Embed Size (px)
Citation preview

An Observational Study to Determine the Incidence of Thyroid Dysfunction Among Pregnant Women in Northern Tasmania: Effect of Thyroid
Status on Maternal, Foetal and Neonatal Outcomes
Abdul Majeed, MBBS
Submitted in fulfilment of the requirements for the degree of Master of Biomedical Science
School of Health Sciences Faculty of Health
University of Tasmania
May 2015

I
Declaration
I hereby declare that this thesis entitled An observational study to determine the
incidence of thyroid dysfunction among pregnant women in Northern Tasmania:
effect of low thyroid status on maternal, foetal and neonatal outcomes contains no
material which has been accepted for a degree or diploma by the University or any
other institution, except by way of background information and duly acknowledged
in the thesis, and to the my knowledge and belief no material previously published or
written by another person except where due reference is made in the text of thesis,
nor does the thesis contain any material that infringes copyright.
Date: 29/05/2015 Signed:
Authority of access
This thesis may be made available for loan and limited copying and communication
in accordance with the Copyright Act 1968.
Date: 29/05/2015 Signed:

II
Statement of ethical conduct
The research associated with this thesis abides by the international and Australian
codes on human and animal experimentation, the guidelines by the Australian
Government’s Office of Gene Technology Regulator and the rulings of the Safety,
Ethics and Institutional Biosafety Committees of the University.
Date: 29/05/2015 Signed:
Full Name: Abdul Majeed

III
Acknowledgements
First, I would like to thank Prof. Alhossain Khalafallah for encouraging me towards
medical research. Special thanks to Prof. Dominic Geraghty for his trust and support.
I would also like to thank the University of Tasmania and the Clifford Craig Medical
Research Trust for giving me this opportunity and for the sponsorship. Special thanks
to Mr Peter Milne, the CEO of the Clifford Craig Medical Research Trust.
Launceston, Tasmania for logistic and monetary support.
My supervisors were my guidance, I would like to sincerely acknowledge Dr.
Murray Adams, Prof. Madeleine Ball, Prof. Alhossain Khalafallah and Dr. Iain
Robertson for their advice, tolerance and being there whenever needed.
I shall not forget to thank Mary Sexton who always covered my absence while I was
on leave, she was a great support. I extend my gratitude to the lovely and a very co-
operative staff of the Pathology Department at the Launceston General Hospital (Dr.
Terry Brain, David Seaton, Shirley Rix, Deanne Yunk, Scott Green, Diane Adams,
Lauren Curtis, Tania McCutcheon, Gerald Bates, Barbara Jessup, Wade Clarkson
and Clinton Trevett) for their great help and special thanks to the participants who
donated with their precious blood and time. Many thanks to the Staff at the QV
antenatal clinic and the labour ward (Dr. Irena Nikakis and Dr. Eileen Phuah). I also
appreciate the kindness and help I received from the Department of Patient
Information.

IV
Finally, I would like to thank my wife Safa, for her understanding, love and full
support throughout these years. Many thanks as well to my mother and the rest of my
large family for their continuous moral support.

V
TABLE OF CONTENTS
Declaration .................................................................................................................... I
Authority of access ........................................................................................................ I
Statement of ethical conduct ....................................................................................... II
Acknowledgements .................................................................................................... III
List of Figures ......................................................................................................... VIII
List of Tables.............................................................................................................. IX
List of abbreviations .................................................................................................... X
Summary of the thesis ............................................................................................. XIII
1 LITERATURE REVIEW ..................................................................................... 1
1.1 Introduction ........................................................................................................... 2
1.2 Iodine and Iodine Deficiency Disorder (IDD) ...................................................... 4
1.2.1 Background ............................................................................................. 4
1.2.2 Iodine & iodine metabolism ................................................................... 6
1.2.3 IDD ....................................................................................................... 10
1.3 Thyroid Gland ..................................................................................................... 12
1.3.1 General anatomy and physiology ......................................................... 12
1.3.2 Thyroid hormones and pregnancy ........................................................ 15
1.4 Thyroid diseases and pregnancy ......................................................................... 16
1.4.1 IDD Complications in pregnancy ......................................................... 21
1.5 Iron 26

VI
1.5.1 Iron requirement ................................................................................... 28
1.5.2 Iron Deficiency Anaemia (IDA) during pregnancy .............................. 28
1.5.3 Possible complications of IDA in pregnancy ....................................... 29
1.5.4 IDA and thyroid disease ....................................................................... 30
1.6 Screening for IDD in pregnancy ......................................................................... 31
1.6.1 Screening tools and interpretation of results ......................................... 33
1.7 Cord blood and neonatal thyroid assessment ...................................................... 36
1.8 Aims and Hypothesis .......................................................................................... 37
2 Materials and Methods ........................................................................................ 38
2.1 Study Design ....................................................................................................... 39
2.1.1 Ethics .................................................................................................... 39
2.1.2 Recruitment ........................................................................................... 39
2.2 Sample collection and handling .......................................................................... 43
2.3 Tests principles ................................................................................................... 44
2.4 Data collection, entry and storage ....................................................................... 45
2.5 Data analysis ....................................................................................................... 45
2.5.1 Methods of statistics ............................................................................. 45
3 RESULTS ........................................................................................................... 49
3.1 Description of the study population .................................................................... 50
3.2 Study outcomes ................................................................................................... 54
3.2.1 Incidence of thyroid abnormalities in the study population ................. 54

VII
3.2.2 Association of maternal and foetal complications rate with thyroid
status ..................................................................................................... 57
3.2.3 Association of rates of neonatal complications with thyroid status ...... 68
3.3 Other considerations ........................................................................................... 73
3.3.1 Association between low thyroid status and iron deficiency anaemia . 73
3.3.2 Examination of surveillance of thyroid function using urinary iodine . 73
3.3.3 Study results-based reference group ..................................................... 74
3.3.4 Cord blood TSH .................................................................................... 76
4 Discussion and conclusion .................................................................................. 78
Bibliography ............................................................................................................... 88
Appendices ............................................................................................................... 108
Appendix 1: Invitation form..................................................................................... 108
Appendix 2: Information sheet and consent form .................................................... 109
Appendix 3: Questionnaire ...................................................................................... 112

VIII
List of Figures
Figure 1-1 Iodine metabolism and transport ................................................................ 7
Figure 1-2 Mechanism of the thyroid hormones regulation....................................... 14
Figure 1-3 Overview of iron transport and metabolism ............................................. 27
Figure 2-1 Study design and Recruitment flow ......................................................... 40
Figure 3-1 Study populations with response rate and recruitment ............................. 51
Figure 3-2 Distribution of gestational age in study population ................................. 53
Figure 3-3 Distribution of predictive risk score in patients with low or normal thyroid
status ................................................................................................................... 67

IX
List of Tables
Table 1-1 TSH upper normal value and prevalence of thyroid dysfunction .............. 17
Table 1-2 Population-based trimester specific intervals for TSH .............................. 20
Table 1-3 Variability of maternal and neonatal complications in association with
thyroid dysfunction ............................................................................................ 24
Table 3-1 Ante-, intra- or post-natal complications in groups defined by thyroid
status ................................................................................................................... 55
Table 3-2 Association of individual antenatal complications and low thyroid status 59
Table 3-3 Association of individual intra-natal complications and low thyroid status1
............................................................................................................................ 62
Table 3-4 The predictive association between symptoms of possible thyroid disease
at clinic visit and the discovery of low thyroid function1 .................................. 65
Table 3-5 Apgar scores at 1 and 5 minutes born to mothers with low or normal
thyroid status ...................................................................................................... 69
Table 3-6 Head circumference of babies born to low thyroid status mothers or
normal mothers................................................................................................... 70
Table 3-7 Requirement for resuscitation of babies born to low thyroid status mothers
or normal mothers .............................................................................................. 71
Table 3-8 Requirement for nursery admission of babies born to low thyroid status
mothers or normal mothers ................................................................................ 72
Table 3-9 Association of low thyroid status1 with various forms of anaemia,
including microcytic (iron-deficiency) anaemia ................................................ 75
Table 3-10 Association between predictor variables and levels of cord TSH1 .......... 77

X
List of abbreviations
AACE American Association of Clinical Endocrinologists
AI Adequate intake
APH Ante-partum haemorrhage
ATA American thyroid association
BD Becton Dickenson
C5 Fifth cervical vertebra
CB-TSH Cord blood TSH
EDTA Ethylenediaminetetraacetic acid
ES Endocrine society
FBC Full blood count
Fe2+ Heme iron
Fe3+ Non-heme iron
FT3 Free triiodthronine
FT4 Free thyroxin
GDM Gestational diabetes mellitus
GHTN Gestational hypertension
HCG Human chorionic gonadotropin
HTN Hypertension
ICCIDD International council for the control of iodine deficiency disorders
ICP-MS Inductively coupled plasma mass spectroscopy
IDA Iron deficiency anaemia
IDD Iodine deficiency disorder
IH Isolated hypothyroxinemia
IOM Institute of medicine

XI
IPH Intrapartum haemorrhage
IQ Intelligence quotient
IRR Incidence rate ratio
IUFGR Intra-uterine foetal growth restriction
LC/MS/MS Liquid chromatography/tandem mass spectrometry
LGH Launceston general hospital
LSCS
MCV
Lower segment caesareans section
Mean corpuscular volume
NHMRC National Health and Medical Research Council
NIS Sodium/iodide symporter
OH Overt hypothyroidism
PPH Postpartum haemorrhage
RDA Recommended dietary allowance
RDS Respiratory distress syndrome
RNI Recommended nutrient intake
ROC Receiver operating curve
RPA Royal Prince Alfred
SCH Subclinical hypothyroidism
T1 First thoracic
T3 Triiodthyronin
T4 Thyroxin
TBG Thyroxin binding globulin
TG Thyroid globulin
TRH Thyrotropine releasing hormone
TISP Tasmanian iodine supplementation program

XII
TPL Threatened premature labour
TPO Thyroid peroxidase
TSH Thyroid stimulating hormone
UI Urinary iodine
UIC Urinary iodine concentration
UIE Urinary iodine excretion
USA United States of America
USI Universal salt iodisation
WHO World Health Organisation

XIII
Summary of the thesis
This thesis comprises four chapters; Literature Review, Materials and Methods,
Results and Discussion/Conclusions. It represents the work conducted by the
candidate during the period April 2013 and May 2015.
Chapter one is a critical review of the scientific literature related to iodine and iodine
deficiency. Firstly, it highlights that Tasmania has had a history of thyroid disease in
the community, including iodine deficiency. More recently, a Tasmanian study
reported that children born to iodine-deficient mothers suffered impaired cognitive
development.
Secondly, it examines the changes occur in thyroid function during pregnancy and
whether these have any influence on pregnancy outcomes. It further analyses
different opinions regarding the role of iron in pregnancy as well as the effect of iron
deficiency anaemia on pregnancy. It also explores the feasibility of iodine level
surveillance in childbearing women as well as potential applications of cord blood in
foetal thyroid assessment.
Studies of thyroid function and iron deficiency during pregnancy in Tasmania are
limited. Furthermore, the application of general screening for thyroid
function/dysfunction during and prior to pregnancy remains controversial. Thus, the
overall aim of the present study was to determine the incidence of thyroid
dysfunction during pregnancy and to investigate whether any possible relationships
exist between low thyroid status and complications occurred during pregnancy and
labour.

XIV
Chapter two summarises the study design, subject recruitment, materials, and
methods used during this study. It further describes sample processing, tests used
during screening, including full blood count, iron studies, maternal, foetal thyroid
function tests (TSH, FT4, FT3 and anti-thyroid peroxidase antibodies), and urinary
iodine concentration.
The results chapter primarily presents the data of the study in a series of tables and
figures, including description of the study population and study outcomes. A
response rate of 28.9% was demonstrated, with 609/636 (95.7%) of participants
successfully screened for thyroid status. Next, incidence of thyroid abnormalities in
the study population was demonstrated; 22 (9 with TSH >3 mU/L, 13 with TSH 2.5-
3mU/L) and 75 with FT4<8.93.4%, representing 3.4% of low thyroid status and
12.3% of isolated hypothyroxinemia, respectively.
Furthermore, possible association of maternal and foetal complications with the
thyroid status was also shown; prolonged labour (IRR 3.31; 95% CI 1.13 to 9.69;
P<0.05) and gestational diabetes (IRR 1.69; 95% CI 0.55-5.25; P=0.36). It also
demonstrates that the study population is iodine deficient; median UIC=117µg/L
with 11.2% of them having developed isolated hypothyroxinemia (FT4<8.9 mU/L)
during pregnancy.
Additionally, CB-TSH results of 402/615 (65%) of babies born to this study cohort
was analysed. It shows a significant decrease of TSH level in the cord blood of
babies born to participants with bleeding complications (APH/IPH) (Mean (SD)

XV
4.91(2.16); 95% CI -5.48 to -2.48; P<0.001) compared to CB-TSH of babies born to
participants without bleeding (Mean (SD) 9.40(5.97)). Although this may not reflect
abnormal foetal thyroid function, it does demonstrate a strong thyroid reaction to
maternal ante-/intra-partum bleeding that needs further investigations.
The last chapter discusses the main outcomes of the study and shows how the
incidence of low thyroid function of this study is unexpectedly low but in line with
international figures. It also discusses the importance of iodine surveillance as well
as general screening for thyroid function prior or at early pregnancy. The chapter
concludes by emphasising the importance of the incidence of thyroid disorder in this
population in Northern Tasmania, and the possibility of an increased incidence of
antenatal complication in association with low thyroid status being equivocal. Since
the main limitation of this study was the small sample size, more statistically
significant outcomes are anticipated with larger scale studies in the future.

1 LITERATURE REVIEW

2
1.1 Introduction
Management of a swollen thyroid gland (Goitre) was first explained by the ancient
Chinese 3500 years ago (Temple, 1999). Iodine deficiency was later recognised to be
the main cause of goitre in some areas of mountainous terrain and other inland places
(Vanderpas, 2006, Richards and Stewart, 2007, Zimmermann, 2010). Tasmania has a
strong history of battling with iodine deficiency and goitre (Gibson, 2006). The
magnitude of the disease was clearly evidenced by pictures and reports in a
Tasmanian publication (Richards and Stewart, 2007). Furthermore, early reports of
medical and surgical treatment for goitre in the Launceston General Hospital (LGH),
were made in late 19th century (Richards and Stewart, 2007). It has been advised that
any health condition caused by iodine deficiency which is preventable by iodine
supplementation is now classified as an Iodine Deficiency Disorder (IDD), by the
World Health Organisation (WHO) (Andersson et al., 2005, Andersson et al., 2012).
The prevalence of thyroid diseases in a form of subclinical hypothyroidism during
pregnancy is estimated to be 1.5-4% (Allan et al., 2000, Casey et al., 2005, Negro
and Mestman, 2011). While the physiology and pathology of the thyroid gland has
been well studied, results of thyroid function tests in laboratories varied considerably
during pregnancy (Burrow, 1990, Glinoer, 1999, Casey and Leveno, 2006, Gärtner,
2009, Hall, 2010). Pregnancy was described as a state of significant hormonal
changes that could result in elevated thyroid stimulating hormone (TSH) and
suppressed thyroxin (T4) (Glinoer, 1999). Thus, maintaining balance between these
changes in iodine replete areas was found to be the key factor for normal progress of
pregnancy and resulted in a better outcome (de Benoist et al., 2003, Glinoer, 2004).

3
It was also reported that maternal thyroid disease during pregnancy has a negative
impact on foetal growth and offspring’s neuropsychological development
(Cranefield, 1962, Koibuchi and Chin, 2000, Delange, 2001, Patel et al., 2011).
Possible association between thyroid disease and iron deficiency anaemia has been
speculated (Hess et al., 2002, Zimmermann and Köhrle, 2002). A recent study
conducted at the LGH found that 20% of pregnant women in Northern-Tasmania had
iron deficiency anaemia (IDA) (Khalafallah et al., 2010). Since pregnancy increases
the demand for many nutrients including iodine and iron, a possible link between
iron deficiency anaemia and IDD during pregnancy was supported (Kramer, 2003).
It is agreed that goitre and hypothyroidism are most common in iodine deficient
areas (Glinoer, 1997, Lazarus and Okosieme, 2000, Glinoer, 2004, Gibson, 2006,
Vanderpump, 2010). However, clinicians only consider testing for thyroid
dysfunction in pregnancy if one or more of the following situations occur; symptoms
exist that suggest the condition; there is a family history of the disease; or there is the
presence of an associated medical condition (Abalovich et al., 2002, Reid et al.,
2010). Nearly a third of women were overlooked when applying a case-finding
approach rather than routine screening (Vaidya et al., 2007). Despite this, general
screening for thyroid function prior or during pregnancy is not a standard practice in
Australia generally and Tasmania in particular. Hence, the actual incidence of
thyroid diseases and its possible complications within the pregnant population of
Tasmania is not yet known. It is also worth mentioning that the study is specific for a
geographical region (Tasmania) that has a persistent history of iodine
deficiency(Hynes et al., 2004). Other studies conducted in different regions of

4
Australian were either among iodine sufficient population or among unknown iodine
status (Gilbert et al., 2008b, Schneuer et al., 2012, Ong et al., 2014).
1.2 Iodine and Iodine Deficiency Disorder (IDD)
1.2.1 Background
Iodine was discovered in the early 19th century by Bernard Courtois, a French
chemist (Richards, 1995). Davy, a British chemist and Gay-Lussac of France
however named the element “Iodine/Iod” in reference to a purple colour in Greek
language (Kelly, 1961, Richards, 1995). Hypothyroidism as a result of goitre is
believed to occur predominantly in regions of mountainous terrain where past
glaciations and heavy rainfall has resulted in the leaching of soil iodine
(Goldschmidt, 1952, Andersson et al., 2005, Zimmermann, 2010). Geographical
isolation and largely self-sufficient food production in a moderately to severe iodine
deficient region worsens the problem (Assey et al., 2006). Tasmania falls under such
a category and is known to be a typical endemic goitre area (Gibson, 2006, Richards
and Stewart, 2007).
Apart from natural causes of iodine deficiency, replacing iodine-based disinfectants
by contemporary non-iodine ones was suggested to be another reason for low-iodine
milk production in Tasmania (Richards and Stewart, 2007). The author also proposed
that introduction of fast food in late 20th century probably had a significant role in re-
appearance of IDD in both developed and developing countries (Richards, 1995,
Richards and Stewart, 2007). IDD has been recognised as a public health problem
affecting many communities globally (Andersson et al., 2012). Australia, including

5
Tasmania, was found to be mildly iodine deficient according to a nationwide study
(Li et al., 2006).
Internationally, iodine supplementation programs were first implemented in the
1920s by the United States of America (USA) and Switzerland (Marine and Kimball,
1920). However, this was not widely adopted until the World Health Organisation
(WHO) launched a Universal Salt Iodisation (USI) programme in the early 1990s
(Andersson et al., 2005). In Tasmania, it was only between the 1950s and 1960s
when iodine tablets were dispersed to people in order to contain goitre and prevent
IDD (Gibson, 2006).
While fortifying bread with iodised salt was recommended by the Tasmanian Iodine
Supplementation Program (TISP) launched in 2001, it was then legislated to be a
mandatory fortification in 2006 (Richards, 1995, Burgess et al., 2007, Richards and
Stewart, 2007). However, it is worth noting that both studies were conducted during
voluntary fortification period. Nevertheless, mild iodine deficiency in Tasmania was
found to be determined, concluded by Menzies Research Institute, Hobart, Tasmania
(Hynes et al., 2004).
In addition, a nine year follow up study of school-aged children who were born to
iodine deficient mothers revealed some cognitive disorder, i.e., reading difficulties
when compared to peers of similar age and school level (Hynes et al., 2013). This
indicates that earlier detection and prevention of iodine deficiency disorders in future
mothers can reduce risk of cognitive disorder in their children.

6
1.2.2 Iodine & iodine metabolism
Recognition of iodine’s importance was related to its essential role in the production
of thyroid hormones; thyroxin (T4) and triiodthyronin (T3). In the stomach and
duodenum, >90% of iodine in the form of iodide was found to be rapidly absorbed
(Taurog, 2000, Trumbo et al., 2001). While the half life of iodine was reported to be
10 hours in normal health and adequate nutritional conditions, it was found to be
reduced in case of iodine deficiency (Taurog, 2000).
Iodine uptake in the thyroid gland is dependent on its supply, with 10% of iodine
uptake enough in case of iodine sufficient supply and >80% of uptake could be
required in insufficient iodine supply (DeGroot et al., 1975). The sodium/iodide
symporter (NIS) system was found to be responsible for iodide transfer into the
thyroid (Eskandari et al., 1997).
In the colloid, the enzyme thyroid peroxidase was established to play a crucial role in
iodine coupling and the production of thyroid globulin (TG), T3 and T4 (Eskandari
et al., 1997, Taurog, 2000, Hall, 2010). Circulating T3 and T4, after reaching the
target organs they release iodine which enter the plasma iodine pool where it is taken
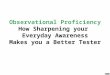
up again by the thyroid or excreted (90%) by the kidneys (Taurog, 2000), (Figure 1-
1).

7
Figure 1-1 Iodine metabolism and transport
At the basal membrane NIS regulate transfer of iodine from the circulation into the thyroid cell. The apical membrane is where the thyroid peroxidase enzyme helps the iodine to couple up with the thyroid globulin.

8
1.2.2.1 Iodine sources
Iodine is commonly available in seawater, seaweeds and seafood. It mainly exists in
the sea water in oxidised form, and in a lesser percentage it reaches the soil which is
again drained back to the sea by the effect of rain (Goldschmidt, 1952). Thus, crops
grown in these washed-off soils would be low in iodine concentration. Consequently,
human and animals consuming food grown in these iodine-poor soils are likely to
develop IDD (WHO, 2001). A study comparing iodine content in crops grown in
iodine-deficient soil and crops grown in iodine-sufficient soil, resulted in 10 μg/kg
and 1 mg/kg of dry weight of iodine, respectively (Assey et al., 2006). Iodine-
deficient soils are common in inland regions, mountainous areas, and places with
frequent flooding, but can also occur in coastal regions (Vitti et al., 2003, Andersson
et al., 2012).
Since consuming large amounts of seaweed was a normal diet for people living on
the coastal regions of Japan, remarkably high iodine intakes amounting to 50 to 80
mg/day have been reported in this population (Zimmermann, 2009). In the mid-
1990s in the United States, the median intake of iodine from food was estimated to
be 240 to 300μg/day for men and 190 to 210μg/day for women. Since salt iodisation
programs have been applied by most countries including Australia, bread has been
the major source for iodine. In addition to bread, milk was mentioned as well to be a
good source for iodine in the USA and Europe (Pearce et al., 2004, Haldimann et al.,
2005). Other publications reported that, using iodophors milk in cleaning milk cans
and cows teats increased the native iodine content of dairy products (Phillips, 1997,
Richards and Statham, 2007).

9
1.2.2.2 Iodine requirements
Definitions related to nutritional requirements were outlined by the Institute of
Medicine (IOM) of the USA (Trumbo et al., 2001). The estimated average
requirement (EAR) is the daily iodine intake that meets the requirement of half of the
healthy individuals in a particular life stage (Trumbo et al., 2001). The recommended
dietary allowance (RDA) however, was defined to be the average daily intake
sufficient to meet the iodine requirement of 97–98% of healthy individuals in a life
stage (Trumbo et al., 2001). The adequate intake (AI) was used if there was
insufficient scientific evidence to calculate an EAR (Trumbo et al., 2001).
Whilst these definitions were widely accepted in the US, the recommended nutrient
intake (RNI) was adopted by WHO (Zimmermann, 2009). RNI was defined as the
intake estimated to cover the needs of “nearly all” healthy individuals in the specified
life stage (Trumbo et al., 2001). It has been recommended for men, non-pregnant and
non-lactating women as the adequate daily iodine intake was 150 μg/d
(Zimmermann, 2009).
During pregnancy, increased production of maternal T4, retained iodine in foetal
thyroid and increased renal clearance, were thought to be the main reasons for
increased iodine demand (Glinoer, 1997). The latest and ongoing WHO’s
recommendation for daily iodine supplementation during pregnancy and lactating has
been reported to be 250 μg/day (Andersson et al., 2007). While iodine
supplementation for pregnant and breastfeeding women in Australia and the New
Zealand in 2006 was 220 μg/d and 270 μg/d respectively, the National Health and
Medical Research Council (NHMRC) instead recommends that 150 μg/day of iodine

10
supplementation was safe and effective for pregnant and breastfeeding women
(NHMRC, 2010). This relatively lower than WHO’s recommendation was further
explained by the NHMR; avoiding any possible foetal thyroid depression.
1.2.3 IDD
This phenomenon was identified globally and defined by the World Health
Organisation (WHO) as any illness related to a thyroid disorder that could be
prevented by dietary iodine supplementation (Zimmermann et al., 2000, Andersson
et al., 2007). While severe iodine deficiency in pregnancy can result in irreversible
brain damage to the foetus (cretinism), mild deficiency can lead to a decreased
intelligence quotient (IQ) in school aged children (Chan and Kilby, 2000, Koibuchi
and Chin, 2000, Delange, 2001, Burgess et al., 2007).
The magnitude of IDD is at a global scale, with approximately 1.5 billion people
affected (Hetzel, 1983, de Benoist et al., 2003, Andersson et al., 2005, Andersson et
al., 2012). Although iodine deficiency was found to have a high prevalence in
developing countries, about 600 million people in Europe were reported to suffer
from a mild-to-severe level of iodine deficiency (Vitti et al., 2003). Subsequently, a
safe, cost-effective and sustainable strategy was conducted using salt iodisation
method to ensure adequate iodine intake in all affected areas (Andersson et al., 2005,
Andersson et al., 2012).
The iodised salt program was adopted by most countries around the globe, with an
estimated 71% of the world’s population benefiting from this strategy (Andersson et
al., 2012). Using Urinary Iodine Excretion (UIE) levels, recommendations were

11
made by WHO/International Council for the Control of Iodine Deficiency Disorders
(ICCIDD): iodine replete, UIE ≥ 100 μg/L; mild iodine deficiency, UIE 50–99 μg/L;
moderate iodine deficiency, UIE 20–49 μg/L; severe iodine deficiency, UIE
< 20 μg/L) (Andersson et al., 2012). Although 24h UI is a better indicator, it is not
practical to be used when conducting large scale studies (World Health Organization,
2007).
During a period of voluntary iodine fortification in Australia, a cross-sectional study
involving 1709 school-aged children from 88 schools comprising almost equal
percentages of boys and girls, reported a borderline iodine deficiency with a median
UIE of 104 μg/L (Li et al., 2006). It was reported that children in South Australia,
NSW and Victorian were either border line or mildly iodine deficient, with median
UIE levels of 101 μg/L, 89 μg/L and 73.5 μg/L, respectively (Li et al., 2006).
Queensland and Western Australian children were found iodine sufficient with
median UIE levels at 136.5 μg/L and 142.5 μg/L, respectively.
The median urinary iodine concentration (UIC) in 285 pregnant women who were
enrolled prior to salt fortification with iodine and 517 enrolled after iodised salt use
in most of Tasmania’s bakeries showed 76 μg/L and 83,5 μg/L, respectively,
indicating a mild iodine deficiency according to the WHO classification (NHMRC,
2010, Burgess et al., 2007). A follow-up study was performed that evaluated the
mental development of school-aged children who were born to iodine deficient
mothers (UIC <150 μg/L) in the previous study (Hynes et al., 2013). The study
resulted in reductions of 10.0%, 7.6% and 5.7% in spelling, grammar and in English-
literacy, respectively, when compared with peers who were born to iodine sufficient

12
mothers (Hynes et al., 2004, Hynes et al., 2013). It was therefore suggested that even
mild iodine deficiency during pregnancy could have long-term adverse affects on
foetal cognitive functions, that had not been sufficiently were not compensated by
the iodine sufficiency strategy that commenced in the state in 2001 (Hynes et al.,
2013).
1.3 Thyroid Gland
The thyroid is one of the largest glands in the human body, regulates metabolism and
growth (Hall, 2010). It produces hormones; thyroxin, triiodthyronin and calcitonin.
Circulating in a very small amounts in the body, they have specific effects on other
organs and systems e.g. cardiovascular, neuropsychology, musculoskeletal and
sexual (Hall, 2010).
1.3.1 General anatomy and physiology
It is located on the front of the neck, hugging the thyroid cartilage and the trachea
from the level of fifth cervical vertebra (C5) to the first thoracic (T1), thus occupying
the front surface of the second to fourth tracheal rings. Butterfly, H and U are the
most common shapes of this gland, formed by two elongated side lobes and a small
lingual (isthmus) lobe that connects the lateral lobes together. The average weight of
the thyroid gland is 25-30g in adults, it is however may enlarge during pregnancy
and menstruation. Its blood supply comes from the superior and inferior thyroid
arteries and innervated by parasympathetic and sympathetic fibres from vagus nerves
and the sympathetic trunk. Biosynthesis of the thyroid hormones take place in the
thyroid functional unit which consists of a monolayer of epithelial cells that is filled

13
with thyro-globuline (colloid) (Marine and Kimball, 1920, Kopp, 2005, Braverman
and Cooper, 2012). For the production of thyroid hormones, Iodine in the form of
iodide (I-) is required, hence transported into this unit using NIS (Eskandari et al.,
1997, Hall, 2010). The thyroid, is responsible for production of a great number of
protein enzymes, structural protein, transport protein and other substances, which
increase general activity throughout the body (Bizhanova and Kopp, 2009).
They stimulate Carbohydrates and fat metabolism as well as increases utilisation of
vitamins (Hall, 2010). Thyroid hormones metabolic effect was demonstrated in an
animal experiments, number and size of mitochondria increased in response to
thyroid hormones ingestion, increases the rate of basic body metabolism up to 60-
100 percent (De La Vieja et al., 2000, Bizhanova and Kopp, 2009, Hall, 2010). The
thyroid hormones, are also responsible for brain maturation and neuropsychological
development (Chan and Kilby, 2000, Glinoer, 2004, de Escobar et al., 2004, Hall,
2010, Yassa et al., 2010). Maintaining thyroid hormones and its functions within
normal and regular secretory level, gained by a specific negative feed-back
mechanism within the hypothalamus-pituitary-thyroid axis (Glinoer, 2004, Hall,
2010).
Secretion of thyroid hormones T4 and T3 is directly stimulated by the TSH; TSH is
secreted from the anterior lobe of the pituitary gland and is stimulated by the
Thyrotropine releasing hormone (THR) in the hypothalamus, hence is called
hypothalamic-pituitary-thyroid axis (Chiamolera and Wondisford, 2009), (Figure 1-
2).

14
Figure 1-2 Mechanism of the thyroid hormones regulation.
Thyrotropin releasing hormone (TRH) in the hypothalamus is activated by the negative feedback of low thyroxin (T4) and triiodthyronin (T3) in the circulation. Secretion of TRH stimulates the anterior lobe of the pituitary gland to produce thyroid stimulating hormone (TSH). TSH stimulates the thyroid gland; synthesis and secretion of T4 and T3 hormones are then compensated.

15
1.3.2 Thyroid hormones and pregnancy
Although increased demand for energy, nutrients, minerals and vitamins is usually a
benign physiological feature of pregnancy, biochemical values of the thyroid
function can still be altered (Burrow, 1990, Glinoer, 1999, Glinoer, 2004). Pregnancy
has been described as a status where dramatic hormonal changes take place that
result in increased thyroxin binding globulin (TBG), an increase in urinary iodine
excretion, increased activity of the placenta, decreased TSH and increased human
chorionic gonadotropin (HCG) (Glinoer, 1999). This results in increased thyroid
hormones, metabolism and an increased demand for iodine (Glinoer, 2004, Yassa et
al., 2010). During the first and second trimesters, level of TBG and T4 increase
under the effect of increased levels of estrogens and HCG, respectively (Epstein et
al., 1994, Glinoer, 1999). Maintaining the balance between these changes and normal
progressing of the pregnancy is achievable in iodine sufficient area, difficult in
iodine insufficient areas (Glinoer, 2004).
1.3.2.1 Role of iodine and thyroid hormones in brain development
The relationship between the thyroid gland, severe iodine deficiency and
neurological manifestations in human (e.g. cretinism) was first established and
documented in the literature (Cranefield, 1962). During foetal development, the
thyroid gland was found to reach maturation at 11-12 weeks of gestational age
(Obregon et al., 2007). The presence of thyroid hormones in foetal neurological
tissues was evidenced by the detection of T4 and T3, it was suggested that T4 and T3
play a crucial role in growth and neuropsychological development during and after
gestation (Chan and Kilby, 2000, Koibuchi and Chin, 2000, Calvo et al., 2002,
Kester et al., 2004, Patel et al., 2011). It was also explained earlier that myelination

16
and neuronal/glial cell differentiation is regulated initially by thyroid hormones at
genes level (Bernal and Nunez, 1995).
1.4 Thyroid diseases and pregnancy
Goitre is one of the prominent sign of thyroid disease in iodine deplete regions
(Andersson et al., 2007, Zimmermann, 2010). While hypothyroidism, as result of
goitre is believed to be more common in iodine-poor regions, an autoimmune-origin
of thyroid diseases (e.g. Grave’s disease and Hashimoto thyroiditis) were found to be
the most common causes in iodine-replete areas (de Benoist et al., 2003, Andersson
et al., 2007, Vanderpump, 2010).
Prevalence of thyroid dysfunction can vary from as low as 0.1 % to as high as 15.5%
(Table 1-1). It was reported by some large-scale studies that the prevalence of
thyroid disease during pregnancy, identifying 0.3-0.5% of overt hypothyroidism
(OH) cases and 1.5-4% of subclinical hypothyroidism (SCH) (Allan et al., 2000,
Casey et al., 2005, Negro and Mestman, 2011). Iodine deficiency was found to play a
negative role in thyroid function, it was emphasised that a higher percentage of
disease to be anticipated more in iodine-deplete areas (Klein et al., 1991, Stagnaro-
Green et al., 2011). Thus, OH and SCH, are the two disorders most commonly
encountered thyroid disorders during pregnancy in iodine poor areas and
consequently believed to be associated with adverse effects on the development of
the foetus and on the course of the pregnancy (Stagnaro-Green et al., 2005).

17
Table 1-1 TSH upper normal value and prevalence of thyroid dysfunction
Source TSH Prevalence / comments
(Hollowell et al., 2002) 4.5 4.3% SCH, 0.3% OH
(Haddow et al., 2004) 1st trimester >5.2 2nd trimester >4.2
4% Hypothyroidism
(Casey et al., 2005) >97.5th percentile 2.5% SCH, 0.2% OH
(Vaidya et al., 2007) 4.2 1.6% SCH, 1% OH
(Marwaha et al., 2008) 4.2 14.2% SCH, 1.3% OH
(Gilbert et al., 2008a) 2.15 4.5% elevated TSH
(Blatt et al., 2012) Trimester specific 15.5% tested positive for gestational hypothyroidism
(Moreno-Reyes et al., 2013) 1st trimester 2.5-3 2nd trimester >3
7.2% (6.8% SCH, 0.4% OH)
(Altomare et al., 2013) 1st trimester 2.5-3 2nd trimester >3
12.3% had high TSH (hypothyroidism)
(Diéguez et al., 2016) 4.5 5.5% (1.9% OH, 3.6 %SCH)

18
As pregnancy has been reported to affect thyroid function, monitoring for thyroid
activity using certain laboratory parameters has been proposed (Glinoer, 1999,
Glinoer, 2004). Upon conception, hCG hormone increases which in turn stimulate
thyrocytes (TG) to induce a transient increase in FT4 levels, which is mirrored by a
lowering of TSH concentrations. Following this period, serum FT4 concentrations
decrease slightly (10–15% on average), and serum TSH values steadily return to
normal. In line with these variations, both FT4 and TSH reference intervals change
throughout pregnancy, depending on gestational age (Vermigllo et al., 1995, Glinoer,
2004). This is generally stabilised by the end of the second trimester when iodine
intake was adequate (Glinoer, 2004). Thus, trimester specific TSH reference was
highly recommended (Table 2-1). The table demonstrates variability in the intervals
from one population to another. Therefore, developing population sample-based
trimester-specific range for TSH is mandatory.
T3/T4 ratio is another parameter found to reflect thyroid stimulation during
pregnancy (Glinoer, 1999). The last parameter proposed for monitoring thyroid
behaviour during pregnancy was TG, it was reported to have tendency to elevate
more in the third trimester of pregnancy (Rasmussen et al., 1989, Glinoer, 1999).
Although measuring FT4 using liquid chromatography/tandem mass spectrometry
(LC/MS/MS) methods have been recommended, using trimester-specific TSH has
been advised to consider as well (Stagnaro-Green et al., 2011).
Thyroid diseases with an autoimmune association, is the most prevalent in iodine
sufficient regions (Moreno-Reyes et al., 2013). It was reported that 10-15% of iodine
sufficient population tested positive to thyroid peroxidase (TPO) antibodies (Glinoer

19
et al., 1994, Pop et al., 1995). The presence of TPO antibodies have been linked to
pregnancy complications, postpartum thyroid dysfunction and progression to a
symptomatic disease (Negro et al., 2011). Furthermore, the risk of spontaneous
abortion and preterm delivery were also increased in women with auto antibodies
(Glinoer et al., 1994). Evidence of complications related to positive thyroid
autoimmune status of pregnant women living in iodine sufficient conditions are far
greater than of negative TPO status. Nevertheless, testing for thyroid antibodies are
found to be of very little clinical help because a clear relationship between these
antibodies and recurrent pregnancy loss could not be established (Negro et al.,
2010b).

20
Table 1-2 Population-based trimester specific intervals for TSH
Trimestera
Reference First Second Third
1 (Haddow et al., 1999) 0.08-2.73 0.39-2.70 _
2 (Stricker et al., 2007) 0.09-2.83 0.20-2.79 0.31-2.90
3 (Panesar et al., 2001) 0.03-2.30 0.03-3.10 0.13-3.50
4 (Soldin et al., 2004) 0.24-2.99 0.46-2.95 0.43-2.78
5 (Bocos-Terraz et al., 2009) 0.03-2.65 0.12-2.64 0.23-3.56
6 (Marwaha et al., 2008) 0.60-5.00 0.43-5.78 0.74-5.70
7 (Blatt et al., 2012) 0.10 - 2.50 0.55 - 2.75 0.43 - 2.91
8 (Diéguez et al., 2016) 0.20- 4.50 _ _
(Gilbert et al., 2008a) 0.02–2.15 _ _
a TSH in mIU/L, with parenthetical data indicating 5th and 95th percentiles (1,3,6) or 2.5th and 97.5th percentiles (2,4,5,7,8)

21
1.4.1 IDD Complications in pregnancy
Maternal, foetal and neonatal complications of untreated thyroid diseases during
pregnancy have been well investigated (Cranefield, 1962, Davis et al., 1989, Millar
et al., 1994, Haddow et al., 1999, Allan et al., 2000, Glinoer, 2001, Abalovich et al.,
2002, Casey et al., 2005, Casey et al., 2006, Casey and Leveno, 2006, Negro et al.,
2011, Sarkar, 2012, Männistö et al., 2013). Although complications due to thyroid
dysfunction during pregnancy can widely be variable, some conditions such as
(gestational diabetes, gestational hypertension, miscarriage, preterm delivery and
foetal death) were frequent outcome (Table 3-1).
1.4.1.1 Obstetric complications
Untreated OH was demonstrated to show negative impact on pregnancy outcome as
well as foetal neuropsychological development (Abalovich et al., 2002, Haddow et
al., 1999). Risk of foetal loss was reported to be as high as 60% among pregnant
women with OH (Abalovich et al., 2002). It was also found that the risk for
gestational hypertension increases to 22% in pregnant women with OH compared to
those without (Leung et al., 1993). It was concluded that risk of foetal death was
found to be increased among a study population with combined OH and pregnancy
(Allan et al., 2000). Although association between GDM and hypothyroidism have
previously been rejected, later publication reported a positive relationship (Casey et
al., 2007, Cleary-Goldman et al., 2008, Korevaar et al., 2013).
Placental abruption and preterm delivery were demonstrated to be three times and 1.8
times, respectively more likely in women with SCH. Preterm deliveries (<32weeks)

22
had a three-fold incidence in subclinical hypothyroidism (Casey et al., 2005,
Stagnaro-Green et al., 2005). A recent study has shown that pregnant women with
SCH are at significant risk of developing gestational diabetes (Negro and Stagnaro-
Green, 2014). Also, the risk of spontaneous abortion and preterm delivery were
increased in women with auto antibodies (Glinoer et al., 1994, Glinoer, 2001).
1.4.1.2 Neonatal complications
Neonates also share risk of complications with maternal thyroid disease with the
birth weight of children born to mothers with OH found to be decreased (Idris et al.,
2005). Although guidelines for early diagnosis and management of overt
hypothyroidism in pregnancy has been well established, complications such as
congenital hypothyoiridism, neuropsychological development (IQ) deficit and foetal
death are still prevalent in some countries (Blazer et al., 2003, Chan and Kilby, 2000,
de Escobar et al., 2004).
It was suggested that untreated hypothyroidism and probable subclinical
hypothyroidism during pregnancy was associated with a risk of a poorer outcome
and a three-fold increased predisposition for learning difficulties (Haddow et al.,
1999). Nevertheless, a study conducted in the Netherlands failed to define any
association between thyroid status in early pregnancy and cognitive development in
offspring (Henrichs et al., 2010). Hypothyroxinemia detected during the first
trimester, irrespective to the increased TSH, associated with a higher risk of poor
neuropsychological development of the progeny (Morreale de Escobar et al., 2000).
In contrast, other studies could not find positive relationship between maternal

23
hypothyroxinemia and impairment of neonatal cognitive development (Oken et al.,
2009, Craig et al., 2012).
Further studies reported that neonatal sepsis, respiratory distress syndrome (RDS),
transient respiratory tachypnoea and apnoea were associated with maternal thyroid
disorders, either primary hypothyroidism or hyperthyroidism (Männistö et al., 2013).
More recently, smaller head circumference and lower brain weight were found being
linked to babies born to TPO positive mothers who were white/non-Hispanic (Wilson
et al., 2014).

24
Table 1-3 Variability of maternal and neonatal complications in association with thyroid dysfunction
Reference Type of thyroid dysfunction Maternal complications Neonatal complications (Toulis et al., 2014) Subclinical hypothyroidism
(SCH) Gestational diabetes (GD)
(Korevaar et al., 2013) SCH Isolated hypothroxinemia (IH)
Premature labour (PL) 2.5-fold increased risk of premature delivery, a 3.4-fold increased risk of spontaneous premature delivery, and a 3.6-fold increased risk of very premature delivery
(Mannisto et al., 2013) Subclinical hypothyroidism(SCH)
Increased risk for GD, Pre-eclampsia Preterm
Preterm babies, sepsis, ARDS
(Karakosta et al., 2012) SCH+Autoimmunity 4-fold increase risk for GD 3-fold increase risk for low birth wt.
(Tudela et al., 2012) SCH 3-fold in GD (Stagnaro-Green, 2011) Overt hypothyroidism(OH) Pre-eclampsia,gestational
hypertension(GHTN) and spontaneous abortion.
cretinism, foetal death
(van den Boogaard et al., 2011)
SCH Pre-eclampsia
(Su et al., 2011) OH SCH
-Increased fetal loss, low birth weight, and congenital circulation system malformations. -Foetal distress, preterm delivery, poor vision development, and

25
IH
neurodevelopment delay. -Foetal distress, small for gestational age, and musculoskeletal malformations.
(De Vivo et al., 2010) SCH Autoimmunity
Increased risk for miscarriage Increased risk for miscarriage
(Ashoor et al., 2010) SCH Increased risk for miscarriage (Negro et al., 2010a) SCH with TPOAB Increased risk for miscarriage (Li et al., 2010) SCH Impaired neuropsychological
development (Benhadi et al., 2009) SCH Foetal death (Vermiglio et al., 2004) IH with iodine deficiency Impaired neurosychological
development(attention deficit and hyperactivity disorder)
(Allan et al., 2000) SCH (TSH>6.0mIU/L) Foetal death (Leung et al., 1993) SCH
Isolated hypothyroxinemia(IH)
GHTN, pre-eclmpsia Preterm labour, GD
Macrosomia

26
1.5 Iron
Iron has been described as a component of metaloproteins that are essential for
biochemical activities; oxygen sensing and transport, electron transfer and catalysis
(Papanikolaou and Pantopoulos, 2005). In the human body iron content was reported
to vary between 3 and 5 grams, 70% of which found being utilised for heme and
hemoglobin synthesis (Ponka et al., 1998). The liver, spleen, bone marrow, muscles,
the kidneys and macrophages of the reticular-endothelial system are other organs
where iron is being utilised and stored (Bernát, 1983, Siah et al., 2006).
Deoxidising the alimentary non-heme (Fe3+) iron to heme (Fe2+) form, is an essential
process to facilitate iron absorption in the duodenum (Figure 1-3) (Pantopoulos,
2004). Whereas there no direct mechanism for iron excretion expressed in mammals,
the normal physiological balance of iron is maintained by dietary compensation for
the normal loss that occurs by desquamation of epithelial cells from the gut, skin, and
genitourinary tract (Bothwell et al., 1979).

27
Figure 1-3 Overview of iron transport and metabolism
(A) Iron transport across duodenal epithelial cells. Reductase of the deudenal cytochrom-b (Dcytb) change ferric iron into ferrous iron. The divalent metal transporter (DMT1) then transport Ferrous iron across the apical membrane of the mature enterocyte. Iron then exported to the circulation by the ferroportin. This step is coupled with reoxidation of ferrous to ferric iron by membrane-bound hephaestin. Plasma iron is immediately scavenged by transferrin (Tf). (B) Schematic representation of the Tf cycle. Plasma Tf binds to its cell surface receptor (TfR) and the complex is internalized by endocytosis. Acidification of the endosome results in the release of ferric iron from Tf and reduction and subsequent transport of ferrous iron across the endosomal membrane by DMT1. The pathway is completed by recycling of the apoTf-TfR complex to the cell surface and release of apoTf. Intracellular iron is utilized for the synthesis of iron-containing proteins and the excess is stored into ferritin. A fraction of chelatable iron defined as “labile iron pool” (LIP) determines the cellular iron status (Pantopoulos, 2004)

28
1.5.1 Iron requirement
During pregnancy the foetus stores approximately 250 mg of iron that is drawn on
during breastfeeding (Fomon, 1993). While daily recommended requirement for
absorbed iron is 0.55 mg per day, breast milk supplies only 0.15 mg of absorbed iron
per day (Fomon, 1993). During child growth 0.5 mg of iron per day is absorbed in
excess of body losses; adequate amounts of iron during growth typically results in a
70-kg man accumulating about 4 g of body iron (Fomon, 1993). Due to menstrual
blood loss women generally have less iron stores than men and requirement for iron
in a healthy childbearing-aged population estimated to be approximately 1.5-2 g per
day (Bothwell et al., 1979, Andrews, 1999).
Although iron bioavailability (absorption) is affected by diet, pregnant women during
the second trimester are still recommended to take >50mg/d regardless of the type of
diet. Despite the fact that there is little evidence to support detrimental maternal or
foetal outcomes, advocating for universal iron supplementation of pregnant women
has been carried out in the industrialised countries (Zimmermann and Hurrell, 2007).
A prenatal iron supplementation in iron-replete, non-anaemic low-income pregnant
women in the USA was found to decrease incidence of preterm delivery and increase
birth weight (Cogswell et al., 2003, Siega-Riz et al., 2006).
1.5.2 Iron Deficiency Anaemia (IDA) during pregnancy
Chlorosis or “the green sickness” was the term used in the medieval age describing
people with pallor (Guggenheim, 1995, Kiple and Ornelas, 2001). Approximately
24.8% of the world’s population is affected by anaemia, 30-40% of the cases were

29
pregnant women and preschool children (Benoist et al., 2008, McLean et al., 2009).
It has been reported that 75% of anaemia in pregnancy has been identified to be of
iron deficiency type (Benoist et al., 2008, McLean et al., 2009, Horowitz et al.,
2013). It was also reported that heavy menstruation, high parity, intrauterine devices
and vegetarian diet were strong contributing factors on the rise of IDA (Zimmermann
and Hurrell, 2007). In Northern Tasmania 20% of pregnant women have been
identified to be suffering from IDA (Khalafallah et al., 2010).
Pregnancy has previously been explained to be a condition when foetal growth and
maternal blood volume expansion lead to increased nutritional demand including
iron (Hallberg, 1995). It was established that iron requirement during pregnancy was
equal to that contained in about 4 units of blood (about 1 kg), most of which is
needed in the last two trimesters (Bothwell et al., 1979).
From a dietary aspect IDA was highly expected when iron requirements are greater
than energy needs and that would be the case in infants and young children,
adolescents, heavily menstruating women and pregnant women (Earl and Wotecki,
1993, Zimmermann and Hurrell, 2007). It was found that women with multiple
pregnancies were susceptible to IDA as well as their offspring when there were no
enough intervals between pregnancies for the body to re-establish it’s iron stores
(Kilbride et al., 1999).
1.5.3 Possible complications of IDA in pregnancy
Although there is not conclusive evidence regarding the effect of maternal IDA on
infants, cognitive and motor development in school aged children have been shown

30
to be affected (Scholl and Hediger, 1994, Sachdev et al., 2005). IDA was found to
increase the risk of preterm labour, low birth weight and infant mortality particularly
during the first and second trimesters of pregnancy (Brabin et al., 2001).
It was suggested that children who have IDA in infancy are at risk of delayed
developments when compared to those with normal iron status (Lozoff et al., 1991).
In contrast, adverse effects of iron deficiency and/or the absence of iron in the
developing brain on neuromotor development were not conclusive (Beard, 2001).
IDA in third trimester and its effect on child’s mental development were studied in
China, resulted in a significant lower mental development index (Chang et al.,
2013). Susceptibility to/and duration of infections in children, mainly of the upper
respiratory tract was reported to be aggravated by IDA (de Silva et al., 2003).
1.5.4 IDA and thyroid disease
The association between thyroid diseases and anaemia was first reported in the late
19th century when post-thyroidectomised patient developed anaemia, although the
reasons for this were unclear (BOMFORD, 1938). It was reported that 53/202
(26.2%) of patients pre-diagnosed with hypothyroidism had anaemia (Horton et al.,
1976). Furthermore, 60/118 (50.8%) of patients who were studied more closely, were
found to have iron level at the lower margin of the reference interval (<12 µmol/L)
and 42 (35.5%) had a low serum concentration of iron (Horton et al., 1976).
Using haemoglobin only to evaluate IDA was labeled as non-sensitive and non-
specific (Zimmermann, 2008). Although serum ferritin was reported to be a better
parameter in reflecting iron store, it found to be unreliable in the presence of active

31
inflammatory process. Iron saturation transferrin and erythrocyte zinc protoporphyn
were used to determine iron-deficient erythropoiesis, but lacking accurate
diferentiating acute IDA from anaemia of chronic illness was its back-
draw(Zimmermann, 2008). Hence, a combination of serum ferritin and serum
transferring receptor was suggested for evaluating iron store and tissue iron
deficiency, respectively (Zimmermann, 2008) .
IDA has also been found to have a negative impact on maternal thyroid function,
which is compounded in areas where there are nutritional deficiencies (Zimmermann
et al., 2000). In regions of endemic goitre, thyroid response to iodine
supplementation was impaired in children with IDA compared to iron sufficient
children (Zimmermann et al., 2000). In another study, the efficacy of administered
iodised salt was improved in children suffering from goitre, by managing IDA (Hess
et al., 2002). This is supported by another study demonstrating that combined
supplementation with Fe and Iodine had even better effect on thyroid function than
iodine supplementation alone (Eftekhari et al., 2006).
1.6 Screening for IDD in pregnancy
Regardless of the growing evidence of thyroid disorders and its consequences on
pregnancy, foetal growth and neuropsychological development of children, clinicians
have been reported to still prefer a case finding approach rather than generalised
screening for thyroid diseases (Glinoer, 2001, Casey et al., 2005, Casey and Leveno,
2006, Casey et al., 2006, Vaidya et al., 2007). It has been suggested that 20-50% of
pregnant women with suspected thyroid disease would be missed when selectively
approached for thyroid screening (Vaidya et al., 2007, Horacek et al., 2010).

32
A recommendation in favour of generalised screening for thyroid diseases during
pregnancy was made on a joint statement by the American Thyroid Association
(ATA), the American Association of Clinical Endocrinologists (AACE) and the
Endocrine Society (ES) in 2005 (Gharib et al., 2005). In a subsequent meeting the
previous statement has been changed, universal screening of thyroid diseases was not
as effective as a selective screening approach (Stagnaro-Green et al., 2011, Garber et
al., 2012).
In contrast, some European countries have introduced universal screening for thyroid
disease during pregnancy, an approach that has been widely accepted, particularly in
Spain and Belgium (Vila et al., 2014). After a thorough review of the serious impact
of undiagnosed and therefore untreated OH on the mother and foetus, and
neurocognitive development of the unborn child, universal screening has been
strongly suggested (Stagnaro-Green, 2012).
General screening has been found to be cost effective not only when compared with
no screening, but also when compared with screening of high-risk women (Thung et
al., 2009, Dosiou et al., 2012). Although, the latest conjoint statement made by the
American thyroid association don’t recommend a general screening of the thyroid
diseases in pregnancy, disagreement and consequences of late diagnosis and/or
untreated cases have been emphasised by others (Allan et al., 2000, Abalovich et al.,
2002, Gharib et al., 2005, Vaidya et al., 2007, Stagnaro-Green et al., 2011).

33
1.6.1 Screening tools and interpretation of results
1.6.1.1 Screening for maternal thyroid function
Testing for TSH, FT4, FT3 and TPO antibodies are basically required in order to
assess thyroid function. Most biochemical tests are performed using sophisticated
automated devices in the biochemistry sections of medical laboratories.
Immunoassay is the most common method for measuring FT4 and FT3, reliability of
which during pregnancy has been reported to be questionable (Lee et al., 2009).
Chemiluminescent (immunoassay-based) can be refered to substances capable of
yielding higher specific activities when used as direct reagent labels in this context,
and thus provide a basis for the development of ‘ultra-sensitive’, non-competitive,
immunoassay methodologies (Ekins et al., 1989). Enzymes catalysing
chemiluminescent reactions or yielding fluorescent reaction products can likewise be
used as labels yielding high effective specific activities and hence enhanced assay
sensitivities (Ekins et al., 1989).
It has been reported that the serum of pregnant women is characterized by higher
level of TBG and nonesterified fatty acids and by lower concentrations of albumin
compared to the serum of non-pregnant women (Stagnaro-Green et al., 2011). One of
the most sophisticated devices is the dialysate or ultrafiltrate online solid phase
extraction–liquid chromatography/tandem mass spectrometry (LC/MS/MS), it has
been highly recommended for accurate measurement of FT4 (Yue et al., 2008,
Stagnaro-Green et al., 2011). In addition, it was demonstrated that LCMSMS
enhanced diagnostic capabilities by affording the specificity, precision, and limiting
of quantification necessary for the reliable measurement of thyroid hormones. These
methods were found to be especially important in states of disease and during

34
pregnancy when protein binding is a factor that interferes with other methods for
thyroid hormone analysis (Soldin and Soldin, 2011, Hoofnagle and Roth, 2013).
Regardless previous recommendation it has been reported by other authors that
immunoassay performs well, show low results when expected and report high results
when excess of FT4 occurs (Anckaert et al., 2010). Unavailability of LC/MS/MS
prompts each laboratory individually estimated trimester-specific references for TSH
has been recommended to follow instead (Stagnaro-Green et al., 2011). In case
laboratories don’t have their own trimester-specific reference for TSH, the following
reference ranges have been recommended to follow; first trimester, 0.1–2.5 mIU/L;
second trimester, 0.2–3.0 mIU/L; third trimester, 0.3–3.0 mIU/L (Stagnaro-Green et
al., 2011). It is worth mentioning that LGH pathology (where study samples were
processed) reports their reference range for TSH and FT4 in the general population
as (0.47-4.70 mU/L) and (10.0-28.2 pmol/L), respectively.
1.6.1.2 Screening for iodine status
As more than 90% of ingested iodine was found to be excreted by kidneys, urinary
iodine (UI) was thought to be the best source for iodine level evaluation (Vought and
London, 1967). While UI 24 hour urine was described to be a better indicator, UI can
be measured in spot urine specimens from a representative sample of the target group
and expressed as the median, in µg/L (World Health Organization, 2007). For
national school-based surveys of iodine nutrition, the median UI from a
representative sample of spot urine collections from approximately 1200 children (30
sampling clusters of 40 children each) can be used to classify a population’s iodine
status, according to WHO (World Health Organization, 2007).

35
Although the median UI does not provide direct information on thyroid function, a
low value suggests that a population is at higher risk of developing thyroid disorders
(Zimmermann, 2009). It was argued that median UI’s variability from day to day
made it an easy subject for misinterpretation (Andersen et al., 2008). It was further
explained that assuming subjects as iodine deficient with a spot UI of less than 100
μg/L is not acceptable (Zimmermann, 2009). Since 24 hour urine collection was not
practical for large scale screening also to avoid day-to-day variability in spot UI, use
of age- and sex-adjusted (iodine:creatinine) ratio in adults was thought to be a better
alternative (Knudsen et al., 2000). Using the following formula; urinary iodine
(μg/L) × 0.0235 × body weight (kg) = daily iodine intake, a median UI of 100 μg/L
corresponds roughly to an average daily intake of 150 μg.
Currently, UI estimation varies according to the level of technology it is associated
with. Thus, Urinary Iodine in this study was measured directly by ICPMS following
dilution in an ammonium EDTA based diluent using rhodium as an internal standard
(Agilent 7500ce Inductively Coupled Plasma Mass Spectrometer).This analysis was
developed at the Biochemistry Department at the Royal Prince Alfred Hospital,
Sydney. Inductively coupled plasma mass spectroscopy (ICP-MS) is an analytical
technique that is capable of performing quantitative multi-element analysis at trace
concentrations of these elements. An ICP-MS is capable of measuring concentrations
to a level of ng / L of the analyte. Nevertheless, most modern techniques for testing
UI are originally based on the old basic principles (the Sandell-Kolthof reaction)
(World Health Organization, 2007, World Health Organization, 2013). Using the
median urinary iodine concentration, criteria was developed by the WHO to assess

36
iodine intake in target groups. According to results of median UI (μg/L) for pregnant
women, iodine intake was evaluated; UI < 50 μg/L would indicate to insufficient
iodine intake (World Health Organization, 2013). While 150-249 μg/L would
describe adequate iodine intake, 500 μg/L and more would be evaluated as excessive
level (World Health Organization, 2013). Lactating women were categorised
differently bearing in mind iodine excretion in milk as well as in urine; median UI <
100 μg/L would be indicating insufficient intake and a 100 μg/L and more would be
of adequate intake (World Health Organization, 2013).
1.7 Cord blood and neonatal thyroid assessment
Umbilical cord blood has long been endeavoured for evaluating neonatal thyroid
status (Walfish et al., 1979, Henry et al., 2000). Maternal and neonatal
hypothyroidism has a negative impact on the foetal neuropsychological development
(Rovet et al., 1987, Haddow et al., 1999, Idris et al., 2005). Although a well
correlation was reported between TSH results of the umbilical cord blood and the
neonatal venous blood, the latter have been recommended (Walfish et al., 1979,
Jacob and Peters, 2015). Since confirmatory venous blood TSH was required for
elevated cord blood TSH results, recalling the patients back demonstrated to be a
non-practical approach (Walfish et al., 1979, Wu et al., 1999).

37
1.8 Aims and Hypothesis
Aims:
1. To biochemically, determine the rate of thyroid function alterations within a
limited group of obstetric population in northern Tasmania.
2. To determine whether altered thyroid was associated with clinical
complication to the mothers and their babies during pregnancy and delivery.
3. To determine whether iron deficiency anaemia and iodine deficiency are
associated with low thyroid status.
4. To find out whether a general screening of thyroid diseases for pregnant
women, identify more cases than the current routine selective screening.
5. To determine if cord TSH can be used as a screening tool for neonatal
hypothyroidism.
Hypotheses:
1. The number of pregnant women with thyroid disorder can be more significant
if biochemically screened either prior conception or at early pregnancy.
2. Thyroid function disorder during pregnancy has a negative impact on
maternal and foetal wellbeing.
3. Iodine deficiency and low ferritin levels are possible predictors for the
thyroid dysfunction.
4. General biochemical screening for thyroid function is a better approach in
identifying thyroid diseases during pregnancy and preventing associated
complications.
5. Cord blood TSH, a non-invasive tool for neonatal hypothyroidism screening.

38
2 MATERIALS AND METHODS

39
2.1 Study Design
2.1.1 Ethics
The study was approved by the Tasmanian Health and Medical Human Research
Ethics Committee (H119759) and was conducted between 16/04/2012 and
15/04/2014 at the Launceston General Hospital (LGH), Tasmania, Australia.
Informed consent was obtained by all participants.
2.1.2 Recruitment
Since all pregnant women went through pathology for gestational diabetes screening,
thinking of the pathology as a capturing point was foreseeable. Hence, potential
participants were invited to take part in the study while they were waiting at the
pathology for glucose tolerance test (GTT). Upon their interest and prior to consent
for participation, all women were individually informed about the project and
possible outcomes. Pregnant women aged 18 years and above with absence of any
known history of thyroid disease were included in the study (Figure 2-1). The
researcher documented personal information, demographic data, medical history and
medication profiles. Participants with abnormal laboratory results (high TSH levels)
were contacted, the condition explained and referred onto the endocrinologist. It is
worth mentioning that recruitment and sample collection was happening
simultaneously.

40
Figure 2-1 Study design and Recruitment flow
First stage, at pathology reception where invitation and information sheet were handed out to all pregnant women presented for GTT. Second stage, inclusion/exclusion criteria were applied to the interested women and informed consents were obtained. Third stage, a questionnaire was filled by the participant and blood nurses were notified to collect the samples.

41
Data capturing sheet was derived and modified from Abalovich et al 2002 and their
recommended approach for case finding. The data capturing sheet was instituted in
two parts; the first part recorded physical parameters (weight and height) and visible
signs of goitre (enlarged thyroid gland, exophthalmia and pretibial oedema) as
assessed by the study investigator. Gestational age, expected date of delivery, and
type of conception were also documented.
Using thyroid function testing markers (TSH, FT4 and FT3) was set as a screening
tool (predictors) for the study group. Hence, this will divide the study population into
normal, low thyroid status (TSH>2.5mU/L) and isolated low thyroxin
(FT4<8.9pmol/L). Likewise, cord blood samples were also collected as part of the
study from the participants’ babies and were tested for TSH, FT4, FT3 and anti-TPO
antibodies. In addition to that, full blood count (FBC) and iron studies (IS) were part
of the investigations. In addition, urine samples were collected from the participants
for measuring urinary iodine (UI) level.
The second part was the questionnaire form, which was purposely designed to obtain
specific clinical information to identify women who would have been candidates for
thyroid testing based on history and symptoms alone. It includes past and present
medical history, obstetrics & gynaecological history, medications, dietary history and
symptoms of hyperthyroidism or hypothyroidism. All abnormal findings were
documented by the investigator and discussed with the principal investigator for
further investigations as required. This may include referral for thyroid ultrasound or
to an endocrinologist if clinically required. Participant’s GP’s were notified with any
abnormality and action plan.

42
Furthermore, records of maternal, foetal and neonatal complications were collected
in order to determine the incidence rate in each group of thyroid status. Clinical
outcomes in the study cohort are divided into two groups; antenatal (maternal/foetal)
complications and neonatal wellbeing parameters.
Ante-partum complications are defined by the presence of the following parameters:
oligohydromnious, polyhydromnious, gestational diabetes mellitus (GDM),
gestational hypertension (GHTN) and pre-eclampsia, infection, placenta previa,
threatened premature labour (TPL), ante-partum haemorrhage (APH), intra-uterine
foetal growth restriction (IUFGR) and organ anomalies, macrosomia, biliary disease
and abdominal or pelvic surgery. Intra-partum complications are defined by the
presence of the following: cord prolapsed, prolonged labour, instrumental delivery,
intrapartum haemorrhage (IPH), pyrexia and hypertension (HTN). Post-partum
complications are defined by the presence of postpartum haemorrhage (PPH) and
wound infection. Neonatal parameters include Apgar scores, head circumference,
resuscitation and nursery admission.
Once the questionnaire was completed, participants were given a copy of the signed
consent with two pathology forms (Antenatal) for blood and urine samples.
Antenatal pathology forms requested collection of blood and testing for TSH, free
thyroxin (FT4), free triiodthronine (FT3), and anti-TPO antibodies as well as urine
sample for iodine level. IS and a FBC were also performed to test for the presence of
concomitant IDA. A cord-blood pathology form was attached to a copy of the
consent of each participant and placed in the participant’s medical record.

43
Participants’ medical records were also marked with a pink-coloured label in order to
help the labour ward nursing staff identify the participants easily.
2.2 Sample collection and handling
Fasting blood (10 ml) and urine (15 ml) specimens were collected from consented
participants during daytime working hours. Blood samples were collected into
different tubes according to the requested test. Specimens for FBC were collected in
purple top BD Ethylenediaminetetraacetic acid (EDTA)-Vacutainer (K2E) tubes
(Becton Dickenson and company, Franklin Lakes, NJ, US). Blood for TSH, FT4,
FT3, anti-TPO antibodies and IS were collected in gold top BD Vacutainer (SST II)
tubes. Similarly, cord blood samples for TSH, FT4, FT3, and anti TPO-antibodies
were collected in gold top BD Vacutainer (SST II) tubes. Urine samples for iodine
measurement were collected in plain sterile containers.
Blood samples for FBC were tested within 30 minutes of collection, while samples
for TSH, FT4, FT3 and anti-TPO antibodies were centrifuged at 4000 x g for five
minutes and one aliquot of serum were forwarded to the Biochemistry laboratory for
routine testing for TSH, FT4, FT3, while another 2-3 aliquots are stored at -700 C.
Urine samples were divided equally between two conical tubes and paired with anti-
TPO antibody samples, then stored at -700C. Approximately one hundred frozen
samples were collected and transported to the Royal Prince Alfred (RPA) Hospital,
Pathology, Sydney for analysis. Cool boxes with dry ice were used to keep the
sample temperatures at -700C during interstate transportation.

44
2.3 Tests principles
Blood samples were analysed by Sysmex XE-5000 (Sysmex Corporation - Global -
Kobe, Japan). Test principle in this device is based on the fluorescence flow
cytometry method. Three parameters in FBC were considered; Haemoglobin (Hb),
Haematocrit (Hct), Mean Corpuscular Volume (MCV). Concomitantly, samples for
TSH, FT3, FT4 and Ferritin were assayed using The VITROS Immunodiagnostic
System (VITROS ECI, Ortho-Clinical Diagnostics, Inc. Rochester NY, U.S.A.). All
assays on the VITROS Analyzer employ an enhanced chemiluminescence detection
reaction.
Serum iron level and transferrin were tested using an Architect C8000 (Abbott
Laboratories. Abbott Park, Illinois, U.S.A.). Iron was determined by using the direct
colorimetric method without deproteinisation in the human serum. Transferrin
measurement on the other hand was based on an immunoturbidimetric procedure,
which measures increasing sample turbidity caused by the formation of insoluble
immune complexes.
Antenatal and cord blood serum aliquots for anti-TPO antibodies along with urine
iodine samples were processed at the RPA, Sydney. Anti-TPO antibodies were
measured using an IMMULITE 2000 systems analyzer (SEIMENS). It is a solid-
phase, enzyme-labelled, chemiluminescent sequential immunometric assay.
Iodine in urine was measured directly by Inductively Coupled Plasma Mass
Spectroscopy (ICP-MS) after a dilution in an ammonium EDTA based diluents in a
quantitative application using rhodium as an internal standard. ICP-MS is an

45
analytical technique that is capable of performing quantitative multi-element analysis
at trace concentrations of these elements. An ICP-MS is capable of measuring
concentrations to a level of ng / L of the analyte.
2.4 Data collection, entry and storage
Data was collected using three sources of information. Firstly, questionnaire-derived
information (the modified data capturing sheet) was used to express approximately
one hundred parameters. A mixed of Qualitative and quantitative data was coded
from this source. The second source was the LGH Pathology test results for FBC, IS,
TSH, FT4 and FT3. Thirteen test parameters were obtained for each participant from
this source. The third data source was the RPA, Sydney where results for urine
iodine, urine creatinine and anti-TPO antibodies were collected. Data were entered
on a daily basis into a password protected electronic data sheet and saved in the
hospital O-drive. Original paper documents (consents, questionnaire and results)
were sorted into numeric order according to participant’s trial identification number,
each in a separate folder and stored in locked drawers.
2.5 Data analysis
2.5.1 Methods of statistics
The rate of complication events in the mother and baby associated with various
predictor variables was estimated as the incidence rate ratio (IRR; 95% confidence
intervals; P-values) using multivariate Poisson regression. The covariates were
selected using backward stepwise regression (P-value for removal = 0.22; P-value for
entry = 0.12). An incidence rate ratio (IRR) of 1.00 indicates that the rate in the

46
group being compared with the comparator group (e.g. low thyroids with normal
ones) is of no difference between the two groups; an IRR greater than 1.00 means the
group has a higher rate than the comparator group; an IRR less than 1.00 means that
the rate is lower than in the comparator group.
Variables for possible selection include for pre- and intra-natal complications: low
thyroid status, BMI, first baby, history of prematurity or PET, gestation at
delivery<37weeks, APH, hypertension/PET in this pregnancy, oligo- or poly-
hydramnios, sex of baby, GDM, infection, placenta previa, TPL, IUGR, macrosomia,
abdo/pelvic surgery, FBS, MCV, Hb. For post-natal complications the same list was
used, plus prolonged labour, intra-partum haemorrhage and mode of delivery.
Where the complications were measured as a continuous variable (i.e. APGAR
scores at 1minute and 5 minutes or head circumference), regression coefficients
(coef; 95% confidence intervals; P-values) were estimated using multivariate general
linear modelling: covariates were selected using backward stepwise regression. The
covariates shown were each categorical variables, with the coefficient being the
estimated difference found when the covariate is present. Mean and difference (95%
confidence intervals; P-values) estimated by general linear modelling, adjusting for
the same covariates for each complication.
Where continuous covariates were evaluated for association with outcomes, z-scores
of variables were used ({variable-meanvariable}/SDvariable), using either natural value or
log10 transformation. Z-scores have two advantages when used in multivariate
regression analyses: 1) the regression constant is corrected to the mean of all of the

47
continuous variables (rather than to an abstract zero for all of the included variables,
i.e. it remains in the middle of the data rather than at the edge of the raw data range);
and 2) each variable is corrected to a single unit of value (units of 1 standard
deviation), so that all variable coefficients have the same scale, and the magnitude of
the association of each variable can be compared directly, rather than having to do
complex mental arithmetic to correct for different units of measurement and value
ranges.
In order to determine whether any symptoms or combination of symptoms elicited at
the initial antenatal clinic visit could predict the presence of low thyroid status, the
association between the results from the thyroid symptoms questionnaire and the
subsequent determination of women with low thyroid status was estimated using
multivariate Poisson regression, with variables for inclusion in the final model
selected by backward stepwise regression. All the questions were included unless
there was at least one positive result in both the low and normal thyroid status
women (any zero results make interpretation of the regression coefficients extremely
problematical). Pre-pregnancy tremor, weight loss, carpal tunnel syndrome and
antenatal hair loss were excluded for this reason. The regression coefficients for the
final model were then used to calculate for each woman a combined risk score (see
Equation 1 in results section).
The optimum threshold for identification of low thyroid status was then selected,
using receiver operating curve (ROC) analysis, based on judgement of the estimated
sensitivity and specificity. The statistical significance of the estimated ROC area
(whether the observations may have arisen by chance) was determined by

48
comparison of the ROC area with a normally distributed randomly-generated set of
numbers with the same mean and standard deviation as the risk score. All analyses
were performed using Stata MP2 versions 13.2 (StataCorp, College Station, Texas
USA).

49
3 RESULTS

50
3.1 Description of the study population
During the study period, approximately a total of 2200 pregnant women of Northern
Tasmania attended the pathology for gestational diabetes screening, mainly were
referred from the Queen Victoria antenatal clinic, LGH. The target population were
invited, 636 (28.9%) responded and consented to take part in the study. The study
also includes data collected from 625 babies born to the mothers recruited to this
study as well as investigation of their cord blood. Out of 636 participants, 609
(95.7%) were successfully screened for thyroid status. Gestational age at presentation
and recruitment was around 26 weeks (median 26.4; inter-quartile range 25 to 27.6;
range 12.6 to 37.7) with no difference in recruitment age distribution between the
normal and low thyroid status groups (P > 0.90), (Figure 3-1).

51
Figure 3-1 Study populations with response rate and recruitment Response rate was 29% of 2200 pregnant women approached with invitation.
Biochemical thyroid screening was processed to 95.7% of the participants and
67% of their babies cord blood. Low thyroid status was found in 3.4% of the
pregnant cohort.

52
Using thyroid function testing markers (TSH, FT4 and FT3) as a screening tool, the
study population was divided into three main categories; low thyroid status (TSH >
3mU/L and TSH >2.5mU/L), isolated low free thyroxin level (FT4 < 8.9pmol/L) and
normal (comparator group). Among consented participants, 397 (63.1%) are
multiparous (have previously been pregnant) and 232 (36.88%) are nulliparous (first
time pregnant) with a median age of 29 years. The median age of gestation at
recruitment was 26 weeks and gestational age at delivery was 39.4 weeks (Figure 3-
2).

53
Figure 3-2 Distribution of gestational age in study population Most participants were recruited when they were between 24 and 28
weeks of gestational age.

54
The study data also shows that 612 (96.2%) reported being conceived naturally. The
breakdown of ethnic background was 503 (79%), 27 (4.24%), 11 (1.7%) and 4
(0.7%) representing Caucasian, Asian, indigenous Australian and African,
respectively. No ethnic background was provided for 87 (13.7%) participants.
Data of sub-population of 625 babies’ shows that 615 (97.9%) were born alive with
male to female ratio of 1:1.04 (49% and 51% respectively). The total number of
clinically observed complications for this study group is 269; 9 events (3.3%) are
distributed in the group of low thyroid status, 135 (50.2%) events are distributed
among the group category with low FT4 and 125 (46.5%) events of complications
are distributed variably in the group of cohorts who have normal thyroid function.
3.2 Study outcomes
3.2.1 Incidence of thyroid abnormalities in the study population
Thyroid function screening results for its 609 pregnant women (Table 3.1) shows 22
(3.4%) with low thyroid function (9 with TSH > 3 mU/L and 13 with TSH 2.5-3
mU/L), 75 (12.3%) with free thyroxin level (FT4) < 8.9 pmol/L and 272 (44%) with
results within the normal ranges for thyroid function. Table 3-1 shows the rate of all
recorded complications in each of these groups.
Additionally, results of thyroid peroxidase (TPO) antibodies showed 39/585(6.3%)
TPO-positive and 546/585 (93.3%) were negative. The average of TSH results was
1.2 mU/L in the TPO+ve group, not much different from 1.3 mU/L in the TPO-ve
group.

55
Table 3-1 Ante-, intra- or post-natal complications in groups defined by thyroid status
Total events
P-value1
Normal (N=272)
FT4 (8.9-15) (N=240)
FT4(<8.9) (N=75)
TSH2(2.5-3.0)
(N=13)
TSH2(>3.0) (N=9)
n (%) n (%) n (%) n (%) n (%) Antepartum complications Oligohydroamnios 14 >0.90 7 (2.6%) 4 (1.7%) 3 (4.0%) 0 (0.0%) 0 (0.0%) Polyhydromnios 5 >0.90 3 (1.1%) 0 (0.0%) 2 (2.7%) 0 (0.0%) 0 (0.0%) GDM 49 0.70 23 (8.5%) 15 (6.3%) 9 (12.0%) 1 (7.7%) 1 (11.1%) GHT/PET 38 0.39 22 (8.1%) 10 (4.2%) 6 (8.0%) 0 (0.0%) 0 (0.0%) Infection 7 >0.90 3 (1.1%) 3 (1.3%) 1 (1.3%) 0 (0.0%) 0 (0.0%) Placenta previa 5 0.17 1 (0.4%) 2 (0.8%) 1 (1.3%) 1 (7.7%) 0 (0.0%) TPL 35 >0.90 18 (6.6%) 14 (5.8%) 2 (2.7%) 0 (0.0%) 1 (11.1%) APH 9 >0.90 2 (0.7%) 7 (2.9%) 0 (0.0%) 0 (0.0%) 0 (0.0%) IUGR/organ malformation
16 >0.90 7 (2.6%) 8 (3.3%) 1 (1.3%) 0 (0.0%) 0 (0.0%)
Macrosomia 8 >0.90 2 (0.7%) 4 (1.7%) 2 (2.7%) 0 (0.0%) 0 (0.0%) Biliary disease 6 0.20 4 (1.5%) 1 (0.4%) 0 (0.0%) 0 (0.0%) 1 (11.1%) Surgery 4 >0.90 3 (1.1%) 1 (0.4%) 0 (0.0%) 0 (0.0%) 0 (0.0%) Intrapartum complications Cord prolapse 0 0.036 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) Prolonged labour 8 0 (0.0%) 5 (2.1%) 2 (2.7%) 0 (0.0%) 1 (11.1%) Forceps 7 0.010 3 (1.1%) 4 (1.7%) 0 (0.0%) 0 (0.0%) 0 (0.0%) IPH 4 0.74 1 (0.4%) 1 (0.4%) 1 (1.3%) 1 (7.7%) 0 (0.0%) Pyrexia 5 0.17 3 (1.1%) 0 (0.0%) 2 (2.7%) 0 (0.0%) 0 (0.0%) HTN 9 >0.90 5 (1.8%) 3 (1.3%) 1 (1.3%) 0 (0.0%) 0 (0.0%) Postpartum complications PPH 35 0.66 15 (5.5%) 13 (5.4%) 5 (6.7%) 1 (7.7%) 1 (11.1%) Wound infection 5 0.62 3 (1.1%) 1 (0.4%) 1 (1.3%) 0 (0.0%) 0 (0.0%)

56
1 P-value estimated using Fischer’s exact test 2 Estimate of proportion of cases in sample with elevated TSH results: 3.4% (95%CI 2.1% to 5.2%)
Abbreviations: GDM Gestational diabetes; GHT/PET Gestational hypertension/Pre-eclamptic toxaemia; TPL Threatened premature labour; APH Ante-partum haemorrhage; IUGR Intra-uterine growth retardation; Surgery Abdominal or pelvic surgery; Forceps Any instrumental delivery (e.g. forceps or Ventouse); IPH Intrapartum haemorrhage; HTN Hypertension; PPH Postpartum haemorrhage

57
3.2.2 Association of maternal and foetal complications rate with thyroid status
Table 3-1 shows the total number of all complications during three consecutive
periods of pregnancy/labour and distribution rate of these complications among
different thyroid status groups. Results in Table 3-2 summarise rates and associations
of complications in the low thyroid status group. Because of the relatively low
number in the result group (22 with low thyroid status), as well as the limited events
of complications, it was difficult to clearly identify any small to moderate increase in
their rate of incidence.
Results of the statistical analysis presented in tables 3-1 and 3-2 don’t show any
significant association between ante-natal complications and low thyroid status.
Although GDM results in Table 3-2 affecting 2 out of 22 of the same group (IRR
1.69; 95% CI 0.55-5.25; P= 0.36) doesn’t reflect a possible association with low
thyroid status, covariates including BMI, log.fasting blood sugar and history of PET
demonstrate significant relationship. While the former two show predictive values
with (IRR 2.20; 95%CI 1.73 to 2.81; P < 0.001) and (IRR 1.25; 95%CI 1.00 to 1.55;
P= 0.46), respectively, the latter shows protective values (IRR 0.63; 95%CI 0.41 to
0.96; P= 0.032).
Other associations between individual complications and different covariates are
demonstrated in table 3-2; macrosomia is assumed to be affected more with other
factors than with low thyroid status. Log.fasting blood sugar, BMI, maternal age,
gravid>2 and gestational diabetes, show positive association with a great incidence
increase in the last two with (IRR 13.4; 95%CI 2.34 to 76.6; P= 0.004) and (IRR
8.28; 95%CI 2.44 to 28.0; P= 0.001), respectively. While a positive association is

58
found between PET/Gestational hypertension and (log.haemoglobin, BMI and
maternal age), history of PET, MCV and gravida >2 are negatively associated. Also,
threatened premature labour is assumed predictable by increased history of
prematurity (IRR 3.69; 95%CI 1.81 to 7.51; P < 0.001) and assumed protected by
less history of PET (IRR 0.61; 95%CI 0.42 to 0.91; P= 0.014).
Although results couldn’t clearly identify any significant association of GDM with
low thyroid, it was positively associated with ante-partum haemorrhage (IRR13.9;
95%CI 4.79 to 213; P < 0.001). Table 3-3 reflects a possible association between
prolonged labour (PL) and low thyroid status (IRR 3.31; 95% CI 1.13 to 9.69; P=
0.029). While there are no other intra-natal complications associated with low
thyroid status, maternal age and log.ferritin were found positively associated with
prolonged labour with 90% and 53% of incidence increase, respectively.

59
Table 3-2 Association of individual antenatal complications and low thyroid status
Gestational diabetes Present (%) Absent IRR 95%CI P-value Low Thyroid 2 (9.1%) 20 1.69 (0.55 to 5.25) 0.36 Normal 47 (8.0%) 540 1.00 Covariates2 Log. Fasting Blood Sugar3 2.20 (1.73 to 2.81) <0.001 History of PET 0.63 (0.41 to 0.96) 0.032 BMI3 1.25 (1.00 to 1.55) 0.046 Macrosomia Present (%) Absent IRR 95%CI P-value Low Thyroid 0 (0.0%) 22 0.00 (0.00 to 0.00) 0.00 Normal 8 (1.4%) 579 1.00 Covariates2 MCV3 1.71 (0.94 to 3.10) 0.08 Log. Fasting Blood Sugar3 2.12 (1.30 to 3.47) 0.003 History of PET 4.73 (0.70 to 32.1) 0.11 BMI3 2.12 (1.40 to 3.21) <0.001 Maternal age3 1.92 (1.14 to 3.22) 0.013 Gravida 1 1.00 Gravida>2 13.4 (2.34 to 76.6) 0.004 Gestational diabetes 8.28 (2.44 to 28.0) 0.001 Infection Present (%) Absent IRR 95%CI P-value Low Thyroid 0 (0.0%) 22 0.00 (0.00 to 0.00) <0.001 Normal 7 (1.2%) 580 1.00 Covariates2 History of Prematurity 3.42 (0.62 to 18.8) 0.16 Log. Ferritin3 1.40 (1.06 to 1.85) 0.017 IUGR/Organ malformation Present (%) Absent IRR 95%CI P-value Low Thyroid 0 (0.0%) 22 0.00 (0.00 to 0.00) <0.001 Normal 16 (2.7%) 571 1.00 Covariates2

60
BMI3 0.69 (0.40 to 1.21) 0.19 PET / Gestational hypertension Present (%) Absent IRR 95%CI P-value Low Thyroid 0 (0.0%) 22 0.00 (0.00 to 0.00) <0.001 Normal 38 (6.5%) 549 1.00 Covariates2 Log. Haemoglobin3 1.44 (1.10 to 1.88) 0.008 MCV3 0.70 (0.54 to 0.90) 0.005 Gravida 2 0.51 (0.26 to 1.00) 0.05 Gravida>2 0.30 (0.14 to 0.66) 0.003 History of Prematurity 1.90 (0.91 to 3.97) 0.09 History of PET 0.30 (0.17 to 0.52) <0.001 BMI3 1.59 (1.24 to 2.03) <0.001 Maternal age3 1.41 (1.07 to 1.85) 0.013 Threatened premature labour Present (%) Absent IRR 95%CI P-value Low Thyroid 1 (4.5%) 21 0.58 (0.14 to 2.44) 0.46 Normal 34 (5.8%) 553 1.00 Covariates2 MCV3 1.20 (0.90 to 1.60) 0.21 Log. Ferritin3 1.18 (0.93 to 1.49) 0.17 History of Prematurity 3.69 (1.81 to 7.51) <0.001 History of PET 2.72 (0.68 to 10.9) 0.16 Maternal age3 0.61 (0.42 to 0.91) 0.014 Gravida 2 2.14 (0.96 to 4.77) 0.06 Gravida>2 1.88 (0.71 to 4.95) 0.20 Antepartum haemorrhage Present (%) Absent IRR 95%CI P-value Low Thyroid 0 (0.0%) 22 0.00 (0.00 to 0.00) <0.001 Normal 9 (1.5%) 578 1.00 Covariates2 Log. Fasting Blood Sugar3 0.45 (0.23 to 0.87) 0.02 History of Prematurity Large (Large to Large) <0.001 BMI3 0.31 (0.11 to 0.89) 0.03

61
Maternal age3 1.64 (0.99 to 2.71) 0.05 Gravida 2 10.7 (0.84 to 135) 0.07 Gravida>2 5.15 (0.57 to 46.8) 0.15 Gestational diabetes 31.9 (4.79 to 213) <0.001
1 Low thyroid status defined as TSH>2.5 2 Incidence rate ratio (IRR; 95% confidence intervals; P-values) estimated using multivariate Poisson regression: covariates were selected using backward stepwise regression, retained when P<0.22) 3 Continuous covariates used z-scores of variables ({variable-meanvariable}/SDvariable), using either natural value or log10 transformation

62
Table 3-3 Association of individual intra-natal complications and low thyroid status1
Prolonged labour Present (%) Absent IRR2 95%CI P-value Low Thyroid 1 (4.8%) 21 3.31 (1.13 to 9.69) 0.029 Normal 7 (1.2%) 580 1.00 Covariates2 Log. Ferritin3 1.53 (1.08 to 2.19) 0.018 Maternal age3 1.90 (1.04 to 3.47) 0.036
1 Low thyroid status defined as TSH>2.5 2 Incidence rate ratio (IRR; 95% confidence intervals; P-values) estimated using multivariate Poisson regression: covariates were selected
using backward stepwise regression, retained when P<0.22) 3 Continuous covariates used z-scores of variables ({variable-meanvariable}/SDvariable) , using either natural value or log10 transformation

63
Despite the fact that symptoms of thyroid disease are non-specific, the predictive
association between possible symptoms of thyroid disease at clinic visit and the
discovery of low thyroid function biochemically was also investigated, Table 3-4.
Palpitation (pre-pregnancy) was positively associated with low thyroid status as well
as with normal thyroid function; 5 (22.7%), 73 (12.6%), respectively (IRR 2.78; 95%
CI 1.00 to 7.70; P= 0.05). Dizziness (pre-pregnancy) also shows association with low
thyroid group 10 (45%) and 189 (32%) in the normal group (IRR 2.15; 95% CI 0.88
to 5.23; P= 0.09). there were no other statistically significant associations.
A combined risk score for low thyroid status was created from the coefficients of this
analysis using Equation 1 (the coefficient values are the natural logs of the IRRs
from Table 3-4):
𝑅𝑅𝑅𝑅𝑅𝑅𝑅𝑅 𝑅𝑅𝑠𝑠𝑠𝑠𝑠𝑠𝑠𝑠 = −2.8676 + (𝑃𝑃𝑃𝑃𝑃𝑃𝑃𝑃𝑅𝑅𝑃𝑃𝑃𝑃 ∗ 1.0215) + (𝐷𝐷𝑅𝑅𝐷𝐷𝐷𝐷𝐷𝐷𝑃𝑃𝑃𝑃 ∗ 0.7647)
+ (𝐷𝐷𝐷𝐷𝑅𝑅𝑃𝑃𝐷𝐷𝑠𝑠𝐷𝐷 ∗ −0.492) + (𝐼𝐼𝑠𝑠𝑠𝑠𝑅𝑅𝐼𝐼𝑃𝑃𝐼𝐼𝑃𝑃𝑠𝑠𝐷𝐷𝑠𝑠𝐷𝐷 ∗ −1.3638)
+ (𝐷𝐷𝑅𝑅𝑃𝑃𝑠𝑠𝑠𝑠ℎ𝑠𝑠𝑠𝑠𝑃𝑃𝐷𝐷𝑠𝑠𝐷𝐷 ∗ −0.7612)
This risk score had a range of values as shown in Figure 3-3. A threshold for
prediction of the presence of low thyroid status was investigated using receiver
operating characteristic (ROC) analysis, which suggested an optimum threshold
value of -3.25 and above for this risk score. Comparison of the ROC area with the
random null hypothesis showed a ROC area of 0.744 (95%CI 0.636 to 0.852;
Chi2=8.05; P=0.005). Using this value (-3.25), 15 of 22 (sensitivity or true positive
68.2%; 95%CI 45.1% to 86.1%) patients with low thyroid status were identified as
possible cases whilst 164 of 580 (1-specificity or false positive 28.3%; 95%CI 24.6%
to 32.1%) patients with normal thyroid status were identified as possible cases (IRR
5.15; 95%CI 2.13 to 12.4; P < 0.001).

64
However, relatively large numbers of patients with low and normal thyroid status had
risk scores close to the threshold of -3.25, and minor changes to the threshold chosen
appeared to produce large alterations in the sensitivity and specificity estimates for
the risk score.

65
Table 3-4 The predictive association between symptoms of possible thyroid disease at clinic visit and the discovery of low thyroid function1
Low thyroid Normal thyroid Variable N (% of 22) N (% of 580) IRR2 95%CI P-value Variables included in prediction model Palpitations PP 5 (22.7%) 73 (12.6%) 2.78 (1.00 to 7.70) 0.05 Dizzy PP 10 (45.5%) 189 (32.6%) 2.15 (0.88 to 5.23) 0.09 Irritable Now 3 (13.6%) 183 (31.6%) 0.26 (0.08 to 0.84) 0.024 Dyspnoea Now 9 (40.9%) 328 (56.6%) 0.59 (0.26 to 1.31) 0.19 Diarrhoea Now 9 (40.9%) 348 (60.0%) 0.47 (0.21 to 1.05) 0.06
Variables not included in model: Each IRR is variable effect when combined with the above model Tired PP 6 (27.3%) 125 (21.6%) 1.42 (0.49 to 4.16) 0.52 Tired Now 13 (59.1%) 404 (69.7%) 0.98 (0.42 to 2.27) >0.90 Constipation PP 2 (9.1%) 31 (5.3%) 1.26 (0.33 to 4.75) 0.74 Constipation Now 8 (36.4%) 194 (33.4%) 1.00 (0.44 to 2.26) 0.99 Heat intolerance PP 3 (13.6%) 72 (12.4%) 1.22 (0.36 to 4.14) 0.75 Heat intolerance Now 11 (50.0%) 256 (44.1%) 1.35 (0.62 to 2.93) 0.45 Cold intolerance PP 8 (36.4%) 197 (34.0%) 1.05 (0.46 to 2.41) 0.90 Cold intolerance Now 3 (13.6%) 135 (23.3%) 0.56 (0.17 to 1.87) 0.35 Insomnia PP 4 (18.2%) 135 (23.3%) 0.75 (0.25 to 2.25) 0.60 Insomnia Now 8 (36.4%) 221 (38.1%) 0.99 (0.40 to 2.47) >0.90 Hair loss PP 1 (4.5%) 68 (11.7%) 0.31 (0.04 to 2.48) 0.27 Leg cramps PP 3 (13.6%) 80 (13.8%) 0.83 (0.23 to 2.97) 0.78 Leg cramps Now 12 (54.5%) 295 (50.9%) 1.32 (0.55 to 3.16) 0.54 Carpal tunnel syndrome Now 3 (13.6%) 80 (13.8%) 1.21 (0.33 to 4.37) 0.77 Palpitations Now 6 (27.3%) 172 (29.7%) 0.67 (0.29 to 1.56) 0.35

66
Arrhythmias PP 2 (9.1%) 46 (7.9%) 0.89 (0.21 to 3.77) 0.88 Arrhythmias Now 2 (9.1%) 53 (9.1%) 0.93 (0.24 to 3.70) 0.92 Dyspnoea PP 2 (9.1%) 55 (9.5%) 0.89 (0.17 to 4.66) 0.89 Irritable PP3 5 (22.7%) 135 (23.3%) 2.47 (0.94 to 6.50) 0.07 Nausea & vomiting PP 2 (9.1%) 16 (2.8%) 1.93 (0.47 to 8.01) 0.36 Nausea & vomiting Now 10 (45.5%) 273 (47.1%) 1.11 (0.48 to 2.52) 0.81 Diarrhoea PP 13 (59.1%) 400 (69.0%) 1.58 (0.55 to 4.48) 0.39 Weight gain PP 1 (4.5%) 54 (9.3%) 0.59 (0.08 to 4.19) 0.60 Weight gain Now 2 (9.1%) 44 (7.6%) 1.32 (0.34 to 5.16) 0.69 Weight loss Now 1 (4.5%) 22 (3.8%) 0.82 (0.08 to 8.37) 0.87 Depression PP 7 (31.8%) 211 (36.4%) 0.97 (0.38 to 2.49) >0.90 Depression Now 3 (13.6%) 80 (13.8%) 1.44 (0.41 to 5.12) 0.57 Tremor Now 1 (4.5%) 38 (6.6%) 0.62 (0.08 to 4.83) 0.65 Headache PP 13 (59.1%) 272 (46.9%) 1.61 (0.67 to 3.88) 0.29 Headache Now 10 (45.5%) 313 (54.0%) 0.86 (0.37 to 2.03) 0.73 Dizzy Now 12 (54.5%) 310 (53.4%) 1.00 (0.37 to 2.66) >0.90
1 Low thyroid function defined as TSH<2.5. 2 Association between predictive variables and low thyroid function, expressed as incidence rate ratio (IRR; 95% confidence intervals; P-values),
estimated by Poisson regression; variables to be included in the final model were selected by backward stepwise regression from the list of variables shown in the table (PP=symptoms present pre-pregnancy; Now= symptoms present at the clinic visit).
3 The variable Irritable PP was excluded from the final model: the prevalence in the two groups was similar, and the apparent possible association (IRR 2.47; P=0.07) was judged to be a statistical quirk. Inclusion of the variable in ROC analysis made little difference to the final results. Abbreviations: PP (pre-pregnancy), Now (during pregnancy)

67
Figure 3-3 Distribution of predictive risk score in patients with low or normal thyroid status Relatively large numbers of patients with low and normal thyroid status had risk scores close to the threshold of -3.25, and minor changes to the threshold chosen appeared to produce large alterations in the sensitivity and specificity estimates for the risk score.

68
3.2.3 Association of rates of neonatal complications with thyroid status
Apgar scores, head circumference, resuscitation and nursery admission were the
parameters defining outcomes of neonates born to mothers with different thyroid
status. Mean Apgar scores at 1 minute of 8.69 (SD 1.08; 95% CI -0.11 to 0.82; P=
0.14) and at 5 minutes value of 9.39 (SD 1.08; 95% CI -0.22 to 0.43; P= 0.52) in the
low thyroid group are similar to the normal group (Table 3-5). Similarly, newborns’
head circumference in table 3-6 show results with a mean value of 32.3 (SD 1.41;
95% CI -0.60 to 0.58; P > 0.90) among babies born to mothers with low thyroid, as
well as the normal ones. These values do not demonstrate any association between
babies head circumference and the thyroid status of the mothers. Likewise, the
requirement for resuscitation and nursery admission to the babies (Tables 3-7, and 3-
8) do not show an association with their mothers’ thyroid condition.
Apart from the statistically insignificant association between the requirement of
resuscitations and low thyroid status, other predictors show positive association
(table 3-8) including delivery < 37 weeks, IUGR, IPH and placenta previa. Nursery
admission also was associated positively with other predictors such as delivery < 37
weeks, GHT/PET, GDM, infection, IUGR and LSCS.

69
Table 3-5 Apgar scores at 1 and 5 minutes born to mothers with low or normal thyroid status
n<8 (%) n 8+ Mean Apgar
(SD) Coef.2 95%CI P-value
Apgar at 1 minute Low Thyroid1 3 (13.6%) 19 8.69 (1.08) 0.35 (-0.11 to 0.82) 0.14 Normal 98 (16.7%) 489 8.34 (2.23) Covariates2 Delivery<37weeks -0.56 (-1.11 to 0.00) 0.050 Male baby -0.21 (-0.49 to 0.07) 0.14 IPH -1.21 (-2.17 to -0.25) 0.014 Apgar at 5 minutes Low Thyroid1 1 (4.5%) 21 9.39 (1.08) 0.11 (-0.22 to 0.43) 0.52 Normal 31 (5.3%) 556 9.28 (2.23) Covariates Delivery<37weeks -0.66 (-1.14 to -0.18) 0.007 Male baby -0.25 (-0.47 to -0.04) 0.019 IPH -0.37 (-0.95 to 0.21) 0.21 LSCS 0.24 (0.03 to 0.44) 0.023
1 Low thyroid status defined as TSH>2.5; numbers shown are those with Apgar scores < 8 or 8-10 2 Regression coefficient (the estimated difference found when the covariate is present )(coef.; 95% confidence intervals; P-values) estimated
using multivariate general linear modelling: covariates were selected (low thyroid status, BMI, first baby, history of prematurity or PET, gestation at delivery<37weeks, APH, hypertension/PET in this pregnancy, oligo- or poly-hydramnios, sex of baby, GDM, infection, placenta previa, TPL, IUGR, macrosomia, abdo/pelvic surgery, FBS, MCV, Hb) using backward stepwise regression, retained when P<0.22); the covariates shown were each categorical variables

70
Table 3-6 Head circumference of babies born to low thyroid status mothers or normal mothers
Mean (SD) Coef.2 95%CI P-value Low Thyroid1 32.3 (1.41) -0.01 (-0.60 to 0.58) >0.90 Normal 32.3 (1.69) Covariates BMI3 0.28 (0.15 to 0.40) <0.001 APH -1.68 (-2.54 to -0.81) <0.001 Oligohydroamnios 0.72 (-0.11 to 1.55) 0.09 Male baby 0.34 (0.10 to 0.58) 0.006 GDM -0.47 (-0.98 to 0.04) 0.07 Infection -1.08 (-1.93 to -0.23) 0.013 Macrosomia 1.89 (0.91 to 2.86) <0.001 Abdo/pelvic surgery -1.89 (-3.20 to -0.58) 0.005 Delivery<37weeks 2.24 (1.59 to 2.90) <0.001
1 Low thyroid status defined as TSH>2.5; numbers shown are those with Apgar scores < 8 or 8-10 2 Regression coefficient (coef.; 95% confidence intervals; P-values) estimated using multivariate general linear modelling: covariates
were selected (low thyroid status, BMI, first baby, history of prematurity or PET, gestation at delivery<37weeks, APH, hypertension/PET in this pregnancy, oligo- or poly-hydramnios, sex of baby, GDM, infection, placenta previa, TPL, IUGR, macrosomia, abdo/pelvic surgery, FBS, MCV, Hb) using backward stepwise regression, retained when P<0.22); the covariates shown were each categorical variables, with the coefficient being the estimated difference found when the covariate is present
3 Continuous covariates used z-scores of variables ({variable-meanvariable}/SDvariable), using either natural value or log10 transformation Abbreviations: APH Antepartum haemorrhage; GDM Gestational diabetes

71
Table 3-7 Requirement for resuscitation of babies born to low thyroid status mothers or normal mothers
Required (%) None IRR2 95%CI P-value Low Thyroid1 3 (13.6%) 19 0.78 (0.31 to 1.94) 0.59 Normal 95 (16.2%) 492 1.00 Covariates BMI3 1.13 (0.95 to 1.35) 0.16 Placenta Previa 6.26 (3.38 to 11.60) <0.001 GHT/PET 1.69 (0.99 to 2.88) 0.05 TPL 1.50 (0.93 to 2.43) 0.10 IUGR 2.36 (1.17 to 4.73) 0.016 Prolonged labour 2.08 (0.67 to 6.43) 0.21 IPH 2.32 (1.50 to 3.60) <0.001 Gravida 1 1.44 (1.00 to 2.07) 0.05 Delivery<37weeks 2.69 (1.81 to 3.98) <0.001
1 Low thyroid status defined as TSH>2.5 2 Incidence rate ratio (IRR; 95% confidence intervals; P-values) estimated using multivariate Poisson regression: covariates
were selected using backward stepwise regression, retained when P<0.22) 3 Continuous covariates used z-scores of variables ({variable-meanvariable}/SDvariable), using either natural value or log10 transformation Abbreviations: GHT/PET Gestational hypertension/Pre-eclamptic toxaemia; TPL Threatened premature labour; IUGR
Intra-uterine growth retardation; IPH Intrapartum haemorrhage

72
Table 3-8 Requirement for nursery admission of babies born to low thyroid status mothers or normal mothers
Nursery (%) None IRR2 95%CI P-value Low Thyroid1 1 (4.5%) 21 0.38 (0.12 to 1.24) 0.11 Normal 58 (9.9%) 529 1.00 Covariates BMI3 1.04 (0.78 to 1.38) 0.81 History of Prematurity 0.94 (0.54 to 1.65) 0.83 History of PET 1.99 (0.90 to 4.36) 0.09 GHT/PET 3.71 (1.78 to 7.71) <0.001 GDM 2.00 (1.18 to 3.38) 0.010 Infection 3.50 (1.14 to 10.8) 0.029 Placenta previa 3.24 (1.56 to 6.73) 0.002 TPL 1.84 (1.04 to 3.25) 0.035 IUGR/organ 3.69 (1.87 to 7.25) <0.001 Surgery 3.23 (1.16 to 9.04) 0.025 MCV3 1.74 (1.31 to 2.31) <0.001 Delivery<37weeks 6.51 (4.08 to 10.4) <0.001 LSCS 2.04 (1.31 to 3.18) 0.002
1 Low thyroid status defined as TSH>2.5 2 Incidence rate ratio (IRR; 95% confidence intervals; P-values) estimated using multivariate Poisson regression: covariates were
selected using backward stepwise regression, retained when P<0.22) 3 Continuous covariates used z-scores of variables ({variable-meanvariable}/SDvariable), using either natural value or log10 transformation
Abbreviations: GHT/PET Gestational hypertension/Pre-eclamptic toxaemia; GDM Gestational diabetes; TPL Threatened premature labour; IUGR Intra-uterine growth retardation; IPH Intrapartum haemorrhage; LSCS Lower segment Caesarean section

73
3.3 Other considerations
3.3.1 Association between low thyroid status and iron deficiency anaemia
Ferritn level (body iron reserve) in the study cohort was used to define Iron
Deficiency Anaemia. Results show that 193 pregnant women out of 590 (32.7%)
have iron store level below 10mg/l. Although these results do not demonstrate
association between ferritin level and thyroid status, data in (Table 3-9) clearly
define the presence of macrocytic anaemia in 5 out of 22 participants whose TSH
screening revealed low thyroid status.
3.3.2 Examination of surveillance of thyroid function using urinary iodine
Urinary Iodine is another proposed predictor in this study. We were able to
successfully screen 587 participants, all under similar conditions (time and place).
Calculation of the median urinary iodine concentration resulted in 117 µg/L.
However, an adequate iodine intake for pregnant women is best achieved when
median UIC is between 150-249 µg/L levels according to the latest recommendation
by WHO (World Health Organization, 2013). Thus, the result of 117µg/L still
reflects inadequate iodine intake for our pregnant women. Furthermore, 27/241
(11.2%) iodine deficient participants developed isolated hypothyroxinemia during
pregnancy. Additionally, results of median UIC was correlated with results of urine
creatinine of the same cohort. Although r (592) =0.44 reflects almost a large positive
effect, relevant p-value of (p=3.1) however indicates statistically a non-significant
correlation.

74
In order to find a possible association between (UIC and TSH) and (UIC and FT4),
correlation and regression formulas were used. Data analysis revealed very little
effect with no statistical significance r (588) = 0.017, p=0.67 and r (588) = 0.022,
p=0.55 for (UIC and TSH) and (UIC and FT4), respectively.
3.3.3 Study results-based reference group
TSH results (irrespective to TPO status) in the study group have been re-calculated,
they fall between the range of 0.16 mU/L (95% CI 0.75, 0.64) and 2.64 mU/L (95%
CI 1.93, 3.34).
Similarly, results for FT4 of the study cohort have also been re-calculated for the
group reference range, LL =7.10 pmol/L (95% CI 5.36, 8.83) and UL =14.02pmol/L
(95% CI 12.28, 15.75).
Data derived from TPOAB results in this study has however been calculated. Out of
585 of total participants, 546 (93.3%) showed negative results for TPO antibodies.
Nevertheless, their TSH results range between 0.15mU/L (95% CI 0.84, 0.53) and
2.6mU/L (95% CI 1.9, 3.3).
TPO antibodies were tested positive only in 39/585 participants (6.6%). However,
their TSH results are distributed between 0.04mU/L (95% CI 0.8, 0.76) and
3.05mU/L (95% CI 2.27, 3.82).
Calculation of cutoff values for TSH according to TPO status revealed almost
0.5mU/L difference in favor of TPO positive group where only two of TSH results
showed above 3.05mU/L and similar number of participants has UIC < 117ug/L
without any identifiable association between them. However, because of the small
number of positive TPO results, we cannot draw a valid conclusion without making
unsubstantiated assumptions.

75
Table 3-9 Association of low thyroid status1 with various forms of anaemia, including microcytic (iron-deficiency) anaemia
Group2 N Group total
% Group3
% Total3
Mean ferritin (SD)
IRR4 95%CI P-value5
No anaemia 9 256 3.5% 1.5% 18.8 (18.7) 1.00 Normocytic anaemia 5 175 2.9% 0.8% 32.2 (105.0) 0.81 (0.28 to 2.39) >0.90 Microcytic anaemia 4 134 3.0% 0.7% 8.3 (5.5) 0.85 (0.27 to 2.71) 0.78 Macrocytic anaemia 4 25 16.0% 0.7% 31.1 (43.5) 4.55 (1.51 to 13.74) 0.022
1 Low thyroid status defined as TSH>2.5. 2 Women were classified as having: 1) No anaemia (Hb≥120); 2) Normocytic anaemia (Hb<120, MCV 85-96); 3) Microcytic
anaemia (Hb<120, MCV <85 or Ferritin <10); 4) Macrocytic anaemia (Hb<120, MCV >96). 3 Percentages were calculated as % of each group, and % of total (N=590) women. 4 Likelihood of occurrence of low thyroid status was estimated as incidence rate ratio (IRR; 95% confidence intervals; P-values)
using Poisson regression with no covariates. 5 P-values were adjusted for multiple comparisons using the Holm method.

76
3.3.4 Cord blood TSH
Cord blood samples of 402/615 (65%) babies were collected and the reasons for low
percentage in cord blood collection were; either due to insufficient samples or simply
forgotten during labour chaos. Cord TSH results in table 3.10 (Mean 8.11; 95% CI -
2.74 to 0.4; P= 0.008) of 121 babies born by operative lower segment Caesareans
section (LSCS), demonstrate relatively lower TSH levels compared to results of
babies born by instrumental support or those who were born normally.
Table 3-10 reflects results of babies born to participants with bleeding complications
(APH/IPH), show lower estimates compared to participants without bleeding (Mean
(SD) 4.91(2.16); 95% CI -5.48 to -2.48; P < 0.001). Similarly, the same table shows
that cord TSH results of babies born to women with previous history of pregnancy
are slightly lower compared to those who were born to first time pregnant
participants.

77
Table 3-10 Association between predictor variables and levels of cord TSH1
N Mean (SD) 2 Mean Δ2 95%CI P-value
Normal thyroid 387 9.27 (5.92) 0.00 Low thyroid 15 9.81 (6.66) 0.45 (-2.62 to 3.53) 0.77
Normal vaginal delivery 222 9.73 (6.22) 0.00 Instrumental delivery 59 10.07 (6.89) -0.38 (-2.35 to 1.58) 0.70 LSCS4 121 8.11 (4.67) -1.57 (-2.74 to -0.41) 0.008 No history 367 9.21 (5.98) 0.00 History of prematurity 35 10.17 (5.60) 1.53 (-0.39 to 3.45) 0.12 No haemorrhage 392 9.40 (5.97) 0.00 APH or IPH 10 4.91 (2.16) -3.98 (-5.48 to -2.48) <0.001 Normal labour 396 9.33 (5.96) 0.00 Prolonged labour 6 6.74 (3.75) -2.09 (-5.14 to 0.96) 0.18
Primigravida 145 10.43 (6.72) 0.00 Multigravida 257 8.65 (5.36) -1.92 (-3.23 to -0.62) 0.004
Log10 Hb (reg. coef3) 402 2.07 (0.03) 0.53 (0.08 to 0.99) 0.022
1 Cord TSH measurements were collected in 402 patients 2 The mean (standard deviation) and mean difference between presence or absence of predictor variables was estimated using
general linear modelling (95% confidence intervals; P-values). Predictor variables to be included in the model were selected using backwards stepwise regression (P-value for removal = 0.22; P-value for entry = 0.12), with low thyroid status as a forced entry variable. For the categorical variables, the base comparator variable is assigned a mean difference of 0.
3 For haemoglobin, log10 transformation was used due to non-normal distribution, and this value was further transformed as a z-score ((Hb-mean)/SD): the regression coefficient (95% confidence intervals; P-value) shown is the rise in cord TSH associated with each 1 standard deviation rise in Log10 Hb.
4 No difference in the mean difference of cord TSH was seen between emergency (N=43) and elective (N=78) lower segment Caesarean section (0.01; 95%CI 2.03 to -2.02; P>0.90)

78
4 DISCUSSION AND CONCLUSION

79
This study has demonstrated that approximately 3.4% of the Northern Tasmanian
women could be at risk of developing thyroid dysfunction during their pregnancy
with (TSH>2.5-3mU/L and >3mU/L) when measured between end of the second
trimester and start of the third. Additionally, 12.3% of the same pregnant population
could be labelled with the controversial status of (Isolated Hypothyroxinemia) when
applying <8.9pmol/L for FT4 as a cut-off. The results also suggest that antenatal
complications defined in this study are not associated with low thyroid status. The
outcomes of this study also suggest that the risk for experiencing prolonged labour as
an intra-natal complication can be increased up to three-fold with low thyroid status
(IRR 3.31; 95% CI 1.13 to 9.69; P= 0.029).
There was no positive association between iron deficiency anaemia (IDA) and low
thyroid status could be demonstrated in this thesis. This study was not able to clearly
demonstrate whether a symptom based risk score for thyroid dysfunction during
pregnancy would be better than biochemical screening. Although CB-TSH
demonstrated a positive association with maternal complications (IPH), its role in
assessing foetal thyroid status has not been established. A 41% of the study
population had iodine deficiency during pregnancy and 11.2% of this subpopulation
developed isolated hypothyroxinemia.
Despite more than 2200 subjects being approached to enrol in the study, the consent
rate was relatively low (28%). The main reason for this is most likely to be the
single-centred study design, as well as the general lack of awareness of the
consequences of iodine deficiency within the targeted study population. Although it
was expected that the incidence rate of low thyroid function during pregnancy would

80
be higher than 3.4%, this is in line with internationally estimated figures for
subclinical hypothyroidism in pregnancy (1.5-4 %), (Allan et al., 2000, Casey et al.,
2005, Negro and Mestman, 2011). Furthermore, the results of this study suggest that
the rate of prolonged labour as an intra-natal complication was greater in pregnant
women with decreased thyroid function (IRR 3.31; 95% CI 1.13 to 9.69; P= 0.029).
There has been conflicting reports on the association between gestational diabetes
and hypothyroidism (Casey et al., 2007, Cleary-Goldman et al., 2008, Korevaar et
al., 2013). No clear association (P= 0.36) between these were shown in the current
study. It has previously been suggested that finding associations between
complications occurring during pregnancy and thyroid function disorder was a
difficult task (Negro and Mestman, 2011). Furthermore, it has been reported that
inappropriate sample size is a common problem which occurs while investigating
complication rates in overt or subclinical hypothyroidism during pregnancy (Negro
and Mestman, 2011). These are in agreement with the current study.
Although epidemic goitre is a strong part of Tasmanian history, the main culprit
(iodine deficiency) remains persistent (Gibson, 2006, Burgess et al., 2007). It has
also been reported that iodine deficiency is the main reason for subclinical
hypothyroidism (SH) in iodine deplete areas (de Benoist et al., 2003, Hynes et al.,
2004, Li et al., 2006, Andersson et al., 2007, Vanderpump, 2010). Despite iodine-
fortification in Tasmania being mandatory, a nine year follow-up study of school-
aged children who were born to iodine deficient mothers were found to have
difficulties in reading and grammar when compared to peers of the same age
(Burgess et al., 2007, Hynes et al., 2013).

81
The symptom-based risk score using commonly accepted indicators of thyroid
dysfunction has some ability to differentiate low and normal thyroid status. There
doesn’t appear to be clear rationale for the variables included in the risk score. It may
require orders of magnitude larger patient groups to reliably identify all the possible
symptomatic expressions of low thyroid status. Also, the relatively small numbers of
patients found with low thyroid status, as well as the relatively unstable estimates
associated with nearby alternative thresholds, means that uncertainties around the
usefulness of the risk score need to be considered.
The estimation of the coefficients to be included in the risk score, and the calculation
of the patient risk scores for the purpose of evaluation of efficacy of differentiation
were performed on the same patients, rather than on two separate groups, as would
be preferable (due to insufficient numbers of patients with low thyroid status). A
broader objection to this particular expression of a symptomatic screening test for
potential low thyroid status is that it was not conducted completely in a primary
antenatal clinic where pregnant women undergo a routine check-up from early
gestational age with consequent follow-up throughout all pregnancy period.
IDA during pregnancy has been previously reported to cause obstetric and neonatal
complications as well as neuro-psychological development (Scholl and Hediger,
1994, Brabin et al., 2001, Sachdev et al., 2005). A positive relationship between IDA
and low thyroid function has also been shown (Zimmermann et al., 2000). Although
the current study demonstrates low ferritin level in 32.7% of study participants, there
is no evidence of associations with low thyroid status.

82
In contrast, macrocytic anaemia was reported in 4 of 22 (18%) of low thyroid status.
In another study, 57.1% of participants with hypothyroidism were reported to have
either microcytic or macrocytic anaemia (Omar et al., 2010), with similar findings
different explanations reported by (Tudhope and Wilson, 1960, Fein and Rivlin,
1975, Horton et al., 1976). Although causes of macrocytosis in the general
population can vary, including drugs, alcoholism, hypothyroidism and bone marrow
dysplasia, deficiency of vitamin-B12 and folate were most prevalent in the obstetric
population (Van der Weyden and Campbell, 1988, Colon-Otero et al., 1992, Savage
et al., 2000, Kaferle and Strzoda, 2009, Tripathi et al., 2012). Further studies are
required to differentiate that macrocytosis found in this study subgroup of low
thyroid status, against those caused by vitamin-B12 and folate deficiencies.
The effect of iodine deficiency on the incidence of thyroid dysfunction has also been
investigated. Although iodised salt has been promoted for the last decade and
consumption of iodine-contained multi-vitamins, median urinary iodine of 117µg/L
derived from study cohort results reflects deficiency according to WHO’s latest
recommendations (World Health Organization, 2013). While 11.2% of the study
iodine deficient population was labelled with isolated hypothyroxinemia (IH), it was
reported to be approximately of 25-30% in other iodine deficient population (Berbel
et al., 2009, Moleti et al., 2009, Krassas et al., 2010).
Normal reference range for FT4 in the general population provided by LGH
pathology is 10.00-28.2pmol/L. Thus, considering the fact of physiological changes
in the thyroid regulation that occur in pregnancy (discussed earlier), a lower cutoff
was considered. Since there is no standard reference range to define

83
hypothyroxinemia, lower bound (<8.9pmol/L) of FR4 used in the study was a result
of statistical assumptions. Nevertheless, now we can set our own reference range for
FT4 based on study cohort results. Results of free thyroxin of the study cohort have
been recalculated for the group reference range, LL =7.10pmol/L (95% CI 5.36,
8.83) and UL =14.02pmol/L (95% CI 12.28, 15.75).
Applying the group lower bound (<7.1) as a cutoff will result in a remarkable
decrease in number of isolated hypothyroxinemia to only 1.47% (9/609). Further
clinical studies are required to justify the validity these biomedical references. The
relevance of iodine deficiency and IH with possible health consequences on foetal
neuropsychological development were also investigated and published (Morreale de
Escobar et al., 2000, Negro and Mestman, 2011). Although a recent publication
reported a negative effect of maternal iodine deficiency on offspring’s reading
ability, it was not verified whether IH was a contributing factor (Hynes et al., 2013).
It is therefore recommended to follow-up of the iodine deficient population of this
study, to determine whether neuropsychological consequences are due to iodine
deficiency alone, IH alone or when combined.
It has been suggested that maternal IH has no impact on normal IQ development of
offspring, according to a recent study (Grau et al., 2015). In contrast, association
between hypothyroxinemia and autism has been suggested (Román et al., 2013).
Also, a survey review of the European clinical institutions resulted in lack of a
standard approach regarding hypothyroxinemia in pregnancy (Vaidya et al., 2012).
These reports encourage further follow-up of IH cases of this study to be considered.

84
Persistence of iodine deficiency in Tasmania was reported a decade ago. In view of
this fact, it was hoped that mandatory fortification and awareness would halt this
public health issue. Nevertheless, median UIC of 117ug/L of our pregnant
participants still reflects inadequate iodine intake. According to the latest
recommendation by WHO; an adequate iodine intake for pregnant women is best
achieved when median UIC is between 150-249 µg/L levels (World Health
Organization, 2013). Retrospective analysis of this population and data related to
their diet maybe required in order to investigate the causes and factors contributed to
this result. Also, comparing this outcome with a non-pregnant population will lead to
determine individual factors from combined ones.
Neonatal hypothyroidism causes serious neurological disorder in children. It is
relatively rare, affecting one in 3500-4000, the diagnosis is conducted by screening
neonatal TSH in the venous blood obtained via heel prick (Grueters and Krude,
2006). As symptoms and signs are indistinguishable at early infancy, it is essential to
initiate this biochemical neonatal screening for early diagnosis and treatment
(Vanderpump, 2010). Cord blood is accessible via normal or operative deliveries,
testing for TSH in the cord blood (CB-TSH) was thought to be a less invasive
alternative in this study.
Although there are no general standardised normal values for CB-TSH,
recommendations for a cut off value vary between 20mU/L and 14mU/L (Manglik
et al., 2005). Variable levels of CB-TSH according to type of delivery as well as
according to history of previous pregnancy have been demonstrated in this study.
Since low cord TSH results for babies born by LSCS and for babies born to first time

85
pregnancy (Table 3-11) can’t be explained at this stage, investigating the role of
anaesthesia and stress on the thyroid in non-pregnant and during delivery, may help
to clarify the variable levels of CB-TSH.
A decrease of more than 50% in results of CB-TSH of ten babies born to participants
who suffered IPH/APH was demonstrated, compared to babies born without maternal
complications (Table 3-10). Although this may not reflect low thyroid status in the
newborn babies, they do demonstrate strong variability in reaction of the foetal
thyroid towards different maternal obstetric conditions (ante-/intra-partum bleeding).
A number of factors limited this study. The major limitation lies within the design of
the study; single-centre recruitment lead to a small selected group. Analysing data in
small numbers, made it difficult to determine whether increases in complication rates
were statistically significant. The absence of parallel clinical assessment by an
obstetrician for all pregnant women, made a comparison between case selective and
generalised screening not feasible in this study. In addition, circadian variation of UI
keeps the question of over-estimation or under-estimation wide open.
The number of cord blood samples collected was low, possibly due to unpredictable
labour times. Lack of own method-specific and trimester specific reference range for
TFT in pregnancy that could add more specificity to the study. Using more
sophisticated screening tools like chromatography/tandem-mass spectrometry
(LC/MS/MS) was not available. Analysis of cord blood TSH results could have
been of more value if compared against neonatal TSH results for the same babies.

86
A larger scale study is clearly required to determine the true incidence of pregnancy
complications (including gestational diabetes and prolonged labour) in women with
low thyroid function in Tasmania. A valid comparison between well implemented
symptom-based risk score and biochemical screening is feasible with a collective
team work between pathology and ante natal clinic. A retrospective analysis can
compare cord TSH of this study with the neonatal TSH to determine potential
associations. A positive association may reveal CB-TSH as a valid alternative for the
current neonatal screening. In addition, a retrospective study investigating detailed
diet of the cohort may reveal causes of iodine deficiency found in this pregnant
population.
Furthermore, calculation of cutoff values for TSH according to the TPO status
revealed almost 0.5mU/L difference in favor of TPO positive group where only two
of TSH results showed above 3.05mU/L and similar number of participants has UIC
< 117ug/L without any identifiable association between them. However, because of
the small number of positive TPO results, we cannot draw a valid conclusion without
making unsubstantiated assumptions. When applying the upper bound of TSH (>2.6)
derived from the study cohort with TPO-ve, 4.95% (27/546) of these participants
may be at risk of developing thyroid dysfunction regardless being negative to TPO
antibodies. Since the original study was not designed to set TSH reference ranges
according to TPO status, applying this in future studies is strongly warranted in order
to find their significance and validity for this specific population.
In conclusion, this study demonstrates that a small percentage of pregnant women
living in iodine-poor Tasmania are prone to thyroid dysfunction. Complications that

87
may occur during pregnancy and delivery could be due to low thyroid function, but
was not able to be clearly proven in this study. Although prior or early-pregnancy
testing for iodine level and thyroid function can help early identify iodine deficiency
and thyroid disorder, justifying a general screening will require further studies with
multicentre-recruitment and ante-natal clinics involvement. Approving the use of
cord blood as a screening tool for neonatal hypothyroidism will require further work.
This includes comparing current CB-TSH results with neonatal TSH to determine a
valid association. Further investigation is also required to determine whether the
unexpected association between CB-TSH and IPH/APH is a constant relationship,
not raised by chance.

88
Bibliography
ABALOVICH, M., GUTIERREZ, S., ALCARAZ, G., MACCALLINI, G., GARCIA, A. & LEVALLE, O. 2002. Overt and subclinical hypothyroidism complicating pregnancy. Thyroid, 12, 63-68.
ALLAN, W., HADDOW, J., PALOMAKI, G., WILLIAMS, J., MITCHELL, M., HERMOS, R., FAIX, J. & KLEIN, R. 2000. Maternal thyroid deficiency and pregnancy complications: implications for population screening. Journal of Medical Screening, 7, 127-130.
ALTOMARE, M., LA VIGNERA, S., ASERO, P., RECUPERO, D., CONDORELLI, R. A., SCOLLO, P., GULISANO, A., MAGRO, E., TUMINO, D., TUMINO, S., VICARI, E., LEANZA, V., D’AGATA, R. & CALOGERO, A. E. 2013. High prevalence of thyroid dysfunction in pregnant women. Journal of Endocrinological Investigation, 36, 407-411.
ANCKAERT, E., POPPE, K., VAN UYTFANGHE, K., SCHIETTECATTE, J., FOULON, W. & THIENPONT, L. M. 2010. FT4 immunoassays may display a pattern during pregnancy similar to the equilibrium dialysis ID-LC/tandem MS candidate reference measurement procedure in spite of susceptibility towards binding protein alterations. Clin Chim Acta, 411, 1348-53.
ANDERSEN, S., KARMISHOLT, J., PEDERSEN, K. M. & LAURBERG, P. 2008. Reliability of studies of iodine intake and recommendations for number of samples in groups and in individuals. Br J Nutr, 99, 813-8.
ANDERSSON, M., DE BENOIST, B., DELANGE, F. & ZUPAN, J. 2007. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: conclusions and recommendations of the Technical Consultation. Public health nutrition, 10, 1606-1611.
ANDERSSON, M., KARUMBUNATHAN, V. & ZIMMERMANN, M. B. 2012. Global iodine status in 2011 and trends over the past decade. The Journal of nutrition, 142, 744-750.
ANDERSSON, M., TAKKOUCHE, B., EGLI, I., ALLEN, H. E. & BENOIST, B. D. 2005. Current global iodine status and progress over the last decade towards the elimination of iodine deficiency. Bulletin of the World Health Organization, 83, 518-525.
ANDREWS, N. C. 1999. Disorders of iron metabolism. N Engl J Med, 341, 1986-95.

89
ASHOOR, G., MAIZ, N., ROTAS, M., JAWDAT, F. & NICOLAIDES, K. H. 2010. Maternal thyroid function at 11 to 13 weeks of gestation and subsequent fetal death. Thyroid, 20, 989-93.
ASSEY, V. D., GREINER, T., MZEE, R., ABUU, H., MGOBA, C., KIMBOKA, S. & PETERSON, S. 2006. Iodine deficiency persists in the Zanzibar Islands of Tanzania. Food & Nutrition Bulletin, 27, 292-299.
BEARD, J. L. 2001. Iron biology in immune function, muscle metabolism and neuronal functioning. The Journal of nutrition, 131, 568S-580S.
BENHADI, N., WIERSINGA, W. M., REITSMA, J. B., VRIJKOTTE, T. G. & BONSEL, G. J. 2009. Higher maternal TSH levels in pregnancy are associated with increased risk for miscarriage, fetal or neonatal death. Eur J Endocrinol, 160, 985-91.
BENOIST, B. D., MCLEAN, E., EGLL, I. & COGSWELL, M. 2008. Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia, World Health Organization.
BERBEL, P., MESTRE, J. L., SANTAMARIA, A., PALAZON, I., FRANCO, A., GRAELLS, M., GONZALEZ-TORGA, A. & DE ESCOBAR, G. M. 2009. Delayed neurobehavioral development in children born to pregnant women with mild hypothyroxinemia during the first month of gestation: the importance of early iodine supplementation. Thyroid, 19, 511-9.
BERNAL, J. & NUNEZ, J. 1995. Thyroid hormones and brain development. European Journal of Endocrinology, 133, 390-398.
BERNÁT, I. 1983. Iron deficiency. Iron Metabolism. Springer.
BIZHANOVA, A. & KOPP, P. 2009. Minireview: The sodium-iodide symporter NIS and pendrin in iodide homeostasis of the thyroid. Endocrinology, 150, 1084-90.
BLATT, A. J., NAKAMOTO, J. M. & KAUFMAN, H. W. 2012. National status of testing for hypothyroidism during pregnancy and postpartum. J Clin Endocrinol Metab, 97, 777-84.
BLAZER, S., MOREH-WATERMAN, Y., MILLER-LOTAN, R., TAMIR, A. & HOCHBERG, Z. 2003. Maternal hypothyroidism may affect fetal growth and neonatal thyroid function. Obstet Gynecol, 102, 232-41.

90
BOCOS-TERRAZ, J. P., IZQUIERDO-ÁLVAREZ, S., BANCALERO-FLORES, J. L., ÁLVAREZ-LAHUERTA, R., AZNAR-SAUCA, A., REAL-LÓPEZ, E., IBÁÑEZ-MARCO, R., BOCANEGRA-GARCÍA, V. & RIVERA-SÁNCHEZ, G. 2009. Thyroid hormones according to gestational age in pregnant Spanish women. BMC research notes, 2, 1.
BOMFORD, R. 1938. Anaemia in myxoedema: and the role of the thyroid gland in erythropoiesis. QJM, 7, 495-536.
BOTHWELL, T. H., CHARLTON, R., COOK, J. & FINCH, C. A. 1979. Iron metabolism in man. Iron metabolism in man.
BRABIN, B. J., PREMJI, Z. & VERHOEFF, F. 2001. An analysis of anemia and child mortality. The Journal of nutrition, 131, 636S-648S.
BRAVERMAN, L. E. & COOPER, D. 2012. Werner & Ingbar's the thyroid: a fundamental and clinical text, Lippincott Williams & Wilkins.
BURGESS, J. R., SEAL, J. A., STILWELL, G. M., REYNOLDS, P. J. & ET AL. 2007. A case for universal salt iodisation to correct iodine deficiency in pregnancy: another salutary lesson from Tasmania. Medical Journal of Australia, 186, 574-6.
BURROW, G. H. 1990. Thyroid status in normal pregnancy. J Clin Endocrinol Metab, 71, 274-5.
CALVO, R. M., JAUNIAUX, E., GULBIS, B., ASUNCIÓN, M., GERVY, C., CONTEMPRÉ, B. & DE ESCOBAR, G. M. 2002. Fetal tissues are exposed to biologically relevant free thyroxine concentrations during early phases of development. Journal of Clinical Endocrinology & Metabolism, 87, 1768-1777.
CASEY, B. M., DASHE, J. S., SPONG, C. Y., MCINTIRE, D. D., LEVENO, K. J. & CUNNINGHAM, G. F. 2007. Perinatal Significance of Isolated Maternal Hypothyroxinemia Identified in the First Half of Pregnancy. Obstetrics & Gynecology, 109, 1129-1135.
CASEY, B. M., DASHE, J. S., WELLS, C. E., MCINTIRE, D. D., BYRD, W., LEVENO, K. J. & CUNNINGHAM, F. G. 2005. Subclinical hypothyroidism and pregnancy outcomes. Obstetrics & Gynecology, 105, 239-245.

91
CASEY, B. M., DASHE, J. S., WELLS, C. E., MCINTIRE, D. D., LEVENO, K. J. & CUNNINGHAM, F. G. 2006. Subclinical hyperthyroidism and pregnancy outcomes. Obstetrics & Gynecology, 107, 337-341.
CASEY, B. M. & LEVENO, K. J. 2006. Thyroid disease in pregnancy. Obstetrics & Gynecology, 108, 1283-1292.
CHAN, S. & KILBY, M. 2000. Thyroid hormone and central nervous system development. Journal of Endocrinology, 165, 1-8.
CHANG, S., ZENG, L., BROUWER, I. D., KOK, F. J. & YAN, H. 2013. Effect of iron deficiency anemia in pregnancy on child mental development in rural China. Pediatrics, 131, e755-e763.
CHIAMOLERA, M. I. & WONDISFORD, F. E. 2009. Minireview: Thyrotropin-releasing hormone and the thyroid hormone feedback mechanism. Endocrinology, 150, 1091-6.
CLEARY-GOLDMAN, J., MALONE, F. D., LAMBERT-MESSERLIAN, G., SULLIVAN, L., CANICK, J., PORTER, T. F., LUTHY, D., GROSS, S., BIANCHI, D. W., D’ALTON, M. E. & CONSORTIUM, F. T. F. 2008. Maternal Thyroid Hypofunction and Pregnancy Outcome. Obstetrics & Gynecology, 112, 85-92.
COGSWELL, M. E., PARVANTA, I., ICKES, L., YIP, R. & BRITTENHAM, G. M. 2003. Iron supplementation during pregnancy, anemia, and birth weight: a randomized controlled trial. The American journal of clinical nutrition, 78, 773-781.
COLON-OTERO, G., MENKE, D. & HOOK, C. 1992. A practical approach to the differential diagnosis and evaluation of the adult patient with macrocytic anemia. The Medical clinics of North America, 76, 581-597.
CRAIG, W. Y., ALLAN, W. C., KLOZA, E. M., PULKKINEN, A. J., WAISBREN, S., SPRATT, D. I., PALOMAKI, G. E., NEVEUX, L. M. & HADDOW, J. E. 2012. Mid-gestational maternal free thyroxine concentration and offspring neurocognitive development at age two years. J Clin Endocrinol Metab, 97, E22-8.
CRANEFIELD, P. F. 1962. The discovery of cretinism. Bull Hist Med, 36, 489-511.

92
DAVIS, L. E., LUCAS, M. J., HANKINS, G. D., ROARK, M. L. & GARY CUNNINGHAM, F. 1989. Thyrotoxicosis complicating pregnancy. American journal of obstetrics and gynecology, 160, 63-70.
DE BENOIST, B., ANDERSSON, M., TAKKOUCHE, B. & EGLI, I. 2003. Prevalence of iodine deficiency worldwide. The Lancet, 362, 1859-1860.
DE ESCOBAR, G. M., OBREGON, M. J. & DEL REY, F. E. 2004. Role of thyroid hormone during early brain development. European Journal of Endocrinology, 151, U25-U37.
DE LA VIEJA, A., DOHAN, O., LEVY, O. & CARRASCO, N. 2000. Molecular analysis of the sodium/iodide symporter: impact on thyroid and extrathyroid pathophysiology. Physiol Rev, 80, 1083-105.
DE SILVA, A., ATUKORALA, S., WEERASINGHE, I. & AHLUWALIA, N. 2003. Iron supplementation improves iron status and reduces morbidity in children with or without upper respiratory tract infections: a randomized controlled study in Colombo, Sri Lanka. The American journal of clinical nutrition, 77, 234-241.
DE VIVO, A., MANCUSO, A., GIACOBBE, A., MOLETI, M., MAGGIO SAVASTA, L., DE DOMINICI, R., PRIOLO, A. M. & VERMIGLIO, F. 2010. Thyroid function in women found to have early pregnancy loss. Thyroid, 20, 633-7.
DEGROOT, L. J., STANBURY, J. B. & MEANS, J. H. 1975. The thyroid and its diseases, Wiley Biomedical Division, Wiley.
DELANGE, F. 2001. Iodine deficiency as a cause of brain damage. Postgraduate Medical Journal, 77, 217-220.
DIÉGUEZ, M., HERRERO, A., AVELLO, N., SUÁREZ, P., DELGADO, E. & MENÉNDEZ, E. 2016. Prevalence of thyroid dysfunction in women in early pregnancy: does it increase with maternal age? Clinical endocrinology, 84, 121-126.
DOSIOU, C., BARNES, J., SCHWARTZ, A., NEGRO, R., CRAPO, L. & STAGNARO-GREEN, A. 2012. Cost-effectiveness of universal and risk-based screening for autoimmune thyroid disease in pregnant women. The Journal of Clinical Endocrinology & Metabolism, 97, 1536-1546.

93
EARL, R. & WOTECKI, C. 1993. Institute of medicine. Iron deficiency anemia: recomended guidelines for the prevention, detection and management among US children and women of childbearing age. Institute of medicine: Iron deficiency anemia: recomended guidelines for the prevention, detection and management among US children and women of childbearing age.
EFTEKHARI, M. H., SIMONDON, K. B., JALALI, M., KESHAVARZ, S. A., ELGUERO, E., ESHRAGHIAN, M. R. & SAADAT, N. 2006. Effects of administration of iron, iodine and simultaneous iron-plus-iodine on the thyroid hormone profile in iron-deficient adolescent Iranian girls. Eur J Clin Nutr, 60, 545-52.
EKINS, R., CHU, F. & MICALLEF, J. 1989. High specific activity chemiluminescent and fluorescent markers: Their potential application to high sensitivity and ‘multi‐analyte’immunoassays. Journal of bioluminescence and chemiluminescence, 4, 59-78.
EPSTEIN, F. H., BURROW, G. N., FISHER, D. A. & LARSEN, P. R. 1994. Maternal and fetal thyroid function. New England Journal of Medicine, 331, 1072-1078.
ESKANDARI, S., LOO, D. D., DAI, G., LEVY, O., WRIGHT, E. M. & CARRASCO, N. 1997. Thyroid Na+/I− symporter Mechanism, stoichiometry, and specificity. Journal of Biological Chemistry, 272, 27230-27238.
FEIN, H. & RIVLIN, R. 1975. Anemia in thyroid diseases. The Medical clinics of North America, 59, 1133-1145.
FOMON, S. J. 1993. Iron. In: Nutrition of Normal Infants. St., 239-259.
GARBER, J. R., COBIN, R. H., GHARIB, H., HENNESSEY, J. V., KLEIN, I., MECHANICK, J. I., PESSAH-POLLACK, R., SINGER, P. A. & WOEBER, K. A. 2012. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocrine Practice, 18, 988-1028.
GÄRTNER, R. 2009. Thyroid diseases in pregnancy. Current Opinion in Obstetrics and Gynecology, 21, 501-507.
GHARIB, H., TUTTLE, R. M., BASKIN, H. J., FISH, L. H., SINGER, P. A. & MCDERMOTT, M. T. 2005. Subclinical thyroid dysfunction: a joint statement on management from the American Association of Clinical

94
Endocrinologists, the American Thyroid Association, and the Endocrine Society. Journal of Clinical Endocrinology & Metabolism, 90, 581-585.
GIBSON, H. B. 2006. Surveillance of iodine deficiency disorders in Tasmania 1949-1984, Myola House of Publishing.
GILBERT, R. M., HADLOW, N. C., WALSH, J. P., FLETCHER, S. J., BROWN, S. J., STUCKEY, B. G. & LIM, E. M. 2008a. Assessment of thyroid function during pregnancy: first-trimester (weeks 9-13) reference intervals derived from Western Australian women. Med J Aust, 189, 250-3.
GILBERT, R. M., HADLOW, N. C., WALSH, J. P., FLETCHER, S. J., BROWN, S. J., STUCKEY, B. G. & LIM, E. M. 2008b. Assessment of thyroid function during pregnancy: first-trimester (weeks 9–13) reference intervals derived from Western Australian women. Med J Aust, 189, 250-3.
GLINOER, D. 1997. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev, 18, 404-33.
GLINOER, D. 1999. What happens to the normal thyroid during pregnancy? Thyroid, 9, 631-635.
GLINOER, D. 2001. Potential consequences of maternal hypothyroidism on the offspring: evidence and implications. Hormone Research in Paediatrics, 55, 109-114.
GLINOER, D. 2004. The regulation of thyroid function during normal pregnancy: importance of the iodine nutrition status. Best Practice & Research Clinical Endocrinology & Metabolism, 18, 133-152.
GLINOER, D., RIAHI, M., GRÜN, J.-P. & KINTHAERT, J. 1994. Risk of subclinical hypothyroidism in pregnant women with asymptomatic autoimmune thyroid disorders. The Journal of clinical endocrinology and metabolism, 79, 197-204.
GOLDSCHMIDT, V. 1952. Geochemical aspects of the origin of complex organic molecules on the Earth, as precursors to organic life. New Biol, 12, 97-105.
GRAU, G., AGUAYO, A., VELA, A., ANIEL-QUIROGA, A., ESPADA, M., MIRANDA, G., MARTINEZ-INDART, L., MARTUL, P., CASTAÑO, L. & RICA, I. 2015. Normal intellectual development in children born from women with hypothyroxinemia during their pregnancy. Journal of Trace Elements in Medicine and Biology, 31, 18-24.

95
GRUETERS, A. & KRUDE, H. 2006. Update on the management of congenital hypothyroidism. Hormone research, 68, 107-111.
GUGGENHEIM, K. Y. 1995. Chlorosis: the rise and disappearance of a nutritional disease. The Journal of nutrition, 125, 1822-1825.
HADDOW, J. E., KNIGHT, G. J., PALOMAKI, G. E., MCCLAIN, M. R. & PULKKINEN, A. J. 2004. The reference range and within-person variability of thyroid stimulating hormone during the first and second trimesters of pregnancy. Journal of Medical Screening, 11, 170-174.
HADDOW, J. E., PALOMAKI, G. E., ALLAN, W. C., WILLIAMS, J. R., KNIGHT, G. J., GAGNON, J., O'HEIR, C. E., MITCHELL, M. L., HERMOS, R. J. & WAISBREN, S. E. 1999. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. New England Journal of Medicine, 341, 549-555.
HALDIMANN, M., ALT, A., BLANC, A. & BLONDEAU, K. 2005. Iodine content of food groups. Journal of food Composition and Analysis, 18, 461-471.
HALL, J. E. 2010. Guyton and Hall Textbook of Medical Physiology: Enhanced E-book, Elsevier Health Sciences.
HALLBERG, L. 1995. Results of surveys to assess iron status in Europe. Nutrition reviews, 53, 314-322.
HENRICHS, J., BONGERS-SCHOKKING, J. J., SCHENK, J. J., GHASSABIAN, A., SCHMIDT, H. G., VISSER, T. J., HOOIJKAAS, H., DE MUINCK KEIZER-SCHRAMA, S. M., HOFMAN, A., JADDOE, V. V., VISSER, W., STEEGERS, E. A., VERHULST, F. C., DE RIJKE, Y. B. & TIEMEIER, H. 2010. Maternal thyroid function during early pregnancy and cognitive functioning in early childhood: the generation R study. J Clin Endocrinol Metab, 95, 4227-34.
HENRY, G., SOBKI, S. H., AL-BESHARA, N. M., HARKONEN, M. E. & MILLER, H. R. 2000. Thyroid function in cord blood. Saudi medical journal, 21, 36-39.
HESS, S. Y., ZIMMERMANN, M. B., ARNOLD, M., LANGHANS, W. & HURRELL, R. F. 2002. Iron deficiency anemia reduces thyroid peroxidase activity in rats. The Journal of nutrition, 132, 1951-1955.

96
HETZEL, B. 1983. Iodine deficiency disorders (IDD) and their eradication. The Lancet, 322, 1126-1129.
HOLLOWELL, J. G., STAEHLING, N. W., FLANDERS, W. D., HANNON, W. H., GUNTER, E. W., SPENCER, C. A. & BRAVERMAN, L. E. 2002. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab, 87, 489-99.
HOOFNAGLE, A. N. & ROTH, M. Y. 2013. Improving the measurement of serum thyroglobulin with mass spectrometry. The Journal of Clinical Endocrinology & Metabolism, 98, 1343-1352.
HORACEK, J., SPITALNIKOVA, S., DLABALOVA, B., MALIROVA, E., VIZDA, J., SVILIAS, I., CEPKOVA, J., MC GRATH, C. & MALY, J. 2010. Universal screening detects two-times more thyroid disorders in early pregnancy than targeted high-risk case finding. European Journal of Endocrinology, 163, 645-650.
HOROWITZ, K. M., INGARDIA, C. J. & BORGIDA, A. F. 2013. Anemia in pregnancy. Clinics in laboratory medicine, 33, 281-291.
HORTON, L., COBURN, R., ENGLAND, J. & HIMSWORTH, R. 1976. The haematology of hypothyroidism. QJM, 45, 101-123.
HYNES, K. L., BLIZZARD, C. L., VENN, A. J., DWYER, T. & BURGESS, J. R. 2004. Persistent iodine deficiency in a cohort of Tasmanian school children: associations with socio‐economic status, geographical location and dietary factors. Australian and New Zealand journal of public health, 28, 476-481.
HYNES, K. L., OTAHAL, P., HAY, I. & BURGESS, J. R. 2013. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. The Journal of Clinical Endocrinology & Metabolism, 98, 1954-1962.
IDRIS, I., SRINIVASAN, R., SIMM, A. & PAGE, R. C. 2005. Maternal hypothyroidism in early and late gestation: effects on neonatal and obstetric outcome. Clinical endocrinology, 63, 560-565.
JACOB, H. & PETERS, C. 2015. Screening, diagnosis and management of congenital hypothyroidism: European Society for Paediatric Endocrinology Consensus Guideline. Archives of disease in childhood-Education & practice edition, edpract-2014-307738.

97
KAFERLE, J. & STRZODA, C. E. 2009. Evaluation of macrocytosis. American family physician, 79, 203-208.
KARAKOSTA, P., ALEGAKIS, D., GEORGIOU, V., ROUMELIOTAKI, T., FTHENOU, E., VASSILAKI, M., BOUMPAS, D., CASTANAS, E., KOGEVINAS, M. & CHATZI, L. 2012. Thyroid dysfunction and autoantibodies in early pregnancy are associated with increased risk of gestational diabetes and adverse birth outcomes. J Clin Endocrinol Metab, 97, 4464-72.
KELLY, F. C. 1961. Iodine in medicine and pharmacy since its discovery—1811-1961. Proceedings of the Royal Society of Medicine, 54, 831.
KESTER, M. H., DE MENA, R. M., OBREGON, M. J., MARINKOVIC, D., HOWATSON, A., VISSER, T. J., HUME, R. & DE ESCOBAR, G. M. 2004. Iodothyronine levels in the human developing brain: major regulatory roles of iodothyronine deiodinases in different areas. Journal of Clinical Endocrinology & Metabolism, 89, 3117-3128.
KHALAFALLAH, A., DENNIS, A., BATES, J., BATES, G., ROBERTSON, I., SMITH, L., BALL, M., SEATON, D., BRAIN, T. & RASKO, J. 2010. A prospective randomized, controlled trial of intravenous versus oral iron for moderate iron deficiency anaemia of pregnancy. Journal of internal medicine, 268, 286-295.
KILBRIDE, J., BAKER, T. G., PARAPIA, L. A., KHOURY, S. A., SHUQAIDEF, S. W. & JERWOOD, D. 1999. Anaemia during pregnancy as a risk factor for iron-deficiency anaemia in infancy: a case-control study in Jordan. International Journal of Epidemiology, 28, 461-468.
KIPLE, K. F. & ORNELAS, K. C. 2001. The Cambridge world history of food. Food Service Technology, 1, 61-62.
KLEIN, R., HADDOW, J., FALX, J., BROWN, R., HERMOS, R., PULKKINEN, A. & MITCHELL, M. 1991. Prevalence of thyroid deficiency in pregnant women. Clinical endocrinology, 35, 41-46.
KNUDSEN, N., CHRISTIANSEN, E., BRANDT-CHRISTENSEN, M., NYGAARD, B. & PERRILD, H. 2000. Age- and sex-adjusted iodine/creatinine ratio. A new standard in epidemiological surveys? Evaluation of three different estimates of iodine excretion based on casual urine samples and comparison to 24 h values. Eur J Clin Nutr, 54, 361-3.

98
KOIBUCHI, N. & CHIN, W. W. 2000. Thyroid hormone action and brain development. Trends in Endocrinology & Metabolism, 11, 123-128.
KOPP, P. (ed.) 2005. Thyroid hormone synthesis, New York: Lippincott Williams Wilkins.
KOREVAAR, T. I., SCHALEKAMP-TIMMERMANS, S., DE RIJKE, Y. B., VISSER, W. E., VISSER, W., DE MUINCK KEIZER-SCHRAMA, S. M., HOFMAN, A., ROSS, H. A., HOOIJKAAS, H., TIEMEIER, H., BONGERS-SCHOKKING, J. J., JADDOE, V. W., VISSER, T. J., STEEGERS, E. A., MEDICI, M. & PEETERS, R. P. 2013. Hypothyroxinemia and TPO-antibody positivity are risk factors for premature delivery: the generation R study. J Clin Endocrinol Metab, 98, 4382-90.
KRAMER, M. S. 2003. The epidemiology of adverse pregnancy outcomes: an overview. J Nutr, 133, 1592S-1596S.
KRASSAS, G., POPPE, K. & GLINOER, D. 2010. Thyroid function and human reproductive health. Endocrine reviews, 31, 702-755.
LAZARUS, J. & OKOSIEME, O. E. 2000. Hypothyroidism in Pregnancy.
LEE, R. H., SPENCER, C. A., MESTMAN, J. H., MILLER, E. A., PETROVIC, I., BRAVERMAN, L. E. & GOODWIN, T. M. 2009. Free T4 immunoassays are flawed during pregnancy. Am J Obstet Gynecol, 200, 260 e1-6.
LEUNG, A. S., MILLAR, L. K., KOONINGS, P. P., MONTORO, M. & MESTMAN, J. H. 1993. Perinatal outcome in hypothyroid pregnancies. Obstet Gynecol, 81, 349-53.
LI, M., EASTMAN, C. J., WAITE, K. V., MA, G., ZACHARIN, M. R., TOPLISS, D. J., HARDING, P. E., WALSH, J. P., WARD, L. C. & MORTIMER, R. H. 2006. Are Australian children iodine deficient? Results of the Australian national iodine nutrition study. Medical Journal of Australia, 184, 165.
LI, Y., SHAN, Z., TENG, W., YU, X., FAN, C., TENG, X., GUO, R., WANG, H., LI, J., CHEN, Y., WANG, W., CHAWINGA, M., ZHANG, L., YANG, L., ZHAO, Y. & HUA, T. 2010. Abnormalities of maternal thyroid function during pregnancy affect neuropsychological development of their children at 25-30 months. Clin Endocrinol (Oxf), 72, 825-9.

99
LOZOFF, B., JIMENEZ, E. & WOLF, A. W. 1991. Long-term developmental outcome of infants with iron deficiency. New England Journal of Medicine, 325, 687-694.
MANGLIK, A. K., CHATTERJEE, N. & GHOSH, G. 2005. Umbilical cord blood TSH levels in term neonates: a screening tool for congenital hypothyroidism. Indian Pediatr, 42, 1029-32.
MANNISTO, T., MENDOLA, P., GREWAL, J., XIE, Y., CHEN, Z. & LAUGHON, S. K. 2013. Thyroid diseases and adverse pregnancy outcomes in a contemporary US cohort. J Clin Endocrinol Metab, 98, 2725-33.
MÄNNISTÖ, T., MENDOLA, P., REDDY, U. & LAUGHON, S. K. 2013. Neonatal outcomes and birth weight in pregnancies complicated by maternal thyroid disease. American journal of epidemiology, 178, 731-740.
MARINE, D. & KIMBALL, O. 1920. Prevention of simple goiter in man: fourth paper. Archives of Internal Medicine, 25, 661.
MARWAHA, R., CHOPRA, S., GOPALAKRISHNAN, S., SHARMA, B., KANWAR, R., SASTRY, A. & SINGH, S. 2008. Establishment of reference range for thyroid hormones in normal pregnant Indian women. BJOG: An International Journal of Obstetrics & Gynaecology, 115, 602-606.
MCLEAN, E., COGSWELL, M., EGLI, I., WOJDYLA, D. & DE BENOIST, B. 2009. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005. Public Health Nutr, 12, 444-54.
MILLAR, L. K., WING, D. A., LEUNG, A. S., KOONINGS, P. P., MONTORO, M. N. & MESTMAN, J. H. 1994. Low birth weight and preeclampsia in pregnancies complicated by hyperthyroidism. Obstetrics & Gynecology, 84, 946-949.
MOLETI, M., LO PRESTI, V. P., MATTINA, F., MANCUSO, A., DE VIVO, A., GIORGIANNI, G., DI BELLA, B., TRIMARCHI, F. & VERMIGLIO, F. 2009. Gestational thyroid function abnormalities in conditions of mild iodine deficiency: early screening versus continuous monitoring of maternal thyroid status. Eur J Endocrinol, 160, 611-7.
MORENO-REYES, R., GLINOER, D., VAN OYEN, H. & VANDEVIJVERE, S. 2013. High prevalence of thyroid disorders in pregnant women in a mildly iodine-deficient country: a population-based study. The Journal of Clinical Endocrinology & Metabolism, 98, 3694-3701.

100
MORREALE DE ESCOBAR, G., JESUS OBREGON, M. A. & ESCOBAR DEL REY, F. 2000. Is Neuropsychological Development Related to Maternal Hypothyroidism or to Maternal Hypothyroxinemia? 1. Journal of Clinical Endocrinology & Metabolism, 85, 3975-3987.
NEGRO, R. & MESTMAN, J. H. 2011. Thyroid disease in pregnancy. Best Practice & Research Clinical Endocrinology & Metabolism, 25, 927-943.
NEGRO, R., SCHWARTZ, A., GISMONDI, R., TINELLI, A., MANGIERI, T. & STAGNARO-GREEN, A. 2010a. Increased pregnancy loss rate in thyroid antibody negative women with TSH levels between 2.5 and 5.0 in the first trimester of pregnancy. J Clin Endocrinol Metab, 95, E44-8.
NEGRO, R., SCHWARTZ, A., GISMONDI, R., TINELLI, A., MANGIERI, T. & STAGNARO-GREEN, A. 2010b. Increased pregnancy loss rate in thyroid antibody negative women with TSH levels between 2.5 and 5.0 in the first trimester of pregnancy. The Journal of Clinical Endocrinology & Metabolism, 95, E44-E48.
NEGRO, R., SCHWARTZ, A., GISMONDI, R., TINELLI, A., MANGIERI, T. & STAGNARO-GREEN, A. 2011. Thyroid antibody positivity in the first trimester of pregnancy is associated with negative pregnancy outcomes. The Journal of Clinical Endocrinology & Metabolism, 96, E920-E924.
NEGRO, R. & STAGNARO-GREEN, A. 2014. Clinical Aspects of Hyperthyroidism, Hypothyroidism, and Thyroid Screening in Pregnancy. Endocrine Practice, 1-34.
NHMRC. 2010. Iodine supplementation for pregnant and breastfeeding women. NHMRC PUBLIC STATEMENT [Online]. Available: http://www.nhmrc.gov.au/guidelines/publications/new45 [Accessed 25/11/2013].
OBREGON, M., CALVO, R., ESCOBAR DEL REY, F. & MORREALE DE ESCOBAR, G. 2007. Ontogenesis of thyroid function and interactions with maternal function.
OKEN, E., BRAVERMAN, L. E., PLATEK, D., MITCHELL, M. L., LEE, S. L. & PEARCE, E. N. 2009. Neonatal thyroxine, maternal thyroid function, and child cognition. J Clin Endocrinol Metab, 94, 497-503.
OMAR, S., HADJ, T. S., KANOUN, F., HAMMAMI, M., KAMOUN, S., BEN, R. N., FEKI, M., SLIMANE, H. & KAABACHI, N. 2010. [Erythrocyte abnormalities in thyroid dysfunction]. La Tunisie medicale, 88, 783-788.

101
ONG, G. S., HADLOW, N. C., BROWN, S. J., LIM, E. M. & WALSH, J. P. 2014. Does the thyroid-stimulating hormone measured concurrently with first trimester biochemical screening tests predict adverse pregnancy outcomes occurring after 20 weeks gestation? J Clin Endocrinol Metab, 99, E2668-72.
PANESAR, N., LI, C. & ROGERS, M. 2001. Reference intervals for thyroid hormones in pregnant Chinese women. Annals of Clinical Biochemistry, 38, 329-332.
PANTOPOULOS, K. 2004. Iron metabolism and the IRE/IRP regulatory system: an update. Ann N Y Acad Sci, 1012, 1-13.
PAPANIKOLAOU, G. & PANTOPOULOS, K. 2005. Iron metabolism and toxicity. Toxicology and applied pharmacology, 202, 199-211.
PATEL, J., LANDERS, K., LI, H., MORTIMER, R. H. & RICHARD, K. 2011. Thyroid hormones and fetal neurological development. Journal of Endocrinology, 209, 1-8.
PEARCE, E. N., PINO, S., HE, X., BAZRAFSHAN, H. R., LEE, S. L. & BRAVERMAN, L. E. 2004. Sources of dietary iodine: bread, cows’ milk, and infant formula in the Boston area. Journal of Clinical Endocrinology & Metabolism, 89, 3421-3424.
PHILLIPS, D. 1997. Iodine, milk, and the elimination of endemic goitre in Britain: the story of an accidental public health triumph. Journal of Epidemiology and Community Health, 51, 391-393.
PONKA, P., BEAUMONT, C. & RICHARDSON, D. R. 1998. Function and regulation of transferrin and ferritin. Semin Hematol, 35, 35-54.
POP, V. J., DE VRIES, E., VAN BAAR, A. L., WAELKENS, J., DE ROOY, H., HORSTEN, M., DONKERS, M., KOMPROE, I., VAN SON, M. & VADER, H. 1995. Maternal thyroid peroxidase antibodies during pregnancy: a marker of impaired child development? The Journal of clinical endocrinology and metabolism, 80, 3561-3566.
RASMUSSEN, N. G., HORNNES, P. J., HEGEDÜS, L. & FELDT-RASMUSSEN, U. 1989. Serum thyroglobulin during the menstrual cycle, during pregnancy, and post partum. Acta endocrinologica, 121, 168-173.

102
REID, S. M., MIDDLETON, P., COSSICH, M. C. & CROWTHER, C. A. 2010. Interventions for clinical and subclinical hypothyroidism in pregnancy. Cochrane Database Syst Rev, 7.
RICHARDS, P. & STATHAM, M. 2007. Iodine deficiency in grazing livestock in Tasmania: thyroid hormone activity in the newborn foal.
RICHARDS, P. A. 1995. Iodine nutrition in two Tasmanian cultures. Medical Journal of Australia, 163, 628-630.
RICHARDS, P. A. C. & STEWART, J. C. 2007. Goitre Monitor: The History of Iodine Deficiency in Tasmania, Foot & Playsted Pty, Limited.
ROMÁN, G. C., GHASSABIAN, A., BONGERS‐SCHOKKING, J. J., JADDOE, V. W., HOFMAN, A., RIJKE, Y. B., VERHULST, F. C. & TIEMEIER, H. 2013. Association of gestational maternal hypothyroxinemia and increased autism risk. Annals of neurology, 74, 733-742.
ROVET, J., EHRLICH, R. & SORBARA, D. 1987. Intellectual outcome in children with fetal hypothyroidism. The Journal of Pediatrics, 110, 700-704.
SACHDEV, H., GERA, T. & NESTEL, P. 2005. Effect of iron supplementation on mental and motor development in children: systematic review of randomised controlled trials. Public health nutrition, 8, 117-132.
SARKAR, D. 2012. Recurrent pregnancy loss in patients with thyroid dysfunction. Indian J Endocrinol Metab, 16, S350-1.
SAVAGE, D. G., OGUNDIPE, A., ALLEN, R. H., STABLER, S. P. & LINDENBAUM, J. 2000. Etiology and diagnostic evaluation of macrocytosis. The American journal of the medical sciences, 319, 343-352.
SCHNEUER, F. J., NASSAR, N., TASEVSKI, V., MORRIS, J. M. & ROBERTS, C. L. 2012. Association and predictive accuracy of high TSH serum levels in first trimester and adverse pregnancy outcomes. J Clin Endocrinol Metab, 97, 3115-22.
SCHOLL, T. O. & HEDIGER, M. L. 1994. Anemia and iron-deficiency anemia: compilation of data on pregnancy outcome. The American journal of clinical nutrition, 59, 492S-500S discussion 500S.

103
SIAH, C. W., OMBIGA, J., ADAMS, L. A., TRINDER, D. & OLYNYK, J. K. 2006. Normal iron metabolism and the pathophysiology of iron overload disorders. Clinical Biochemist Reviews, 27, 5.
SIEGA-RIZ, A. M., HARTZEMA, A. G., TURNBULL, C., THORP, J., MCDONALD, T. & COGSWELL, M. E. 2006. The effects of prophylactic iron given in prenatal supplements on iron status and birth outcomes: a randomized controlled trial. American journal of obstetrics and gynecology, 194, 512-519.
SOLDIN, O. P. & SOLDIN, S. J. 2011. Thyroid hormone testing by tandem mass spectrometry. Clinical Biochemistry, 44, 89-94.
SOLDIN, O. P., TRACTENBERG, R. E., HOLLOWELL, J. G., JONKLAAS, J., JANICIC, N. & SOLDIN, S. J. 2004. Trimester-specific changes in maternal thyroid hormone, thyrotropin, and thyroglobulin concentrations during gestation: trends and associations across trimesters in iodine sufficiency. Thyroid, 14, 1084-90.
STAGNARO-GREEN, A. 2011. Overt hyperthyroidism and hypothyroidism during pregnancy. Clin Obstet Gynecol, 54, 478-87.
STAGNARO-GREEN, A. 2012. Optimal care of the pregnant woman with thyroid disease. The Journal of Clinical Endocrinology & Metabolism, 97, 2619-2622.
STAGNARO-GREEN, A., ABALOVICH, M., ALEXANDER, E., AZIZI, F., MESTMAN, J., NEGRO, R., NIXON, A., PEARCE, E. N., SOLDIN, O. P. & SULLIVAN, S. 2011. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid, 21, 1081-1125.
STAGNARO-GREEN, A., CHEN, X., BOGDEN, J. D., DAVIES, T. F. & SCHOLL, T. O. 2005. The thyroid and pregnancy: a novel risk factor for very preterm delivery. Thyroid, 15, 351-357.
STRICKER, R., ECHENARD, M., EBERHART, R., CHEVAILLER, M., PEREZ, V., QUINN, F. & STRICKER, R. 2007. Evaluation of maternal thyroid function during pregnancy: the importance of using gestational age-specific reference intervals. European Journal of Endocrinology, 157, 509-514.
SU, P. Y., HUANG, K., HAO, J. H., XU, Y. Q., YAN, S. Q., LI, T., XU, Y. H. & TAO, F. B. 2011. Maternal thyroid function in the first twenty weeks of pregnancy and subsequent fetal and infant development: a prospective

104
population-based cohort study in China. J Clin Endocrinol Metab, 96, 3234-41.
TAUROG, A. 2000. Hormone synthesis: thyroid iodine metabolism. Werner & Ingbar’s The Thyroid: a fundamental and clinical text. 8th ed. Philadelphia: Lippincott, Williams & Wilkins, 61-85.
TEMPLE, R. 1999. The Sirius Mystery, Random House.
THUNG, S. F., FUNAI, E. F. & GROBMAN, W. A. 2009. The cost-effectiveness of universal screening in pregnancy for subclinical hypothyroidism. American journal of obstetrics and gynecology, 200, 267. e1-267. e7.
TOULIS, K. A., STAGNARO-GREEN, A. & NEGRO, R. 2014. Maternal subclinical hypothyroidsm and gestational diabetes mellitus: a meta-analysis. Endocr Pract, 20, 703-14.
TRIPATHI, R., TYAGI, S., SINGH, T., DIXIT, A. & MALA, Y. 2012. Clinical evaluation of severe anemia in pregnancy with special reference to macrocytic anemia. Journal of Obstetrics and Gynaecology Research, 38, 203-207.
TRUMBO, P., YATES, A. A., SCHLICKER, S. & POOS, M. 2001. Dietary reference intakes: vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. Journal of the American Dietetic Association, 101, 294-301.
TUDELA, C. M., CASEY, B. M., MCINTIRE, D. D. & CUNNINGHAM, F. G. 2012. Relationship of subclinical thyroid disease to the incidence of gestational diabetes. Obstet Gynecol, 119, 983-8.
TUDHOPE, G. & WILSON, G. 1960. Anaemia in hypothyroidism: incidence, pathogenesis, and response to treatment. Quarterly Journal of Medicine, 29, 513-537.
VAIDYA, B., ANTHONY, S., BILOUS, M., SHIELDS, B., DRURY, J., HUTCHISON, S. & BILOUS, R. 2007. Detection of thyroid dysfunction in early pregnancy: universal screening or targeted high-risk case finding? Journal of Clinical Endocrinology & Metabolism, 92, 203-207.
VAIDYA, B., HUBALEWSKA-DYDEJCZYK, A., LAURBERG, P., NEGRO, R., VERMIGLIO, F. & POPPE, K. 2012. Treatment and screening of

105
hypothyroidism in pregnancy: results of a European survey. European Journal of Endocrinology, 166, 49-54.
VAN DEN BOOGAARD, E., VISSENBERG, R., LAND, J. A., VAN WELY, M., VAN DER POST, J. A., GODDIJN, M. & BISSCHOP, P. H. 2011. Significance of (sub)clinical thyroid dysfunction and thyroid autoimmunity before conception and in early pregnancy: a systematic review. Hum Reprod Update, 17, 605-19.
VAN DER WEYDEN, M. B. & CAMPBELL, L. 1988. Clinching the diagnosis: macrocytic anemia. Pathology, 20, 353-7.
VANDERPAS, J. 2006. Nutritional epidemiology and thyroid hormone metabolism. Annu. Rev. Nutr., 26, 293-322.
VANDERPUMP, M. 2010. The epidemiology of thyroid disease. British medical bulletin, 99, 39-51.
VERMIGLIO, F., LO PRESTI, V. P., MOLETI, M., SIDOTI, M., TORTORELLA, G., SCAFFIDI, G., CASTAGNA, M. G., MATTINA, F., VIOLI, M. A., CRISA, A., ARTEMISIA, A. & TRIMARCHI, F. 2004. Attention deficit and hyperactivity disorders in the offspring of mothers exposed to mild-moderate iodine deficiency: a possible novel iodine deficiency disorder in developed countries. J Clin Endocrinol Metab, 89, 6054-60.
VERMIGLLO, F., PRESTI, V., ARGENTINA, G. S., FINOCCHIARO, M., GULLO, D., SQUATRITO, S. & TRIMARCHI, F. 1995. Maternal hypothyroxinaemia during the first half of gestation in an iodine deficient area with endemic cretinism and related disorders. Clinical endocrinology, 42, 409-415.
VILA, L., VELASCO, I., GONZALEZ, S., MORALES, F., SANCHEZ, E., TORREJON, S., SOLDEVILA, B., STAGNARO-GREEN, A. & PUIG-DOMINGO, M. 2014. Controversies in endocrinology: On the need for universal thyroid screening in pregnant women. Eur J Endocrinol, 170, R17-30.
VITTI, P., DELANGE, F., PINCHERA, A., ZIMMERMANN, M. & DUNN, J. T. 2003. Europe is iodine deficient. The Lancet, 361, 1226.
VOUGHT, R. L. & LONDON, W. T. 1967. Iodine intake, excretion and thyroidal accumulation in healthy subjects. J Clin Endocrinol Metab, 27, 913-9.

106
WALFISH, P. G., GINSBERG, J., ROSENBERG, R. A. & HOWARD, N. J. 1979. Results of a regional cord blood screening programme for detecting neonatal hypothyroidism. Archives of disease in childhood, 54, 171-177.
WHO, U. 2001. ICCIDD (2001) Assessment of the iodine deficiency disorders and monitoring their elimination. WHO, Geneva, 1-107.
WILSON, R. E., SALIHU, H. M., GROER, M. W., DAGNE, G., O’ROURKE, K. & MBAH, A. K. 2014. Impact of Maternal Thyroperoxidase Status on Fetal Body and Brain Size. Journal of Thyroid Research, 2014.
WORLD HEALTH ORGANIZATION, W. 2007. Assessment of iodine deficiency disorders and monitoring their elimination: a guide for programme managers.
WORLD HEALTH ORGANIZATION, W. 2013. Urinary iodine concentrations for determining iodine status in populations.
WU, L., SAZALI, B., ADEEB, N. & KHALID, B. 1999. Congenital hypothyroid screening using cord blood TSH. Singapore medical journal, 40, 23-26.
YASSA, L., MARQUSEE, E., FAWCETT, R. & ALEXANDER, E. K. 2010. Thyroid hormone early adjustment in pregnancy (the THERAPY) trial. Journal of Clinical Endocrinology & Metabolism, 95, 3234-3241.
YUE, B., ROCKWOOD, A. L., SANDROCK, T., LA'ULU, S. L., KUSHNIR, M. M. & MEIKLE, A. W. 2008. Free thyroid hormones in serum by direct equilibrium dialysis and online solid-phase extraction--liquid chromatography/tandem mass spectrometry. Clin Chem, 54, 642-51.
ZIMMERMANN, M., ADOU, P., TORRESANI, T., ZEDER, C. & HURRELL, R. 2000. Persistence of goiter despite oral iodine supplementation in goitrous children with iron deficiency anemia in Cote d'Ivoire. The American journal of clinical nutrition, 71, 88-93.
ZIMMERMANN, M. B. 2008. Methods to assess iron and iodine status. Br J Nutr, 99 Suppl 3, S2-9.
ZIMMERMANN, M. B. 2009. Iodine deficiency. Endocrine reviews, 30, 376-408.
ZIMMERMANN, M. B. 2010. Symposium on 'Geographical and geological influences on nutrition' Iodine deficiency in industrialised countries. The Proceedings of the Nutrition Society, 69, 133-43.

107
ZIMMERMANN, M. B. & HURRELL, R. F. 2007. Nutritional iron deficiency. The Lancet, 370, 511-520.
ZIMMERMANN, M. B. & KÖHRLE, J. 2002. The impact of iron and selenium deficiencies on iodine and thyroid metabolism: biochemistry and relevance to public health. Thyroid, 12, 867-878.

108
Appendices Appendix 1: Invitation form

109
Appendix 2: Information sheet and consent form

110

111

112
Appendix 3: Questionnaire

113

114

115