Embed Size (px)
Citation preview

217
American Journal of Clinical Hypnosis Copyright ©2008 by the American Society of Clinical Hypnosis50:3, January 2008
Address correspondences and reprint requests to:Dr. C. Alexander Simpkins727 Salem CourtSan Diego, CA 92109E-mail: [email protected]
An exploratory outcome comparison between an Ericksonianapproach to therapy and brief dynamic therapy
C. Alexander Simpkins and Annellen M. SimpkinsSan Diego, California
Abstract
The purpose of this study was to determine whether an Ericksonian approachto therapy using hypnosis (ET) was as effective as brief dynamic therapy(BDT), a long-standing and well-researched form of psychotherapy. Thestudy used a comparative pretest/posttest design with four paper andpencil tests [Clark Personal and Social Adjustment Scale (CPSAS),Hopkins Symptom Checklist (HSCL), Target Complaint (TC), andGlobal Improvement (GI)] and six therapy sessions. The investigatorsattempted to choose design features that would not interfere with theunique qualities of ET while maintaining empirical regularity. No statisticallysignificant difference was found except on HSCL where ET was superior.An interesting finding was that without direct discussion of the targetcomplaint, ET brought about the same improvement on targeted problemsas BDT. ET subjects reported gaining understanding of their problems asmuch as BDT subjects, but from a different source. The results of thisstudy are a step toward empirical confirmation of ET as an evidence-basedtreatment alternative for psychotherapy.
Keywords: Clinical hypnosis, therapeutic effectiveness, efficacy inhypnosis, non-specific factors, utilization, unconscious, indirectsuggestion.
Milton Erickson has had a profound effect on the field of hypnosis andpsychotherapy. A large body of anecdotal literature now exists describing hissuccessful treatments (Zeig, 2006b, 2003, 1983; Erickson & Rossi, 2006, 2006a, 2006b;Haley, 1985 a, b, c, 1973; Erickson & Keeney, 2006; Short, Erickson & Erickson, 2005;Battino, 2005; Lankton, 2004; Simpkins & Simpkins, 2004, 2001a, 2000; Yapko, 2003,2001; Haley & Haley, 2003), to name just a few. With more than 120 Erickson Institutes(www.ericksonfoundation.org) treating clients and two-thirds of them in countries outsideof the United States, Ericksonian theory and methods are being used worldwide.
Untitled-17 12/14/2007, 8:54 AM217

218
Ericksonian approach to therapy and brief dynamic therapy comparison
Literature Pro and ConNot everyone agreed with Erickson during his lifetime or over the decades following
his death. For example, Hilgard held a well-researched, but different view on susceptibility(Hilgard, 1967). Social role-playing and sociocognitive theories reinterpreted the notions ofthe hypnotic state or an unconscious mind (Sarbin & Coe, 1972; Barber 2000; Kirsch &Lynn, 1995, Lynn & Sherman, 2000). Interest in Erickson’s work has also generated criticswho questioned Erickson’s claims (Mathews & Edgette, 1997). Thoughtful rebuttals anduseful interpretations such as from Lankton, (Mathews & Edgette, 1997, Lankton & Lankton,1983) and Gilligan (Mathews & Edgette, 1997; Gilligan, 1987) answered some of theseobjections and proposed useful modifications for integrating Erickson’s ideas into modernpractice.
Even though Kuhn (1962) believed the real work of science begins when a communityof scientists adopts a paradigm, Lynn and Rhue (1991) point out that the field of hypnosiscontinues to remain divided about which paradigm is best. But regardless of disagreementsand division, a growing and respected body of research shows that clinical hypnosis iseffective for varying problems (Lynn & Kirsch, 2006), and there is a general trend towardvalidation of hypnotherapy (Alladin, Sabatini, & Amundson 2007).
In Popper’s influential interpretation of science (Popper, 1959), scientific progressresults from a combination of innovative, creative theories and careful research. MiltonErickson was a creative innovator who left a legacy for psychotherapy. His method fortherapy using hypnosis is certainly worthy of careful research.
PurposeThis study was intended as an exploratory step to test the efficacy of an Ericksonian
approach to therapy using hypnosis (ET) as a primary treatment method for short-termpsychotherapy. The investigators attempted to create a research design that would adhereto as rigorous empirical standards as possible without interfering with the individualistic,nonstandard methods used by Erickson.
Brief dynamic therapy (BDT) was compared to ET in order to have a distinctivecontrast. Also, BDT has been validated as a possibly efficacious therapy (Chambless et. al.,1998). Comparing a new therapy with a possibly efficacious or efficacious treatment is oneof the design methods suggested by APA for efficacy studies (Chambless et. al, 1998).
Definitions
Psychotherapy EffectivenessThe effectiveness of psychotherapy is defined as the change in four dimensions: social/
environmental, internal/experiential, target problem, and global improvement. Four instrumentswere used to measure this change: Clark Personal and Social Adjustment Scale (CPSAS),Hopkins Symptom Checklist (HSCL), Global Improvement (GI), and Target Complaint (TC).
Ericksonian Therapy (ET)ET is defined as a form of psychotherapy using hypnosis and originated by Milton
Erickson. As used here, ET refers to the five-stage paradigm of the dynamics of tranceinduction and suggestion introduced by Rossi in 1976 consisting of 1) fixation of attention,2) depotentiating habitual frameworks and belief systems, 3) unconscious search, 4)unconscious processes, 5) hypnotic response (Erickson & Rossi, 1979; Erickson & Rossi
Untitled-17 12/14/2007, 8:54 AM218

219
Simpkins, Simpkins
2006b). This 5-stage paradigm includes less traditional methods of problem solving exemplifiedin the published works of Milton Erickson (Erickson & Rossi, 2006). More specifically, ET istypified by the use of utilization technique (Erickson and Rossi, 2006a, 2006b; Zeig, 2006a;Short, Erickson, & Erickson-Klein, 2005; Erickson 1965, 1959), therapeutic binds (Erickson &Rossi, 1975), indirect suggestion (Erickson & Rossi, 1976), confusion technique (Erickson,1964), therapeutic stories (Erickson & Keeney, 2006, Rosen, 1982), naturalistic induction(Erickson, 1958b), and especially, the use of many of these techniques in combination. ETdoes not rely on conscious insight.
Brief Dynamic Therapy (BDT)BDT is defined as an eclectic approach to therapy that guides clients toward greater
awareness and understanding of their problems and the resistances to resolving them. For thepurposes of this study, BDT did not use hypnosis. This method relies on conscious insight(Wolberg, 1977, 1964, 1948; Whitehorn, 1947, 1944; Bellak & Small, 1965), meaning a clear, rationalunderstanding of the cause of the target complaint from dynamics, motivations, behaviors,attitudes, and beliefs. Then a working-through phase followed, with corresponding experience ofthe emotional significance (Wolberg, 1977). Support for appropriate mature restraint, both cognitiveand behavioral, was given during this phase. The last stage focused on intervention, both verbaland action-oriented, and expansion of client potentials to resolve the target complaint.
UnconsciousThe unconscious is the storehouse of learning (Erickson & Rossi, 2006 Vol. I, 1).
Erickson believed that unconscious functioning is naturally healthy, filled with potential andpositive intelligence (Simpkins & Simpkins, 2001b). The foundation of better functioning shouldbe the naturally healthy unconscious. Therefore, encouraging conscious awareness wouldnot enhance therapeutic progress, but instead, would lead away from the source of healthyfunctioning. Hypnosis returns clients to the source of their healthy capacities. From there,people can unlearn their learned limitations and then discover and develop better possibilities.
For BDT, the unconscious is defined as a storehouse of repressions and negativeinstinctual impulses that cause the problematic symptoms. For BDT, the foundation ofhealthy functioning is through establishing conscious mental functioning. The role ofpsychotherapy in BDT is to bring the key elements of symptom-causing unconsciousprocesses to consciousness. Then new insights can be learned from them, like the “aha”experience one may have of a pattern in an ambiguous gestalt formation. (Bellak and Small1965, 32) The experience of insight permits problem solving with better cognitive integrationand understanding.
ConsciousConscious refers to deliberate attention to outward or inward events, experiences,
thoughts, beliefs, behaviors and feelings involving the use of awareness with cognitive processes.
UtilizationUtilization is where the therapist goes along with the dominant presenting behavior,
response, or interest as a means of holding the client’s attention, improving rapport, andenhancing the client’s feeling of being understood, as well as encouraging the resolution ofthe client’s difficulties (Erickson 1959). Personal memories and sensations of the client arethe best starting place. By turning attention inwards using hypnosis, people find a wealth of
Untitled-17 12/14/2007, 8:54 AM219

220
Ericksonian approach to therapy and brief dynamic therapy comparison
experiences to draw on. The approach of utilizing personal experiences has evolved into amethod to facilitate psychotherapy more generally: the Utilization Method. (Zeig, 2006a).
Suggestion, Indirect Suggestion, and IndirectionThis study used Erickson’s definition of suggestion based in the natural tendency
of suggestibility: the ability of the mind to respond to an idea. The unconscious mindresponds best when suggestions are open-ended, leaving room for the unconscious torespond in its own way and time. This automatic level of functioning can be engaged andused in psychotherapy to help accomplish goals that might be difficult to do consciously.Erickson developed a complex lexicon and syntax of indirect suggestions to communicatewith the unconscious (Erickson & Rossi, 2006b).
Erickson’s Creative Research MethodsMilton Erickson had strong opinions about how his method should be researched,
which he discussed with the investigators on many occasions (1976-1980). One commonassumption in laboratory research is that if all factors are kept equal, identical conditionsshould yield identical results. However, due to the unique and individualistic way peoplerespond to hypnosis, Erickson believed that identical inductions might not necessarily yieldidentical trances. “An awareness of the variability of human behavior and the need to meetit should be the basis of all hypnotic technique.” (Erickson, 1958a, 71) This insight waspivotal for researching hypnosis.
Erickson felt that restricting and isolating variables in the laboratory risks creating anartificial situation that does not reflect the complexity of the actual phenomena of hypnosis. Withthis recognition, if research is to yield useful data, it should make room for variability in humanbehavior by individualizing the therapeutic experience. According to Erickson, neither researchersnor therapists should impose their will, but instead should just set the stage for subjects to beable to respond as they would naturally. Erickson found: “The simpler and more permissive andunobtrusive the technique is, the more effective it has proved to be, both experimentally andtherapeutically, in the achievement of significant results” (Erickson, 2006, Vol. I, 15).
Erickson addressed these problems by doing his own research naturalistically(Erickson, 1958b; Simpkins, 2003). The naturalistic approach allowed him to observephenomena in the midst of their interrelationships without intruding artificially. Theuniqueness of the individual and his or her situation was not subtracted from the experimentso it could be studied. He observed many subjects under similarly flexible conditions to helphim formulate generalized conclusions that would influence his therapeutic work in years tocome. His approach informed this study.
Problem StatementThe question this study asked was whether ET is as effective as, or more effective
than, BDT in terms of treatment outcomes on the following measures: Clark Personal andSocial Adjustment Scale (CPSAS), Hopkins Symptom Checklist (HSCL), Global Improvement(GI), and Target Complaint (TC).
HypothesisH
0: µ
ET - µ
BDT < 0. ET will be less effective than BDT on the measures used.
H1: µ
ET - µ
BDT > 0. ET will be at least as effective as, or more effective than BDT on the
measures used.
Untitled-17 12/14/2007, 8:54 AM220

221
Simpkins, Simpkins
Experimental DesignThe study used a comparative pretest/posttest design employing two groups,
Group I, ET, and Group II, BDT. Each participant received a preliminary one-hour interview,two pretests, six 1-hour weekly treatment sessions, four posttests and one final debriefinginterview. A BDT Checklist and an ET Checklist served as general guidelines to direct theclient’s therapeutic processes as well as to standardize the treatments used by theinvestigators.
ParticipantsInvestigators made a deliberate effort to solicit a random sampling of subjects.
Participants (n = 27) were chosen at random using a pseudo-random number generator froma pool of people who answered signs posted in public areas. Signs were placed in a widevariety of settings (universities, grocery stores, the YMCA, health food stores, and businesses)on notice areas in upper, middle, and lower income communities throughout San Diego toattract as wide a range of subjects as possible. The research offered low-cost, ($60 for 6sessions and two interviews) short-term treatment.
Participants were between the ages of 21 and 65 years, 13 men and 14 women witha median age of 38. They came from a broad range of lifestyles, communities, socioeconomicstatus, and races. Occupations included homemakers, students, unemployed, laborers,business executives, secretaries, professionals, nurses, and artists.
None of the participants had any prior experience with psychotherapy or hypnosis.No specific class of problems was petitioned, but each participant was asked to choose someproblem or difficulty to focus on as the target complaint. Problems included: interpersonaldifficulties, life goals that included job and direction, stress, anxiety, uncomfortable body,difficulty concentrating, lack of motivation, creative blocks, insecurity, low confidence, andpoor self control in weight and smoking.
TherapistsThe therapist/investigators had equal experience and training in both ET and BDT.
Their training in ET came from direct personal studies with Milton Erickson and Ernest Rossi.Rossi was consulted during this study to ensure authenticity of the paradigm used. Theinvestigators also trained in hypnosis under G. Wilson Shaffer at Johns Hopkins Universityand Harold Greenwald at U.S.I.U. Their training in BDT came from a number of variedsources. They did personal studies with John C. Whitehorn and Jerome D. Frank along withan internship at Johns Hopkins University Phipps Clinic. They also trained with LawrenceKubie and did an internship at Sheppard Pratt Hospital under Kubie. They receivedsupervision under James Spivack of Towson State University in BDT with outpatientpopulations as well.
MeasuresFour measures were used: CPSAS, HSCL, TC and GI. This study chose these four
measures because they covered four different dimensions: social/environmental, internal/experiential, target problem, and global improvement. All four measures are well researchedand have been used by the Johns Hopkins Hospital Phipps researchers who had conductedcomparative studies of different methods of therapy over a 25-year period. These fourmeasures used in combination could also reveal comparative data about possibledifferences between treatments.
Untitled-17 12/14/2007, 8:54 AM221

222
Ericksonian approach to therapy and brief dynamic therapy comparison
The CPSAS (Clark, 1968) is a self-report instrument composed of 14 multiple-choice itemsabout work, family, self, and interpersonal relationships. The CPSAS was designed to assess clients’evaluations of general feelings about life, job, and interpersonal relationships in common senseterms, to show adjustment or lack of it in the client’s systems of interaction. The assumptions behindthe test include the expectancy that harmony with the often contradictory demands and needs ofones social network is important (Clark, 1968). The test score total is found by adding the scores foreach of the 14 items. When the score goes up between pre- and posttest, improvement is indicated.
The CPSAS measure correlated relatively high (r = .77) with the Social IneffectivenessScale validated by (Gurland et al. 1972). The test has continued to be used in therapeutic effectivenessstudies (Rosenberg, NK, Hougaard, E., 2005). Reliability was .70 over a 6 week period for psychoticinpatients at Bayview House Psychiatric Hospital and validity scores of patient samples (M = 4.39)compared to normal students (M = 7.88). The adjustment measure correlates 0.56 with the 100-itemtrue-false self-report Cornell Index that measures adjustment (p <. 01, df = 42) (Clark 1968).
The HSCL (Derogatis et. al., 1974) is a self-report instrument that asks clients to ratea wide variety of somatic and psychic complaints such as subjective experiences ofuncomfortable thoughts, body sensations, emotions, and lack of confidence. The itemsdescribe typical symptoms people often get when they are suffering from fears, anxiety, andconflicts. The test consists of 58 multiple-choice items. The rating is from “least distressed”to “most distressed” over the previous week. Scores for each item are added together for thetotal. When the sum of the scores on the items goes down, improvement is indicated.
The HSCL was tested with 2500 subjects: 1800 outpatients at 3 psychiatric hospitalsand 700 normals. Reliability coefficients in test-retest were 0.75. Internal consistency coefficientswere 0.80-0.87. Construct validity was tested in several tests and the degree of separationbetween mean distress levels of normal samples and the two outpatient samples (n = 2000)provided substantial measure of construct validity (Derogatis et al., 1974).
The GI (Frank, Hoehn-Saric, and Gurland, 1968) is a self-report measure that asksclients to rate their degree of change or improvement in general from “worse” to “a lotbetter” since therapy began. The GI is a posttest or follow-up test only. This test helped tobalance the CPSAS and HSCL by giving clients the opportunity to evaluate their generalfunctioning as contrasted to the detailed complaints described in the CPSAS and HSCL.This test has been used in numerous research projects and has been judged by experiencedpractitioners to possess adequate face validity (Fink, Hoehn-Saric, and Gurland, 1968;Frank et al., 1974).
The TC (Battle et al., 1966) is another posttest and follow-up measure. The TCallows clients to directly describe and rate their problem specific to the therapeutic goals.The TC met the needs of this investigation in providing a measure that focused on onlyone problem as the therapeutic goal. Validity on the TC was found by comparing it to theGI, the Social Ineffectiveness Scale, and the Discomfort Scale (Battle et al., 1966). Reliabilitywas tested by measuring the stability of clients’ perceptions of their main problems beforeand after treatment. Therapists’ ratings were also compared with each other and withclient ratings. From these studies, Battle determined that target complaints could beobtained reliably from the patient (Battle et al, 1966).
Interview ProceduresIn the initial interview, all clients were asked general history and background
questions from an Interview Checklist. The questions covered three main groups of data:general information, personal information, and the background and nature of the target
Untitled-17 12/14/2007, 8:54 AM222

223
Simpkins, Simpkins
problem. Following the interview, participants were given a general description of the twotreatment modalities. The theoretical premise of each method was stated briefly, and thensubjects were assigned to one of the two groups by mutual consent. A cooperative approachto the treatment situation was encouraged just as in a typical psychotherapy initial interview.(See Discussion)
The two pretests were administered. Participants were told that any questionsabout the tests or the study would be answered in the final debriefing interview.
Therapeutic ProceduresTherapy was conducted in a team manner with an unrestricted give and take flow
from both investigator/therapists with the participant/clients. Both investigators recordedon separate copies of the checklists, thus ensuring objectivity.
Procedures for ETThe target complaint that was to be the focus of therapy was determined at the time
of the interview, but was not discussed directly during the sessions. Each session beganwith a 10 minute general discussion of whatever was of interest to the client. This allowedtime to focus the client’s attention on his or her own concerns. Without specifically referringto the central concerns, trance was induced using the orienting mode most natural to theclient. Incorporating utilization, contents for trance inductions were determined by theclient’s interests during the session. Trance techniques were chosen from the ET Checklist.Techniques systematically chosen from all five sections were used with every subject ineach session, to lead them into trance.
The ET Checklist had five parts: fixation of attention, depotentiating conscioussets, unconscious search, unconscious processes, and hypnotic response. Ideomotorsignaling was established to stay attuned to the client’s experiences. Clients related to thetherapeutic process through varied hypnotic phenomena such as changes in muscle tonus,inability to move, hand levitation, automatic writing and drawing, and speaking in trance.Indirect suggestions and stories guided clients into a broad range of hypnotic experiencesincluding sensory experiences, images, memories, and hallucinations.
Procedures for BDTTherapy began with a description of the problem area and proceeded through the
three stages from the BDT Checklist: uncovering, working through, and expanding potentials.The six sessions drew from all three stages of the checklist, but earlier sessions used the firstand second stage while middle and later sessions drew more from the second and third stages.
Stage one taught clients how to observe their thoughts, emotions, and sensations withoutjudgment. Clients were encouraged to bring out related feelings, memories, attitudes, and experiences.They were taught to recognize subtle body feelings, emotions, and peripheral thoughts.
Stage two concentrated on patterns of defense, attitudes, beliefs, and values. Asthese were discussed, clients were encouraged to feel as well as observe the underlyingemotions that were elicited. Special attention was given when values, beliefs, and attitudeswere in conflict with each other and with emotions. Personal meanings of experiences werediscussed as well.
Stage three emerged from the added insights and feeling-sense of the conflict thatclients uncovered in the earlier stages. Clients explored new perspectives and flexible use ofdefenses. By the time they had gone through the three stages, they expressed an
Untitled-17 12/14/2007, 8:54 AM223

224
Ericksonian approach to therapy and brief dynamic therapy comparison
understanding of where the problem came from, insight into the nature of the conflict withrecognition of the defenses involved, and ability to distinguish between their actual personalsituation and their distortions. The final session emphasized work on new potentials forchange with some practical ways to implement these changes into everyday life.
Posttest and Debriefing InterviewThe eighth meeting began with administration of posttests followed by a final
interview. Clients were asked to elaborate on change in the target complaint, general changes,and any tools or learning they felt they had acquired from treatment. After all therapeuticprocedures and research procedures were completed, clients were encouraged to ask anyquestions about the research. Candid disclosure of the project was then given.Data Analysis Methods
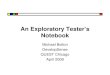
CPSAS and HSCL were calculated for means for pretest scores, posttest scores andpre/post difference scores. The student t test for significance was applied to all three sets ofdata at p < .05. The GI and TC, being posttests only, were calculated for the posttest scores,and the t test applied to these data. Distributions percents of scores for each test weregraphed and labeled for comparison to normal distributions (Figures 1-8).
Figure 1 Figure 2
Figure 3 Figure 4
Untitled-17 12/14/2007, 8:54 AM224

225
Simpkins, Simpkins
ResultsHypothesis
1
For three of the four measures, there was no significant difference at p < .05 betweenET and BDT. At p < .05, CPSAS t (27) = 1.99, TC t (27) = 0.36, and GI t (27) = 0.63. ET wassignificantly more effective than BDT on the HSCL t (27) = 4.11 at p <. 05. Therefore, the nullhypothesis was rejected.
Regarding power, 1-ß = 0.92 for CPSAS and TC strongly recommended rejecting thenull hypothesis. GI had weaker power (1-ß = 0.41). The power on the HSCL measure (1-ß =0.59) made it moderately likely that there was a significant difference between the two groups.
AssumptionThe assumption that all distributions would approach the normal curve was
supported for all of the curves except for the GI measure for BDT, which was skewed at thehigh end (Figures 1-8). Although there were differences between variances of some of thedistributions of the scores, this did not violate the assumption for the t test (Witte & Witte1980). “In practice t test gives pretty accurate results even when there are fairly largedifferences in the population variances” (Aron & Aron 2003, 356).
Figure 5 Figure 6
Figure 7 Figure 8
Untitled-17 12/14/2007, 8:54 AM225

226
Ericksonian approach to therapy and brief dynamic therapy comparison
DiscussionPsychotherapy has made progress in understanding therapeutic effectiveness and
the factors that influence it. Pioneers such as Jerome D. Frank and the Johns HopkinsUniversity Phipps Clinic psychotherapy research group (Frank, Hoehn-Saric, Imber, Liberman,& Stone, 1978) ushered in a new era for psychotherapy research. Their 25-year PsychotherapyResearch Project gave an early template for non-specific factors as ingredients of successfulpsychotherapy (Simpkins & Simpkins, 2002; Frank and Frank, 1991). Recent meta-analyses(Miller, Duncan, & Hubble, 1997, 1996) have continued to confirm what Frank and his teamfirst concluded: psychotherapy is effective, but there is no significant difference betweeneffectiveness of methods used to accomplish it. This research along with clinical experienceled the investigators to form their hypotheses.
Table 1: Pre/Post CPSAS Means, Standard Deviations, Effect Size
Group N Pre-treatment Post-treatmentMean SD Mean SD t d 1-ß
ET 16 38.87 7.39 43.06 5.76 1.99 .13 .92BDT 11 40.09 5.60 42.40 4.84
Table 2: Pre/Post HSCL Means, Standard Deviations, Effect Size
Group N Pre-treatment Post-treatmentMean SD Mean SD t d 1-ß
ET 16 32.37 7.39 17.34 9.31 4.11 .80 .59BDT 11 34.09 25.15 30.90 25.40
Table 3: Posttest TC Mean Scores, Standard Deviations
Group N Mean SD t d 1-ß
ET 16 4.18 .73 .31 .13 .92BDT 11 4.09 .67
Table 4: Posttest GI Mean Scores, Standard Deviations
Group N Mean SD t d 1-ß
ET 16 4.18 .73 1.90 1.12 .41BDT 11 4.81 .34
Untitled-17 12/14/2007, 8:54 AM226

227
Simpkins, Simpkins
Assignment of Treatment Method
The attempt to identify empirically supported therapies (ESTs) imposes particularassumptions on the use of randomized controlled trial (RCT) methodology thatappear to be valid for some disorders and treatments, but substantially violatedfor others (Weston, Novotny, & Thompson-Brenner 2004, 631).
What Weston, Novotny, & Thompson-Brenner advocate is “a thorough goingassessment of the empirical status of not only the data, but also the methods used to assignthe appellations empirically supported or unsupported (Weston, Novotny, & Thompson-Brenner 2004, 632). The current study attempted to be sensitive to possible design featuresthat could interfere with the special needs for testing ET, beginning with the assignment ofsubjects to treatment group.
In private practice, some clients strongly request hypnotherapy whereas others areadamantly against hypnosis and prefer a talking form of therapy. Some of the general,uninitiated public experience hypnosis through the filter of such concerns as losing control,religious issues, and invasion of privacy to name a few. Thus, when participants learn thathypnosis might be involved and that they could be randomly assigned to receive hypnosis,those who had a prior bias against hypnosis would be likely to either drop out or resist.Furthermore, if someone entered the study to receive hypnosis and was not given hypnosis,they might be disappointed and resistant. Although sophisticated hypnotic practitionersand researchers know that these concerns can be sensitively addressed, they are issues thatcould intrude upon the cooperation of a research subject. To best replicate the real-worldclinical situation and attempt to bypass these potentially intrusive factors, the investigatorsdecided to randomize before assigning treatment methods, and once admitted into the study,allow subjects to participate in choosing their treatment method.
Subjects in this study could enter into collaboration by taking part in selecting thetreatment method they preferred. “The ideal ‘scientist subject’ can be cultivated in bothclinical and experimental laboratory settings by forming an investigator-subject partnershipaimed at producing the most accurate data” (Barabasz & Barabasz 1992, 199). This study,therefore, was able to better maintain collaboration while at the same time creating a contextto examine the process of psychotherapy’s effective action. Allowing subjects to participatein selecting their treatment included the subjects’ natural inclination toward one method orthe other, to permit the positive effect of non-specific factors with both methods. A futurestudy could be done using random assignment of subjects to treatment as a means ofcomparison, to attempt to bypass the effect of each individual’s personal concerns. A muchlarger sample size or meta-analysis might correct for the potential randomization problem.
ET Results DiscussionThe statistics indicated that there were generally similar effects from the two
treatments but that there were some specific differences that were revealed by the measures.ET had a larger change and effect size on the HSCL, a test that addresses physiological andinternal discomforts. This finding supports some of the recent research that has foundhypnosis especially helpful for pain (Miller, & Bowers. 1986; Hilgard & Hilgard, 1975)headaches (Llaneza-Ramos, 1989), anxiety (Benson et al., 1978), obstetrics (Abramson &Heron, and 1950), general women’s discomforts (Hornyak & Joseph, 2000), stress (Bryant etal., 2005), and other problems that typically involve physical discomfort. Hypnosis clientsoften reported feeling more comfortable, less anxious, and less stressed, which is a typical
Untitled-17 12/14/2007, 8:54 AM227

228
Ericksonian approach to therapy and brief dynamic therapy comparison
byproduct of hypnosis. Therapists who do not use hypnosis as their primary treatmentmight want to add this skill to assist with these types of problems. Research supportshypnosis as an adjunct to cognitive behavioral therapy (Kirsch, Montgomery & Saperstein;1995; Allison & Faith, 1996).
The ET group never received any direct work on the target complaint, but theresults on the TC measure were very similar for both groups. This statistic shows supportfor Erickson’s idea that therapy is not just the specific result of the therapist intervention:change takes place within the client. This finding can encourage therapists to offer open-ended interventions that elicit personally meaningful responsiveness from clients andencourage inner processing instead of directing the client with overly specific or standardizedtechniques. As further support for this idea, Lynn, Green, Jaquith, & Gasior, (2003) found thatsubjects receiving lenient instructional sets far outperformed subjects who were givenstringent instructions when tested for suggestibility, subjective involvement, involuntariness,quickness of response, satisfaction, and imaginative ability.
Qualitative InformationThe closing interviews revealed some additional information. All participants were asked
to specify what they had learned from treatment. Everyone expressed satisfaction that they hadgained new tools for working with themselves, but the two groups reported receiving different skills.
ET participants felt that they could trust and use their unconscious mind as a tool.Often they experienced this as simply happening without quite knowing why. One participantsaid, “Things are just kind of happening; I’m not sure why, but I am more relaxed, and I cantrust my intuitive self.” Another said, “My unconscious has opened up more and it doesmore. This feels good.” The tools this group acquired tended to be an intuitive ability tosense their inner needs and a willingness to listen to their inner voice.
BDT participants felt that their awareness acted as a distinct guide to sense situations,notice reactions, and trace feelings and thoughts. “I’m looking at feelings as opposed to surfacethoughts. I can examine them since I am aware of them,” remarked one BDT participant. Anothersaid, “It’s the awareness: stopping, stepping back, away from being immersed in it all, to look atit from the outside. I’m noticing things more and making an effort to observe my surroundings.”
Many ET participants also expressed a new ability to be objective, like the insightparticipants. One ET client said, “It feels like something, a clouded something in me has helpedme stand back and look at things more objectively and be more relaxed instead of getting freakedout.” So, despite differences in treatment methods, participants seemed to develop a similarobjectivity. Though both groups felt they gained objectivity, each believed it came from a differentsource: BDT from a clear awareness, and ET from a supportive unconscious. Both groups feltthey gained greater understanding of themselves and their problems.
The research indicates that ET can be an effective method to bring aboutpsychotherapeutic change. Further research will disclose more. As Heraclites, the wise earlyGreek philosopher said, “Wisdom is one thing: to grasp the knowledge of how all things aresteered through all” (Barnes 2001, 53).
Untitled-17 12/14/2007, 8:54 AM228

229
Simpkins, Simpkins
References
Aaron, A., & Aron, E. (2003). Statistics for psychology. Upper Saddle River: New Jersey:Prentice Hall.
Abramson, M. & Heron, W. (1950). An objective evaluation of hypnosis in obstetrics:Preliminary report. American Journal of Obstetrics and Gynecology, 59, 1069-1074.
Alladin, A. Sabatini, L. & Amundson, J.K. (2007). What we ought to mean by empiricalvalidation in hypnotherapy: Evidence-based practice in clinical hypnosis.International Journal of Clinical and Experimental hypnosis, 55, 2.
Allison D. & Faith M. (1996). Hypnosis as an adjunct to cognitive-behavioral psychotherapyfor obesity: A meta-analytic reappraisal. Journal of Consulting & ClinicalPsychology, 64, 3, 513-516.
Barabasz, A. & Barabasz, M. (1992). Research designs and considerations. Contemporaryhypnosis research, In M. Nash, & E. Fromm, Eds. New York: Guilford Press.
Barber, T. (2000). A deeper understanding of hypnosis: Its secrets, its nature, its essence.American Journal of Clinical Hypnosis, 42: 3-4, 208-273.
Barnes, J. (2001). Early Greek philosophy. London: Penguin Books.Battino, R. & South, T. (2005). Ericksonian approaches: A comprehensive manual. Norwalk,
CT: Crown House Publishing Limited.Battino, R. & South, T. (2002). Metaphoria: Metaphor and guided metaphor for
psychotherapy and healing. Norwalk, CT: Crown House Publishing Limited.Battle, C., Imber, S., Hoehn-Saric, R., Stone, A., Nash, E., & Frank, J. (1966). Target complaints
as criteria of improvement. American Journal of Psychotherapy, 20, 184-192.Bellak, L. & Small, L. (1965). Emergency psychotherapy and brief psychotherapy. New York:
Grune & Stratton, Inc.Benson H., Frankel F., Apfel R. Daniels M., Schniewind H., Nemiah J., Sifneos P., Crassweller
K., Greenwood M., Kotch J., Arns P., & Rosner B. (1978). Treatment of anxiety: Acomparison of the usefulness of self-hypnosis and a meditational relaxationtechnique. An overview. Psychotherapy & Psychosomatics, 30, 3-4, 229-242.
Bryant, R., Moulds, M., Guthrie, R, & Nixon, R. (2005). The additive benefit of hypnosis andcognitive-behavioral therapy in treating acute stress disorder. Journal of Consultingand Clinical Psychology, 73, 2, 334-340.
Chambless, D. L. Baker, M. J., Baucom, D. H., Beutler, L. E., Calhoun, K. S., & Daiuto, A.(1998). Update on empirically validated therapies II. Clinical Psychologist, 51, 4.
Clark, A. (1968). The personality and social network adjustment scale. Human Relations, 21,85-96.
Derogatis, L., Lipman, R., Rickels, K., Uhlenhuth, E., & Covi, L. (1974). The Hopkins symptomchecklist (HSCL): A self-report symptom inventory. Behavioral Science, 19, 1-15.
Erickson, M. (1965). The use of symptoms as an integral part of hypnotherapy. AmericanJournal of Clinical Hypnosis. 8, 57-65.
Erickson, M. (1964). The confusion technique in hypnosis. American Journal of Clinicalhypnosis. 6, 183-207.
Erickson, M. (1959). Further techniques of hypnosis: Utilization techniques. AmericanJournal of Clinical Hypnosis, 2, 2-21.
Erickson, M. (1958a). Deep hypnosis and its induction. In L. Le Cron (Ed), Experimentalhypnosis (pp. 70-112). New York: Macmillan.
Untitled-17 12/14/2007, 8:54 AM229

230
Ericksonian approach to therapy and brief dynamic therapy comparison
Erickson, M. (1958b). Naturalistic techniques of hypnosis. American Journal of ClinicalHypnosis, 1, 3-8, 70-114.
Erickson, M. (1943). Hypnotic investigation of psychosomatic phenomena: Psychosomaticinterrelationships studied by experimental hypnosis. Psychosomatic Medicine, 5,51-58.
Erickson, M. & Rossi, E. (2006). The neuroscience editions: The complete works of MiltonH. Erickson M.D.: On hypnosis, psychotherapy, and rehabilitation CD Rom. In E.Rossi, R. Erickson-Klein & K.L. Rossi. (Eds.). Phoenix: Milton H. EricksonFoundation Press.
Erickson, M. & Rossi, E. (2006a). The neuroscience editions: Healing in hypnosis, reframingin hypnosis, mind-body communications in hypnosis & creative choice in hypnosisCD Rom. Phoenix, AZ: Milton H. Erickson Foundation Press.
Erickson, M. & Rossi, E. (2006b). The neuroscience editions: Hypnotic realities,hypnotherapy and experiencing hypnosis CD Rom. Phoenix, AZ: Milton H. EricksonFoundation Press.
Erickson, M. & Rossi, E. 1976. Two-level communication and the microdynamics of tranceand suggestion. American Journal of Clinical Hypnosis. 18, 153-171.
Erickson, M. & Rossi, E. 1975. Varieties of double binds. American Journal of ClinicalHypnosis, 17, 143-157.
Erickson, B. & Keeney, B. (2006). Milton H. Erickson, M.D.: An American healer. Sedona,Arizona, AZ: Ringing Rocks Press.
Frank, J. & Frank, J. (1991). Persuasion and healing: A comparative study of psychotherapy.Baltimore, MD: The Johns Hopkins University Press.
Frank, J. & Frank, J, Hoehn-Saric, R., Imber, S., Liberman, B., Stone, A. (1978). Effectiveingredients of successful psychotherapy. New York: Brunner/Mazel, Publishers.
Frank, J. & Frank, J. (1974). Therapeutic components of psychotherapy: A 25-year progressreport of research. Journal of Nervous and Mental Disorders, 159, 324-342.
Freud, S. (1965). Introductory lectures on psychoanalysis. New York: W. W. Norton, Inc.Gilligan, S. (1987). Therapeutic trances: The cooperation principle in Ericksonian
hypnotherapy. New York: Brunner/Mazel.Haley, J. & Richeport-Haley, M. (2003). The art of strategic therapy. New York: Brunner-Routledge.Haley, J. (1985). Conversations with Milton H. Erickson, M.D.: Volume I: Changing
individuals. New York: Triangle Press.Haley, J. (1985). Conversations with Milton H. Erickson, M.D.: Volume II: Changing couples.
New York: Triangle Press.Haley, J. (1985). Conversations with Milton H. Erickson, M.D.: Volume III: Changing
children and families. New York: Triangle Press.Haley, J. (1973). Uncommon therapy: The psychiatric techniques of Milton H. Erickson,
M.D. New York: W.W. Norton & Company, Inc.Hilgard, E. & Hilgard, J. (1975). Hypnosis in the relief of pain. Los Altos, CA: William Kaufman.Hilgard, E. & Hilgard, J. (1967). Individual differences in hypnotizability. In J. Gordon (Ed).
Handbook of clinical and experimental hypnosis. (391-443). New York: Macmillan.Hornyak, L. & Green, J. (2000). Healing from within: The use of hypnosis in women’s health
care. Washington D.C.: American Psychological Association.Kirsch, I. & Saperstein, G. (1995). Hypnosis as an adjunct to cognitive-behavioral
psychotherapy: A meta-analysis. Journal of Consulting and Clinical Psychology,63, 214-220.
Untitled-17 12/14/2007, 8:54 AM230

231
Simpkins, Simpkins
Kirsch, I. & Saperstein, G. & Lynn, S. (1995). The altered state of hypnosis: Changes in thetheoretical landscape. American Psychologist, 50, 846-58.
Lankton, S. (2004). Assembling Ericksonian therapy: The collected papers of StephenLankton, Volume I: 1985-2002. Phoenix, AZ: Zeig, Tucker & Theisen, Inc.
Lankton, S. & Lankton. (1983). The answer within: A clinical framework of Ericksonianhypnotherapy. New York: Brunner/Mazel.
Llaneza-Ramos, M. (1989). Hypnotherapy in the treatment of chronic headaches. PhilippineJournal of Psychology, 22, 17-25.
Lynn, S.J. & Rhue, J.W. (1991). Theories of hypnosis: Current models and perspectives. NewYork: The Guilford Press.
Lynn, S. & Sherman, S. (2000). The clinical importance of sociocognitive models of hypnosis:Response set theory and Milton Erickson’s strategic interventions. AmericanJournal of Clinical Hypnosis, 42: 3-4, 294-315.
Lynn, S. & Sherman, S. & Kirsch, I. (2006). Essentials of clinical hypnosis: An evidencebased approach. Washington, DC: American Psychological Association.
Kuhn, T. (1962). The structure of scientific revolutions. Chicago: University of Chicago Press.Mathews, W.J. & Edgette, J.H. (1997). Current thinking and research in brief therapy:
Solutions, strategies, narratives, Vol. I. New York: Brunner/Mazel, Publishers.Miller, S., Duncan, B. & Hubble, M. (1997). Escape from Babel: Toward a unifying language
for psychotherapy practice. New York: W.W. Norton & Company, Inc.Miller, S., Duncan, B. & Hubble, M. (1996). Handbook of solution-focused brief therapy. New
York: Jossey-Bass, Inc.Melis, P., Rooimans, W., Spierings, E., & Hoogduin, C. (1991). Treatment of chronic tension-
type headache with hypnotherapy: A single-blind time controlled study. Headache,31, 10, 686-689.
Miller, M. & Bowers, K. (1986). Hypnotic analgesia and stress inoculation in the reduction ofpain. Journal of Abnormal Psychology, 95,1, 6-14.
Popper, K. (1959). The logic of scientific discovery. New York: Basic Books.Raz, A. & Shapiro, T. (2002). Hypnosis & neuroscience: A crosstalk between clinical and
cognitive research. Archives of General Psychiatry, 59, 85-90.Rainvillea, P. Hofbauerb, R., Tomá Pausb R., Duncana, G., Bushnella, M., & Pricec, D. (1999).
Cerebral mechanisms of hypnotic induction and suggestion, Journal of CognitiveNeuroscience, 11, 110-125.
Rossi, E. (2002). The psychobiology of gene expression: Neuroscience and neurogenesis inhypnosis and the healing arts. New York: W.W. Norton & Company.
Rossi, E. (1993). The psychobiology of mind-body healing: New concepts of therapeutichypnosis. New York: W.W. Norton & Company.
Rossi, E. & Cheek, D. (1988). Mind-body therapy: Methods of ideodynamic healing inhypnosis. New York: W.W. Norton & Company.
Sarbin, T. & Coe, W. (1972). Hypnosis: A social psychological analysis of influencecommunication. New York: Holt, Rinehart and Winston, Inc.
Short, D., Erickson, B., & Erickson-Klein, R. (2005). Hope and resliliency: Understandingthe psychotherapeutic strategies of Milton H. Erickson, M.D. Norwalk, CT: CrownHouse Publishing Company Limited.
Simpkins, C. & Simpkins, A. (2005). Effective self hypnosis: Pathways to the unconsciouswith Audio CD. San Diego, CA: Radiant Dolphin Press.
Untitled-17 12/14/2007, 8:54 AM231

232
Ericksonian approach to therapy and brief dynamic therapy comparison
Simpkins, C. & Simpkins, A. (2004). Self-hypnosis for women with audio CD. San Diego, CA:Radiant Dolphin Press.
Simpkins, C. & Simpkins, A. (2003). Milton H. Erickson’s naturalistic approach: An importantcontribution to experimental methodology, Milton H. Erickson FoundationNewsletter, 23:2, 10-11.
Simpkins, C. & Simpkins, A. (2002). Research brief on brief therapy. Milton H. EricksonFoundation Newsletter, 22:3, 12-13.
Simpkins, C. & Simpkins, A. (2001a). Timeless teachings from the therapy masters. SanDiego, CA: Radiant Dolphin Press.
Simpkins, C. & Simpkins, A. (2001b). Your unconscious is a lot smarter than you are: Researchon hypnosis and the brain. Milton H. Erickson Foundation Newsletter, 21:3, 14.
Simpkins, C. & Simpkins, A. (2001c). Self-hypnosis plain and simple. Boston: TuttlePublishing.
Weston, D, Novotny, C.M., & Thompson-Brenner, H. (2004). The empirical status ofempirically supported psychotherapies: Assumptions, findings, and reporting incontrolled clinical trials. Psychological Bulletin, 130: 4, 631-663.
Whitehorn, J. (1944). The concept of meaning and cause in psychodynamics. AmericanJournal of Psychiatry, 104, 289-296.
Whitehorn, J. (1956). Stress and emotional health. American Journal of Psychiatry, 112, 10-18.Whitehorn, J. (1947). The person, the situation, and the reaction: Psychotherapeutic strategy.
Acta Medical Scaninavia Supp., 196, 626-33.Witte, R. & Witte, J. (1997). Statistics. Fort Worth, TX: Harcourt Brace College Publishers.Wolberg, L. (1948). Medical hypnosis, Vol. 1 & II. New York: Grune & Stratton.Wolberg, L. (1964). Hypnoanalysis. New York: Grune & Stratton.Wolberg, L. (1977). Techniques of psychotherapy. Vol. I & II. New York: Grune & Stratton.Yapko, M. (2003). Trancework: An introduction to the practice of clinical hypnosis, 3rd ed.
New York: Brunner Routledge.Yapko, M. (2001). Treating depression with hypnosis: Integrating cognitive-behavioral
and strategic approaches. New York: Brunner Routledge.Zeig, J. (2006a). Confluence: The selected papers of Jeffrey K. Zeig. Vol. I. Phoenix, AZ:
Zeig, Tucker, Theisen, Inc.Zeig, J. (2006b). Advanced techniques of hypnosis and therapy: Milton H. Erickson therapy
within a marital system (1978) DVD. Phoenix, AZ: Milton H. Erickson FoundationPress.
Zeig, J. (2003). Advanced techniques of hypnosis and therapy: Milton H. Erickson M.D.working with resistance (1979) DVD. Phoenix: Milton H. Erickson Foundation Press.
Zeig, J. (2002). Brief therapy: Lasting impressions. Phoenix: Milton H. Erickson Foundation Press.Zeig, J. (1983). Symbolic hypnotherapy: Hypnotherapy session conducted by Milton H.
Erickson, M.D.: Lecture and discussion by Jeffrey K. Zeig, Ph.D. Phoenix, AZ:Milton H. Erickson Foundation Press.
Zeig, J. & Geary, B. (2001). The handbook of Ericksonian psychotherapy. Phoenix, AZ: TheMilton H. Erickson Foundation Press.
Untitled-17 12/14/2007, 8:54 AM232


![An Exploratory Assessment of Situational Effects in · PDF fileAn Exploratory Assessment of ... been sounded in marketing studies of personality [9], attitudes [18], brand ... AN EXPLORATORY](https://img.pdfslide.us/doc/110x75/5a87d5537f8b9a001c8e19c6/an-exploratory-assessment-of-situational-effects-in-exploratory-assessment-of.jpg)