Embed Size (px)
Citation preview

1
An evaluation of the psychological wellbeing and quality
of life of a small subsection of post-Myocardial Infarction
outpatients attending the Leeds Community Cardiac
Rehabilitation Service
Leanne Messham
Commissioned by Dr Penny Morris, Consultant Clinical Psychologist, Leeds Teaching
Hospitals NHS Trust

2
1. Introduction
1.1 Myocardial Infarction
A Myocardial Infarction (MI) is an outcome of cardiovascular disease and is
commonly known as a heart attack. The British Heart Foundation released statistics
showing that within England in 2012, 141,000 people were hospitalised with an MI
(BHF, 2014). The subsequent impact can be life threatening and have significant
implications in the immediate time following the cardiac event (e.g. Alsén, Brink,
Brändström, Karlson, & Persson, 2010; Barth, Schumacher, & Herrmann-Lingen,
2004). Therefore, understanding the impact of an MI and the needs of this population is
important in improving healthcare and health outcomes, including service structure (e.g.
utilising resources) and its potential economic impact.
1.2 Impact of an MI
1.2.1 Psychological and physical wellbeing
There is evidence highlighting the higher prevalence of anxiety and depression
in post-MI patients compared to the general population. For example, Lane, Carroll,
Ring, Beevers, & Lip (2002) assessed patients at three time points following their
cardiac episode. They found that symptoms of both depression and anxiety were
present from the initial assessment during the acute phase of the MI (2-15 days). These
symptoms increased during the following first year, with half of the sample
experiencing a degree of anxiety and/or depression. Another study reported a lower
frequency (20%) of post-MI patients experiencing a clinically significant degree of
depression (Ruo et al., 2003).
The relationship between psychological wellbeing and physical functioning is
also well established in the literature. Physical health outcomes are rated by mortality
Service Evaluation Project Leeds Community Cardiac Rehabilitation ServiceService Evaluation Project Leeds Community Cardiac Rehabilitation Service

3
and morbidity (risk of further cardiac events). There is an increased risk of sudden
death following an MI (Barth, Schumacher, & Herrmann-Lingen, 2004; Nielsen,
Vestergaard, Christensen, Christensen, & Larsen, 2013). One factor that influences
this association between MI and mortality is depression (van Melle et al., 2004;
Frasure-Smith et al., 2000); evidence suggests that even sub-clinical levels of
depression can affect this association (Bush et al., 2001). In terms of morbidity, a
meta-analysis of those having been assessed as depressed three months post-MI had a
2-2.5% increased risk of subsequent cardiac related problems within the following 2
years (van Melle et al., 2004). Post-MI patients’ mental health status was also
associated with an increased risk of secondary cardiac complications (Nielsen,
Vestergaard, Christensen, Christensen, & Larsen, 2013). Mental health status was
determined through a validated questionnaire assessing vitality, role-emotion and
mental health (p.2). Alongside cardiac disease severity, this relationship was also
related to factors such as physical activity, depression and anxiety all pertaining to a
persons’ quality of life (QoL).
It is noteworthy that these studies utilise different methods of identifying
psychological wellbeing. For example, identifying depression through interviews
versus self-report measures. Interviews are thought to be a conservative measure,
which may underestimate the severity of psychological difficulties, and may mask
other potential variables (Meijer et al., 2011). However, other evidence suggests that
there was no difference between these two methodologies when assessing for morbidity
factors (Barth et al., 2004).

4
1.2.2 Health Related Quality of Life
The psychological wellbeing of post-MI patients is also known to impact on
their perceived QoL. A large-scale study was conducted analysing the difference in self-
reported QoL and health status between those showing signs of depression and those
who did not (Ruo et al., 2003). This included participants who have experienced a range
of difficulties with Coronary Heart Disease (CHD) with over half of the sample
experiencing an MI. Those who showed signs of depression based on the Patient Health
Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001) were more likely to
experience mild symptom burden, mild physical limitation and mildly reduced QoL
(Ruo et al., 2003). However, studies specifically related to an MI found that after six
months anxiety and depression was significantly associated with greater problems
carrying out physical activities (Dickens et al., 2006). The greater level of impact
identified in this smaller scale study may be explained by the use of a HRQoL measure
that has greater sensitivity than broader QoL measures (Simpson & Pilote, 2003).
HRQoL refers to the impact the specific health problem has on different areas of a
persons’ functioning such as ‘physical, mental, emotional, and social’ aspects (Healthy
People, 2017). In summary, this evidence shows that having an MI can have a
significant impact on a persons’ QoL and is associated with the extent that it affects a
person’s psychological wellbeing.
1.3 Cardiac Services
1.3.1 Cardiac Rehabilitation
The National Institute for Health and Clinical Excellence (NICE, 2013)
recommends that all MI patients should be referred to a cardiac community
rehabilitation (CCR) programme. This should address health education, exercise and
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

5
stress management. Encouragingly, the 2016 annual report for the National Audit of
Cardiac Rehabilitation found that there has been an increase in CCR attendance up to
50% (BHF, 2016). However the BHF continues to emphasise the on-going need for an
improved understanding of MI patients’ needs and improvements to be made their
cardiac rehabilitation.
1.3.2 Leeds Cardiac Community Rehabilitation Education and Exercise
Programme
The Leeds Institute for Quality Healthcare (LIQH) leadership contributed to
improvements within the Leeds cardiology service. In collaboration with the wider team
they developed recommendations to progress the quality of psychological care of post-
MI patients. As medical professionals are found to under-recognise mental health
problems in this population they recommended the use of validated screening tools
(Ziegelstein et al., 2005). In light of this, the Community Cardiac Rehabilitation (CCR)
nurse-led team at Leeds are encouraged to implement measures of depression and
anxiety.
CCR includes home-based, individual and group based interventions, with
group-based interventions being the most commonly used in the UK (BHF, 2016). Part
of the Leeds CCR is the educational and exercise group programme targeted at those
who have been discharged from cardiac inpatient services. This involves a rolling 12-
session programme facilitated by cardiac-rehabilitation nurse specialists and a
specialist gym instructor. They also have access to a mental health practitioner and other
professionals who provide the educational sessions. Taken from the service leaflet, the
aim of this programme is to improve confidence in a safe environment, receive health
information and advice on their individual recovery, to facilitate peer
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

6
support and improve physical fitness. These groups run at five locations across the city
of Leeds (John Charles Centre, Kirkstall Centre, Armley Centre, John Smeaton and Holt
Park).
In terms of improving the rehabilitation service further, the literature on the
impact of an MI has limited applicability because it does not assess those specifically
within this type of CCR service. Through consultation with the Leeds team it was
apparent that some members assumed that patients attending their community group
programme might not experience a significant impact on their HRQoL or psychological
wellbeing. However, there is little objective evidence about this.
1.5 Aims of this evaluation
The aims of this evaluation were developed through meetings with the
commissioner, the wider multidisciplinary cardiac team and the lead nurse specialist of
the CCR.
The primary aims of this service evaluation were:
1) To measure the prevalence of depression and anxiety in post-MI patients
2) To measure the disease specific health-related quality of life of post-MI
patients
3) To investigate the relationship between depression and anxiety with health-
related quality of life of post-MI patients
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

7
This also included two additional exploratory aims:
1) To investigate the effect of participants’ time point in the programme on
the outcome measures. This was to explore whether those at different
points in the group programme require additional monitoring and support.
2) To provide any observations on the experience of using outcome measures
in this community-based setting.
A second evaluation conducted in partnership with this project aimed to
understand staff’s satisfaction with caring for the psychological needs of post-MI
patients and patients’ satisfaction receiving this service.
2. Methodology
2.1 Design & Analysis
This service evaluation was performed using a questionnaire survey
administered at one time point and used purposive sampling. Participants were at
different stages in the 12-session rolling group programme. At a group on any given
date, one participant may be in session 1 and another may be in session 5. Therefore,
the session number relates to the number of sessions attended by an individual
participant at their point of recruitment. Participants joined the programme at different
lengths of time since their MI and therefore this time frame does not relate to their
session number.
Three self-report questionnaires were administered and demographic
information including their employment status was also collected. Participants who
were not currently working but planned to return to employment were asked to rate
their confidence to return to work on a scale from 1 (‘least confident’) to 10 (‘most
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

8
confident’). Recruitment took place between June and September 2017 on 14 separate
occasions. Recruitment difficulties occurred due to the limited number of eligible
participants attending the group programme during the recruitment time frame. Due to
the small sample size only descriptive statistics could be calculated due to insufficient
power for inferential statistics.
The cardiac team had concerns about the feasibility of more sophisticated
methodologies e.g. repeated measures. This was due to the nurses’ limited capacity to
support data collection and the risk of burdening patients as another evaluation was
also being conducted with the CCR. This limited the design and research questions
that could be answered. As a result a new tool for measuring disease (MI) specific
HRQoL was used to provide novel findings that fit within the time constraints of the
service.
Ethical approval was gained from the University of Leeds (MREC16-093) and
R&D approval from Leeds Community Healthcare NHS Trust. Difficulties occurred
when seeking R&D approval as this required additional information regarding the
wellbeing of patients to participate. Through liaising with Health Research Authority,
the local R&D team and the cardiac MDT the protocol was adapted and approval
gained.
2.2 Participants
Twenty-three participants took part in this evaluation that met the following
inclusion criteria:
o Experienced an Myocardial Infarction (MI)
o Currently attending the Leeds Cardiac Community Rehabilitationeducation and exercise programme
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

9
o MI was their only identified cardiac-related health problem
o English as a spoken language
2.3 Measures
Generalised Anxiety Disorder (GAD-7)
The GAD-7 (Spitzer, Kroenke, Williams, & Lowe, 2006) is a short self-report
questionnaire assessing symptoms related to anxiety. Participants rate how frequently in
the past two weeks they have experienced each of the items from 0 (‘not at all’) to 4
(‘nearly every day’). These scores are classified into four categories of anxiety: 0-4
‘minimal’, 5-9 ‘mild’, 10-14 ‘moderate’ and 15-21 ‘severe’. For the purpose of this
evaluation, scores of 0 were categorised as ‘no symptoms’ and 1-4 as ‘minimal’
symptoms totaling five categories.
Patient Health Questionnaire (PHQ-9)
The PHQ-9 (Kroenke, Spitzer, & Williams, 2001) is a short self-report
questionnaire assessing symptoms related to depression. Participants rate how
frequently in the past two weeks they have experienced each of the items from 0 (‘not
at all’) to 3 (‘nearly every day’). The data was then categorised into the five clinical
classifications of depression of 0-4 ‘minimal’, 5-9 ‘mild’, 10-14 ‘moderate’, 15-19
‘moderately severe’, and 20-27 ‘severe’. For the purpose of this evaluation, scores of 0
were categorised as ‘no symptoms’ and 1-4 as ‘minimal’ symptoms totaling six
categories.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

10
Myocardial Infarction Dimensional Assessment Scale (MIDAS-35)
The MIDAS-35 (Thompson et al., 2002; Appendix B) is a self-report
questionnaire assessing the impact of health related difficulties specifically for post-MI
patients and recommended for cardiac rehabilitation. A licence was obtained from the
University of Oxford. The questionnaire has proven to have good construct validity
between the subscales of the MIDAS-35 and a generic QoL measure, and a very high
internal consistency on both single items and subscale scores.
This measure includes seven subscales of physical activity, insecurity,
emotional reaction, dependency, diet, concerns over medication and side effects.
Participants are asked to score how frequently they experience each of the items on a
scale of 0 (‘not at all’) to 4 (‘all of the time’). The total percentage for each subscale is
calculated and an overall total. The higher the percentage the more difficulties they
experience and the worse their health is understood to be. To make sense of this data,
the scores were split into five categories (0-20%, 21-40%, 41-60%, 61-80% and 81-
100%). Missing data was limited and handled according to the MIDAS-35 manual,
imputing the average total score for that individual.
2.4 Procedure
Participants were recruited from all centres used by the CCR. Initially, the lead
nurse of each group identified potential participants who met the inclusion criteria and
all of these patients were invited to take part in the evaluation. The researcher provided
each potential participant with the information sheet to read and an opportunity to ask
any questions before they decided whether to participate. Participants provided written
consent, completed the self-report questionnaires with guidance from the researcher
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
11

11
and had the opportunity to debrief while waiting for the group session to begin.
Participation took approximately 15 minutes.
3. Results
3.1 Service and sample
3.1.1 Demographic information
During the recruitment period, a total of 278 outpatients having experienced an
MI were referred to the Leeds CCR. Approximately 50% of these outpatients were
assessed for and were reported to have completed the group programme.
Of all those invited to take part (N =26), one patient declined taking part,
another was unable to take part due to their significant auditory difficulties and
another was omitted later on as it was medically unclear whether the individual had
experienced an MI. The final sample was a small subsection of MI patients (N =23).
The participants were comprised of 71% males and 29% females. This is similar to the
UK prevalence rates with approximately three times more men experiencing an MI
than women (Bhatnagar et al., 2015). This sample had a total average age of 61 years
old with a lower average age for men (58 years old) and women (67 years old)
compared to some published national data on MI patients (UCL, 2014).
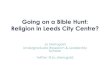
As stated in the methodology, Graph 1 shows that participants took part in the
evaluation at different sessions (more information in Appendix C) and more
participated earlier on in the group programme. Within the same session participants
were generally at different lengths of time since their MI. As it was obscured on the
graph, two participants from different groups participating at session three were 63
days since their MI and two participants scored within close range (51 and 52 days) at
session five.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
12

12
Graph 1. Relationship between participants’ group session number and the number of
days between their MI and participation
3.1.2 Employment
Out of the sample, nine participants reported working. Three of these
participants reported working fewer days per week since their MI with one of these
participants reporting that this was because of psychological factors. Furthermore, ten
participants reported that they had retired. Three of those reported retiring after their MI
with one stating that this was a direct consequence of the physical impact of their MI
and the other two participants reporting that this was an expected retirement for their
age. Lastly, three participants reported not working but had not retired. Of these,
one stated this was for both physical and psychological reasons and reported their
confidence returning to work as very low (2 out of 10). The other two reported this
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

13
was because of physical reasons and were confident about returning to work (10 out of
10). One participant did not provide any employment information.
3.2 Primary Aims
3.2.1 Anxiety and depression
These descriptive statistics are taken from the GAD-7 and PHQ-9. The subscales
pertaining to emotional and psychological wellbeing from the MIDAS-35 are presented
in the HRQoL results section.
Graph 2. The prevalence of anxiety post-MI
No symptoms Minimal Mild Moderate Severe
Clinical Classification of Anxiety
Graph 2 represents the prevalence of anxiety following an MI. One in 5 (22%)
of the sample showed signs of anxiety falling within a clinical classification (mild-
severe, N = 5). Specifically, as displayed in graph 1, two participants showed signs of
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Pe
rce
nta
ge
of
pa
rtic
ipa
nts
45%
40%
35%
30%
25%
20%
50%
15%
10%
0%
5%

14
at least mild anxiety and two showed signs of moderate anxiety, with one participant
scoring within the severe range. Three participants scored above the threshold for a
possible diagnosis of generalised anxiety disorder (>10). The majority of the sample
experienced some degree of anxiety, with nearly half of the sample experiencing
minimal anxiety (N = 11).
There is no published data for the UK general population using the GAD-7
therefore data from a German sample has been provided (Lowe et al., 2008). The
normative sample (n=5036) had an average age of 48.4 years old that is below the
average age in this sample and fewer male participants (approximately 50%). The
prevalence rates available showed that a larger proportion of the MI sample scored in
the moderate (9%) and severe (4%) ranges compared to the general population (5%
and 1% respectively).
Graph 3. The prevalence of depression post-MI
Nosymptoms
Minimal Mild Moderate Moderatelysevere
Severe
Clinical Classification of Depression
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Pe
rce
nta
ge
of
Pa
rtic
ipa
nts
45%
40%
35%
30%
25%
20%
50%
15%
10%
0%
5%

15
Graph 3 represents the prevalence of depression following an MI. One in four
(26%) of the sample showed signs of depression falling within a clinical
classification (mild-moderately severe, N = 6). Specifically, three participants showed
signs of mild depression with another three scoring within the moderately severe
range. No participants showed symptoms of depression at a moderate and severe
range. However, the majority of the sample experienced some degree of depression
symptoms, with just below half of the sample showing minimal signs of depression
(N= 10).
There is no published data for the UK general population using the PHQ-9 so
data from a German sample has been provided (Kocalevent, Hinz, & Brähler, 2013).
Data was taken from a subsection of this population (N=2693) that have similar
characteristics to the current sample (Hinz et al., 2016). The average age is 62.3 years
old with a larger proportion of male participants (59%). The normative data combined
the moderate severe (≥15-19) and severe (≥20-27) classifications used in this current
evaluation into one classification (severe: ≥15-27). The prevalence rates showed that a
smaller proportion of the MI sample scored in the mild range (13%) and the moderate
range (0%) compared to the general population (21.2% and 5.1% respectively). A
larger proportion of the MI sample scored in the moderately severe and severe range
combined (13%) compared to the general population in the severe range (1.5%).
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

16
3.2.2 Disease Specific HRQoL
These descriptive statistics below represent the HRQoL scores from the MIDAS-
35.
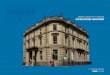
Graph 4. The frequency of participants scoring within each severity range for the
HRQoL sub-scales
MIDAS-35 Subscales
The worst health status was identified as those scoring in the highest range (81-
100%). As displayed in graph 4, the subscales that participants reported had the
greatest impact on their health status were concerns about medication (range 0-100%),
followed by diet (range 0-92%) and dependency (range 0-92%). At least one
participant scored within the 61-80% range for each subscale and at least one participant
scored within the 41-60% range for all subscales except for dependency. For all
subscales at least three participants scored with the 21-50% range.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
18
0-20%
21-40%
41-60%
61-80%
81-100%
16
14
Num
bero
fpar
ticip
ants 12
10
8
6
4
2
0

17
The largest proportion of participants for all subscales scored within the 0-20%
range, which was the lowest scoring category. A greater number of participants
reported experiencing milder but noteworthy problems with side effects (range 0-
63%), then emotional reaction (range 0-69%) followed by insecurity (range 0-61%). In
addition, all participants experienced difficulties with physical activity (range 2- 67%)
although only 9 participants rated problems in this area above 20%.
3.2.3 HRQoL, Anxiety and Depression
The HRQoL results were then stratified by the individuals’ clinical classification
of depression and anxiety.
Graph 5. Average total HRQoL score for those within each clinical classification of
anxiety
No symptoms Minimal Mild Moderate Severe
Clinical Classifications of Anxiety
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Ave
rage
tota
lqu
alit
yo
flif
e(%
)
40%
80%
60%
30%
20%
70%
50%
10%
0%

18
Graph 6. Average total HRQoL score for those within each clinical classification of
depression
Nosymptoms
Minimal Mild Moderate ModeratelySevere
Severe
Clinical Classifications of Depression
Graph 5 and 6 show that those who experience more severe anxiety and
depression also experience a larger subjective impact on their overall HRQoL. There
was also a difference between those who experienced no symptoms of anxiety and
depression with those who experience minimal symptoms. Those with minimal levels of
anxiety and depression whose scores didn’t reach a clinical classification experience
lower HRQoL demonstrated by a worse score on the impact of their health, compared to
those experiencing no symptoms.
3.3 Additional Exploratory Aim
3.3.1 Time point in the programme and outcome measures
Further exploratory analysis looked at the effect of participants’ time point in the
programme (the patients session number when competing the evaluation) on the
outcome measures. From graphical data there was a weak correlation suggesting that
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Ave
rage
tota
lqu
alit
yo
flif
e(%
)
40
60
30
20
50
10
0

19
those earlier on in the group may experience a worse HRQoL and greater difficulties
with anxiety and depression.
4. Discussion
Overall this evaluation provides evidence on the HRQoL and prevalence of
anxiety and depression in a small subsection of post-MI patients within the Leeds CCR
group programme. The results are discussed in light of the literature and the Leeds
service.
4.1. Primary aims
4.1.1 Anxiety and depression
In relation to their psychological wellbeing, 22% of the sample experienced
symptoms of anxiety and 26% experienced symptoms of depression that fell between
mild-severe ranges. This shows that some of those attending the CCR groups experience
a clinically meaningful impact on their psychological wellbeing that warrants
monitoring and may be consistent with diagnostic criteria. When compared to
the general population, those in this MI sample may experience more severe
depression and anxiety at a clinical level (≥10; Hinz et al., 2016, Lowe et al., 2008).
This may also support the need for targeted intervention in this area for MI patients.
However it is difficult to draw conclusions from this comparison due to the differences
in sample size, demographics and culture. There was also evidence of a significant
psychological impact from the measure of HRQoL (subscales of insecurity and
emotional reaction) with patients experiencing difficulties such as feeling irritable, bad
tempered, stressed and anxious about dying. These findings challenge the
Service Evaluation Project Leeds Community Cardiac Rehabilitation ServiceService Evaluation Project Leeds Community Cardiac Rehabilitation ServiceService Evaluation Project Leeds Community Cardiac Rehabilitation Service

20
assumption that those within the CCR education and exercise group are functioning
well and show that there is a spectrum of severity in relation to their psychological
wellbeing.
There was also evidence that a larger proportion of this subsection of post-MI
patients experience sub-clinical levels of depression and anxiety compared to no
reported difficulties at all. Even milder psychological difficulties are known predict
further cardiac-related problems (Bush et al., 2001). This suggests that using clinical
classifications may not offer an adequate or effective assessment of a client’s needs. The
second part of this service evaluation addresses how the nursing team are using
psychological measures. It may be that a more flexible approach to analysing the
information gained through screening tools needs to be taken.
4.1.2 HRQoL
In relation to the impact on HRQoL, all areas assessed appeared to be
important, with several participants experiencing their most frequent difficulties in the
areas of medication concerns, diet and side effects. There were a higher number of
participants experiencing less frequent but noteworthy difficulties across all other
subscales (physical activity, instability, emotional reaction and dependency). This
evidence shows that there is a spectrum of discrete factors that have the potential to be
unrecognised in relation to a persons’ HRQoL and therefore may signify possible
unmet need. This also adds to the importance of identifying how measures are used
within this service, for instance it may be that reading the items instead of using scores
may provide a better sense of a person’s experiences in order to better meet their
needs.

21
In relation to physical activity, all participants rated some degree of difficulty
in this area (e.g. being slowed down, lacking energy and thinking twice about
undertaking physical activity). Albeit this was one of several subscales where fewer
people rated more significant problems in this area. Alongside most participants
functioning well enough that they could engage in some level of activity (e.g.
continuing work or engaging in exercise). However this contrasts other studies (e.g.
Dickens et al., 2006) that have found a greater impact of the MI on physical activity.
This may be due to the specificity of the measures used in other studies to target
physical activity and not address the variety of QoL factors assessed by this project.
Although the MIDAS-35 is a valid measure there are two important factors
limiting the interpretation and application of its outcomes. As this measure is specific
to myocardial infarction there is no normative data available to assess how the results
compare to other population groups. Also, there were difficulties interpreting what
signifies a clinically significant impact on their QoL and subjectively applied
classifications had to be applied to analyse the data.
4.1.3 Anxiety, depression and HRQoL
In addition to these findings, those experiencing more frequent symptoms of
anxiety or depression experienced a greater impact on their overall HRQoL. This
evaluation also showed that seven participants reported a degree of physical or
psychological impact on their ability to work causing them either to retire, work at a
slower pace or were delayed returning to work. It may be appropriate to assume that
having an MI may have financial implications for the individual, and economically for
employers and healthcare services. Therefore, addressing these difficulties may also
impact on someone’s ability to continue working (Kisley & Simon, 2005). However,

22
there may be other variables contributing this effect. Also, potential participants not
attending the group when the researcher was present limited the sample size and
therefore the generalisability of these findings. Despite these limitations, these findings
are consistent with the wider literature on post-MI patient’s psychological wellbeing
affecting their QoL (e.g. Ruo et al., 2003).
4.2 Additional exploratory aims
4.2.1 Time point in the programme
There was preliminary evidence suggesting that those earlier on in the group
programme may experience worse HRQoL, depression and anxiety. Anecdotal
support comes from several participants who referred to having greater difficulties at
the beginning of the group. This suggests that patients earlier in the group programme
may require additional monitoring and support. However, this is only preliminary
evidence with no inferential statistical analysis. In addressing these secondary
exploratory aims there were a number of limitations of note. For instance, the spread
of participants across group sessions was limited (no participants from sessions 10
and 11). Furthermore, there may be confounding variables such as individual
characteristics and stressful life events that may influence patient outcomes. Finally,
the analysis did not take into account the length of time since each participant’s MI.
Therefore, the data must be interpreted with caution and no definitive conclusions can
be drawn. Future investigations using a repeated measures design would allow for a
robust assessment of the effectiveness of the group programme at improving patient
outcomes.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

23
4.2.2 Observations
The current service pathway for addressing the psychological wellbeing needs
of those attending the group includes the advised use of two standardised measures
used during the assessment, a mental health talk within the education part of the group
programme which addresses stress and stigma and the ability to signpost the
individual to the mental health practitioner for further support. Precise figures on
referral rates to the individual support service were unable to be provided but the
mental health practitioner believed that referrals from the group programme were very
few. Compared to the findings of this service evaluation, this may not reflect the level
of need within this part of the service. This is not a novel finding that patients with
depression post-MI may not receive appropriate healthcare for this and has been
attributed to a lack of confidence and competence of medical practitioners (e.g.
Dickens et al., 2006; Ziegelstein et al., 2005).
In terms of the Leeds CCR, one hypothesis for this is that the psychological
measures already being implemented are not highlighting an accurate sense of a
persons’ psychological wellbeing. Observations made during this service evaluation
suggest potential factors that may be contributing to this discrepancy. Firstly, the nurses
have limited opportunities to spend on-to-one time with patients to ensure their
understanding and mindful reflection upon their experiences. This appeared to be
affected by the size of the group on the day, lack of privacy and the needs of the other
group members. There were also suggestions of patient factors such as their willingness
to receive mental health support, which may be due to stigma. It is hoped that the
secondary CCR evaluation will obtain more valid and reliable information about staff
and patients experiences of using these tools/psychological care.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

24
4.3 Recommendations
A more detailed copy of the recommendations can be found in appendix A.
Ø To promote the mental health and QoL needs of those post-MI patients
attending the Leeds CCR education and exercise programme amongst the
nursing team.
Ø For nurses to improve how consistently they implement and use the outcomes
from psychological screening tools.
Ø To consider implementing a MI-specific QoL measure such as the MIDAS-35
utilised in this evaluation, to improve the identification of the specific needs of
these patients.
Ø To review the content of the CCR group programme, comparing the needs
highlighted from this evaluation to the current content.
Ø To review the ways in which individual’s needs are identified and met, namely,
considering the way in which these tools are delivered to ensure meaningful and
accurate recordings, and how the information is used.
4.4 Dissemination of findings
The findings of this service evaluation have been presented to the Leeds doctoral
course and commissioners. In addition, they will be disseminated within the Leeds
cardiology service and at the Leeds Community Healthcare NHS Trust research event.
This will also be written up for publication in conjunction with the second part of this
service evaluation.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

25
4.5 Conclusions
The Leeds CCR service provides a range of support in the important time
period following patients’ MI, as advocated by NICE guidance (2013) and British
Heart Foundation (2014, 2016). Their education and exercise group programme treats
people with varying experiences. There is evidence that a small proportion of this
population group are experiencing problems with their psychological wellbeing with
some reaching levels warranting clinical monitoring, diagnosis and intervention for
anxiety and depression. In addition, a greater proportion of this population report
problems with their quality of life related to their MI across the areas of physical
activity, insecurity, emotional reaction, dependency, medication concerns, diet and
side effects. In light of this, recommendations associated with clinical practice have
been provided.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

26
References
Alsén, P., Brink, E., Brändström, Y., Karlson, B., & Persson, L. (2010). Fatigue aftermyocardial infarction: Relationships with indices of emotional distress, andsociodemographic and clinical variables. International Journal Of NursingPractice, 16(4), 326-334.
Barth, J., Schumacher, M., & Herrmann-Lingen, C. (2004). Depression as a risk factorfor mortality in patients with coronary heart disease: a meta-analysis.Psychosomatic Medicine, 66(6), 802–13.
Bhatnagar, P., Wickramasinghe, K., Williams, J., Rayner, M., & Townsend, N. (2015).The epidemiology of cardiovascular disease in the UK 2014. Heart, 101(15), 1182-1189.
Beck, A.T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961) An inventoryfor measuring depression. Archives of General Psychiatry, 4, 561-571.
British Heart Foundation. (2014). Retrieved fromhttps://www.bhf.org.uk/publications/statistics/cardiovascular-disease-statistics-2014
British Heart Foundation. (2016). Retrieved fromhttps://www.bhf.org.uk/publications/statistics/national-audit-of-cardiac-rehabilitation-annual-statistical-report-2016
Bush, D., Ziegelstein, R., Tayback, M., Richter, D., Stevens, S., Zahalsky, H., &Fauerbach, J. (2001). Even minimal symptoms of depression increase mortalityrisk after acute myocardial infarction. The American Journal OfCardiology, 88(4), 337-341.
Child, A., Sanders, J., Sigel, P., & Hunter, M. S. (2010). Meeting the psychologicalneeds of cardiac patients: an integrated stepped-care approach within a cardiacrehabilitation setting. The British Journal of Cardiology, 17, 175-9.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

27
Dickens, C., McGowan, L., Percival, C., Tomenson, B., Cotter, L., Heagerty, A., &Creed, F. (2006). Contribution of depression and anxiety to impaired health-relatedquality of life following first myocardial infarction. The British Journal OfPsychiatry, 189(4), 367-372.
Frasure-Smith, N., Lesperance, F., Gravel, G., Masson, A., Juneau, M., Talajic, M., &Bourassa, M. (2000). Social Support, Depression, and Mortality During the FirstYear After Myocardial Infarction. Circulation, 101(16), 1919-1924.
Healthy People. (2017). Retrieved fromhttps://www.healthypeople.gov/2020/about/foundation-health-measures/Health-Related-Quality-of-Life-and-Well-Being
Kisely, S. & Simon, G. E. (2005). An international study of the effect of physical illhealth on psychiatric recovery in primary care. Psychosomatic Medicine, 67, 116–122.
Kroenke, K., Spitzer, R., & Williams, J. (2001). The PHQ-9. Journal Of GeneralInternal Medicine, 16(9), 606-613.
Lane, D., Carroll, D., Ring, C., Beevers, D., & Lip, G. (2002). The prevalence andpersistence of depression and anxiety following myocardial infarction. BritishJournal Of Health Psychology, 7(1), 11-21.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Lowe, B., Decker, O., MŸller, S., Brähler, E., Schellberg, D., Herzog, W., & Herzberg,P. (2008). Validation and Standardization of the Generalized Anxiety DisorderScreener (GAD-7) in the General Population. Medical Care, 46(3), 266-274.
Hinz, A., Mehnert, A., Kocalevent, R., Brähler, E., Forkmann, T., Singer, S., &Schulte, T. (2016). Assessment of depression severity with the PHQ-9 in cancerpatients and in the general population. BMC Psychiatry, 16(1).
Kocalevent, R., Hinz, A., & Brähler, E. (2013). Standardization of the depressionscreener Patient Health Questionnaire (PHQ-9) in the general population. GeneralHospital Psychiatry, 35(5), 551-555.

28
Meijer, A., Conradi, H., Bos, E., Thombs, B., van Melle, J., & de Jonge, P. (2011).Prognostic association of depression following myocardial infarction withmortality and cardiovascular events: a meta-analysis of 25 years ofresearch. General Hospital Psychiatry, 33(3), 203-216.
Morley, D., Jenkinson, C., & Churchman, D. (2011). MIDAS-35- MyocardialInfarction Dimensional Assessment Scale User Manual. Oxford UniversityInnovation Limited.
National Institute Centre for Health and Care Excellence. (2013). Retrieved fromhttps://www.nice.org.uk/guidance/cg172/chapter/1-Recommendations#cardiac-rehabilitation-after-an-acute-myocardial-infarction-mi-2
Nielsen, T., Vestergaard, M., Christensen, B., Christensen, K., & Larsen, K. (2013).Mental health status and risk of new cardiovascular events or death in patientswith myocardial infarction: a population-based cohort study. BMJ Open, 3(8),e003045.
Ruo, B., Rumsfeld, J., Hlatky, M., Liu, H., Browner, W., & Whooley, M. (2003).Depressive Symptoms and Health-Related Quality of Life. JAMA, 290(2), 215.
Schweikert, B., Hunger, M., Meisinger, C., Konig, H., Gapp, O., & Holle, R. (2008).Quality of life several years after myocardial infarction: comparing theMONICA/KORA registry to the general population. European Heart Journal,30(4), 436-443.
Simpson, E. & Pilote, L. (2003). Quality of life after acute myocardial infarction: asystematic review. Canadian Journal of Cardiology, 19(5), 507-511.
Spitzer, R., Kroenke, K., Williams, J., & Lšwe, B. (2006). A Brief Measure forAssessing Generalized Anxiety Disorder. Archives Of Internal Medicine, 166(10),1092.
Stewart, M. (2007). The Medical Outcomes Study 36-item short-form health survey(SF-36). Australian Journal Of Physiotherapy, 53(3), 208.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

29
Thompson, D., Jenkinson, C., Roebuck, A., Lewin, R., Boyle, R., & Chandola, T.(2002). Development and validation of a short measure of health status forindividuals with acute myocardial infarction: the myocardial infarctiondimensional assessment scale (MIDAS). Quality of Life Research, 11(6), 535-43.
University of London. (2014). Myocardial Ischaemia National Audit Project.Retrieved fromhttps://www.ucl.ac.uk/nicor/audits/minap/documents/annual reports/minap-public-report-2014
van Melle, J., de Jonge, P., Spijkerman, T., Tijssen, J., Ormel, J., & van Veldhuisen,D. (2004). Prognostic Association of Depression Following MyocardialInfarction With Mortality and Cardiovascular Events: A Meta-analysis.Psychosomatic Medicine, 66(6), 814-822.
Ziegelstein, R., Kim, S., Kao, D., Fauerbach, J., Thombs, B., & McCann, U. (2005).Can Doctors and Nurses Recognize Depression in Patients Hospitalized With anAcute Myocardial Infarction in the Absence of FormalScreening?. Psychosomatic Medicine, 67(3), 393-397.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

30
Appendix A
Full Recommendations
Ø To promote the mental health and QoL needs of post-MI patients in the Leeds CCR
education and exercise programme amongst the nursing team. This is with the
purpose of developing their awareness that a small proportion of this population are
experiencing significant difficulties with anxiety and depression, and a greater
proportion experience significant problems across a range of factors associated with
HRQoL.
Ø For nurses to improve how consistently they implement and use the outcomes from
psychological screening tools, at least at initial assessment and discharge
appointments. Assessing these difficulties between the beginning and end of the
group programme may enable more individualised and effective healthcare through
improved identification of needs in line with guidelines (NICE, 2013).
Ø To consider implementing a MI-specific QoL measure such as the MIDAS-35 utilised
in this study, to improve the identification of the specific needs of these patients.
This may help tailor the group programme and individual support. The advantages
of this particular measure are that it also encompasses an assessment of
psychological wellbeing and it may be considered to replace the two current
screening measures so not burden patients. However consideration must be taken
before such a change is made and consultation with patients is advised.
Ø To review the content of the CCR group programme, comparing the needs highlighted
from this evaluation to the current content. For example, evaluating whether the
mental health talk adequately addresses the range of potential emotional and
psychological problems experienced.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

31
Ø To review the ways in which individual’s needs are identified and met, namely,
considering the way in which these tools are delivered to ensure meaningful and
accurate recordings, and how the information gathered is used. This may include
reviewing the competing demands that nurses are under during the group to
meaningfully utilise objective measures of wellbeing and functioning. This will be
directly addressed within the second part to this service evaluation.
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service

32
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
Appendix BMI Dimensional Assessment Scale (MIDAS-35)
Removed from online report for copyright reasons.

33
Appendix C
Table 1. Number of participants recruited at each session in the group programme
Session Number ofNumber Participants
1 1
2 3
3 4
4 4
5 3
6 2
7 1
8 0
9 3
10 0
11 0
12 2
Service Evaluation Project Leeds Community Cardiac Rehabilitation Service
34