Embed Size (px)
Citation preview

Scand J Thor Cardiovasc Surg 23: 33-37, 1989
AN IN VITRO STUDY OF PROSTHETIC HEART VALVE SOUND
Lars I . Thulin,' Helmut Red, ' Martin Giersiepen' and Christian L . O h '
From the 'Department of Cardiothoracic Surgery, University Hospital, Lund, Sweden and 'Helmholtz Institute for Biomedical Engineering, Aachen, West Germany
(Accepted for publication September 15, 1988)
Abstract. Patients with an implanted mechanical heart valve sometimes experience the closing sounds of the valve as dis- turbing. To study the generation of valve sounds in general. a pulse duplicator study was carried out. testing eight com- monly used types of prosthetic valves in the aortic position. Pulse rate was set at 70 beatshin, stroke volume at 7 0 ml and mean 'aortic' pressure at 100 mmHg. Despite the con- trolled conditions, there was great variability of the closing sound. in both intensity and spectral composition, making noise comparisons and spectral characterization (kono- print') difficult. In general, bileaflet mechanical valves pro- duced less noise than did tilting disc valves, particularly those with large opening angles. One small-size (23 mm) tilting disc valve produced 50% less noise than large types. The plastic ball valve, the porcine and the polyurethane trileaflet valve all were very quiet.
Key words: heart valve prostheses, valve sound, noise, in vitro study, pulse duplicator, sound spectroanalysis.
In contrast to native human heart valves, most mech- anical heart valve prostheses produce distinct metal- lic sounds when they open and close. The closing sound often is the louder. This sound, when experi- enced by the patient as disturbing, can also be characterized as noise, and can undoubtedly affect the quality of life after otherwise successful valve surgery. In a survey of 281 patients with one or more implanted mechanical heart valves (Bjork-Shiley or St. Jude), 8% claimed that they were often disturbed and 25% that they were sometimes disturbed by the valve sounds (11).
Depending on the patient's constitution, heart rhythm, hearing acuity and environmental factors, subjective perception of the valve noise can vary ( 5 , 6). In order to study the generation of prosthetic valve sounds in general, and to compare different prostheses in standardized test conditions, we per- formed an in vitro pulse duplicator study.
MATERIAL A N D METHODS Testing conditions Eight different heart valve prostheses, usually of 27 mm size, were studied (Table I ) . The tests were performed at the Helmholtz Institute for Biomedical Engineering in Aachen, using a previously described (8) pulse duplicator system (Fig. I ) . All prostheses (including a polyurethane valve) were studied in the aortic position. A polyurethane valve (3). which generated almost no noise, was used in the mitral position as a standard. An aqueous glycerol solution with viscosity 3.6 cp (similar to that of human blood) was used as test fluid. The net forward stroke volume was set at 70 ml and the 'aortic' mean pressure at 100 mmHg (Table 11). As a certain degree of leakage was incorporated in the design of some of the evaluated prostheses, t h e pump stroke volume had to be correspondingly increased in these test runs to compensate for the leak flow. The pulse rate was set at 70/min. In a second test series, the pulse rate was increased to l00lmin and the mean 'aortic' pressure to 110 mmHg.
Sound-recording system A microphone (Electrovoice 635 A) was placed 10 cm from the aortic test chamber (Fig. 2). The sounds were recorded with a NAGRA 3 tape recorder on audiotape PER 525. The
Table I . Functional characteristics of the tested valves
Size Opening Valve name Type (mm) angle
Omniscience Tilting disc 27 80" Hall-Kaster Tilting disc 27 75" Bjork-Shiley convexo- concave Tilting disc 27 60"
Bjork-Shiley Monostrut Tilting disc 27 70" Bjork-Shiley Monostrut Tilting disc 23 70" Duromedics Bileaflet 27 76" St. Jude Medical Bileaflet 27 85" Starr-Edwards Plastic ball 27 - Polyurethane (Aachen design) Plastic trileaflet 27 -
Carpentier-Edwards Porcine bio- 27 - prosthesis
3-898241 Scand J Thor Cardrovasc 23
Scan
d C
ardi
ovas
c J
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Bro
wn
Uni
vers
ity L
ibra
ry o
n 08
/25/
12Fo
r pe
rson
al u
se o
nly.

34 L. I . Thulin et al.
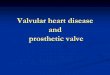
Fig. I. Hydraulic analogue model of the left heart and sys- temic circulation (Helmholz Institute. Aachen). 1, aortic valve; 2, rigid aortic root; 3, electromagnetic flow probe; 4, characteristic resistance; 5, adjustable compliance; 6, peripheral resistance; 7. adjusting mechanism for 6; 8, fluid reservoir; I I , left atrium; J2. mitral valve; 13. elastic ven- tricular sac; 24, rigid plexiglass housing; 15, hydraulic pumps; 15 a, low-pressure piston; 1.5 6 , high-pressure pis- ton; 15 c. electromagnetic servovalve.
Table 11. Tesr conditions
Test Chamber amplifier computer plotter
analyser oscilloscope
Fig. 2. Schematic presentation of recording system
dB I
60-
* O L 0 16 63 250 l k 4k 16k Hz
frequency
Fig. 3. Digital frequency analysis of closing sound of the 27 mm Bjork-Shiley Monostrut valve (mean of 18-20 beats).
valve closing sound, together with the aortic pressure curve. was visually displayed on an oscilloscope which was filmed with a Grundig videocamera. Furthermore, spectro- analysis was made of each valve beat and displayed sepa- rately on another oscilloscope.
Valve sound analysis When the pulse duplicator system had been adjusted to pro- duce the predetermined flow and pressure, 25 consecutive beats were recorded and filmed. The valve opening sounds were found to be faint and were not further analyzed.
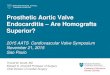
For analysis of the closing sounds of the prosthesis, a di- gital frequency analyzer (Bruel & Kjaer 2131) was used. The analyzer selected 16 sec (corresponding to 18-20 beats) and displayed the results as mean sound intensity (in dB) in re- lation to sound frequency (in kHz). as shown in Fig. 3.
To eliminate the noise produced by the pulse duplicator itself, and to obtain a basis for comparisons of different prostheses, the sound generated by the polyurethane valve in aortic position was used as 0 reference. From the sound spectrum curves a sound index was calculated (Fig. 4). using the difference between the tested valve and the polyurethane valve in the sound frequency area perceived by the human ear (100 Hz-16 kHz). The area between the two curves was planigraphically measured and the smallest area was arbitrarily set as 100 units.
1. Valves in aortic position 2. Net forward stroke volume 70 ml 3. Mean 'aortic' pressure 100 mmHg RESULTS 4. Pulse rate 70 beatslmin 5. Microphone placed 1Ocm from the test chamber
Despite the seemingly controlled conditions, the valve closing sounds varied considerably in both
Scand I Thor Cardiovasc 23
Scan
d C
ardi
ovas
c J
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Bro
wn
Uni
vers
ity L
ibra
ry o
n 08
/25/
12Fo
r pe
rson
al u
se o
nly.

In vitro study of prosthetic heart valve noise 35
dB i ,valve at test
60- polyurethane
0 ' HZ 100 250 lk 4k 16k
frequency
zoL/. Fig. 4. The area between the two curves represents the sound index. Smallest observed area set as 100 units.
intensity and spectral appearance (Fig. 5). The bi- leaflet valves often produced double closing sounds with varying distance between the sound peaks. Sur- prisingly, even the disc valves had considerable beat- to-beat difference, sometimes displaying two compo- nents of the closing sound-ne weak and one strong (Fig. 6). The same observation was made in another study (9). Direct comparison of the intensity of clos- ing sound from the different mechanical prostheses was therefore difficult. In general, however, the clos- ing sounds of the bileaflet valves were weaker than those of the tilting disc valves.
The closing-sound intensity of the mechanical valves was dependent on many factors, including valve size. Thus the 23 mm Bjork-Shiley Monostrut valve produced about 50% less sound than did the 27 mm Monostrut valve in identical conditions, using the sound index for comparison. Another seemingly important factor was the backward velocity of the test fluid in the aorta a t the moment of valve closure. Prostheses with a large opening angle produced more sound than those with a small opening angle.
The Starr-Edwards prosthesis generated very little noise in these experiments. The occluder, a silicon ball, produced only a soft sound when returning to the valve ring during closure.
The only tested biologic valve (Carpentier-Ed- wards), and the polyurethane valve (produced by the Helmholtz Institute) were both very quiet. and the closing sounds were almost undetectable on the oscil- loscope.
DISCUSSION
That many patients with an implanted mechanical heart valve are disturbed by sounds from the valve is
unquestioned. In the aforementioned survey of 281 patients (Il) , performed 2.5 years postoperatively, disturbance from the mechanical valve sounds was described as serious by 2 % , frequent by 6% and oc- curring in certain situations by 25%. The perception of valve sound varied with factors such as heart rhythm (patients with atrial fibrillation being more disturbed than those with sinus rhythm), hearing acuity (less disturbance in old than in young pa- tients) and various environmental factors (disturb- ance as a rule greater in a quiet environment).
Although a pulse duplicator study in controlled conditions eliminates patient-related factors, i t intro- duces other disturbing elements. Most important of these is the noise of the pulse duplicator itself, in- cluding vibrations and resonance in the system (7) . In the present study it was not possible to distinguish the sound produced by the prosthesis as such from that of the pulse duplicator system, but the 'sound index' was helpful in eliminating at least some of the basic noise generated by the system.
In all the tested mechanical valves there was sur- prising beat-to-beat variability of the closing sound, which impeded comparisons between valve types. Some conclusions were possible, however, viz. that more sound seemed to be generated by valves open- ing to large angles than by those with small opening angles, and by large as compared with small valves.
In addition to the described tests, we performed runs with higher mean 'aortic' pressure, i.e. 110 mmHg. In these experiments the intensity of the closing sounds was considerably (c. 20%) increased, indicating that the aortic pressure at the time of clo- sure is of definite importance for the intensity of sound. This tallies with the clinical observation that many patients are particularly disturbed by the valve noise when they feel 'nervous' o r perform physical work.
Echocardiography has proved ineffective for diag- nosis of early prosthetic valve malfunction (1. 2). Great value has instead been claimed for sound spectroanalysis of valve clicks (4, 10). However, our observations (wide variance of closing sound even under controlled conditions and even between indi- vidual beats of the same prosthesis), seem to raise serious doubts as to whether sound analysis can be of any true help in clinical practice. There appears to be no distinct 'sonoprint' characterizing a specific model or type, and generated sounds scem to be highly dependent on prevailing hemodynamic condi- tions.
Scund J T h r Cardiovasc 2.1
Scan
d C
ardi
ovas
c J
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Bro
wn
Uni
vers
ity L
ibra
ry o
n 08
/25/
12Fo
r pe
rson
al u
se o
nly.

36 L. I . Thulin et al.
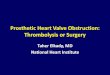
Bjork Shiley 60” CC 27 mm Bjork-%ley Monostrut 27 rnrn Omniscience 27 mm Hall-Kaster 27 mm
St Jude Medical 27 mrn Duromedicr 27 mm Biork Shiley Monostrut 23 mm
Fig. 5. Examples of closing sound of different tested valves (single beat), demonstrating some characteristics of inten- sity and spectral appearance.
The findings in the present study should be cau- tiously interpreted and are not directly applicable to clinical situations. Technical factors such as reso- nance in the pulse duplicator system, transmission of
the generated sounds, etc. can distort results in such experiments. Furthermore, individual patient char- acteristics add complexity to the generation and per- ception of valve sounds in clinical settings.
Fig. 6. Three consecutive beats of a 27 mm Bjork-Shiley Monostrut prosthesis. demonstrating two components of the closing sound and differences in sound intensity and
spectral appearance. Arrows indicate the first component of the closing sound in two of the beats.
Scand J Thor Cardrovasc 23
Scan
d C
ardi
ovas
c J
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Bro
wn
Uni
vers
ity L
ibra
ry o
n 08
/25/
12Fo
r pe
rson
al u
se o
nly.

REFERENCES 1. Balkoura-Christpoulos MH, Resnekov L, Kittle CF.
Malfunction of a disc valve prosthesis. Detection by phonocardiography. Chest 1973; 63: 624.
2. Demany MA, Zimmerman HA. Thrombosis of a mi- tral disc valve prosthesis. Diagnostic importance o f the absent opening click. Am Heart J 1970; 80: 816.
3. Herold M, Lo HB, Reul H, Muckter H, Taguchi K, Giersipen M. Birkle G, Hollweg G, Rau G , Messmer BJ. The Helmholtz-Institute trileaflet polyurethane- heart valve prosthesis: design, manufacturing and first in-vitro and in-vivo results. In: Planck H et al. (eds.) 1987. Polyurethanes in Biological Engineering 11. Elsevier Science Publishers BV, Amsterdam.
4. KagawaY, Sato N. Nitta S , HongoT.Tanaka M. Mohri H. Horiuchi T. Real-time sound spectroanalysis for diagnosis of malfunctioning prosthetie valves. J Thorac Cardiovasc Surg 1980; 79: 671-679.
5 . Kupari M, Harjula A, Mattila S. Auscultatory charac- teristics of normally functioning Lillehei-Kaster, Bjork- Shiley, and St Jude heart valve prostheses. Br Heart J 1986; 55: 364-370.
In vitro study of prosthetic heart valve noise 37
6. Meno F. Reddv PS. Bernardi L. Heart sound Dropa-
7 .
8.
9.
10.
gation in the human thorax. Clin Phys Physiol'Meas 1985; 6: 123-129. Olin CL. Pulsatile flow studies of prosthetic aortic valves. Scand J Thor Cardiovasc Surg 1971; 5: 1-12. Reul H. Giersiepen M. Knott E. Laboratory testing of prosthetic heart valves. Engineering in Medicine 1987; 16: 67-76. Schondube F, Keusen H, Messmer BJ. Physical anal- ysis of the Bjork-Shiley prosthetic valve sound. J Thorac Cardiovasc Surg 1983; 86: 136141. Soubank DW. Yoganathan AP, Harrison EC. Corcoran WH. A quantitative method for the in vitro study of sounds produced by prosthetic aortic heart valves. Part 111: an experimental comparative study of the sounds produced by normal and simulated-abnormal Smeloff aortic prostheses. Medical and Biological Engineering and Computing 1984; 22: 48-54.
11. Thulin L. Quality of life after heart valve replacement with mechanical prostheses. Quality of Life and Car- diovascular Care, Winter 1987/Spring 1988; 4: 3744 .
S c a d J Thor Cardiovasc 23
Scan
d C
ardi
ovas
c J
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Bro
wn
Uni
vers
ity L
ibra
ry o
n 08
/25/
12Fo
r pe
rson
al u
se o
nly.