Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1965, 28, 152
An evaluation of surgical treatment for spinal cordcompression due to metastatic carcinoma
RODERICK SMITH
From the Departments of Neurology and Neurosurgery of The London Hospital
The rising incidence of neoplastic disease in the pastthree decades (Registrar General, 1962), coupledwith improvement in surgical and medical treatment,has resulted in an increasing number of patients withmalignant deposits in an around the spinal cord beingreferred for surgical evaluation. The management ofthese cases has given rise to considerable discussion.Laminectomy and decompression in all cases of
spinal cord compression is advocated by Perese(1958), Rogers (1958), and Dinning (1961) on thegrounds that surgery is necessary to establish adiagnosis and that the patient may benefit from theoperation. Torma (1957) reviewed 250 case historiesfrom Scandinavian hospitals and concluded thatsurgery was unlikely to result in a remission ofsymptoms, but that patients should nonetheless beoffered a laminectomy and decompression.Other authors, notably Elsberg (1941), Rasmussen,
Kernohan, and Adson (1940), and Arseni, Simion-escu, and Horwath (1959), have emphasized thatmost cases of paresis or paralysis are not improvedby operation, and that when the compression isclearly caused by a malignant secondary depositsurgery should be directed at the relief of pain.Laminectomy and decompression should be con-sidered only as one of the methods which might beemployed to make the patient comfortable. Thegeneral acknowledgement of a poor prognosis in thiscondition has led to attempts to differentiate pre-operatively those patients who are likely to be helpedby operation from those who are not.
Barron, Hirano, Araki, and Terry (1959) triedto separate those patients who were not likely to behelped by surgery on the basis of the clinical pictureand the pathology of the primary. Reviewing 38cases, they concluded that operation is unlikely toprove valuable where the patient exhibits a flaccidparaplegia, where sensory loss is complete, wheretotal paraplegia has developed in less than 72 hours,or where the primary tumour is a carcinoma of thelung.A different point of view is put forward by Larson,
Wetzel, Brochner, and Ruge (1961), who reviewed23 cases, and concluded that although laminectomy
15:
does not improve most patients, it may arrest thecourse of the compression and preserve any remain-ing function.
It is understandable that this difference of opinionshould exist. Many reported series consist of arelatively small number of patients with widelyvarying types of primary tumour. Carcinomas,sarcomas, leukaemias and lymphomas, and myelo-mata are frequently considered together. The numberof individual cases of each type is not large, and thepart played by surgery in determining a successfulor unsuccessful outcome is difficult to assess. Inaddition, there is no general agreement as to whatconstitutes significant improvement following opera-tion. Some authors consider that a partial return ofmotor function, even though the patient remainsbedfast, is sufficient justification for the operation(Barron et al., 1959; Dinning, 1961; Larson et al.,1961). Others demand a return to independent ambu-lation.With these considerations in mind it was decided
to review cases of spinal cord compression due tocarcinoma submitted to operation at the LondonHospital. The study was limited to cases of metastaticcarcinoma, as the literature contains a number ofencouraging reports of the beneficial results oflaminectomy with or without radiation in cases ofmultiple myeloma (Svien, Price, and Bayrd, 1953;Clarke, 1956; Jacox and Kahn, 1933; McKissock,Bloom, and Chynn, 1961). Cases of Hodgkin'sdisease and lymphosarcoma have been shown torespond equally well either to surgical decompres-sion followed by radiation (Love, Miller, and Roer-nohan, 1954), or a combination of radiation andchemotherapy (Williams, Diamond, and Craver,1958).
Fifty-two cases (35 men and 17 women) of second-ary carcinoma were available for analysis. Histo-logical proof of malignancy was obtained in all,but full post-mortem examination was achieved inonly 10. Two patients are still living, 49 have died,and one was lost to follow-up. A tumour depositcorresponding to the level of the lesion was foundin 51 cases. The remaining patient died during the
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

An evaluation of surgical treatment for spinal cord compression due to metastatic carcinoma
induction of anaesthesia, and permission for nec- before the development of symptoms of spinal cordropsy was refused. compression, and eight of these presented with
Table I gives the site of the primary neoplasm secondary deposits at extraspinal sites. In an addi-responsible for the spinal cord compression. tional 14 cases, the presence of primary carcinoma
was discovered during the course of pre-operativeTABLE I investigation. In the remaining 22 cases, the nature
of the compressing tumour was unknown.PRIMARY SITES OF METASTATIC SPINAL DEPOSITS the clinica ictumrith major o tSiteNo.of Cases Site No.of Cases
The clinical picture in the majority of patientsSite No. of Cases Site No. of Cases was remarkably similar. Thirty-nine presented with
Lung 12 Thyroid 2 the complaint of radicular pain of increasing severityPresumed lung 16 Skin I followed in weeks or months by the development ofProstate 4 Breast 3Presumed prostate 3 Bladder 1 weakness, sphincter disturbance, and areas of sensoryStomach I Oesophagus 1 loss or paraesthesia below the level of the lesion. OfRectum I Pancreas 1*Kidney 2 Unknown
I
the 13 cases which might be considered atypical,five presented with paraesthesia and numbness,
Precise confirmation of the primary site was three with weakness, one with funicular pain, onepossible in 29 cases. Of the remaining 23, four were with a dull, aching back pain, and one case developedclassed as secondary carcinoma of unknown origin. radicular pain and weakness simultaneously. InThe remainder have been grouped according to the two cases radicular pain was the only complaint,presumed primary site, which was determined by the and no neurological abnormalities were found onhistological nature of the spinal tumour, x-ray examination. In all cases the symptoms were pro-examination, and the clinical appearance of the gressive.patient. On examination 50 patients were found to have a
combination of weakness and sensory loss. In 12,this took the form of cord transection with complete
TABLE IL paraplegia, incontinence, and a dense sensory lossSITE OF THE LESION IN RELATION TO THE SPINE below the level of the lesion. Nine patients had com-
Spinal Site No. of Cases Spinal Site No. of Cases plete motor loss but retained some appreciation ofsensation. In the remainder, neither weakness nor
Cervical 5 Thoraco-lumbar 1Cervico-thoracic 2 Lumbar 10 sensory loss was complete.Thoracic 33 Sacral 1 There was considerable variation in the duration
of symptoms before operation. It was generallyTable II shows the site of the lesion in relation to shorter in patients with a primary growth in the
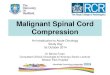
the spinal column. In seven cases the tumour in- lung. In these the mean duration of symptoms wasvolved the cord over four adjacent segments, in 11 weeks as compared with 23 weeks in the prostaticseven cases over three, and in eight cases over two. group and 13 weeks in the other tumours. Figure IIn the remainder the tumour deposit was found at a shows the individual cases from the onset ofsingle level. In 48 cases the deposit was extradural, symptoms until the time of operation. It can be seenin two cases it was intradural, and in one, in addition that seven of the 12 cord transactions became com-to a large extradural tumour involving bone, a plete in less than 72 hours. In one case this followedsmall intradural deposit was found. Thirty-three lumbar puncture. Similarly, two of the nine casescases had gross involvement of vertebral bodies at with complete paraplegia but incomplete sensory lossthe level of the lesion. became so in the same period of time.
In one patient a partially extruded intramedullary Twenty-three patients exhibited a flaccid type ofsecondary deposit from a bronchogenic primary weakness, and in 14 of these the site of the primarywas discovered at operation. At necropsy this patient tumour was the lung. In three, the primary waswas found to have developed carcinomatous menin- prostatic and the remaining seven were dividedgitis with spread of the tumour caudally along the between five primary sites. Seven of the patientssurface of the cord. Another example of intradural with flaccid weakness had no radicular pain, butmetastases proved to have diffuse involvement of complained of a dull aching back pain made worsethe cauda equina. With the exception of this case, by movement. Forty-six patients were generally fitwhere the diagnosis of carcinomatous meningitis at the time of operation. The remaining six werewas made before operation, surgery was undertaken described as wasted and ill-looking, and had de-in the hope of removing any tumour encountered veloped infected pressure sores.and decompressing the cord. Radiographs of the spine were obtained in all
Sixteen cases were known to have carcinoma cases, and myelography, by either the lumbar or
153
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

Roderick Smith
OPERATIONONSET of SYMPTOMS DEATH
I ~ ~~~~1i).. 1
I1 01©
LUNG
ILI3
I.I I2 0
0I I 00DI*
l I0L 100
UNKNOWN
STOMACH
RECTUM
KIDNEY
THYROID
BREAST 0(
BLADDEROESOPHAGZUS0
PANCREAS 0
I I
weeks
cisternal route or by a combination of both, wasperformed in 35. A block to the passage of conftastmedia was demonstrated in 33, and a filling derectin the remaining two. Collapse of one or morevertebral bodies at the site of the lesion was revealedin 14 cases.Post-mortem examination was obtained in 10
patients in this series. The majority of these died inhospital soon after operation, and this selectioncontains an obvious bias. On examination only one'case proved to have a solitary metastasis at the spinalsite. In the others the tumour had spread to at leastone additional site, and in three cases there waswidespread dissemination.As mentioned previously, one patient was sub-
mitted to operation in order to confirm the diagnosisof carcinomatous meningitis, which proved to becorrect. In the remaining 51, surgery was undertakenin the hope of effecting a regression of symptomsand signs and a return to useful activity. There weretwo operative deaths; one following the inductionof anaesthesia and the other during the operation.The record of the remaining 49 is summarized in
Table III.
TABLE IIIRESULTS OF LAMINECTOMY AND DECOMPRESSION WITH
REMOVAL OF THE SPINAL TUMOURLost to follow-upSurviving more than six weeksSurviving more than 20 weeksMinimally improved ..
Significantly improved ..
Made worse ..
Unchanged
..I32168137
.. 20
DISCUSSION
Assessment following operation showed that 21patients could be considered improved in that therewas some regression of symptoms and signs, but ineight of these this was minimal and consisted only ofan increased appreciation of sensation or the abilityto initiate weak voluntary movements of the pre-viously paralysed limbs. Thirteen were significantlyimproved, that is, they were restored to independentwalking with or without the aid of sticks or crutches.Comparison of the two groups revealed that none
FIG. 1. Individual cases of carcinomatous spinal cordcompression grouped according to the natureofthe primarytumour. Thepresence anddurationofparaplegia is indicatedby shading. Black shading represents a functional transec-tion of the cord while those cases with complete paraplegiabut an incomplete loss of the ability to perceive sensationare indicated by cross-hatching. A wedge-shaped mark indi-cates the onset of weakness. A cross within a circle denotesthose patients showing significant improvement.
154
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

An evaluation of surgical treatment for spinal cord compression due to metastatic carcinoma
of the 16 surviving less than six weeks made asignificant recovery and four were minimally im-proved. It is possible that these patients might havecontinued to improve had they not been harbouringa rapidly progressing carcinoma. Fisher (1963)states that the early return of sensory function follow-ing laminectomy indicates a good prognosis. It maybe that the debilitation and cachexia which ac-company the terminal stages of malignant diseaseproduce metabolic changes in the damaged cordinhibiting a return of function. Tarlov (1957) hasnoted how animals which had completely recoveredfrom experimental paraplegia could become para-lysed once again if suffering from severe systemicinfection or failing health. Alternatively, they weresimply overtaken by the primary disease beforesignificant recovery could take place. Whatever thereason, the only encouraging results were foundamong the 32 patients surviving longer than sixweeks; of these, 13 made a good recovery. Five ofthese, however, died within the next 14 weeks,leaving among the 16 long-term survivors, only eightwho could be described as significantly improved byoperation (Table IV).
Surgical intervention then was of little benefit tothe majority of patients included in this series, but itis useful to consider what factors may differentiatethose cases which were helped by operation fromthose which were not.
TABLE IVRESULTS OF LAMINECTOMY IN METASTATIC CARCINOMA
Minimal improvement. .. 8Significant improvement .. 13Significant improvement for more than20 weeks... 8
TABLE VRESULTS AS A FUNCTION OF THE CLINICAL PICTURE
Afinimal SignificantTotal Improve- Significant ImprovementCases ment Improvement >20 Weeks
Flaccid weakness 23Wasting and debilitation 6Total cord transection 12
(11 followed)Total cord transectiondeveloping in less than72 hr. 7Complete paraplegiawith some sensorysparing 9Complete paraplegiawith some sensorysparing developing inless than 72 hr. 2Collapse of vertebralbody at level of lesion 9Known carcinomabefore operation 26
4 4 31 2 12 1 1
2 1 1
Table V displays the results in 48 cases as a func-tion of factors which could be assessed pre-opera-atively and which have been reported to be ofprognostic value.
It is apparent that in patients with known car-cinoma before operation, or flaccid weakness, theincidence of improvement is approximately that ofthe series as a whole. The total number of cases ineach of the other groups is too small to permit anysignificant conclusions, but it should be noted thatneither severe wasting, total cord transectiondeveloping in less than 72 hours, nor collapse of avertebral body at the site of compression, pre-cluded a successful result. The level of the lesionin the spine did not apparently significantly influencethe outcome as the distribution of improved cases(Table VI) resembles the overall distributionshown in Table II.
TABLE VILEVEL OF THE
Level of Lesion
CervicalCervico-thoracicThoracicThoraco-lumbarLumbarSacralTotal
LESION IN CASES SHOWING IMPROVEMENTAFTER SURGERY
Minimal SignificantTotal Improve- Significant ImprovementCases ment Improvement >20 Weeks
5 1 - -2 2 1
33 4 10 71
10 1 2 -I I - -
52 8 13 8
More interesting, however, is a consideration ofthe results grouped according to the site of theprimary lesion (Table VII); the outstanding featureis that all the cases of carcinoma of the prostatewere significantly improved.
TABLE VIIRESULTS AS A FUNCTION OF THE PRIMARY SITE
Minimal SignificantTotal Improve- Significant Improvement
Site of Primary No. ment Improvement >20 Weeks
Carcinoma lungCarcinoma prostateCarcinoma site unknownCarcinoma thyroidCarcinoma breastCarcinoma kidneyCarcinoma stomach
2774222
5 4_ 7_ I
26
2
3 2 1
The number of cases of thyroid, breast, renal,and other tumours shown in Table VII are too smallto permit any significant conclusion, but the cases
1 1 - of lung and prostatic metastases can be considered6 6 5 further.
155
I
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

Roderick Smith
The results here confirm the unfavourable prog-nosis of metastases arising from bronchogenicprimaries. With two exceptions, surgical interven-tion in this group was of little value. Aside from thegood result, one of these was in no way unusual.The other presented with a six months' history ofslowly progressive cord compression and a shadowat the apex of the right lung. One week beforeoperation he became completely paraplegic follow-ing a lumbar puncture. Laminectomy and removalof the spinal tumour was followed by a course ofradiotherapy to both the spine and the rightpulmonary apex. Thoracotomy, four months afterthe laminectomy, revealed only a carcinomatouspleural nodule. The patient made a good functionalrecovery, and eventually died two and a half yearsafter the original operation. The duration of pre-operative symptoms in this case is more than twicethe mean and this, together with the apparent radio-sensitivity and peripheral location of the primary,may explain the good result.The other case illustrates the difficulty involved
in attempting to predict the eventual outcome in anyindividual patient. This man presented with ahistory of back pain and weakness for three months.Examination revealed a lesion at T5, and chestradiographs showed a hilar mass extending into theleft lower lobe. Following laminectomy and theremoval of an extradural carcinomatous deposit,he received a course of radiotherapy to the site ofthe spinal lesion but none to the primary. There wasa rapid return of function to the lower limbs and heremained well and active for the next 20 months,finally succumbing more than two years after theoperation from extension and dissemination of theprimary.
Thirteen other cases of carcinoma of the lung,with a similar clinical picture, were not helped byoperation, and it is difficult to decide why thispatient did so well. It may be significant that inboth cases cited above the duration of symptomspre-operatively exceeded the mean for the group.Tarlov (1957) has shown that experimental para-plegia caused by a gradual compression is potentiallyreversible for a longer period than when caused by anacute lesion. In addition the longer history suggests abiologically less aggressive primary than in thosecases where the period between the onset of symp-toms and death is only a matter of a few weeks.
TABLE VIIIRESULTS IN 20 CASES WITH A HISTORY OF PRE-OPERATIVE
SYMPTOMS OF EIGHT WEEKS OR LESS
Minimally improved . . ISignificantly improved .. 2Significantly improved for more than20 weeks... 0
In the case of lung primary, when patients showingany improvement after operation are grouped, it isseen that only one of these (case 14) had a pre-operative history of less than eight weeks. Excludingthis case, the mean for the others is 13 weeks, and itseems likely that it is in this group that any possiblysuccessful results may be expected. Conversely, ahistory of eight weeks or less seems to have a mostunfavourable prognosis (Table VIII). In this group,of 14 cases of carcinoma of the lung, 12 patientsshowed no improvement; one was minimally im-proved, but survived less than two weeks; and theother, while initially significantly improved, rapidlydeteriorated and died within seven weeks of opera-tion. Five other similar cases with metastases fromvarying primary sites were wholly unimproved. Thesingle case of prostatic carcinoma in this categorywas also significantly improved, but again the post-operative survival was relatively limited and thepatient died within 20 weeks. It appears that even inthis relatively more benign tumour a short historyindicates a poor prognosis.
Generally, however, the cases of prostatic metas-tases present a very favourable picture of the sevenpatients submitted to surgery. All were significantlyimproved. As mentioned, one succumbed within20 weeks, but this patient (42) was ill and wastedand had developed diffuse metastases before opera-tion. One patient (50) is still living and shows nosign of a recurrence of his paresis. The mean sur-vival in the remaining patients was 28 months, andall were ambulatory until a few months beforedeath. Marshall, Tavel, and Schulte (1962) havereported similarly good results in eight of 13 cases ofprostatic metastases followed post-operatively foran average of eight and a half months.The results obtained in these cases most probably
reflect the relatively benign nature of the primarytumour. Figure 1 shows that the progression ofsymptoms was more gradual. The mean intervalbetween the onset of symptoms and operation was23 weeks compared with 11 weeks in the lungtumours and 14 weeks in the others. In addition thepalliative measures generally employed in the treat-ment of incurable prostatic carcinoma can be em-ployed in conjunction with laminectomy and removalof the spinal deposit. The beneficial effects of orchi-dectomy and the administration of oestrogens arewell known (Goodwin, 1961), and spinal depositsmay respond to these measures. The remission ofcomplete paraplegia presumed to be caused byprostatic metastases has been reported following theadministration of oestrogens (Edelman, 1949),and more recently after adrenalectomy (Bowers,1962). In addition, prostatic carcinoma is frequentlyradiosensitive (Rusche and Jaffe, 1958; Flocks,
156
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

An evaluation of surgical treatment for spinal cord compression due to metastatic carcinoma
Culp, and Elkins, 1959), and the two patients withthe best results in this series received a course ofradiotherapy to the site of the spinal lesion followingoperation.
CONCLUSIONS
From the cases reviewed here, it appears that whilethe outlook for patients with carcinomatous cordcompression is bleak, it is not hopeless and that veryworthwhile results may sometimes be obtained bysurgical removal of the spinal deposit. For a numberof reasons, laminectomy and decompression withattempted removal of the tumour would appear to beadvisable in all but a minority of cases. In nearlyhalf the cases in this study the operation was neces-sary to establish a diagnosis and, as there was nodifference in the success rate in the two groups, thepresence of malignancy in a patient suffering fromspinal cord compression should not in itself justifya refusal to operate.The procedure is not hazardous and the operative
mortality, considering the nature of the disease,should be generally acceptable. While the majorityof patients were unimproved, the number showingmarked improvement was nearly twice the total ofthose made worse, and the fear of increasing thepatients' disability should not be considered asignificant contraindication.Another factor which does not in itself justify
surgery, but which may make the operation moreacceptable to the patient, is that where pain ispresent and severe it is frequently improved bylaminectomy and decompression.
Patients who are not likely to benefit, however,should be spared the stress of an operation. Inassessing these cases it appears that a short historyof progressive symptoms is the most reliable indica-tion of those who will do badly, and when this iscombined with other factors such as flaccid weakness,vertebral collapse, total paraplegia, long-standingparaplegia, or paraplegia of sudden onset, the chancesof recovery are very slight. In the absence of a shorthistory, however, the presence of one or more of theother factors should not be grounds for refusingoperation. The nature of the primary tumour is alsoundoubtedly very important in establishing theprognosis. In view of the good results reported hereand elsewhere in cases of prostatic metastases, itwould seem that surgery should be offered to all butterminal cases. In patients with carcinoma of thelung, the results of surgery are likely to be mostdisappointing, but the absence of any features whichclearly distinguish the rare cases, which both im-prove and survive, from the majority force the con-clusion that surgery is necessary in all cases except
those with a short history if the maximum number areto be helped. Other primary tumours are not re-presented here in sufficient numbers to permit anyfirm conclusion, but in the absence of any definiteevidence it would seem reasonable, as in carcinomaof the lung, to continue to offer operation to allexcept those with a short history of progressivesymptoms and signs.
Finally, although no attempt was made to assessthe effects of radiotherapy, it was apparent that manyof the patients showing significant improvement hadundoubtedly benefited from irradiation of the spinallesion, and it might be profitable if this were em-ployed following surgery whenever there is a sugges-tion that the tumour may be radiosensitive.
SUMMARY
A review of 48 cases of spinal cord compression dueto secondary carcinoma submitted to surgery at theLondon Hospital revealed 13 cases in which therewas significant improvement after operation. Of theremainder, eight were slightly improved, 20 un-changed, and seven made worse.Only 16 patients lived more than 20 weeks after
operation. Eight of these were from the group show-ing significant improvement.
In assessing the prognosis for an individual case,it appears that a short pre-operative history is themost reliable guide to those patients who will showno improvement. In the absence of such a history,signs such as complete paraplegia, long-standingparaplegia, paraplegia of sudden onset, flaccidweakness, vertebral collapse, or severe wasting donot present an insuperable barrier to recovery andshould not be grounds for refusing operation. Thepathology of the primary tumour is also most im-portant. All patients reported here with carcinomaof the prostate were significantly improved, andoperation is recommended in all but terminal cases.Conversely, of 28 cases of carcinoma of the lung onlyfour were significantly improved, but it appears tobe impossible to differentiate pre-operatively fromthe majority the rare case which will improve.Laminectomy and decompression, with attempted
removal of the spinal tumour, is recommended in allcases of spinal cord compression due to secondarycarcinoma, except those with a short history ofprogressive symptoms and signs.
I wish to express my gratitude to Dr. R. A. Henson andMr. D. W. C. Northfield, both for their advice and forpermission to examine their patients.
REFERENCES
Arseni, C. N., Simionescu, M. D., and Horwath, L. (1959). Ttimors ofthe spine. Acta psychiat. scand., 34, 398-410.
157
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from

Roderick Smith
Barron, K. D., Hirano, A., Araki, S., and Terry, R. D. (1959).Experiences with metastatic neoplasms involving the spinalcord. Neurology (Minneap.), 9, 91-106.
Bowers, R. F. (1962). Adrenalectomy for hopeless carcinoma of theprostate. Arch. Surg., 84, 421-424.
Clarke, E. (1956). Spinal cord involvement in multiple myelomatosis.Brain, 79, 332-348.
Dinning, T. (1961). Malignant spinal extradural tumours. Aust. N.Z.J. Surg., 31, 126-133.
Edelman, I. S. (1949). Paraplegia secondary to metastatic prostaticcarcinoma treated with stilbestrol. Ann. intern. Med., 31, 1098.
Elsberg, C. A. (1941). Surgical Diseases ofthe Spinal Cord, Membranes,and Nerve Roots. Hoeber, New York.
Fisher, A. (1963). Observations on the prognostic signs followingrelief of spinal cord compression. Proc. Aust Assn. Neurol., 1,
31-34.Flocks, R. H., Culp, D. A., and Elkins, H. B. (1959). Present status of
radioactive gold therapy in management of prostatic cancer.J. Urol. (Baltimore), 81, 178-184.
General Register Office (1964). Registrar General's statistical reviewof England and Wales for the year 1962. Part 1. Tables, Medi-cal. H.M.S.O., London.
Goodwin, W. E. (1961). Current concepts concerning treatment ofcancer of the prostate gland. In Proc. 4th nat. Cancer Confer-ance, University of Minnesota, 1960, pp. 495-99. Lippincott,Philadelphia.
Jacox, H. W., and Kahn, E. A. (1933). Multiple myeloma with spinalcord involvement. Amer. J. Roentgenol., 30, 201.
Larson, S., Wetzel, N., Brochner, R., and Ruge, D. (1961). The surgicaltreatment of metastatic epidural tumors. Quart. Bull Northw.Univ. med. Sch., 35, 4244.
Love, J. G., Miller, R. H., and Roernohan, J. W. (1954). Lymphomasof spinal epidural space. Arch. Surg., 69, 66-76.
McKissock, W., Bloom, W. H., and Chynn, K. Y. (1961). Spinal cordcompression caused by plasma-cell tumours. J. Neurosurg.,18, 68-73.
Marshall, S., Tavel, F. R., and Schulte, J. W. (1962). Spinal cord com-pression secondary to metastatic carcinoma of the prostatetreated by decompressive laminectomy. J. Urol. (Baltimore),88, 667-673.
Perese, D. M. (1958). Treatment of metastatic extradural spinal cordtumors; a series of 30 cases. Cancer (Philad.), 11, 214-221.
Rasmussen, T. B., Kernohan, J. W., and Adson, A. W. (1940).Pathologic classification, with surgical consideration, of intra-spinal tumors. Ann. Surg., 111, 513-530.
Rogers, L. (1958). Malignant spinal tumours and the epidural space.Brit. J. Surg., 45, 416-422.
Rusche, C. F., and Jaffe, H. L. (1958). Treatment of bladder and pros-tatic cancer by combined interstitial isotope radiation and thecobalt bomb. J. Urol. (Baltimore), 79, 474-489.
Svien, H. J., Price, R. D., and Bayrd, E. D. (1953). Neurosurgicaltreatment of compression of the spinal cord caused by mye-loma. J. Amer. med. Ass., 153,784-786.
Torma, T. (1957). Malignant tumours of the spine and the spinalextradural space; a study based on 250 histologically verifiedcases. Acta chir. scand., suppl. 225 pp.
Tarlov, L. M. (1957). Spinal Cord Compression. Thomas, Springfield,Illinois.
Williams, H. M., Diamond, H. D., and Craver, L. F. (1958). Thepathogenesis and management of neurological complications inpatients with malignant lymphomas and leukemia. Cancer(Philad.), 11, 76-82.
158
Protected by copyright.
on Decem
ber 6, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.28.2.152 on 1 A
pril 1965. Dow
nloaded from



![SciForschen ISSN 2379-7150 · CNS tumors [11]. Neurosurgical approach Surgical intervention for spinal cord ependymomas remains the mainstay treatment option. Due to spinal cord compression](https://img.pdfslide.us/doc/110x75/5f0d49097e708231d43996e0/sciforschen-issn-2379-7150-cns-tumors-11-neurosurgical-approach-surgical-intervention.jpg)