, 1.56)
1.23 (0.71, 2.12)
0.93 (0.66, 1.30)
1.32 (0.85, 2.04)
1.13 (0.78, 1.63)
0.99 (0.67, 1.46)
0.98 (0.69, 1.40)
**
1.18 (0.71, 1.96)
0.81 (0.57, 1.14)
1.44 (0.68, 3.03)
0.83 (0.49, 1.40)
1.27 (0.74, 2.21)
1.67 (0.98, 2.85)
0.91 (0.66, 1.27)
1.28 (0.85, 1.92)
1.05 (0.78, 1.43)
1.34 (0.81, 2.20)
0.83 (0.60, 1.13)
0.94 (0.64, 1.38)
1.38 (0.99, 1.91)
1.02 (0.71, 1.45)
0.86 (0.62, 1.20)
**
1.08 (0.68, 1.73)
0.95 (0.69, 1.30)
1.22 (0.60, 2.48)
0.70 (0.43, 1.15)
0.92 (0.54, 1.58)
1.75* (1.07, 2.88)
0.97 (0.71, 1.31)
0.83 (0.55, 1.23)
0.96 (0.71, 1.29)
1.32 (0.81, 2.17)
0.80 (0.59, 1.10)
1.08 (0.74, 1.59)
1.17 (0.85, 1.61)
0.68* (0.47, 0.98)
1.03 (0.74, 1.42)
**
0.93 (0.59, 1.47)
0.77 (0.56, 1.05)
1.78 (0.91, 3.47)
0.74 (0.46, 1.19)
0.88 (0.51, 1.50)
1.39 (0.84, 2.31)
0.86 (0.63, 1.15)
1.13 (0.77, 1.64)
1.00
1.00
1.00
1.00
1.10 (0.76, 1.58)
1.00 (0.68, 1.47)
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
Social Deprivation

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix B99
B DEFINITIONS
30-day acute myocardial infarction (AMI) in-hospital mortality: The risk-adjusted rate of all-cause in-hospital death occurring within 30days of first admission to an acute care hospital with a diagnosis of acute myocardial infarction (AMI). Canada rate does not include Quebec.
30-day stroke in-hospital mortality: The risk-adjusted rate of all-cause in-hospital death occurring within 30 days of first admission to anacute care hospital with a diagnosis of stroke. Canada rate does not include Quebec.
Aboriginal: Aboriginal identity refers to whether the person reported identifying with the Aboriginal peoples of Canada. This includes those whoreported being an Aboriginal person, that is, First Nations (North American Indian), Métis or Inuit and/or those who reported Registered or TreatyIndian status, that is registered under the Indian Act of Canada, and/or those who reported membership in a First Nation or Indian band.
Aboriginal population: Aboriginal people living in a geographic area as a proportion of the total population.
Age-specific fertility rate: Number of live births per 1,000 females in a specific age group compared to the number females in the agegroup.
All cancers, deaths: Age-standardized rate of death per 100,000 population.
All other circulatory diseases, deaths: Age-standardized rate of death per 100,000 population.
All other respiratory diseases, deaths: Age-standardized rate of death per 100,000 population.
Ambulatory care sensitive conditions: Age-standardized acute care hospitalization rate for conditions where appropriate ambulatory careprevents or reduces the need for admission to hospital, per 100,000 population under age 75 years.
Arthritis: Population aged 15 and over who reported that they have been diagnosed by a health professional as having arthritis. Arthritis includes rheumatoid arthritis and osteoarthritis, but excludes fibromyalgia.
Asthma: Population aged 12 and over who reported that they have been diagnosed by a health professional as having asthma.
Bike helmet use: Population aged 12 and over who reported that they always wore a helmet when riding a bicycle in the last 12 months.
Body Mass Index (BMI): A number calculated from a person's weight and height and a fairly reliable indicator of body fatness for most people.
Bronchitis, emphysema and asthma, deaths: Age-standardized rate of death per 100,000 population.
Caesarean section: Proportion of women delivering babies in acute care hospitals by caesarean section.
Cancer incidence: Cancer incidence refers to new primary sites of malignant neoplasms.
Cardiac revascularization: Age-standardized rate of coronary artery bypass graft (CABG) surgery performed on inpatients in acute care hospitals or percutaneous coronary interventions (PCI) performed on patients in acute care hospitals, same day surgery facilities or catheterization laboratories, per 100,000 population age 20 years and over. Canada rate does not include Quebec.
Causality: Relating causes to the effects they produce. A cause is an event, condition, characteristic (or a combination) which plays an important role in the occurrence of an outcome.
Cerebrovascular diseases, deaths: Age-standardized rate of death per 100,000 population.
Children in low income families: Population of children aged 17 and under living in economic families with incomes below the low-incomecut-offs. An economic family refers to a group of two or more persons who live in the same dwelling and are related to each other by blood,marriage, common-law or adoption.
Chronic obstructive pulmonary disease (COPD): Population aged 35 and over who reported being diagnosed by a health professional withchronic bronchitis, emphysema or chronic obstructive pulmonary disease (COPD).
Circulatory diseases, deaths: Age-standardized rate of death per 100,000 population due to circulatory diseases including ischemic heartdisease, cerebrovascular disease and other circulatory diseases.
Community: A group of people living in the same locality with boundaries defined by Nova Scotia Community Counts.
Community Health Boards (CHBs): Active volunteer advisory board within Capital Health representing the people and neighbourhoods withinthe health board area.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix B100
Confidence Interval (CI): A range around a value that indicates how precise the value is. The 95% Confidence Interval indicates that 95% ofthe time the true value of the variable will be within the confidence interval. If the confidence interval does not include zero, then the result is statistically significant.
Contact with a medical doctor in the past 12 months: Population aged 12 and over who reported having consulted with a medical doctor inthe past 12 months. Medical doctor includes family or general practitioners as well as specialists such as surgeons, allergists, orthopedists, gynecologists or psychiatrists. For population aged 12 to 17 includes pediatricians.
Coronary artery bypass graft (CABG): Age-standardized rate of coronary artery bypass graft surgery performed on inpatients in acute care hospitals per 100,000 population age 20 and over.
Crude birth rate: Birth rate is the number of live births, of a given geographic area in a given year, per 1,000 mid-year total population of thesame geographic area in the same year.
Current smoker, daily or occasional: Population aged 12 and over who reported being a current smoker. Daily smokers refer to those who reported smoking cigarettes every day. Does not take into account the number of cigarettes smoked. Occasional smokers refer to those whoreported smoking cigarettes occasionally.
Dependency ratio: Dependency ratio is the number of youth (ages 0 to 19 years), number of seniors (age 65 years and above) or both (youthand seniors) relative to the total number of people aged 20 to 64 years in the population. It is usually presented as the number of dependentsfor every 100 people in the working age population.
Deprivation index: A relative scale from 1 (20% least deprived) to 5 (20% most deprived) for the indication of total, material and social deprivation.
Diabetes: Population aged 12 and over who reported that they have been diagnosed by a health professional as having diabetes. Diabetes includes females 15 and over who reported that they have been diagnosed with gestational diabetes.
Dissemination area: Determined by Statistics Canada, it is an area comprised one or more neighbouring blocks of house representing a population of 400 to 700 persons.
Doctors rate - General/family physicians rate: Total number of general practitioners and family physicians per 100,000 population. Physician counts include all active physicians in clinical and non-clinical practice as of December 31 of the reference year.
Doctors rate - Specialist physicians: Total number of specialist physicians per 100,000 population.
Employment population ratio (employment rate): Proportion of the population 15 years and older that is employed relative to the total population 15 years and older.
Exposure to second-hand smoke at home: Non-smoking population aged 12 and over who reported that at least one person smoked insidetheir home every day or almost every day. Smoking includes cigarettes, cigars and pipes.
Exposure to second-hand smoke in the past month, in vehicles and/or public places: Non-smoking population aged 12 and over who reported being exposed to second-hand smoke in private vehicles and/or public places on every day or almost every day in the past month.Smoking includes cigarettes, cigars and pipes.
Fertility rate: The average number of children that would be born per woman if all women lived to the end of their child-bearing years and hadchildren according to the age-specific fertility rates for that area and time period.
Food insecurity: The inability to acquire or consume an adequate diet quality or sufficient quantity of food in socially acceptable ways, or theuncertainty that one will be able to do so.
Fruit and vegetable consumption, 5 times or more per day: Indicates the usual number of times (frequency) per day a person reported eating fruits and vegetables. Measure does not take into account the amount consumed.
Functional health, good to full: Population aged 12 and over reporting measures of overall functional health, based on 8 dimensions of functioning (vision, hearing, speech, mobility, dexterity, feelings, cognition and pain).
Health adjusted life expectancy at birth (HALE): Health adjusted life expectancy (HALE) is the number of years in full health that an individual can expect to live given the current morbidity and mortality conditions.
Health disparities: Differences in health status among distinct segments of the population that may or may not be health inequities.
Health inequities: Differences in health status among groups that are considered unfair, unjust, or preventable as well as socially producedand systematic in their distribution across the population.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix B101
Heavy drinking: Population aged 12 and over who reported having 5 or more drinks on one occasion, at least once a month in the past year.Heavy drinking refers to having consumed five or more drinks, per occasion, at least once a month during the past year.
High blood pressure: Population aged 12 and over who reported that they have been diagnosed by a health professional as having high bloodpressure.
High school graduates aged 25 to 29: Population aged 25 to 29 who have a secondary (high) school graduation certificate or equivalent.'High school certificate or equivalent' refers to the possession of a secondary (high) school graduation certificate or its equivalent, regardless ofwhether other educational qualifications are held or not.
Hip replacement: Age-standardized rate of unilateral or bilateral hip replacement surgery performed on inpatients in acute care hospitals per100,000 population age 20 years and over.
Hospitalized acute myocardial infarction (AMI) event rate: Age-standardized rate of new AMI events admitted to an acute care hospital per100,000 population age 20 and older. New event is defined as a first-ever hospitalization for an AMI or a recurrent hospitalized AMI occurringmore than 28 days after the admission for the previous event in the reference period.
Hospitalized hip fracture event rate: Age-standardized rate of new hip fractures admitted to an acute care hospital per 100,000 populationage 65 years and over. New event is defined as a first-ever hospitalization for hip fracture or a subsequent hip fracture occurring more than 28days after the admission for the previous event in the reference period. A person may have more than one hip fracture event in the referenceperiod.
Hospitalized stroke event rate: Age-standardized rate of new stroke events admitted to an acute care hospital per 100,000 population age20 and older. New event is defined as a first-ever hospitalization for stroke or a recurrent hospitalized stroke occurring more than 28 days afterthe admission for the previous event in the reference period.
Hysterectomy: Age-standardized rate for hysterectomy provided to inpatients in acute care hospitals, per 100,000 women age 20 and over.Immigrant: For the 1991 to 2006 censuses, the term 'immigrants' refers to persons who are, or have ever been, landed immigrants in Canada.A landed immigrant is a person who has been granted the right to live in Canada permanently by immigration authorities.
Infant mortality: Infant mortality corresponds to the death of a child under one year of age expressed as a rate per 1,000 live births.Inflow/outflow ratio – Overall: A ratio of the number of discharges from relevant facilities (acute care/same day surgery) within a given regiondivided by the number of discharges generated by residents of that region.
Influenza immunization, less than one year ago: Population aged 12 and over who reported when they had their last influenza immunization(flu shot).
Injuries within the past 12 months causing limitation of normal activities: Population aged 12 and over who sustained injuries in the past12 months which are serious enough to limit normal activities. Repetitive strain injuries are not included. For those with more than one injury inthe past 12 months, refers to "the most serious injury", as identified by the respondent.
Injuries within the past 12 months, sought medical attention: Population aged 12 and over who sustained injuries in the past 12 monthsand who sought medical attention from a health professional in the 48 hours following the injury.
Injury hospitalization rate: Age-standardized rate of acute care hospitalization due to injury resulting from the transfer of energy (excludingpoisoning and other non-traumatic injuries), per 100,000 population.
Injury mortality: Unintentional injury mortality is the age-standardized rate of death per 100,000 population. Unintentional injuries are classified according to the World Health Organization, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) and can include external causes such as transport accidents, falls, poisoning, drowning and fire, but not complications ofmedical and surgical care.
Internal migrant: Number or proportion of people that lived in a different Canadian municipality one year before the current census (1-year internal migrants) or at the time of the previous census (5-year internal migrants).
Ischemic heart diseases, deaths: Age-standardized rate of death per 100,000 population.
Knee replacement: Age-standardized rate of unilateral or bilateral knee replacement surgery performed on patients in acute care hospitals orsame-day surgery facilities, per 100,000 population age 20 years and over.
Labour force: Consists of people aged 15 years and over that are currently employed and people who are unemployed but were available tostart work in the week prior to enumeration and looked for work in the past 4 weeks. The labour force excludes persons living on reserves andother Aboriginal settlements in the provinces, full-time members of the Canadian Armed Forces, and institutionalized populations.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix B102
Leisure-time physical activity, moderately active or active: Population aged 12 and over who reported a level of physical activity, based ontheir responses to questions about the nature, frequency and duration of their participation in leisure-time physical activity. Respondents areclassified as active, moderately active or inactive based on an index of average daily physical activity over the past 3 months. For each leisuretime physical activity engaged in by the respondent, average daily energy expenditure is calculated by multiplying the number of times the activity was performed by the average duration of the activity by the energy cost (kilocalories per kilogram of body weight per hour) of the activity. The index is calculated as the sum of the average daily energy expenditures of all activities. Respondents are classified as follows:
≥ 3.0 kcal/kg/day = physically active;1.5 to 2.9 kcal/kg/day = moderately active;< 1.5 kcal/kg/day = inactive.
Life expectancy at age 65: Life expectancy is the number of years a person would be expected to live, starting from birth (for life expectancyat birth) or at age 65 (for life expectancy at age 65), on the basis of the mortality statistics for a given observation period.
Life expectancy at birth: Life expectancy is the number of years a person would be expected to live, starting from birth, on the basis of themortality statistics for a given observation period. Life satisfaction (satisfied or neither/unsatisfied): Derived from the CCHS question: “Overall,how satisfied are you with your life in general?” and dichotomized into satisfied and neither/unsatisfied with life.
Life satisfaction, satisfied or very satisfied: Population aged 12 and over who reported being satisfied or very satisfied with their life in general.
Logistic regression: A statistical approach to model the relationship between a dependent variable and one or more independent variables.Logistic regression estimates the probability of an event occurring allowing the calculation of an odds ratio.
Lone-parent families: The percentage of lone-parent families among all census families. Census family refers to a married or common-law couple or lone parent with at least one never-married son or daughter living in the same household.
Long-term unemployed: The long term unemployed includes unemployed individuals who last worked in or before 2005. Long-term unemployment excludes institutional residents.
Low birth weight: Live births less than 2,500 grams, expressed as a percentage of all live births (birth weight known).
Low-income cut-offs (LICOs): Low-income cut-offs (LICOs) represent levels of income where people spend disproportionate amounts ofmoney for food, shelter and clothing. They are based on family and community size and are updated to account for changes in the consumerprice index. LICO data exclude institutional residents and were not derived for economic families or unattached individuals in the territories oron Indian reserves.
Low income rate: Population in economic families and unattached individuals with incomes below the low-income cut-off (LICO). An economicfamily refers to a group of two or more persons who live in the same dwelling and are related to each other by blood, marriage, common-law oradoption.
Material deprivation: A component of total deprivation, and for this population health status report, determined from three factors: 1) the proportion of persons without a high school degree; 2) the ratio of employment to population; and 3) average personal income.
Mean age: The average age of a defined population.
Median age: Median age is the age at which 50% of the population is older and 50% is younger.
Morbidity: Incidence of poor health and disease in a population.
Mortality: Mortality is the death rate, which can be measured as total mortality (all causes of death combined) or by selected cause of death.All counts and rates are calculated using the total population (all age groups).
Odds Ratio: The odds ratio has been used to determine whether a particular exposure is a risk factor for a particular outcome, and to comparethe magnitude of various risk factors for that outcome. If the odds ratio equals 1, the exposure does not affect the odds of the outcome. If theodds ratio is greater than 1, the exposure is associated with higher odds of outcome. If the odds ratio is less than 1, the exposure is associatedwith lower odds of the outcome (Szumilas, 2010).
Overweight or obese: A Body Mass Index greater than or equal to 25 kg/m2. Body mass index (BMI) is calculated by dividing the respondent'sbody weight (in kilograms) by their height (in metres) squared. The index is calculated for the population aged 18 and over, excluding pregnantfemales and persons less than 3 feet (0.914 metres) tall or greater than 6 feet 11 inches (2.108 metres).
Pain or discomfort, moderate or severe: Population aged 12 and over who reported that they usually have pain or discomfort.
Pain or discomfort that prevents activities: Population aged 12 and over who reported having pain or discomfort that prevents activities.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix B103
Participation and activity limitation, sometimes or often: Population aged 12 and over who reported being limited in selected activities(home, school, work and other activities) because of a physical condition, mental condition or health problem which has lasted or is expected tolast 6 months or longer.
Peer Group: A Peer Group is composed of health regions with similar characteristics, determined by Statistics Canada through the comparisonof 24 sociodemographic variables and geographic factors. CDHA is in Peer Group A which includes 34 other health districts throughoutCanada.
Perceived life stress: Population aged 15 and over who reported perceiving that most days in their life was quite a bit or extremely stressful.Perceived health, very good or excellent: Population aged 12 and over who reported perceiving their own health status as being either excellentor very good or fair or poor, depending on the indicator.
Perceived mental health, very good or excellent: Population aged 12 and over who reported perceiving their own mental health status asbeing excellent or very good or fair or poor, depending on the indicator.
Percutaneous coronary intervention: Age-standardized rate of percutaneous coronary interventions (PCI) performed on patients in acutecare hospitals, same day surgery facilities or catheterization laboratories, per 100,000 population age 20 years and over. Rates for Quebec arenot available due to differences in data collection. Canada rate does not include Quebec.
Place: Refers to the political, social, cultural and historical meanings attached to a location.
Pneumonia and influenza, deaths: Age-standardized rate of death per 100,000 population.
Population density: Population density is the number of persons per square kilometer. The calculation for population density is total populationdivided by land area.
Population living within a Metropolitan Influenced Zone: Strong Census Metropolitan Area and Census Agglomeration Influenced Zones(MIZ) indicate the proportion of the population living in Census Metropolitan Areas (CMA), Census Agglomerations (CA) and communities thatfall outside CMAs and/or CAs that have at least 30% of the employed labour force commuting to CMAs and/or CAs. Metropolitan influencedzone (MIZ) is a category assigned to a municipality not included in either a census metropolitan area (CMA) or a census agglomeration (CA). Amunicipality within a province is assigned to a census MIZ category depending on the percentage of its resident employed labour force thatcommute to work in the core of any CMA or CA.
Post-secondary graduates aged 25 to 54: Population aged 25 to 54 who have obtained a post-secondary certificate, diploma, or degree.'Highest certificate, diploma or degree' refers to the highest certificate, diploma or degree completed based on a hierarchy which is generallyrelated to the amount of time spent 'in-class'. Post-secondary graduates exclude institutional residents.
Potential years of life lost (PYLL): Potential years of life lost (PYLL) is the number of years of potential life not lived when a person dies “prematurely”, defined for this indicator as before age 75.
Productive portion: The portion of the population of working age, i.e. aged 15 to 64 years.
Regular medical doctor: Population aged 12 and over who reported that they have a regular medical doctor.
Respiratory diseases: Age-standardized rate of death per 100,000 population due to pneumonia, bronchitis and other respiratory diseases.
Rural: Rural areas are those with a population density of less than 400 persons per km2.
Self-rated mental health: Derived from the CCHS question: “In general, would you say your mental health is: excellent, very good, good, fairor poor?”, and dichotomized into positive (excellent, very good, or good mental health and negative (fair or poor) mental health. For the population health status report, the population was aged 15 and over.
Self-reported mood disorder: Derived from the question: “Do you have a mood disorder such as depression, bipolar disorder, mania or dysthymia? (Interviewer Note: Include manic depression)” and dichotomized into two categories, have a mood disorder and do not have a mooddisorder. For the population health status report, the population was aged 15 and over. For the peer ranking (Appendix D), the population wasaged 12 and over.
Sense of community belonging: Population aged 12 and over who reported their sense of belonging to their local community as being verystrong or somewhat strong. For the population health report, the population was aged 15 and over.
Sex: The biological and physiological characteristics that define men and women.
Smoking status: Daily and non-daily smokers (occasional smokers) defined as a smoker.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix B104
Social connectedness: Refers to the relationships people have with others and the benefits these relationships can bring to the individual aswell as to society. It includes relationships with family, friends, colleagues and neighbours, as well as connections people make through paidwork, sport and other leisure activities, or through voluntary work or community service.
Social deprivation: A component of total deprivation, and for this population health status report, determined by three factors: 1) the proportion of persons living alone; 2) the proportion of single-parent families; and 3) the proportion of persons who are widowed, separated ordivorced.
Social determinants of health: Factors that influence the health of populations, including income and social status, social support networks,education, employment/working conditions, social environments, physical environments, personal health practices and coping skills, healthychild development, gender, and culture.
Social support: Refers to the types of support available and includes emotional support, instrumental support, appraisal support and informational support.
Space: The physical location and physical features, both built and natural, of an environment. Suicide and self-inflicted injury mortality: Suicideand self-inflicted injury mortality is the age-standardized rate of death per 100,000 population. All rates are calculated using the total population (all age groups) and are calculated based on the average of three consecutive years of data.
Suburban: Suburban areas are peripheral communities located some distance from the centre core. Suburban areas do not have a specificpopulation density but are generally residential districts typically surrounding a city.
Total, all causes of death: Age-standardized rate of death from all causes per 100,000 population.
Total deprivation: Composed of material and social deprivation, and determined from six factors: 1) the proportion of persons without a highschool degree; 2) the ratio of employment to population; 3) average personal income; 4) the proportion of persons living alone; 5) the proportion of single-parent families; and 6) the proportion of persons who are widowed, separated or divorced.
Understanding Communities Unit: The Understanding Communities Unit (UCU) is the Unit within Public Health Services, CDHA, that is responsible for the population health assessment and surveillance core functions of public health practice, as well as for research, evaluation,program planning, quality assurance, and knowledge translation functions.
Unemployment: Proportion of the labour force aged 15 and over who did not have a job during the reference period. The labour force consistsof people who are currently employed and people who are unemployed but were available to work in the reference period and had looked forwork in the past 4 four weeks. The reference period refers to a one-week period (from Sunday to Saturday) that usually includes the 15th dayof the month.
Unintentional injuries, deaths: Age-standardized rate of death per 100,000 population. External causes of unintentional injuries includetransport accidents, falls, poisoning, drowning and fires, but not complications of medical and surgical care.
Urban: Urban areas are those with a population density greater than 400 persons per km2.
Visible minority: Visible minority refers to whether a person belongs to a visible minority group as defined by the Employment Equity Act. TheEmployment Equity Act defines visible minorities as "persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white incolour".
Wait time for hip fracture surgery (Proportion with surgery within 48 hours): Proportion with surgery within 48 hours: Risk-adjusted proportion of hip fracture patients age 65 and older who underwent hip fracture surgery within 48 hours of admission to hospital. Rates forQuebec are not available due to differences in data collection. Canada rate does not include Quebec.
Youth unemployment: Proportion of the Labour force for youths, aged 15 to 24 years, who did not have a job during the reference period. Thelabour force consists of people who are currently employed and people who are unemployed but were available to work in the reference periodand had looked for work in the past 4 four weeks. The reference period refers to a one-week period (from Sunday to Saturday) that usually includes the 15th day of the month.

C UNIVERSITY & COLLEGE INSTITUTIONS IN HALIFAX PENINSULA
P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix C105
Publically Funded College Nova Scotia Community College - Institute of Technology Campus
Publically funded university University of King's CollegeNova Scotia College Of Art And Design UniversityDalhousie UniversitySaint Mary's UniversityAtlantic School of Theology
Private Registered College Academy of Learning CollegeAtlantic Flight Attendant Academy LimitedCAT Centre for Arts and Technology Canada Inc.Concepts Career CollegeEastern College English CanadaICT® Northumberland CollegeNova Scotia College of Early Childhood Education SocietyRavensberg College
Type of Educational Institution Name of Institution
Note. Data from Nova Scotia Community Counts. (2013). Map Centre with filter: Education Assets - Community Colleges and Universities. Retrieved November 20,2013 from: http://www.novascotia.ca/finance/communitycounts/map_centre/chb.html# Greater Halifax Partnership. (n.d.) Studying in Halifax. Retrieved November20, 2013 from http://www.greaterhalifax.com/en/home/livinginhalifax/Education/default.aspx and Department of Labour and Advanced Education. Private CareerColleges Division. (n.d.) Registered Colleges - filter by City/Town, Category. Retrieved November20, 2013 from: http://pcc.ednet.ns.ca/By_Category-Location

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix D106
D SUMMARY OF DEMOGRAPHIC INDICATORS FOR CAPITAL HEALTH, COMMUNITY HEALTH BOARDS AND COMMUNITIES
Dist
rict H
ealth
Aut
horit
y/Co
mm
unity
Hea
lth
Boar
d / C
omm
unity
Depr
ivatio
nSc
ore
TotalPopulation
TotalReporting
Population DensityPerson per sq km
Popu
latio
na
By A
ge G
roup
s (Ye
ars,
% To
tal P
opul
ation
)Vi
sabl
e M
inor
ities
Non
Imm
igra
nt
Visa
ble
Min
oriti
esb
(Tota
l & %
of T
otal
)Ab
orig
inal
Iden
tityb
(Tota
l & %
of T
otal
)
Total
Material
Social
LoneParent
Born in NS
Citiz
ensh
ip &
Imm
igra
tionb
(Tota
l & %
of T
otal
)Fa
mily
Stru
ctur
ea
(% of
All F
amilie
s)
Common-law
Married
Total
Under 20
20-29
30-39
40-49
50-64
65 & Older
Male
Non-PermanentResidents
Immigrants
Canadian Citizen
Non Canadian
Born Outside NS
Total
TotalReporting
Aboriginal Identity
Other
South Asian(Eg. East Indian)
Chinese/Korean/Japanese
Arab/West Asian
Black
Female
412,51
859
.221
.514
.913
.415
.621
.313
.340
6,29
08.8
9.2
8.3
3.5
1.7
1.4
0.2
2.0
406,29
62.5
406,29
096
.23.8
67.4
23.6
7.9
1.2
67.9
15.4
16.6
90,932
101.0
20.6
13.9
13.8
15.4
21.6
14.6
89,276
9.9
9.8
9.0
1.9
2.6
1.0
0.2
4.2
89,357
1.3
89,362
94.9
4.5
67.2
20.7
10.7
0.7
68.0
15.7
16.2
88,396
153.0
26.8
10.1
13.6
18.4
21.1
10.3
87,944
4.8
4.1
4.1
1.3
0.9
0.8
0.1
1.7
87,928
1.9
87,929
97.4
2.1
67.8
25.3
6.0
0.2
75.1
11.5
13.4
68,210
942.7
19.8
13.8
12.9
15.3
22.8
15.5
67,202
8.1
7.0
6.6
3.9
0.3
0.3
0.2
3.4
67,229
2.3
67,277
97.9
1.4
67.6
25.3
5.9
0.1
62.4
15.9
21.4
24,598
6.6
21.9
9.1
12.1
16.3
25.1
15.3
24,509
1.5
0.8
0.9
0.7
0.4
0.1
0.0
0.3
24,499
2.6
24,494
99.0
0.4
79.7
17.4
2.5
0.0
71.7
14.4
14.0
73,295
3,31
7.8
15.1
28.8
13.8
11.8
17.8
12.9
72,157
15.1
14.8
12.3
3.8
2.9
2.5
0.1
5.8
72,161
1.2
72,151
91.3
8.1
57.3
26.2
11.9
3.7
57.6
23.4
19.2
43,593
242.0
25.4
11.7
13.6
17.1
22.0
10.0
43,385
8.3
7.5
7.3
6.3
0.2
0.3
0.0
1.5
43,433
2.1
43,385
98.8
0.4
68.4
27.0
4.1
0.1
70.4
12.5
16.8
22,078
15.4
22.5
9.1
11.7
15.5
23.6
17.5
21,571
2.5
2.5
2.3
1.7
0.0
0.2
0.0
0.6
21,571
2.0
21,574
99.0
0.9
82.9
14.0
2.8
0.1
69.7
15.9
14.4
Commun
ity
12
111
,556
100.3
31.5
6.6
14.9
22.1
18.1
7.0
11,529
7.2
7.1
5.2
3.3
0.2
1.2
0.3
2.2
11,534
2.2
11,530
97.2
2.5
64.9
28.8
5.8
0.0
81.9
9.7
8.3
11
19,43
176
.629
.86.8
14.3
21.6
19.9
8.6
9,48
71.2
0.5
0.5
0.0
0.0
0.6
0.0
0.6
9,48
20.9
9,48
097
.91.8
69.6
24.8
5.4
0.0
81.8
10.3
8.0
11
111
,526
108.8
29.1
8.1
11.8
19.9
22.6
8.6
11,572
1.1
0.0
0.8
0.0
0.0
0.1
0.0
1.0
11,583
1.6
11,575
96.9
3.0
67.1
25.8
6.7
0.3
79.9
10.8
9.7
33
31,02
445
.526
.79.4
14.4
20.8
22.6
6.3
1,02
46.9
0.8
1.5
6.2
0.0
0.0
0.0
0.7
1,02
41.5
1,02
998
.30.7
76.5
19.2
1.8
0.0
71.7
15.4
12.0
33
310
,712
445.4
28.0
10.5
15.6
19.7
18.6
8.0
10,675
1.9
0.5
1.3
1.3
0.0
0.0
0.0
0.6
10,674
1.2
10,679
99.2
0.4
70.6
26.4
2.4
0.0
73.4
11.8
14.4
23
23,20
224
.125
.810
.312
.718
.521
.610
.93,22
73.0
2.8
1.2
1.8
0.1
0.6
0.0
0.5
3,23
22.3
3,22
299
.20.2
75.0
22.2
2.9
0.0
75.2
13.0
10.9
12
13,24
667
.323
.88.8
12.0
18.1
26.7
11.3
3,34
40.2
0.0
0.2
0.0
0.0
0.0
0.0
0.2
3,34
80.6
3,35
397
.32.6
76.7
17.0
5.8
0.0
76.8
13.8
10.9
22
32,73
468
.822
.58.8
11.3
16.8
27.0
14.2
2,59
40.0
0.1
0.0
0.0
0.0
0.0
0.0
0.0
2,59
40.0
2,60
498
.50.6
82.3
10.4
6.0
0.0
73.0
14.3
13.2
11
225
,161
802.6
25.2
11.5
12.6
16.7
23.7
10.1
25,076
6.9
6.1
5.9
4.3
0.3
0.3
0.0
2.0
25,130
1.9
25,094
98.6
0.4
67.6
26.9
5.0
0.0
72.4
10.9
16.2
11
22,46
839
.322
.58.8
10.7
17.2
26.8
14.6
2,40
71.4
1.8
0.1
1.3
0.0
0.0
0.0
0.1
2,40
10.6
2,41
598
.60.0
69.8
24.1
4.8
0.0
75.1
14.2
10.8
13
13,32
645
.225
.710
.711
.419
.522
.211
.23,27
10.9
0.0
0.0
0.0
0.0
0.0
0.0
0.9
3,26
81.7
3,27
198
.51.2
77.6
19.6
0.7
1.2
72.8
12.6
13.2
11
13,20
143
.425
.910
.912
.917
.324
.29.4
3,07
80.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
3,08
70.5
3,09
098
.20.0
74.9
21.8
1.5
0.0
77.0
13.2
10.6
24
12,66
350
.724
.08.4
11.4
17.7
22.4
15.9
2,70
51.8
0.0
1.5
1.5
0.0
0.0
0.0
0.3
2,71
00.0
2,69
810
00.0
82.3
15.3
2.0
0.0
73.8
14.3
10.5
24
23,83
543
.722
.710
.415
.118
.223
.19.9
3,83
23.0
3.7
0.0
1.2
0.0
0.0
0.0
1.8
3,84
21.4
3,84
798
.00.6
79.8
15.6
3.0
0.0
72.1
17.9
11.2
23
33,03
495
.728
.711
.016
.617
.618
.47.1
3,05
70.2
0.0
0.2
0.0
0.1
0.1
0.0
0.0
3,06
42.3
3,05
299
.60.3
73.1
25.6
0.7
0.2
73.3
14.1
13.0
13
164
015
.317
.89.8
8.9
15.0
29.2
21.3
631
0.3
0.0
0.3
0.0
0.0
0.0
0.0
0.3
636
0.0
636
96.1
3.6
76.1
14.2
8.6
0.0
76.6
12.9
11.4
23
25,01
628
.426
.610
.214
.118
.520
.610
.05,09
60.7
0.0
0.7
0.0
0.2
0.2
0.2
0.1
5,10
00.8
5,09
699
.00.6
75.2
22.2
2.6
0.0
72.9
13.3
13.8
13
27,11
981
.326
.89.9
16.5
17.9
20.1
8.9
6,98
20.9
0.6
0.0
0.6
0.0
0.0
0.0
0.3
6,97
72.7
6,96
499
.30.1
71.9
25.1
2.6
0.0
72.6
13.8
14.3
35
31,06
16.6
23.5
8.2
12.3
17.4
23.5
14.8
1,05
63.5
2.3
2.5
0.0
0.0
0.9
0.0
2.6
1,05
70.1
1,05
599
.10.3
81.7
15.0
1.9
0.0
71.6
15.5
10.6
22
39,38
814
9.3
27.5
10.9
18.3
18.5
17.4
7.7
9,34
27.2
7.7
5.6
3.5
0.6
0.6
0.0
2.5
9,36
32.7
9,35
398
.90.4
73.1
21.9
4.4
0.0
71.0
13.6
15.9
22
32,41
113
.822
.17.1
8.5
17.7
27.8
16.5
2,41
20.7
0.0
0.0
0.0
0.0
0.5
0.0
0.2
2,41
52.9
2,41
298
.21.1
72.8
19.9
6.6
0.4
75.4
12.0
11.6
31
423
,616
1,41
5.8
22.8
11.4
12.1
16.3
22.9
14.5
23,530
8.4
7.6
6.9
5.3
0.2
0.2
0.0
2.7
23,530
1.2
23,570
98.5
0.5
68.8
25.1
5.0
0.0
68.3
12.4
19.3
31
418
,553
458.6
24.1
12.1
11.4
16.1
22.7
13.8
18,269
12.6
12.8
11.4
0.9
4.2
2.8
0.2
4.5
18,268
1.8
18,277
93.7
5.9
58.2
26.2
14.3
0.7
75.3
11.4
13.3
35
21,02
420
.220
.79.6
12.3
16.8
25.9
15.6
983
5.3
1.8
6.0
0.4
0.0
1.9
0.0
3.0
986
0.3
986
98.6
0.6
80.8
15.3
1.5
0.0
69.3
19.0
9.8
24
23,50
114
.022
.09.0
15.2
16.0
25.3
11.5
3,42
70.4
0.0
0.0
0.4
0.0
0.0
0.0
0.0
3,42
72.9
3,43
499
.50.0
77.9
20.4
0.6
0.0
72.8
16.1
10.3
24
12,34
314
.422
.59.6
12.2
16.1
25.3
13.2
2,35
01.4
0.0
0.5
0.3
0.0
0.0
0.0
1.1
2,34
10.3
2,34
597
.12.4
82.0
13.6
4.0
0.0
71.2
17.0
12.7
44
43,06
357
.420
.77.8
10.3
14.1
25.4
21.0
3,08
11.4
0.0
1.7
0.0
0.0
0.0
0.0
1.4
3,08
11.6
3,07
299
.90.0
88.5
9.3
1.8
0.0
74.1
12.0
13.8
34
21,82
27.6
21.0
9.2
13.1
16.3
25.2
14.1
1,82
41.2
0.0
1.6
1.0
0.0
0.0
0.0
0.2
1,81
92.5
1,82
398
.50.7
83.7
13.4
2.9
0.0
69.6
17.3
11.4
Capi
tal H
ealth
Com
mun
ity H
ealth
Brd
.Ch
eucto W
est
Cobe
quid
Dartm
outh
E. Sho
re / Musqu
odob
oitHa
lifax P
enins
ulaSo
uthe
astern
West H
ants
Com
mun
ityHa
mmon
ds Plains
Tantallon
Fall R
iver
Sackville
Up. S
ackville
North
Mid. Sackville
Porte
rs Lake
Prospe
ctHe
rring
Cove
Cole Ha
rbou
rWaverley
Lantz
Hatche
t Lake
Falm
outh
Sambro
Elmsdale
Pegg
y’s Cove
Enfield
Beaver Ban
kWind
sor F
orks
Timbe
rlea
St. M
arga
ret’s Bay
Dartm
outh East
Bedford
Smith
s Co
rner
Mou
nt Unia
cke
Brookly
nHa
ntsport
Newp
ort C
orne
r

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix D107
Dist
rict H
ealth
Aut
horit
y/Co
mm
unity
Hea
lth
Boar
d / C
omm
unity
Depr
ivatio
nSc
ore
TotalPopulation
TotalReporting
Population DensityPerson per sq km
Popu
latio
na
By A
ge G
roup
s (Ye
ars,
% To
tal P
opul
ation
)Vi
sabl
e M
inor
ities
Non
Imm
igra
nt
Visa
ble
Min
oriti
esb
(Tota
l & %
of T
otal
)Ab
orig
inal
Iden
tityb
(Tota
l & %
of T
otal
)
Total
Material
Social
LoneParent
Born in NS
Citiz
ensh
ip &
Imm
igra
tionb
(Tota
l & %
of T
otal
)Fa
mily
Stru
ctur
ea
(% of
All F
amilie
s)
Common-law
Married
Total
Under 20
20-29
30-39
40-49
50-64
65 & Older
Male
Non-PermanentResidents
Immigrants
Canadian Citizen
Non Canadian
Born Outside NS
Total
TotalReporting
Aboriginal Identity
Other
South Asian(Eg. East Indian)
Chinese/Korean/Japanese
Arab/West Asian
Black
Female
32
421
,379
1,17
3.4
23.4
12.1
13.0
16.4
22.7
12.5
21,332
2.7
1.7
3.0
1.6
0.3
0.3
0.0
0.5
21,313
2.6
21,318
99.0
0.2
74.9
22.0
2.2
0.0
68.5
12.2
19.2
12
23,04
498
.925
.39.8
16.0
15.2
25.0
8.8
3,06
32.2
0.5
1.5
1.9
0.0
0.0
0.0
0.3
3,05
34.6
3,06
398
.20.5
75.4
20.7
3.2
0.0
64.0
17.3
18.1
32
411
,740
295.6
26.4
13.1
16.7
17.1
17.0
9.3
11,681
2.1
2.1
0.0
0.5
0.0
0.5
0.0
1.1
11,676
2.5
11,672
99.2
0.4
64.4
32.1
3.0
0.0
65.6
17.6
17.3
44
43,91
633
.621
.610
.613
.616
.924
.611
.83,87
70.3
0.0
0.4
0.0
0.0
0.3
0.0
0.0
3,87
01.1
3,86
798
.80.6
77.8
19.2
2.2
0.0
68.6
16.7
16.0
22
31,48
520
.016
.28.6
10.4
16.6
27.5
21.8
1,47
11.8
0.0
2.1
0.0
0.0
0.0
0.0
1.8
1,47
00.0
1,47
098
.80.7
70.0
22.0
7.6
0.0
75.5
14.3
10.6
33
32,25
113
.419
.59.0
10.0
16.0
26.1
20.1
2,26
33.8
0.0
0.0
0.0
3.8
0.0
0.0
0.0
2,26
82.6
2,26
398
.11.5
75.3
19.2
5.5
0.0
71.7
14.5
13.8
55
11,00
124
.417
.57.9
12.5
18.2
26.9
16.7
989
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
991
0.0
989
97.9
2.3
87.2
7.8
5.1
0.0
75.0
12.3
10.8
45
22,26
931
.925
.911
.58.9
15.5
25.3
13.8
2,25
269
.268
.769
.868
.60.0
0.0
0.0
0.6
2,24
73.7
2,24
799
.80.0
88.0
11.0
0.6
0.0
55.5
6.3
37.0
55
41,56
22.9
17.5
6.0
8.3
12.9
27.9
27.7
1,61
00.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
1,60
76.0
1,61
299
.70.0
89.1
9.6
0.6
0.0
77.9
10.7
12.4
34
41,44
512
.720
.18.6
11.0
16.1
26.6
17.8
1,41
80.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
1,42
01.8
1,41
499
.80.0
84.8
12.2
2.9
0.0
70.5
15.4
14.3
33
42,08
213
.419
.87.8
11.3
15.8
28.3
17.7
2,04
50.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
2,04
20.0
2,04
597
.12.5
76.2
17.1
5.7
0.7
71.6
13.4
13.9
41
534
,439
1,28
1.2
17.7
19.4
14.5
12.9
18.5
16.7
33,689
17.1
18.3
15.2
2.3
5.6
2.3
0.2
6.7
33,694
1.2
33,694
91.1
8.6
57.5
23.1
17.5
1.2
65.9
17.3
16.4
41
518
,764
4,09
6.9
19.3
24.2
13.3
12.9
18.3
12.5
18,516
11.1
10.9
8.4
2.5
1.9
1.7
0.2
4.8
18,531
0.6
18,510
93.6
5.4
62.2
23.7
11.0
1.9
62.8
18.5
19.0
54
54,82
320
9.5
22.2
9.4
9.1
13.5
21.3
24.3
4,36
73.4
4.8
1.9
1.1
0.0
0.0
0.0
2.3
4,36
33.2
4,35
998
.71.1
80.8
14.5
4.4
0.0
62.2
15.5
22.7
41
59,90
496
9.1
16.6
12.6
12.5
13.4
23.2
21.8
9,26
012
.812
.612
.82.1
2.2
0.3
0.0
8.2
9,42
51.5
9,25
092
.16.7
61.9
21.0
15.1
1.7
66.2
15.9
18.2
41
520
,055
2,94
9.3
11.8
41.0
11.4
8.3
14.5
13.1
19,804
16.6
17.0
13.1
0.1
3.8
5.6
0.0
7.1
19,785
0.3
19,785
85.2
14.7
45.0
30.9
14.9
8.4
63.0
28.0
9.7
42
524
,719
1,52
2.1
18.5
13.5
12.6
14.5
22.8
18.2
24,041
5.8
5.2
4.3
1.2
0.5
0.4
0.2
3.5
24,041
2.6
24,027
97.9
1.7
65.9
25.9
7.3
0.1
64.4
16.1
19.1
42
515
,789
2,13
0.8
17.4
19.8
13.7
14.6
20.6
13.8
15,725
12.9
10.9
11.2
2.6
3.8
1.3
0.2
5.0
15,725
1.8
15,740
93.5
5.8
66.1
21.8
10.0
1.4
58.8
18.8
21.9
53
520
,192
3,08
7.5
13.4
26.6
16.8
12.5
19.0
11.7
19,655
17.5
16.8
14.9
8.8
2.7
0.8
0.1
5.1
19,664
1.9
19,655
94.2
4.9
58.6
28.2
9.9
2.1
48.0
28.6
23.7
55
579
42.1
18.3
5.8
6.4
14.2
28.1
28.0
832
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
832
6.1
837
99.3
0.0
89.7
9.8
0.0
0.0
73.4
12.3
13.1
55
496
97.4
23.9
7.8
12.4
16.1
22.9
15.6
957
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
957
0.0
957
100
0.0
89.7
9.1
1.1
0.0
67.8
15.0
16.0
45
11,07
11.4
19.0
7.3
10.3
15.4
27.5
18.5
942
0.6
0.7
0.6
0.4
0.0
0.0
0.0
0.2
942
0.0
942
99.8
0.0
83.8
15.4
0.3
0.0
74.5
10.9
15.8
55
42,18
834
.223
.38.5
11.7
15.7
24.1
17.3
2,20
86.1
4.9
4.7
4.6
0.0
0.1
0.0
1.4
2,20
61.3
2,21
298
.80.3
87.7
9.2
2.8
0.0
66.3
17.7
15.0
11
15,63
987
.623
.89.8
13.2
20.0
24.0
8.7
5,62
41.7
1.2
1.4
1.2
0.2
0.0
0.0
0.3
5,62
90.7
5,62
498
.21.0
72.8
22.1
4.0
0.6
79.5
11.8
8.8
55
394
16.9
21.6
8.8
10.2
13.6
26.2
21.8
954
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
959
0.0
954
100
0.0
87.7
11.8
0.9
0.0
69.2
14.1
16.4
55
31,86
92.9
18.2
5.6
9.5
14.0
28.5
24.1
1,86
60.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
1,86
42.5
1,86
299
.50.0
85.7
12.2
1.7
0.0
75.6
12.6
11.5
44
32,05
53.4
21.5
8.0
11.4
15.3
26.0
16.9
2,02
72.9
3.3
3.0
2.0
0.0
0.0
0.0
0.9
2,02
71.9
2,02
798
.90.0
84.1
14.0
1.7
0.0
71.8
13.3
14.1
54
510
,864
801.8
22.2
12.6
13.6
15.9
23.2
11.9
10,834
9.9
8.1
8.9
5.2
0.2
0.3
1.0
3.2
10,873
2.3
10,863
98.4
1.1
77.2
16.1
5.9
0.0
53.6
17.0
28.9
53
519
,238
672.9
17.5
17.3
14.2
15.1
22.4
13.5
18,996
10.8
8.7
9.5
5.7
0.2
0.3
0.5
4.1
19,023
3.2
19,043
97.1
2.2
68.2
25.0
5.3
0.0
50.5
20.9
27.8
Sackvill
e South-
Lowe
r Sackville
Lake Echo
Eastern Pa
ssag
eCh
ezzetcook
Hacketts Cove
Musqu
odob
oit Harbo
urTerence Ba
yPreston
Sheet H
arbo
urJedd
ore
Hubb
ards
Clayton Pa
rkHa
lifax C
hebu
cto
Wind
sor
Armda
le-No
rthwe
st Arm
Halifa
x Citade
lDa
rtmou
th Sou
thFairview
Halifa
x Needh
amMoser Rive
rSu
mmerville
Uppe
r Musqu
odob
oitTh
ree Mile Plains
Lawr
encetown
Kempt Sho
reSh
ip Ha
rbou
rMidd
le Musqu
odob
oitSp
ryfield
Dartm
outh North

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix D108
Dist
rict H
ealth
Aut
horit
y /Co
mm
unity
Hea
lth B
oard
/Co
mm
unity
Depr
ivatio
nSc
ore
Total Population
% of Low Income Families
% A
ge 2
0 &
Over
w/ P
ost-
Seco
ndar
y Ce
rtific
ate,
Dipl
oma
or
Degr
ee
Popu
latio
na
Inco
mec
Hous
ehol
dsc
Educ
atio
nalc
Atta
inm
ent
Total
Material
Social
Lang
uage
Spo
ken
at H
ome
Mot
her T
ongu
eIn
divid
ual
Empl
oym
ent
Rate
(%)
Fam
ily
English
Own %
Rent %
Need Repair %
French
Both
English
French
Both
Median (in $)
Average (in $)
> 25 Yeasr Old
15 to 24Yeasr Old
Vehicle
PublicTransport
Walk toWork
Median (in $)
Average (in $)
Value (in $)
Monthly MortgagePayments (in $)
Average MonthlyRent (in $)
Labo
urc
Tran
spor
tatio
n (%
)
408,29
294
.80.9
0.2
90.6
2.5
0.4
28,291
36,387
66,019
77,052
9.9
84.0
64.9
35.1
35.6
209,32
497
474
565
.258
.376
.511
.39.9
89,960
93.0
0.7
0.2
88.1
2.3
0.4
30,366
36.499
67,129
75,528
9.9
85.2
60.8
39.2
32.4
206,37
295
563
165
.260
.482
.911
.43.7
88,053
96.6
0.9
0.2
93.0
2.5
0.3
33,7
9841
,434
79,3
1787
,410
6.7
85.6
86.9
13.0
31.4
214,80
91,
043
402
71.1
55.5
88.8
6.7
2.9
67,609
95.6
1.2
0.2
91.8
3.0
0.4
29,423
35,804
64,725
75,205
12.5
82.6
56.1
43.6
36.5
171,60
783
857
162
.559
.972
.517
.67.2
24,527
98.8
0.6
0.1
96.4
2.0
0.2
26,589
31,788
59,206
64,635
7.6
72.9
91.4
9.1
45.1
146,36
572
342
359
.346
.694
.60.8
2.5
72,290
90.2
0.9
0.2
84.2
2.5
0.4
25,543
34,986
68,054
80,119
15.7
88.2
37.7
62.2
36.6
252,
344
965
761
62.2
62.1
44.6
16.0
34.2
43,388
97.0
1.6
0.3
93.4
3.7
0.4
32,095
36,347
71,133
75,531
6.1
85.0
87.3
12.4
35.0
174,11
394
332
171
.056
.484
.011
.32.7
21,740
98.9
0.3
0.1
97.0
1.2
1.0
24,2
7729
,880
52,8
0858
,747
8.7
72.3
82.1
17.8
42.6
145,
819
714
582
56.8
48.2
91.5
0.4
6.4
C
12
111
,501
96.6
1.2
0.2
92.9
2.8
0.5
39,290
49,654
95,131
105,59
84.3
90.7
97.5
2.6
22.0
277,85
61,26
311
376
.756
.996
.31.2
1.1
11
19,42
298
.30.5
0.2
94.7
2.5
0.2
38,015
43,237
85,607
92,025
3.1
89.8
92.7
6.9
29.5
240,49
21,09
549
973
.660
.596
.90.5
1.7
11
111
,530
98.2
1.0
0.1
95.2
2.5
0.2
38,375
48,405
88,439
102,94
44.1
89.8
91.6
8.0
33.1
256,56
71,14
531
874
.253
.794
.32.0
1.3
33
31,02
398
.30.6
0.6
96.6
1.9
0.1
31,757
35,184
64,366
70,577
5.6
81.5
94.9
5.1
39.0
163,21
591
521
975
.454
.890
.47.0
0.4
33
310
,702
98.4
0.7
0.1
95.9
2.3
0.3
32,356
36,536
71,703
74,675
7.0
81.7
92.8
7.4
28.7
182,35
795
538
974
.958
.687
.19.5
1.7
23
23,21
097
.81.0
0.2
95.0
2.8
0.4
33,107
38,375
69,799
78,753
5.4
80.1
95.0
5.2
35.9
191,51
798
914
770
.545
.696
.90.4
1.9
12
13,23
998
.60.5
0.0
95.7
1.9
0.1
33,134
37,800
79,088
80,794
2.6
83.1
92.0
7.8
32.7
203,02
195
554
368
.051
.595
.70.4
0.9
12
12,72
998
.00.5
0.2
95.1
1.5
0.2
31,055
35,194
69,097
72,053
7.9
87.2
88.5
12.0
45.5
227,32
696
830
267
.055
.686
.69.0
2.3
11
225
,141
96.5
1.5
0.3
92.8
3.7
0.3
32,549
37,686
75,494
79,862
5.7
87.2
88.2
11.6
33.4
182,71
298
531
572
.259
.082
.812
.72.4
11
22,46
897
.61.3
0.3
94.3
2.8
0.3
38,228
47,286
87,906
104,56
22.5
89.2
91.7
7.8
35.9
240,82
31,03
432
368
.661
.893
.73.4
1.3
13
13,30
699
.20.6
0.2
97.1
1.5
0.5
26,265
33,124
60,529
67,001
4.6
74.0
89.0
11.5
39.3
162,12
782
539
967
.355
.296
.90.0
1.4
11
13,20
497
.90.8
0.3
94.9
2.2
0.5
30,877
37,249
69,800
78,159
5.2
79.7
92.6
8.2
43.5
188,64
794
736
665
.151
.995
.90.3
1.2
24
22,67
099
.40.5
0.0
97.6
1.1
0.1
26,605
32,432
59,610
65,846
5.4
80.3
90.7
7.9
36.3
165,71
672
930
760
.543
.595
.20.6
2.8
24
23,84
098
.70.5
0.0
96.2
1.8
0.1
28,732
31,579
62,715
66,706
6.0
75.9
94.8
6.3
43.6
169,44
185
710
867
.668
.195
.62.0
3.0
22
33,03
798
.20.2
0.2
96.3
1.2
0.2
31,127
34,708
67,069
71,001
4.3
80.6
87.9
11.9
28.3
179,64
093
156
573
.964
.197
.80.0
2.0
13
164
098
.30.0
0.0
93.4
2.5
0.0
30,173
32,575
59,062
66,563
2.6
78.3
90.4
10.0
45.3
169,85
573
123
159
.50.0
98.4
1.3
8.2
23
25,02
499
.00.5
0.1
96.3
1.8
0.4
32,810
37,902
71,799
76,545
4.8
77.0
81.0
18.6
32.4
189,48
11,00
554
570
.257
.995
.60.4
2.1
22
27,06
498
.41.0
0.1
96.3
2.2
0.2
31,237
35,078
67,077
72,901
6.6
82.9
97.1
3.4
34.6
154,88
987
310
070
.058
.090
.06.4
1.5
23
21,06
199
.20.7
0.0
97.1
1.1
0.1
26,022
31,656
61,033
64,666
2.1
75.3
89.8
10.0
37.8
151,17
576
530
263
.245
.998
.80.6
0.8
22
39,37
995
.70.9
0.3
92.3
2.7
0.3
33,173
37,213
70,262
74,547
7.0
85.8
89.4
10.2
32.0
178,16
81,05
639
776
.957
.590
.84.8
2.6
22
32,40
898
.90.5
0.2
96.6
1.2
0.2
33,437
41,798
80,346
88,958
2.8
86.8
85.7
14.1
34.4
255,41
789
577
962
.659
.196
.00.0
2.6
31
423
,566
96.0
1.8
0.4
92.1
3.6
0.6
31,822
36,614
71,404
77,947
9.3
86.5
79.9
79.8
37.2
179,35
992
741
564
.860
.780
.612
.94.0
31
418
,429
91.3
1.0
0.2
85.4
2.6
0.3
35,587
48,412
91,183
103,48
58.2
90.9
76.4
23.5
25.3
259,09
01,14
767
866
.954
.086
.07.2
4.9
35
21,02
499
.10.9
0.0
96.7
1.7
0.1
22,370
28,542
52,891
58,368
1.3
67.5
90.3
9.7
46.3
116,58
569
252
261
.042
.699
.10.0
0.4
24
23,50
799
.00.6
0.1
96.5
2.2
0.0
27,731
31,588
63,572
64,326
5.2
74.5
90.6
9.7
41.7
170,23
581
554
866
.741
.895
.51.8
0.6
24
12,34
099
.30.4
0.0
97.9
0.8
0.0
25,762
28,983
53,179
57,024
8.1
73.1
90.7
8.2
47.7
139,69
668
122
160
.243
.896
.10.0
1.7
44
43,05
999
.20.1
0.0
97.7
0.9
0.0
22,518
29,883
53,190
60,738
10.5
74.6
78.3
21.3
42.1
171,95
272
750
658
.361
.682
.40.4
15.1
34
21,82
699
.40.5
0.0
97.7
0.8
0.1
26,268
24,030
52,637
57,898
6.9
71.1
89.6
9.8
46.5
136,15
966
048
663
.352
.496
.40.0
2.4
Capi
tal H
ealth
Com
mun
ity H
ealth
Brd
.Ch
eucto W
est
Cobe
quid
Dartm
outh
E. Sho
re / Musqu
odob
oitHa
lifax P
enins
ulaSo
uthe
astern
West H
ants
Com
mun
ityHa
mmon
ds Plains
Tantallon
Fall R
iver
Sackville
Up. S
ackville
North
Mid. Sackville
Porte
rs Lake
Prospe
ctHe
rring
Cove
Cole Ha
rbou
rWaverley
Lantz
Hatche
t Lake
Falm
outh
Sambro
Elmsdale
Pegg
y’s Cove
Enfield
Beaver Ban
kWind
sor F
orks
Timbe
rlea
St. M
arga
ret’s Bay
Dartm
outh East
Bedford
Smith
s Co
rner
Mou
nt Unia
cke
Brookly
nHa
ntsport
Newp
ort C
orne
r

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix D109
Dist
rict H
ealth
Aut
horit
y /Co
mm
unity
Hea
lth B
oard
/Co
mm
unity
Depr
ivatio
nSc
ore
Total Population
% of Low Income Families
% A
ge 2
0 &
Over
w/ P
ost-
Seco
ndar
y Ce
rtific
ate,
Dipl
oma
or
Degr
ee
Popu
latio
na
Inco
mec
Hous
ehol
dsc
Educ
atio
nalc
Atta
inm
ent
Total
Material
Social
Lang
uage
Spo
ken
at H
ome
Mot
her T
ongu
eIn
divid
ual
Empl
oym
ent
Rate
(%)
Fam
ily
English
Own %
Rent %
Need Repair %
French
Both
English
French
Both
Median (in $)
Average (in $)
> 25 Yeasr Old
15 to 24Yeasr Old
Vehicle
PublicTransport
Walk toWork
Median (in $)
Average (in $)
Value (in $)
Monthly MortgagePayments (in $)
Average MonthlyRent (in $)
Labo
urc
Tran
spor
tatio
n (%
)
32
421
,319
98.0
0.8
0.1
94.9
2.7
0.3
28,265
33,056
64,896
69,533
9.3
80.2
80.6
19.2
39.7
166,88
990
446
767
.955
.881
.811
.84.7
12
23,05
497
.81.2
0.0
95.7
2.8
0.3
32,582
35,401
66,941
70,083
6.3
83.9
93.2
7.0
39.1
147,70
086
446
570
.842
.495
.40.7
1.7
32
411
,565
96.9
1.9
0.3
93.4
4.2
0.6
32,835
35,210
63,783
68,976
6.8
84.2
83.6
16.0
37.2
145,93
387
443
271
.951
.084
.210
.53.6
44
43,92
598
.50.7
0.0
95.8
2.4
0.2
28,874
33,695
63,901
67,063
6.2
76.4
91.6
8.9
49.0
158,57
878
153
061
.747
.994
.21.9
1.2
22
31,48
998
.10.5
0.2
94.7
2.0
0.2
30,314
36,579
67,771
79,577
2.6
79.7
87.5
12.5
44.4
226,58
076
561
563
.270
.096
.10.7
1.1
33
32,20
999
.60.1
0.0
95.8
1.6
0.0
28,669
33,334
64,737
72,706
2.7
79.3
89.0
10.5
44.7
172,88
974
450
957
.652
.793
.10.0
4.3
55
199
997
.60.5
0.0
96.6
1.5
0.0
25,666
28,769
58,488
61,776
4.3
61.9
95.1
3.7
45.0
153,05
077
20.0
58.8
78.4
96.3
00
45
22,27
399
.40.4
0.1
98.6
0.9
0.0
19,576
24,069
45,927
51,327
13.1
60.5
83.4
16.5
45.3
177,94
773
840
751
.652
.576
.418
.23.0
55
51,53
799
.50.3
0.0
98.6
1.0
0.0
19,019
24,363
43,132
49,737
16.2
61.2
86.1
14.4
47.2
104,43
555
427
742
.236
.092
.21.6
4.1
34
41,44
599
.20.3
0.3
96.6
1.7
0.0
21,512
28,219
49,806
55,712
8.0
77.2
91.5
9.3
53.1
139,45
768
955
555
.476
.290
.81.4
4.4
33
42,08
098
.70.1
0.1
95.7
1.5
0.3
30,792
35,728
68,880
71,104
7.8
80.7
86.1
13.5
42.8
200,39
272
843
663
.255
.894
.00
4.1
41
534
,025
87.0
0.8
0.2
80.1
2.6
0.5
30,666
37,443
68,888
77,695
10.8
90.8
39.2
60.6
24.7
210,25
397
680
065
.962
.478
.115
.54.6
41
518
,582
92.3
0.9
0.3
87.1
2.4
0.3
26,877
36,570
74,667
87,302
11.7
88.9
47.9
52.2
37.9
280,98
01,07
478
565
.261
.148
.115
.730
.4
54
54,49
897
.70.3
0.0
95.4
0.9
0.0
25,684
32,018
47,923
56,083
17.6
72.6
55.7
44.0
38.1
163,44
677
258
750
.047
.979
.40
18.0
41
59,38
392
.40.9
0.2
86.8
2.5
0.4
31,319
39,449
70,554
82,501
9.6
85.9
56.2
43.6
32.7
222,65
11,02
176
061
.263
.172
.817
.75.6
41
519
,679
86.0
1.0
0.1
78.2
2.5
0.5
27,477
42,740
91,904
114,37
114
.494
.930
.769
.130
.232
3,46
51,10
388
461
.462
.831
.59.7
54.6
42
524
,272
95.5
1.0
0.2
91.3
2.9
0.4
29,792
37,946
64,396
79,487
10.8
82.1
54.1
45.8
34.7
192,93
491
065
261
.256
.469
.718
.19.6
42
515
,725
91.2
0.7
0.2
86.1
2.2
0.3
24,819
30,657
53,136
64,064
15.9
83.1
41.0
59.6
35.2
210,40
884
963
857
.760
.864
.623
.69.1
53
519
,856
93.1
0.9
0.3
87.5
2.7
0.6
23,397
29,579
51,713
57,765
20.5
85.0
34.9
64.7
42.3
206,15
985
770
163
.864
.042
.916
.733
.5
55
579
799
.50.0
0.0
99.0
1.1
0.0
16,247
21,685
37,755
43,978
16.0
45.8
95.4
5.1
52.6
104,17
836
910
236
.030
.786
.80
11.5
55
497
099
.40.2
0.0
97.9
0.8
0.0
16,932
24,200
41,017
46,285
15.0
68.1
91.5
6.9
54.1
101,14
756
019
043
.058
.098
.00
1.0
45
11,06
599
.30.6
0.0
98.9
1.4
0.0
18,687
25,619
42,232
50,968
12.5
58.8
90.8
10.9
48.1
92.411
489
630
48.6
098
.30
1.1
55
42,17
699
.30.4
0.0
98.6
0.6
0.1
23,681
26,550
48,177
51,508
6.6
66.1
87.1
13.0
45.3
123,21
663
059
953
.748
.293
.10
4.7
11
15,63
497
.81.4
0.5
93.9
3.5
0.4
35,019
38,612
78,879
81,093
2.7
87.7
96.5
3.3
34.3
209,80
41,00
388
73.3
56.0
94.6
1.8
1.3
55
394
999
.50.3
0.0
97.4
0.7
0.0
16,887
23,033
39,120
47,006
11.1
58.0
95.9
4.1
54.5
90,136
492
040
.751
.394
.10
5.2
55
31,87
699
.50.1
0.1
98.5
0.8
0.0
20,487
26,844
50,010
55,009
11.0
62.3
92.0
8.4
48.4
111,53
956
353
852
.029
.490
.11.0
4.2
44
42,03
599
.70.2
0.2
97.5
1.0
0.0
22,329
28,792
50,713
56,333
9.2
69.8
86.6
13.8
52.1
125,07
756
052
556
.051
.294
.30.8
3.6
54
510
,838
96.2
0.3
0.0
92.6
1.7
0.3
22,530
27,934
46,749
54,794
23.8
72.1
52.1
47.8
42.9
144,14
878
256
956
.650
.970
.422
.44.9
53
519
,135
95.4
0.8
0.2
92.1
2.3
0.3
25,747
32,054
54,201
65,015
19.4
78.2
33.4
66.1
37.6
138,65
466
464
361
.062
.364
.623
.48.9
Sackville So
uth - Lowe
r Sackville
Lake Echo
Eastern Pa
ssag
eCh
ezzetcook
Hacketts Cove
Musqu
odob
oit Harbo
urTerence Ba
yPreston
Sheet H
arbo
urJedd
ore
Hubb
ards
Clayton Pa
rkHa
lifax C
hebu
cto
Wind
sor
Armda
le-No
rthwe
st Arm
Halifa
x Citade
lDa
rtmou
th Sou
thFairview
Halifa
x Needh
amMoser Rive
rSu
mmerville
Uppe
r Musqu
odob
oitTh
ree Mile Plains
Lawr
encetown
Kempt Sho
reSh
ip Ha
rbou
rMidd
le Musqu
odob
oitSp
ryfield
Dartm
outh North
Note: a 2011 Canadian Census data, b 2011 National Household Survey data, c 2006 Canadian Census data, NA – no data available for this level. Other – Filipino, Latin American,Southeast AsianGovernment of Nova Scotia. (2013). Nova Scotia Community Counts. Retrieved October 3, 2013 http://www.gov.ns.ca/finance/communitycounts/geogpage.asp

E RANKING OF CAPITAL HEALTH AGAINST PEER GROUPS
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix E110
Dependency ratio (%)
Ambulatory care sensitive conditions (per 100,000 population)
Seniors, 65 years and over, as a proportion of total population (%)
5 year internal migrants (%)
1 year internal migrants (%)
Hysterectomy (per 100,000 population)
Infant mortality (per 1,000 live births)
Injury hospitalization (per 100,000population)
Coronary artery bypass graft (per100,000 population)
Fruit and vegetable consumption, 5times or more per day (%)
Unemployment (%)
Pain or discomfort that prevents activities (%)
Hospitalized acute myocardial infarction event rate (per 100,000population)
Life expectancy at age 65 (years)
Suicides and self-inflicted injuries,deaths (per 100,000 population)
Youth, under 20 years, as a proportion of total population (%)
Aboriginal population (%)
Chronic obstructive pulmonary disease (COPD) (%)
Immigrant population (%)
Hip replacement (per 100,000 population)
Wait time for hip fracture surgery(proportion with surgery within 48 hrs.)
Hospitalized hip fracture event rate(per 100,000 population)
30-day acute myocardial infarction(AMI) in-hospital mortality (rate)
Perceived life stress (%)
All of the other health units in the peer group have more dependents (people aged 0 to 19 yearsor 65 years and above) relative to the total number of people aged 20 to 64 years.
32 of the other health units in the peer group have higher rates of ambulatory care sensitive conditions than CDHA.
31 of the other health units in the peer group have more seniors (65 years and over) in their population compared to CDHA.
There are 3 health units in the peer group who have fewer 5 year internal migrants compared toCDHA.
There are 3 health units in the peer group who have fewer 1 year internal migrants compared toCDHA.
30 of the health units in the peer group have higher rates of hysterectomy than CDHA.
There are 29 health units in the peer group who have higher rates of infant mortality compared toCDHA (ranking out of 34).
29 health units in the peer group have higher rates of injury hospitalization compared to CDHA.
There are 28 health units in the peer group that have higher rates of coronary artery bypass graftcompared to CDHA.
There are 28 health units in the peer group that have populations who consume fruits and vegetables more, on average, than the population in CDHA.
There are 27 health units in the peer group with higher unemployment compared to CDHA.
26 health units in the peer group have higher proportions of the population reporting they havepain or discomfort that prevents activities compared to CDHA.
There are 25 health units in the peer group with higher rates of hospitalized acute myocardial infarction events compared to CDHA.
There are 25 health units in the peer group with higher life expectancy at age 65 compared toCDHA.
There are 25 health units in the peer group with higher rates of suicides and self-inflicted injuryrelated deaths compared to CDHA (ranking out of 34).
There are 25 health units with higher proportions of young people (under 20 years) in their population compared to the population in CDHA.
There are 25 health units that have higher proportions of aboriginal population compared toCDHA.
24 health units in the peer group have higher proportions of the population with COPD comparedto the population in CDHA (ranking out of 34).
24 health units in the peer group have larger immigrant populations compared to CDHA.
There are 24 health units in the peer group with higher rates of hip replacement (per 100,000population) compared to the CDHA rate.
23 health units in the peer group have a higher proportion of patients needing hip fracture surgerywho get the surgery within 48 hours (ranking out of 28).
22 health units in the peer group have higher hospitalized hip fracture event rates compared tothe CDHA rate.
There are 21 health units in the peer group that have higher rates of 30-day acute myocardial infarction (AMI) in-hospital mortality compared to CDHA (ranking out of 28).
21 health units in the peer group have larger proportions of the population who report experiencing perceived life stress compared to the population in CDHA.
50.2
227.0
11.7
11.5
3.6
286.0
3.3
425.0
53
37.7
6.2
12.6
187.0
19.4
8.6
21.7
1.4
4.3E
7.2
103.0
66.9
442.0
7.3
21.1
35th
33rd
32nd
32nd
31st
31st
30th
30th
29th
29th
28th
27th
26th
26th
26th
26th
26th
25th
25th
25th
24th
23rd
22nd
22nd
Indicator Cap HealthEst. Rank* Interpretation

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix E111
Injuries within the past 12 monthscausing limitation of normalactivities (%)
Hospitalized stroke event rate (per100,000 population)
Breast cancer incidence (per100,000 population)
Ischemic heart diseases, deaths (per100,000 population)
High blood pressure (%)
Injuries in the past 12 months,sought medical attention (%)
Prostate cancer incidence (per100,000 population)
Sense of community belonging (%)
Cardiac revascularization (per100,000 population)
Caesarean section (proportion)
Mood disorder (%)
Knee replacement (per 100,000population)
Percutaneous coronary intervention(per 100,000 population)
Youth unemployment aged 15 to 24 (%)
Second-hand smoke, exposure athome (%)
Overweight (%)
Functional health, good to full (%)
Bronchitis, emphysema and asthma,deaths (per 100,000 population)
Circulatory diseases, deaths (per100,000 population)
Current smoker, daily (%)
Long-term unemployment (%)
Diabetes (%)
Cerebrovascular diseases, deaths(per 100,000 population)
Children in low income families (%)
21 health units in the peer group report larger proportions of the population who had injurieswithin the past 12 months causing limitation of normal activities, compared to the CDHA population.
There are 20 health units in the peer group with higher hospitalized stroke event rates comparedto CDHA (ranking out of 28).
There are 20 health units in the peer group with higher rates of breast cancer compared to theCDHA rate (ranking out of 34).
20 health units in the peer group report higher rates of ischaemic heart disease death comparedto CDHA (ranking out of 34).
There are 20 health units in the peer group that have higher proportions of their populations withhigh blood pressure compared to the population in CDHA.
9 health units in the peer group have larger proportions of the population who had injuries in thepast 12 months and sought medical attention compared to the CDHA population.
There are 19 health units in the peer group with higher rates of prostate cancer compared to theCDHA rate (ranking out of 34).
There are 19 health units in the peer group that have higher proportions of their population reporting a sense of community belonging compared to the population in CDHA.
18 health units in the peer group have higher rates of cardiac revascularization compared to therate in CDHA (ranking out of 28).
18 health units in the peer group have higher proportions of caesarean section among the population compared to CDHA.
CDHA falls exactly in the middle of the peer group with respect to the proportion of the populationwho report having a mood disorder.
CDHA falls exactly in the middle of the peer group with respect to the rates of knee replacementin the population.
There are 16 health units in the peer group with higher rates of percutaneous coronary intervention compared to the CDHA rate (ranking out of 28).
There are 16 health units in the peer group with higher proportions of youth unemployment intheir populations compared to CDHA (ranking out of 32).
16 health units in the peer group have higher proportions of the population who report exposureto second hand smoke at home compared to the population in CDHA (ranking out of 34).
There are 16 health units in the peer group that have a higher percentage of people overweight inthe population compared to CDHA.
There are 16 health units in the peer group with higher proportions of the population reportinggood to full functional health, compared to CDHA.
There are 15 health units in the peer group that have higher rates of bronchitis, emphysema andasthma related deaths compared to the rate in CDHA (ranking out of 34).
There are 15 health units in the peer group that have higher rates of circulatory disease relateddeaths compared to the rates in CDHA (ranking out of 34).
15 health units in the peer group have reported higher proportions of the population who are current, daily smokers, compared to CDHA.
13 health units in the peer group have reported higher proportions of the population with long-term unemployment compared to CDHA.
13 health units in the peer group have reported higher proportions of the population with diabetescompared to CDHA.
There are 13 health units in the peer group that have higher rates of cerebrovascular disease related deaths compared to the rates in CDHA (ranking out of 34).
13 health units in the peer group have reported higher proportions of children aged 17 and underliving in low income families, compared to the proportion in the CDHA population.
15.5
113.0
11.9
82.5
17.2
8.5
8.6
67.1
221.0
26.4
7.6
189.0
169.0
14.2
6.8E
35.6
79.3
2.4
169.9
17.4
3.1
6.4
33.5
15.4
22nd
21st
21st
21st
21st
20th
20th
20th
19th
19th
18th
18th
17th
17th
17th
17th
17th
16th
16th
16th
14th
14th
14th
14th
Indicator Cap HealthEst. Rank* Interpretation

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix E112
Current smoker, daily or occasional(%)
Pain or discomfort, moderate or severe (%)
Population living within a Metropolitan Influenced Zone (%)
Second-hand smoke, exposure in vehicles and/or public places (%)
Participation and activity limitation,sometimes or often (%)
Life satisfaction, satisfied or verysatisfied (%)
Life expectancy at birth (years)
Colorectal cancer incidence (per100,000 population)
Total mortality, all causes of death(per 100,000 population)
Lung cancer incidence (per 100,000population)
Leisure-time physical activity, moderately active or active (%)
Regular medical doctor (%)
Pneumonia and influenza, deaths(per 100,000 population)
Low income (%)
Population density (persons per km2)
Respiratory diseases, deaths (per100,000 population)
All other respiratory diseases, deaths(per 100,000 population)
Unintentional injuries, deaths (per100,000 population)
Overweight or obese (%)
30-day stroke in-hospital mortality(rate)
Obese (%)
Asthma (%)
Visible minority population (%)
Lone-parent families (%)
All cancers, deaths (per 100,000population)
13 health units in the peer group have reported higher proportions of the population who are current (daily or occasional) smokers compared to CDHA.
12 health units in the peer group have higher proportions of the population who report moderateor severe pain or discomfort compared to the population in CDHA.
12 health units in the peer group have reported higher proportions of the population who are living within a Metropolitan Influenced Zone compared to CDHA.
11 health units in the peer group have higher proportions of the population who report exposureto second hand smoke in vehicles and/or public places compared to the population in CDHA.
11 health units in the peer group have higher proportions of the population who report participation and activity limitation (sometimes or often) compared to the population in CDHA.
11 health units in the peer group have higher proportions of the population who report being satisfied or very satisfied with their life compared to the population in CDHA.
There are 10 health units in the peer group with higher life expectancy for the population compared to the life expectancy for CDHA.
There are 10 health units in the peer group that have higher rates of colorectal cancer comparedto the rates in CDHA (ranking out of 34).
There are 10 health units in the peer group that have higher rates of total mortality compared tothe rates in CDHA (ranking out of 34).
There are 10 health units in the peer group that have higher rates of lung cancer (compared tothe rates in CDHA (ranking out of 34).
10 health units in the peer group have higher proportions of the population who report participatingin moderately active or active leisure-time physical activity compared to the population in CDHA.
10 health units in the peer group have higher proportions of the population who report having aregular medical doctor compared to the population in CDHA.
There are 9 health units in the peer group that have higher rates of pneumonia and influenzadeaths compared to the rates in CDHA (ranking out of 34).
9 health units in the peer group have higher proportions of the population who are considered low income, compared to the population in CDHA.
9 health units in the peer group have a higher population density compared to CDHA.
There are 8 health units in the peer group that have higher rates of respiratory disease deathcompared to the rates in CDHA (ranking out of 34).
There are 8 health units in the peer group that have higher rates of all other respiratory diseasedeaths compared to the rates in CDHA (ranking out of 34).
There are 8 health units in the peer group that have higher rates of unintentional injury relateddeaths compared to the rates in CDHA (ranking out of 34).
There are 8 health units in the peer group that have a higher percentage of people either overweight or obese in the population compared to CDHA.
7 health units in the peer group have higher rates of 30-day stroke in-hospital mortality comparedto CDHA (ranking out of 28).
There are 7 health units in the peer group that have a higher percentage of people obese in thepopulation compared to CDHA.
7 health units in the peer group have higher proportions of the population who have asthma, compared to the population in CDHA.
7 health units in the peer group have higher proportions of visible minorities in their populationscompared to the population in CDHA.
6 health units in the peer group have reported higher proportions of lone-parent families, compared to the proportion in the CDHA population.
There are 6 health units in the peer group that have higher rates of all cancer mortality comparedto the rates in CDHA (ranking out of 34).
22.5
13.5
95.3
15.2
34.7
93
80.6
18.8
583.4
50.8
56.8
92.2
13.3
14.1
57.0
50.9
35.2
28.8
58.0
18.7
22.4
10.7
7.3
16.4
182.2
14th
13th
13th
12th
12th
12th
11th
11th
11th
11th
11th
11th
10th
10th
10th
9th
9th
9th
9th
8th
8th
8th
8th
7th
7th
Indicator Cap HealthEst.
Rank* Interpretation

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix E113
Perceived mental health, very goodor excellent (%)
Arthritis (%)
Doctors rate - General/family physicians (per 100,000 population)
Low birth weight (% of live births)
Doctors rate - Specialist physicians(per 100,000 population)
Perceived health, very good or excellent (%)
Inflow/outflow ratio - Overall (ratio)
All other circulatory diseases, deaths(per 100,000 population)
High school graduates aged 25 to 29 (%)
Bike helmet use (%)
Post-secondary graduates aged 25to 54 (%)
Heavy drinking (%)
Influenza immunization (%)
Contact with a medical doctor in thepast 12 months (%)
6 health units in the peer group have higher proportions of the population who report very good orexcellent perceived mental health compared to the population in CDHA.
6 health units in the peer group have higher proportions of the population living with arthritis compared to the population in CDHA.
There are 6 health units in the peer group that have higher rates of general/family physiciansamong their population compared to the rates in CDHA.
5 health units in the peer group have higher rates of low birth weight babies (per 100 live births)compared to the rate in CDHA (ranking out of 34).
There are 4 health units in the peer group that have higher rates of specialist physicians amongtheir population compared to the rates in CDHA.
3 health units in the peer group have higher proportions of the population who report very good orexcellent perceived health compared to the population in CDHA.
CDHA has the 4th highest inflow/outflow ratio compared of other health units in the peer group.
There are 2 health units in the peer group that have higher rates of all other circulatory diseasemortality compared to the rates in CDHA (ranking out of 34).
There are 2 health units with higher proportions of high school graduates (aged 25-29 years) intheir populations compared to the population in CDHA.
There is only 1 health unit with higher proportions of reported bike helmet use in their populationscompared to the population in CDHA.
There is only 1 health unit with higher proportions of post-secondary graduates (aged 25-54years) in their population compared to the population in CDHA.
CDHA has the highest reported proportion of heavy drinking among its population compared toother health units in the peer group.
CDHA has the highest proportion influenza immunization among its population compared to otherhealth units in the peer group.
CDHA has the highest proportion of its population reporting contact with a medical doctor in thelast 12 months, compared to the populations in other health units of the peer group.
76.7
24.0
131.0
6.2
172.0
63.5
1.43
54.0
90.3
76.1
68.3
22.8
41.1
86.1
7th
7th
7th
6th
5th
4th
4th
3rd
3rd
2nd
2nd
1st
1st
1st
Indicator Cap HealthEst. Rank* Interpretation
Note. *The rank is based on 35 health units in Peer Group A, unless otherwise noted. The data source was Statistics Canada. 2013. Health Profile. Statistics CanadaCatalogue No. 82-228-XWE. Ottawa. Released January 29, 2013. Accessed from http://www12.statcan.gc.ca/health-sante/82-228/index.cfm?Lang=E

F SUMMARY OF THE LITERATURE FOR THE HEALTH OUTCOMES
C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix F114
OBESITY
It has been reported that rates of overweight and obesity are increasing across Canada, with Nova Scotia having a higher ratethan the national average (Statistics Canada, 2013k). Beingoverweight or obese may create an increased risk for developinghealth related issues. Obesity has been associated with a varietyof lifestyle factors such as physical activity level and healthy diet.Obesity has also been associated with many lifestyle relatedchronic diseases such as heart disease, diabetes and high bloodpressure (Guh, Zhang, Bansback, Amarsi, Birmingham, & Anis,2009; Orpana, Berthelot, Kaplan, Feeny, McFarland, & Ross,2010). The burden of obesity is not just a health issue but alsoan economic burden. The economic burden of obesity has beenreported to be in the range of $4.6 to $7.1 billion in Canada(PHAC & CIHI, 2011).
There is growing evidence of a relationship between obesity anddeprivation (CIHI, 2008; Matheson, Moineddin, & Glazier, 2008;McLaren, 2007). CIHI (2008) found an increased number ofthose self-reporting overweight and obesity in categories ofhighest total deprivation compared to those in the category oflowest total deprivation. Using Canadian Community Health Survey data and a material deprivation index composed of sixvariables, Matheson et al. (2008) reported the association between obesity and material deprivation varied for males andfemales. For women, those living in the most deprived neighbourhoods were more likely to have a higher BMI whilemales in the least deprived neighbourhoods were more likely tohave a higher BMI. The researchers suggested that the commonly accepted factors for weight gain and higher BMIs,that is lifestyle and behaviourial factors, are not the full explanation.
Fruit and vegetable consumption is commonly used as a measure for healthy eating. However, the relationship betweenbeing overweight or obese and fruit and vegetable consumptionis less clear. Some research suggests a diet with adequate levelsof fruits and vegetables decreases one’s chance of being overweight or obese (Giskes et al., 2011; Vioque et al., 2008).Other reviews have not found conclusive evidence (Heo et al.,2011; Ledoux et al., 2011) but the overall health benefits of diethigh in fruits and vegetables has been well documented.
Literature suggests an association between socioeconomic status and fruit and vegetable consumption with lower socio-economic groups more likely to consume less fruits and vegetables in their diets (Dubowitz et al., 2008; Giskes et al.,2010). Dubowitz et al. (2008) reported individuals living inneighbourhoods with increasing deprivation were less likely toconsume five portions of fruit and vegetables on five or moredays of the week. The researchers suggested efforts to increasethe availability of fresh foods in disadvantaged neighbourhoodsmay improve diets. The link between deprivation and overweight
or obese may be associated with reduced availability of freshfoods and fitness amenities in areas of higher deprivation. Giventhe association between material deprivation and overweight orobese, individuals residing in areas of higher material deprivationmay have limited resources to buy food. Access to food as a riskfactor for obesity was also explored by Lopez (2007). The studyfindings suggested an association between the presence of asupermarket and a decreased risk of being obese. It was suggested that food access may be a priority for reducing obesity.
Low income neighborhoods have been described as “fooddeserts” due to the lack of readily available produce or “foodswamps” because of the concentration of unhealthy fast,processed and packaged foods (Dubowitz et al., 2013). Thelower consumption of fruits and vegetables among lower socioeconomic groups may be due to an increased likelihood offast food and take-out consumption (Glanz et al., 1998; Pereira,et al., 2005). A recent study of the relationship between fastfood restaurant density and social and material deprivation inNova Scotia was conducted by Jones, Terashima, and Rainham(2009). The researchers reported community-level deprivation inNova Scotia was associated with fast food outlet density addingto the body of literature linking the environment to obesity. Robitaille et al. (2010) also reported urban settings with a higherlevel of deprivation had an increased likelihood of a fast-foodrestaurant in close proximity of the school.
There is a growing body of literature that supports the link between obesity, food security and deprivation. Using 2005CCHS data, Slater et al. (2009) food insecurity was predictive foroverweight and obesity, but only for women. The authors arguedfood insecurity was directly linked to low income, and this situation was frequently exacerbated for women in single parentfamilies. For women in single parent families, there were increased levels of body mass index, which could be a result ofrelying on eating energy dense and low nutrient foods. A reviewconducted by Franklin et al. (2012) reported that one in sevenAmerican households experience food insecurity at times duringthe year as lack of money and other resources hinder their abilityto maintain consistent access to nutritious foods. Based on 19studies conducted in the preceding 7 years, the review suggested that food insecurity and obesity continued to bestrongly and positively associated in women.
The association between being overweight or obese and beingphysically inactive has been identified in a number of studies including the systematic review of the evidence for the physicalactivity guidelines for adults in Canada (Warburton, Charlesworth,Ivey, Nettleford, & Bredin, 2010). The physical activity guidelinesfor adults aged 18 to 64 years recommends at least 150 minutes of moderate to vigourous intensity aerobic physical activity per week in periods of 10 minutes or more, and muscleand bone strengthening activities at least 2 days per week.
As noted in the Methodology, a review of the literature was conducted to identify the risk and community factors associated with thehealth outcomes as well as the potential impact of material and social deprivation on the outcomes. The findings of the literature reviewfor each health outcome have been summarized in this appendix.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix F115
The authors’ state physical activity appears to have a role in theprevention of obesity and co-morbidities associated with obesity.
The built environment can be defined as all of the buildings,spaces and products, including our homes, schools, workplaces,parks, business centres, and roads (Duranceau & Bergeron,2013). The importance of the built environment on physical activity and obesity has been identified in a number of reports.As succinctly stated by Lopez (2007), “Where one lives may affect obesity status”. Duranceau and Bergeron (2013) suggested that the built environment plays a supportive role inphysical activity among youth but additional evidence is necessary to allow for specific recommendations on modificationson the built environment.
Further evidence of the association between the built environment and physical activity was provided by Black andMacinko (2008). In a review of 37 studies, the researchers founda consistent association between body mass index and neighborfeatures that discourage physical activity. In a second study conducted by Black and Macinko (2010), the association between area income, fitness amenities and obesity was explored for neighborhoods in New York during the period of2003 to 2007. The researchers found that the increased area income and availability of local fitness amenities was significantlyassociated with reduced obesity (p < .001). Analyses for obesityby fitness amenities were not included in this population healthreport. However, the geographic distribution of parks and parkfeatures and trails suggests a concentration in urban areas.
Studies on mental health and obesity have established that obesity was significantly associated with mood disorders (Chen,Jiang, & Mao, 2009; Gadalla, 2009). Gadalla found that the oddsof obesity among those with a mood disorder or a mood disorderand anxiety were 1.50 times higher compared to those with nei-ther disorder. Chen et al. (2009) found that individuals with ab-normal body weight (being underweight, overweight or obese) atincreased risk of depression. While there is no clear causal rela-tionship established between obesity and mental health prob-lems, some studies argue that obesity is a predictor ofdepression (Roberts, Deleger, Strawbridge, Kaplan, 2003; Lu,2007 and Gariepy et al. 2010b). Vanasse et al. (2012) suggestedthe prevalence of mood disorders was higher in material and socially deprived areas, recommending improvement of materialconditions to impact population mental health. While continuedresearch is needed to fully explain the link between deprivationand moods disorders, there is an increased awareness of the social aspect of mental health. There is a need to consider thecircumstances of people’s lives, such as employment and income, as important contributors to the mental wellbeing of individuals (Friedli, 2009).
ALCOHOL
Alcohol use impacts our culture, economy, politics, health statusand relationships. Over- consumption of alcohol can have negative effects on our community, our health and our lives. InHalifax Regional Municipality, there were over 1000 arrestsmade for impaired driving of a vehicle or a boat in 2012 (HalifaxRegional Police, 2013).
The Nova Scotia alcohol strategy, ‘Changing the Culture of Alcohol Use in Nova Scotia’ reports an average of 3,100 hospitaladmissions (42,000 hospital days) in Nova Scotia that can be attributed to alcohol, with 230 alcohol-related deaths occurringannually (Department of Health Promotion and Protection, 2007).Other undesirable outcomes linked to alcohol include physicaland sexual assaults, and family and intimate partner violence (CDC, 2011). Many chronic diseases (such as gastrointestinal diseases, eight types of cancer, and heart disease) are linked to either alcohol use or alcohol dependence(CDC, 2011).
Patterns of consumption have revealed trends towards harmfulbehaviours. In 2011, 17.4% (95% CI 16.9 – 18.0) of Canadiansreported having 5 or more drinks on one occasion, at least oncea month in the previous year (Statistics Canada, 2013g). In NovaScotia, 25.1% (95% CI 19.6 – 25.1) reported having 5 or moredrinks, while in Capital Health, 26.4% (95% CI 21.5 – 31.2) reported having 5 or more drinks (Statistics Canada, 2013g). Thepercentages were based on a population aged 12 years andolder so the estimate rates may be reduced. Interestingly, thedaily consumption of alcohol in Capital Health and Nova Scotiawas less than the daily consumption among Canadians. In2009/10, 7.1% of Canadians reported daily alcohol consumptionin the past year. In Capital Health and Nova Scotia, the percentageof people who consumed alcohol daily was 5.6% and 5.0%, respectively. While daily drinking may be less likely, heavy drinking is more likely.
The findings of a number of studies have shown that lower socioeconomic status is associated with an increased likelihoodof heavy drinking (Batty et al., 2008; Baumann et al., 2007) andincreased harmful impacts from heavy alcohol consumption(Cerdá et al. 2011; Erskine et al., 2010; Batty et al., 2008).There is evidence that drinking habits of men may be more influenced by socioeconomic status than women (Matheson etal., 2012; McKinney, CM., Chartier, KG., Caetano, R., & Harris,2012). A U-shaped pattern has been found in the literature.Those who are most economically deprived and those who areleast economically deprived have been found to report more frequent alcohol consumption than those with average deprivation (Matheson et al., 2012).
Studies have shown that people who drink are more likely tosmoke, and there is a correlation between alcohol and tobaccodependence (Grant, Hasin, Chou, Stinson, & Dawson, 2004). Thelink between tobacco smoking and deprivation was noted in astudy by Baumann et al. (2007) who found tobacco use was related to poverty, educational level and working conditions.
In accordance with Statistics Canada (2013c), life satisfaction isa subjective measure of individual well-being. The relationshipbetween life satisfaction and heavy drinking has been exploredin a number of studies. Koivumaa-Honkanen et al. (2012) examined the bi-directional relationship between life satisfactionand alcohol accounting for genetic and familial factors. Thestudy found that the higher the level of alcohol consumption, thestronger was the relationship with life dissatisfaction among theparticipants, more strongly than vice-versa. Paul, Grubaugh,Frueh, Ellis and Egede (2011) also found heavy drinking was associated with less life satisfaction.

C A P I TA L H E A LT H • P O P U L A T I O N H E A L T H S T A T U S R E P O R T
Appendix F116
There is some evidence of a relationship between deprivationand life satisfaction. Bellis et al. (2012) found that positive lifesatisfaction was strongly associated with lower deprivation.
In addition to the influence of deprivation and risk factors onheavy drinking, community factors must also be considered.Studies have shown communities with a high density of alcoholoutlets are associated with higher rates of violence, drinking anddriving, motor vehicle related pedestrian injuries; child abuseand neglect; and alcohol related deaths (Campbell et al., 2009;Stockwell et al., 2011; Task Force on Community PreventiveServices, 2009). Ahern, Margerison-Zilko, Hubbard, and Galea(2013) reported an increased prevalence in binge drinking withincreased alcohol outlet density. The relationship was nonlinearand strongest at densities of more than 80 outlets per squaremile. Pereira, Wood, Foster, and Haggar (2013) stated consumption of alcohol at harmful levels was more likely amongparticipants with greater access to liquor stores. The researchersalso found the mean number of liquor stores to be higher inareas with a lower socioeconomic index.
MENTAL HEALTH
The World Health Organization (WHO, 2011b) defines mentalhealth as “a state of well-being in which the individual realizeshis or her own abilities, can cope with the normal stresses oflife, can work productively and fruitfully, and is able to make acontribution to his or her community.” Positive mental health isincreasingly being linked with positive overall health with somearguing that it is impossible separate mental health from physi-cal health (Prince et al., 2007). A recent national report foundthat people reporting higher levels of positive mental health wereless likely to self-report adverse health outcomes (CIHI, 2009).One’s mental health status is influenced by a variety of determinants throughout their life span including biological, social, and economical determinants (CIHI, 2009).
In addition to the physical and emotional consequences of mental illness, mental illness also poses huge economic burdenon our society. It is estimated that the direct cost of mental illness in Canada is around $43.3 billion and the indirect costsare estimated at $6.3 billion (Risk Analytica, 2011). It is projected that mental illness will be the leading cause of disability in high income countries by 2030 (Mathers & Loncar,2006).
Since 2003, self-rated negative mental health has been gradually increasing in Canada. This is true for Nova Scotia andCapital Health. Recent results from the CCHS indicated moreNova Scotians report fair or poor mental health when comparedto the rest of Canada. This percentage was even higher for people who live within the Capital Health boundaries. The area ofmental health is gaining more attention and recently the NovaScotia government released a provincial mental health and addictions strategy, “Together we can: The plan to improve mental health and addictions care for Nova Scotians”(Departmentof Health and Wellness, 2012). The strategy has five priorityareas: intervening and treating early for better results; shorterwaits, better care; aboriginal and diverse communities; workingtogether differently; and reducing stigma.
A number of reports have found a significant association betweenself-reported negative mental health and total deprivation withan increased likelihood of reporting negative mental health forthose in the most deprived category compared to those in theleast deprived category (CIHI, 2008). Stafford and Marmot(2003) suggested that neighbourhood deprivation increased therisk of poor mental health. However, mental health was operationalized as depression and not self-rated mental health.This association was also found for both material and socialdeprivation.
Mental health studies clearly demonstrate that a relationship exists between the severity of emotional disorders and availability of social support (Cohen, Gottlieb, & Underwood,2000), and much research has identified a lack of available social support within poor populations (Kessler, 1982). Poor populations display a higher prevalence of risk factors associated with stressful events as well as lower protective factors related to a lack of social support. Bellis et al. (2012)argue that in deprived communities, a concentration of low lifesatisfaction and low mental well-being in younger age groupsmay relate to individuals having more adverse childhood experiences and less access to resources. They argue that thesemay play a contributory role in their increased risk for anti-socialbehaviors and violence. This association was also found for bothmaterial and social deprivation.
In a recent study, Charles, Piazza, Mogle, Sliwinski, and Almeida(2013) found that with a heightened reaction to daily stressors,there are long-term implications with a heightened likelihood ofreporting anxiety and depressive disorders. A relationship between stress in daily life and deprivation was not found in thispopulation health status report. This is contrary to the literaturewhich states high levels of stress among those with adverse social and material living conditions (Mikkonen & Raphael,2010). This chronic stress leads to an increased vulnerability forchronic diseases such as cardiovascular and immune systemdiseases and diabetes.
Studies which have explored the relationship between obesityand mental health have suggested the association is bidirectional, where obese persons are more likely to developdepression over time and depressed persons are more likely tobecome obese (National Obesity Observatory, 2011). The bidirectionality emphasizes the complexity of the relationship,particularly when considering the risk factors, such as age andsocioeconomic status, which may influence the direction orstrength of the association.
The evidence supporting the influence of physical activity onmental health is inconclusive. While there are studies which report an association between moderate to vigourous physicalactivity and mental health (Wang, Orpana, Morrison, de Groh,Dai, & Luo, 2012; Teychenne, Ball, & Salmon, 2008), others report no association (Van Berkel, Proper, van Dam, Boot,Bongers, & van der Beek, 2013). An association between physical activity and deprivation was not found in this populationhealth status report.

P O P U L A T I O N H E A L T H S T A T U S R E P O R T • C A P I TA L H E A LT H
Appendix F117
Poor oral health has been associated with a lower quality of life,affecting daily functioning, and self-esteem and has been linkedto cardiovascular disease, respiratory infections, diabetes, poornutrition, osteoporosis, and rheumatoid arthritis (King, 2012).Oral health is an important part of physical health. A recentCochrane review found that people with mental illness have agreater risk of developing oral disease and have a greater needfor oral treatment than the general population (Khokhar, Clifton,Jones, & Tosh, 2011).
A recent study by Ravaghi, Quinonez, and Allison (2013) lookedinto the magnitude of oral health inequalities in Canada for 4oral health outcomes, the number of decayed teeth, number ofmissing teeth, number of filled teeth, and oral pain in the pastyear. Socioeconomic status was measured as household incomeand the relative concentration index was used to quantify healthinequalities. The study found significant deviation from equalityfor all four outcomes with the greatest inequality occurring in thenumber of decayed teeth between the worse off and most affluent. The study also found that a consistently greater inequality for all outcomes existed for women compared to men.Another study by Elani, Harper, Allison, Bedos, and Kaufman(2012) looked into socioeconomic inequalities and oral health inCanada and the United States over the past 35 years. The authors identified that oral health outcomes have improved foradults in both countries and that both countries have demonstrated a decline in absolute socioeconomic inequalitiesin oral health.
Khaled, Bulloch, Exner, & Patten (2009) found a high prevalence(21.9%) of major depression among current smokers than non-smokers (12.2%) in the general Canadian population usingCCHS data. This prevalence was especially elevated amongsmokers in the younger age groups.
The correlation between sense of belonging and mental healthhas been suggested by a number of studies. While the conceptof belonging is difficult to quantify, a strong sense of belonginghas been associated with better self-reported health. One studyconducted a regional assessment to explore sense of communitybelonging and health (Kitchen et al., 2012). The authors indentified a significant and consistent association betweensense of belonging and health, particularly mental health. Thestudy also showed that sense of belonging was lowest amongyouth, residents of high-rise apartments and among single-parents and highest among seniors, people residing in single-detached homes and couples with children. A 2008 review studyexamined the evidence on relationship between characteristicsof neighborhoods and mental health. The author indicates thatthere is some evidence that persons who reported witnessing abeating, abuse or murder were more likely to experience depression if they lived in neighbourhoods with high rates of violent crimes (Kim, 2008). The same review also found thatwomen who experienced negative life events and at the sametime lived in disadvantaged neighbourhoods were more likely todevelop major depression. Another study found similar results(Stafford et al., 2007). Fear of crime was associated with poorermental health. Those participants who reported greater fear were1.93 times more likely (95% CI 1.55-2.41) to have depressionthan those who reported lower fear of crime.

Public Health Services7 Mellor Ave., Unit 5, Dartmouth, NS Canada B3B 0E8Tel: 902.481.5800 Website: http://www.cdha.nshealth.ca/public-health