Embed Size (px)
Citation preview

An evaluation of the TherapyCompetency Logbook from the
supervisor perspective.
Mandip Dosanjh
Commissioned by Dr Tracey Smith and Dr Ciara Masterson

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 2
Contents Page
1. Introduction............................................................................................................... 31.1 DClinPsy Programme Accreditation......................................................................... 31.2 Evidencing Competency ........................................................................................... 31.4 Existing Competency Frameworks ........................................................................... 41.5 The Leeds DClinPsy Competency Framework......................................................... 51.6 Placements ................................................................................................................ 5
2. Methodology .................................................................................................................. 62.1 Design Amendments.................................................................................................. 62.2 Design ....................................................................................................................... 62.3 Participants............................................................................................................... 72.4 Procedure .................................................................................................................. 72.4.1 Recruitment............................................................................................................ 72.4.2 Consent .................................................................................................................. 72.4.3 Data Collection ...................................................................................................... 82.5 Data Analysis ............................................................................................................ 82.6 Credibility checks ..................................................................................................... 82.7 Ethics......................................................................................................................... 9
3. Results ............................................................................................................................ 93.1 Interviews.................................................................................................................. 93.2 Validation process................................................................................................... 173.3 Recommendations................................................................................................... 18
4. Discussion..................................................................................................................... 194.1 Key findings............................................................................................................ 194.2 Strengths ................................................................................................................. 224.3 Limitations .............................................................................................................. 234.4 Dissemination of results.......................................................................................... 23
5. References .................................................................................................................... 256. Appendices................................................................................................................... 27

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 3
1. Introduction
This service evaluation project (SEP) investigated placement supervisors’ views on using
the Therapy Competency Logbook (TCL) to assess trainees’ competencies on the
Doctorate in Clinical Psychology (DClinPsy) training programme, at the University of
Leeds (UoL).
1.1 DClinPsy Programme Accreditation
DClinPsy programmes must comply with the Health Care Professions Council
(HCPC;2015) standards and the British Psychological Society will accredit programmes
according to their own standards for accreditation (BPS, 2017). The BPS and HCPC
provide standards of proficiency to ensure safe and effective practice, thus, developing
competent “psychologists who will be fit for purpose” (BPS, 2014, p. 1). These
professional bodies have a significant role in developing guidelines to inform the
curriculum of DClinPsy programmes; therefore, courses are often revising their
curriculum to maintain their accreditation. Whilst the BPS (2014) expect all standards to
be met, they are not prescriptive in how standards are achieved. They recognise that
programmes will achieve the standards in different ways based upon their distinctive
course identities (BPS, 2014).
1.2 Evidencing Competency
Demonstrating trainees’ competence in the delivery of therapy has always been a course
requirement; however, in 2014 the BPS revised guidelines stated that courses must find a
way to ‘evidence’ trainee’s therapy skills “in at least two evidence-based models of
formal psychological interventions, of which one must be cognitive-behaviour therapy”
(BPS, 2014, p. 12). This shift to evidencing reflects professionals’ opinion that
psychological interventions are delivered based upon a set of underpinning skills and that

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 4
these skills should be understood and deployed by those delivering such interventions
Roth & Pilling, 2015).
The BPS were not prescriptive in how courses operationalised this new requirement;
however, therapy skills were required to be evidenced against a “credible and robust”
framework (BPS, 2014, p.24) and where possible “benchmarked against recognised
criteria” (BPS, 2014, p. 24) as this would produce a credible competency framework “to
quality assure trainee work against” (BPS, 2014, p.29). The transition to competency-
based training presents many challenges for how clinical competence can be
implemented and assessed (Tweed, Graber & Wang, 2010). For instance, competencies
described at a general level result in everyone meeting the specification whereas
competencies that define too exhaustively result in many not fulfilling the criteria (Roth
& Pilling, 2008).
1.4 Existing Competency Frameworks
The BPS (2015) have provided their own version of a competency framework, it is called
‘the BPS Centre for Outcomes Research and Effectiveness’. The BPS encourage courses
to use or adapt their competency framework to evaluate trainee skill development.
The BPS (2015) centre for outcomes research and effectiveness (CORE) produced a
competency framework to evaluate trainee’s skills development and they encouraged
courses to use or adapt this framework. The BPS provide examples of therapy
frameworks in CBT, Psychodynamic and Systemic Therapies. In addition, courses could
also draw upon existing frameworks, such as Roth and Pilling’s (2008) CBT competency
framework and the Cognitive Therapy Rating Scale (CTS-R). Roth and Pilling’s (2008)
CBT framework was informed by manualised CBT interventions used within randomised
controlled trials in the treatment of anxiety and depression. Their framework is
considered a tool to inform programme curriculum, whereas the CTS-R is more useful to
capture assessment of adherence and competence, as it is a validated measure of clinical
competence in the delivery of CBT during training (Blackburn, James, Milne, & Reichelt,

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 5
2001). Without such clear and formal processes to evaluate trainees’ competencies, the
evaluation process becomes an idiosyncratic and individualised rating process (Tweed et
al., 2010); therefore, the introduction of evidencing trainees’ therapy skills systematically
provides a quality check system of competence.
1.5 The Leeds DClinPsy Competency Framework
In 2014, the Leeds DClinPsy programme developed the TCL in response to the BPS
guidelines. The document includes a range of therapeutic models for trainees to evidence
their plus one other model of therapy from: Cognitive Analytic Therapy, Systemic,
Acceptance and Commitment Therapy, Compassion Focused Therapy and Intensive
Short-Term Dynamic Psychotherapy and psychodynamic. The TCL was developed partly
based on Roth and Pilling’s (2008) framework and partly from consultation with local
experts and supervisors to develop each model-specific competency framework. The
involvement of local clinicians may have increased the ecological validity of the
competency framework, as Roth and Pilling’s (2008) competency framework emerged
from clinical trials, and thus, lacks representation of how routine clinical practice
corresponds to the framework.
1.6 Placements
In accordance with the BPS (2014) regulations, all placements are supervised by clinical
psychologists who have completed training in supervision that has either been recognised
by the BPS or provided by the UoL. The UoL also provides regular workshops on
supervisory skills and training events to ensure their trainees receive effective
supervision. Trainees are provided with the TCL before their first placement commences.
They are advised to focus on completing the CBT competency within the first two years
of training, whilst focusing on the plus one model in the final year. The course expects
both supervisors and trainees to contribute to the completion of the TCL.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 6
Aims
The course was interested in the supervisor’s experiences of using the TCL. The SEP
sought to understand whether:
the TCL is a useful and meaningful document to assess trainees’ competencies.
supervisors understand how to use the TCL to assess trainees’ competencies.
any adaptions or changes are required to the TCL.
supervisors have any training needs in relation to the TCL.
2. Methodology
2.1 Design Amendments
The final design was qualitative methodology; however, the original design was mixed
methods. Data from the focus group (stage 1) was intended to generate the online
questionnaire (stage 2). Recruitment for the focus group was successful, however, it was
impossible to get everyone together and therefore represented an unfeasible data
collection method. An amendment was requested to conduct short individual interviews
(stage 1) to then inform the online questionnaire (stage 2); however, unexpectedly, the
initial analysis of the individual interviews provided rich data. Therefore, it was
considered more ethical to use the resource of time to analyse the data set to its fullest
potential as opposed to beginning to develop the questionnaire. An amendment was then
requested to withdraw stage 2 and a validation process was implemented instead.
2.2 Design
Participants took part in a brief individual interview. Participants were given a choice of
telephone or face-to-face interview. A semi-structured interview schedule was used to
guide the interview (see Appendix 1). Interviews were then transcribed and analysed
using thematic analysis (Braun & Clarke 2006).

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 7
2.3 Participants
Inclusion criteria: qualified clinical psychologists who were supervisors for the DClinPsy
placements, who either were currently supervising or had supervised within the last three
years.
Exclusion criteria: not a qualified clinical psychologist or had not completed the
supervisor training.
The sample size was determined by current thematic analysis guidelines.
Thematic analysis can be applied to a minimum sample size of two participants (Fugard
& Potts, 2015). In addition, the project aimed to recruit at least one representative from
the five main clinical areas that clinical psychologists work in (health, forensics, child,
adult mental health and learning disabilities); therefore, the sample size aimed for 2-5
participants. 260 supervisors were emailed to take part in the project. The response rate
was five participants (child n=3, health n=1 and forensic n=1) and I checked that they had
offered a placement over the last three years.
2.4 Procedure
2.4.1 Recruitment
Participants were recruited from the placement supervisor list. The DClinPsy
administrative team sent an email invitation to the supervisors, with the participant
information sheet (PIS) (see Appendix 2). Participants responded to the principal
investigator by email if they wanted to participate. Recruitment operated on a first come
first served basis, with a view to selecting the most representative sample in terms of the
clinical areas; thus, using purposive sampling to ensure a representative sample.
2.4.2 Consent

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 8
The participants signed a consent form (see Appendix 3) before the interview was
conducted.
2.4.3 Data Collection
All participants chose a telephone interview. Interviews lasted approximately 20-30
minutes and were recorded. The audio file was then transferred to a secure drive on
university computers.
2.5 Data Analysis
The interviews were transcribed verbatim and analysed using thematic analysis (Braun &
Clark, 2006). The researcher followed Braun and Clarke’s (2006) four phases of data
analysis (see Appendix 4). Thematic analysis is one type of qualitative methodology and
“is a method for recognising and organizing patterns in content and meaning in
qualitative data” (Willig, 2013, p.58). Thematic analysis is appropriate to explore realist,
phenomenological or social constructionist research questions (Willig, 2013); therefore, it
was a suitable method of analysis, as the research question was interested in the
supervisors’ experiences of using the TCL. Other qualitative approaches were considered,
such as grounded theory (GT), but GT was considered inappropriate as the project did not
aim to generate a theory from the data to explain the phenomenon being investigated
(Charmaz, 1995).
2.6 Credibility checks
The initial themes and refinement of themes were quality checked with the commissioner
on several occasions and the commissioner was in agreement with how the themes were
developing. Furthermore, raw data extracts have been incorporated to support the themes.
In addition, a validation process was incorporated and the themes were presented at a
supervisor training event to see whether the themes fitted with their experiences of using
the TCL. The supervisors chose from responses: agree, disagree or don’t know (see
Appendix 5).

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 9
2.7 Ethics
Ethical approval was provided by the UoL School of Medicine Research and Ethics
Committee on the 5 July 2017. Informed consent was provided by participants to take
part in the project after reading the PIS and in addition, they were given the opportunity
to ask questions.
3. Results
3.1 Interviews
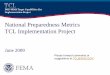
The analysis of data produced four themes and 12 subthemes (see figure 1). These will be
discussed in more detail below.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 10
Figure 1: thematic map
Theme 1: Challenges
The supervisors can experience challenges when using the TCL.
Pressure: Supervisors can experience a sense of pressure to provide the right experiences
on placements to ensure successful completion of the TCL. They feel that either the
service context (for example, forensic service) or their own limited experience is often in
conflict with the TCL or trainees’ expectations; therefore, at times, making it difficult to
meet competencies.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 11
“we have a family therapy team here…she was more the reflecting team...because
she couldn’t be the interviewer… I think some of it was harder, to score her on.”
Participant 3
“… if it was just up to me, to say that I am passing somebody on… say a CAT
placement, that would be really worrying…I’ve had third years come before,
wanting CAT and I said we need to get you extra CAT therapy because I’m not,
erm, au fait with that.” Participant 5
Supervisor Opportunities: Some supervisors would like to be able to provide more
expertise in other models, however, these opportunities are limited due to funding or
time. Therefore, sometimes supervisors can feel deskilled in meeting the trainees’ and the
TCLs expectations.
“…they happen to be supervised by somebody who has taken the time and effort
and possibly money to do that extra training…which is hard given that there is
hardly any time or funding available for extra training.” Participant 2
“…if this is what trainees are coming to me and they need, I need to be able to
provide that… I know very little about ACT, but I would like to know more.”
Participant 5
Finding a way: In light of such challenges, there is successful navigation and supervisors
are able to find a way to complete the TCL. Supervisors have learnt to think flexibly
when evidencing trainees’ competencies.
“we do use narrative and solution focused… and I suppose the skills of either, sort
of wangled in the generic competencies or we’ve looked at how closely aligned
they are to aspects of other models...” Participant 1

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 12
Theme 2: Uncertainty
Supervisors do have some doubts concerning the purpose of, and how to use, the TCL.
Level of evidence: Supervisors are unsure about how much evidence is required and
what format the evidence should take to prove a trainee’s competencies.
“how much evidence do we need to be able to confidently tick a box? Is it enough
for a trainee to say oh yeah I did that in a session or is it something that we have
to see on video or hear on audio or to actually see that, you know a formulation,
to see the visual product of that.” Participant 1
Truthful Reflection: Some supervisors are curious as to whether the TCL can truly
capture a trainee’s competence. They wonder what ticking a box represents, as doing
therapy and doing it well are two different things.
“…it tells you that they’ve done something but it does not tell you the quality of
that generic assessment or the quality of the initial formulation.” Participant 5
“…could somebody tick all the boxes and still be not very good at doing therapy?
Well, er, yes…” Participant 4
Also, some supervisors feel that a missed opportunity within the TCL is not being able to
evidence a trainee’s skills in models that are not listed in the TCL.
“It does sort of constrain, you know, what you can mark people on. They might
have lots of fantastic skills but, they’ve got to fit, you know, those six boxes.”
Participant 3
Capturing Therapy: Supervisors are hesitant as to whether any document could truly
capture therapy skills, as this is a difficult task. They perceive the quantifying of therapy

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 13
skills as a reductionist approach that potentially conflicts with what clinical psychology
is.
“I don’t think it’s useful as a mechanistic, yes you can do this, no you can’t do
this…I’m not sure anything works that well as a kind of a black or white, pass or
fail assessment…because it’s really experiential isn’t it? therapy and really hard
to capture that and to quantify it…” Participant 4
“…relying purely on, kind of accumulative description of things is rather removed
from what that skill will actually in tail in practice after qualification.” Participant
2
In addition, some supervisors think that the TCL is ‘missing something’ when assessing
trainees competence.
“It’s very much an approach and an attitude it’s not just, about ticking off doing
certain things. You could, do a lot of these things and still not really be working
systemically…” Participant 3
“…there is something that happens with a therapist and a client and I think it’s
missing that… it’s more than the alliance… whatever it is that makes, helps that
person come back to a session week after week. It’s that, that I don’t think is
being captured…” Participant 5
A living document: Some of the supervisors have noticed that the TCL is not used as an
active document throughout placement.
“… when it’s been presented to me, it’s usually been, around a mid-placement or
end of placement. I rarely see it at the beginning...” Participant 5

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 14
Furthermore, some supervisors seem unsure of how to integrate the TCL within the
placement and, because of this, the TCL can feel like an ‘add on’ and consequently a
tick-box exercise.
“clarity, in maybe… whether it’s intended to be, its primary function is around,
kind of, a memory aid for trainees after the course or kind of thinking about what
they’ve have achieved. Or whether it’s meant to be something that is meant to be
used more actively in supervision, that could be helpful.” Participant 1
“It felt like an add on, erm which perhaps it shouldn’t do, but it did… I do
wonder, where there’s a bit more help in thinking about embedding it, how we
embed it within supervision would be really helpful actually… But actually, a lot
of the things in there are really, really important. To make sure it just doesn’t
become a ticking exercise.” Participant 3
Some supervisors wonder whether the TCL should have a more active role within the
placement.
“…when I get my next one, erm, definitely on my radar now, to make better use
of it. Because it is really a comprehensive document, I think it could be used a bit
more.” Participant 5
Theme 3: Responsibility
This theme illustrates the role of responsibility and whose responsibility it is to complete
the TCL.
Partnership: When it comes to completing the TCL, trainees and supervisors have
different roles. Supervisors perceive the trainees to be responsible for taking the lead.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 15
“I think the main thing is having a trainee who can understand what it is for and
how to use it. So they are able to guide the supervisor in how to most
appropriately use it as a tool.” Participant 2
Supervisors see their role as supporting as opposed to being responsible for the
completion of the TCL. Supervisors support the trainees to notice skills that they have not
logged but are competent in and they use the TCL as a reflective tool to support the
trainee’s development.
“Some of the trainees, have not remembered what they’ve done or they’ve not
given themselves credit, what they’ve done work wise and I’ve said no no,
highlight to them, that was a rupture, yes you dealt with that.” Participant 5
“I see our job as supervisors to help them think about where there might have
been challenges in achieving certain skills, perhaps the skills they’ve not managed
to tick off. Why that might be or if it’s just they missed something or not noticed
that they were doing something.” Participant 1
Collaboration: This partnership of leading and supporting produces a collaborative
process in completing the TCL. The collaborative process has been a positive experience
and has facilitated meaningful conversations.
“Yes, it’s defiantly been collaborative and there had been times where I have
reminded them, and they have reminded me and we’ve had real discussions about
it.” Participant 5
Change: Supervisors are wondering whether they need to take on more responsibility in
how the TCL is used. This shift to joint responsibility, may encourage better use of the
TCL within placement.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 16
“I need to find a way of embedding it a bit better, rather than it being a, a bit more
of a tick box exercise.” Participant 3
Theme 4: Document Composition
Supervisors are generally satisfied with the format of the TCL and the document is fit for
purpose.
Direction: The supervisors feel that the TCL provides clear direction on how to assess
whether a trainee is competent as it breaks down the therapy skills, which helps the
supervisors to focus on what to look for.
“…it’s really helpful for having a framework for understanding what is it that you
are doing. You know, breaking it down…” Participant 4
“it’s really nice to have something that is really specific, so you know what you
are looking for. I was talking to colleagues just now, how we often don’t, talking
about how I, observing an trainee and kind of, what I’m sort of looking out for
and you know, how you do feedback. Erm, it’s nice to have a different model.”
Participant 3
The TCL also provides a framework for thinking as it directs the supervisor to identify
any gaps in the trainees’ development.
“…So it’s easy to see isn’t it, cos you’ve got a boxes, oh I’ve done that but we
haven’t done anything to do with that, so it does kind of prompt you, whereas if,
if you didn’t have it you might not think about all those aspects.” Participant 4

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 17
Structure: The supervisors think that the layout is clear, accessible to use, flexible as to
the information that can be entered, and the content is appropriate.
“I like that it’s got little columns and that it er directs you into where to put things
into it… I like that…almost, you do have a bit more freedom to put in what you
feel is relevant…” Participant 2
“…most things seemed really appropriate.” Participant 3
In addition, most of the supervisors think the reflective box is a good way of evidencing
learning and competencies.
“an opportunity to write down and reflect, what you have done with it…It’s more
about, kind of, being exposed to the concepts and using them. Having to write in
the reflection box, I guess is, is evidence of that isn’t it. That someone is engaging
with the concepts.” Participant 4
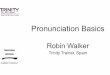
3.2 Validation process
The graph shows how strongly the themes resonated with a wider pool of supervisors
(n=11) (see figure 2). There was strong agreement for most of the subthemes, with the
exception of ‘supervisor opportunities’ and ‘collaboration’, which were less supported
but still relatively strong. On the rating document (see Appendix 5), some of the
supervisors (n=5) had not provided a rating for some of the subthemes but they had
written a qualitative entry, therefore, I made an assumption to determine their agreement
rating where possible, based on their qualitative comment.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 18
0
20
40
60
80
100
120
Chart Title
Agree Do not agree Not sure
Figure 2: Graph to show the results from the validation process.
3.3 Recommendations
The recommendations from the interviews and the validation process have not been
arranged in relation to the themes, as they are standalone. The list of recommendations
was generated by the participants. Recommendations were not considered if they were
not feasible, not clearly expressed or impractical.
Evidence format: the TCL could have a column to indicate which format the
skill was evidenced in: for example, audio or live.
Model the TCL on the neuropsychology document: as it is better at evidencing
how the skill was proven.
Confidence rating in competency of that skill: doing a skill once may not be a
marker of confidence and thus competency; therefore, it could be useful to track
progress in confidence.
Further training in therapy models: the course could upskill the supervisors.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 19
Consider evaluating process and relational elements of therapy.
Transparent rating scale: different levels of competency status: for example, a)
started doing, b) getting better, c) advanced.
4. Discussion
4.1 Key findings
The results indicated that generally the supervisors are satisfied with the document and it
is fit for purpose. In addition, the results have also identified adaptations that could
improve the TCL.
Aim 1: to establish whether the TCL is a useful and meaningful document to assess
trainees’ competencies.
The TCL is perceived to be a meaningful document as it can promote rich discussions
(‘Collaboration’) and some supervisors’ willingness to have a more active role in
completing the TCL (‘Change’) indicates that they see value in the document. The
supervisors also feel that the TCL is a useful resource to guide the assessment of the
trainees’ competencies (‘Document Composition’). The TCL also appears to be a useful
reflective tool to support trainees’ development in skills competency (‘Partnership’). The
supervisors also feel that the reflective element is a more meaningful process of
evaluation, compared to a standalone tick column (‘Structure’). The importance of
reflective practice has been argued by Schön to be just as important as technical
knowledge (for example, specific CBT techniques); and both are required to enable good
clinical decisions (as cited in Fisher et al., 2015, p. 731-732). Furthermore, the BPS
(2015. p. 45) state that trainees should “monitor and review their own progress and
develop skills in self-reflection and critical reflection on practice”. The TCLs
incorporation of logging reflections may be an important developmental skill for trainees.
Indeed a study found that clinical psychologists report the use of reflection and reflective

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 20
practice within their clinical work as benefitting them and their clients (Fisher, Chew &
Leow, 2015).
Aim 2: to establish whether supervisors understand how to use the TCL to assess
trainees’ competencies.
Generally, supervisors understood how to use the TCL to assess trainees’ competencies
(‘Document Composition’), although there are two issues. Firstly, supervisors are unsure
about how much and what format the evidence should take to verify a trainee’s
competence (‘Level of evidence’). Beck et al., (2014) outlined several different
approaches to assess trainees’ skills, other than hearing the trainee’s account of therapy.
This should include a combination of live observations, joint working and watching
videos of the therapy sessions, both during the trainee’s initial sessions and as they begin
mastering specific intervention techniques; all of which are methods of evidencing that
what the course advocates.
Secondly, supervisors are uncertain about how to integrate the TCL as an active
document within placement (‘A living document’). It has been suggested that even
though competence frameworks have been developed to inform a curriculum, such
frameworks can also guide the supervision process (Roth & Pilling, 2008) and it is
apparent from the analysis that this does not appear to be routinely happening on
placements. Therefore, the TCL may need a more active role within placement as it tends
to be introduced at the mid or end of placement visit. If the integration of the TCL within
placement was improved and embedded within supervision, it might be less vulnerable to
becoming a tick-box exercise or an afterthought, thus transitioning into a more
meaningful document with a purpose.
The subtheme ‘pressure’ does also indicate that supervisors are not entirely clear
on how to use the TCL as the DClinPsy programme does not expect supervisors to
comment on model skills that they themselves are not competent within. Furthermore,

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 21
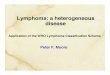
Recommendations Training
- on the frequency and type of evidence required to verify a trainee’sskill competency.
- supporting supervisors to integrate the TCL as an active documentthroughout placement. For instance, embedding within supervision.
Changes to TCLTCL may benefit from a column to indicate which format the skill wasevidenced in: for example, audio. This may encourage the supervisorsuse of different observation techniques. Furthermore, this tangiblestructure, may provide supervisors with some clarity and confidence inevidencing competency.
Trainees and supervisors owning joint responsibility for completion ofTCL.
Supervisors need to go back to the TCL guideline documents. Inaddition, the course may need to be more explicit in explaining theirexpectations of supervisors.
this is also explained in the document, ‘guidance for supervisors’, which is given to
supervisors by the programme. If supervisors were more familiar with this document, it
could alleviate their anxieties around a need to meet the TCL and trainees’ expectations.
To improve the supervisors understanding on how to use the TCL to assess
trainees’ competencies, the course may want to consider the following recommendations
listed in figure 3.
Figure 3: Recommendation box
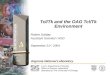
Aim 3: to establish whether any adaptions or changes are required to the TCL.
The results have shown that the TCL may benefit from being adapted, in light of
supervisors’ current experiences of using the document; some of these changes have

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 22
already been listed in figure 3, in addition further recommendations for changes are listed
in figure 4.
Figure 4: Recommendation box
Aim 4: to establish whether supervisors have any training needs in relation to the TCL
The results in relation to Aim 4 were highlighted in Aim 2. It was discussed in Aim 2 that
supervisors require further training to improve their understanding of how to use the
TCL. Firstly, supervisors are unsure about how much and what format the evidence
should take to verify a trainee’s competence and secondly, supervisors are uncertain
about how to integrate the TCL as an active document within placement. The
recommendations for these training needs are listed in figure 3.
4.2 Strengths
The initial themes and refinement of themes were quality checked with the commissioner
on several occasions. This credibility check reduced potential bias, and enhanced the
reliability of the findings and was conducted in adherence to guidelines for good
qualitative research (Elliot et al.,1999). Furthermore, raw data extracts were used to
support the themes. This transparency of analysis is considered an important check of
Recommendations: DClinPsy course to consider the following adaptations
Evaluating a trainee’s personal embodiment of a model. Evaluating a trainee’s competency in engaging with process and
relational issues within therapy. Transparent rating scale: recording skill competency in a more
transparent way in an attempt to determine the difference between beingable to do therapy well and doing therapy. It has been recommended thatrating scales can be a useful measure of professional competency as theyreflect growth and the development of skills as well indicating areas ofimprovement (Leigh et al., 2007).
A section for models that are not within the TCL.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 23
quality, reliability and validity within qualitative research (Elliot’s et al.,1999; Yardley,
2008). In addition, a validation process was incorporated to see whether the themes
resonated with a wider pool of supervisors. This process of triangulation provides further
validity to the findings.
4.3 Limitations
The SEP aimed to recruit the most representative sample in terms of the clinical areas in
which that trainees work, however, the SEP was unsuccessful in securing a wide
representative sample, as there was no representation from adult mental health (AMH)
and learning disabilities (LD). Therefore, the findings may not necessarily resonate with
supervisors within these areas. A missed opportunity at the validation process that could
have rectified this would have been to collect information on which clinical areas the
supervisors worked within. This information could have provided a consensus on whether
the themes resonated with clinicians from AMH and LD. In addition, the nature of
qualitative methodology and the small sample size impacts upon the generalisability of
results to the wider population. There may also be bias in the participants who chose to
participate, for instance in their motivations.
4.4 Future research considerations
The course may want to consider commissioning a quantitative SEP that evaluates the
TCL from the supervisor’s perspective. The project could generate an online
questionnaire that has been informed by the findings of this SEP. A quantitative approach
will provide a broader perspective on the findings. In addition, in light of this project’s
limitations, this future research may allow for a more representative sample in terms of
the clinical areas that the supervisors work in.
4.4 Dissemination of results

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 24
A poster and oral presentation for this SEP were presented at the UoL SEP conference on
Friday 26th October 2018.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 25
5. References
Beck, J. G., Castonguay, L. G., Chronis‐Tuscano, A., Klonsky, E. D., McGinn, L. K., & Youngstrom, E. A. (2014). Principles for training in evidence‐based psychology: Recommendations for the graduate curricula in clinical psychology. ClinicalPsychology: Science and Practice, 21(4), 410-424.
Blackburn, I. M., James, I. A., Milne, D. L., Baker, C., Standart, S., Garland, A., &Reichelt, F. K. (2001). The revised cognitive therapy scale (CTS-R): psychometricproperties. Behavioural and cognitive psychotherapy, 29(4), 431-446
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitativeresearch in psychology, 3(2), 77-101.
British Psychological Society, BPS. (2014). Standards for Doctoral programmes inClinical Psychology. Retrieved September 30, 2018 from:https://www1.bps.org.uk/system/files/Public%20files/PaCT/dclinpsy_standards_approved_may_2014.pdf
British Psychological Society, BPS. (2015). Standards for the accreditation of Doctoralprogrammes in clinical psychology. Retrieved September 30, 2018 from:https://www1.bps.org.uk/system/files/Public%20files/PaCT/clinical_accreditation_2015_web.pdf
British Psychological Society, BPS. (2017). Standards for Doctoral programmes inClinical Psychology. Retrieved September 30, 2018 from:https://www.bps.org.uk/sites/bps.org.uk/files/Accreditation/Clinical%20Accreditation%20Handbook%20(2017).pdf
Charmaz, K. (1995). Grounded Theory. In J.A., Smith, R, Harré & L, Van Langenhove.(Eds.), Rethinking methods in psychology (pp. 27-49). London: Sage.
Elliott, R., Fischer, C. T., & Rennie, D. L. (1999). Evolving guidelines for publication ofqualitative research studies in psychology and related fields. British journal of clinicalpsychology, 38(3), 215-229.
Fisher, P., Chew, K., & Leow, Y. J. (2015). Clinical psychologists’ use of reflection andreflective practice within clinical work. Reflective Practice, 16(6), 731-743.
Fugard, A. J., & Potts, H. W. (2015). Supporting thinking on sample sizes for thematicanalyses: a quantitative tool. International Journal of Social ResearchMethodology, 18(6), 669-684.
Leigh, I. W., Smith, I. L., Bebeau, M. J., Lichtenberg, J. W., Nelson, P. D., Portnoy, S., ... &Kaslow, N. J. (2007). Competency assessment models. Professional Psychology:Research and Practice, 38(5), 463.
Roth, A. D., & Pilling, S. (2008). Using an evidence-based methodology to identify thecompetences required to deliver effective cognitive and behavioural therapy fordepression and anxiety disorders. Behavioural and Cognitive Psychotherapy, 36(2), 129-147.
Roth, A., & Pilling, S. (2015). A competence framework for psychological interventionswith people with persistent physical health conditions report. NHS Education forScotland and the Improving Access to Psychological Therapies programme. UniversityCollege London. Retrieved February 2, 2019 from:

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 26
https://www.uea.ac.uk/documents/246046/11991919/Physical+LTC+Competence+Framework.pdf/fa58d42d-8df9-4b4f-bb00-a8681eaa0321
Smith, J., Flowers, P., & Larkin, M. (2009). Interpretative Phenomenological Analysis:theory, method and research. London: Sage.
Tweed, A., Graber, R., & Wang, M. (2010). Assessing trainee clinical psychologists' clinicalcompetence. Psychology Learning & Teaching, 9(2), 50-60.
Willig, C. (2013). Introducing qualitative research in psychology. London: McGraw-HillEducation (UK).
Yardley, L. (2008a). Demonstrating validity in qualitative psychology. Qualitativepsychology: A practical guide to research methods, 2, 235-251.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 27
6. Appendices
Appendix 1: Semi Structured Interview Guide (Version 1) (30.06.18)
Introductions Thank them for taking part. Outline SEP aims and ask if they have any questions about the
evaluation. Explain confidentiality.
Setting the scene questions How many trainees have you used the TCL with? What parts of the TCL have you used with your trainees? Have you ever used other competency frameworks, other than the TCL?
Topic area: usefulness/practicalities of TCL
1. What do you think about the concept of competency description and evaluation?
2. How useful is the document to assess and record the trainee’s competencies?(Prompts: is there anything you like about the TCL document? is there anything you do not likeabout the TCL document? Any suggestions for improvements?)
Topic area: Support
3. How confident do you feel in completing the TCL?(Prompts: do you feel like you need more support in how to complete the TCL? What parts of theTCL may you struggle with/works well? What do you think contributes to this low/highconfidence? What would you suggest would help e.g. further training?)
Topic area: Understanding
4. When you have completed the form with a trainee, how exactly have you gone about it? E.g. haveyou completed it together?(Prompts: Do all trainees approach the task in the same way? Do you always approach it in thesame way?)
5. How have you found this experience?(Prompts: Is there anything that makes it easier or harder to complete?)
Topic area: Meaningfulness
6. How meaningful do you think the TCL is, as an assessment document to capture and record thetrainees’ competencies?(Prompts: What do you see as the value in completing the TCL? are there any drawbacks? how doyou feel about completing the TCL?)
Closing: Is there anything else that you think might be helpful for me to know?

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 28
Appendix 2: Participant information sheet (version 1) (30/06/18)
“Evaluating the Therapy Competency Logbook from the supervisor perspective”
You are being invited to participate in this service evaluation because you are aplacement supervisor for the Leeds Dclin course. This information sheet describes theService Evaluation Project (SEP) and explains what will be involved if you choose totake part.
Who is conducting the study?
My name is …….. and I am a Psychologist in Clinical Training on the Leeds DClinProgramme.
What is the purpose of this study?
The British Psychological Society (BPS) is a professional body in the UK forpsychologists and psychology. The BPS stipulates that for accreditation, the ClinicalPsychology training programme must evidence that trainees are competent in the deliveryof therapeutic models. The guidelines require trainees to be competent in the delivery ofCognitive Behavioural Therapy plus one other model of therapy.
In 2016, the course evaluated the Therapy Competency Logbook from the traineeperspective and there is now a need to complete this from the supervisor perspective. Weare interested in finding out about your experiences of using the log book. The interviewsare being held to generate data which can then be used to develop a questionnaire for thesecond part of the evaluation, which will be an online survey.
What will participating in this evaluation involve?
If you agree to take part in the evaluation you will be invited to take part in the first stage,which is a brief individual interview. The interview will involve having a conversationabout your experiences of using the logbook. The purpose of the interview is to informthe development of a questionnaire (second stage). The interview will either be face toface or over the telephone and will last around 20-30 minutes. If you choose a face toface interview, the venue will either be your place of work or the University of Leeds.The interview will be recorded using an encrypted Dictaphone.
Right to withdrawYour participation is voluntary and you have the right to change your mind if you wish tono longer take part. You may withdraw prior to or during the interview. Also, you haveone week to withdraw your data from the date of interview.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 29
What will happen to the information I give?
Any information that you provide will be kept confidential. Any notes will not personallyidentify you and will be held securely (locked away when not in use) and shredded at thefirst opportunity. The audio recording of the interview will be immediately transferredfrom the recording device into an audio file, which will be stored on a secure server onthe university of Leeds computer network. The audio recording will then be immediatelyerased from the recording device after transfer to the computer. Your data on the audiofile will then be transcribed for the purpose of analysis and then permanently deletedfrom the server. Your transcript will be anonymous and will not have any identifiableinformation. Some of your anonymised quotations may appear in a report.
Dissemination of findings The SEP is a university assignment and a report will be written on the findings
and submitted for marking. The report will be disseminated to the clinical tutors at the university. The findings will be shared at the placement poster event at the University of
Leeds DClin Psychology course in September 2018. The findings may be submitted and published in the Clinical Psychology Forum,
in order to share good practice amongst training courses.
What will happen to my information after completion of the project?
All evaluation documentation will be hand delivered to the DClin research office for safekeeping. All electronic files will be copied over and stored on a secure drive and madeavailable to the department, which is restricted to a small number of research supportstaff. After 3 years all respective evaluation related documentation will be shredded andelectronic files will be deleted from the secure drive by research support staff
Confidentiality
The principle investigator will maintain confidentiality. Please be aware that a breach ofconfidentiality may be required if in the unlikely event there are concerns raised overyour practice and/or you disclose any information that is a cause for concern. In thisevent, the principle investigator will raise their concerns with you and wherever possiblewill discuss any action required with you first. Discussion may then need to take placewith third parties e.g. commissioner and supervisor of the SEP project.
What are the possible benefits of taking part?
The supervisor perspective could provide valuable information as to whether anythingneeds to be adapted or changed to ensure that trainee’s competencies are being assessedin a useful and time efficient way. Furthermore, it is important to know whethersupervisors feel confident in using the logbook to support trainees in documenting their

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 30
competencies. Also, the findings may indicate a need to change and/or offer additionaltraining and support to supervisors.
What are the possible disadvantages and risks of taking part?
You will need to give up some of your time and it is acknowledged that your availabilitymay be limited. There are no known risks of taking part in the project, however in theunlikely event of experiencing distress because of participating in this project; you cancontact Dr Tracey Smith (Clinical Tutor) at the University of Leeds.
Contact details
If you have any queries please email …….. (Psychologist in Clinical Training) on……...Alternatively, you can contact the commissioner of the project, Dr Tracey Smith [email protected]
This study has been reviewed and given ethical approval from the School of MedicineResearch Ethics Committee on the (05/07/2018), ethics project number (…….. ).

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 31
Appendix 3: Consent form (version 1) (30/06/18)
Evaluating the Therapy Competency Logbook from the supervisor perspective
I have read and understand the information sheet provided forthis SEP evaluation.
I have been given the opportunity to ask questions about theSEP and the answers have been satisfactory.
I understand that my participation is voluntary.
I understand that I may withdraw prior to or during theinterview without giving a reason and I can withdraw my dataone week after the completed interview date.
I know that the interview will be digitally recorded and thentranscribed. I understand that any personally identifableinformation will be removed from the transcript of the interviewand that I will not be identifable in any future reports,publications or presentations.
I understand that the data collected will be securely stored on auniversity server and password protected. I am aware of whatwill happen to my data after the SEP is complete.
If you would like a summary of the SEP, please provide anemail address, so it can be emailed
………………………………………………………………………………………………………………………………………………
Participant’s Name (Printed): ________________________Participant’s signature: _________________________ Date: __________Principle investigator’s signature: _______________________ Date: __________
Thank you for agreeing to take part in this study.Your contribution is very much appreciated

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 32
Appendix 4: Table summary of the phase of Thematic Analysis (Braun & Clarke, 2006)
Phase Description of the process
Phase 1
Familiarising yourself with
your data
involves immersion within the data in search of meaning and
patterns (reading and re-reading).
Note down initial ideas
Phase 2
Generating initial codes Generate initial list of ideas and what is interesting in the
data.
Produce initial codes from the data. The code identifies parts
of the data that are interesting to the analyst.
Organising data into meaningful groups.
Working systematically through the entire data set,
identifying interesting aspects in the data may form the basis
of repeated patterns across the data set.
Phase 3
Searching for themes
Sorting the codes into potential themes.
Beginning to analyse the codes and how differenee codes
may combiner to produce an overarching theme.
Phase 4
Reviewing themes
Refinement of themes is done by checking that they work in
related to the coded extracts (phase 1) and the entire data set
(phase 2), generating a thematic map.
Phase 5
Defining and naming themes
Define & further refine themes by identifying the essence of
the theme, the overall story and clear names for the themes.

Service Evaluation Project Evaluation of the TCL
Prepared on the Leeds D.Clin.Psychol. Programme, 2016 33
Appendix 5: Rating Document for validation process
Tick, Cross, Question mark next to subtheme
Qualitative box
X
?
Conflict
1. Pressure
2. SupervisorOpportunities
3. Finding away