Embed Size (px)
Citation preview

1
QUEENSLAND UNIVERSITY OF TECHNOLOGY
SCHOOL OF PHYSICAL AND CHEMICAL SCIENCES
AN IMRT CLASS SOLUTION FOR PATIENTS WITH SKIN LESIONS OF THE TEMPLE REGION THAT HAVE SPREAD TO THE PAROTID GLAND
February 2006
Submitted by Amy O’Rourke to the School of Physical and Chemical Sciences, Queensland University of
Technology in fulfillment of the requirements of the degree of Masters of Applied Science (Research)

2
ABSTRACT
Patients with skin lesions of the temple region that have spread to the parotid gland are
commonly treated with three-dimensional conformal radiation therapy (3DCRT).
3DCRT has associated limitations when treating this disease. 3DCRT requires this
disease site to be treated with two junction regions, resulting in poor dose conformity
to the tumour target. Proximity of critical structures to the target volume can make
dosimetry difficult, “especially for concave-shaped targets in close proximity to
sensitive normal structures” (Saw.C et al., 2002, p76).
Intensity modulated radiation therapy (IMRT) is a relatively new treatment technology
that has potential to overcome limitations associated with 3DCRT (Garden.A et al.,
2004). IMRT has been reported to have significant advantages over conventional
3DCRT treatment, by improving dose to the tumour and lowering doses to critical
structures (Adams.E et al., 2001).
Research has been conducted into the optimal IMRT treatment for specific head and
neck carcinomas. They are identified as class solutions. “A class solution can be
defined as the historical experience in designing RT plans for a particular site”
(Intensity Modulated Radiation Therapy Collaborative Working, 2001, p913).
This study was performed to establish an optimal IMRT class solution for patients with
skin lesions of the temple region that have spread to the parotid gland, and to determine
if it is the superior treatment option over 3DCRT treatment. Dosimetry planning was
performed on computerised tomography data sets of nine patients with this disease site.
One optimised 3DCRT dosimetry plan and eight optimised IMRT plans with specific
beam arrangements were calculated. Clinical and statistical analysis was performed
on; critical structures, conformity indices (CI) and dose volume histogram (DVH)
range analysis of the planning target volume (PTV).

3
Analysis of IMRT plans revealed that the 7-beam arrangement and 4-beam ipsilateral
arrangement produced significantly lower doses to the majority of critical structures
(P<0.05). The 7-beam IMRT arrangement produced the best and second best CI and
DVH PTV results, but these were not significantly different to the majority of other
beam arrangements. This indicates that the 7-beam arrangement with defined beam
angles of; 40°,120°,160°,200°,240°,300°,0°, is the superior IMRT treatment plan, and
thus class solution for this disease site. Clinical analysis confirmed results.
Analysis was performed on IMRT class solution results compared with 3DCRT results.
CI was significance higher and DVH PTV range was significantly lower for the IMRT
class solution (P<0.05). The class solution delivered significantly higher doses to the
majority of critical structures in comparison to the 3DCRT plan (P<0.05). This
indicates that the IMRT class solution is superior to 3DCRT in terms of PTV
conformity and homogeneity, but not in terms of doses to critical structures.
Skin lesions of the temple region with tumour extension to the parotid gland, is a
complicated disease site. Investigations into current and potential radiation therapy
treatments will guide treatment options and facilitate outcomes for patients with this
disease.

4
CONTENTS Title Page 1 Abstract 2 Contents 4 List of Figures 7 List of Tables 9 Statement of Original Authorship 10 Acknowledgments 11 Introduction 12 1.1 Introduction 12 1.2 Aims 13 1.3 Hypothesis 13 Background Literature Review 14 2.1 Current Radiation Therapy Procedure 14 2.2 Incidence and Survival of Disease 14 2.2.1 Incidence of Malignant Parotid Primary 14
2.2.2 Incidence of Temple Skin Primary 17 2.2.3 Incidence and Survival of Disease at the Royal Brisbane and 19 Women’s Hospital (RBWH)
2.3 Treatment Options and Survival 19 2.4. Anatomy of the Parotid Gland and Surrounding Structures 21
2.4.1 Lymph Supply 23 2.5 Stabilisation 25 2.6 Prescription Terminology 25 2.7 Surrounding Anatomical Critical Structures 26 2.8 Radiation Tolerances of Critical Structures 31 2.9 Radiation Treatment Technique Transition 35 2.10 3DCRT Limitations 36 2.10.1 3DCRT and Critical Structure Limitations 36
2.10.2 IMRT Overcoming Critical Structure Limitations 37
2.10.3 3DCRT and Monoisocentric Junctions 40 2.10.4 3DCRT and Junction Limitations 41 2.10.5 IMRT Overcoming Junction Limitations 46
2.11 Radiation Doses 47
2.12 Beam Arrangements 48 2.12.1 Beam Arrangements Using 3DCRT 48 2.12.2 Beam Arrangements Using IMRT 49
2.13 Class Solutions and Benefits 51 2.14 Summary 51

5
Method and Materials 53 3.1 Sample Group 53 3.2 Personnel 54 3.3 Equipment 55 3.4 Data Collection Procedure 57 3.4.1 Patient Positioning 57 3.4.2 Computerised Tomography (CT) Scanning Procedure 57 3.4.3 Planning Target Volume (PTV) Acquisition 58 3.4.4 Dose Prescribing 58 3.5 Plan Dosimetry 59 3.6 Critical Structures 60 3.6.1 Outlining Critical Structures 60 3.7 Beam Arrangements 61 3.7.1 3DCRT Beam Arrangements 61 3.7.2 IMRT Beam Arrangements 64 3.8 Dose Volume Histograms 65 3.9 Ethics Approval-RBWH/QUT 66 3.10 Analysis of Results 67 3.10.1 Bland and Altman 67 3.10.2 DVH Range Analysis on PTV 67 3.10.3 Mean Doses 67 3.10.4 Conformity index (CI) 68 3.10.5 Statistical Analysis 68 Results 70 4.1 Computerised Tomography (CT) data 70 4.2 Volume Structure Analysis 70 4.2.1 Structure Volumes 70 4.2.2 Bland and Altman Analysis 71 4.3 3DCRT Dosimetry 73 4.4 Conformity Index (CI) 74 4.4.1 Repeated Measures Anova on CI 74 4.5 DVH Range Analysis of the PTV 76 4.6 Mean Doses 77 4.6.1 Mean Contralateral Parotid Gland Dose 79 4.6.2 Mean Maximum Brain Dose 79
4.6.3 Mean Maximum Brainstem Dose 80 4.6.4 Mean Maximum External Auditory Meatus Dose 80 4.6.8 Mean Maximum Ipsilateral Lens Dose 81 4.6.6 Mean Maximum Contralateral Lens Dose 81 4.6.7 Mean Maximum Ipsilateral Retina/optic Nerve Dose 82 4.6.8 Mean Maximum Contralateral Retina/optic Nerve Dose 82 4.6.9 Mean Maximum Optic Chiasm Dose 83 4.6.10 Mean Maximum Oral Cavity Dose 83 4.6.11 Mean Maximum Spinal Cord Dose 84

6
4.7 Grouped Results 84 4.8 Radiation Oncologist Clinical Analysis of IMRT Plans 86 4.9 IMRT Vs 3DCRT 86 4.9.1 CI 87 4.9.2 DVH Range Analysis of the PTV 89 4.9.3 Critical Structure Analysis 89 4.10 Radiation Oncologist Clinical Analysis of 3DCRT and 7-beam 91 IMRT plans Discussion 92 5.1 Structure Volume Analysis 92 5.2 3DCRT Dosimetric Considerations 93 5.3 IMRT Dosimetric Considerations 95 5.4 DVH Range Analysis of the PTV 96 5.5 IMRT CI Analysis 97 5.6 IMRT Critical Structure Analysis 98 5.7 IMRT Mean Contralateral Parotid Dose 99 5.8 Superior IMRT Plan 99 5.9 IMRT Class Solution 100 5.10 IMRT Vs 3DCRT 101 5.11 Radiation Oncologist Clinical Preference 102 5.12 Future Directions 103 Conclusion 105 References 107 Appendices 114 Appendix A Documentation from Nucletron Pty Ltd confirming free
software supply for a period of 90 days 114 Appendix B Ethics approval confirmation from Professor W Egerton of
the RBWH Human Ethics Research Committee 115 Appendix C QUT email confirming ethical issues were uncompromised 116

7
LIST OF FIGURES Figure Description Page
1. Patients’ age at time of death from non-melanoma skin cancer, between 1994-1998 18 2. Pie graph demonstrating location of primary lesions causing death
after metastasising 18 3. Surgical reconstruction of disease in temple region and parotid
region 20 4. Anatomical position of the parotid gland 22 5. Facial nerve passing through the parotid gland 23 6. Lymphatics of the parotid gland and drainage towards the auricular
skin and temple scalp 24 7. Illustration detailing different volumes defined by ICRU 26 8. CT axial slice demonstrating position of the spinal cord and the
mandible 27 9. CT axial slice demonstrating position of the brainstem, parotids and
oral cavity 28 10. CT axial slice demonstrating position of the lenses, retina/optic
nerves and brain 29 11. CT axial slice demonstrating position of the optic chiasm 30 12. CT axial slice demonstrating position of the EAM 31 13. A transverse outline of a parotid patient showing the PTV
extending towards critical structures 37 14. Picture demonstrating IMRT plan Vs 3DCRT plan 38 15. Demonstration of superior and inferior asymmetric jaws 41 16. Photo of thermoplastic shell showing three separate treatment areas 42 17a.Photon isodose curve with straight edge penumbra 43 17b.Electron isodose curve with bulging penumbra 43 18a.Photo showing matching of the anterior oblique photon field to the
electron field on skin 44 18b.Photo showing matching of the posterior oblique photon field to
the electron field on skin 44 19. CT axial slice demonstrating spinal cord as the only critical
structure in the lower cervical photon field 46 20. Optimal IMRT class solution 50 21. Vacuum seal four point shell 55 22a.Lateral view of thermoplastic shell 55 22b.Anterior view of thermoplastic shell 55 23a.Siemens somatom sensation IV scanner 56 24. Standard dose prescription used at the RBWH 58 25. Wedge direction of anterior and posterior oblique fields 62 26. Photo of temple electron field matching on skin at the point where
the divergent edges of the oblique photon fields cross 63

8
27. Diagrammatic representation of IMRT beam angles for left sided lesion 65
28. 3DCRT dose volume histogram and summary output 66 29. Bland and Altman plot of body structure volumes 72 30. Graph of CI for each beam arrangement 74 31. Graph of Mean CI vs beam arrangement number 75 32a. Beam arrangement-3 demonstrating PTV conformity distribution 76 32b. Beam arrangement-9 demonstrating PTV conformity distribution 76 33. Graph of mean DVH PTV range vs beam arrangement number 77 34. Graph of mean contralateral parotid vs beam arrangement number 79 35. Graph of mean maximum brain dose vs beam arrangement number 79 36. Graph of mean maximum brainstem dose vs beam arrangement number 80 37. Graph of mean maximum eam vs beam arrangement number 80 38. Graph of mean maximum ipsilateral lens dose vs beam arrangement
number 81 39. Graph of mean maximum contralateral lens dose vs beam arrangement
number 81 40. Graph of mean maximum ipsilateral retina/optic nerve dose vs beam
arrangement number 82 41. Graph of mean maximum contralateral retina/optic nerve dose vs
beam arrangement number 82 42. Graph of mean maximum optic chiasm dose vs beam arrangement number 83 43. Graph of mean maximum doses to oral cavity vs beam arrangement number 83 44. Graph of mean maximum spinal cord dose vs beam arrangement number 84 45a&b. Improved CI is visualised by the 95% isodose line in the 7-beam
IMRT arrangement when compared to the 3DCRT plan 88 46a. DVH demonstrating 3DCRT distribution 89 46b. DVH demonstrating IMRT distribution 89 47a&b. Mean and mean maximum doses to critical structures for the
7-beam IMRT arrangement and the 3DCRT beam arrangement 90 48. DVH’s of 3DCRT plans from different CT data sets demonstrating
similarities in PTV 93 49. 3DCRT axial slice of junction region demonstrating poor coverage
of the PTV 94 50. DVH demonstrating compromise made when determining optimal
IMRT distribution 95 51a. DVH demonstrating 3DCRT distribution 97 51b. DVH demonstrating IMRT distribution 97 52a. 7 beam IMRT distribution demonstrating doses to critical structures 99 52b. Beam arrangement-5 IMRT distribution, demonstrating dose to
critical structures 99

9
LIST OF TABLES
Table Description Page
1 Incidence of various histopathological types of parotid 15 2 TNM classification for parotid carcinomas 6 3 Reported literature detailing radiation tolerances of head
and neck critical structures 32 4 Disease primary classification of patient data 54 5 Critical structures, tolerance and order of importance as determined
by radiation oncologist 60 6 Beam arrangement used on each CT data set 65 7 Beam arrangement number associated with beam arrangement 70 8 Comparison of structure volumes for one CT data set 71 9 Body structure volume data 71 10 Doses from 3DCRT plans with different photon-electron junction
matching techniques 73 11 Repeated measures ANOVA 78 12 Grouped results 85 13 Table demonstrating any significant difference between measures
of 3DCRT plans and the 7-beam IMRT arrangement 87

10
STATEMENT OF ORIGINAL AUTHORSHIP
“The work contained in this thesis has not been previously submitted for a degree or diploma at any other higher education institution. To the best of my knowledge and belief, the thesis contains no material previously published or written by another person except where due reference is made.”
Signed ………………………..
Dated ………………………..

11
ACKNOWLEDGEMENTS
I would like to thank the following people:
Ms Michelle Oppelaar, the supervisor of this study, for her continued encouragement
and feedback.
Mr Greg Rattray, for his continued time, knowledge and support.
Prof Brian Thomas, for his continued time and support especially with statistical
analysis in this research project.
Nucletron, for assistance and use of software that made this study possible.
Royal Brisbane and Women’s Hospital, for the use of equipment and data that made
this study possible.
My family and friends, for their encouragement.

12
CHAPTER 1 INTRODUCTION
1.1 INTRODUCTION
An area treated with radiation therapy is skin carcinoma of the temple region that has
spread to the parotid gland. The conventional radiation therapy treatment procedure
involves three-dimensional conformal radiation therapy (3DCRT). At the Royal
Brisbane and Women’s Hospital in Brisbane (RBWH) of Queensland, eighty-six
patients were treated with 3DCRT between 1998 and 2003 (RBWH, 2005).
3DCRT has associated limitations, especially when treating this disease. Proximity of
critical structures to the target volume can make dosimetry difficult. If the tumour
extends or curves around critical structures it is difficult to achieve the required dose to
the tumour while still keeping critical structures under dose tolerance.
In order to treat skin carcinomas of the temple region that have extended to the parotid
gland with 3DCRT, the treatment field must be divided into three areas, which results
in two junction regions. A 3DCRT treatment with more then one junction region can
cause underdosing and overdosing of the tumour target volume.
Intensity Modulated Radiation Therapy (IMRT) is a relatively new radiation treatment
technology. IMRT is an advanced form of 3DCRT that utilises modulated radiation
beam intensities. Some researchers suggest that “only a few meaningful retrospective
studies are available that show its potential and possible drawbacks” (Gregoire.V and
Maingon.P, 2004, p110). In contrast other researchers propose that IMRT may have
the potential to overcome limitations associated with 3DCRT (Garden.A et al., 2004).
IMRT has been reported to have significant advantages over conventional 3DCRT
treatment, by improving dose to the tumour and lowering doses to critical structures
(Adams.E et al., 2001).
Treating temple skin lesions with extensions to the parotid gland with IMRT enables
the treatment field to be divided into two areas, resulting in only one junction region.

13
This has the potential to reduce overdosing and underdosing. To treat this region with
IMRT, an optimum plan must be established.
Determining the optimum IMRT treatment plan demands a detailed process requiring
much research. The optimum IMRT treatment plan is identified as a class solution. A
class solution is defined as a solution that “consists of the criteria for optimisation and
the specification of the beam techniques used, typically including beam direction and
number” (Intensity Modulated Radiation Therapy Collaborative Working, 2001, p913).
1.2 AIM:
The aim of this study was to determine the optimal class solution for IMRT treatment
for patients who have skin lesions of the temple region with tumour extensions to the
parotid gland and determine if it is the superior treatment option over 3DCRT
treatment.
1.3 HYPOTHESIS:
The optimal IMRT class solution, for patients with temple skin lesions that extend to
the parotid gland, is the superior treatment modality. The IMRT class solution will
enable; avoidance of problems in the junction region and lower doses to critical
structures, allowing a potential increase in dose to the target volume and thus the
potential to increase local control.

14
CHAPTER 2 BACKGROUND LITERATURE REVIEW
2.1 Current Radiation Therapy Procedure Patients treated with radiation therapy for skin carcinomas of the temple region with
extensions to the parotid gland, undergo a standard treatment procedure. Patients
participate in a simulation procedure that can be reproduced for daily treatment. Data
is acquired for the radiation oncologist to define the tumour target and dose
prescription. Radiation therapists produce a radiation therapy plan with acquired data
in accordance with the dose prescription. Patients proceed to a course of fractionated
radiation therapy treatment. A standard fractionated course is 1 treatment/day, 5
days/week, for 6 weeks.
The above procedure is a simple overview that has many complicated steps. For this
research study, only steps that relate directly to, or impact on aims of this study will be
addressed.
2.2 Incidence and Survival of Disease
This research study is primarily concerned with tumour in the skin temple region and
in the parotid gland. The origin of this disease type may vary. The primary disease
may be in the parotid gland and spread to the skin of the temple region. Alternatively
the primary disease may be in the temple region, and spread to the parotid gland. The
incidence and survival data for both alternatives will be addressed.
2.2.1 Incidence of Malignant Parotid Primary
As malignant parotid tumour type and histology varies, it is difficult to find in the
literature incidence and survival rates for patients who have had spread of disease
specifically to the temple region. Incidence and survival data of malignant parotid
tumours, is well documented and provides a good indication of potential incidence of
spread of disease to upper skin regions.

15
Malignant tumours of the parotid gland are rare. “Malignant salivary gland neoplasms
constitute approximately 1% to 3% of all head and neck neoplasms”(Bhattacharyya.N
and Fried.M, 2005, p39). Parotid malignancies account for 50-70% of these salivary
gland neoplasms (Pohar.S et al., 2005). Incidence rates are nearly equal between
sexes. “Age standardised incidence rates per 100 000 for malignant salivary gland
tumours in the United States are 1.0 and 0.7 for males and females respectively”
(Zbaren.P et al., 2003, p57).
Malignant parotid carcinomas have large variations in histology, staging and clinical
behaviour. A study conducted in Sweden by Walhlberg et al, recorded the incidence of
various histopathological types of parotid carcinomas (Table 1).
Table 1-Incidence of various histopathological types of parotid cancer in Sweden 1960-1969, 1970-
1979, 1980-1989 and 1990-1995, respectively according to gender(Wahlberg.P et al., 2002, p707).
Malignant parotid carcinomas may present at different stages. Staging is used to define
the extent of disease. TNM classification is standardly used, and detailed in table 2.

16
Table 2-TNM classification for parotid carcinomas (Licitra.L et al., 2003, p219).
Primary Tumour (T) TX Primary tumour cannot be assessed T0 No evidence of primary tumour T1 Tumour 2 cm or less in greatest dimension without
extraparenchymal extension T2 Tumour more than 2 cm but not more than 4 cm in
greatest dimension without extraparenchymal extension T3 Tumour having extraparenchymal extension without seventh
nerve involvement and/or more than 4 cm but not more than 6 cm in greatest dimension
T4 Tumour invades base of skull, seventh nerve, and/or exceeds 6 cm in greatest dimension
Regional Lymph Nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Metastasis in a single ipsilateral lymph node, 3 cm or less in
greatest dimension N2 Metastasis in a single ipsilateral lymph node, more than 3 cm
but not more than 6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N2a Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension
N2b Metastases in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension
N2c Metastases in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N3 Metastasis in a lymph nodes more than 6 cm in greatest dimension Distant Metastases (M) MX Distant metastases cannot be assessed M0 No distant metastases M1 Distant metastases
Patterns of spread for malignant carcinomas are difficult to predict because of diverse
biological behaviour (Harish.K, 2004). Due to low incidence rates, varying
histopathological types, staging and routes of spread, survival statistics are minimal.
This fact is supported by many researchers,

17
“Overall rarity, determination of survival statistics and predictive factors
influencing survival has been largely dependent on single institutional series
spanning multiple decades. Most such series have been somewhat limited by
sample size and by their retrospective analysis. In addition, the wide variety of
histoplathologies that may be encountered in salivary gland malignancy
contributes to variability in survival” (Bhattacharyya.N and Fried.M, 2005,
p39).
2.2.2 Incidence of Temple Skin Primary
Skin lesions of the temple region may be the primary disease that spreads to the parotid
gland. The majority of primary skin lesions are non-melanoma skin cancers (NMSC)
which are comprised of 80% basal cell carcinomas (BCC) and 20% squamous cell
carcinomas (SCC) (Barzilai.G et al., 2005). Other less common non-melanoma skin
lesions are: merkel cell carcinoma, kaposi’s sarcoma and lymphoproliferative disorders
(Nolan.R et al., 2005).
For Caucasians the life time risk of a SCC is 8-11% and for BCC is 28-33% (Lai.S and
Weber.R, 2004). Australia has the highest reported incidence of SCC in the world,
estimated to be 205 per 100 000 population annually (Khurana.V et al., 1995). A study
by Nolan et al was conducted in Western Australia. This study determined that
“during the five years of 1994 and 1998, 120 patients died of NMSC” (Nolan.R et al.,
2005, p103). These deaths occurred mainly in the elderly (Figure 1).

18
Figure 1- Figure demonstrating patients’ age at time of death from non-melanoma skin cancer,
between 1994-1998. Grey bars=all deaths, black bars=comorbidities leading to immune deficiency
(Nolan.R et al., 2005, p103).
At the RBWH between 1998 and 2000, 498 men and 272 women had primary skin
lesions treated by the oncology department (RBWH, 2003). These statistics are for
skin lesions in general. This research is concerned with skin lesions of the temple
region. Unfortunately, RBWH statistics do not break down to skin site. Nolan et al
presented breakdown statistics on primary lesion site (Figure 2).
Figure2- Pie graph demonstrating location of primary lesions causing death after metastasising
(Nolan.R et al., 2005, p104).

19
NMSC lesions have a high probability of spread to the parotid and neck region. The
result of this spread is the particular area of interest in this research project. “The
occult metastases rate in the neck in the presence of metastases in the parotid gland
was 20%” (Barzilai.G et al., 2005, p855).
2.2.3 Incidence and Survival of Disease at the Royal Brisbane and Women’s
Hospital (RBWH)
Incidence and survival rates for patients who have been treated at the RBWH for skin
lesions of the temple region with spread of disease to the parotid gland or vice-versa is
documented. Most recent figures indicate that between 1998 and 2003, eighty-six
patients were treated with radiation therapy at the RBWH for this disease site (RBWH,
2005).
Of the eighty-six patients treated at the RBWH radiation oncology department between
1998 and 2003, seventy-one are still alive today. Thus an 83% survival rate exists.
This figure cannot be quoted as a five year survival rate because some patients
included in these figures were treated at the end of 2002.
2.3 Treatment Options and Survival
There are a number of treatment modalities available to patients with disease in the
parotid gland, skin temple region and the lower neck region. Common treatment
options include; surgery, chemotherapy, radiation therapy or a combination of
treatments.
Treatment of the parotid gland and skin temple region can involve surgery alone
(Figure 3).

20
Figure 3- Figure demonstrating surgical excision of disease in temple region and parotid region
(Plopper.C et al., 2004, p409).
A study conducted by Khurana et al, claims surgery alone achieved disease free
survival of 61% at five years (Khurana.V et al., 1995, p448). In contrast other
researchers suggest local recurrence occurs in 20-70% of patients treated with surgery
alone (Rowbottom.C et al., 2001, p163). Complications are associated with surgery
and include permanent facial palsy, Frey’s syndrome, and anesthesia in the
periauricular skin (Licitra.L et al., 2003, p222).
Chemotherapy in the treatment of parotid lesions is rarely used alone. Marandas et al
believe that chemotherapy alone has not been proved an effective treatment option
(Marandas.P et al., 1990). For the site of interest in this research project, there is
limited recent data available to determine survival rates for chemotherapy used alone.
Licitra et al suggest, “for both major and minor salivary gland tumours chemotherapy
is only suitable for individual clinical use” (Licitra.L, et al, 2003, p220). Thus
chemotherapy alone is not a common treatment option for parotid tumours or ones that
have spread to or from the temple skin region.
Radiation therapy alone is not a successful treatment option for skin lesions of the
temple region that have spread to the parotid gland. A literature review by Laramore et
al determined a 26% local control rate (Laramore.G, 1987, p1421). Side-effects
associated with radiation therapy may include; xerostomia, pain in jaw, hearing deficits,

21
bone necrosis and cataract formation (Nutting.C et al., 2001). The degree and severity
of side-effects depend on the dose prescribed and dose distribution.
The preferred treatment option for tumours in the skin region of the temple with
extension to the parotid gland or vice-versa, is a combination of surgery and post-
operative radiation therapy (O'Brien.C et al., 2002). A study by Delcharco et al
determined that disease control was 90% for surgery and postoperative radiotherapy
and 53% for surgery alone (Delcharco.J et al., 1998).
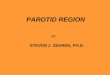
2.4 Anatomy of the Parotid Gland and Surrounding Structures
Anatomy of the parotid gland and surrounding structures challenge the delivery of
radiation therapy. The parotid gland and closely associated critical anatomy make it
difficult to deliver a radical tumour dose, without overdosing other important structures.
The anatomical information presented below will detail situation, function and
composition as related to this research topic.
The parotid glands are the largest of the salivary glands. They are situated on each side
of the face, below the left and right ear. The gland lies in the space between the ramus
of the mandible and the anterior border of the sternocleidomastoid muscle (Figure 4).

22
Figure 4- Figure demonstrating anatomical position of the parotid gland (Snell.R, 2004, p744).
The parotid glands are enclosed in a fascial capsule and function to produce serous
saliva, containing enzymes (Thibodeau.G and Patton.K, 2003). Structures within the
gland provide blood supply, venous and lymph drainage. Blood supply is from the
external carotid artery and its branches. Venous drainage is via the retromandibular
vein. Lymph drainage is into the parotid lymph nodes and the deep cervical lymph
nodes (Snell.R, 2004).
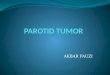
The facial nerve and its branches pass through the parotid gland. The facial nerve
controls muscles of facial expression. Thus facial paralysis is a complication of
surgical treatment options (Marieb.E, 1998) (Figure 5).

23
Figure 5- Figure demonstrating the facial nerve passing through the parotid gland (Snell.R, 2004,
p744).
Part of the parotid gland that lies superficial to the facial nerve is called the superficial
lobe. The portion of the gland that lies deep to the nerve is called the deep lobe. The
majority of parotid tumours originate in the superficial lobe. This may be a result of
the superficial lobe being larger, as there is no pathological difference between the two
lobes (DeVita.V et al., 1997).
The parotid glands function to produce saliva. “60-65% of total salivary volume is
produced in the parotid glands” (Cooper.J et al., 1995, p1153). Saliva plays a major
role in mastication, digestion, swallowing and speech. It provides lubrication for the
oral cavity, protects against bacterial infection and inhibits enamel decalcification
(Cooper.J et al., 1995).
2.4.1 Lymph Supply
Lymph node drainage may help predict metastatic spread of parotid cancers.
Lymphatics in and around the parotid consist of two groups; the periparotid and

24
intraparotid lymph nodes. The parotid gland will mainly drain to intra-parotid nodes.
These nodes will drain to the upper, middle and deep jugular lymph nodes (DeVita.V
et al., 1997)
The parotid gland will rarely drain to periparotid nodes which lie superficial to the
gland capsule and drain to the external auditory canal, the facial and auricular skin and
the temple scalp. These nodes are particularly important drainage sites for squamous
carcinomas and melanomas of adjacent skin (DeVita.V et al., 1997) (Figure 6). Barzili
et al support this by suggesting intra-protid and periparotid nodes can be at risk for
metastatic disease originating in skin cancer, particularly from the temple (Barzilai.G
et al., 2005).
Figure 6- Figure demonstrating lymphatics of the parotid gland and drainage towards the
auricular skin and temple scalp (Moore.K and Agur.A, 2002, p567).

25
2.5 Stabilisation
Patients treated for tumours of the temple skin region with spread to the parotid are
positioned in a stabilisation shell. A shell provides a reproducible position and
minimises head movement during treatment.
Different types of stabilisation devices can be used as controversy exists as to which is
the better device. Two popular stabilisation shells are thermoplastic or vacuum formed
shells. In 1995, a study by Welten et al, suggested that, “no substantial difference in
patient setup accuracy between both types of masks was detected” (Weltens.C et al.,
1995, p499). Many researchers suggest thermoplastic shells are a better alternative in
terms of accuracy (Lord.L et al., 2003) although others state, “there is no level 1
evidence that thermoplastic materials are more accurate” (Roques.T et al., 2005, p942).
Different forms of stabilisation devices are used but all provide similar and accurate
head stabilisation.
2.6 Prescription Terminology
The radiation oncologist marks target regions onto the CT data sets. Specific target
regions have defined prescription terminology that is referred to throughout this project.
Terminology such as; gross target volume (GTV), clinical target volume (CTV) and
planning target volume (PTV) are universally accepted concepts of radiation therapy.
The international commission on radiation units and measurements (ICRU) established
guidelines and recommendations with a publication in 1993 and a supplementary
publication in 1999. The publication is referred to as, “Report 50,” and the
supplementary publication is “Report 62.” Both reports define important areas of
volume.
Report 50 defined GTV as the innermost volume and is the gross palpable, visible or
demonstrated extent and location of malignant growth. CTV was defined as a region
containing the GTV with the addition of a volume to account for uncertainties in

26
microscopic spread. The PTV, has a margin added to the CTV to account for
geometric uncertainties (ICRU, 1993).
Report 62 redefined the PTV by introducing the internal margin (IM) and setup
margin (SM). IM accounts for variation in size, shape and position of the CTV. SM
accounts for uncertainties in patient-beam positioning (ICRU, 1999). ICRU defines
the volume formed by the CTV and the IM as the internal target volume (ITV) (Purdy.J,
2004). This is illustrated in Figure 7
Figure 7- Illustration detailing different volumes defined by ICRU (Purdy.J, 2004, p28).
ICRU recommended the use of these defined volumes as standard terminology when
prescribing and recording radiation therapy treatment.
This research project recognises and refers to prescription terminology defined by
ICRU.
2.7 Surrounding Anatomical Critical Structures
Surrounding anatomical critical structures to the PTV are outlined on the CT data sets
and are detailed below.

27
The parotid gland lies within close proximity to radiation sensitive critical structures.
These include; the contralateral external auditory meatus (eam), spinal cord, ipsilateral
lens and retina/optic nerve, contralateral lens and retina/optic nerve, brain, brain stem,
optic chiasm, oral cavity, mandible and contralalateral parotid gland.
The spinal cord (Figure 8) can be easily visualised on CT data sets. The spinal cord is
a round cylindrical structure situated between the spinus process and vertebral discs of
the spine. The spine extends from the upper border of the atlas to the junction between
the first and second lumbar vertebrae (Standring.S et al., 2005).
Figure 8- CT axial slice demonstrating position of the spinal cord and the mandible. (CT data
courtesy of RBWH)
The brainstem (Figure 9) is structurally and functionally a compact region that contains
vital cardiac and respiratory centres. It is situated at the posterior cranial fossa
(Standring.S et al., 2005). The brain is visualised as grey matter and is enclosed by
bony skull (Figure 10).

28
Figure 9- CT axial slice demonstrating position of the brainstem, parotids and oral cavity. (CT
data courtesy of RBWH)
The lenses, retina/optic nerves and brain (Figure 10) can be seen clearly on CT scans.
The lens is a transparent, encapsulated body that is visualised towards the anterior of
the eyeball (Standring.S et al., 2005). The retina is the inner most coat of the eyeball
that extends to the optic nerve which arises from the eyeball (Thibodeau.G and
Patton.K, 2003). The brain is visualised as grey matter contained within the skull.

29
Figure 10- CT axial slice demonstrating position of the lenses, retina/optic nerves and brain. (CT
data courtesy of RBWH)
The optic chiasm (Figure 11) is a small anatomical structure that is more difficult to
see on CT scans. It is the cross over point of the optic nerves (Tortora.G and
Reynolds-Grabowski.S, 2000)

30
Figure 11- CT axial slice demonstrating position of the optic chiasm. (CT data courtesy of RBWH)
The oral cavity (Figure 9) and mandible (Figure 8) are easily visualised on a CT scan.
The oral cavity is the space between the roof and the floor of the mouth and is
surrounded by the mandible. The mandible is a bony structure that can be easily seen.
It is the lower jaw and is the largest and strongest bone of the face (Thibodeau.G and
Patton.K, 2003).
Parotid gland anatomy has been described previously. On a CT scan (Figure 9) it can
be visualised laterally on a number of CT slices as an encapsulated grey structure.
The eam (Figure 12) can also be seen on a number of axial slices. It is a canal shaped
structure visualised laterally near the temporal bone and the ear drum (Tortora.G and
Reynolds-Grabowski.S, 2000).

31
Figure 12- CT axial slice demonstrating position of the EAM. (CT data courtesy of RBWH)
2.8 Radiation Tolerances of Critical Structures
In order to deliver radiation therapy to the PTV, normal tissue and critical structures
surrounding the PTV are irradiated. Radiation therapy treatment planning is made
difficult by internal inhomogeneity of the head and proximity of the parotid glands to a
number of critical structures (Bragg.C et al., 2002). Critical anatomical structures have
specific radiation tolerances and are outlined on CT data sets in this research project.
Literature documents radiation tolerances for a number of critical structures (Table 3).
If radiation tolerances to the volume of the critical structure are exceeded, detrimental
complications result.

32
Table 3-Reported literature detailing radiation tolerances of head and neck critical structures
(Emami.B et al., 1991, p111).
(Td 5/5=Probability of 5% complication within 5 years from treatment)
(Td50/5=Probability of 50% complication within 5 years from treatment)
The most common side-effect of radiation treatment to all head and neck tumours is
xerostomia, dental caries and loss of taste. Xerostomia or dry mouth syndrome is a
primary symptom because “saliva becomes scant, sticky and viscous as a result of
changes in its composition during a course of radiotherapy” (Stone.H et al., 2003,
p533). There is an overall decrease in salivary gland output that can last a number of
years and cause; oral discomfort, difficulty chewing and swallowing, increased
incidence of dental caries and impaired taste (Henson.B et al., 1998). Xerostomia
symptoms are usually permanent and cause a significant impact on quality of life
(Chao.K et al., 2001).
Morbidity associated with irradiation of the salivary glands has a positive correlation
with radiation dose. Traditional research defines dose limits. The radiation tolerance
of the parotid gland is 46 Gy for a 50% chance of developing xerostomia (Emami.B et
al., 1991). More recent research suggests an exponential relationship between saliva
flow reduction and mean parotid dose, “stimulated saliva flow at 6 months after
treatment is reduced exponentially, for each gland independently, at a rate of

33
approximately 4% per Gy of mean parotid dose” (Chao.K et al., 2001, p907). Thus an
optimal radiation dosimetry plan for a patient with skin lesions of the temple region
that have spread to the parotid gland should involve minimal mean dose to the
contralateral parotid gland in order to avoid temporary morbidity of xerostomia.
A late side-effect of radiation may include hearing loss. The middle ear and external
auditory meatus are usually within the PTV. The Cochlea, semi-circular canals and the
vestibulo-cochlea nerve lie close to the PTV and often receive a high dose (Nutting.C
et al., 2001). High doses to these structures can have detrimental effects. Schot et al
suggests there is a greater then 30% incidence of hearing loss of at least 10 dB in
patients treated with doses ranging from 38 Gy in 15 fractions to 50 Gy in 25 fractions
(Schot.L et al., 1992). Nutting reports ipsilateral hearing loss in 54% of parotid cancer
patients with conventional radiation therapy techniques (Rowbottom.C et al., 2001).
Thus hearing loss is a complication of concern associated with radiation therapy to the
parotid gland.
Anatomical visual pathways are important critical structures. Radiation tolerances are
demonstrated in table 3 and are supported by other researchers. Cook, et al,
determined a radiation tolerance of the optic chiasm as, “TD 5/5 of 50 Gy or slightly
higher” (Cook.B et al., 2004, p409). Yi, et al, determined that, “radiation doses up to
60 Gy given in conventional fractionation appears to be well tolerated by the optic
nerve” (Yi.W et al., 2004, p408). Doses exceeding tolerance may result in radiation
induced optic injury, resulting in blindness as an endpoint complication (Emami.B et
al., 1991).
Exceeding radiation tolerance to lenses has a complication endpoint of cataract
formation (Table 3). Lenses are positioned superior to the parotid gland tumour target,
but still receive dose. The dose that occurs on lenses depends on a variety of factors
including; dose delivered, proximity to the PTV and the number of treatment fields
used. Cataract formation is an undesirable side-effect of radiation dose to lenses, but in
some cases may be an acceptable trade-off for potential tumour cure (Pawlicki.T et al.,

34
2004). Cataract formation can be reduced by surgery, thus the complication endpoint
is not as concerning as other critical structures.
The brain and brainstem have complication endpoints of infarction necrosis.
Infarction necrosis is a serious detrimental side-effect that can result in death (Debus.J
et al., 1997). Studies of radiation exposure to brain tissue reveal, “pallor of white
matter consistent with diffuse cerebral edema and demyelination” (Emami.B et al.,
1991, p110). Steen et al supports this research by determining “changes in white
matter, usually at doses greater than 50 Gy, which are consistent with radiation-
induced normal tissue damage” (Steen.R et al., 2001, p79). As a result Emami et al
suggests a brain tolerance dose of 4500 cGy and a brain stem dose of 5000 cGy
(Emami.B et al., 1991).
The spinal cord’s endpoint complication is myelitis necrosis (Table 3). Myelitis
necrosis is characterised by inflammation of the spinal cord with associated motor or
sensory function leading to death of the living tissue (Anderson.D et al., 2002). Spinal
cord damage is a grave complication of radiation therapy (Branislav.J et al., 2002).
Radiation myelopathy is another spinal cord complication. It is characterised by,
“progressive development of sensory, motor, or prioceptive deficits… that may lead to
spastic paralysis, loss of significant function, or even death” (Kuo.J et al., 2002, p138).
Radiation induced spinal cord injuries are avoided by applying dose constraints to this
critical structure. “To minimise the chance of spinal cord complication, treatment
regimes commonly limit the spinal cord dose to less than 20 Gy in 5 fractions, 30 Gy
in 10fractions, or 50 Gy in 25 fractions” (Kuo.J et al., 2002, p139).
Osteonecrosis is an end point complication from radiation exposure to the mandible.
Osteonecrosis can occur when a total dose exceeding 65 Gy is applied with standard
fractionation (Glanzmann.C and Gratz.K, 1995). In contrast, a study by Jereczek-fossa
et al, determined doses as high as 74.4 Gy in the mandible were associated with

35
osteonecrosis, although this research was conducted with a small sample group
(Jereczek-Fossa.B et al., 2003).
The endpoint complication of irradiating the oral cavity is oral mucosa reaction which
leads to; pain, degrees of dysphagia, hoarseness and in severe toxicity, difficulty with
breathing (Cooper.J et al., 1995). Literature indicates that doses of 20-30 Gy to the
oral cavity at 1.8-2 Gy per fraction results in mucosa linings becoming erythematous.
At this dose, 20-30% of taste cells in the oral cavity are destroyed. After a further 10-
20 Gy, mucositis results, leading to desquamation (Cooper.J et al., 1995).
2.9 Radiation Treatment Technique Transition
In recent years radiation therapy has seen transition in techniques, from two-
dimensional radiation therapy (2DRT) to three-dimensional conformal radiation
therapy (3DCRT) and finally to IMRT.
2DRT is a traditional treatment used in a large majority of centres. 2DRT treatment
uses rectangular beams and usually allows a 6 mm margin between the edge of the
PTV and the collimator to account for the beam penumbra (Rowbottom.C et al., 2001).
2DRT planning utilises a two-dimensional planning system that does not account for
scatter from adjacent planning slices.
3DCRT is replacing 2DRT in many centres including the RBWH. 3DCRT uses a
three-dimensional planning system. Radiation plans use geometrically shaped beams
of uniform intensity defined from the beam’s eye view by a conformal block
(Rowbottom.C et al., 2001). In recent times, the introduction of multileaf collimators
(MLC’s) has replaced conformal blocks. “The introduction of MLC’s to shape
radiation beam portals has made conformal therapy a standard delivery technique”
(Budgell.G, 2002, p241). 3DCRT is also able to calculate the contribution to dose
from scatter from other slices.

36
3DCRT has many advantages over conventional 2D radiation therapy. Advantages
include; a decrease in dose to normal tissue, a decrease in side-effects and the potential
for dose escalation. Many studies have shown that 3DCRT minimises dose to normal
tissue. According to Perez et al, conformal radiation therapy spares more normal tissue
than standard 2D radiation therapy (Perez.C et al., 2000).
A decrease in dose to surrounding tissue results in a decrease in side effects. This
enables the opportunity to explore dose escalation to the target volume while still
keeping surrounding tissues to acceptable tolerance levels. “3DCRT overcame several
of the shortcomings and limitations of conventional two-dimensional planning”
(Esiashvili.N et al., 2004, p47). Thus a transition of radiation techniques can be seen
from 2DRT to 3DCRT.
2.10 3DCRT Limitations
3DCRT has associated limitations especially when treating skin lesions of the temple
region that have spread to the parotid gland. Limitations are associated with proximity
of critical structures to the target volume and the junction regions that are required to
treat the spread of disease with 3DCRT. The junction regions required by 3DCRT will
be discussed in detail in section 2.10.4. IMRT may have the potential to overcome
limitations.
2.10.1 3DCRT and Critical Structure Limitations
Proximity of critical structures can make dosimetry difficult. If the target volume
extends or curves around critical structures it is difficult to achieve the required target
dose while still keeping critical structures under tolerance (Figure 13). The degree of
3D shaping available is limited regardless of the number of beams applied (Budgell.G,
2002). Often, compromises must be made between the target dose and tolerance doses
of critical structures. Thus 3DCRT does not always provide an optimal solution when
critical structures are in close proximity to the target volume.

37
Figure 13- A transverse outline of a parotid patient showing the PTV extending towards critical
structures. Figure adapted from ((Nutting.C et al., 2001, p164).
2.10.2 IMRT Overcoming Critical Structure Limitatio ns
3DCRT is not adequate, “especially for concave-shaped targets in close proximity to
sensitive normal structures” (Saw.C et al., 2002, p76). Figure 14 demonstrates
dosimetry of a 3DCRT plan versus an IMRT plan. It can be seen that the IMRT
delivers a higher and more conformal dose to the target volume, while 3DCRT is not
able to conform high dose to the concave shaped target volume that is in close
proximity to the critical structure of the spinal cord.

38
Figure 14- Picture demonstrating dosimetry of an IMRT plan versus a 3DCRT plan. The 90%
isodose line conforms to the PTV for IMRT dosimetry, but not for 3DCRT dosimetry. The isodose
line conforming to the PTV for 3DCRT dosimetry is the 62% isodose line (Cozzi.L et al., 2004,
p621).
IMRT is an advanced form of 3DCRT. The difference being that IMRT enables the
advantages of 3DCRT to be taken to a higher level while overcoming the limitations.
IMRT can provide a solution when “conventional 3DCRT as just defined, cannot
produce a satisfactory treatment plan because of limitations of the method along with
the geometry of the problem” (Verhey.L, 1999, p78).
IMRT is a relatively new technology that may have the potential to overcome
limitations associated with 3DCRT. In 2004, Garden et al stated, “the use of IMRT for
the treatment of head and neck cancers is less than a decade old” (Garden.A et al.,
2004, p103). In this short time IMRT has flooded literature with controversy regarding
clinical advantages.

39
Some researchers suggest that not enough randomised trials have been conducted to
provide supportive evidence of IMRT benefits. “Only a few meaningful retrospective
studies are available that show its potential and its possible drawbacks” (Gregoire.V
and Maingon.P, 2004, p110). Garden et al support limited evidence based studies,
“justification for the benefits of IMRT compared with standard approaches has been
primarily theoretical” (Garden.A et al., 2004, p103).
In contrast, other researchers suggest the benefits of IMRT can undoubtedly overcome
limitations presented by conventional radiation treatment techniques.
“IMRT has two advantages for the treatment of head and neck cancers (ie, an
improvement in tumour coverage and better avoidance of normal tissues
resulting in a reduction in toxicity)” (Garden.A et al., 2004, p103).
“IMRT was found to offer significant advantages over conventional and
conformal radiation therapy, giving improved PTV homogeneity and reduced
dose to critical structures” (Adams.E et al., 2001, p587).
The suggested benefits of IMRT can be applied to difficult dosimetry treatments such
as skin carcinomas of the temple region with extensions to the parotid gland.
A skin lesion of the temple region with extensions to the parotid gland is an attractive
site for IMRT. Critical structures and radiation sensitive organs are in close proximity
to the target volume. High dose gradients offer potential therapeutic gain and
potentially improved mortality rates. “Dose escalation to the parotid using IMRT
should improve the likelihood of uncomplicated tumour control” (Bragg.C et al., 2002,
p737).
There is potential for reduced morbidity through spared structures. “IMRT in treating
cancers of the parotid, allows considerable sparing of critical structures without any
reduction in the quality of the coverage of the target” (Bragg.C et al., 2002, p737).

40
IMRT can provide a solution where the target volume is in close proximity to critical
structures.
2.10.3 3DCRT and Monoisocentric Junctions
Traditionally all head and neck tumours that are treated with radiation therapy are
divided into two areas that are matched by one junction. The purpose of treating two
separate areas with one junction is to treat the primary tumour bed and draining
lymphatics while limiting the dose to normal structures (Fabrizio.P et al., 2000).
The two areas are the lower cervical field or supraclavicular field and the face fields or
upper neck fields. “In many instances, right and left lateral parallel opposed fields
matched to an anterior supraclavicular field are used to ensure coverage of the primary
and nodal sites” (Sohn.J et al., 1995, p809).
The technique used to match these fields with one junction, is called the
monoisocentric technique. Currently most centers use the monoisocentric technique
(Dabaja.B et al., 2005). This technique avoids the problem of beam divergence
because each beam is half-beam blocked to the central axis. At the junction there is a
non-divergent beam edge so that the match between the two fields is exact, with no
theoretical overlap (Dabaja.B et al., 2005). The half-beam block is created with
asymmetric jaws (Figure 15). The superior jaws will remain at zero or at the junction
while the inferior jaws treat the lower cervical fields. The inferior jaws will remain at
zero or at the junction region while the superior jaws treat the upper face fields. This
technique also reduces the possibility of geometric error when moving to a second
isocentre.

41
Figure 15- The top two figures demonstrate the superior jaws treating the upper face fields while
the inferior jaws remain at the junction. The bottom two figures demonstrate the inferior jaws
treating the lower cervical nodes while the superior jaws remain at the junction (Manske.M et al.,
2004, p87).
2.10.4 3DCRT and Junction Limitations
3DCRT has limitations when more than one junction is required. Many treatment sites
need more than one junction. For example the treatment of lesions of the skin temple
region that have spread to the parotid gland or vice-versa.
Historically, this disease site would be treated with an anterior lower cervical photon
field or an anterior and posterior lower cervical photon field. The upper face fields are
treated with anterior and posterior oblique parotid photon fields. Both oblique fields
traditionally utilise tissue compensators called wedges, to improve dose homogeneity.
As a result, treating the upper face parotid area with obliques is often called the
ipsilateral wedged pair technique (Yaparpalvi.R et al., 1998). The area of skin on the
temple field is treated with one electron field.

42
Traditionally the region requiring treatment is divided into three separate areas (Figure
16). The three areas are; 1= lower cervical field, 2= parotid photon field, 3= temple
field. Junction number one (Figure 16) is positioned between fields one and two.
Junction number two (Figure 16) is positioned between fields two and three.
Figure 16- Photo of thermoplastic shell showing three separate treatment areas. 1=lower cervical
field, 2=parotid photon field, 3=temple field (Photo courtesy of RBWH).
Junction 1 separates the lower cervical fields and the upper parotid photon fields to
ensure coverage of the primary disease and nodal sites. Junction 2 is situated between
an electron field and the parotid photon fields. The electron field is needed to treat the
temple region where the PTV is at a shallow depth. Electrons are able to deposit dose
at a more shallow depth then photons, while still maintaining full dose on skin surfaces
with the use of wax bolus.
Junction two, separating the parotid photon fields and the electron field introduces
problems. This junction is often located close to the lenses. The contralateral lens
often receives high dose from the diverging posterior oblique parotid photon field. The

43
ipsilateral lens often receives high dose from the temple electron field, depending on
the size and position of this field.
Homogenous dose at this photon-electron junction region is desirable but does not
occur. Inhomogenous dose between an abutting photon and electron field is a
characteristic when the two beam penumbras are added together, and is a major
limitation for treating this disease site with 3DCRT. Photon fields have a straight edge
penumbra while electron fields bow out in the penumbra region (Figure 17a&b).
“Because the electron and photon beams have different penumbras, matching of these
beams results in an inhomogeneous dose distribution in the junction region”
(Kemikler.G, 2006, p183).
Figure 17a- Photon isodose curve Figure 17b- Electron isodose curve
with straight edge penumbra bulging at penumbra.
(Washington.C and Leaver.D, 2004, p508). (Washington.C and Leaver.D, 2004, p532).
To treat this junction daily, on alternate days the electron field edge is matched to the
divergent edges of the oblique fields on skin (Figure 18a&b). Although electron and

44
photon fields are matched on skin, they overlap at depths and spread out laterally with
increasing depth (Sun.C et al., 1998). Thus an area of underdosage and overdosage is
unavoidable because of beam divergence (Kemikler.G, 2006).
Figure 18a-Matching anterior oblique photon field to the electron field on skin (photo courtesy of
RBWH).
Figure 18b-Matching posterior oblique photon field to the electron field on skin (photo courtesy of
RBWH)

45
The region of high dose will occur on the photon side of the junction because electrons
will bulge out into this region. Low dose will occur on the electron side of the junction
because photons do not bulge out into the electron field and only electron penumbra
dose will occur on this side of the junction. “A hot spot on the photon side and a cold
spot on the electron side were observed in film measurements” (Kemikler.G, 2006,
p186).
Inhomogeneity at the photon-electron junction (junction 2, Figure 16) is further
impacted by patient set-up errors and congruity of the light and radiation field. “A few
mm of mismatch could seriously cause over and under-dose at the junction region”
(Kemikler.G, 2006, p187). Thus set-up errors further enhance inhomogeneity at the
junction region.
There are two types of set-up errors, random and systematic. A systematic error is
where the same error occurs systematically, causing the junction to be misplaced each
fraction. A random error occurs randomly and may cause a blurring of the dose
distribution and could actually reduce the effect of the inhomogeneity in the junction
region. This research project did not attempt to assess treatment set-up errors. All
dosimetry was performed by the author thus any dosimetric systematic errors were
performed across the sample group. As a result, comparisons between the sample
plans account for any errors occurring. Random dosimetric errors could not be
accounted for in this research project
Inhomogeneity at the photon and electron junction region results in areas of high and
low dose coverage of the PTV. A low dose to the PTV is undesirable because it
increases the risk of tumour recurrence and a high dose increases the risk of normal
tissue morbidity (Zhu.L et al., 1998).
Carcinoma of the skin temple region that has spread to parotid gland or vice-versa is a
difficult area to treat with two separate junction regions using 3DCRT. Matching one
junction region can be achieved with monoisocentric jaws, but the second junction

46
between the photon and electron field results in dose inhomogeneities across this
region that are further enhanced with set-up positional errors . 3DCRT has associated
limitations when treating this disease site.
2.10.5 IMRT Overcoming Junction Limitations
IMRT overcomes limitations of 3DCRT when considering two separate junction
regions. IMRT eliminates the need for a second junction between the parotid photon
field and the temple electron field. The temple electron and photon face fields are
treated as one IMRT photon field. Thus dose inhomogeneity across the photon-
electron junction, produced with 3DCRT is removed. As a result set-up uncertainties
will not enhance inhomogeneities in this region.
“One of the ways for overcoming this problem is to use the modulated beams, which
can yield improved dose homogeneity and are less sensitive to set-up errors”
(Kemikler.G, 2006, p187).
Only the temple and upper face regions can be treated with IMRT because IMRT is
only advantageous when the PTV is in close proximity to critical structures. The major
critical structure in the lower cervical photon field is the spinal cord, which is not in
close proximity to the PTV (Figure 19).
Figure 19- CT axial slice demonstrating the spinal cord as the only critical structure in the lower
cervical photon field. (CT axial slice courtesy of RBWH).

47
Thus IMRT is does not offer advantages in the lower cervical fields. Li et al suggest
treating the whole field with IMRT “usually renders treatment plans suboptimal” (Li.J
et al., 2005, p135). An alternative solution is treating the parotid and temple regions
with IMRT and treating the lower cervical region with 3DCRT.
If only one junction exists between the parotid face field and the adjoining lower
cervical photon field, it can be easily treated using monoisocentric jaws, as discussed
in section 2.10.3 (Figure 15). This is still possible when each area is treated with a
different type of radiation therapy.
“IMRT head and neck patients can be effectively treated with the field-
matching technique where superior aspect of the target volume is treated with
IMRT, and the inferior portion of the target volume is treated with a static
anterior-posterior lower anterior neck field, with a common isocenter” (Li.J et
al., 2005, p138).
IMRT treatment can easily junction a cervical field if required. Thus IMRT is capable
of treating a region involving two separate junctions.
This research project is concerned with finding a class solution for skin lesions of the
temple region with spread to the parotid gland. It is acknowledged that treating the
lower cervical photon field is necessary, although no advantage is gained by treating
this region with IMRT, instead a standard 3DCRT field is used. Thus this project will
concentrate on determining a class solution for the parotid photon region and the
temple region.
2.11 Radiation Doses
3DCRT dose prescription for parotid gland tumours and skin lesions of the temple
region that have spread to the parotid gland, is typically a reference dose (RD) of 60
Gy in 30 fractions over 6 weeks (Nutting.C et al., 2001). The aim of treatment is to
treat the PTV to between 95% and 107% of the RD, as recommended in the

48
International Commission on Radiation Units and Measurements Report (Bragg.C et
al., 2002).
An IMRT dose prescription of 60 Gy in 30 fractions over 6 weeks still applies for the
same disease site although aims of treatment differ from 3DCRT. “IMRT dose
distributions are often more heterogeneous within the target” (Galvin.J et al., 2004,
p1617). As a result IMRT research has used guidelines in Radiation therapy Oncology
Group (RTOG) protocol RTOG H-0022, to evaluate dose prescriptions and plans.
“The prescribed dose must cover 95% of the volume of the PTV of the gross
tumour. Not more than 1% of the PTV of the gross tumour can receive a dose
that is less than 93% of the prescribed dose, and not more than 20% of this PTV
can receive a dose that is greater than 110% of the prescribed dose”(Galvin.J et
al., 2004, p1627).
Historically, the radiation energy used to treat head and neck tumours for 3DCRT and
IMRT is 6 Mv photons. Traditional teaching in radiation therapy is, “the deeper the
target, the higher the energy that should be used” (Pirzkall.A et al., 2002, p434).
Pirzkall et al continue to suggest that, “the basic teaching regarding energy holds true
even for IMRT” (Pirzkall.A et al., 2002, p438). Head and neck tumours such as skin
lesions of the temple with extension to the parotid gland, are not deep seated targets, as
a result 6 Mv photon energy is sufficient.
2.12 Beam Arrangements
Beam arrangements for 3DCRT are different to beam arrangements used in IMRT.
2.12.1 Beam Arrangements Using 3DCRT
The optimal unilateral treatment technique for parotid tumours alone using 3DCRT are
the ipsilateral wedged-pair technique and the 3-field and the mixed electron-photon
beam technique (Yaparpalvi.R et al., 1998). As discussed in section 2.10.4, disease in
the skin temple region that has spread to the parotid gland is historically treated with an

49
anterior or anterior and posterior lower cervical photon fields junctioned to ipsilateral
wedged pair parotid photon fields that are junctioned with an electron temple field.
2.12.2 Beam Arrangements Using IMRT
IMRT is still in its infancy (Gregoire.V and Maingon.P, 2004), as a result there is
limited literature on beam arrangements for specific disease sites. “There has been
little investigation into the optimisation of beam–orientations for IMRT compared with
unmodulated beams” (Pugachev.A et al., 2000, p169).
A fundamental step for arranging beams in IMRT is determining the beam number and
angle. “Angle selection is usually based on the experience of the treatment planners or
their intuition or by a trial-and-error approach” (Wang.X et al., 2004, p1326). The
ultimate goal in radiotherapy is to choose the optimal plan that is provided by the
minimum number of beams (Pugachev.A et al., 2000). This enables quality treatment
to be delivered quickly and efficiently.
A small number of researchers have determined IMRT field arrangements for specific
head and neck tumours, although no IMRT literature is specific to the disease site
studied in this research. Researchers such as Bragg and Nutting et al are referenced
throughout this research project, although their work discusses disease of the parotid
alone, without temple involvement.
Three IMRT fields are the minimum justifiable beam number for an IMRT plan.
Bragg et al determined that three beams had the ability to deliver the required dose to
the target, but that it was considerably better in some patients than in others (Bragg.C
et al., 2002).
Researchers also suggest that the target homogeneity may be improved by directing
beams from the same side as the tumour. “Directing a higher proportion of the beams
used from the side ipsilateral to the tumour can reduce the target underdosing and
overdosing” (Bragg.C et al., 2002, p735).

50
A study by Nutting et al determined four field ipsilateral IMRT beam angles,
positioned at 15°, 40°, 140° and 170° from vertical were the optimal IMRT beam
arrangement for parotid cancer patients (Nutting.C et al., 2001) (Figure 20). For the
same tumour type, Bragg et al determined four beams positioned on the ipsilateral
tumour side at 15°, 55°, 125°, 165° from vertical and a direct lateral from the opposing
side produced the optimal IMRT beam arrangement (Bragg.C et al., 2002).
Figure 20- optimal IMRT class solution for parotid carcinoma (Nutting.C et al., 2001, p170).
Researchers suggests that, “nine, equispaced IMRT fields are sufficient to produce an
‘optimal’ treatment plan” (Rowbottom.C et al., 2001, p169). Bragg et al also
suggested that a nine field IMRT plan showed the, “largest improvement over the
3DCRT plan in terms of target dose homogeneity, target underdosing and dose
conformity” (Bragg.C et al., 2002, p734).
A beam arrangement that promotes PTV homogeneity and dose improvements is based
on a nine field equispaced beam arrangement with the removal of beams at 80° and
280° that enter and exit the parotid. This field arrangement was suggested by literature
researchers who determined that it maintained improvements seen in the nine field plan,

51
namely the improved PTV homogeneity and reduced cochlea and parotid gland dose
(Rowbottom.C et al., 2001).
2.13 Class Solutions and Benefits
Much research has been conducted into the optimal IMRT treatment for specific head
and neck carcinomas. They are identified as class solutions and are specific to
individual departments. Some centers have followed class solution protocols for a
number of years and show promising results. For example The Ghent University
Hospital has developed a class solution for ethmoid sinus cancer. The class solution
utilises a high tumour dose that may increase survival rates (Claus.F et al., 2001).
Class solutions for individual tumour sites are developed to produce the optimal
treatment plan with ease.
“A class solution can be defined as the historical experience in designing RT
plans for a particular site …An IMRT class solution for a given treatment site
and stage of disease consists of the criteria for optimisation and the
specification of the beam techniques used, typically including beam direction
and number. Once developed, a class solution may be applied repeatedly to
generate IMRT plans for patients with the same stage of disease at the same site
and for other clinical considerations” (Intensity Modulated Radiation Therapy
Collaborative Working, 2001, p913).
Skin lesions of the temple region with extensions to the parotid gland, is a site that may
benefit from IMRT treatment. To date, no class solution exists for this disease site.
This research project aims to develop the optimal class solution specifically relating to
beam number and angles for this disease.
2.14 Summary
3DCRT is a treatment option for skin lesions of the temple region with spread to the
parotid gland. This treatment has associated limitations that may be overcome with

52
new treatment technologies. IMRT is a relatively new treatment technique that may
overcome limitations introduced with current treatment techniques.
This research proposal is an original and innovative study that will endeavour to
determine the optimal IMRT class solution for patients with skin lesions of the temple
region with spread to the parotid gland. It will be determined if the IMRT class
solution avoids problems of the junction region and lowers dose to critical structures.
Traditional 3DCRT will be assessed and compared to the IMRT class solution to
determine the superior treatment option for patients presenting with this disease site.

53
CHAPTER 3
METHOD AND MATERIALS
3.1 Sample Group
In this retrospective research study, nine patient computerised tomography (CT) data
sets were used. The pre-requisite for inclusion of a CT data set was based on three
areas requiring treatment with three dimensional conformal radiation therapy (3DCRT),
resulting in two junction regions (Figure 16). The three areas requiring treatment are
the:
1. Lower cervical photon fields
2. Parotid photon fields
3. Electron field to the temple region
The junction regions can be easily visualised between fields one and two and between
fields two and three, as detailed in Figure 16.
The CT data sets that fulfilled pre-requisites were randomly chosen from the CT data
base at the Royal Brisbane and Women’s Hospital (RBWH). Six of the CT data sets
had left sided lesions and three CT data sets had right sided lesions. Not all of the CT
data sets had the same primary disease but all had the three areas requiring treatment.
Details of primary lesions are shown in Table 4.

54
Table 4- Table illustrating disease primary and classification of patient data used in this project.
(Information courtesy of RBWH)
Patient Number
Disease Primary
TNM Classification
1
SCC parotid gland
T1N1M0
2 SCC temple region
T3N1M0
3 SCC temple region
T2N1M0
4 SCC temple region
T2N1M1
5
SCC temple region
T1N1M0
6 BCC temple region
T1N0M0
7 SCC temple region
T3N0M0
8 SCC temple region
T1N0M0
9 SCC temple region
T3N0M0
All Case studies in this research project, followed protocol of RBWH. All patients
presenting at the RBWH with skin lesions of the temple region with spread to the
parotid gland, are discussed amongst radiation oncologists. Doctors converse to
determine the optimal treatment regime for each individual patient. All patients
studied in this sample group underwent surgery combined with post-operative radiation
therapy.
3.2 Personnel
The author performed all dosimetric planning for this project. Radiation oncologists,
Dr Lyndall Kelly and Dr Liz Kenny from the RBWH were consulted in their areas of
clinical expertise.
Areas of clinical expertise for the Radiation Oncologists related to;

55
• Determining the superior dosimetric plan
• Determining the dose prescription used in this research project
• Determining critical structures and the required tolerances of structures
• Listing of critical structures in order of importance
3.3 Equipment
Shell stabilisation devices were used to position the patient. The patients used in this
study were stabilised with either a vacuum formed four point shell (Figure 21) or a
thermoplastic four point shell (Figure 22a, 22b). The fact that different stabilisation
devices were used is acknowledged, although has minimal effect on achieving aims of
the study or the final outcome.
Figure 21- vacuum seal four point shell (photo courtesy of RBWH)
Figure 22a-lateral view of thermoplastic Figure 22b- Anterior view of thermoplastic Shell (photo courtesy of RBWH) shell (photo courtesy of RBWH)

56
All patients were CT scanned on a “Siemens Somatom Sensation IV Scanner” (Figure
23). This is a four slice spiral CT scanner with a seventy centimetre aperture (Siemens,
2002).
Figure 23- Siemens Somatom Sensation IV Scanner (Photo courtesy of RBWH)
The “General Electric Medical Systems Advantage Sim 4.1” (Adv Sim) was used to
define the planning target volume (PTV) on each data set. Adv Sim is a computer
system that allows visualisation of CT axial slices and enables volumes or structures to
be drawn onto them.
“Nucletron PLATO Radiation Therapy Planning Software RTS V2.3.1” (PLATO) was
used to perform all three dimensional conformal dosimetric planning. PLATO is a
radiation therapy computer planning system.
Intensity Modulated Radiation Therapy (IMRT) computer planning software was
required for this research project. Nucletron Pty Limited agreed to supply software
free of charge for a period of 90 days (Appendix A). “Nucletron PLATO Lightning
Inverse Treatment Planning V” (ITP) was the software provided and used to perform
all IMRT plans.

57
The “Digital Imaging Communication in Medicine” (DICOM 3) was used to transport
anatomical images between different computer workstations.
All equipment used in this study was provided courtesy of the RBWH.
3.4 Data Collection Procedure
All patients in this research study presented for radiation therapy after undergoing
surgery. A time-period between surgery and radiation treatment exists and is
determined by the radiation oncologist. Data collection procedure followed the
standard RBWH protocol which involves a number of steps including;
• Patient positioning
• CT scanning
• Planning target volume (PTV) acquisition
• Dose prescribing
• Plan dosimetry
3.4.1 Patient Positioning
For radiation therapy, patients were positioned supine, and straight and level. They
were immobilised and stabilised with a shell discussed in section 3.3. The radiation
oncologist determined junction 1 (Figure 16) between the lower cervical photon
region and the upper parotid face region. This line was marked onto the shell with
wire.
3.4.2 Computerised Tomography (CT) Scanning Procedure
Patients were CT scanned in their shell using a Siemens Somatom Sensation IV
scanner.
Standard CT protocol scan parameters were used, which are 120 kV and 350 mAs.
mAs varies for each patient according to size of the area scanned. A CT data set is
reconstructed at 3 mm increments with a slice width of 3 mm. The data set is then
exported via DICOM 3 to Adv Sim.

58
3.4.3 Planning Target Volume (PTV) Acquisition
The PTV is drawn onto axial slices by the radiation oncologist. The CT data set
complete with PTVs, is exported via DICOM 3 to PLATO computer planning software.
3.4.4 Dose Prescribing
A radiation oncologist* determined a dose prescription of 63 Gy reference dose (RD)
in 30 fractions over 6 weeks, using 6 Megavoltage (Mv) photons and 60 Gy at 100% in
30 fractions for the electron temple region. The depth of 100% was specified by the
electron energy chosen by the radiation oncologist for each CT data set. Figure 24
demonstrates a standard dose prescription used in this study.
Figure 24- Figure demonstrating standard dose prescription used at the RBWH- image courtesy of
RBWH.

59
3.5 Plan Dosimetry
For all 3DCRT plans, ICRU Report 50 guidelines were followed to determine an
optimal distribution. 95% of the reference dose was delivered to the PTV while aiming
to keep maximum doses within 107% (ICRU, 1993). Thus 60 Gy was to cover the
PTV without doses exceeding 67.4 Gy.
For all IMRT plans, the Radiation Therapy Oncology Group (RTOG) protocol RTOG
H-0022 was used, to evaluate dose prescriptions and plans. RTOG requirements are;
1) The prescribed dose must cover 95% of the volume of the PTV
2) Not more than 1% of the PTV of the gross tumour can receive a dose that is
less than 93% of the prescribed dose
3) Not more than 20% of this PTV can receive a dose that is greater than 110% of
the prescribed dose (Galvin.J et al., 2004)
The only deviation made from RTOG requirements, was that 95% of the prescribed
dose was to cover 95% of the volume of the PTV. Thus, in every plan, 60 Gy was to
cover 95% of the PTV volume. It was difficult to achieve all three objectives with
each beam arrangement. In order to achieve 1), a compromise was often made
between RTOG requirements: 2) and 3).
In this study, the prescribed dose for 3DCRT and IMRT were the same. Dosimetry
objectives varied slightly for IMRT plans but this does not affect comparisons between
the two techniques.
Nine dosimetric plans were produced on each CT data set, resulting in a total of eighty-
one isodosed distributions. The time taken to perform one IMRT plan varied between
twenty minutes to two hours depending on the geometry of the PTV and associated
structures. The time taken to perform one 3DCRT plan was approximately thirty
minutes.

60
Superior and inferior field lengths of the oblique parotid photon fields for 3DCRT
planning were determined by the radiation oncologist. The anterior and posterior field
sizes of the oblique fields were 0.7 cm outside the PTV. Manipulation of beam angles,
weightings, wedges, multileaf collimators were performed to achieve an optimal
3DCRT plan. Planning experience aided manipulation choices and thus optimisation.
Field sizes for IMRT plans were determined by the computer planning system.
Manipulation of weightings, maximum and minimum doses for the PTV and body
were done to achieve the optimal IMRT plan for each beam arrangement. A trial and
error approach was the strategy used to optimise the IMRT plans.
3.6 Critical Structures
A radiation oncologist* determined critical structures or organs at risk (OAR),
tolerance doses and order of structure importance (Table 5). These were directly used
in the IMRT planning process.
Table 5: Critical structures, tolerance and order of importance as determined by radiation
oncologist.
ORGANS AT RISK MAXIMUM
TOLERANCE (Gy) ORDER OF IMPORTANCE Brain 53 3 Brainstem 45 1 Contra lateral parotid gland 10 7 External auditory meatis (eam) 55 6 contralateral lens 8 9 ipsilateral lens 8 9 contralateral optic nerve/retina 45 4 ipsilateral optic nerve/retina 45 4 Mandible 50 10 Optic chiasm 50 5 Oral cavity 20 8 Spinal cord 45 2
3.6.1 Outlining Critical Structures
Patient anatomy within CT data sets, were outlined using the contouring component of
the PLATO 3DCRT computer planning system. Outlining was performed by the same

61
person for 3DCRT and IMRT to eliminate inter-observer variability. All critical
structures detailed in table 5 were outlined. Anatomical visualisation of critical
structures on CT scans, are detailed in section 2.7.2.
For 3DCRT plans, patient’s bodies were outlined without the inclusion of bolus. To
obtain coverage of the PTV by 95% of the reference dose, different thickness bolus
was required on the skin surface for the parotid photon fields and the temple electron
field. Limitations of the PLATO planning system required different thicknesses of
bolus to be added in PLATO 3D Planning.
For IMRT plans, a constant thickness of bolus was required over the parotid fields to
cover the PTV by 95% of the reference dose. As a result bolus was added at the
outlining stage and not in PLATO planning.
To accommodate different bolus requirements for 3DCRT and IMRT plans, CT data
sets of each patient were outlined twice. To ensure critical structures were not outlined
differently for each set, statistical analysis was performed on structure volumes. Visual
analysis was also undertaken to ensure the correct spatial position.
3.7 Beam Arrangements
Beam arrangements were different for 3DCRT and IMRT. 3DCRT beam
arrangements were consistently similar for all CT data sets.
3.7.1 3DCRT Beam Arrangements
One 3DCRT plan was produced for each CT data set. The lower cervical region was
treated with an anterior or an anterior and posterior photon field. The parotid face
region was treated with the wedged pair technique. Lateral electron fields were added
to the temple region, where the PTV is shallow and close to the skin surface.
For the wedged pair technique, beam angles were dependent on PTV position and the
relation of critical structures. Wedges were used to provide a more homogenous

62
distribution; on the anterior oblique field-wedge was thick to post, on the posterior
field-wedge was thick to anterior (Figure 25).
Figure 25- Figure showing wedge direction of the anterior and posterior oblique fields. (Nutting.C
et al., 2001, p164).
As indicated in section 2.10.4, when treating this disease with 3DCRT, the temple
electron field is matched on the skin to the divergent edges of the anterior oblique and
posterior oblique photon fields on alternate days. At the RBWH, 3DCRT dosimetry is
performed by matching the temple electron field on skin at the point where the
divergent edges of the anterior and posterior oblique photon fields cross one another
(Figure 26). This technique does not replicate how this disease site is treated.

63
Figure 26- Figure demonstrating the temple electron field matching on skin at the point where the
divergent edges of the oblique photon fields cross one another (photo courtesy of the RBWH).
3DCRT dosimetry is performed this way for two reasons. Firstly, it reduces the chance
of error when matching the divergent edge of the photon fields to the electron field in
the 3DCRT computer plan. A small misalignment error may result in an overestimate
of under and overdosage. “A few mm of mismatch could seriously cause over and
under dose to the junction region” (Kemikler.G, 2006, p187). The second reason is for
improved time efficiency in completing the 3DCRT plan.
The divergence of the anterior and posterior oblique photon fields is considered to be
minimal. As a result there is potentially no clinical difference in using this method
versus exactly replicating the matching technique used during treatment. For this
research study, 3DCRT planning was performed following RBWH clinical dosimetry
technique after clinical testing.

64
In order to test dosimetry of the two matching techniques, a 3DCRT plan was
performed using each technique. The minimum, maximum and mean dose to the PTV,
and the dose covering 95% of the PTV in each plan was obtained from DVH output
data. Doses were compared to determine if differences in doses were clinically
significant.
3.7.2 IMRT Beam Arrangements
IMRT beam arrangements varied, and were determined from literature research
detailed in section 2.12.2. In this research project, three IMRT plans used ipsilateral
beams, directed from the same side as the tumour.
Two of the five field beam arrangements were not all directed from the ipsilateral side
of the tumour. One had four beams positioned on the ipsilateral tumour side at 15°,
55°, 125°, 165° and a direct lateral from the opposing side (Figure 27). This beam
arrangement was chosen because Bragg et al determined it to be the IMRT class
solution that produces the optimal beam arrangement for parotid tumours (Bragg.C et
al., 2002).
The other five field beam arrangement uses 2 contralateral beams and 3 ipsilateral
beams (Figure 27). This beam arrangement was used to determine whether there is any
advantage of a five field beam arrangement not being equally spaced.
One seven field and nine field equispaced beam arrangement was chosen based on
research by Rowbottom et al (section 2.12.2). A seven field equispaced beam
arrangement was chosen to see if the advantages of a nine field equispaced beam
arrangement could be maintained with seven fields.
On each patient data set, eight IMRT plans were performed (Table 6) (Figure 27).
IMRT plans for each beam arrangement were considered to be optimised when RTOG
guidelines were adhered to as close as possible.

65
Table 6: Beam arrangement used on each CT data set
BEAM ARRANGEMENT BEAM ANGLE(°)-RT SIDED LESION
BEAM ANGLE(°)-LT SIDED LESION
9 beam equispaced 40,80,120,160,200,240,280,320,360 40,80,120,160,200,240,280,320,360 7 beam equispaced 51,102,153,204,255,300,0 51,102,153,204,255,300,0 7 beam 40,120,160,200,240,300,0 40,120,160,200,240,300,0 5 beam ipsilateral 330,300,240,210,270 30,60,90,120,150 5 beam (3ipsilateral+2 beams) 315,270,225,135,45 45,90,135,320,220 5 beam (4equispaced +1 beam) 345,305,90,235,195 15,55,125,165,270 4 beam ipsilateral 345,320,220,190 15,40,140,170 3 beam ipsilateral 315,270,225 45,90,135 3DCRT plan As required As required
Figure 27-Diagrammatic representation of IMRT beam angles for left sided lesion (not drawn to scale):
ant rt lt post
3.8 Dose Volume Histograms
Cumulative dose volume histograms (DVH) of 100 000 points were used to determine
end points and display a summary output of final plans (Figure 28). DVH analysis was
used in statistical analysis.
9 beam equispaced
7 beam equispaced
7 beam 5 beam (3ipsilateral+2)
4 beam ipsilateral 3 beam ipsilateral 5 beam ipsilateral 5 beam (4equispaced+1)

66
Figure 28-Figure displaying a 3DCRT dose volume histogram and summary output
3.9 Ethics Approval-RBWH/QUT
Ethics approval was sought from the RBWH and Health Service Districts- Human
Resource Ethics Committee, to perform dose distribution investigations on RBWH CT
data sets. The protocol followed to seek ethics approval was subsequently granted by
Professor W Egerton (Appendix B). Following ethics approval from the RBWH, the
Human Ethics Research Committee of the Queensland University of Technology
(QUT) stated that ethical issues were uncompromised, as a result this research project
did not require formal ethics approval from this institution (Appendix C).

67
3.10 Analysis of Results
3.10.1 Bland and Altman
A Bland and Altman plot was performed on all structure volumes. A Bland and
Altman test determined any significant difference between outlining CT data sets twice
for each patient in order to account for bolus. The bias or mean difference was
established and graphed. Limits of agreement (LOA) are equivalent to ± two standard
deviations about the mean. LOA were calculated for each volume and visualised on a
Bland and Altman plot.
3.10.2 DVH Range Analysis on PTV
Analysis was performed on the DVH range for the PTV. Research by Nutting et al in
2001, defined the;
• Minimum PTV= dose received by ≥99% of the PTV
• Maximum PTV= dose received by ≤1% of the PTV
(Nutting.C et al., 2001).
This research project defines the range as the minimum PTV subtracted from the
maximum PTV. The range indicates how well the dosimetric plan fulfilled the PTV
dose prescription within RTOG and ICRU guidelines. The smaller this range, the
better the plan was at covering the PTV and the better the plan was at avoiding
underdosing and overdosing of the PTV.
Repeated measures analysis of variance (ANOVA) was performed on the mean range
of data for all IMRT plans, to determine if significance existed between at least two of
the means when p<0.05.
3.10.3 Mean doses
Mean maximum doses to critical structures and mean dose to the parotid gland were
calculated from summary outputs of all dosimetric plans.

68
3.10.4 Conformity Index (CI)
Conformity index analysis was performed on all plans to determine how tightly the
95% isodose line conformed to the PTV. The CI was calculated using the equation:
CI=VPTV95% × VPTV95%
VPTV Vt
(Bragg.C et al., 2002a)
VPTV95%=Volume of Planning Target Volume receiving 95% of reference dose
Vptv=Volume of Planning Target Volume
Vt=Volume of tissue receiving 95% of reference dose
A CI of 1.0, represents the ideal, “in which the PTV coincides exactly with the treated
volume. A CI of 0 represents a plan in which there is no overlap between the two
volumes” (Bragg.C et al., 2002, p732). In clinical cases, it is rare for the ideal to occur.
For example a plan with a CI of 0.7 is considered to be a plan where the 95% isodose
line conforms well to the PTV (Bragg.C et al., 2002).
3.10.5 Statistical Analysis
Statistical analysis was performed on CI data, mean maximum doses to critical
structures and mean dose to the parotid gland using SPSS for windows version 12.0.1.
Repeated measures ANOVA was used to determine whether there was a statistical
difference between at least two of the;
• mean CI data for all beam arrangements.
• mean maximum doses to all critical structures
• mean parotid doses
If repeated measures ANOVA determined a statistically significant difference between
at least two of the IMRT beam arrangements, further analysis was performed. A

69
“Tukey honestly significant difference” (HSD) test was used to determine which IMRT
beam arrangements were significantly different.
In order to perform the HSD test all results were grouped from lowest value to highest
value. The highest value was statistically compared with the lowest value and then the
2nd lowest value and continued through all results. Next the 2nd highest value was
statistically compared with the lowest value and the 2nd lowest value and continued
through the list. This method of comparisons resulted in the least number of
calculations needed to derive a number of results.
For all results a table was produced listing beam arrangements from worst through to
best to aid in identifying beam arrangements producing the; highest CI, the lowest
mean maximum critical structure dose and the lowest mean contra-lateral parotid dose.
This data was used to determine the preferred IMRT beam arrangement for treating
skin tumours of the temple region that had spread to the parotid gland.
The two best IMRT beam arrangements determined by statistical analysis were shown
by DVH representation to a radiation oncologist at the RBWH. Dr Liz Kenny
determined the best clinical IMRT beam arrangement based on her expert opinion.
This IMRT plan was then compared with the optimised 3DCRT plan.
Comparison of the optimised 3DCRT with the best IMRT beam arrangement plan was
compared for each patient, using the “Students Paired T-test”. The statistical software
package that was used in the analysis was Microsoft excel.
*=Dr Lyndall Kelly

70
CHAPTER 4
RESULTS
4.1 Computerised Tomography (CT) Data
On each CT data set eight IMRT plans and one 3DCRT plan were performed. Detailed
in Table 7 is the beam arrangement number assigned to each beam arrangement. See
section 3.7.2 for details of beam arrangements.
Table 7- Table showing beam arrangement number associated with beam arrangement
BEAM ARRANGEMENT BEAM ARRANGEMENT
NUMBER 9 beam equispaced 1
7 beam equispaced 2 7 beam 3 5 beam ipsilateral 4
5 beam (3ipsilateral +2) 5
5 beam (4equispaced +1) 6 4 beam ipsilateral 7 3 beam ipsilateral 8
3D plan 9
4.2 Volume Structure Analysis 4.2.1 Structure Volumes
Structure volumes were outlined twice for each patient, once for the IMRT plan and
once for the 3DCRT plan as explained in section 3.6.1. Volume data for critical
structures were obtained from DVH associated output. An example is provided in
Table 8. Visual analysis of structure outlining was also performed to ensure that the
critical structure was outlined in the same spatial position on the CT axial slices. All
critical structures were outlined in the same position on both CT data sets.

71
Table 8-Table comparing structure volumes for one CT data set STRUCTURE IMRT VOLUME (cc) 3DCRT VOLUME (cc) Body 5889.7 5362.1 Brain 1249.9 1231.1 Brainstem 8.9 10.6 Eam 0.4 0.2 Ipsilateral lens 0.4 0.4 Ipsilateral retina/optic nerve 4.9 2.8 Mandible 44.2 41.3 Optic chiasm 0.8 1.3 Oral cavity 28 31 Parotid 16.4 17.2 Ptv 182.5 165.5 Contralateral lens 0.5 0.4 Contralateral retina/optic nerve 4 2.5 Spinal cord 11.2 9
4.2.2 Bland and Altman Analysis
Bland and Altman analysis was performed on IMRT and 3DCRT volumes for all
structure volumes in each data set. Table 9 is an example of the data for the body
structure.
Table 9- Body structure volume data
PATIENT CT DATA SET IMRT VOL(cc) 3D VOL(cc)
MEAN VOL(cc)
DIFF(cc) (IMRT-3D)
A 5889.7 5362.1 5625.9 527.6 B 7118.2 6872.3 6995.25 245.9 C 10879.5 10644.6 10762.05 234.9 D 9141.8 8365.8 8753.8 776 E 11819.1 11210 11514.55 609.1 F 7005 6612.2 6808.6 392.8 G 7794.8 7644.3 7719.55 150.5 H 12706.5 12658 12682.25 48.5 I 6978.9 6726.1 6852.5 252.8
Data for structure volumes were graphed on a Bland and Altman plot. A Bland and
Altman plot makes it easy to visualise limits of agreement (LOA) of the IMRT and
3DCRT structure volumes.

72
In the Bland and Altman analysis, the calculated mean difference is the bias. LOA are
defined as ± two standard deviations of the differences about the bias. Thus for the
body volume, LOA were ± 471.9 about 359.8.
Graphed below (Figure 29) is an example of a Bland and Altman plot for body
volumes. On the graphs below, yellow and orange lines represent the LOA. A pink
line represents the bias. This plot visually demonstrates LOA about the mean in order
to determine if LOA are clinically acceptable. Bland and Altman plots were performed
on all volume structures and LOA were determined to be clinical acceptable for
structures.
A clinically acceptable variation in structure volumes was determined when the
magnitude of the LOA was small. A small variation in structure volume would not
alter the planning process or outcome. LOA were considered clinically acceptable for
all structures except the body volume. For example the LOA for body structure were
±471.9 about the mean, compared with LOA of the spinal cord which was ±9.6 about
the mean. It is acknowledged that the body volume was the largest structure volume
outlined and produced the greatest variation. The magnitude of the body LOA
indicates that a variation in outlining body structures occurred between the two CT
data sets.
Figure 29- Bland and Altman plot of body structure volumes.
Bland and Altman Plot of Body Volume
-500
-100
300
700
5000 8000 11000
Mean Body Volume (cc)
Bod
y V
olum
e D
iffer
ence
(cc)
Data
LowerLOA
Mean
UpperLOA

73
Visual analysis of structure outlining was also performed to ensure that the critical
structure was outlined in the same spatial position on the CT axial slices. All critical
structures were outlined in the same position on both CT data sets.
4.3 3DCRT Dosimetry
As discussed in section 3.7.1, 3DCRT dosimetry of the two matching techniques was
performed, producing plans A&B.
• Plan A=electron field matching divergent edges of oblique photon fields where
they cross on skin.
• Plan B=electron field matching the divergent edges of the oblique photon fields
on skin, on alternate days.
The minimum, maximum and mean dose to the PTV, and the dose covering 95% of the
PTV in each plan were obtained from DVH output data (Table 10).
Table 10- Doses from 3DCRT plans with different photon-electron junction matching techniques.
Plan A=electron field matching divergent edges of oblique photon fields where they cross on skin.
Plan B=electron field matching the divergent edges of the oblique photon fields on skin, on
alternate days.
Plan A is the junction matching technique that was used in this research study. There
was no difference between the two plan techniques for minimum dose and 95%
coverage dose. The small difference in maximum dose is minimal and considered
clinically insignificant. The difference of greater than 1 Gy in the mean dose, is of
clinical relevance but does not indicate that over and underdosing of the PTV in the
photon-electron junction region is minimised by performing dosimetry as in Plan B.
Plan A Plan B
Minimum dose (Gy) 21.50 21.50
Maximum dose (Gy) 69.64 69.94
Mean dose (Gy) 60.34 61.48
95% Dose coverage (Gy) 45.00 45.00

74
As a result, for this research study it is assumed that performing dosimetry as per
standard RBWH clinical practice is justified.
4.4 Conformity Index (CI)
CI was calculated for every plan using the equation demonstrated in section 3.10.4.
Values substituted into the equation were obtained from DVH’s associated with the
dose distributions. The mean CI for each beam arrangement is demonstrated in Figure
30. The closer the CI is to 1.0, the more conformal 95% of the reference dose is to the
PTV.
Figure 30-Graph of CI for each beam arrangement
0
0.2
0.4
0.6
Mean CI
1 2 3 4 5 6 7 8 9
Beam arrangement number (refer Table 7)
Graph of Mean CI vs Beam Arrangement Number
Mean CI
4.4.1 Repeated Measure ANOVA on CI
Repeated measures ANOVA was performed on CI results for the IMRT beam
arrangements. A level of significance of 0.05 was used in determining that a
significant difference existed between at least two of the means. A post hoc “Tukey
Honestly Significant Difference” (HSD) test determined which of the beam
arrangements were significantly different.
Figure 31 demonstrates results in order from the lowest CI to the highest CI. Results
show that the CI for beam arrangements-5 and 8 are significantly lower than all other
beam arrangements except for beam arrangement-4 and each other (p<0.05). Beam

75
arrangement-4 was significantly different to the beam arrangements with the four
highest CI values. Beam arrangement-7 was significantly different to beam
arrangement-6 (p<0.05).
Figure 31-Graph of Mean CI vs beam arrangement number. Indicates beam arrangements-
8&5 were significantly different to all beam arrangements except beam arrangement-4 and each
other. Beam arrangement-4 was significantly different to the beam arrangements with the 4
highest CI values. Beam arrangement-7 was significantly different to beam arrangement-6.
0
0.2
0.4
0.6
Mean CI
8 5 4 7 1 6 3 2
Beam arrangement number (refer Table 7)
Graph of Mean CI Vs Beam arrangement
8
5
4
7
1
6
3
2
Figures 32a and 32b, demonstrate CI as a distribution. The isodose distributions are in
cGy per fraction. For example, the reference dose is 63 Gy in 30 fractions, which is
equivalent to 210 cGy per fraction. Thus the daily 95% isodose line that must conform
to the PTV is 200 cGy. The figures demonstrate how beam arrangement-3 is more
conformal than beam arrangement-8.

76
Figure 32a- Beam arrangement-3 demonstrating PTV conformity
Figure 32b- Beam arrangement 8 demonstrating PTV conformity distribution
4.5 DVH Range Analysis of the PTV
Similar to statistical analysis of the CI, repeated measures ANOVA was performed on
mean DVH PTV range data, for IMRT beam arrangements. A level of significance of

77
0.05 was used to determine that a significant difference existed between at least two of
the DVH PTV ranges. A post hoc Tukey HSD test was used to determine which beam
arrangements were significantly different (Figure 33).
Figure 33- Graph of mean DVH PTV range vs beam arrangement number. Indicates that beam
arrangement-4 and 8 were significantly different to the four beam arrangements with the lowest
PTV DVH ranges. No significant difference existed between other beam arrangements.
0
10
20
30
Mea
n P
TV
DV
H
(Gy)
3 2 1 6 5 7 4 8
Beam arrangement number (refer Table 7)
Graph of Mean PTV DVH Range Vs Beam Arrangement Num ber
3 2 1 6 5 7 4 8
4.6 Mean Doses
Mean dose to the contralateral parotid gland and mean maximum doses to all other
critical structures were obtained from DVH associated data. Repeated measures
ANOVA were performed on all doses for all IMRT beam arrangements. Table 11
demonstrates a summary of all results.

78
Table 11- Table showing the results of repeated measures ANOVA.
Structure
Significant difference
P-value
Parotid Yes <0.001 Body No 0.251
Mandible No 0.356 Brain Yes <0.001
Brainstem Yes <0.001 Ipsilateral Lens Yes <0.02
Contralateral Lens Yes 0.001 Ipsilateral
Retina/optic Nerve Yes <0.001 Contralateral
Retina/optic nerve Yes <0.001 Optic Chiasm Yes <0.001 Oral Cavity Yes <0.001 Spinal Cord Yes <0.001
For each structure showing significant difference between at least two of the means,
bar graphs were constructed to visually assess and assist in identifying which beam
arrangements were significantly different to one another (Figures 34-44). On the x-
axis of all graphs, beam arrangement number is visualised from those producing the
highest dose to the lowest dose.
For all structures that showed significant difference, a Tukey HSD test was performed
to determine which particular beam arrangements produced a significantly different
mean dose for the contralateral parotid gland or mean maximum dose for all other
structures. Detailed with figures 34-44 below, are results of the Tukey HSD test for all
critical structures.

79
4.6.1 Mean Contralateral Parotid Gland Dose
Figure 34-Graph showing mean contralateral parotid dose delivered by each IMRT beam
arrangement. Significant difference exists between beam arrangement-7 & 3 and all other
beam arrangements.
0
400
800
1200
Mea
n co
ntal
ater
al
paro
tid d
ose
(cG
y)
8 5 4 6 2 1 3 7
Beam arrangement number (refer Table 7)
Graph of Mean Contralateral Parotid Dose Vs Beam Arrangement Number
8 5 4 6 2 1 3 7
4.6.2 Mean Maximum Brain Dose
Figure 35- Graph of mean maximum brain dose from IMRT beam arrangements. Beam
arrangements-5 and 7 respectively are significantly different to all others except their closest
counterparts . Beam arrangement-8 is significantly higher than all except beam arrangements-
4&1. Beam arrangement-6 is significantly lower then 4, 5 &8.
0
2000
4000
6000
Mea
n m
ax b
rain
dos
e (c
Gy)
5 8 4 1 2 3 6 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Brain Dose vs Beam Arrangement Number
5 8 4 1 2 3 6 7

80
4.6.3 Mean Maximum Brainstem Dose
Figure 36- Graph showing maximum doses to brainstem volume for all IMRT beam
arrangements. Beam arrangement-7 is significantly lower than all other beam arrangements.
Beam arrangement-5 is significantly higher than all others except 8&4. Beam arrangement-6 is
significantly lower to doses higher than beam arrangement-2. Beam arrangement-3 is
significantly different to doses higher than beam arrangement 4.
0
1000
2000
3000
4000
5000
Mea
n m
ax b
rain
stem
dose
(cG
y)
5 8 4 2 1 3 6 7
Beam arrangement number (refer Table 7)
Graph of Mean Max Brainstem Dose vs Beam Arrangemen t Number
5 8 4 2 1 3 6 7
4.6.4 Mean Maximum External Auditory Meatus (eam) Dose
Figure 37- Graph showing mean maximum doses to eam volume for IMRT beam arrangements.
Beam arrangement-7 is significantly different to all other beam arrangements except beam
arrangement-3. Beam arrangement-3 is significantly different to all beam arrangements except
beam arrangement-5&7. Beam arrangement-2 is significantly different to all except beam
arrangement-6. Beam arrangement-6 is significantly different to beam arrangement-2&5.
0.00
500.00
1000.00
1500.00
2000.00
2500.00
Mea
m m
ax e
am d
ose
(cG
y)
2 6 1 8 4 5 3 7Beam arrangement number (refer Table 7)
Graph of Mean Maximum Eam Dose vs Beam Arrangement Number
2 6 1 8 4 5 3 7

81
4.6.5 Mean Maximum Ipsilateral Lens Dose
Figure 38- Graph showing mean maximum doses to ipsilateral lens volume for all IMRT beam
arrangements. Beam arrangement-5 & 7 are significantly different to each other, but no other
beam arrangements are significantly different.
0
500
1000
1500
2000
Mea
n m
axim
um
lens
dos
e (c
Gy)
5 4 3 2 8 1 6 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Ipsilateral Lens Dose Vs Beam Arrangement Number
5 4 3 2 8 1 6 7
4.6.6 Mean Maximum Contralateral Lens Dose
Figure 39- Graph showing maximum doses to contralateral lens volume for all IMRT beam
arrangements. Beam arrangement-7 produces a significantly lower dose then all other beam
arrangements.
0
500
1000
1500
Mea
n m
ax c
onra
late
ral
lens
dos
e (c
Gy)
4 1 8 2 5 6 3 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Contralateral Lens Dose vs Beam Arrangement Number
4 1 8 2 5 6 3 7

82
4.6.7 Mean Maximum Ipsilateral Retina/Optic Nerve Dose
Figure 40- Graph showing maximum doses to ipsilateral retina/optic nerve volume for all IMRT
beam arrangements. Beam arrangement-7 produces a significantly lower dose to all others
except beam arrangement-6. Beam arrangements-5 produces a significantly higher dose to all
beam arrangements with a dose less than beam arrangement-1. Beam arrangements-8
produces a significantly higher dose to all beam arrangements with a dose less than beam
arrangement-2. Beam arrangements-4 produces a significantly higher dose to all beam
arrangements with a dose less than beam arrangement-3.
0
1000
2000
3000
4000
5000
Mea
n m
ax
ipsi
late
ral
retin
a/op
tic n
erve
do
se (c
Gy)
5 8 4 1 2 3 6 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Ipsilateral Retina/optic Nerv e Dose vs Beam Arrangement Number
5 8 4 1 2 3 6 7
4.6.8 Mean Maximum Contralateral Retina/Optic Nerve Dose
Figure 41- Graph showing maximum doses to contralateral retina/optic nerve volume for all
IMRT beam arrangements. Beam arrangement-7 is significantly lower than all other beam
arrangements except beam arrangement-3. Beam arrangement-3 is significantly different to all
other beam arrangements except its closest counterparts.
0
1000
2000
3000
Mea
n m
ax
cont
rala
tera
l
retin
a/op
tic n
erve
dose
(cG
y)
6 8 1 4 2 5 3 7Beam arrangement number (refer Table 7)
Graph of Mean Maximum Contralateral Retina/optic Nerve Dose vs Beam Arrangement Number
6 8 1 4 2 5 3 7

83
4.6.9 Mean Maximum Optic Chiasm Dose
Figure 42- Graph showing mean maximum doses to optic chiasm volume for all IMRT beam
arrangements. Beam arrangement-7 is significantly lower than all other beam arrangements.
Beam arrangement-3 is significantly lower than 4 &8. Beam arrangement-5 is significantly lower
than 4.
0.00
1000.00
2000.00
3000.00
4000.00
Mea
n m
ax o
ptic
chi
asm
do
se (
cGy)
4 8 1 2 6 5 3 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Optic Chiasm Dose vs Beam Arr angement Number
4 8 1 2 6 5 3 7
4.6.10 Mean Maximum Oral Cavity Dose
Figure 43- Graph showing mean maximum doses to oral cavity volume for all IMRT beam
arrangements. Beam arrangements- 8, 5 &4 are significantly higher then beam arrangements-
1,2 ,6 ,3&7 .
0.00
1000.00
2000.00
3000.00
4000.00
Mea
n m
ax o
ral
cavi
ty d
ose
(cG
y)
8 5 4 1 2 6 3 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Dose to Oral Cavity vs Beam Arrangement Number
8 5 4 1 2 6 3 7

84
4.6.11 Mean Maximum Spinal Cord Dose
Figure 44- Graph showing maximum doses to spinal cord volume for all IMRT beam
arrangements. Beam arrangement-7 is significantly different to all other beam arrangements.
Beam arrangement-5 produces a significantly higher spinal cord dose to all beam arrangements
except 2 & 8.
0.00
2000.00
4000.00
6000.00
Mea
n m
ax s
pina
l co
rd d
ose
(cG
y)
5 2 8 4 1 6 3 7
Beam arrangement number (refer Table 7)
Graph of Mean Maximum Spinal Cord Dose vs Beam Arrangement Number
5 2 8 4 1 6 3 7
4.7 Grouped Results
For all results indicated, a table was produced (Table 12) listing beam arrangements
from worst through to best. For critical structures, all beam arrangements are listed
from those producing the highest mean maximum dose to the lowest mean maximum
dose. For conformity index, beam arrangements are listed from those producing the
lowest CI to the highest CI. For mean contralateral parotid dose, beam arrangements
are listed from those producing the highest mean parotid dose to the lowest mean
parotid dose. Thus beam arrangement numbers at the bottom of the list indicate better
results than those at the top of the list.

85
Table 12-Grouped results –beam arrangements listed in order of beam arrangements producing
the worst results (top of table) to beam arrangements producing the best results (bottom of table).
Brain Max
Brain Stem EAM
Contra-lateral retina/ optic nerve
Contra-lateral
lens Optic
Chiasm Oral
Cavity
Ipsi-lateral lens
Ipsi-lateral retina/ optic nerve
Spinal cord
Mean Parotid
5* 5* 2* 6* 4* 4* 8* 5* 5* 5* 8* 8* 8* 6* 8* 1* 8* 5* 4 8* 2* 5* 4* 4* 1* 1* 8* 1* 4* 3 4* 8* 4* 1* 2* 8* 4* 2* 2* 1 2 1* 4* 6* 2* 1* 4* 2* 5* 6* 2 8 2* 1* 2* 3* 3* 5* 5* 6* 5* 6 1 3* 6* 1* 6 6* 3 3 3* 3* 3 6 6 3* 3* 7 7 7 7 7 7 7 7 7 7 7 *=Significantly different to the best result (p<0.05).
CI
PTV DVH Range
8* 8*
5* 4*
4* 7
7 5
1 6
6 1
3 2
2 3
*=Significantly different to the best result (p<0.05).
Table 12 demonstrates that beam arrangement-7 (Table 7) is the best IMRT plan for
delivering the lowest doses to critical structures, followed by beam arrangement-3.
Beam arrangement-2 and beam arrangement-3 are the best IMRT plans for CI and PTV
DVH range.
Critical structure dose, DVH range and CI values are all equally important in
determining which IMRT beam arrangement is considered to provide the best
dosimetric plan for this disease site. Thus a beam arrangement would need to produce

86
good results in all three areas in order to be the best beam arrangement. Good results
are indicated by beam arrangements presenting at the bottom end of table 12. Beam
arrangement-7 produced good results in critical structure dose but not in CI or DVH
range. Beam arrangement-2 produced good results in CI and DVH range, but not in
critical structure dose. Beam arrangement-3 consistently produced good results in
critical structure dose, DVH range and CI values. Thus beam arrangement-3 is
considered to be the best IMRT plan.
4.8 Radiation Oncologist Clinical Analysis of IMRT Plans
Dr Liz Kenny at the RBWH determined the best clinical IMRT beam arrangement
from the dosimetric results and DVH analysis. Particular attention was given to beam
arrangement-3 and beam arrangement-7. Dr Kenny determined that beam
arrangement-3 (7 beam IMRT arrangement) was the best of the IMRT beam
arrangements. This decision was based on the fact that critical structures were
considerably lower but PTV conformity and dose ranges were improved over beam
arrangement-7 (4 beam ipsilateral arrangement).
Conclusion from the clinical preference of the radiation oncologist and statistical
results, is that beam arrangement-3 is the best IMRT beam arrangement to treat skin
lesions of the temple region with spread to the parotid gland.
4.9 IMRT Vs 3DCRT
Statistical analysis was performed on the best IMRT beam arrangement and compared
with results for standard 3DCRT treatment. The student’s paired t-test was performed
using Microsoft excel, to determine if significant difference existed between the mean
CI, mean maximum critical structure doses and PTV dose ranges of the two treatment
options (Table 13). Significant difference was determined with a p-value <0.05.
Where significant difference exists, sections 4.9.1-4.9.3 will explain whether results
indicate that the 7-beam IMRT treatment was better or worse than the 3DCRT
treatment.

87
Table 13- Table demonstrating any significant difference between measures of 3DCRT plans and
the 7-beam IMRT arrangement
Measure
Significant Difference
P-Value if Significantly
different
CI yes <0.05
PTV Range yes <0.05
Brain yes <0.05
Brainstem yes 0.02
Eam yes <0.05
Contralateral ret/optic
nerve
yes <0.05
Contralateral lens yes 0.03
Optic chiasm yes <0.05
Oral cavity no -
Ipsilateral lens no -
Ipsilateral ret/optic nerve no -
Spinal cord yes <0.05
Mandible no -
Body no -
Mean contralateral parotid yes <0.05
4.9.1 CI
The conformity index of the 7-beam IMRT plan was significantly higher than the
3DCRT plan. As a result the 7-beam IMRT plan was greatly improved over the
3DCRT plan. This is demonstrated in figure 45a&b where the 95% isodose line (200
cGy/fraction), is conforming more tightly around the PTV.

88
Figure 45a&b- Improved CI is visualised by the 95% isodose line in the 7-beam IMRT plan when
compared to the 3DCRT plan.
Figure 45a-7-beam IMRT plan
Figure 45b-3DCRT plan

89
4.9.2 DVH Range Analysis of the PTV
The mean PTV dose range was significantly lower for the 7-beam IMRT arrangements
when compared to the 3DCRT beam arrangements. As a result the 7-beam IMRT
distribution was a better distribution around the PTV than the 3DCRT plan. This is
visualised in the slope of the PTV DVH, in figures 46a and 46b. The 3DCRT PTV
DVH is not a steep fall off from the 95% volume mark, when compared to the 7-beam
IMRT PTV DVH.
Figure 46a -DVH demonstrating Figure 46b-DVH demonstrating
3DCRT distribution. IMRT distribution.
4.9.3 Critical Structure Analysis
The mean and mean maximum dose to the majority of critical structures (table 12) was
significantly higher in the 7-beam IMRT plan when compared to the 3DCRT plan.
Figure 47 is a visual demonstration of doses to some critical structures for the two
plans. In this figure, the IMRT plan is delivering approximately; 43 cGy to the oral
cavity, 104 cGy to the spinal cord and 21 cGy to the contralateral parotid gland. The
3DCRT beam arrangement is delivering approximately; 42 cGy to the oral cavity, 42
cGy to the spinal cord and no dose to the contralateral parotid gland.

90
Figure 47a&b- Figures demonstrating mean and mean maximum doses in cGy to critical
structures for the 7-beam IMRT arrangement and the 3DCRT beam arrangement.
Figure 47a-7-beam IMRT beam arrangement
Figure 47b-3DCRT beam arrangement

91
4.10 Radiation Oncologist Clinical Analysis of 3DCRT and 7-Beam IMRT
Plans
Results and DVH outputs were presented to a radiation oncologist at the RBWH to
determine the clinically preferred radiation treatment. Dr Kenny determined
advantages in the 7-beam IMRT arrangement for CI and PTV range, outweighed
increases in radiation doses to critical tissues, if critical structures did not exceed
maximum tolerance doses. The contralateral lens was the only critical structure that
exceeded tolerance dose.

92
CHAPTER 5
DISCUSSION
This research project compared dose distributions of eight different IMRT beam
arrangements and determined the optimal IMRT beam arrangement and thus, class
solution, to treat skin lesions of the temple region with extension into the parotid gland.
This IMRT distribution was compared with the 3DCRT plan to determine the better
treatment option. Comparison was performed by dose based analysis on structure
volume, CI, PTV dose range and critical structures.
5.1 Structure Volume Analysis
This research project required CT data sets of each patient to be outlined twice as
detailed in section 3.6.1. The LOA magnitudes were assessed to determine if outlining
of critical structures were clinically acceptable. Results indicate that for each patient
there was minimal variation between the two outlined CT data sets for all volumes
except the body structure.
The variation in body structure outlining between the two CT data sets can be
explained by the introduction of bolus. Limitations of the PLATO planning system
required 3DCRT CT data sets to be outlined without the inclusion of bolus. Bolus was
added to the 3DCRT data set at a later stage of the planning process, but in a section of
the PLATO planning system that does not incorporate the bolus addition to the
magnitude of body volume structure. IMRT CT data sets required outlining with the
inclusion of bolus. The PLATO planning system includes the bolus addition when
assessing body structure volume. As a result the magnitude of body volume structure
was considerably different between the two data sets.
The differences in body volume structure between the two CT data sets can be
accounted for by the addition of bolus accommodating PLATO planning system
limitations. Thus results concerning doses to structure volumes between IMRT and
3DCRT plans could be compared.

93
5.2 3DCRT Dosimetric Considerations
For all 3DCRT plans, ICRU 50 guidelines were adhered to as closely as possible. The
aim of treatment was for 95% of the reference dose (RD) to cover the PTV while the
maximum dose was not to exceed 107% of the reference dose. DVH range analysis on
the PTV was assessed to determine if guidelines were followed.
The shape of the PTV DVH was similar in all 3DCRT plans. Figure 48 provides two
examples of 3DCRT DVH’s. Both PTV’s as shown on the DVH, fall well short of
achieving 95% of the RD, which is 60 Gy. In both cases it can be seen that
approximately 50 Gy is covering 95% of the PTV.
Figure 48- DVH’s of 3DCRT plans from different CT data sets demonstrating similarities in PTV
The slope of the curve as visualised in figure 48 is steep from the 80% volume position,
but is shallow from the 95% volume position. An ideal plan is one which produces a
PTV DVH that is steep from the 95% volume position. 3DCRT plans in this study did
not achieve the aim of treatment, which is for 95% of the RD to cover the PTV. This is
the reason why the PTV range in 3DCRT plans is so large.

94
PTV DVH’s do not indicate which part of the PTV is not achieving 95% of the RD.
Assessing the axial slices of all 3DCRT plans, visually indicated that the photon-
electron junction was the region not achieving ICRU 50 guidelines.
As described in section 2.10.4, when electrons and photons are junctioned on skin, a
hot spot will occur on the photon side, inferior to the junction and a cold spot will
occur on the electron side, superior to the junction. This cold spot can result in less
than 95% of the RD covering the PTV in this region. For example, Figure 49
demonstrates inadequate coverage of the PTV on the electron side of the photon-
electron junction region. The maximum dose in figure 49 is 167 cGy per fraction
which is 80% of the daily dose required, thus it is impossible for 95% of the daily RD
to cover the PTV. This figure shows that only 126 cGy or 63% is covering the PTV.
Figure 49- 3DCRT axial slice of junction region demonstrating poor coverage of the PTV.
As discussed in section 2.10.4, low dose to the PTV is undesirable because it increases
the risk of tumour recurrence. Conformity of the 95% of the daily dose to the PTV in

95
this junction region is not a concern for IMRT distributions, because as discussed in
the introduction, there is no junction region in the upper face fields.
5.3 IMRT Dosimetric Considerations
For all IMRT plans, RTOG guidelines were adhered to as closely as possible to avoid
underdosing and overdosing of the PTV. In every IMRT plan, 95% of the RD (60 Gy)
covered the PTV, but in order to achieve this, compromises were made between the
maximum and minimum doses to the PTV. In many cases 95% of the PTV could not
be achieved without exceeding the maximum dose (Figure 50). Figure 50 shows 95%
of the PTV receiving 60 Gy, but in order to achieve this goal, approximately 20% of
the volume is receiving greater than 114% of the RD and 4% of the PTV volume is
receiving 93% of the RD.
Figure 50- DVH demonstrating compromise made when determining optimal IMRT distribution.

96
Violation of RTOG and ICRU guidelines results in PTV underdosing and overdosing.
The extent of violation was examined through results of DVH range analysis of the
PTV.
5.4 DVH Range Analysis of the PTV
A more homogenous distribution results from reduced underdosing and overdosing, of
the PTV. The PTV DVH range is a good indicator of a homogenous PTV distribution.
The smaller the PTV DVH range, the steeper the PTV DVH curve is resulting in a
more homogenous the PTV distribution. Section 3.10.2 discussed how the PTV DVH
range was determined. Of all the IMRT distributions, the 7-beam arrangement
produced the best PTV DVH. All IMRT beam arrangements above 7 beams plus the 5
beam- (4 equilateral +1), produced ranges within 1.6 Gy. These four IMRT beam
arrangements were the best at achieving guidelines. Bragg et al supports this finding
by stating, “there is a clear tendency toward better homogeneity when an increasing
number of fields were used” (Bragg.C et al., 2002, p734).
This study introduced three ipsilateral beam IMRT arrangements to determine the
effect on underdosing and overdosing of the PTV. Results demonstrate these beam
arrangements violated guidelines and produced the most underdosing and overdosing
of the PTV. Bragg et al suggested that introducing a number of beams from the same
side as the tumour would reduce target overdosing and underdosing (Bragg.C et al.,
2002). This study determined the opposite to be true.
The average DVH range analysis for the 3DCRT PTV was 47.2 Gy compared to 17.1
Gy for the 7-beam IMRT arrangement. A Statistically significant difference (p<0.05)
was determined between these two figures, indicating the 7-beam IMRT distribution
(Figure 51a) was a better distribution than the 3DCRT distribution (Figure 51b)
because it adheres to guidelines and avoids overdosing and underdosing of the PTV,
especially in the junction region while still achieving 95% dose coverage. This is
shown by the steep fall-off of the PTV from the 95% dose coverage in figure 51b. In

97
comparison, figure 51a shows a shallow PTV fall-off dose from the 99% volume down
to the 80% volume as detailed in section 5.2.
Figure 51a -DVH demonstrating Figure 51b-DVH demonstrating
3DCRT distribution. IMRT distribution.
One hypothesis of this research project was that IMRT would enable avoidance
problems in the junction region. IMRT avoids overdosing and underdosing problems
in the junction region by eliminating the need for a second junction during treatment.
The final outcome is a more homogenous PTV distribution which is indicated by PTV
DVH range statistical analysis.
5.5 IMRT CI Analysis
CI was assessed to determine how well the 95% isodose line conforms to the PTV. Of
all the IMRT plans, the 7-beam equitorial spaced beam arrangement proved to be the
most conformal. Similar to results for DVH PTV analysis, IMRT beam arrangements
above 7 beams plus the 5 beam- (4 equilateral +1), produced ranges within 0.02.
These 4 IMRT beam arrangements were the best at achieving conformity.

98
PTV analysis by CI and DVH range, show that IMRT beam arrangements above 7
beams along with a 5-beam arrangement (4-equitorial + 1ipsilateral), produce adequate
PTV coverage.
5.6 IMRT Critical Structure Analysis
Various IMRT beam arrangements produced different doses to critical structures. The
4-beam ipsilateral IMRT plan consistently produced the lowest dose to all critical
structures. The 7 field beam arrangement produced the next best results by delivering
the lowest dose to the; eam, contralateral lens and retina/optic nerve, spinal cord, oral
cavity and optic chiasm (Figure 52a).
Beam arrangement-5 (3 beam ipsilateral + 2) was the worst IMRT plan, producing the
highest doses to the brain, brainstem, ipsilateral structures and spinal cord (Figure 52b).
Thus there is no advantage to a five field beam arrangement not being equally spaced.
In figures 52a&b, beam arrangement-5 shows a higher dose to the; contralateral and
ipsilateral retina/optic nerve and brain than the 7 beam IMRT arrangement.

99
Figure 52a- 7 beam IMRT distribution Figure 52b- Beam arrangement-5 IMRT
demonstrating doses to critical structures. distribution, demonstrating dose to critical
structures.
5.7 IMRT Mean Contralateral Parotid Dose
Different IMRT beam arrangements were able to reduce the contralateral parotid gland
dose. Reducing dose to the contralateral parotid decreases the radiation side-effect of
xerostomia. Thus improving patient’s quality of life, post radiation therapy and
reducing the cost burden of ongoing medical care provided by medical institutions.
The 4-beam ipsilateral and 7-beam arrangement produced significantly lower doses to
the contralateral parotid than any other IMRT plan.
5.8 Superior IMRT Plan
Studies of IMRT treatment of the parotid gland alone suggest beam arrangement-6 (5
beam (4equispaced +1)) is the superior IMRT treatment plan (Bragg.C et al., 2002).
This study determined that beam arrangement-6 did not produce the best overall results.
Doses to critical structures, PTV conformity and DVH range are all equally important
factors in determining the superior IMRT plan. As detailed in section 4.7, beam
arrangement 3 or the 7-beam IMRT arrangement performed well in all three

100
determining factors. As a result, the 7-beam IMRT arrangement is the superior IMRT
beam arrangement due to highly conformal and homogenous PTV distributions and
reduced critical structure doses.
Dr Liz Kenny of the RBWH confirmed these results with clinical reasoning. She
determined that the 7-beam IMRT arrangement was preferred over the 4-beam
ipsilateral arrangement because of improved PTV conformity and homogeneity.
IMRT treatment can take a long time to deliver, depending on the number of beams.
In 2001, Rowbottom et al determined a 9-beam arrangement to produce the superior
dosimetric plan for parotid gland tumours, although a compromise was made with a 7-
beam IMRT arrangement because it maintained improvements seen with the superior
plan, but a reduced number of beams made it more clinically efficient (Rowbottom.C
et al., 2001).
The 7-beam IMRT arrangement is considered to be clinically efficient to deliver in a
clinical environment. This statement is supported by radiation oncologists of the
RBWH. Thus statistically and clinically the 7-beam IMRT arrangement is the superior
IMRT treatment that is clinical efficient to deliver.
5.9 IMRT Class Solution
As discussed in section 2.13, class solutions for individual tumour sites are developed
to produce the optimal treatment plan with ease. This research determined the superior
IMRT plan, 7-beam arrangement to be the IMRT class solution, with defined beam
angles of; 40°,120°,160°,200°,240°,300°,0°.
A class solution is the, “historical experience in designing RT plans for a particular
site” (Intensity Modulated Radiation Therapy Collaborative Working, 2001, p913).
The historical experience of a class solution is a detailed step by step guide for a
particular disease site. For example, a class solution may involve; patient stabilisation,
PTV and critical structure contouring, prescription protocol, critical structure tolerance

101
dose and importance weightings, beam number and angles, minimum and maximum
dose constraints, quality assurance and treatment delivery.
This research study followed a step by step guide to define an IMRT class solution,
although this study mainly investigated beam numbers and angles. As a result the 7-
beam arrangement forms the basis of this IMRT class solution. Further investigations
may be conducted in support of this study, to determine precise detailed steps in this
class solution.
5.10 IMRT Vs 3DCRT
The optimal 7 beam IMRT arrangement was compared to the standard 3DCRT plan.
Results demonstrate that the IMRT distribution provides better PTV conformity and
dose homogeneity. A study by Cozzi et al supports this conclusion by stating,
“delivered IMRT dose plans showed a systematic and highly significant improvement
in terms of target coverage compared to reference 3DCRT” (Cozzi.L et al., 2004,
p622)
In contrast, analysis determined that higher doses were delivered to the majority of
critical structures with IMRT planning. Only the ipsilateral lens and the oral cavity
received lower doses with the optimal IMRT plan.
One hypothesis of this research project was that the IMRT class solution would enable
lower doses to critical structures, thus allowing an increased tumour dose to be
delivered, resulting in increased local control. Results of this study indicate that higher
doses were delivered to critical structures with IMRT planning. As a result an
increased tumour dose could not be delivered thus increased local control cannot be
assessed. Therefore this hypothesis was disproved.
The mean contralateral parotid dose was also significantly increased with IMRT
planning, although it did not exceed the maximum tolerance dose. Previous research
has determined similar increases in parotid gland doses with IMRT planning.

102
“Unfortunately, the IMRT plan greatly increased the dose to the contralateral parotid
gland” (Rowbottom.C et al., 2001, p170).
To determine if IMRT is the superior treatment modality to 3DCRT, for treating skin
lesions of the temple region with extensions to the parotid gland, improvements in PTV
conformity and homogeneity must outweigh increased critical structure doses.
Doses delivered to critical structures via IMRT are higher than 3DCRT, but still not
exceeding dose tolerances determined in this research project. “In general, IMRT
plans increase the volume of OARs irradiated to low dose” (Rowbottom.C et al., 2001,
p170). Thus increasing doses to critical structures to a safe level is an acceptable
compromise for improved PTV conformity and homogeneity.
Radiation oncologists support this reasoning. Upon assessing PTV and critical
structure doses, the oncologists prefer treating skin lesions of the temple region with
extensions to the parotid gland with IMRT, if tolerance doses of critical structures are
not exceeded. This is because a more conformal and homogenous dose to the PTV will
decrease the risk of tumour recurrence and tissue morbidity.
5.11 Radiation Oncologist Clinical Preference
The superior IMRT beam arrangement delivered an ipsilateral lens dose just beyond its
critical tolerance. Results indicate that a balance exists between lens dose and PTV
conformity. For example, beam arrangement-7 (4-beam ipsilateral plan) produced a
significantly lower contralateral lens dose then the 7-beam IMRT arrangement. The
dose was below critical tolerance, but the trade-off was significantly lower PTV
conformity and poor PTV DVH range. There is no point to exceeding critical structure
dose tolerance if tumour dose is not improved. The 7-beam IMRT does improve
tumour dose, and only just exceeds lens tolerance dose.
If lens tolerance dose is exceeded, the complication end point is cataract formation. As
suggested in section 2.6, this complication may be an acceptable trade-off for potential

103
tumour cure because cataract formation can be reduced by surgery (Pawlicki.T et al.,
2004).
Radiation oncologist clinical preference for IMRT over 3DCRT was preferred to be
determined on a case by case basis, if tolerance doses were exceeded. For IMRT to be
the treatment choice, patients would need to present with an aggressive tumour
requiring PTV conformity and homogeneity that IMRT provides, while still being a
surgical candidate to reduce the radiation side-effect of cataract formation. If tumours
were not aggressive and surgery was not a viable option, 3DCRT would be the
preferred treatment option.
5.12 Future Directions
This research project determined results by assessing nine CT patient data sets. The
pre-requisite for inclusion of a CT data set was based on three field parameters
traditionally treated with 3DCRT. If sample pre-requisite was expanded to include
only patients with aggressive tumours that were medically fit to be potential surgical
candidates, then a more definitive result might be found.
Increasing sample group numbers and testing this class solution in a clinical
environment may influence results and outcomes. Increased sample number may
affect the compromise seen in this study, between the ipsilateral lens dose and PTV
conformity with IMRT plans.
One hypothesis of this study was to determine if the IMRT class solution would enable
avoidance problems in the junction region. IMRT does avoid problems because the
second junction is eliminated from treatment. Although further studies conducted
specifically on dose occurring in the photon-electron junction region with 3DCRT
treatment would better highlight problems.
Dose occurring in the photon-electron junction region in 3DCRT played a role in
determining the superior treatment plan in this research project. This study performed

104
dosimetry as conducted in a clinical setting. Resulting PTV DVH’s demonstrated that
95% of the RD was not covering the PTV, but DVH’s do not indicate the position on
the CT data, where the PTV is not covered by 95%. A future direction of this research
study would be to contour the PTV in the photon-electron junction region as a separate
structure for 3DCRT and IMRT planning. The DVH’s of this structure could then be
compared to accurately assess the dose occurring at this region from 3DCRT and
IMRT. Results from this study may better highlight any inhomogeneities in the
photon-electron junction region, and whether IMRT overcomes these.
This study determined the IMRT 7-beam arrangement as the class solution, with major
focus on determining beam number and arrangement. Current literature reports the
development of computerised beam angle selection and opitimisation algorithms to
determine the optimum beam angles and numbers. For example Wang et al developed
the ‘fast IMRT algorithm’ to provide, “a novel and realistic approach to study the
characteristics of IMRT dose distributions as a function of beam angles” (Wang.X et
al., 2004, p1326). Applying an optimisation algorithm to the disease site studied in
this research project would test the technical feasibility of the IMRT class solution of
the 7-beam IMRT arrangement.
Further studies may be carried out to develop a full and detailed class solution.
Incorporating steps such as; patient selection, patient positioning, critical structure
contouring, prescription protocol, quality assurance process plan and treatment
delivery may aid in developing a full and precise class solution.
The ultimate test of efficacy of a class solution must be the final outcome to the patient
in terms of tumour control and long-term side-effects. This takes time and is difficult
to measure in uncommon disease sites, although future studies may attempt to
document this.

105
CHAPTER 6
CONCLUSION
Skin lesions of the temple region with extensions to the parotid gland, is a treatment
site historically treated with three-dimensional conformal radiation therapy (3DCRT).
3DCRT requires this disease site to be treated with two junction regions, resulting in
poor dose conformity to the tumour target and high doses to critical structures.
Intensity modulated radiation therapy (IMRT) is a relatively new treatment technology
that has potential to overcome limitations associated with 3DCRT (Garden.A et al.,
2004). IMRT enables the disease site to be treated with one junction region, therefore
avoiding junction problems by providing high dose conformity to the tumour target.
This study has shown that the 7-beam IMRT arrangement with defined beam angles of;
40°,120°,160°,200°,240°,300°,0°, is the superior IMRT treatment plan, and thus class
solution for this disease site. This study has also shown that the IMRT class solution is
superior to 3DCRT in terms of planning target volume (PTV) conformity and
homogeneity, but not in terms of doses to critical structures. The resultant higher doses
to critical structures do not afford the potential to increase dose to the target volume
and thus increase local control.
The superior IMRT treatment plan delivered higher doses to the majority of critical
structures than the 3DCRT plan. Although, the only structure that just exceeded
critical tolerance was the ipsilateral lens. The complication end point for exceeding
lens tolerance dose is cataract formation. This study concluded that this complication
end point may be an acceptable trade-off for potential tumour cure because patients
may have the option for cataract formation to be reduced by surgery.
Clinical preference for accepting the IMRT class solution over 3DCRT treatment was
preferred to be determined on a case by case basis. For IMRT to be the treatment
choice, patients would need to present with an aggressive tumour requiring PTV

106
conformity and homogeneity that IMRT provides, while still being a surgical candidate
to reduce the radiation side-effect of cataract formation.
This study into skin lesions of the temple region with extensions to the parotid gland
determined the 7-beam IMRT arrangement to be the optimal IMRT class solution. A
definitive answer determining whether the IMRT class solution is superior to 3DCRT
did not result without conditions applied. This study suggests that the IMRT class
solution is the superior treatment option, only when patients are surgical candidates to
reduce the complication end point of cataract formation. This research study would
provide a good resource base to further investigations into this complicated disease site.

107
REFERENCES
Adams.E, Nutting.C, Convery.D, Cosgrove.V, Henk.J, Dearnaley.D and Webb.S (2001) Potential role of intensity-modulated radiotherapy in the treatment of tumors of the maxillary sinus,International Journal of Radiation Oncology, Biology, Physics, 51, 579-588.
Anderson.D, Keith.J, Novak.P and Elliot.M (2002) Mosby's Medical, Nursing, and
Allied Health Dictionary-6th Edition, Mosby, Missouri, USA. Barzilai.G, Greenberg.E, Cohen-Kerem.R and Doweck.I (2005) Pattern of regional
metastases from cutaneous squamous cell carcinoma of the head and neck,Otolaryngology - Head and Neck Surgery, 132, 852-856.
Bhattacharyya.N and Fried.M (2005) Determinants of survival in parotid gland
carcinoma: a population-based study,American Journal of Otolaryngology, 26, 39-44.
Bragg.C, Conway.J and Robinson.M (2002) The role ofintensity-modulated
radiotherapy in the treatment of parotid tumors,International Journal of Radiation Oncology, Biology, Physics, 52, 729-738.
Branislav.J, Shibamoto.Y and Igrutinovic.I (2002) Absence of Cervical Radiaiton
Myelitis After Hyperfractionated Radiation Therapy With and Without Concurrent Chemotherapy for Locally Advanced, Unresectable, Nonmetastatic Squamous Cell Carcinoma of the Head and Neck,Journal of Cancer Research and Clinical Oncology, 127, 687-691.
Budgell.G (2002) Intensity modulated radiotherapy (IMRT)-an
introduction,Radiography, 8, 241-249. Chao.K, Deasy.J, Markman.J, Haynie.J, Perez.C, Purdy.J and Low.D (2001) A
prospective study of salivary function sparing in patients with head-and-neck cancers receiving intensity-modulated or three-dimensional radiation therapy: initial results,International Journal of Radiation Oncology, Biology, Physics, 49, 907-916.
Claus.F, Gersem.W, Wagter.C, Severen.R, V., Vanhoutte.I, Duthoy.W,
Remouchamps.V, Duyse.B, V., Vakaet.L, Lemmerling.M, Vermeersch.H and Neve.W (2001) An implementation strategy for IMRT of Ethmoid sinus cancer with bilateral sparing of the oiptic pathways,International Journal of Radiation Oncology ,Biology, Physics, 51(2), 318-331.
Cook.B, Withrow.L, Spencer.S, Ove.R and Fiveash.J (2004) Radiation tolerance of the
optic apparatus,International Journal of Radiation Oncology, Biology, Physics, 60, S408-S409.

108
Cooper.J, Fu.K, Marks.J and Silverman.S (1995) Late effects of radiation therapy in the head and neck region,International Journal of Radiation Oncology, Biology, Physics, 31, 1141-1164.
Cozzi.L, Fogliata.A, Bolsi.A, Nicolini.G and Bernier.J (2004) Three-dimensional
conformal vs. intensity-modulated radiotherapy in head-and-neck cancer patients: comparative analysis of dosimetric and technical parameters,International Journal of Radiation Oncology, Biology, Physics, 58, 617-624.
Dabaja.B, Salehpour.M, Rosen.I, Tung.S, Morrison.W, Kian.A and Garden.A (2005)
Intensity-modulated radiation therapy (IMRT) of cancers of the head and neck: Comparison of split-field and whole-field techniques,International Journal of Radiation Oncology, Biology, Physics, 63, 1000-1005.
Debus.J, Hug.E, Liebsch.N, O'Farrel.D, Finkelstein.D, Efird.J and Munzenrider.J
(1997) Brainstem tolerance to conformal radiotherapy of skull base tumors,International Journal of Radiation Oncology, Biology, Physics, 39, 967-975.
Delcharco.J, Mendenhall.W, Parsons.J, Stringer.S, Cassisi.N and Menenhall.N (1998)
Carcinoma of the Skin Metastatic to the Parotid Area Lymph Nodes,Head Neck, 20, 369-373.
DeVita.V, Hellman.S and Rosenberg.S (1997) Cancer Prinicples and Practice of
Oncology Volume 1 Fifth Edition, Lippincott-Raven Publishers, Philadelphia, USA.
Emami.B, Lyman.J and Brown.A (1991) Tolerance of normal tissue to therapeutic
irradiaiton,International Journal of Radiation Oncology *Biology* Physics, 21, 109-122.
Esiashvili.N, Koshy.M and Landry.J (2004) Intensity-modulated radiation
therapy,Current Problems in Cancer, 28, 47-84. Fabrizio.P, McCullough.E and Foote.R (2000) Decreasing the dosimetric effects of
misalignment when using a mono-isocentric technique for irradiation of head and neck cancer,International Journal of Radiation Oncology, Biology, Physics, 48, 1623-1634.
Galvin.J, Ezzell.G, Eisbrauch.A, Yu.C, Butler.B, Xiao.Y, Rosen.I, Rosenman.J,
Sharpe.M and Xing.L (2004) Implementing IMRT in clinical practice: a joint document of the American Society for Therapeutic Radiology and Oncology and the American Association of Physicists in Medicine,International Journal of Radiation Oncology, Biology, Physics, 58, 1616-1634.

109
Garden.A, Morrison.W, Rosenthal.D, Chao.K, Clifford.S and Kian.A (2004) Target coverage for head and neck cancers treated with IMRT: review of clinical experiences,Seminars in Radiation Oncology, 14, 103-109.
Glanzmann.C and Gratz.K (1995) Radionecrosis of the mandibula: a retrospective analysis of the incidence and risk factors,Radiotherapy and Oncology, 36, 94-100.
Gregoire.V and Maingon.P (2004) Intensity-modulated radiation therapy in head and
neck squamous cell carcinoma: an adaptation of 2-dimensional concepts or a reconsideration of current clinical practice,Seminars in Radiation Oncology, 14, 110-120.
Harish.K (2004) Management of primary malignant epithelial parotid tumors,Surgical
Oncology, 13, 7-16. Henson.B, Eisbruch.A, D'Hondt.E and Ship.J (1998) Two-year longitudinal study of
parotid salivary flow rates in head and neck cancer patients receiving unilateral neck parotid-sparing radiotherpy treatment,Oral Oncology, 35, 1-8.
ICRU, International Commission on Radiation Units and Measurements ICRU 50,inc
(1993) In International commission on radiation units and measurements. ICRU, International Commission on Radiation Units and Measurements ICRU 63,inc
(1999) In International commission on radiation units and measurements. Intensity Modulated Radiation Therapy Collaborative Working, G. (2001) Intensity-
modulated radiotherapy: current status and issues of interest,International Journal of Radiation Oncology, Biology, Physics, 51, 880-914.
Jereczek-Fossa.B, Garibaldi.C, Catalano.G, D'Onofrio.A, Pas.T, Bocci.C, Ciocca.M,
DePaoli.F and Orecchia.R (2003) Analysis of mandibular dose distribution in radiotherapy for oropharyngeal cancer: dosimetric and clinical results in 18 patients,Radiotherapy and Oncology, 66, 49-56.
Kemikler.G (2006) Dosimetric effects of matching 6 MV photon and electron fields in
the treatment of head and neck cancers,Radiation Measurements, 41, 183-188. Khurana.V, Mentis.D, O'Brien.C, Hurst.T, Stevens.G and Packham.N (1995) Parotid
and neck metastases from cutaneous squamous cell carcinoma of the head and neck,The American Journal of Surgery, 170, 446-450.
Kuo.J, Cabebe.E, Al-Ghazi.M, Yakoob.R, Ramsinghani.N and Sanford.R (2002)
Intensity-modulated radiation therapy for the spine at the University of California, Irvine,Medical Dosimetry, 27, 137-145.

110
Lai.S and Weber.R (2004) Cutaneous malignancies of the head and neck,Operative Techniques in General Surgery, 6, 132-142.
Laramore.G (1987) Fast neutron radiotherapy for inoperable salivary gland tumors:is it
the treatment of choice?,International Journal of Radiation Oncology *Biology* Physics, 13, 1421.
Li.J, Liu.C, Kim.S, Amdur.R and Palta.J (2005) Matching IMRT fields with static
photon field in the treatment of head-and-neck cancer,Medical Dosimetry, 30, 135-138.
Licitra.L, Grandi.C, Prott.F, Schornagel.J, Bruzzi.P and Molinari.R (2003) Major and
minor salivary glands tumours,Critical Reviews in Oncology/Hematology, 45, 215-225.
Lord.L, May.S, Bailey.M and Smith.L (2003) Is one head and neck immobilization
system as good as another? One center's experience,Medical Dosimetry: Official Journal Of The American Association Of Medical Dosimetrists, 28, 39-43.
Manske.M, Barker.J, Wong.P, Westlake.W, Garden.A, Kian.A and Rosenthal.D (2004)
New equations for matching a low neck field to oblique upper neck fields with collimator rotation in a 3-field monoisocentric setup for head-and-neck cancers,Medical Dosimetry, 29, 86-91.
Marandas.P, Dharkar.D, Davis.A, M, L. A., Ojeda.L, P., Micheau.C, Wibault.P and
Schwaab.G (1990) Malignant tumours of the parotid: a study of 76 patients,Clinical Otolaryngology and Allied Sciences, 15, 103-109.
Marieb.E (1998) Human Anatomy and Physiology-4th Edition, Benjamin/Cummings,
Menlo Park, California. Moore.K and Agur.A (2002) Essential Clinical Anatomy-2nd Edition, Lippincott
Williams and Wilkins, Baltimore, USA. Nolan.R, Chan.M and Heenan.P (2005) A clinicopathologic review of lethal
nonmelanoma skin cancers in Western Australia,Journal of the American Academy of Dermatology, 52, 101-108.
Nutting.C, Rowbottom.C, Cosgrove.V, Henk.J, Dearnaley.D, Robinson.M, Conway.J
and Webb.S (2001) Optimisation of radiotherapy for carcinoma of the parotid gland: a comparison of conventional, three-dimensional conformal, and intensity-modulated techniques,Radiotherapy and Oncology, 60, 163-172.
O'Brien.C, Mcneil.E, Mcmahon.J, Pathak.I, Lauer.C and Jackson.M (2002)
Significance of Clinical Stage, Extent of Surgery and Pathologic Findings in

111
Metastatic Cutaneous Squamous Cell Carcinoma of the Parotid,Head Neck, 24, 417-422.
Pawlicki.T, Luxton.G, Le.Q, Findley.D and Ma.C (2004) Lens dose in MLC-based
IMRT treatments of the head and neck,International Journal of Radiation Oncology, Biology, Physics, 59, 293-299.
Perez.C, Michalski.J, Purdy.J, Wasserman.T, Williams.K and Lockett.M (2000) Three-
dimensional conformal therapy or standard irradiation in localized carcinoma of prostate: preliminary results of a nonrandomized comparison,International Journal of Radiation Oncology, Biology, Physics, 47, 629-637.
Pirzkall.A, Carol.M, Pickett.B, Xia.P, Roach.M and Verhey.L (2002) The effect of
beam energy and number of fields on photon-based IMRT for deep-seated targets,International Journal of Radiation Oncology, Biology, Physics, 53, 434-442.
Plopper.C, Cernea.C, Ferraz.A, Santos.L, D. and Regis.A (2004) Parotidectomy for
primary nonparotid diseases,Otolaryngology - Head and Neck Surgery, 131, 407-412.
Pohar.S, Gay.H, Rosenbaum.P, Klish.D, Bogart.J, Sagerman.R, Hsu.J and Kellman.R
(2005) Malignant parotid tumors: Presentation, clinical/pathologic prognostic factors, and treatment outcomes,International Journal of Radiation Oncology, Biology, Physics, 61, 112-118.
Pugachev.A, Boyer.A and Xing.L (2000) Beam Orientation Optimization in Intensity-
Modulated Radiation Treatment Planning,Medical Physics, 27, 1238-1245. Purdy.J (2004) Current ICRU definitions of volumes: limitations and future
directions,Seminars In Radiation Oncology, 14, 27-40. RBWH (Ed.) (2003) Royal Brisbane and Women's Hospial Division of Oncology-
Outcome Data Statistics 1998-2000, Queensland Government, Queenlsand, Australia.
RBWH (2005) Communication Administration System, RBWH, Brisbane, Australia. Roques.T, Dagless.M and Tomes.J (2005) Randomized trial on two types of
thermoplastic masks for patient immobilization during radiation therapy for head-and-neck cancer: In regard to Sharp et al. (Int J Radiat Oncol Biol Phys 2005;61:250-256),International Journal Of Radiation Oncology, Biology, Physics, 62, 942; author reply 943.

112
Rowbottom.C, Nutting.C and Webb.S (2001) Beam-orientation optimization of intensity-modulated radiotherapy: clinical application to parotid gland tumours,Radiotherapy and Oncology, 59, 169-177.
Saw.C, Zhen.W, Ayyangar.K and Enke.C (2002) Clinical aspects of IMRT--part
III,Medical Dosimetry: Official Journal of the American Association of Medical Dosimetrists, 27, 75-77.
Schot.L, Hilgers.F, Keus.R, Schouwenburg.P and Dreschler.W (1992) Late effiects of
radiotherapy on hearing,Eur Arch Otorhinolaryngol, 249, 305-308. Snell.R (2004) Clinical Anatomy Seventh Edition, Lippincott Williams & Wilkins,
Philadelphia, USA. Sohn.J, Suh.J and Pohar.S (1995) A method for delivering accurate and uniform
radiation dosages to the head and neck with asymmetric collimators and a single isocenter,International Journal of Radiation Oncology, Biology, Physics, 32, 809-813.
Standring.S, Ellis.H, Healy.J, Johnson.D and Williams.A (2005) Gray's Anatomy-The Anatomical Basis Of Clinical Practice-39th Edition, Elsevier Churchill Livingstone, Philadelphia, USA.
Steen.R, Koury.B, Granja.C, Xiong.X, Wu.S, Glass.J, Mulhern.R, Kun.L and
Merchant.T (2001) Effect of ionizing radiation on the human brain: White matter and gray matter T1 in pediatric brain tumor patients treated with conformal radiation therapy,International Journal of Radiation Oncology, Biology, Physics, 49, 79-91.
Stone.H, Coleman.C, Anscher.M and McBride.W (2003) Effects of radiation on
normal tissue: consequences and mechanisms,The Lancet Oncology, 4, 529-536. Sun.C, Cheng.C, Shimm.D and Cassady.R (1998) Dose Profiles in the Region of
Abutting Photon and Electron Fields in the Irradiation of Head and Neck Tumors,Medical Dosimetry, 23, 5-10.
Thibodeau.G and Patton.K (2003) Anatomy and Physiology-5th Edition, Mosby,
Missouri, USA. Tortora.G and Reynolds-Grabowski.S (2000) Principles of Human Anatomy and
Physiology-9th Edition, John Wiley and Sons Inc, New York, USA. Verhey.L (1999) Comparison of three-dimensional conformal radiation therapy and
intensity-modulated radiation therapy systems,Seminars in Radiation Oncology, 9, 78-98.

113
Wahlberg.P, Anderson.H, Biorklund.A, Moller.T and Perfekt.R (2002) Carcinoma of the parotid and submandibular glands--a study of survival in 2465 patients,Oral Oncology, 38, 706-713.
Wang.X, Zhang.X, Dong.L, Liu.H and Wu.Q (2004) Development of methods for
beam angle optimization for IMRT using an accelerated exhaustive search strategy,International Journal of Radiation Oncology, Biology, Physics, 60, 1325-1337.
Washington.C and Leaver.D (2004) Principles and Practice of Radiation Therapy-
Second Edition, Mosby, Philadelphia, USA. Weltens.C, Kesteloot.K, Vandevelde.G and Bogaert.W, V. d. (1995) Comparison of
plastic and Orfit masks for patient head fixation during radiotherapy: precision and costs,International Journal Of Radiation Oncology, Biology, Physics, 33, 499-507.
Yaparpalvi.R, Fontenla.D, Tyerech.S, Boselli.L. and Beitler.J (1998) Parotid gland
tumors: a comparison of postoperative radiotherapy techniques using three dimensional (3D) dose distributions and dose-volume histograms (DVHS),International Journal of Radiation Oncology, Biology, Physics, 40, 43-49.
Yi.W, Smith.D and Constine.L (2004) Optic nerve and chiasmatic tolerance to
radiotherapy,International Journal of Radiation Oncology, Biology, Physics, 60, S408.
Zbaren.P, Schupbach.J, Nuyens.M, Stauffer.E, Greiner.R and Hausler.R (2003)
Carcinoma of the parotid gland,The American Journal of Surgery, 186, 57-62. Zhu.L, Kron.T, Barnes.K, Johansen.S and O'Brien.P (1998) Junctioning of Lateral and
Anterior Fields in Head and Neck Cancer: A Dosimetric Assessment of the Monoisocentric Technique (Including Reproducibility),International Journal of Radiation Oncology, Biology, Physics, 41, 227-232.

114
Appendix A Documentation from Nucletron Pty Ltd confirming free software supply for a period of 90 days

115
Appendix B Ethics approval confirmation from Professor W Egerton of the RBWH Human Ethics Research Committee

116
Appendix C QUT email confirming ethical issues were uncompromised