Embed Size (px)
Citation preview

An inpatient treatment model for adults with mild
intellectual disability and challenging behaviour
K. I. Xenitidis, J. Henry, A. J. Russell, A. Ward & D. G. M. Murphy
The Maudsley and Bethlem Royal NHS Trust, and Department of Psychological Medicine, Institute of Psychiatry, London, UK
Abstract
Following the closure of the large mental handicap
hospitals in the UK, the majority of people with intellectual
disability (ID) are currently living in the community.
However, people with ID who also exhibit challenging
behaviour (CB) have been the most difficult-to-place group
and use a large amount of service resources. A variety of
service options have been proposed for the assessment
and treatment of CBs, but there is little information on the
effectiveness of these alternatives. The Mental Impairment
Evaluation and Treatment Service (MIETS) is one of these
service options and the aim of the present study is to
describe and evaluate this service. The present authors
studied the first 64 patients admitted to MIETS following
its opening. A within-subject comparison research design
was used. Demographic and clinical data were obtained
from case records and the effectiveness of MIETS
interventions was evaluated by comparing the number of
incidents of challenging behaviour, the use of seclusion, and
the place of residence before and after the MIETS
intervention. Only 10 (17.5%) of the patients had been
admitted from community facilities, but 48 (84.2%) of the
patients were discharged to community placements
(P < 0.0001). The MIETS also significantly reduced the
frequency and severity of challenging behaviours
(P < 0.0001). It is concluded that the MIETS is an effective
treatment model for people with ID and CB, and that
there is no place for therapeutic nihilism in this difficult-to-
place group of patients.
Keywords challenging behaviour, inpatienttreatment model, service evaluation
Introduction
Challenging behaviour (CB) in people withintellectual disability (ID) has been defined as`culturally abnormal behaviour(s) of such intensity,frequency or duration that the physical safety of theperson or others is likely to be placed in seriousjeopardy, or behaviour which is likely to seriouslylimit or delay access to and frequent use of ordinarycommunity facilities' (Emerson 1995). In recentyears, service provision for people with ID hasundergone dramatic changes in the UK; it hasshifted from institutional settings towards care in thecommunity under the influence of the philosophy ofnormalization and the deinstitutionalizationmovement (Wolfensberger 1972; King's FundCentre 1987). In particular, the provision of servicesfor people with ID and mental health problems orCB has been the subject of research and debate, anda variety of service models have been proposed(Gravestock & Bouras 1995; Bouras et al. 1995; Day1994). However, CBs have been a significantobstacle to resettlement in the community, and a
Correspondence: Dr Kiriakos Xenitidis, Department of Psychological
Medicine, Institute of Psychiatry, De Crespigny Park, Denmark Hill,
London SE5 8AF, UK. E-mail: [email protected]
# 1999 Blackwell Science Ltd
Journal of Intellectual Disability Research
VOLUME 43 PART 2 pp 128±134 APRIL 1999128

frequent cause of requests for admission or re-admission to hospitals (Mansell 1994). Following theclosure of the large mental handicap hospitals, avariety of alternative services have been developedfor patients who are difficult to place because oftheir CBs. Service models include community-basedteams (Allen & Lowe 1995), specialist staffed houses(Emerson et al. 1992) or in-patient hospital units(Hoefkens & Allen 1990). These servicedevelopments have exposed the high cost to theNational Health Service (NHS) and the socialservices of caring for people with ID and CB.Currently, the NHS spends over £600 million onservices for people with ID. In addition, localauthorities spend approximately £400 million (AuditCommission 1992). The proportion of thisexpenditure generated by people exhibiting CB isestimated to be at least 5.7% of that budget (i.e. £57
million) since the prevalence of CB in people withID has been estimated at between 5.7% (Qureshi &Alborz 1992) and 14% (Borthwick-Duffy 1994).However, little information is currently available onthe effectiveness of the various alternative in-patientservice options.
The Mental Impairment Evaluation andTreatment Service (MIETS) is a 13-bed in-patientunit situated at the Bethlem Royal Hospital, Kent,UK, which offers a multidisciplinary assessment andtreatment service for people with mild to moderateID and severe CB. Its origin and philosophy, and aninitial evaluation of its first years of operation havealready been published (Murphy et al. 1991; Murphy& Clare 1991). Since the publication of these earlystudies, the MIETS model has evolved and a muchlarger number of patients have had completedadmission episodes in the unit. The aims of thepresent study were to: (1) describe the demographicand clinical characteristics of the users of theMIETS service; and (2) determine the effectivenessof the unit in reducing levels of CB and resettlingpatients into the community.
Method
Population and data collection
All case notes of patients admitted to MIETS sinceits opening in May 1987 were examined and datawere systematically collected on:
1 personal characteristics (e.g. gender, age, ethnicbackground and intellectual level);
2 Admission and discharge data [e.g. referralquestions (reasons for referral), accommodationof origin, legal status on admission anddischarge placement]; and
3 Clinical data (e.g. frequency of incidents of CBand use of seclusion, additional psychiatric anddevelopmental disorders, and epilepsy).
Outcome measures
A within-subject (`before and after') comparisonresearch design was used.
Three main outcome measures were used tomeasure the effectiveness of the MIETSinterventions:
1 Improvement of patients' accommodation status.A good outcome was defined as admissionfrom a non-community setting (e.g. hospitals,Special Hospitals and prisons), but dischargeto a community setting (e.g. own home, orsheltered or other supported residentialfacility).
2 Reduction of frequency of aggression. The totalnumber of incidents recorded for each patientwas used as an indicator of behaviouraldisturbance. A baseline measurement ofbehavioural disturbance was obtained during a4-week assessment period between the sixth andtenth week after admission (weeks 6±10 wereselected to minimize the `honeymoon' effect).This baseline measurement was compared withthe total number of incidents recorded in thepost-treatment period of the last 4 weeks of thepatients' stay at MIETS. The unit's incidentreport forms, which were completed by nursing/care staff immediately after each incident, wereused as a record of CB.
3 Reduction of severity of aggression. The use ofseclusion was used as a proxy measure of theseverity of aggression. Measurements wererecorded during the same periods as describedabove, i.e. during weeks 6 and 10, and in thelast 4 weeks prior to discharge, and the samesources of information were used. Thedifficulties of using seclusion as a measure ofseverity of aggression are discussed below.
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
129

Statistical analysis
The discharge outcome data was analysed using theStatistical Package for Social Sciences (SPSS). Therelationship between origin and destination ofpatients and the significance of the differencesbetween the two groups of good and poor outcomewas examined using non-parametric statistics (chi-squared and McNemar's test).
Data pertaining to the reduction of CB wasanalysed using the STATA package. Rates of violentincidents and use of seclusion in the periods beforeand after the MIETS intervention were calculated,and the rate ratio was used as a measure of relativerisk to examine the difference between the `exposed'(post-treatment) and the `unexposed' (pre-treatment). As these rates may vary randomly andcluster in patients, poisson regression analysis wasused to yield the adjusted rate ratios.
Results
Sixty-four patients were admitted to MIETS duringthe period of the study.
Demographic and clinical characteristics
The patients were predominantly young Caucasianmales with a mean full-scale intelligence quotient(IQ) of 65 (range = 46±84, SD = 8.96). Themajority of the patients were admitted under asection of the Mental Health Act. The mostcommon type of CB was aggression, followed bysexual challenging behaviour and fire-setting. Mostpatients had had some contact with the law prior totheir admission to MIETS, and a significantminority had been in prison and/or Special Hospital.The majority of the patients had additional mentaldisorders and/or epilepsy superimposed on their ID(Table 1).
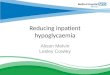
Placement at a community facility
Out of the 64 patients, 57 were included in thedischarge outcome analysis. Seven patients wereexcluded because five had too short a duration ofstay (less than 4 weeks) for any therapeuticintervention to take place, and discharge data wereunavailable or meaningless for two subjects. Out of
these 57 patients, 47 (82.5%) were admitted fromnon-community settings (e.g. hospitals, SpecialHospitals and prisons), whereas 10 (17.5%) wereliving in a community facility (e.g. own home, orsheltered or other supported residential facility) priorto admission. Nevertheless, following the MIETSintervention, 48 (84.2%) of the MIETS patientswere discharged to community facilities and nine(15.8%) to non-community placements. Out of the10 patients coming from community placements, allwere discharged to community placements. Out of
Table 1 MIETS patient characteristics (n = 64). For mean scores,
the range is shown in brackets
Characteristic Score
Mean age (years) 28 (17±46)
Gender:
male 46 (71.9%)female 18 (28.9%)
Ethnic origin:
Caucasian 51 (79.7%)
Afro-Caribbean 9 (14.1%)African 3 (4.7%)
Asian 1 (1.6%)
Mean duration of stay (months) 12.84 (0±29)Mean IQ 64 (46±84)
Legal status on admission:
informal 27 (42.2%)
formal:Section 2 37 (57.8%)
Section 3 1 (1.6%)
Section 35 10 (15.6%)
Section 37 10 (15.6%)Section 37/41 11 (17.2%)
Section 38 3 (4.7%)
Probation Order 1 (1.6%)Challenging behaviour:
aggression 25 (44.6%)
aberrant sexual behaviour 11 (19.6%)
fire-setting 10 (17.9%)self-injurious behaviour 4 (7.1%)
other 8 (14.3%)
Forensic history:
any involvement with the law 41 (64.1%)history of imprisonment 28 (43.8%)
Special Hospital admission 11 (17.2%)
Clinical conditions:
psychotic illness 31 (48.4%)non-psychotic 12 (18.8%)
no psychiatric diagnosis 11(17.2%)
autism 11 (17.2%)epilepsy 16 (25%)
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
130

the 47 patients admitted from non-communitysettings, 38 were discharged to community and nineto non-community settings (P < 0.0001) (Fig. 1).
This subsample of patients admitted from non-community (n = 47) was divided into two outcomegroups: good (discharged to community) and poor(discharged to non-community settings). Thedifferences between the two groups were examinedin terms of demographic, clinical and behaviouralcharacteristics. Out of all the characteristicsexamined, the only statistically significant differencebetween the two groups was fire-setting behaviour.Those who were referred for fire-setting weresignificantly more likely to have a poor outcome interms of community placement (P < 0.05) (seeTable 2).
Reduction of frequency of aggression
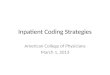
Out of the 64 patients, six were excluded from thisanalysis because five of them had not stayed longenough to have meaningful `before and after'measures, and data was missing for one patient. Therate of incidents before the MIETS intervention wascalculated for the 58 valid cases as 0.75 incidents perperson per week. The rate of incidents prior todischarge was 0.33 incidents per person per week.The rate ratio indicative of the MIETS treatmenteffect was then calculated at 0.45 (95% confidenceintervals = 0.34±0.58, P < 0.0001) (Fig. 2).
Reduction of the use of seclusion (a proxy forseverity of aggression)
Similarly, the rates of seclusion episodes before andafter the MIETS intervention were calculated at 0.15
and 0.04 incidents per person per week, respectively.The rate ratio was calculated as 0.24 (95%confidence intervals = 0.11±0.49, P < 0.0001)(Fig. 2).
Discussion
A variety of approaches have been used in themanagement of CB in people with ID. The earlyliterature focused mostly on pharmacotherapy andbehavioural therapy in the context of a mentalhandicap hospital ward. More recently, ascommunity care has been implemented, various
Origin
10
4760
50
Nu
mb
er o
f p
atie
nts
40
30
20
10
0
48
9
Destination
Figure 1 MIETS effect on accommodation status: (&) non-com-
munity; (&) community; and (*) P < 0.0001.
Table 2 Differences between the good versus poor outcome groups
(n = 47)
Outcome group
Characteristic Poor Good
Type of challenging behaviourAggressive:
no 5 17
yes 4 18Sexual:
no 7 30
yes 2 5
Fire-setting:no 5 32
yes 4 4
Self-injurious:
no 8 32yes 1 3
Other:
no 6 28yes 3 7
Demographic characteristicsGender:
no 8 26
yes 1 12
Mean age 27.56 28.76
Clinical characteristicsPsychosis:
no 3 16
yes 6 19
Autism:no 9 26
yes 0 7
Epilepsy:
no 6 25yes 3 11
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
131

community-based treatment models have beensuggested (Emerson et al. 1988) and communitychallenging behaviour teams (CBTs) have beendeveloped. However, there remained a core ofpatients whose treatment in the community was notpossible because of the nature and severity of theirCB. Increasing recognition of this problem has ledto the creation of special behavioural inpatient units,i.e. challenging behaviour units (CBUs). Bothcommunity CBTs and inpatient CBUs have theirsupporters and criticsÐmainly on clinical,ideological and economic grounds. The advantagesand disadvantages of the various specialized serviceshave been summarized by Newman & Emerson(1991).
MIETS was established by the South-east ThamesRegional Health Authority (SETRHA) in 1987 to assistin the community placement of people with mild andmoderate ID and CB. It provides a comprehensivemultidisciplinary assessment followed by activetreatment and placement recommendations. Themethod which MIETS has developed and uses is basedon the request from the referrers to formulate specificclinical questions (`referral questions'), and thequantification of each CB before and after anytherapeutic intervention. In this way, the referrers canexpect specific answers to their questions and the effectof the treatment can be measured and any changesclearly demonstrated. Treatment is based on theprinciples of sequential single hypothesis testing andfunctional analysis. To put it simply, a CB is assessedand quantified, hypotheses for the origin and functionof the behaviour are generated, and a single hypothesisis tested at a time. Therapeutic interventions differaccording to the individual patient's needs, and may bebehavioural, pharmacological, psychological or social.Thus, each patient receives an individualized treatment
programme and its effectiveness is constantlymonitored.
In the present study, community placement wasselected as a main outcome measure because MIETSitself originated from the need to assist the communityplacement of adults with ID and CB. This need wasalso reflected in the referral questions pattern since`placement recommendations' was an explicit requestat the point of admission for more than 50% of thepatients. Moreover, even for those patients for whom aplacement profile had not been explicitly requested, itis probable that its development was an implicitexpectation of the referrers for their patients. In termsof outcome, although the majority of the MIETSpatients were discharged to community facilities, thismay not be a specific MIETS effect. Rather, it mayreflect the change of philosophy towards communitycare, and the willingness of the local authorities toaccept people with ID and CB in communityplacements. However, this is unlikely to be the wholeexplanation for the successful community placementof most patients because a significant decrease in CBwas also achieved. When the two good and pooroutcome groups were examined, the onlycharacteristic that differed significantly between thetwo groups was fire-setting behaviour. Thischaracteristic was significantly commoner in the pooroutcome group. Of course, this result may reflect thereluctance of the community to tolerate individualswith a history of fire-setting. The difficulties posed bysmall numbers also need to taken into account.
This is a retrospective cohort study and inherentto its design is the limitation of the retrospectivecollection of data relying basically on the patient'scase notes. In terms of outcome data, it has to benoted that the focus was on changes in aggressivebehaviour, although other types of CB occurred.This was not only because aggressive CB was thecommonest CB given as a reason for referral, butalso because there are relatively few opportunities toobserve and measure change in other behaviours,such as sexual CB and fire-setting, in the setting ofan inpatient unit. A further difficulty of the presentstudy lies in the use of seclusion as a proxy measureof severity of aggression. Although the severity of aparticular aggressive incident is one of the factorswhich may lead to seclusion, other factors likepatient characteristics and environmental variables(Rangecroft et al. 1997) clearly play a role as well.
0.8 0.75
0.33
CB incidentsrate ratio 5 0.45*
Seclusion episodesrate ratio 5 0.24*
0.15
0.04
Rat
es (
inci
den
ts o
f C
Bp
er p
erso
n/w
eek)
0.6
0.4
0.2
0
Figure 2 MIETS effect on challenging behaviour: (&) pre-treat-
ment; (&) post-treatment; and (*) P < 0.0001.
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
132

Although MIETS is clinically effective, inpatientservices can be relatively expensive. However, astudy on the cost effectiveness of MIETS (Dockrellet al. 1995) concluded that `the high cost of the timein MIETS may be a good investment when seen inthe dynamic context of the costs and quality of lifeopportunities of the subsequent care'. Nevertheless,the present authors are seeking ways to reduce thecost by reducing the length of inpatient stay, an issuewhich was raised in an earlier study on MIETS(Gaskell et al. 1995). Thus, the present authors arecurrently carrying out a placebo-controlled trial ofthe ability of a nurse-led MIETS outreach team toreduce the length of inpatient stay by a pre-admission community intervention programme.
Finally, the current study did not attempt toaddress the question of how long patients remainedin their community placements after discharge fromMIETS. Thus, the present authors cannot make anyrecommendations on the generalizability of theirtreatment outcomes to other settings or the stabilityof these results over time. However, these questionsare the subject of ongoing follow-up research.Nevertheless, the present authors have demonstratedthat significant clinical improvement can be achievedin people with ID and CB, and that there is no roomfor therapeutic nihilism in this difficult-to-placegroup of patients.
Acknowledgements
We wish to thank all those who worked hard to developthe MIETS service, particularly Drs L.B. Campbell, T.Holland, G. Murphy and I. Clare. We are also gratefulto Dr Jan Neeleman for his extremely helpfulcomments on methodological issues and KorneliaKampmann for her assistance with data collection.
Dr K. Xenitidis was supported by a trainingfellowship (Health Services Research) from theSouth Thames NHS Executive.
References
Allen D. & Lowe K. (1995) Providing intensive communitysupport to people with learning disabilities andchallenging behaviour: a preliminary analysis ofoutcomes and costs. Journal of Intellectual DisabilityResearch 39, 57±82.
Audit Commission (1992) Community Care: Managing theCascade of Care. HMSO, London.
Borthwick-Duffy S. A. (1994) Prevalence of destructivebehaviors. In: Destructive Behavior in DevelopmentalDisabilities: Diagnosis and Treatment (eds T.Thompson & D. B. Gray), pp. 3±23. Sage, ThousandOaks, CA.
Bouras N., Holt G. & Gravestock S. (1995) Communitycare for people with learning disabilities: deficits andfuture plans. Psychiatric Bulletin 19, 134±7.
Day K. (1994) Psychiatric services in mental retardation:generic or specialised provision? In Mental Health inMental Retardation (ed. N. Bouras), pp. 328±40.Cambridge University Press, Cambridge.
Dockrell J. E., Gaskell G., Normand C. & Rehman H.(1995) An economic evaluation of the resettlement ofpeople with learning disabilities and challengingbehaviour. Social Science in Medicine 7, 895±901.
Emerson E. (1995) Challenging Behaviour. Analysis andIntervention in People with Learning Difficulties. CambridgeUniversity Press, Cambridge.
Emerson E., Beasley F., Offord G. & Mansell J. (1992) Anevaluation of hospital-based specialised housing forpeople with seriously challenging behaviours. Journal ofIntellectual Disability Research 36, 291±307.
Emerson E., Cummings R., Barrett S., Hughes H.,McCool C. & Toogood A. (1988) Challenging behaviourand community services: Who are the people whochallenge services? Mental Handicap 16, 16±19.
Gaskell G., Dockrell J. & Rehman H. (1995) Communitycare for people with challenging behaviours andlearning disability: an evaluation of an assessment andtreatment unit. British Journal of Clinical Psychology 34,
383±95.
Gravestock S. & Bouras N. (1995) Services for adults withlearning disabilities and mental health needs. PsychiatricBulletin 19, 288±90.
Hoefkens A. & Allen D. (1990) Evaluation of a specialbehaviour unit for people with mental handicaps andchallenging behaviour. Journal of Mental DeficiencyResearch 34, 213±28.
King's Fund Centre (1987) Facing the Challenge; AnOrdinary Life for People with Learning Difficulties andChallenging Behaviour. King's Fund, London.
Mansell J. (1994) The challenge of providing high qualityservices. In: Mental Health in Mental Retardation (ed. N.Bouras), pp. 328±40. Cambridge University Press,Cambridge.
Murphy G. & Clare I. (1991) MIETS: a service optionfor people with mild mental handicaps andchallenging behaviour or psychiatric problems. 2.Assessment, treatment, and outcome for service usersand service effectiveness. Mental Handicap Research 4,
180±206.
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
133

Murphy G., Holland A., Fowler P. & Reep U. (1991) MIETS: aservice option for people with mild mental handicaps andchallenging behaviour or psychiatric problems. 1. Philosophy,service and service users. Mental Handicap Research 4, 41±66.
Newman I. & Emerson E. (1991) Specialised treatmentunits for people with challenging behaviours. MentalHandicap 19, 113±19.
Qureshi H. & Alborz A. (1992) Epidemiology of challengingbehaviour. Mental Handicap Research 5, 130±45.
Rangecroft M. E. H., Tyrer S. P. & Berney T. P. (1997)The use of seclusion and emergency medication in ahospital for people with learning disability. British Journalof Psychiatry 170, 27±37.
Wolfensberger W. (1972) The Principle of Normalization inHuman Services. National Institute on MentalRetardation, Toronto.
Received 9 July 1998; revised 1 October 1998
Journal of Intellectual Disability Research VOLUME 43 PART 2 APRIL 1999
K. I. Xenitidis et al . Mild intellectual disability and challenging behaviour
# 1999 Blackwell Science Ltd, Journal of Intellectual Disability Research 43, 128±134
134