Embed Size (px)
Citation preview

4k14 0031 Mp 45 Thursday Dec 04 08:24 AM SV-CVIR (v. 20, #6) 0031 (0254)
Cardiovasc Intervent Radiol (1998) 21:45–49
CardioVascularand InterventionalRadiologyq Springer-Verlag New York Inc. 1998
Laboratory Investigations
An Experimental Study of Endovascular Stenting with SpecialReference to the Effects on the Aortic Vasa Vasorum
Jun-Ichiro Sanada, Osamu Matsui, Jun Yoshikawa, Toshihiko MatsuokaDepartment of Radiology, Kanazawa University School of Medicine, 13-1 Takara-machi, Kanazawa 920, Japan
Table 1. Types of stents and periods after stent placement
Dog no. Types of stents Weeks after stentplacement
1 BS, PU-CS 42 BS, PU-CS 43 BS, PU-CS 84 BS, PU-CS 125 PU-CS 126 BS, PU-CS 207 BS, PU-CS 258 BS, PU-CS 409 BS, PU-CS 45
BS Å bare stent; PU-CS Å polyurethane covered stent
AbstractPurpose: To evaluate the effects of bare stents andcovered stents on the aortic wall, especially the vasavasorum.Methods: Eight bare stents and nine covered stentswere placed in the infrarenal aorta of nine dogs. Thedogs were euthanized at 4 – 45 weeks after stentplacement. The vasa vasorum was evaluated by mi-crostereoscopy with vascular casting, and the his-topathology of the aortic wall was examined by lightmicroscopy.Results: In the unstented normal aorta, vasa vaso-rum nourished the adventitia and the outer media,and the intima and inner media were avascular. Inthe stented segment, vascular dilatation and prolif-eration of vasa vasorum, medial atrophy, and inti-mal hyperplasia were observed, more prominent forcovered stents than for bare stents.Conclusion: Intravascular stent placement causednot only medial atrophy and intimal hyperplasia butalso proliferation of the vasa vasorum, probably dueto hypoxia in the aortic wall.
Keywords:Aorta—Arteries—Graftsandprostheses—Grafts, interventional procedure—Stents and prosthe-ses—Vasa Vasorum
In the normal aorta, the adventitia and outer third ofthe media are nourished through the vasa vasorum,and the intima and inner third of the media are avas-cular and are oxygenated by direct diffusion fromthe intraluminal blood flow. The middle third of themedia is variably supplied by both sources [1]. It isreported that disturbances of the microcirculation inthe arterial wall cause stagnation of interstitial flu-ids, hypoxia, disturbance of nutrition, decreased
Correspondence to: J. Sanada, M.D.
metabolic activity, and increased permeability in thearterial wall. Under these circumstances intimal hy-perplasia or degeneration of the medial layer mayprogress [2]. To evaluate the effects of endovascularstenting on the blood supply to the arterial wall, itis essential to identify not only histopathologicalchanges but also morphological changes in the vasavasorum.
The purpose of this study was to evaluate the his-topathological changes of the aortic wall and the alter-ations of the architecture of the vasa vasorum followingbare metallic stent and covered stent placement in acanine abdominal aorta.
Materials and Methods
Nine dogs weighing 8–13.5 kg (average weight, 9.3 kg) were usedfor this study. The animals were anesthetized with intramuscularketamin hydrochloride (50 mg/kg). The femoral artery was per-cutaneously punctured and a 7 Fr sheath (25 cm in length, Me-dikit, Tokyo, Japan) was introduced into the infrarenal aorta. Theluminal diameter of the abdominal aorta was measured on angi-ography (after correction for magnification) which was performedjust before stent placement. The average diameter of the stentedsegments was 9 mm. A stent was advanced through the sheathwith a stent pusher. When the stent reached the target position,holding the stent pusher, the sheath was withdrawn and the stent

4k14 0031 Mp 46 Thursday Dec 04 08:24 AM SV-CVIR (v. 20, #6) 0031 (0254)
J. Sanada et al.: Effects of Endovascular Stenting on the Aortic Vasa Vasorum46
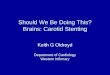
Fig. 1. Photomicrograph of a cross-section of the abdominal aortaobtained 40 weeks after the bare-stent placement. Moderate intimalhyperplasia made up of smooth muscle cells covers the stent wire(arrowheads). Some medial atrophy is seen at the site of contact withthe stent wire. The internal elastic lamina appears intact (Elastica vanGieson stain). Bar Å 100 mm.
Fig. 2. Photomicrograph of a cross-section of the abdominal aortaobtained 40 weeks after the covered-stent placement. Marked atrophyof the entire media and disappearance of the internal elastic laminaare seen. Intraluminal thrombus is also seen (arrow) (Elastica vanGieson stain). Arrowhead indicates the membrane of the coveredstent. Stent wires were removed. Bar Å 300 mm.
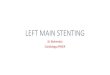
Fig. 3. Longitudinal sections (A, B) and cross-section (C) of anormal aorta obtained by microstereoscopy. A The vasa vasorumarising from the proximal trunk of the lumbar artery mainly runsparallel to the longitudinal axis of the aorta (arrows), then thesevessels anastomose and form a rich network situated in the periaor-tic tissue and adventitia. B, C From the adventitial plexus, arteri-oles arise and reach the border between the adventitia and themedia. The arterioles situated in the border between the adventitiaand the media form the second plexus (solid curved arrows). Aris-ing from their inner surface, some precapillary arterioles penetratethe outer media (open curved arrows). No vessels are seen in theinner media or intima. L Å the proximal trunk of the lumbar artery;bars Å 2 mm (A), 600 mm (B), and 400 mm (C).
was released. One or two stents were placed in the same manner.The bare stent was a single body Gianturco Z stent with an un-constrained diameter of 10 mm and a length of 10 mm. The cov-ered stent was constructed from a bare stent that was coveredoutside the wire framework with a thin polyurethane membrane(30 mm thick). No anticoagulants or antiplatelet agents were ad-ministered during follow-up. The animals were euthanized at 4,
8, 12, 20, 25, 40, and 45 weeks after stent placement. Each intervalhad one or two dogs. Eight bare stents were placed in eight aortasand nine polyurethane-covered stents in nine aortas (Table 1). Allstents were placed in the infrarenal aorta; the bare and coveredstents were placed in craniocaudal sequence except in dog 5.Throughout these experiments, animal care was conducted incompliance with the ‘‘Principles of Laboratory Animal Care’’

4k14 0031 Mp 47 Thursday Dec 04 08:24 AM SV-CVIR (v. 20, #6) 0031 (0254)
J. Sanada et al.: Effects of Endovascular Stenting on the Aortic Vasa Vasorum 47
Table 2. Proliferation of vasa vasorum at the site of bare-stent place-ment
Dogno.
Weeks afterstent placement
Degree of proliferation of vasavasorum
A-M OM IM NI
1 4 0 0 None None2 4 / / None None3 8 / / None /4 12 // /// None /6 20 / // None /7 25 / / None /8 40 0 0 None /9 45 0 0 None None
0 Å No proliferation; / Å mild; // Å moderate; /// Å markedproliferation; none Å no vascularization; A-M Å in the border be-tween the adventitia and the outer media; OM Å in the outer media;IM Å in the inner media; NI Å in the neointima
Table 3. Proliferation of vasa vasorum at the site of covered-stentplacement
Dogno.
Weeks afterstent placement
Degree of proliferation of vasavasorum
A-M OM IM NI
1 4 / / None /2 4 // // None None3 8 / // None /4 12 // // / ///5 12 /// /// // ///6 20 / // None None7 25 // / None /8 40 / / None /9 45 / / None //
Symbols and abbreviations same as in Table 2
(formulated by the National Society for Medical Research) andthe ‘‘Guide for the Care and Use of Laboratory Animals’’ (NIHPublication no. 80-23, revised 1985).
Preparation of Specimens
Just before sacrifice, the infrarenal aorta and the inferior vena cava(IVC) were catheterized via the femoral artery and vein. After 5000IU of heparin was intravenously administered, the animals weregiven an overdose of pentobarbital. Immediately after sacrifice, thestented area was ligated proximally and distally, and large branchesof the abdominal aorta were also tied. The aortic segment was flushedwith normal saline under 150 mmHg pressure from the catheterplaced in the infrarenal aorta. After exsanguination was completed,the aortic segment was perfused with silicone rubber compounds (Mi-crofil, Flow Tek Inc., Boulder, CO, USA). The aortas were excisedand allowed to cure overnight at 47C for hardening of the Microfil.The specimens were longitudinally bisected for microscopic and mi-crostereoscopic examinations. The former specimens were fixed with10% neutral buffered formalin for 48 hr, embedded in paraffin, sec-tioned at 2- or 3-mm thickness, and stained with hematoxylin andeosin stain and Elastica van Gieson stain. The latter specimens weredehydrated with 25%, 50%, 75%, 95%, and absolute ethyl alcoholfor 24 hr at each concentration and were cleared with methyl salic-ylate for 12–24 hr.
Results
Histopathological Changes in the Aortic Wall
With the bare stents (Fig. 1) a thin, translucent layer ofneointima containing smooth muscle cells completelycovered the stent. No mural thrombus was observed.Some medial atrophy was seen at the site of contactwith the stent wire. Over time, whole medial atrophyprogressed. The internal elastic lamina appeared intactand no inflammatory cell infiltrates were observed atany time.
With the covered stent (Fig. 2), although medialatrophy was seen only at the site of contact with thestent wire in the early weeks, at 40 or 45 weeks con-siderable atrophy of the entire media with a decrease
of smooth muscle cells and elastic fibers was seen. Theinternal elastic lamina disappeared and marked intimalthickening was also observed. These histopathologicalchanges were more prominent than those observed atthe site of bare stent placement.
Morphological Changes in the Vasa Vasorum
The normal aortic vasa vasorum (Fig. 3) arises fromthe proximal trunk of the lumbar artery, mainly runningparallel to the longitudinal axis of the aorta. Thereafterthese vessels, anastomosing each other, form a rich net-work situated in the periaortic tissue and the adventitia.Arterioles, arising from this plexus reached the borderbetween the adventitia and the media and form the sec-ond plexus. Arising from their inner surface, some pre-capillary arterioles penetrated the outer media. Novessels were seen in the inner media or the intima.
With the bare stent (Table 2, Fig. 4), at 4 weeksfollow-up, the vasa vasorum situated in the adventitiaslightly dilated and increased in number, and small ves-sels located in periaortic tissues proliferated. Vasa va-sorum situated in the adventitia, the border between theadventitia and the media, and the outer media increasedup to 12 weeks, and neointimal vascularization wasseen from 8 weeks. Thereafter these vascular prolifer-ations gradually decreased and at 45 weeks the num-bers of vasa vasorum situated in the adventitia and theborder between the adventitia and the media returnedto baseline. At this time, almost all of the newly formedvessels located in the neointima disappeared. No vas-cularization at the inner media was observed at anytime.
With the covered stent (Table 3, Fig. 5), at 8 weeks,more precapillary arterioles, arising from the vascularplexus situated in the border between the adventitia andthe media penetrated the outer media. Dilatation andproliferation of the adventitial vasa vasorum were alsoseen. Numerous capillary vessels were found in the

4k14 0031 Mp 48 Thursday Dec 04 08:24 AM SV-CVIR (v. 20, #6) 0031 (0254)
J. Sanada et al.: Effects of Endovascular Stenting on the Aortic Vasa Vasorum48
Fig. 4. Longitudinal sections (A, C) and cross-section (B) obtainedat the site of bare-stent placement. A, B At 12 weeks follow-up,vasa vasorum situated in the adventitia (straight arrows), the borderbetween the adventitia and the media (curved arrows), and theouter media (open curved arrow) increase up to this time, andneointimal vascularization is seen (arrowheads). C At 45 weeks,the numbers of vasa vasorum situated in the adventitia (straight ar-row) and the border between the adventitia and the media (curvedarrow) returned to baseline. At this time, almost all of the newlyformed vessels located in the neointima have disappeared. Stentwires are also seen. S Å hole corresponding to removed stentwires. Bars Å 400 mm (A and B) and 800 mm (C).
Fig. 5. Cross-sections obtained 8 (A), 12 (B), and 45 (C) weeks aftercovered-stent placement. A Arising from the vascular plexus situatedin the border between the adventitia and the media, more precapillaryarterioles penetrate the outer media (open curved arrows). B Markeddilatation and proliferation of the adventitial vasa vasorum are seen. Inthe border between the adventitia and the media, more new vesselsthan those seen in the normal aortic wall are also seen (solid curvedarrow). From that plexus, more precapillary arterioles penetrate theouter media (open curved arrow), and reach the inner media (open ar-row) and anastomose with the newly formed vessels in the neointima(open arrowheads). Many vessels are seen in the neointima (solid ar-rowheads). C Although the adventitial vasa vasorum is still dilated(straight arrow), the new vessels situated in the border between the ad-ventitia and the media (solid curved arrow), and precapillary arteriolesin the outer media (open curved arrow) have decreased in number. AÅ adventitia, M Å media, NI Å neointima; bars Å 600 mm (A) and400 mm (B and C).

4k14 0031 Mp 49 Thursday Dec 04 08:24 AM SV-CVIR (v. 20, #6) 0031 (0254)
J. Sanada et al.: Effects of Endovascular Stenting on the Aortic Vasa Vasorum 49
neointima between the native aortic wall and themembrane, and in the intraluminal thrombus as a resultof recanalization. At 12 weeks, marked dilatation andproliferation of the adventitial vasa vasorum werefound. In the border between the adventitia and themedia, more new vessels were seen. From that plexus,more precapillary arterioles penetrated the outer media,and reached the inner media and anastomosed with thenewly formed vessels in the neointima. Thereafter,these vascular proliferations gradually decreased. At 45weeks, although the adventitial vasa vasorum was stilldilated, the new vessels situated in the border betweenthe adventitia and the media, and the precapillary ar-terioles in the outer media had decreased in number.
Discussion
The normal aortic vasa vasorum, forming a network inthe adventitia and the border between the adventitia andthe media, extended to the outer media, the intima andinner third of the media were avascular. This findingsubstantiates the view that the intima and inner mediaare oxygenated by direct diffusion from the intralu-minal blood flow [1, 2].
At the site of stent placement vascular dilatationand proliferation of vasa vasorum, medial atrophy, andintimal hyperplasia were observed, and were moreprominent with the covered stent than with the barestent. The possibility has been suggested that hypoxiaof the arterial wall is the most important factor in de-veloping the vasa vasorum [3–8]. The hypoxic condi-tion is attributed to several factors such as reducedoxygen content in arterial blood flow, a change in thethickness of an arterial wall, and obstruction of the vasavasorum. The factors that reduce oxygen supply at thesite of bare stent placement are the thickness of the stentwire, thrombus around the stent wire, intimal hyper-plasia, and impairment of the blood flow in the vasavasorum due to permanent compression of the arterialwall by the stent [9]. In addition to the above factors,at the site of covered stent placement the oxygen supplyfrom the intraluminal blood will be impeded by themembrane of the covered stent, thrombus inside andoutside the membrane, and the marked intimal hyper-plasia. As a result, the more severely hypoxic conditionmay promote a more prominent proliferation of thevasa vasorum at the site of covered stent placement.
We also found that in the chronic state following stentplacement the degree of the dilatation and proliferationof the vasa vasorum had decreased. The previous reportsuggested that this probably occurred because the effectof the stent on the aortic vasa vasorum was temporary[9]. However, the medial atrophy and intimal hyperplasia
persisted despite the fact that proliferation of the vasavasorum had abated. It is reported that a close relationshipexists between the degree of intimal hyperplasia and pro-liferation of the vasa vasorum, and that development ofthe vasa vasorum promotes the intimal hyperplasia [3–5,8, 10–12]. We think that in the acute state the vasa va-sorum develops excessively to maintain the decreasedblood supply in the aortic wall and promotes the intimalhyperplasia, and in the chronic state it gradually subsideswith medial atrophy. Further evaluation of this hypothesisis necessary.
In conclusion, intravascular stent placement causednot only medial atrophy and intimal thickening but alsoprominent proliferation of the vasa vasorum in the aorticwall, probably due to severe hypoxemia induced by bare-and covered-stent placement. These changes were moreprominent following covered-stent placement than fol-lowing bare-stent placement. The prominent proliferationof vasa vasorum following covered-stent placement maybe necessary to maintain sufficient blood flow to the aorticwall. However, there was the possibility that the devel-opment of the vasa vasorum would promote the progres-sion of the intimal hyperplasia.
References
1. Heistad DD, Marcus ML (1979) Role of vasa vasorum in nour-ishment of the aorta. Blood Vessels 16(5):225–238
2. Nakata Y, Shionoya S (1973) Microcirculation and metabolismin the vascular wall concerned with the vasa vasorum. Jpn CircJ 37(3):217–227
3. Dıaz-Flores L, Dominguez C (1985) Relation between arterialintimal thickening and the vasa-vasorum. Virchows Arch [A]406(2):165–177
4. Nakata Y, Shionoya S (1966) Vascular lesions due to obstructionof the vasa vasorum. Nature 212:1258–1259
5. Barker SG, Talbert A, Cottam S, Baskerville PA, Martin JF(1993) Arterial intimal hyperplasia after occlusion of the adven-titial vasa vasorum in the pig. Arterioscler Thromb 13(1):70–77
6. Wilens SL, Malcolm JA, Vazquez JM (1965) Experimental in-farction (medial necrosis) of the dog’s aorta. Am J Pathol47(4):695–702
7. Okuyama K, Yaginuma G, Takahashi T, Sasaki H, Mori S (1988)The development of vasa vasorum of the human aorta in variousconditions. A morphometric study. Arch Pathol Lab Med112(7):721–725
8. Zemplenyi T, Crawford DW, Cole MA (1989) Adaptation toarterial wall hypoxia demonstrated in vivo with oxygen micro-cathodes. Atherosclerosis 76(2–3):173–179
9. Pisco JM, Correia M, Esperanca-Pina JA, de Sousa LA (1993)Vasa vasorum changes following stent placement in experimen-tal arterial stenoses. J Vasc Interv Radiol 4(2):269–273
10. Heistad DD, Armstrong ML, Marcus ML (1981) Hyperemia of theaortic wall in atherosclerotic monkeys. Circ Res 48(5):669–675
11. Sakariassen KS, Powell JS, Raines EW, Ross R (1987) Selective ex-pression of platelet-derived growth factor B-chain mRNA by humanendothelial cells and by human peripheral blood monocytes but notby smooth muscle cells. Thromb Haemost 58:261–267
12. Dıaz-Flores L, Valladares F, Gutierrez R, Varela H (1990) Therole of the pericytes of the adventitial microcirculation in thearterial intimal thickening. Histol Histopathol 5(2):145–153