Embed Size (px)
Citation preview

dental radiology
JOHN W. PREECE, D.D.S. American Academy of Dental Radiology Depurtment of Dental Diagnostic Sciences School of Dentistry, The University of Texas Health Science Center at Sun Antonio 7703 Floyd Curl Dr. Sun Antonio, Texas 78284
An investigation of potential applications of intensifying screens in intraoral radiography R. G. Stephens, D.D.S., M.Sc.,* S. L. Kogon, D.D.S., M.Sc.,** and J. A. Reid, D.D.S., F.A.A.D.R.,*** London, Ontario, Canada
DEPARTMENT OF ORAL MEDICINE, FACULTY OF DENTISTRY, UNIVERSITY OF WESTERN ONTARIO
In medicine, the somewhat degraded image from the screen/film system is accepted for most diagnostic purposes in the interest of radiation thrift. In dentistry, however, the superb image resolution and sharpness of the radiation-intensive, direct-exposure film is the standard for intraoral radiography. There may be occasions in dental practice where such quality is not necessary, thus making the high level of exposure difficult to justify. In a laboratory study, screen-type radiographs were effectively substituted for ultraspeed film in the monitoring stages of endodontic therapy and as posttreatment films in operative dentistry. Even with a slow system, the radiation exposure was one sixteenth of the usual periapical dose If clinical trials support these conclusions, only the lack of a practical periapical cassette limits the application of this significant method of radiation reduction to dental practice.
T here are few instances in medical radiology when images are formed solely by direct exposure of film to x-ray photons. Such use is restricted by the prohibitively large radiation doses required. Tradi- tionally, intensifying screens have been used to substantially reduce radiation by employing the property of fluorescence to expose light-sensitive radiographic film. It takes significantly fewer x-ray photons to produce the fluorescent effect and subse- quent exposure of the film by visible light than to produce a latent image by direct exposure to x-rays. With suitable screen/film combinations, x-ray doses of one fifteenth to one fiftieth or less will darken film
This research was supported in part by Ontario Ministry of Health Grant No. M322A5. *Professor, Division of Oral Radiology. **Associate Professor and Chairman, Division of Oral Medi- cine. ***Professor and Chairman, Division of Oral Radiology.
0030.4220/82/ I10591 + 06$00.60/O @ 1982 The C. V. Mosby Co.
to a given density compared to the direct-exposure method.’ Although intensifying screens inevitably cause some degradation in the quality of the image, the dramatic radiation reduction is an accepted exchange for virtually all diagnostic purposes in medicine.
In dentistry, we have become accustomed to the fine detail and exceptional image sharpness of direct-exposure intraoral film. However, cephalome- try and recently pantomography, both of which use intensifying screens, have made us more accustomed to examining images of lesser resolution and sharp- ness. These films are perfectly acceptable when used appropriately. The degraded image inherent in screen/film systems has undoubtedly been a limiting factor in considering this technique for intraoral radiography. Another drawback to the intraoral use of intensifying screens is the lack of a suitable periapical-size cassette. In order to be effective, intensifying screens must be in intimate contact with
591

592 Stephens, Kogon, and Reid Oral Surg. November. 1982
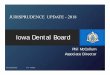
Fig. 1. Periapical view on direct-exposure film of an upper premolar with trial files in position (A). The superb resolution and sharpness of the intracanal image are evident. In B, the high subject contrast permits the location of file tips despite the loss of quality in the screen/film image.
Table I. Technique data
Timer E.S.E. Film I Screen /~~~~kVp~rnA~~??~~t$ / Generator accuracy (mRI
Kodak DF-57 No screen 96 S. S. White Spacemaker 184 Cronex 2DC Cronex speed 6
70 IO 40 par 90 long-beam tube
t 1 pulse/set. 11.5
the film.’ Traditionally, this has been achieved by pressing the screen and film together in a spring- loaded rigid casing. Although miniaturization of the standard cassette is probable, at this time cassettes suitable for periapical use are not commercially available. In addition to the customary rigid cassette, medical radiography has developed, for certain pro- cedures, a flexible cassette system. The screen/film combination is placed in an opaque plastic pouch with close contact achieved by evacuating the air and sealing the open end. With the use of this vacuum sealing method, it is possible to produce cassettes of any size.
These two factors, degradation of the image and lack of a suitable cassette, have established direct- exposure film as the standard for intraoral radiogra- phy.
Radiographs are essential diagnostic aids, and
their accurate interpretation is a prerequisite to correct treatment decisions. In intraoral radiogra- phy, the base line for radiographic quality is the direct-exposure film. However, there are occasions in dental therapy when radiographs are taken not for their diagnostic value but to assist in monitoring techniques. In addition, radiographs may be used to assess the development of teeth and their eruption, determine the seating of intra- or extracoronal attachments, satisfy third-party requests, and a vari- ety of other reasons which could be broadly classified as nondiagnostic. Some of these radiographs, while important, may not be retained and are of no long-term value to the patient or the dentist. If it could be shown that substitution of screen/film images for these purposes would not mislead the dentist or prejudice treatment, considerable radia- tion reduction could be effected. To give some

Volume 54 Number 5
Potential applications of intensifying screens 593
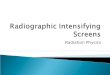
Fig. 2. Radiographs illustrate the trial file and final obturation steps in endodontic technique. A and B, Monitoring films using the screen/film combinations. C and D, Direct-exposure control films.
perspective to this reduction, a single direct-exposure periapical film taken at 70 kVp under optimum conditions may have an entrance skin exposure of approximately 180 to 230 mR.* That is about six times the entrance skin exposure of a standard chest radiograph with screen-type film and is sixteen times the amount of radiation needed to expose one periap- ical film with a slow screen/film system.
In the last 5 years there have been dramatic innovations in intensifying screen technology. Numerous screens, some using rare earth phosphors and having a variety of physical characteristics, are available.2*3 From this wider range of screens, it should be possible to select a screen/film combina- tion to produce an image which, although not as sharp as that on the direct-exposure film, might safely be used, at least in nondiagnostic instances.
This laboratory study was designed to test the use of a screen/film combination in two types of restor- ative treatment. First, endodontic procedures were
*This range applies to generators in the Division of Oral Radiol- ogy. Measurements were made with a Keithley digital dosime- ter.
performed on human necropsy specimens with screen-type film as the working or monitoring radio- graph, and, second, the capability of the system in disclosing overhanging or ill-fitting margins of resto- rations was evaluated. In addition, the potential of the flexible vacuum-sealed cassette for intraoral use was examined.
METHOD
With the use of necropsy material, endodontic procedures were performed on fifteen single- and multi-rooted teeth. The specimens were set in clear casting resin* and trimmed flat to a thickness of 25 mm. to simulate soft-tissue scatter and to aid in orientation. The endodontic technique used in these tests is taught at the University of Western Ontario, Faculty of Dentistry. Biomechanical preparation was carried to within 1 mm. of the radiographic apex. Both gutta-percha and silver point obturations were performed. Radiographs using the selected screen/ film system were made at the following stages of endodontic treatment: working length determination
*Lewiscraft Co., Toronto, Ontario, Canada.

594 Stephens, Kogon, and Reid Oral Surg. November. 1982
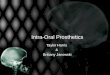
Fig. 3. Typical amalgam extrusions on the mesial and distal are shown in the screen/film image in A and in the direct-exposure image in B.
with a 20/ 1 OOmm. diameter endodontic file in place, master point fit, and final obturation. At each of these stages a control radiograph using direct- exposure film was made. These controls were not processed until treatment was completed. All treat- ment decisions and technique adjustments were made by reference only to the screen/film image. Therefore, the final obturation was the result of information derived solely from the screen/film sys- tem.
The screen/film combination selected has been used for many years in dental pantomography. A Cronex* Par Speed screen was combined with Cro- nex 2DC film. The screen phosphor is calcium tungstate rated at medium speed. Cronex 2DC is a high-contrast, low-speed film. This combination is often used as the reference (1 X speed) when rating the relative speed of screen/film systems.2 A 5 by 12 inch spring-loaded rigid metal cassette provided the screen/film contact. The limiting resolution of the screen/film combination was measured at seven line pairs per millimeter by means of the x-ray test pattern model 07-553 type 53G.t The control films were Kodak Ultra-Speed DF57, speed D intraoral film. The generator produced an entrance skin expo- sure of 184 mR in 96 impulses. This exposure
*Cronex is a trade mark of E. I. DuPont de Nemours and Company, Wilmington. Del. f’Nuclear Associates, Inc.. Westbury, N. Y.
provided acceptable image densities in the diagnostic range of 0.25 to 2.00. The technique data are shown in Table I. To obtain equivalent diagnostic densities with the screen/film system, an exposure time of six impulses was needed. Densities were measured with a direct-reading densitometer (MacBeth Quanta- Log). The timer was checked for accuracy by the spinning-top method. All films were processed in an S. S. White Auveloper at 25.6” C with a 41/2-minute cycle. The radiographs were viewed in a darkened room with light-shielding frames at 2.5 x magnifica- tion.
To demonstrate the potential role of screen film in other monitoring situations, the test combination was used to show interproximal metallic overhangs. These tests were carried out on prepared natural teeth in sawdust blocks.
RESULTS AND DISCUSSION
Endodontic technique was chosen as the study model because it clearly demonstrates the role of diagnostic and monitoring radiographs. The preoper- ative or diagnostic film must be highly detailed so that the clinician can evaluate the patency of the root canals, the presence of lateral canals, dilacerations, root anomalies, and fractures. Currently, only the direct exposure film can satisfy these requirements. All subsequent films can be termed monitoring or working films. These films are used to visualize the relative position of the opaque file, master point or

Volume 54 Number 5
Potential applications of intensifying screens 595
final obturation in relation to the radiolucencies of the root canal, and the apical periodontal ligament space. This intracanal image exhibits a high degree of subject contrast which we believed might compen- sate for the loss of sharpness inherent in the screen/ film system (Fig. 1). The monitoring film is an aid in determining the root canal length (which may require more than one radiograph if difficulties are encountered) and in confirming the length and fit of the master point. Finally, the consistency, homogene- ity, and position of the obturation are evaluated. Acceptance or correction of the file or master point location is largely dependent on radiographic inter- pretation and therefore critical to the success of the final obturation.
In this study the screen/film image, without exception, was sufftciently sharp to permit accurate estimation of root canal length, guide adjustments of trial files, evaluate the fit of the master cone or silver point, and record the completed obturation. These observations were confirmed by reference to the control films (Fig. 2). In spite of the degraded shadows of the adjacent tissues, the intracanal image was sufficiently sharp to make technique decisions essential to good endodontic treatment. One must not allow the less sharp images of the surrounding trabeculae, cortical bone, crown outline, and other features to detract from the primary intent of the film, which is assessment of the intracanal image. The encouraging results of this study suggested that a clinical trial of a screen/film system for monitoring endodontic treatment was indicated. This work is currently in progress.
In the restorative phase of the study deliberately created inadequacies of amalgam restorations were readily detected in the images on screen-type film (Fig. 3).
Even if proved effective in clinical trials, the incorporation of screen/film systems into general use will be hindered by the lack of a suitable periapical cassette. Unfortunately, cassettes would have to be individually prepared, as the cost of intensifying screens makes their use in a disposable format prohibitive. There have been attempts to fabricate periapical cassettes. 4, 5 The principal difficulty in making a small cassette is the need to incorporate some means of obtaining close screen/film contact (Fig. 4). Traditionally, this adaptation has been achieved by mechanically pressing the screen against the film in a spring-activated rigid cassette. Minia- tures of this kind are not available. An occlusal-size cassette has been marketed but proved to be flimsy and therefore unreliable. More recently the vacuum method has been used to provide the necessary
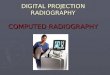
Fig. 4. Radiographs of the test pattern were made with the screen/film system in a periapical-size cassette designed for extraoral use (Condy-ray, Rinn Corp., Elgin, Ill.). In A, resolution of seven line pairs per millimeter was achieved by using the vacuum method of obtaining inti- mate screen/film contact. In B, film and screens were firmly packaged but without vacuum. Resolution is 2.9 line pairs per millimeter. Gross image unsharpness is evident.
contact in a flexible cassette (Fig. 5). This system is well established in medicine, and its intraoral use has been reported in dentistry.s A Picker-Amplatz* unit applying this principle can fabricate flexible intra- oral cassettes of any size. However, the capital cost is so great that its routine use is impractical at the moment.
Increasing concern over population exposure to ionizing radiation has induced the dental profession to investigate several approaches to decreasing patient dosage. Advancements in equipment and films and more discrimination in patient selection have contributed to a general improvement in the risk/benefit ratio. In an attempt to explore the possibility of a further substantial reduction in radi- ation exposure, the potential role of screen/film systems in intraoral radiography has been exam- ined.
It should be quite clear that this study was not an attempt to show that intraoral screen/film systems can yield images comparable in resolution and sharp- ness with those of the direct-exposure film. This cannot be done. However, the price exacted for the exceptional image quality of the nonscreen film is a high relative level of patient exposure. In the wide
*Picker International Corporation, White Plains, N. Y.

596 Stephens, Kogon, and Reid Oral Surg. November, 1982
Fig. 5. Screen/film radiographs of the final obturation of the premolar shown in Fig. 1, comparing image qualities of the rigid pressure-type cassette (A) with the vacuum-pouch cassette (B).
spectrum of dental diagnosis and treatment there are some situations in which the fine detail and sharp- ness of the direct-exposure film may not be essential. If it can be shown by clinical trials that the screen/ film system can be used without risk to the patient, then the reduction in exposure would represent an outstanding contribution to radiation safety. This should induce the profession and the industrial com- munity to develop a practical intraoral cassette for general dental use.
CONCLUSIONS
1. The screen/film system used in this laboratory study required only one sixteenth of the radiation needed to produce image densities equivalent to these on direct-exposure periapical film. For a patient, this would represent a substantial reduction in expo- sure.
2. The somewhat degraded image inherent in the screen/film system was quite adequate for its moni- toring role in the endodontic procedures completed.
3. The screen-type film image was effectively used to detect a range of overhanging margins of restorations in extracted teeth.
4. Screen/film combinations, vacuum-sealed in flexible pouches, produce images of sharpness to equal that of radiographs exposed in traditional rigid cassettes.
5. Clinical trials of the effectiveness of screen/ film systems in nondiagnostic situations are recom- mended.
The authors thank Mr. D. Dwyer, a senior dental student, for preparations of specimens.
REFERENCES
I.
2.
3.
4.
5.
Christensen, E. E., Curry, T. S., and Dowdey, J. E.: An Introduction to the Physics of Diagnostic Radiology, ed. 2, Philadelphia. 1978, Lea & Febiger, Publishers, pp. 145, 116. Skucas, J., and Gorski, J.: Application of Modern Intensifying Screens in Diagnostic Radiology, Med Radiogr. Photogr. 56: 25-36, 1980. Rao, G. U. V.. Fatouros, P. P., and James, A. E.: Physical Characteristics of Modern Radiographic Screen-Film Sys- tems, Invest. Radiol. 13: 460-469, 1978. Dawood, F. F., and Manson-Hing, L. R.: Evaluation of New Radiographic Screens for Intraoral Radiography, ORAL SURG. 48: 178-186, 1979. Okano, T., and Inoue, T.: Introduction of the Intensifying Screen in Intraoral Radiography, J. Stomatol. Sot. Jap. 44: 492, 1977.
Reprint requests to: Dr. R. G. Stephens Division of Oral Radiology Faculty of Dentistry The University of Western Ontario London, Ontario N6A, 5B7, Canada