Embed Size (px)
Citation preview
An enduring contributionThe RACGP’s 2016 Rose-Hunt Award winner John Litt has left an indelible mark on healthcare delivery in Australia
www.racgp.org.au/goodpractice
INSIDE
Award winnersThe best of general practice for 2016
NutritionThe productive relationship between GPs and dietitians
Specific interestsIntegrative medicine in general practice
ISSUE 10, OCTOBER 2016
3902_BP_MALE_MASTERCLASS_GP_210X275.indd 1 7/09/2016 2:37 pm
Good Practice is printed on PEFC certified paper, meaning that it originates from forests that are managed sustainably. PEFC is the Programme for the Endorsement of Forest Certification schemes. PEFC is an international certification programme promoting sustainable forest management which assures consumers that a forest product can be tracked from a certified, managed forest through all steps of processing and production in the supply chain by a Chain of Custody process.
3Reprinted from Good Practice Issue 10, October 2016
Editorial notes
© The Royal Australian College of General Practitioners 2016. Unless otherwise indicated, copyright of all images is vested in the RACGP. Requests for permission to reprint articles must be made to the editor. The views contained herein are not necessarily the views of the RACGP, its council, its members or its staff. The content of any advertising or promotional material contained within Good Practice is not necessarily endorsed by the publisher.
We recognise the traditional custodians of the land and sea on which we work and live.
12
18
ContentsIssue 10, October 2016
10
06
16
04 Your College
RACGP news and events for October.
06 Rose-Hunt
Prevention in practice Associate Professor John Litt has
always strived to create a framework for providing patients with the best
possible care.
10 GP of the Year
State of the heart No matter where medical training
took her, Tasmania’s Dr Jane Cooper was always destined to ply her trade
at home.
12 General Practice Supervisor of the Year
Sharing knowledge Medical educator Dr Rohan Gay wants
to pass on what he has learned and contribute to general practice knowledge
in Australia.
14 General Practice Registrar of the Year
Hometown roots Dr Chris Hughes is passionate about
rural general practice and serving his community.
16 Rural Registrar of the Year Challenge accepted
Dr Fintan Andrews thrives on the demands and conditions of
rural general practice.
18 General Practice of the Year Community service The staff members at Ararat Medical Centre work hard to meet the needs of patients, students and employees.
20 Honorary Fellowship Mind the gaps Dr Jill Benson has spent much of her career working to fill knowledge gaps in general practice and beyond.
22 Conference for General Practice Full list of GP16 award winners.
23 General Practice Management Toolkit Managing the wellbeing of staff and self Providing GPs with the skills to better look after themselves and their practice teams.
24 Nutrition Working with dietitians The relationship between GPs and Accredited Practising Dietitians.
26 RACGP Specific Interests Integrative medicine Navigating complementary medicines by assessing and disseminating the latest evidence.
Published by
The Royal Australian College of General Practitioners 100 Wellington Parade East Melbourne Victoria 3002
T 03 8699 0414 E [email protected] W www.racgp.org.au/goodpractice
ABN 34 000 223 807 ISSN 1837-7769
Editor: Paul HayesJournalist: Amanda LyonsGraphic Designer: Frances StandenProduction Coordinator: Beverley GutierrezPublications Manager: Jenni Stiffe
Advertising enquiriesSye Hughes:T 0474 500 770E s y e . h u g h e s @ r a c g p . o r g . a u
4 Reprinted from Good Practice Issue 10, October 2016
Imag
es R
AC
GP
YOUR COLLEGE
Updated resources
The RACGP’s recent Conference for General Practice, GP16, was home to presentations and updates of a number of key RACGP resources.
Federal Health Minister Sussan Ley addressed conference delegates, discussing the launch of the Federal Government’s Health Care Home pilots. These pilots, which are designed to allow better care provision for patients with chronic disease and complex comorbidities, share many similarities with the medical home concept at the heart of the RACGP’s Vision for general practice and a sustainable healthcare system funding model. Their introduction and progress are of strong interest to the RACGP and its members.
GP16 was also the setting for the release of the 9th edition of the RACGP’s Guidelines for preventive activities in general practice (Red Book). The updated edition explores a number of topics, including the impact of new technologies on preventive practice, issues in primary care screening activities for conditions such as cancer and cardiovascular disease, and advice for GPs in dealing with health inequality.
The RACGP’s General practice management of type 2 diabetes has also been updated and will be available this month. The 2016–18 edition includes expanded sections concerning practice guidelines on clinical assessment, management of diabetes
glycaemic emergencies, and several other relevant topics. The updated guide also incorporates important new evidence and subsequent revisions to clinical practice.
The General Practice Mental Health Standards Collaboration (GPMHSC), a GP16 gold sponsor, released its new Mental health training standards for 2017–19, which will take effect on 1 January 2017. These standards are available as two separate resources – a guide for GPs and a guide for training providers.
The GPMHSC has also released two new resources on suicide prevention, designed to assist GPs in providing care for patients and communities dealing with suicide.
Mental health trainingstandards 2017–19A guide for general practitioners
Mental health trainingstandards 2017–19A guide for training providers
5Reprinted from Good Practice Issue 10, October 2016
RACGP events calendar
October 2016
VIC
Perform CPR – A workshop for GPsTuesday 11 October, 6.00–8.00 pm, RACGP House, East Melbourne
Contact 03 8699 0488 or [email protected]
NSW
Clinical Emergency Management Program – AdvancedSaturday to Sunday 15–16 October, 8.30 am – 5.00 pm, Sydney Boulevard Hotel
Contact 02 9886 4710 or [email protected]
WA
CPR certification courseThursday 13 October, 6.30–8.30 pm, College House, Perth
Contact 08 9489 9555 or [email protected]
WA
Grand round series 2016 – Session 3Wednesday 19 October, 6.30–9.00 pm, College House, Perth
Contact 08 9489 9555 or [email protected]
NSW
Clinical Emergency Management Program – IntermediateFriday 14 October, 8.30 am – 5.00 pm, Sydney Boulevard Hotel
Contact 02 9886 4710 or [email protected]
SA
Fellowship and Awards CeremonySunday 23 October, 2.00–6.00 pm (arrivals from 1.00 pm), Adelaide Oval
Contact 08 8267 8310 or [email protected]
VIC
Psychodynamic principles workshop for GPs (part 1)Saturday 15 October, 9.00 am – 5.00 pm, RACGP House, East Melbourne
Contact 03 8699 0488 or [email protected]
NSW
Skin cancer essentialsSaturday 29 October, 8.30 am – 4.45 pm, Royal North Shore Hospital, St Leonards
Contact 02 9886 4736 or [email protected]
TAS
Perinatal in practice: Managing perinatal mood disordersSaturday 15 October, 8.45 am – 5.00 pm, Ulverstone
Contact 03 6234 2200 or [email protected]
WA
Procedures in the practiceSaturday 29 October, 8.30 am – 4.00 pm, College House, Perth
Contact 08 9489 9555 or [email protected]
QLD
Fellowship and Awards CeremonySaturday 15 October, 3.00–5.00 pm (guests seated at 2.30 pm), Brisbane Convention and Exhibition Centre
Contact 07 3456 8930 or [email protected]
QLD
Psychodynamic principles for GPs (Part 1) Saturday 29 October, 8.45 am – 5.00 pm, The Ville, Townsville
Contact 07 3456 8930 or [email protected]
Visit www.racgp.org.au/education/courses/racgpevents for further RACGP events.
competition
Five RACGP student members were winners of the recent GP16 photo competition, which asked entrants to ‘show how you embrace the digital age in your studies or daily general practice’. Each winner received full delegate registration for GP16, four nights’ accommodation and return airfare to Perth, valued at up to $2990.
The GP16 photo competition winners were:• Zach Dawes (Queensland) • Jazmin Daniells (New South Wales) • Joanne Mackson (New South Wales) • John Mauder (Queensland) • Sebastian Kirby (Victoria)Visit the RACGP Facebook page to access a gallery of the winning entries for the GP16 photo competition.
Dementia guidelinesThe RACGP has endorsed the National Health and Medical Research Council’s (NHMRC) Clinical practice guidelines and principles for people with dementia, recognising the condition as a national health priority.
‘One in 10 older Australians has a diagnosis of dementia and it is absolutely vital to improve the quality and consistency of care for people with declining cognition,’ RACGP Immediate Past President Dr Frank R Jones said.
‘Dementia has an enormous impact on the lives of the carers and their families, as well as those people diagnosed with the disease.
‘The cost of dementia on the health and aged care systems in Australia is staggering and calculated at more than $4.9 billion per annum.’
The new NHMRC guidelines include 109 recommendations that reflect current evidence regarding dementia care. These recommendations are designed to help GPs and other healthcare professionals better respond to the needs and preferences of people living with dementia, and their carers and families.
‘The guidelines will help address timely diagnosis and provide support for carers, living well with dementia, pharmacological and non-pharmacological management of symptoms, and end-of-life care,’ Dr Jones said.
Imag
e Jo
hn L
itt
6 Reprinted from Good Practice Issue 10, October 2016
Prevention in practice
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AW
PAUL HAYES
Associate Professor John Litt has always strived to create a framework for providing patients with the best possible care.
When reflecting on the general practice career of South Australia’s Assoc Prof John Litt, one of the most oft-repeated healthcare adages comes to mind: prevention is better than cure.
Assoc Prof Litt has had a sustained interested in prevention for more than 35 years. As one of the driving forces behind many of the RACGP’s guidelines in areas such as smoking cessation, immunisation, disease prevention, abuse and violence, and men’s health, he has spent a significant amount of his career working to help improve patient outcomes by assisting GPs in their implementation of a range of clinical and prevention activities.
‘I would hope that we have made an impact by having people look at prevention more seriously,’ he told Good Practice.
While a contributor to many other guidelines, Assoc Prof Litt was most deeply involved in the development of the RACGP’s Putting prevention into practice: Guidelines for the implementation of prevention in the general practice setting (Green Book), which was first published in 1996. The Green Book offers GPs a framework and a variety of effective strategies to improve the delivery of prevention activities.
‘We know what to do, but we don’t necessarily know the best way of doing it,’
Assoc Prof John Litt’s work throughout general practice has been dedicated to improving patient outcomes and helping GPs better implement clinical and prevention activities.

7Reprinted from Good Practice Issue 10, October 2016
Assoc Prof Litt said. ‘The Green Book largely was what was known best practice and what framework would assist people to deliver that.’
Material for the current edition of the Green Book was largely drawn from Assoc Prof Litt’s PhD in the area of prevention.
‘My PhD was far too long [nearly 1000 pages] and dry, so hopefully the Green Book was something more readable for GPs and practice nurses. It is a cut-down guide,’ he said. ‘That second edition came out in 2006 and plans for a new edition are underway.’
This kind of effort, designed to help all patients and the broader healthcare system across Australia, has played a major role in Assoc Prof Litt winning a number of awards throughout his career, including this year’s Rose-Hunt Award, the highest accolade the RACGP bestows on any of its members (refer to breakout on page 8 for more information).
Jack of many tradesAssoc Prof Litt has an extensive education and academic background, having undertaken general practice training in Australia and overseas. He holds diplomas in obstetrics and gynaecology, a master’s degree in clinical epidemiology, and fellowships in general practice and public health medicine in addition to his PhD.
Assoc Prof Litt graduated from his medical studies at the University of Adelaide in 1978 and commenced general practice training in Australia. This was followed by more training in Canada, where he became a junior faculty member in the Department of Family Medicine at McMaster University in Ontario.
‘I enjoyed the training in public health that I did while working in the McMaster University Family Practice,’ he said. ‘It helped me to integrate my long-term interest in prevention with population health.’
Assoc Prof Litt later returned to Adelaide and joined Flinders University’s Discipline of Primary Care and Community Medicine (later the Department of General Practice) in 1987, where he remained until his retirement at the beginning of 2016.
‘My day job was the Associate Professor in General Practice and I was the General Practice Teaching Coordinator,’ he said.
Assoc Prof Litt’s time as General Practice Teaching Coordinator allowed him the chance to further the educational opportunities for students involved in his chosen medical specialty.
‘That role meant ensuring that general practice, and the whole repertoire of
associated skills, was visible in the curriculum,’ he said. ‘With the assistance of the Foundation Chair in Primary Care, Anthony Radford, and other GPs Deane Southgate, Andrew Ramsay, Geoff Stranks and Louis Pilotto, we managed to get a lot of things introduced [to the Flinders University curriculum].
‘We are now talking to medical students about how to assess domestic violence, men’s health, high-level communication and counselling skills, and the value of continuity of care, especially when managing patients with complex care needs.’
Assoc Prof Litt’s contribution to the Flinders University Medical School was recognised in 2014 when he was awarded a Dean’s Award for outstanding service to the school over an extended period.
Working for the communityWhile much of his work falls under the umbrella of ‘prevention’, there are a number of specific areas in which Assoc Prof Litt has made major impacts on healthcare delivery.
It is very satisfying to know that some other people think that you have actually made a difference
In particular, his work has led to significant strides in immunisation, especially among people aged 65 and older.
‘Kids’ immunisation, quite legitimately, gets a lot of airtime, but adult diseases like influenza and pneumococcal and, more recently, shingles actually have a large burden of vaccine-preventable illness [VPIs],’ he said. ‘I conducted the first national influenza and pneumococcal survey in Australian about 16 years ago and followed that up about five years ago with the Australian Zoster Study.
‘Both surveys asked older patients and their GPs about their understanding of these conditions and what they thought about getting immunised.’
These efforts to increase immunisation among older people bore significant fruit in the early 1990s when Assoc Prof Litt and a public health colleague, Dr Peter Lake, helped to establish the South Australian Influenza Advisory Group following a flu scare.
‘We started that to try to promote better influenza vaccine uptake among at-risk groups,’ he said. ‘All of the bigger companies
had encouraged their employees to get the flu vaccine and, as a consequence, a lot of older people and people with chronic illness missed out on getting it as there wasn’t enough available.
‘We got key stakeholders involved – pharmacists, public health people, practice nurses, nursing homes, local government – and discussed strategies to improve coverage.
‘In 1993, 29% of people older than 65 had a flu shot. In recent times, we have managed to get coverage levels of over 80%.’
Assoc Prof Litt’s interest in counselling has also allowed him to offer his considerable expertise to help GPs in their daily practice.
‘There are two areas of counselling that have probably been most notable within the RACGP,’ he said.
‘They are motivational interviewing, in terms of providing skills for GPs and registrars to assist patients making health-related behaviour changes, and upskilling clinicians in assessing and managing domestic violence and patients who smoke.’
After attending an early workshop with the primary authors of the RACGP’s Abuse and violence: Working with our patients in general practice (White Book) – Dr Libby Hindmarsh and Prof Kelsey Hegarty – Assoc Prof Litt suggested the subject of bullying would be an appropriate addition.
‘Including a chapter on bullying was important because it is so pervasive in the community,’ he said. ‘Parents with children are well aware of cyber bullying and its consequences, but are not necessarily confident in how to tackle it.
‘We thought it was really useful for GPs to know about bullying and be able to recognise when it is occurring in a range of settings, including within the family.
‘Delineating the boundary between the normal rough-and-tumble in a family and persistent bullying by either siblings or parents can be challenging. GPs have access to families and have an opportunity to have a look and see what’s happening when children present with a range of problems that may be related to bullying.’
Assoc Prof Litt has also served as Deputy Chair of the RACGP Expert Committee – Quality Care (REC–QC) (formerly the National Standing Committee on Quality Care) since 2000. This role has included working on a number of guidelines and position statements, particularly Guidelines for preventive activities in general practice (Red Book), which has just released its 9th edition. >>

Imag
e Jo
hn L
itt
8 Reprinted from Good Practice Issue 10, October 2016
>> Assoc Prof Litt believes guidelines such as these also present an important opportunity for GPs to assess the treatment areas that are not necessarily of benefit, or where the evidence suggests not implementing some aspects of prevention is a better course of action.
‘One of the chapters I instigated [in the Red Book] was on the indeterminate and unproven screening tests,’ he said.
‘Everyone wanted to know what works, but I think we’d all agree you also want to know what doesn’t work, or where the evidence is unclear. It can save the GP some time by not having to offer screening strategies that don’t improve the health and wellbeing of the patient.’
Self-reflectionAssoc Prof Litt understands the value of general practice research, having undertaken a considerable amount throughout his career.
‘I think there are still a lot of things in medicine that are not known,’ he said.
Assoc Prof Litt also believes in the power of healthcare professionals’ involvement in research, especially in asking questions about how they deliver care and what they could potentially be doing better.
‘Better quality of care requires that you have an understanding of the denominator in order to measure how well you are
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AWA
RD
RO
SE-H
UN
T AW
AR
D R
OSE
-HU
NT
AW
Assoc Prof Litt is ‘humbled’ by the Rose-Hunt Award and happy to know that so many of his colleagues feel his work has made a difference.
doing,’ he said. ‘GPs often report that they use best practice guidelines with all of their patients, but until we measure their performance using some objective criteria
like patient surveys or clinical audit, we don’t really know how well they are doing.
‘Audit is a very simple way to do it. It’s not technically research, but it actually makes you think about asking a clinical question that is important. For example, am I doing well with my patients with diabetes? Do I have all of the kids in my practice up to date with vaccination?
‘So you have to reflect on what you are doing and I think that is an essential skill for all clinicians: to be able to ask themselves, am I doing this well? And do I have some objective evidence that I am doing it well?
‘Self-reflection is a core skill of a healthcare professional and audit is one way of assisting this process in a systematised way. I think it helps to renew the profession and encourages you to make sure you are doing the best you possibly can.’
Being named the Rose-Hunt Award winner for 2016 – the year of his retirement – has allowed Assoc Prof Litt an opportunity for a new level of self-reflection, one that encompasses an entire career.
‘I am really humbled and chuffed to receive the Rose-Hunt Award. It is very satisfying to know that some other people think that you have actually made a difference,’ he said.
‘When you retire you start to reflect on whether you have spent your time productively. It can be a challenging question to answer.’
‘To actually have someone say they think you have made a difference gives you a warm inner-glow. I have a real sense of privilege to have worked alongside many inspirational GPs like Mark Harris, Libby Hindmarsh and Kelsey Hegarty, not to mention the varied and dynamic chairs of the [REC–QC] and its predecessor, the Prevention and Community Medicine Committee, including Brian Kable, Barb Jones, Paul Mercer, Shiong Tan, Ron Tomlins and Evan Ackermann.
‘I look at the people who have received the Rose-Hunt Award in the past and I stand in awe and admiration. There have been many outstanding recipients and it is very gratifying to be able to be included in a group like that.’
The Rose-Hunt Award
The Rose-Hunt Award is the RACGP’s highest accolade.
The award was a gift to the RACGP from the UK’s Royal College of General Practitioners (RCGP) in commemoration of two of the RCGP’s founding members, Dr Fraser Rose and Lord Hunt of Fawley (the first Honorary Secretary).
The Rose-Hunt Award is given to an RACGP Fellow or member who, in the opinion of Council, has rendered outstanding service in the promotion of the objects of the RACGP by individual patient care, organisation, education, research or any other means.
Outstanding service may be over a period of 10 years or a substantial and significant contribution to general practice over a shorter period.
The inaugural Rose-Hunt Award was presented to one of the RACGP’s founding fathers, Dr William Arnold Conolly, in October 1974.
The NEW edition of the Red Book is out now.
Visit racgp.org.au/redbook

Imag
es J
ane
Coo
per
10 Reprinted from Good Practice Issue 10, October 2016
PAUL HAYES
No matter where medical training took her, Tasmania’s Dr Jane Cooper always seemed destined to ply her trade at home.
GP
OF
THE
YEA
R G
P O
F TH
E YE
AR
GP
OF
THE
YEA
R G
P O
F TH
E YE
AR
GP
OF
THE
YEA
R G
P O
F TH
E YE
AR
GP
OF
THE
YEA
R G
P O
F TH
E YE
AR
GP
OF
THE
YEA
R G
P O
F TH
E
State of the heart
Many rural GPs throughout Australia grew up outside of the major cities, and more still love the rural way of life. For Dr Jane Cooper, a GP in the north-west of Tasmania and the RACGP’s 2016 GP of the Year, life as a rural healthcare professional is more personal.
‘I am currently living in Devonport and I actually grew up and went to school here,’ she told Good Practice.
Dr Cooper’s love of general practice was also first kindled in Devonport, where her mother worked as a practice manager.
‘When I was at university I would do some weekend reception work and support one of the older GPs,’ she said. ‘He was a traditional, old-school GP and I feel really lucky to have worked with him.’
Pathway to homeAfter completing her primary and high school career in Devonport, Dr Cooper undertook her medical degree at the University of Tasmania in Hobart. Keen to roll up her sleeves and get started in some
practical medicine, Dr Cooper soon decided on her career path.
‘I probably had interest at that stage around rural health, because I had grown up in the country, and moved back up to Burnie [approximately 45 km from Devonport] and did my internship resident year at the Northwest Regional Hospital,’ she said. ‘That was very hands-on and that’s why I chose to do it: to get in and start learning and doing things.’
Confident in the idea that she wanted to follow a rural healthcare route, Dr Cooper ultimately made the move to the mainland.
‘I thought that I wanted to take a rural pathway of some sort, but this was prior to the advanced skills and some of the rural training that the RACGP now has,’ she said.
‘So I chose pathways to rural centres like Tamworth [New South Wales] and Toowoomba [Queensland].’
Dr Cooper undertook training in some advanced skills before returning to rural medicine back in Tasmania.

11Reprinted from Good Practice Issue 10, October 2016
‘I came home and did some general practice in Sheffield, Railton and Spreyton [all near Devonport],’ she said.
‘There was a clinic that had three components and you could work in those three practices. That was very rural and it was really good.’
While Dr Cooper also spent time in Katherine, in the Northern Territory, where she did a hospital term as a resident and undertook some fly-in fly-out services, she was soon back in her home state.
‘After these experiences I came back home and settled down and worked in most of the practices in the area,’ she said. ‘Right now I am here in Devonport.
‘I have been here for nearly 20 years and I have a very loyal patient base. They are just a lovely bunch of patients, and I am now looking after the children of the children who I have looked after.
‘That’s really exciting.’
Youth servicesDr Cooper currently works at Don Medical Clinic, which she originally started by herself – ‘in a one-room practice with just me and a laptop’ – at Don College in 2013 after she spoke with two local social workers in Devonport and realised there was a need for a better level of services for the town’s young people.
‘They both impressed upon me the lack of youth-friendly practices and youth-friendly GPs, that it was hard to get young people in to see the doctor and sometimes the
Having grown up in the north-west Tasmanian town of Devonport, Dr Jane Cooper is happy to now be practising medicine and raising her own family there.
environments weren’t conducive to young people feeling comfortable,’ Dr Cooper said.
One of those social workers was a staff member of Don College, which is home to students in years 11 and 12, who suggested Dr Cooper set up a clinic in an available room on the campus. Seeing an opportunity to provide some much-needed healthcare services to young people, Dr Cooper’s well established local roots helped get the practice up and running.
‘When you’re in a small town you often know a lot of people, which really helps when you are going to do something a little bit different,’ she said. ‘The principal of Don College, John Thompson, and I went to school together.
‘He was really keen to have an on-campus health service that would complement what he had already established as a whole-school focus, which included a police officer, a social worker, a youth worker and a chaplain, along with all of the teaching staff.
‘Having a GP on campus would really support that. That’s how Don Medical Clinic started.’
I have been here for 20 years ... and I am now looking after the children of the children I have treated
While the youth-focused clinic was an immediate success, the financial realities of operating a single-doctor bulk-billing service for young people soon became apparent.
‘Here I was, doing this fairly special work and providing a need for the community, but I wasn’t getting access to practice incentive payments or any of those sorts of things,’ Dr Cooper said.
With those more ‘traditional’ avenues for funding largely inaccessible, Dr Cooper was forced to look outside the box for some additional support. A fund for social determinants projects established by the previous Labor Government provided an opportunity for Dr Cooper to work with others in her local community.
‘I met a lot of the same people I work with in the youth sector within Devonport and I thought, if we all got together and collaborated on a project we would be successful in getting this money – it was $300,000 for the Devonport community – and we were successful,’ she said.
‘From that, we were able to establish the Hub Program, which involved me as a GP, Don College had a representative, Wise Employment Agency had a person involved, Youth and Family Community Connections, an NGO [non-government organisation], had a person involved, and we had a person from the council.
‘This was one opportunity where I was able to experience collaborating within the community and set up a program where we were all very much linked and supporting each other. It’s been really exciting.
‘Once I set up the on-campus clinic, I got to liaise with the teachers to see what the issues [affecting young people] were. We have had people self-referring to the clinic, teachers referring, social workers referring, parents referring.
‘It’s been very much accepted as a place to go with hopefully not too much stigma.’
Dr Cooper’s work with young people in Devonport has extended outside of the walls of Don Medical Clinic – which has now expanded to include a mainstream three-doctor practice in the centre of town – and elsewhere through the local community.
‘The other thing I did after opening the clinic is work with the headspace team on ways to establish headspace in Devonport. A satellite service has since been established, with the main practice based in Launceston,’ Dr Cooper said.
‘This community, which had very limited health services, currently has a very well-established network of people who are very passionate about young people’s health and wellbeing.’
While she has accomplished so much for the health of those in her hometown, especially its young people, Dr Cooper understands there is always more to be done. And being named the RACGP’s 2016 GP of the Year only strengthens that resolve.
‘It makes me really proud to be a GP and it really provides me with some very positive feedback that some of the work I do has been acknowledged,’ she said.
‘I have worked a little bit beyond what I needed to do, but I am extremely passionate about young people’s health and, for me, this is an opportunity to put young people’s health on that national radar and that’s really, really exciting.
‘When I was notified that I had won the award, that was my first thought: this is our next step to putting young people’s needs on the map.’
Imag
es W
AG
PE
T
12 Reprinted from Good Practice Issue 10, October 2016
Knowledge sharing
SUPE
RV
ISO
R O
F TH
E YE
AR
SU
PER
VIS
OR
OF
THE
YEA
R S
UPE
RV
ISO
R O
F TH
E YE
AR
SU
PER
VIS
OR
OF
THE
YEA
R S
UPE
RV
ISO
R O
F TH
E YE
AR
SU
PER
VIS
OR
OF
THE
YEA
R S
UP
Dr Rohan Gay has trained registrars for 14 years and believes education also helps lift the standards of supervisors and their practice.
AMANDA LYONS
Medical educator Dr Rohan Gay wants to pass on what he has learned and contribute to general practice knowledge in Australia.
Western Australia’s Dr Rohan Gay, recipient of the RACGP’s 2016 General Practice Supervisor of the Year Award, has a long and eventful history in general practice education.
‘I’ve been an examiner for the RACGP since 2005 and a QA [quality assurance] examiner since 2012,’ he told Good Practice. ‘And we [Walter Road East General Practitioners] were awarded WAGPET [Western Australian General Practice Education and Training] Training Practice of the Year in 2007 and 2015.’
Dr Gay tutored for the University of Western Australia from 2009–12, has run WAGPET education sessions on dermatology and diabetes, and been an
external clinical teacher since 2003. He has worked as a general practice supervisor for 14 years and is currently training his 24th and 25th registrars.
It was Dr Gay’s own medical learning process that initially inspired him to become a teacher himself.
‘Anyone who goes into general practice training soon realises there’s a lot more to it than they’ve been led to believe from their experiences in hospital,’ he said.
‘Despite the training program, there’s a lot of self-discovery along the way. I think, generally, after about five to 10 years – probably more towards 10 years – you start feeling you’ve got a handle on being a GP. Then you feel ready to pass it on and save other people the trouble.’
Dr Gay sees teaching as an opportunity to cast a broader influence over medical practice.
As a supervisor, if you’re doing something well and you want it to spread beyond your practice, you have the opportunity to teach other people ... a little bit of you goes out with every registrar
‘Once you’ve developed your own systems and explored what does and doesn’t work, you want to pass it on, particularly if you feel you’re doing well in certain areas,’ he said.
‘It’s your way of contributing to how medicine is practised in the country.’
Traditional and digitalDr Gay completed his own general practice education training in Sydney in the mid-1990s.

13Reprinted from Good Practice Issue 10, October 2016
‘It was the height of the medical centre boom in New South Wales and I think the state was “over-doctored” then,’ he said.
Seeking a return to a more ‘traditional’ form of general practice, Dr Gay moved to Perth and has now been based there for more than 20 years. There was one area of general practice, however, in which he wanted to avoid traditionalism – the use of computers.
‘When I came over [to Perth], the practice I was in had a mixture of A5 index cards and A4 paper records,’ he said.
Dr Gay has since seen a lot of change involving the increasing functionality of medical software, from generating scripts right through to collecting patient health data on pathologies, weight and blood pressure.
‘I think now is a time where information technology has allowed general practice to really come into its own, if you’re conscientious about it,’ Dr Gay said.
Information technology now assists in the monitoring of patients with chronic disease within Dr Gay’s own practice.
‘[This has resulted in] an integrated, systematic approach to chronic disease management which optimises use of practice staff, practice nurses and recall systems, and makes the job of administering chronic disease management easier,’ he said.
This interest in and implementation of computers in general practice has led Dr Gay to a position as a clinical adviser to the National eHealth Transition Authority (NEHTA), and also to its successor, the Australian Digital Health Agency (ADHA), since 2015.
Teaching tools Dr Gay is proactive in his approach to teaching, using his own experience as a practising GP and supervisor to help anticipate which skills and knowledge he needs to impart to general practice registrars.
‘It’s good to have some formal session plans for conditions and presentations you’re worried about early on in the teaching term, so you’re not surprised by a registrar who might have a different approach,’ he said.
This method includes sessions on subjects that present regularly in general practice and the abilities needed to treat them, such as musculoskeletal problems, minor surgery and other procedural skills.
‘All of those basic things, just do them formally and get them off the agenda. Then registrars feel more comfortable and confident,’ he said. ‘I also feel more confident
Dr Gay’s practice, Walter Road East General Practitioners in Perth, has been the recipient of several awards for training in recent years.
that when they come to do these procedures. I know what to expect.’
While it is important to adhere to teaching models, Dr Gay has learned that some of his own innovations, borne of years of clinical experience, can also be helpful to registrars.
‘For example, we have a treatment room session which is all about getting foreign bodies out of ears and eyes,’ he said. ‘I have actually developed my own models for extracting corneal foreign bodies. I put gelatine caps into the eyes of a dummy head and you can use burrs and other things to scrape them out.’
Dr Gay has some practical advice for GPs who may be considering becoming general practice supervisors but who aren’t ready to dive straight in.
‘If you’re unsure about it, the usual pathway is to start doing external clinical teaching,’ he said. ‘That gives you an opportunity to visit lots of other practices and see how they’re doing supervision, and get an idea of what to expect of registrars.’
Dr Gay believes that supervisors themselves, and even their practice as a whole, gain as much as the students from the teaching relationship.
‘I think teaching is probably the best value CME [continuing medical education] activity available because it is relevant to the task, focused around general practice, and also focused on your particular practice circumstances,’ he said. ‘It really lifts the
standard, not just of my own practice, but the other doctors as well.’
The knowledge passed on by general practice supervisors also has the chance to develop a life outside of a GP’s own practice.
‘You can have an influence on your patients and that’s great,’ Dr Gay said. ‘But if you think you’re doing something well and you want it to spread beyond your practice, you have the opportunity to teach other people. A little bit of you goes out with every registrar.’
Dr Gay explained that although supervisors are provided with guidance from training organisations, much of the most effective teaching processes are developed by the supervisors themselves.
‘There’s a big gap between what’s prescribed and filling up the teaching hours, and you have your own ideas about what should be taught,’ he said.
For this reason – among many – Dr Gay is glad of the validation that comes of being named the RACGP’s 2016 General Practice Supervisor of the Year.
‘It’s nice to receive acknowledgement that what you’ve been doing has been the right way,’ he said. ‘It’s good recognition that what I’ve been teaching has fulfilled the needs of the people who nominated me.’
14 Reprinted from Good Practice Issue 10, October 2016
Hometown roots
Imag
e C
hris
Hug
hes
REG
ISTR
AR
OF
THE
YEA
R R
EGIS
TRA
R O
F TH
E YE
AR
REG
ISTR
AR
OF
THE
YEA
R R
EGIS
TRA
R O
F TH
E YE
AR
REG
ISTR
AR
OF
THE
YEA
R R
EGIS
TRA
R O
F TH
E YE
AR
REG
ISTR
A
AMANDA LYONS
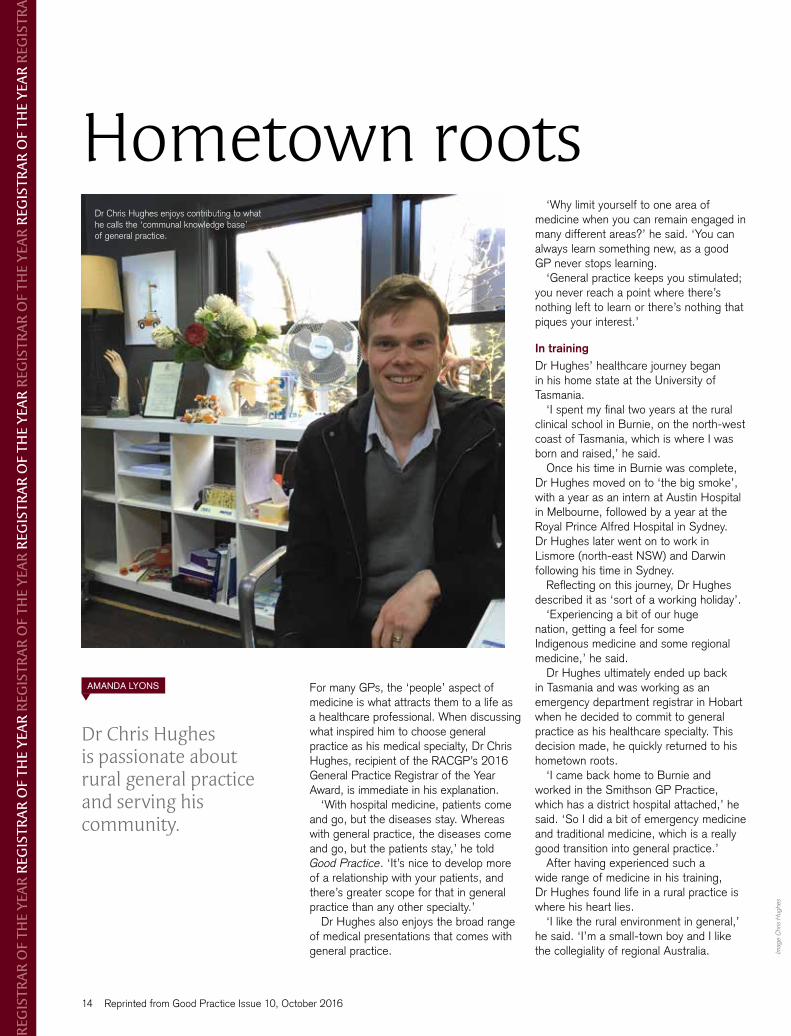
Dr Chris Hughes is passionate about rural general practice and serving his community.
For many GPs, the ‘people’ aspect of medicine is what attracts them to a life as a healthcare professional. When discussing what inspired him to choose general practice as his medical specialty, Dr Chris Hughes, recipient of the RACGP’s 2016 General Practice Registrar of the Year Award, is immediate in his explanation.
‘With hospital medicine, patients come and go, but the diseases stay. Whereas with general practice, the diseases come and go, but the patients stay,’ he told Good Practice. ‘It’s nice to develop more of a relationship with your patients, and there’s greater scope for that in general practice than any other specialty.’
Dr Hughes also enjoys the broad range of medical presentations that comes with general practice.
‘Why limit yourself to one area of medicine when you can remain engaged in many different areas?’ he said. ‘You can always learn something new, as a good GP never stops learning.
‘General practice keeps you stimulated; you never reach a point where there’s nothing left to learn or there’s nothing that piques your interest.’
In trainingDr Hughes’ healthcare journey began in his home state at the University of Tasmania.
‘I spent my final two years at the rural clinical school in Burnie, on the north-west coast of Tasmania, which is where I was born and raised,’ he said.
Once his time in Burnie was complete, Dr Hughes moved on to ‘the big smoke’, with a year as an intern at Austin Hospital in Melbourne, followed by a year at the Royal Prince Alfred Hospital in Sydney. Dr Hughes later went on to work in Lismore (north-east NSW) and Darwin following his time in Sydney.
Reflecting on this journey, Dr Hughes described it as ‘sort of a working holiday’.
‘Experiencing a bit of our huge nation, getting a feel for some Indigenous medicine and some regional medicine,’ he said.
Dr Hughes ultimately ended up back in Tasmania and was working as an emergency department registrar in Hobart when he decided to commit to general practice as his healthcare specialty. This decision made, he quickly returned to his hometown roots.
‘I came back home to Burnie and worked in the Smithson GP Practice, which has a district hospital attached,’ he said. ‘So I did a bit of emergency medicine and traditional medicine, which is a really good transition into general practice.’
After having experienced such a wide range of medicine in his training, Dr Hughes found life in a rural practice is where his heart lies.
‘I like the rural environment in general,’ he said. ‘I’m a small-town boy and I like the collegiality of regional Australia.
Dr Chris Hughes enjoys contributing to what he calls the ‘communal knowledge base’ of general practice.
15Reprinted from Good Practice Issue 10, October 2016
More people in health and community services choose HESTA for their super
2015 RAINMAKER EXCELLENCE AWARDS
WINNERWORKPLACE SUPER PRODUCT OF
THE YEAR - VALUE CHOICE
Supports your industry | Low fees | A history of strong returns
Issued by H.E.S.T. Australia Ltd ABN 66 006 818 695 AFSL 235249, the Trustee of Health Employees Superannuation Trust Australia (HESTA) ABN 64 971 749 321. Investments may go up or down. Past performance is not a reliable indicator of future performance. Product ratings are only one factor to be considered when making a decision. See hesta.com.au for more information. Before making a decision about HESTA products you should read the relevant Product Disclosure Statement (call 1800 813 327 or visit hesta.com.au for a copy), and consider any relevant risks (hesta.com.au/understandingrisk)
1797_HESTA_generic_RACGP_186x106.indd 1 28/06/2016 12:58 PM
‘In terms of work, I like the fact that you can really engage with a community and be helpful in people’s lives.’
Looking back on his time as a general practice registrar, Dr Hughes recalled his experiences with inspiring supervisors.
‘[They are] rural GPs who are multi-talented and multi-skilled and work well under pressure,’ he said. ‘They really confirmed that I do want to be a rural GP.’
Today, Dr Hughes has settled with his wife and newborn child in the small town of Wynyard close to where he grew up. He works at the Saunders Street Clinic, which he described as ‘a beautifully designed clinic with a lovely group of people and a relaxed, inviting atmosphere’.
ResearchDr Hughes received his RACGP Fellowship at the end of 2015 and is nearing completion of his Fellowship in Advanced Rural General Practice (FARGP). While the FARGP has helped broaden Dr Hughes’ skill-set in care delivery for rural patients, it also provided unexpected additional benefit.
‘It was part of my FARGP to do a six-month community-based project, with the
option to make it a research-type project,’ he said. ‘I was a little apprehensive, having never done research in my undergraduate career, but it has been such a good learning experience. I think more GPs should get involved with it.
‘I know there are barriers for GPs and general practice registrars to do research, but it’s been fun – a lot more fun than I thought it would be – and it’s a good skill-set to develop in your career. It has been a highlight for me.’
Dr Hughes’ FARGP research project, ‘E-referrals: Why are we still faxing?’ focuses on eHealth, a subject he feels is vital to the future of general practice, particularly in rural and regional areas.
‘I think [eHealth] has the potential to be a game changer for rural medicine because of the obvious constraints of remoteness,’ he said. ‘It just bridges that gap, to be able to get up your screen and talk with an urban specialist and get the best expertise on your care.
‘But, more than that, I think eHealth is an area where we are really dragging our feet in general practice in comparison with a lot of other industries and fields. We’re still faxing, we’re still posting letters.’
Dr Hughes would like to continue conducting general practice research through his career and has found a good local source of support and encouragement.
‘There’s a thriving research community based at the rural clinical school [at the University of Tasmania],’ he said. ‘They’ve been really helpful with getting my research off the ground and ironing out the creases.
‘I hope to be involved more going forward because it’s enjoyable and it’s nice to contribute to the communal knowledge base.’
Dr Hughes described being named as the RACGP’s 2016 General Practice Registrar of the Year as ‘a really pleasant surprise’.
‘It’s a very touching, unexpected achievement that firms my choice to be a rural GP,’ he said.
The accolade crowns what has been a deeply satisfying training journey.
‘I enjoyed all of my different terms as a junior doctor. It’s been nice to see a broad range of different things, different acute medical care,’ Dr Hughes said. ‘And coming back to my home community and being able to contribute has been a real highlight.’

Imag
es F
inta
n A
ndre
ws
16 Reprinted from Good Practice Issue 10, October 2016
AMANDA LYONS
Dr Fintan Andrews thrives on the demands and conditions of rural general practice.
Dr Fintan Andrews, the RACGP’s 2016 Rural Registrar of the Year, may not originally be from a rural community, but he has discovered a strong affinity for life in the country during his time in Broome, a coastal town in the Kimberley region of Western Australia.
‘I was born in Tasmania, then grew up in Perth, mostly,’ he told Good Practice. ‘I still really like Perth, but I prefer living in a small regional town.’
Dr Andrews earned his undergraduate degree in exercise rehabilitation science at the University of Western Australia. He worked in this field for two years before returning to study, this time in medicine, at the University of Notre Dame in Fremantle.
Upon completion of his medical studies, Dr Andrews worked as a resident and also completed a diploma of obstetrics. He is now in his second year of general practice training in Broome.
‘I worked a whole year in private general practice last year,’ Dr Andrews said. ‘This year I am doing the FARGP [Fellowship in Advanced Rural General Practice],
doing half of my time in ED [emergency department] and half in obstetrics.’
Dr Andrews has found that the FARGP offers an invaluable opportunity to further prepare for the challenges of a life and career in rural general practice.
‘I’m pretty keen on being a rural GP, but there’s a lot of raw hospital medicine involved and I found that training can be a little short otherwise,’ he said.
‘The FARGP gives you another year ... to work in a supported environment.’
Broome GPThe overall appeal of regional living is tied directly into Dr Andrews’ work in the Kimberley.
‘You can still be a generalist [in rural healthcare]. You get to see a little bit of everything in a broad range of people,’ he said. ‘And I like living in a country town and knowing most of the people.
‘Unlike the potentially impersonal nature of tertiary medicine, where people might be more inclined to be less polite on the phone because they don’t know each
Challenge accepted
RU
RA
L R
ESG
ISTR
AR
OF
THE
YEA
R R
UR
AL
RES
GIS
TRA
R O
F TH
E YE
AR
RU
RA
L R
ESG
ISTR
AR
OF
THE
YEA
R R
UR
AL
RES
GIS
TRA
R O
F TH
E YE
AR
RU
RA
L R
ESG
ISTR
AR
OF
THE
Dr Fintan Andrews has embraced the often demanding nature of rural general practice.

17Reprinted from Good Practice Issue 10, October 2016
other, you generally know most of your other colleagues in a smaller town and I like that work environment.’
Working in a place like Broome, a major tourist town with a population that swells and declines in accordance with the seasons, presents its own unique challenges and conditions for a healthcare professional.
According to Dr Andrews, while the area fills with tourists during the dry season in the middle of the year, the wet season sees a significant number of Aboriginal and Torres Strait Islander patients come into the town from remote communities.
‘The work changes quite significantly depending on the time of the year,’ he said. ‘So at this time of the year [the dry season] it’s a lot of “grey nomads”, whereas in the wet season it’s mostly Indigenous health,’ he said.
‘So we have sicker people in the wet season, but fewer numbers, and a lot more people in the dry season, but they are not nearly as sick.’
There are other specific challenges that come with working in a regional area, such as access to specialist care.
‘You don’t have an MRI [magnetic resonance imaging] at your fingertips, for example, so to
organise an MRI is an amazing effort – a two-and-a-half hour flight to Perth,’ Dr Andrews explained. ‘Or trying to get someone to see an orthopaedic surgeon, who visits four times a year, if the patient doesn’t have access to private healthcare, can be difficult.’
But Dr Andrews feels these types of inherent challenges have a definite upside.
‘In some ways that’s what I like about it, because it forces you to do a lot of that work yourself, or the beginning of that work, rather than more segregated medicine where you might say, “This will need an orthopaedic surgeon”. It’s more hands-on,’ he said.
‘One day you might be doing what anyone would be doing as an ED doctor. You might have a resuscitation, then you get to deliver a baby, then you see someone with a common cold and another with mental health issues, all in one day. You do absolutely everything, which is really cool.’
Dr Andrews is also keen to acknowledge that living and working in Broome supplies him with the best of both worlds in terms of life in regional and urban locations.
‘We’re a pretty big regional centre; I can still go out for a nice meal,’ he said. ‘The people who work in really remote places like Halls
Creek and Fitzroy Crossing [in the Kimberley region] probably face a little bit more of a challenge.
‘But in Broome, we’ve got a pretty nice work–life balance and I don’t think we can really complain a lot.’
This type of modest outlook was echoed by Dr Andrews’ reaction to winning the RACGP’s 2016 Rural Registrar of the Year Award.
‘It’s surprising and very flattering to win it, especially when I’m surrounded by so many good doctors,’ he said.
‘The nicest thing is not the award as such, but rather that my colleagues thought to nominate me.
Dr Andrews enjoys the work–life balance available to him as a GP in Broome, WA.

18 Reprinted from Good Practice Issue 10, October 2016
GEN
ERA
L PR
AC
ITC
E O
F TH
E YE
AR
GEN
ERA
L PR
AC
TIC
E O
F TH
E YE
AR
GEN
ERA
L PR
AC
ITC
E O
F TH
E YE
AR
GEN
ERA
L PR
AC
TIC
E O
F TH
E YE
AR
GEN
ERA
L PR
AC
ITC
E O
F TH
E
Community serviceAMANDA LYONS
The staff members at Ararat Medical Centre work hard to meet the needs of patients, students and employees.
Victoria’s Ararat Medical Centre, recipient of the RACGP’s 2016 Practice of the Year Award, has deep roots within its community. Dating back to the early 1960s, the practice started when three local doctors – Dr Frank de Crespigny Jnr, Dr Peter Trigg and Dr Ian Matthews – joined forces to create a single clinic.
The practice is still in its original High Street premises, although these have been modified over the years as the number of doctors and other staff members grew. Today, Ararat Medical Centre employs 15 doctors (a number that varies depending on registrars), four nurses and five administrative staff members – quite an expansion from the original three GPs.
However, according to Dr Derek Pope, GP and current practice principal, there are no plans for further renovations at Ararat Medical Centre.
‘I think we’ve reached the physical limits now, unless we start building out over the car park,’ he told Good Practice.
Ararat is a small town in the south-west of Victoria with a population of about 8000. In addition to providing healthcare to the
local population, Ararat Medical Centre also operates satellite services throughout the wider catchment area, which encompasses about 12,000 people.
‘A lot of the smaller towns around the region no longer have any medical services,’ Dr Pope explained. ‘So we go out to three places – Willaura, Elmhurst, Lake Bolac – and provide a service once or twice a week.’
The patient demographic across the region is quite broad, including almost all age groups.
‘We treat from birth – literally – because we’re probably one of the few remaining practices in the country, or at least in Victoria, that does obstetrics,’ Dr Pope said.
Ararat Medical Centre’s doctors also carry out procedures at the local hospital and take turns providing after-hours care at the clinic. While this can be challenging, it provides opportunities to practise a wide range of medical skills that might not be available in other settings.
‘Anaesthetics, obstetrics, emergency care, excisions; basically anything you feel comfortable doing, there is an opportunity to do it here,’ Dr Pope said.
Training assistanceThe diversity of presentations at Ararat Medical Centre makes it an ideal training ground for young doctors.
‘Registrars and medical students sometimes mention that within a day

19Reprinted from Good Practice Issue 10, October 2016
or two of getting to the practice, they’re doing things that they’ve never tried or seen before, or have only been exposed to once or twice,’ Dr Pope said.
Dr Pope believes it is not only the students who benefit from training at Ararat Medical Centre.
‘It keeps us on our toes,’ he said. ‘When a medical student or a registrar asks you a curly question, you have to think carefully before answering, so we’ve got to keep up our own knowledge.
‘And we’re getting registrars or medical students straight out from teaching. They know the latest information that hasn’t hit the textbooks, and sometimes not even the medical journals, so that’s always very useful. We get a lot of cross-fertilisation of ideas.’
It can also be socially refreshing to have new people coming through the practice.
‘Different faces and opportunities to socialise. Just having the people coming and going makes it interesting,’ Dr Pope said.
In turn, Ararat Medical Centre puts effort into creating some social and learning opportunities for its general practice registrars and medical students.
‘We try to introduce them into the town. We get them to meet various people, get involved in sporting groups,’ Dr Pope said. ‘On the professional level, we hold regular
tutorials and meetings at lunchtime and after hours, as well as regular clinical meetings.’
The clinic also has a policy of vertical integration, mixing students of different experience levels.
‘At the moment, we’ve got Deakin [University] medical students, plus the registrars, so there’s a lot of interaction between them. They can learn from each other very well,’ Dr Pope said. ‘And we’re going to put something in the middle – hopefully, we are getting general practice interns next year as well.’
Mindful of the difficulties of relocating to a regional area, Ararat Medical Centre puts a lot of effort into assisting its general practice registrars make the transition.
‘We want to try and make the practice and the town as inviting as possible,’ Dr Pope said. ‘[For example], we make sure we have accommodation available, so registrars don’t have to be looking in an area where there’s often not a lot around.’
Country lifeWhile rural living does present its challenges, Dr Pope believes it also comes with plenty of benefits, and the relationship GPs can build with patients is chief among them.
‘You get to know your patients very well,’ Dr Pope said. ‘You look after them during
pregnancy, you look after them as they get older, you admit them to the local hospital.
‘I think patients tend to be very loyal. They’ll see one doctor for many, many years and even if they go away, they will often come back.
‘There’s a feeling of continuity.’Dr Pope believes working at Ararat
Medical Centre also offers a range of non-professional benefits.
‘It takes me roughly 90 seconds to get to work, and another couple of minutes to get out in the countryside,’ Dr Pope said. ‘No traffic, everything in town is relatively close, and yet if I want to get away for a weekend, the Grampians are only 45 minutes away.
‘It’s a pleasant lifestyle.’For the staff members at Ararat Medical
Centre, winning the RACGP’s 2016 Practice of the Year Award is a welcome surprise and affirmation of their efforts.
‘It’s recognition of all the really hard work that everyone’s done over the years at the practice. Not just the doctors, but the reception and managerial staff, the nursing staff, the practice manager, the office manager,’ Dr Pope said.
‘As a whole, the practice runs very smoothly and everyone’s always had a good working relationship with each other. In a way, the award is a recognition of that.’
Left: Ararat Medical Centre non-clinical leadership team (L–R), nurse unit manager Vicki Parsons, practice manager Garry Hurst and reception supervisor Denise McGrath. Below: Practice partners (L–R) Dr Chee Sheng Wang, Dr Derek Pope, Dr Michael Connellan and Dr Eric Van Opstal.
Imag
es A
rara
t Med
ical
Cen
tre
Imag
e R
AC
GP
PAUL HAYES
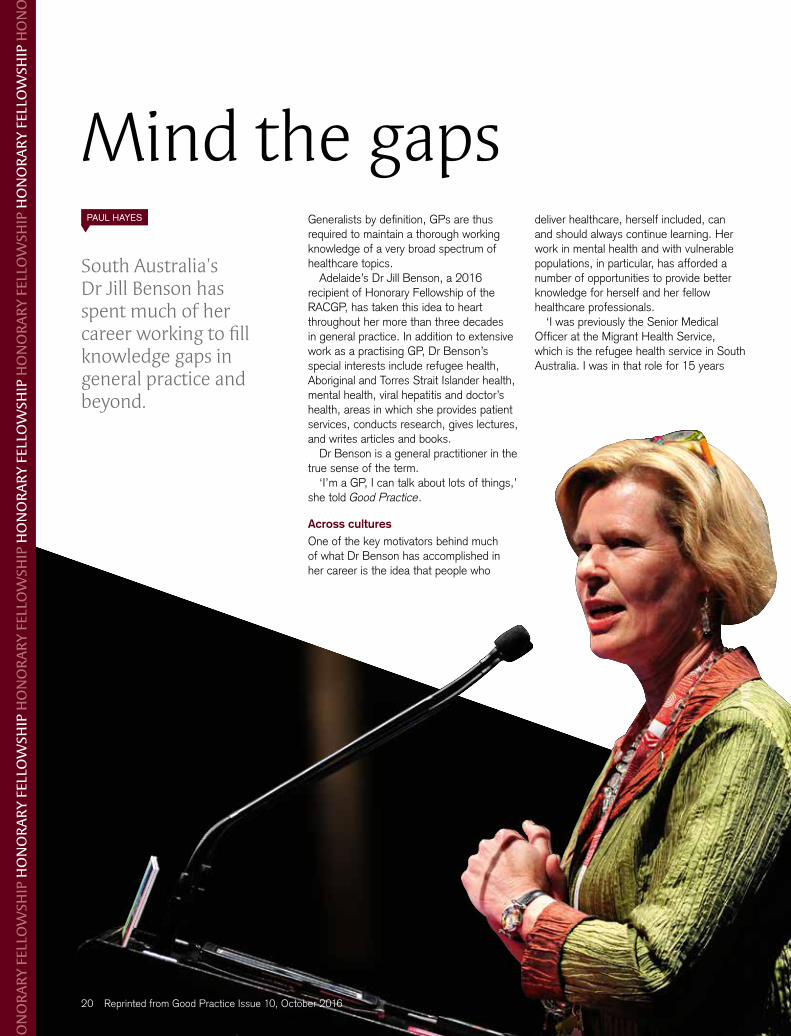
South Australia’s Dr Jill Benson has spent much of her career working to fill knowledge gaps in general practice and beyond.
Mind the gaps
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
RA
RY
FELL
OW
SHIP
HO
NO
R
Generalists by definition, GPs are thus required to maintain a thorough working knowledge of a very broad spectrum of healthcare topics.
Adelaide’s Dr Jill Benson, a 2016 recipient of Honorary Fellowship of the RACGP, has taken this idea to heart throughout her more than three decades in general practice. In addition to extensive work as a practising GP, Dr Benson’s special interests include refugee health, Aboriginal and Torres Strait Islander health, mental health, viral hepatitis and doctor’s health, areas in which she provides patient services, conducts research, gives lectures, and writes articles and books.
Dr Benson is a general practitioner in the true sense of the term.
‘I’m a GP, I can talk about lots of things,’ she told Good Practice.
Across culturesOne of the key motivators behind much of what Dr Benson has accomplished in her career is the idea that people who
20 Reprinted from Good Practice Issue 10, October 2016
deliver healthcare, herself included, can and should always continue learning. Her work in mental health and with vulnerable populations, in particular, has afforded a number of opportunities to provide better knowledge for herself and her fellow healthcare professionals.
‘I was previously the Senior Medical Officer at the Migrant Health Service, which is the refugee health service in South Australia. I was in that role for 15 years

Reprinted from Good Practice Issue 10, October 2016
and I found lots of gaps in the evidence,’ she said. ‘I was one of the founding members of the Refugee Health Network of Australia [RHeaNA], which is still going, and the South Australian Refugee Health Network, which was active for about 10 years. I am also part of the WONCA [World Organization of Family Doctors] special interest group in refugees.’
These experiences opened Dr Benson’s eyes to what people did not know in terms of healthcare delivery for these patients. She resolved to undertake a PhD on refugee health, on which she is now placing the finishing touches.
‘From the experiences I was having working with the refugee patients, I could see that the answers for some of those gaps [in the evidence] were there, so that’s what my PhD is about,’ she said. ‘My research into refugee health has been an enormously fulfilling and important thing.’
I have wanted to publish [my research] because I wanted it to be available in the public domain
Dr Benson is also part of the WONCA special interest group on mental health, an area in which she has done extensive work in Australia and overseas to help patients and, again, other healthcare professionals.
‘I have done two overseas stints with my mental health hat on,’ she said. ‘One was to a remote area of eastern Nepal, where I went twice. The first time was with a GP hat on to help with their exams. The second time I had a joint position with departments of psychiatry and general practice of B.P. Koirala Institute of Health Sciences, which is the medical, dental and nursing school in Dharan.
21
‘Then I did a three-year stint with the WHO [World Health Organization] in Vanuatu, with an organisation called the Pacific Islands Mental Health Network. That was a volunteer position, which was two months a year.
‘I was part of a team of two, writing a policy and strategy for mental health for the country. I wrote an interactive mental health training program to help them set up remote mental health clinics, then mentored the nurses into using those. I then set up a peer-support network.’
Dr Benson’s work with other cultures also includes Aboriginal and Torres Strait Islander peoples, when she wears her ‘public health hat’.
‘I have positions in remote Aboriginal communities, so I set up an organisation called Kakarrara Wilurrara Health Alliance,’ she said. ‘That is an alliance of the health services of three remote Aboriginal communities, Yalata, Oak Valley [SA] and Tjuntjuntjara [WA]. I’m the Medical Director of that organisation.
‘I also work as a GP at a Mount Gambier [in south-eastern SA] Aboriginal health service called Pangula Mannamurna.’
All of this work with patients from differing cultures again led Dr Benson to undertake research and provide previously unavailable knowledge to people in the healthcare industry. Working with Queensland GP Dr Jill Thistlethwaite, she released the book Mental health across cultures: A practical guide for health professionals in 2009.
‘When I wrote that book there wasn’t a lot about working in mental health across cultures, so I wanted to write something that would be helpful for GPs,’ she said. ‘Because I’d worked across cultures a lot, I felt I had some skills that I’d learned along the way, mostly from [knowing] patients and making mistakes.
‘I thought it would be useful to share that with people, because not everyone has the opportunity to spend as much time working across cultures; people are likely to do it in bits and pieces. So [it was important for me] to actually write something to share those skills.’
Dr Benson’s work in medical publications, which also includes a significant number of journal articles, has been completed with this idea of knowledge sharing firmly in mind.
‘For a lot of my writing, it’s about the idea that I have learnt a whole lot of information and people don’t know it, and it’s much easier for them to be able to read it than for them to
make the same mistakes I made, or have to have the experiences at the depth that I have had them,’ she explained.
‘The research I have done is mainly because I have felt there has been a gap in the literature, there has been something that needs to be researched that is going to make a difference to the protocols and evidence-based guidelines that are there.
‘I have wanted to publish because I wanted it to be in the public domain.’
All of this work across cultures eventually culminated in Dr Benson being awarded an Order of Australia (AM) in 2012 for her work with refugees, Aboriginal and Torres Strait Islander peoples and in mental health.
Healthy outlookMuch of the expertise and experience Dr Benson accumulated throughout her professional life came together in a recent career move into a role as a medical educator with the South Australian training organisation, GPEx.
‘I feel like this brings all of the skills I have gathered over the years into one place, as I now have an opportunity to teach and mentor the next generation of GPs,’ she said.
With so many different healthcare roles across a number of interests and locations, Dr Benson has developed an important perspective on her profession.
‘I have lots of jobs [in medicine] and I think that is one of the things that keeps me safe from burning out,’ she said. ‘I’ve managed to learn from my children that medicine isn’t about owning the outcomes. The outcomes don’t belong to us, the outcomes are what I call a miracle.
‘I think that’s one of the things that has kept me from [wearing down] – if things don’t work out, it’s not because I’m a bad person or a bad doctor, it’s because that’s life. And if things do work out, it’s not necessarily because I’m a good doctor, it’s because things worked out.’
This desire to simply be the best doctor she can, and knowing so many other GPs strive for the same thing, is why Dr Benson feels receiving an accolade like Honorary Fellowship of the RACGP is ultimately for something bigger than her own achievements.
‘It’s not just about me, but about all of the GPs who are working in the sort of areas that I am, because they all work at the hard end of the spectrum,’ she said.
‘I am one of a group of people who could equally receive this.’
Dr Jill Benson believes it is important to disseminate the knowledge she has gathered over more than 30 years in medicine in order to help other doctors provide the best possible care.
22 Reprinted from Good Practice Issue 10, October 2016
RACGP Academic Session Awards 2016Rose-Hunt AwardAssoc Prof John Litt, SA
Honorary FellowshipDr Jill Benson, SA; Dr Stephen Wilson, WA
RACGP Aboriginal and Torres Strait Islander Health ‘Standing Strong Together’ AwardDr Jamie Fernando and the Glen Centre, Central Coast Drug and Alcohol Residential Rehabilitation, NSW
General Practitioner of the Year AwardDr Jane Cooper, Tas
General Practice Supervisor of the Year AwardDr Rohan Gay, WA
General Practice Registrar of the Year AwardDr Chris Hughes, Tas
Rural Registrar of the Year AwardDr Fintan Andrews, WA
General Practice of the Year AwardArarat Medical Centre, Vic
RACGP Rural Medical Undergraduate Student Bursary AwardMaeve Barlow, NSW
Brian Williams Award (RACGP Rural)Dr Patrick Giddings, NSW
Monty Kent-Hughes Memorial AwardDr Daniel Wilson, SA (2015.2 exam cycle) Dr Jessica Borgas, SA (2016.1 exam cycle)
RACGP Foundation Research Awards• Therapeutic Guidelines Limited
(TGL)/RACGP Research Grant: Assoc Prof Michelle Guppy, NSW; Dr Carissa Bonner, NSW; Prof Jane Gunn, Vic
• HCF Research Foundation/RACGP Research Grant: Dr Tejas Kanhere, NSW; Prof Moyez Jiwa, Vic
• RACGP/Diabetes Australia Research Grant: Assoc Prof Michelle Guppy, NSW
• RACGP/ANEDGP Research Grant: Dr Colin Goodson, SA
• RACGP/MDA National Best General Practice Research Article in Australian Family Physician (AFP) Award: Dr Clare Willix, WA
• RACGP Indigenous Health Award: Ms Charmaine Earnshaw, ACT; Miss Madeline Thomson, ACT; Mr Luke Walker, NSW
• RACGP Family Medical Care Education and Research (FMCER) Grant: Dr Andrew Davey, NSW; Dr Karen Price, Vic; Dr Miriam Brooks, NSW
• RACGP Chris Silagy Research Scholarship: Dr Elizabeth Sturgiss, ACT
• RACGP PWH Grieve Memorial Award: Dr Su-Yin Yeong, NSW
• RACGP Rex Walpole Travelling Fellowship: Dr Scott Allison, Qld
GP1
6 AW
AR
D W
INN
ERS
GP1
6 AW
AR
D W
INN
ERS
GP1
6 AW
AR
D W
INN
ERS
GP1
6
23Reprinted from Good Practice Issue 10, October 2016
GENERAL PRACTICE MANAGEMENT TOOLKIT
Managing the wellbeing of staff and self
PAUL HAYES
The 11th module in the RACGP’s General Practice Management Toolkit aims to provide GPs with the ability to better look after themselves and their practice teams.
As is the case with so many healthcare professionals, GPs can often be guilty of thinking of themselves last.
‘People in general practice are excellent at providing care to patients, but this often comes at the expense of GPs’ own health and wellbeing,’ GP and practice owner Dr Neville Steer told Good Practice.
According to Dr Steer, the notion that GPs often take better care of others than of themselves is particularly true when it comes to non-physiological issues.
‘GPs frequently do well with regard to areas such as healthy eating, not smoking, moderate drinking and avoiding excess weight gain,’ he said. ‘However, many doctors experience psychological distress at levels many times higher than those in the general community.
‘Achieving appropriate work–life balance is a common issue for doctors.’
The 11th module in the RACGP’s General Practice Management Toolkit (the Toolkit) is designed to help GPs develop the necessary tools to support themselves and others within their practice.
Managing the wellbeing of staff and self includes information on areas such as personal healthcare, staff health issues, occupational
health and safety, workplace assessment for stress and risk, and doctors’ health advisory services.
Upon completion of the module, GPs and practice staff will be able to:• understand sources of stress in
general practice• recognise personal health needs and
potential problem areas• recognise risks to personal safety• understand the process of conducting a
violence risk analysis for the workplace• identify the potential signs of patient agitation
and the techniques for conflict de-escalation• identify practice design elements that reduce
risk and violence.‘Discussing a practice approach [to such matters] at a staff meeting, backed up with resources and procedures, can make the
workplace safer,’ Dr Steer, key GP author of the Toolkit, said.
Dr Steer believes that, in addition to potential issues of stress among GPs and staff members, it is particularly important to address matters of personal security within a practice.
‘The module also discusses issues around safety and risk management in the workplace,’ he said. ‘For example, some practices are regularly confronted by agitated and drug-affected patients, which is both stressful and dangerous.
‘It is important to examine a general practice’s approach to minimising risks and improving safety.’
The idea of ‘minimising risks and improving safety’ within a practice can involve some practical planning and strategy, such as the use of emergency buttons to summon help in difficult situations or ensuring a practice’s layout allows for easy access to entry and exit points.
‘Office hazards can be addressed by using a check list and conducting a “walk through” as an internal audit,’ Dr Steer said. ‘This may include tripping hazards from items being left on the floor, electrical hazards with overloaded power boards, or physical hazards from poorly designed work stations.
‘Practice owners have a duty of care to take reasonable steps to create a safe work environment.’
In the event of an agitated patient, it is vital members of the practice team know how to best handle the situation.
‘Staff training is also important,’ Dr Steer said. ‘In some situations, early intervention to avoid escalation can be effective in containing problems.
‘Medical receptionist staff members, for example, can frequently observe the behaviours of patients who are agitated and effectively intervene to manage the situation.
‘And providing doctors and staff with de-briefing opportunities after stressful incidents is another way of helping manage work stress.’
Module 11
General practice management toolkit
Managing the wellbeing of staff and self
Module
11
Visit www.racgp.org.au/your-practice/business/managementtoolkit for more information on the RACGP’s General practice management toolkit.
24 Reprinted from Good Practice Issue 10, October 2016
NUTRITION
Working with dietitiansCLAIRE HEWAT
The relationship between GPs and Accredited Practising Dietitians.
GPs are a key referral source for Accredited Practising Dietitians (APDs), who in turn can help GPs improve patient outcomes.
A 2015 survey conducted by the Dietitians Association of Australia (DAA), ‘Working with dietitians – A survey for GPs and practice nurses’, was designed to assess existing communication and relationships between primary healthcare professionals and APDs. A total of 180 GPs and practice nurses took part in the survey, with responses revealing several opportunities for GPs and APDs to work more closely together.
Dietitian vs nutritionistAlmost all of the surveyed GPs and practice nurses (99%) refer patients to a dietitian, whereas 8% refer to a nutritionist, demonstrating a preference for appropriately qualified allied health professionals.
The survey also indicated that more than half of GPs and practice nurses (53%) provide nutrition advice several times a day.
APDsThe APD credential is the only one for medical nutrition therapy recognised by the Federal Government (including Medicare, Department of Veterans Affairs and the National Disability Insurance Scheme) and most private health funds.
APDs undertake ongoing training and education to comply with the DAA’s guidelines for evidence-based practice and are committed to the DAA’s ‘Code of professional conduct’ and ‘Statement of ethical practice’.
More than half of the surveyed GPs and practice nurses (59%) were aware of the APD credential, with similar levels of awareness among consumers (46%). Despite this awareness, only 33% of GPs and practice nurses surveyed are certain the dietitian to whom they refer is an APD, while 39% assume they are an APD.
While GPs and consumers can use the ‘Find an APD’ tool on the DAA website to locate a local APD, the survey indicated only 18% of respondents currently use it, with word-of-mouth (60%) and a personal introduction (53%) the most common means used to find and select a dietitian.
Reasons and barriers for referralAccording to the survey, the key reasons GPs and practice nurses refer patients to a dietitian include more comprehensive, individualised, specific diet advice (92%); specific nutritional management of chronic conditions (63%); and a personalised plan (59%).
The three most common medical conditions for referral to a dietitian were diabetes mellitus (97%), overweight and obesity (95%) and food intolerances or coeliac disease (80%).
The most common barriers for referral identified were cost (49%); waiting times at community health/outpatient facilities (24%); inadequate feedback from dietitians (20%); and an assumption that patients would not see a dietitian (28%).
A majority of surveyed GPs and practice nurses (84%) knew patients could receive a Medicare rebate for seeing an APD, but only 26% use a Chronic Disease Management (CDM) (formerly Enhanced Primary Care) Medicare item number to refer to dietitians.
Referring patients to an APD under a CDM plan provides opportunity to reduce the costs for many patients and to increase feedback from dietitians due to reporting requirements.
Room for improvementTwo-thirds of respondents (68%) felt referral would be further encouraged if dietitians kept GPs and practice nurses informed of the advice they were giving, and half (52%) felt that a visit and explanation via personal contact by the dietitian would encourage referrals.
The DAA has communicated these results to APDs and developed tools to make regular communication with GPs easier and more efficient. The DAA will continue to support APDs to build relationships with GPs, with the ultimate goal of working together to help improve the health outcomes of as many patients as possible.
Author bioClaire Hewat is the CEO of the Dietitians Association of Australia (DAA), the first Accredited Practising Dietitian to be appointed to this position. She was previously a director on the DAA board and a member of the NSW branch executive.
Hewat has many years of experience in a number of areas, including clinical, food service, community and public health nutrition, diabetes education and private practice, and in various aspects of health service management.
Broad scopeAccredited Practising Dietitians (APDs) can help with many conditions, including osteoporosis, fertility, pregnancy, menopause, arthritis, food allergies and intolerances, hypertension, nutrient deficiencies, and gastroenterology or digestive conditions.
Visit http://daa.asn.au/for-health-professionals/choosing-your-nutrition-expert to access ‘Improving patient outcomes through medical nutrition therapy’, a list of conditions and information on how APDs can help manage them.
Visit http://daa.asn.au for more information on the Dietitians Association of Australia’s (DAA) ‘Code of professional conduct’ and ‘Statement of ethical practice’.
Contact the DAA at [email protected] for a summary of ‘Working with dietitians – A survey for GPs and practice nurses’.
TRIENNIUM UPDATE
130 points
1CPR
2Category 1
activities including 1QI activity
Complete your QI requirement for the QI&CPD 2014 –16 triennium
What is Quality Improvement (QI)?
Quality Improvement (QI) is the process where an opportunity to change practices occurs as a result of learning.
Professional advice and a large body of evidence demonstrate Quality Improvement activities leading to positive change in practices, particularly when involving a whole practice team approach.
For more information visit racgp.org.au and search ‘QI&CPD’
racgp.org.au Healthy Profession.Healthy Australia.
Plan, Do, Study, Act (PDSA)
Clinical audit Small group learning
Supervised Clinical Attachment (SCA)
Evidence Based Medicine Journal Club
GP research
Examples of QI activities:

26 Reprinted from Good Practice Issue 10, October 2016
RACGP SPECIFIC INTERESTS
Integrative medicineAMANDA LYONS
The RACGP Specific Interests Integrative Medicine working group helps GPs navigate complementary medicines by assessing and disseminating the latest evidence.
The term ‘complementary medicine’ (CM) encompasses a very broad field, ranging from nutrition and lifestyle interventions to herbal medicines and mind–body therapies. Although CM has traditionally been considered outside the remit of general practice, in the view of the Integrative Medicine Specific Interest working group, the two don’t have to be separate.
‘We see integrative medicine as the blending of evidence-based complementary therapies with conventional medicine,’ Dr Carolyn Ee, new Chair of the Integrative Medicine working group, told Good Practice.
‘My ultimate aim would be to have enough good-quality evidence, and enough translation of the evidence into clinical practice, that every doctor would be able to integrate these therapies where there is clear evidence for benefit.’
As a research fellow at the National Institute of Complementary Medicine, which is hosted by the Western Sydney University, Dr Ee is well qualified to oversee these efforts.
‘I see [the working group] as a great way of combining my own search for the evidence and serving the needs of the doctors in the working group and, more broadly, all GPs, whether or not they identify as integrative GPs,’ she said.
The Integrative Medicine working group assesses and collates research on complementary therapies, compiling
the relevant information into a bi-monthly members’ newsletter.
‘We have an editorial board that looks at all the evidence that’s come in, all the new systematic reviews and cohort studies looking at the effects of different nutritional parameters on health, as well as clinical trials,’ Dr Ee explained.
‘We don’t just cherry-pick the best or the most positive trials. We put everything up on our newsletter. We recently posted a couple of trials which showed that certain supplements were not helpful and, in fact, were potentially dangerous.
‘This is an important way to inform our members of the need to be vigilant and consider carefully before they prescribe supplements.’
Patient-centredUnderstanding what needs to be taken into account when considering CM is increasingly important for GPs.
‘We know that more than half of our patients are using complementary therapies, such as supplements or techniques like acupuncture or meditation,’ Dr Ee said. ‘And about half of these patients will not ask us about them or tell us they are taking supplements or using these practices. So there is a bit of a disconnect between what they’re doing and what we know.’
Dr Ee believes it is important for GPs to be sensitive when it comes to CM in order to avoid alienating patients. If those patients don’t return to their GP, she said, they may end up receiving no guidance from a conventional medicine perspective. Dr Ee thus feels it is important to encourage openness and quality dialogue when discussing CM.
‘Patients would then come to us for advice before making their own decisions, or relying on the media or their friends’ experiences, which may not be appropriate or apply to them,’ she said.
Dr Ee also believes general practice can benefit from broadening its scope to include evidence-based complementary therapies that are not pharmaceutical in nature.
‘Things like mindfulness meditation, gentle therapies like yoga and tai chi that have an
increasing body of evidence to show that they do benefit our patients,’ she said. ‘And we need to know the supplements or western herbs that can help our patients, particularly for conditions that are very hard to treat. Premenstrual syndrome, for example.’
Dr Ee has found that patients often turn to CM when experiencing a health problem that has been difficult to solve in other ways.
‘It comes from a patient need that hasn’t been met,’ she said. ‘They’re struggling with a health issue that hasn’t been resolved. We need to recognise this signal.’
The philosophy of integrative medicine is ultimately concerned with placing the patient’s health needs at the centre.
‘I’m hoping that if GPs are open, our patients will tell us about these treatments and if what we’re prescribing is not adequate. So we need to look at other ways of helping them achieve the best outcomes,’ Dr Ee said.
About the working group
The RACGP’s Specific Interest Integrative Medicine working group began as a network in 2009 and became a working group in 2012. It gathers and assesses up-to-date evidence on complementary medicines (CM) and therapies in order to help GPs discuss existing CM treatments with patients, or recommend CM treatments where appropriate.
This information is disseminated to members via a bi-monthly newsletter, and members are provided access to additional online resources. The working group is also planning a Diploma in Integrative Medicine for GPs.
Visit www.racgp.org.au/yourracgp/faculties/specific-interests or contact [email protected] for more information or to join the network.

GP17RACGP CONFERENCE
ICC Sydney
gp17.com.au #GP17Sydney
Sydney 26–28 October 2017
SAVE the
date
GP17 is the must attend event on the general practice calendar
Connect with colleagues, up-skill your clinical knowledge, all whilst enjoying the natural beauty and vibrancy that Sydney has to offer.
Register your interest to attend at gp17.com.au
The
foun
da
tion of patient centred care
G
eneral practic
e
gp
GP17-check-Full-page-v2.indd 1 13/09/2016 9:02:02 AM
GENERAL PRACTICECONFERENCE & EXHIBITION
11–13 NOVEMBERMelbourne Convention & Exhibition Centre
Australia’s leading educational event for the entire General Practice team – register now for 10% off!
Why attend GPCE?
• Earn all of your QI&CPD points in one weekend
• Attend five ALMs, 140+ seminars & practical workshops
• Meet suppliers & network
• Hear the latest clinical updates & guidelines
• FREE accredited CPR training
• FREE entry to the GPCE exhibition
Don’t miss our LAST face-to-faceevent of thistriennium
PLATINUM SPONSORORGANISED BY
Book before 12 October for your 10% Early Bird discount.
Find out more at GPCE.COM.AU/MELBOURNE
AusFamilyPhysician_FullPageAd_Melb_Oct16.indd 1 12/09/2016 10:22:19 AM





























