Embed Size (px)
Citation preview

European Journal of
Nuclear Medicine Original article
An evaluation of Technegas as a ventilation agent compared with krypton-81 m in the scintigraphic diagnosis of pulmonary embolism Gary Cook and Susan E.M. Clarke
Department of Nuclear Medicine, Guys Hospital, London SE1 9RT, UK
Received 24 August 1991 and in revised form 24 February 1992
Abstract. A ventilation agent that provides good quality lung images, which is cheap, easy to use and non-toxic, with a low radiation dose, has long been sought. Techne- gas, an ultrafine aerosol of technetium-99m-labelled car- bon, was developed with these qualities in mind. We have studied Technegas in a clinical setting to evaluate some of these qualities. Twenty-five patients referred with a diag- nosis of suspected pulmonary embolism were investigat- ed during the same study using both krypton-81m and Technegas as ventilation agents in conjunction with99mTc-macroaggregated albumin as a perfusion agent. Technegas provided images which were of satisfac- tory quality. Images were obtained relatively easily and without discomfort to the patient, and Technegas has the advantage of always being available. A semi-quantitative regional assessment was employed which showed a good correlation (r = 0.499, P < 0.001) between Technegas and krypton-8 lm ventilation. We report on an effect not pre- viously found to be significant, that is lung regions were better ventilated with Technegas than with krypton-8 lm. This altered the diagnostic probability rating of pul- monary embolism in a number of patients (n = 3, 12%) compared with krypton-81m. This effect was also noted in a further 8 patients (32%) without a change in the diagnostic probability. We offer possible explanations for this phenomenon.
Key words: Pulmonary embolism- Ventilation perfusion scintigraphy - Technegas - Technetium-99m
Eur J Nucl Med (1992) 19:770-774
In t roduct ion
Technetium-99m Technegas is a new substance devel- oped for lung ventilation scintigraphy. It is an ultrafine
Offprint requests to: S.E.M. Clarke
aerosol of 99mTc-labelled carbon formed by burning 99mTc-pertechnetate in a carbon crucible at 2500 ° C in the presence of argon. The particles produced are of the order of 140 nm in diameter (Strong and Agnew 1989). These are inhaled by the subject via a mouthpiece. Technegas has been likened to 'radioactive soot' (Butch et al. 1986) and has properties shared by both gases and aerosols. Its penetration characteristics are gas-like, as it has a smaller and more uniform particle size than other aerosols (Burch etal. 1986; Hilson et al. 1989; Isawa et al. 1991 ; Strong and Agnew 1989). The regional distribution of Technegas has been found to be no differ- ent to that of xenon-133 in both normal lungs (Amis et al. 1990) and in lungs with severe airflow limitation (Crawford et al. 1990). Central bronchial deposition oc- casionally occurs, however, especially in patients with chronic obstructive airways disease (De Geeter et al. 1989; Zwinenburg et al. 1990), a feature well recognized with aerosols (Alderson et al. 1984).
Technegas has previously been compared clinically with xenon-133 (Mannting et al. 1990; Rimkus and Ash- burn 1990; Sullivan et al. 1988), and krypton-81m (Pel- tier et al. 1990; Shields et al. 1989; Hilson et al. 1989; Zwinenburg et al. 1990; James et al. 1991 a) both quanti- tatively and qualitatively in patients with known chronic lung disease and for the investigation of pulmonary em- bolism. Generally, it has compared favourably, giving similar or better diagnostic information of good quality. Most authors report that patients and technicians have found the system easy to use, but its quality and justifica- tion for use have been questioned (De Geeter et al. 1989; Zwinenburg et al. 1990). Minor side effects, thought to be due to first breath hypoxia, have been noted but can easily be negated by the simultaneous administration of oxygen to the patient (James et al. 1991 b; Isawa et al. 1991).
Technegas seems to have gained wide acceptance in Australia (Murray 1991) but so far has generated rela- tively few reports in the literature. In a survey of 360 hospitals in the UK, only 2 used Technegas as a ventila- tion agent (White et al. 1991).
© Springer-Verlag 1992

We have compared Technegas with s~mKr in 25 pa- tients refer red with suspec ted p u l m o n a r y e m b o l i s m to- ge ther wi th a qua l i t a t ive a n d semi -quan t i t a t i ve eva lua- t ion. We also r e p o r t on an effect n o t p rev ious ly h igh- l ighted, namely , Technegas m a y increase the p r o b a b i l i t y scor ing o f p u l m o n a r y e m b o l i s m as a d iagnos is . We offer a poss ib le e x p l a n a t i o n for this p h e n o m e n o n .
Patients and methods
Twenty-five patients were prospectively studied, having been re- ferred to the Department of Nuclear Medicine for further investiga- tion of suspected pulmonary embolism. There were 20 women and 5 men patients. Their ages ranged from 20 to 80 years, mean 48.1 years. Six patients were known to have either clinical, radiographic or lung function evidence of chronic lung disease, and 12 patients were current smokers. The presenting complaints of patients varied between pleuritic chest pain (12), dyspnoea (7), pleuritic pain and dyspnoea (4) and unexplained pulmonary hypertension (2). Pa- tients slowly inhaled Technegas via a mouthpiece with a nose clip attached from residual volume to total lung capacity and were asked to breath-hold for about 5 s whilst in a sitting position. If a count rate of 2 Kcount/s was not obtained, further breaths were taken, requiring 3M breaths. Patients unable to breath-hold, inhaled Technegas during tidal breathing, which produced the nec- essary count rate in most cases. Images were then taken in three views (posterior, left posterior oblique, right posterior oblique) with 300 Kprecounts per view. Immediately after these images had been acquired, 81mKr was administered via a facemask during tidal breathing to 300 Kprecounts per view. The same three views were used to obtain images.
Following the ventilation images, the patients were injected in- travenously with 100 MBq of 99mTc-macroaggregated albumin, and the same views were again acquired with the addition of an anterior view, 500 Kprecounts being obtained.
The resultant images were reviewed by a physician with experi- ence in nuclear medicine (SEMC) who was blinded as to whether
771
81mKr or Technegas was the ventilation agent, the two sets of im- ages on each individual being reviewed at different times.
The results were scored for the probability of pulmonary embo- lism in accordance with the criteria suggested by Biello et al, (1979), i.e. low, moderate or high probability. The image quality was scored on a scale from I to 4 indicating good quality, adequate quality, poor quality and not of diagnostic quality, respectively. A semi-quantitative method of assessing ventilation images was adapted from Secker Walker et al. (1970) and Fazio et al. (/982), each lung being divided into three horizontal segments on the pos- terior view and scored from 0 to 4, indicating normal, mildly re- duced, moderately reduced, markedly reduced and absent ventila- tion, respectively. The scores of each of the 6 segments for each pair of lungs were then compared for each ventilation agent.
Statistical analysis was carried out by calculating the correlation coefficient of the Technegas and 81mKr scores and by using the Wilcoxon test for differences between the quality of images.
Results
Seven patients had a moderate or high probability of pulmonary embolism (3 and 4, respectively) when 8 ~mKr was used as a ventilation agent. All 7 of these had the same probability rating in the Technegas studies, Of the 18 remaining studies, 15 resulted in the same probability rating with both ventilation agents, i.e. low probability. The 3 r ema in ing s tudies all showed a m a t c h e d segmenta l defect when 81mKr was employed , acqu i r ing a low p r o b - abil i ty, whereas when Technegas was used, the pe r fus ion defects c o r r e s p o n d e d wi th n o r m a l l y ven t i l a t ed areas, in- d ica t ing a m o d e r a t e p r o b a b i l i t y (Fig. 1).
N o n e o f these 3 pa t ien t s h a d p u l m o n a r y a n g i o g r a p h y pe r fo rmed , b u t c l inical fo l low-up has sugges ted tha t pa r - enchyma l lung disease was p resen t r a the r t h a n p u l m o - na ry embol i sm.
A B C
Fig. 1. Right posterior oblique (RPO) views of A perfusion, B Krypton-81m ventilation, C Technegas ventilation showing reduced perfusion at the right lung base posteriorly with a matched pattern with 81mKr ventilation but mismatch with Technegas

772
A B C
Fig. 2. RPO views of A perfusion, B s~mI<h" ventilation, C Technegas. Scans show a perfusion defect in the right posterior lung with near matching with 81mKr. There is mismatch with Technegas
Eight further patients showed relative areas of venti- lation/ventilation mismatch which did not, however, af- fect the probability rating. These all showed ventilation defects with slmKr which were less marked with Techne- gas. In general, these were in areas of reverse mismatch with S~mKr (i.e. ventilation worse than perfusion) or ar- eas that showed a degree of ventilation/ventilation mis- match rather than complete mismatch, with Technegas showing smaller ventilation defects (Fig. 2). Most of the ventilation/ventilation mismatches were seen to occur in the lower portions of the lungs.
The image quality was found to be better with slmKr (mean score 3.8) than Technegas (mean score 3.2; P < 0.002). Technegas received a score of 2 (poor quality) in 2 cases, both of which were elderly patients with dysp- noea and one of whom also had chronic obstructive airways disease. No images were thought to be of non- diagnostic quality with either agent, although 3 patients showed some evidence of central bronchial deposition of Technegas, 2 of whom were known to have chronic obstructive airways disease. Fifteen patients showed some evidence of stomach activity with Technegas, but neither of these features interfered with image interpreta- tion.
A semi-quantitative comparison of Technegas and s 1 mKr showed a good correlation (r = 0.499, P < 0.001).
Discussion
Technegas was designed with the shortcomings of other ventilation agents in mind and generally satisfies most of these in that it is cheap, always available and easy to use, delivers a low radiation dose (Burch et al. 1989) and, for the most part, produces good quality images. These, however, may not be of as good a quality as
SlmKr. Technegas is not an ideal ventilation agent, as it is not a true gas and therefore cannot be expected to represent exactly true regional ventilation. Technegas does have the advantage of not being cleared from the lung once the particles stick to the alveolar wall and hence is suitable for multiple images and single photon emission tomography (SPET) studies (Lemb et al. 1989). Technegas has also been used to assess ventilation abnor- malities in neonates (Kropp et al. 1989) and in intubated patients requiring assisted ventilation (Burch etal. 1989).
A modified form of Technegas, produced by altering the atmosphere in which the carbon particles are gener- ated, has recently been employed by Monaghan et al. (1991) to identify opportunistic infection and other dif- fuse lung pathology.
One disadvantage of Technegas is that the ventilation study usually needs to be performed prior to perfusion imaging, thereby possibly exposing the patient with nor- mal perfusion to extra, unnecessary radiation. Sullivan et al. (1988) and James et al. (1991 a) have obtained im- ages in the reverse order and have found them to be of diagnostic quality. This method involves giving a small dose of perfusion agent and achieving a higher count rate of Technegas activity. Problems could be anti- cipated, however, with the longer acquisition times of perfusion images (4-10 times) and with obtaining a high- er Technegas count rate in frail patients.
Our qualitative comparison of Technegas with slmKr showed the former to have lower scores (P<0.002), but these did not interfere with image interpretation except in 2 patients who were both elderly and dyspnoeic when only limited views could be obtained.
The semi-quantitative comparison showed a good correlation (r = 0.499, P < 0.001) between regional venti-
773
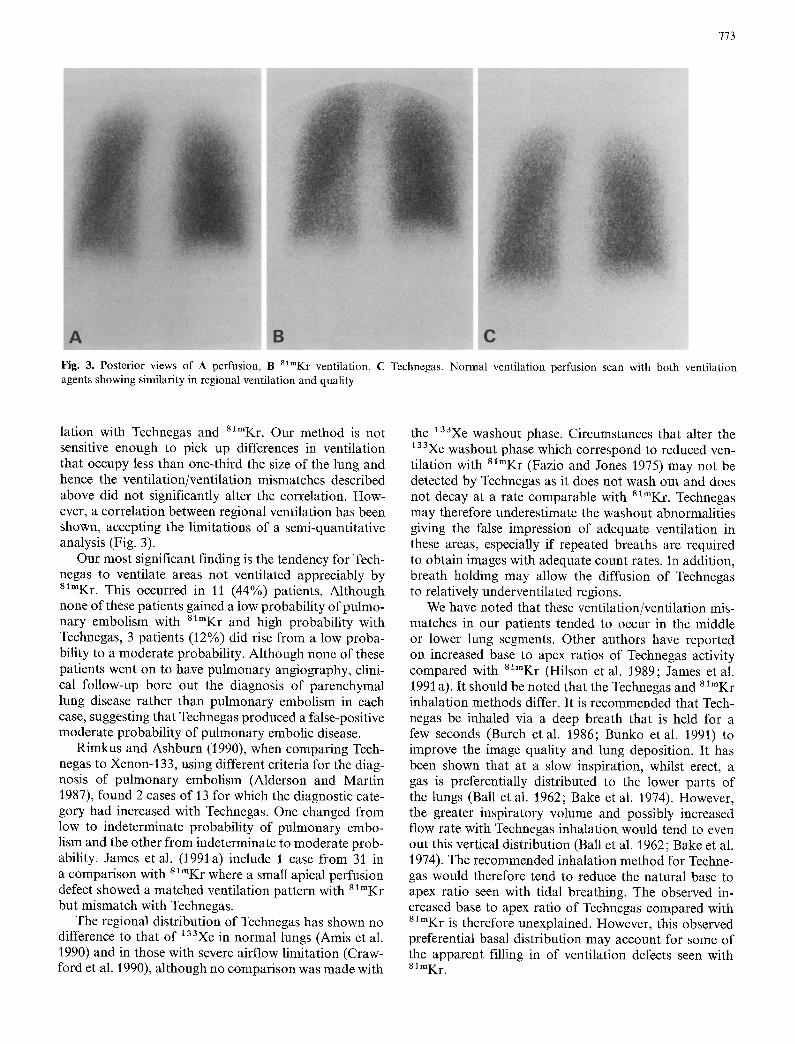
Fig. 3. Posterior views of A perfusion, B 81mKr ventilation, C Technegas. Normal ventilation perfusion scan with both ventilation agents showing similarity in regional ventilation and quality
lation with Technegas and 81mKr. Our method is not sensitive enough to pick up differences in ventilation that occupy less than one-third the size of the lung and hence the ventilation/ventilation mismatches described above did not significantly alter the correlation. How- ever, a correlation between regional ventilation has been shown, accepting the limitations of a semi-quantitative analysis (Fig. 3).
Our most significant finding is the tendency for Tech- negas to ventilate areas not ventilated appreciably by slmKr. This occurred in 11 (44%) patients. Although none of these patients gained a low probability of pulmo- nary embolism with 81mKr and high probability with Technegas, 3 patients (12%) did rise from a low proba- bility to a moderate probability. Although none of these patients went on to have pulmonary angiography, clini- cal follow-up bore out the diagnosis of parenchymal lung disease rather than pulmonary embolism in each case, suggesting that Technegas produced a false-positive moderate probability of pulmonary embolic disease.
Rimkus and Ashburn (1990), when comparing Tech- negas to Xenon-133, using different criteria for the diag- nosis of pulmonary embolism (Alderson and Martin 1987), found 2 cases of 13 for which the diagnostic cate- gory had increased with Technegas. One changed from low to indeterminate probability of pulmonary embo- lism and the other from indeterminate to moderate prob- ability. James et al. (1991a) include 1 case from 31 in a comparison with slmKr where a small apical perfusion defect showed a matched ventilation pattern with s ~ K r but mismatch with Technegas.
The regional distribution of Technegas has shown no difference to that of '33Xe in normal lungs (Amis et al. 1990) and in those with severe airflow limitation (Craw- ford et al. 1990), although no comparison was made with
the 133Xe washout phase. Circumstances that alter the 133Xe washout phase which correspond to reduced ven- tilation with 8'mKr (Fazio and Jones 1975) may not be detected by Technegas as it does not wash out and does not decay at a rate comparable with 81mKr. Technegas may therefore underestimate the washout abnormalities giving the false impression of adequate ventilation in these areas, especially if repeated breaths are required to obtain images with adequate count rates. In addition, breath holding may allow the diffusion of Technegas to relatively underventilated regions.
We have noted that these ventilation/ventilation mis- matches in our patients tended to occur in the middle or lower lung segments. Other authors have reported on increased base to apex ratios of Technegas activity compared with 81mKr (Hilson et al. 1989; James et al. 1991 a). It should be noted that the Technegas and 81mKr inhalation methods differ. It is recommended that Tech- negas be inhaled via a deep breath that is held for a few seconds (Butch et al. 1986; Bunko et al. 1991) to improve the image quality and lung deposition. It has been shown that at a slow inspiration, whilst erect, a gas is preferentially distributed to the lower parts of the lungs (Ball et al. 1962; Bake et al. 1974). However, the greater inspiratory volume and possibly increased flow rate with Technegas inhalation would tend to even out this vertical distribution (Ball et al. 1962; Bake et al. 1974). The recommended inhalation method for Techne- gas would therefore tend to reduce the natural base to apex ratio seen with tidal breathing. The observed in- creased base to apex ratio of Technegas compared with 8~mKr is therefore unexplained. However, this observed preferential basal distribution may account for some of the apparent filling in of ventilation defects seen with 81 mKr"

774
The possibility of Technegas showing the true ventila- tion pattern in these cases of ventilation/ventilation mis- match is unlikely. The alternative, that 81mKr shows falsely absent ventilation given that the perfusion defects match these 81mKr ventilation defects, would be difficult to explain.
Our observations of false-positives with Technegas have not previously been brought to the fore. The appar- ent filling-in of ventilation defects with Technegas in 11 (44%) of our patients [with an altered diagnostic catego- ry in 3 out of 25 (12%)] obviously has important clinical implications. A significant number of patients may be subjected to unnecessary treatment with anticoagulants or at least to further invasive investigation such as pul- monary angiography.
Conclusion
We conclude that Technegas is a ventilation agent which is relatively easy to use and produces satisfactory quality images. However, its use may lead to an increase in the diagnostic probability of pulmonary embolism when compared with 81mKr, resulting in possibly important clinical consequences. Further study of this phenomenon is required to evaluate this potentially useful agent.
References
Alderson PO, Martin EC (1987) Puhnonary embolism: diagnosis with multiple imaging modalities. Radiology 164: 297-312
Alderson PO, Biello DR, Gottschalk A, Hoffer PB, Kroop SA, Lee ME, Rammana L, Siegel BA, Waxman AD (1984) Tc-99m- DTPA aerosol and radioactive gases compared as adjuncts to perfusion scintigraphy in patients with suspected pulmonary embolism. Radiology 153:515-521
Amis TC, Crawford AB, Davison A, Engel LA (1990) Distribution of inhaled 99m technetium labelled ultrafine carbon particle aerosol (Technegas) in human lungs. Eur Respir J 3(6):679-685
Bake B, Wood L, Murphy B, Macklem PT, Milic-Emili J (1974) Effect of inspiratory flow rate on regional distribution of in- spired gas. J Appl Physiol 37(1): 8-17
Ball WC, Stewart PB, Newsham LGS, Bates DV (1962) Regional pulmonary function studied with xenon-133. J Clin Invest 41(3):519-531
Biello DR, Mattar AG, McKnight RC, Siegel BA (1979) Ventila- tion-perfusion studies in suspected pulmonary embolism. Am J Radiol 133 : 1033-1037
Bunko H, Seto M, Kuji I, Miyauchi T, Hisada K (1991) Lung ventilation imaging with Technegas: clinical study of lung depo- sition and ventilation/perfusion. Kaku-Igaku 28 : 229-239
Burch WM, Sullivan PJ, McLaren CJ (1986) Technegas-a new ven- tilation agent for lung scanning. Nucl Med Commun 7:865-871
Crawford ABH, Davison A, Amis TC, Engel LA (1990) Intrapul- monary distribution of 99m technetium labelled ultrafine car- bon aerosol (Technegas) in severe airflow obstruction. Eur Re- spir J 3(6): 686-692
De Geeter F, Bossuyt A, Jonckheer M (I 989) Comparison of Tech- negas to s l"Kr as a ventilation agent. Eur J Nucl Med 15:442
Fazio F, Jones T (1975) Assessment of regional ventilation by con- tinuous inhalation of radioactive krypton 81m. Br Med J 3 : 673-676
Fazio F, Wollmer P, Lavender JP, Barr MM (1982) Clinical ventila- tion imaging with In-113m aerosol: a comparison with Kr-81m. J Nucl Med 23 : 306-314
Hilson AJW, Pavia D, Diamond PD, Agnew JE (1989) An ultra- fine 99m-Tc-aerosol (Technegas) for lung ventilation scintigra- phy - a comparison with Kr-81m. J Nucl Med 30:744
Isawa T, Teshima T, Anazawa Y, Miki M, Motomiya M (1991) Technegas for inhalation lung imaging. Nucl Med Commun 12:47-55
James JM, Herman KJ, Lloyd J J, Shields RA, Testa H J, Church S, Stretton TB (1991 a) Evaluation of 99Tc~' Technegas ventila- tion scintigraphy in the diagnosis of pulmonary embolism. Br J Radiol 64: 711-719
James JM, Prescott MC, Leahy BC, Lloyd JJ, Shields RA, Testa HJ (1991b) Hypoxia during Technegas inhalation. Nuel Med Commun 12:287
Kropp J, Buhr W, Biersack HJ (1989) Lung inhalation scintigraphy in newborns. A study with the new tracer Technegas. J Nucl Med 30: 744
Mannting F, Morgan MG, Hedenstrom H, Maripuu E, Hedenstier- na G (1990) A comparative study of Xe-133 and Tc-99m-gas for assessment of regional ventilation. Eur J Nucl Med 16: 429
Monaghan P, IPC Murray, Mackey DWJ, Van-der-Wall H, Walker BM, Jones PD (1991) An improved radionuclide technique for the detection of altered pulmonary permeability. J Nucl Med 32:1945--1949
Murray IPC (1991) Clinical experience with Teehnegas. Clin Nucl Med 16:247-250
Peltier P, De Faucal P, Chetanneau A, Chatal JF (1990) Compari- son of technetium-99m aerosol and krypton-8 l m in ventilation studies for the diagnosis of pulmonary embolism. Nucl Med Commun 11 : 631-638
Rimkus DS, Ashburn WL (1990) Lung ventilation scanning with a new carbon particle radioaerosol (Technegas). Clin Nucl Med 15 : 222-226
Secker Walker RH, Jackson JA, Goodwin J (1970) Resolution of pulmonary embolism. Br Med J 4:135-139
Strong JC, Agnew JE (1989) The particle size distribution of tech- negas and its influence on regional lung deposition. Nucl Med Comm 10:425-430
Sullivan PJ, Burke WM, Burch WM, Lomas FE (1988) A clinical comparison of Technegas and xenon-133 in 50 patients with suspected pulmonary embolus. Chest 94:300-304
White PG, Hayward MWJ, Cooper T (1991) Ventilation agents - what agents are currently used? Nucl Med Commun 12:349- 352
Zwinenburg A, Royen EV, Dongen AV, Zanin D (1990) Experi- ence with 99mTc-Technegas as a ventilation tracer; comparison with 81mKr-gas. Eur J Nucl Med •6:440