Embed Size (px)
Citation preview

An Overview of the Alberta Screening & Prevention Initiative
Improvement Facilitator Training Session 1 Day 1
Objectives
• Overview of TOP • The Origins of ASaP• The ASaP Opportunity• The Benefits of ASaP• The ASaP Intervention • Improvement Facilitator Support• The Medical Home
Toward Optimized Practice
• Clinical Practice Guideline Program
• Clinical Process Improvement Program/s – Customized – Targeted
initiatives

The Origins of ASaP
National Context– Council of
Federation Health Innovation Initiative Working Group
– C – Change Cardiovascular Harmonized National Guideline Endeavour
Alberta Context – Integrated clinics
project – Pharmacy project – Worksite project
– ASaP project in partnership with key organizations
AHS
TOP

The ASaP Partnerships A7

Why ASaP?
• Family physicians do an outstanding job of screening individual patients during focused screening visits.
• The challenge is more than one-third of patients simply do not “self-present.”
• The majority of these patients are attached to physicians
• Evidence says the most effective behavior change tool is an invite from their primary care provider and team to complete screening
• There are a number of physicians in Alberta who have tried opportunistic and/or outreach engagement of patients for screening – it works !
• Methods are time and cost effective• ASaP will bring those methods to PCNs for PCNs to
provide to participating clinics
A2
The ASaP Opportunity
The ASaP Initiative is focused on supporting primary care providers ( physicians and nurse practitioners) and team members to offer a screening and prevention bundle to all their patients through enhanced opportunistic and planned outreach methods, targeting patients who do not present for screening care.

Maneuvers Menu for AdultsManeuver Age (years) Interval
Blood Pressure 18+ Annual Weight 18+ AnnualHeight 18+ Once lifetimeExercise Assessment 18+ AnnualTobacco Use Assessment 18+ AnnualAlcohol Use Assessment 18+ AnnualInfluenza Vaccination/ Screen 18+ AnnualPap Test Females 21 – 69 3 years
Plasma Lipid ProfileMales 40 – 74
Females 50 – 74 3 years
CV Risk CalculationMales 40 – 74
Females 50 – 74 3 years
Diabetes ScreenOne of:- Fasting Glucose- Hgb A1c- Diabetes Risk Calculator
40+ 3 years
Colorectal Cancer ScreenOne of:- FOBT/FIT- Flex Sigmoidoscopy- Colonoscopy
50 – 74
2 years5 years10 years
Mammography Females 50 - 69 (74*) 2 years
A3
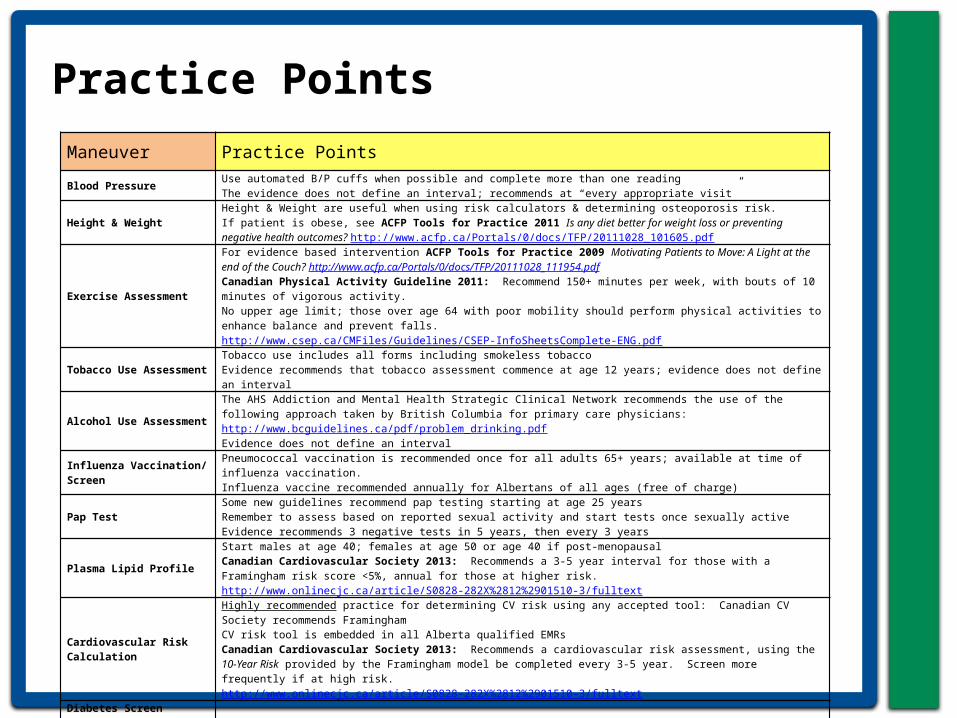
Practice Points
Maneuver Practice Points
Blood PressureUse automated B/P cuffs when possible and complete more than one readingThe evidence does not define an interval; recommends at “every appropriate visit”
Height & WeightHeight & Weight are useful when using risk calculators & determining osteoporosis risk. If patient is obese, see ACFP Tools for Practice 2011 Is any diet better for weight loss or preventing negative health outcomes? http://www.acfp.ca/Portals/0/docs/TFP/20111028_101605.pdf
Exercise Assessment
For evidence based intervention ACFP Tools for Practice 2009 Motivating Patients to Move: A Light at the end of the Couch? http://www.acfp.ca/Portals/0/docs/TFP/20111028_111954.pdf Canadian Physical Activity Guideline 2011: Recommend 150+ minutes per week, with bouts of 10 minutes of vigorous activity. No upper age limit; those over age 64 with poor mobility should perform physical activities to enhance balance and prevent falls. http://www.csep.ca/CMFiles/Guidelines/CSEP-InfoSheetsComplete-ENG.pdf
Tobacco Use Assessment
Tobacco use includes all forms including smokeless tobacco Evidence recommends that tobacco assessment commence at age 12 years; evidence does not define an interval
Alcohol Use Assessment
The AHS Addiction and Mental Health Strategic Clinical Network recommends the use of the following approach taken by British Columbia for primary care physicians: http://www.bcguidelines.ca/pdf/problem_drinking.pdfEvidence does not define an interval
Influenza Vaccination/ Screen
Pneumococcal vaccination is recommended once for all adults 65+ years; available at time of influenza vaccination.Influenza vaccine recommended annually for Albertans of all ages (free of charge)
Pap TestSome new guidelines recommend pap testing starting at age 25 yearsRemember to assess based on reported sexual activity and start tests once sexually active Evidence recommends 3 negative tests in 5 years, then every 3 years
Plasma Lipid Profile
Start males at age 40; females at age 50 or age 40 if post-menopausalCanadian Cardiovascular Society 2013: Recommends a 3-5 year interval for those with a Framingham risk score <5%, annual for those at higher risk. http://www.onlinecjc.ca/article/S0828-282X%2812%2901510-3/fulltext
Cardiovascular Risk Calculation
Highly recommended practice for determining CV risk using any accepted tool: Canadian CV Society recommends FraminghamCV risk tool is embedded in all Alberta qualified EMRsCanadian Cardiovascular Society 2013: Recommends a cardiovascular risk assessment, using the 10-Year Risk provided by the Framingham model be completed every 3-5 year. Screen more frequently if at high risk. http://www.onlinecjc.ca/article/S0828-282X%2812%2901510-3/fulltext
Diabetes Screen- Fasting Glucose OR- Hgb A1c OR- Diabetes Risk
Calculator
Recommended to use a Diabetes Risk Calculator (e.g. CANRISK, FINDRISC)Canadian Task Force on Preventive Health Care 2012: Does not recommend routine screening for Type 2 diabetes for adults at low to moderate risk of diabetes as determined with a validated risk calculator. http://www.cmaj.ca/content/184/15/1687
Colorectal Cancer Screen- FOBT/FIT OR- Flex
Sigmoidoscopy OR- Colonoscopy
FIT test proposed to be available fall 2013
Mammography*New guidelines recommend mammography for women to age 74 years Clinical Breast Examination not indicated in conjunction with mammography
Benefits of ASaP to Primary Care Providers & Their Teams
• Customized screening processes
• Patient panel processes and lists
• Enhance role of teams & EMR
• Improvement Tools & Resources
A2

Benefits of ASaP to Primary Care Organizations
• Practice Facilitation Identification & Training
• EMR support • Improvement
Results reported for providers, clinic and PCO
• Access to QI training Tools and resources
A2

How will this occur?
• Toward Optimized Practice will offer training, tools and resources to identified facilitators within primary care networks to support the screening and prevention improvements.
• Following training, primary care organizations will:– engage physicians to participate – offer practice facilitation to primary care
providers and team members to support the development of customized processes at the primary care organization and/or
clinic levels.
13
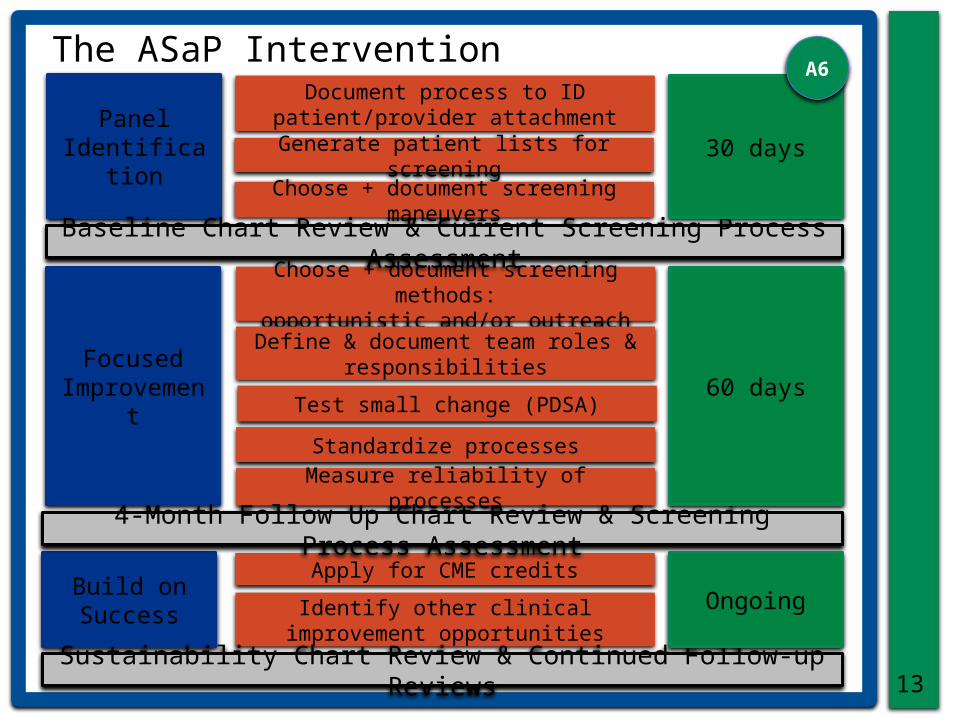
The ASaP Intervention
Panel Identificatio
n
Focused Improvemen
t
Build on Success
Document process to ID patient/provider attachment
Generate patient lists for screening
Choose + document screening methods:
opportunistic and/or outreach
Choose + document screening maneuvers
Define & document team roles & responsibilities
Test small change (PDSA)
Standardize processes
Measure reliability of processes
Apply for CME credits
Identify other clinical improvement opportunities
Baseline Chart Review & Current Screening Process Assessment
4-Month Follow Up Chart Review & Screening Process Assessment
Sustainability Chart Review & Continued Follow-up Reviews
30 days
60 days
Ongoing
A6

14
Improvement Facilitator Training
Improvement Facilitator –
Building PCN Quality Improvement (QI)
Knowledge and Capacity
TOP Clinical Process Advisor•Designated QI support
specialist
Quality Improvement
Training in Cohort
•2+1+1 = 4 days face-to-face
•Cohort Webinars
Community of Learning
• Training Cohort• Other Cohorts• QI community
building
QI Knowledge Resources•Institute for
Healthcare Improvement (IHI):
Open School•Other resources
Electronic Medical Record
Knowledge Resources•Screening and
prevention
H4

PCN will be invited to • Identify improvement facilitators who will be
provided with the resources and mentorship to support clinics and primary care organizations implementing this initiative.
• Participate in planning and implementation activities to locally select changes to maximize screening and prevention methods and results.
• Participate in planning and implementation activities to support emerging communities of practice in facilitation and EMR use.
• Coordinate and deliver, with support, physician engagement events.
• Identify staff members who will receive resources, tools and methods to conduct standardized chart reviews.

Benefits of ASaP to Albertans
• Improve screening offers
• Improve early detection
• Progress toward patient-centred medical home
A2

The Medical Home A9
What is the difference between a medical
home and a medical hotel?
In your home, someone cares about you
even when you are not in their room.

Primary Care Sustainable Results for Active Participation in ASaP
A10









![Tabletop Exercise Facilitator Handbook Template · Web viewFOR OFFICIAL USE ONLYAbout this Facilitator Guide FACILITATOR HANDBOOK [Exercise Name]Facilitator Handbook FACILITATOR HANDBOOK](https://img.pdfslide.us/doc/110x75/5ae2303b7f8b9a0d7d8bfd35/tabletop-exercise-facilitator-handbook-viewfor-official-use-onlyabout-this-facilitator.jpg)


















