Embed Size (px)
Citation preview

14
Dow
nst
ate
Res
earc
h2008
Dow
nstate
Research
2008
15Douglas Lazzaro, MD, chairman of SUNY Downstate’s
Department of Ophthalmology, says “the retina is an areawhere there’s tremendous new research activity going on,”much of it featured here.
Downstate now has a director of ophthalmic research,William J. Brunken, PhD, whose investigations into retinalproteins called laminins and netrins may one day help restoresight to the visually impaired. Brahim Chaqour, PhD, investi-gates the molecular underpinnings of diabetic retinopathy, amicrovascular disease that is one of the leading causes ofblindness in the United States, all in an effort to develop treat-ments that may one day prevent the disease.
Gladys Teitelman, PhD, a diabetes researcher who has con-centrated mostly on the regeneration of insulin-producing pan-
creatic beta cells, has widened her investigations toalso include diabetic retinopathy. DanielRosenbaum, MD, chairman of Downstate’sDepartment of Neurology, uses the retina as a modelfor understanding what happens to brain cells duringstrokes. And Ivan Bodis-Wollner, MD, DSc, director ofthe Parkinson’s Disease and Related Disorders, Centerof Excellence of the National Parkinson Foundation,explores how changes in the retina both signal and influ-ence the development of Parkinson’s disease.
“The research we’re doing at Downstate is leading to newunderstandings of retinal diseases and the nervous system,”Dr. Lazzaro says. “Most importantly, we’re creating potentialnew avenues of treatment.”
RESEARCHRETINOPATHY
The retina, the light-sensitive inner layer of the eye, is an area ofgreat scientific significance. Not only does it enable vision, it is anextension of the brain. The retina is composed of neural tissue,much like that larger organ from which it emerges during fetaldevelopment. As a result, research into the workings of the retina hasa great impact on medical science’s understanding of and treatmentof dysfunctions in the brain, as well as in the retina itself.
TO SAVEANDLIVES
SIGHT

17
tive description of the relationshipbetween the retina’s dopaminergicand dopamine-sensitive cells. A majoradvance in the Parkinson’s disease field,the model has been used to predict theretina’s response to new and existingParkinson’s treatments.
In the last several years, Dr. Bodis-Wollner has employed a new imagingtechnology called Optical CoherenceTomography (OCT) to detect micro-scopic changes in the retina. Says Dr.Bodis-Wollner, “the ability to imagethe retina may revolutionize theprocess of evaluating and monitoringthe neuronal changes that occur inParkinson’s disease.”
Using OCT, he has been among thefirst to measure the retinas of individu-als with Parkinson’s disease. Often,they are 15 to 20 percent thinner thannormal. “This loss may be a major rea-son why Parkinson’s patients have trou-ble detecting contrast,” Dr. Bodis-Wollner says. “And we’ve learned thatthe area of the retina affected inParkinson’s may impair visual cogni-tion,” the ability to respond to and cat-egorize visual images.
Dr. Bodis-Wollner looks forward tofurthering this research by acquiring thelatest generation OCT equipment.“With these machines, we hope to beable to specify dopaminergic cells, inaddition to measuring the retina’sthickness,” he notes. Giving researchers
Dow
nstate
Research
2008
Dow
nst
ate
Res
earc
h2008
16
RETINOPATHY RESEARCH Ivan Bodis-Wollner, MD, DSc
L ike many illnesses affecting thenervous system, Parkinson’s dis-ease is difficult not only to treat
but also to monitor.New evidence suggests that the
degenerative motor disorder begins inthe peripheral nervous system and thenworks its way to the central nervoussystem — most importantly, to thebrain. Once established there, this dis-ease can cause a host of neurologicalproblems: tremors, motor impairment,communications difficulties, and men-tal disturbances.
Visual problems were not thoughtto be part of Parkinson’s disease, how-ever. From the time the illness was firstdescribed in the early 1800s, untilmore than 150 years later, the loss ofvisual acuity and the difficulty in dis-tinguishing contrast many Parkinson’spatients experience were attributed toother causes, such as aging, cataracts,and glaucoma.
But in the late 1970s, Ivan Bodis-Wollner, MD, DSc, professor of neurolo-gy and ophthalmology and director ofUniversity Hospital’s Parkinson’sDisease and Related Disorders Center,one of the National ParkinsonFoundation’s Centers of Excellence,showed that Parkinson’s disease itselfcan have a negative impact on vision.
In 1978, using electrophysiology —brain-wave monitoring through exter-nally applied electrodes — he was thefirst to document delayed visual pro-cessing in the brains of individualswith Parkinson’s disease. Following
that, he used the method again, thistime discovering among Parkinson’spatients deficits in contrast-sensitivity— difficulty distinguishing an imagefrom its background.
Importantly, as part of thatresearch, he showed that vision changesin tandem with neurological function-ing. “When a patient doesn’t movewell,” Dr. Bodis-Wollner explains, “hedoesn’t see well.”
Motor problems in Parkinson’s dis-ease are caused by the death of neuronsthat secrete and process an importantneurotransmitter called dopamine. Dr.Bodis-Wollner ’s research establishedthat the death of these neurons, called“dopaminergic” cells, is also responsiblefor Parkinson’s-related visual problems.“Without dopaminergic cells, dopamine-sensitive cells are deprived of dopamine”he notes, “and are no longer able tomake very important decisions thatrelate to vision and to motor execution.”
In the late 1990s, intrigued bythe role dopaminergic cells play inthe vision of Parkinson’s patients,Dr. Bodis-Wollner developed a quantita-
An Eye IntoParkinson’s Disease
“The ability to image the retina mayrevolutionize the process of evaluating andmonitoring the neuronal changes that occurin Parkinson’s disease.”
Dr. Bodis-Wollner with M. Asim Javaid, MD, postdoctoral research fellow, Sofya Glazman, MD,coordinator, Parkinson’s Disease and Related Disorders Center of Excellence of the NationalParkinson Foundation.
FIG 1 FIG 2
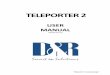
Fig 1 The OCT of the retina of a healthy subject (46 years of age). Thebottom of the picture represents the outer layers of the eye; the top, theinner layers. The dip, or “valley”, in the center is normal: retinal neuronsare pushed to the side to allow light to penetrate to the outer layers,where photoreceptors are located.
Fig 2 The OCT of the retina of a Parkinson’s disease patient (50 years ofage). The “valleys” - top and center - represent the loss of neurons in theinner retina, including the nerve cells which transmit visual information tothe brain.
access to cell counts could dramaticallyalter the course of clinical trials for newParkinson’s treatments.
Until recently, “investigators havehad to rely on clinical observations andwait a minimum of 18 months to discov-er the impacts of potential neuroprotec-tive treatments on the brain’s dopamin-ergic pathways and, thus, on disease pro-gression,” Dr. Bodis-Wollner explains.With the detailed counts of retinaldopaminergic cells and information on
retinal thinning that advanced OCTequipment can provide, researchers maybe able to assess much more quickly andaccurately whether a new treatment hasarrested neuronal degeneration.
Dr. Bodis-Wollner notes, “OCTshould be able to help quite a lot in ourquest for neuroprotective agents —agents that can stop the dying-off ofdopaminergic cells.” And with that, helpstop the progression of Parkinson’s dis-ease itself.
Ivan Bodis-Wollner, MD, DSc

W illiam J. Brunken, PhD, iskeenly interested in the archi-tecture of the eye’s light-sensi-
tive inner layer, the retina.“As an undergraduate,” says Dr.
Brunken, an associate professor ofanatomy and cell biology, ophthalmolo-gy, and neurology, “I got hooked on theretina’s elegantly organized structure.Its columnar organization is very care-fully constructed, with a gorgeous sym-metry to it.”
Dr. Brunken, director of SUNYDownstate’s division of ophthalmicresearch, explores the molecular signalsthat create, maintain, and sometimesdeform and destroy that structure.
His investigations into proteinsfound in the retina’s extracellularmatrix, the biological scaffolding thatbinds its cells together, may lead totreatment breakthroughs for a numberof ocular diseases. These include dia-
betic retinopathy, age-related maculardegeneration, and retinopathy of pre-maturity, a vision-loss problem associ-ated with premature birth. His researchmay even help restore vision to thosewhose retinal problems have resultedin blindness.
Dr. Brunken has spent much of hisrecent career studying two specific retinalproteins, laminins and netrins, which hedescribes as guidance molecules. “Theytell cells where to go and how to functionwhen they get there,” he explains.
Without laminins and netrins, reti-nal development is disrupted and visionitself may well be impossible. Moreover,laminins and netrins “stabilize synaps-es,” the junctions between brain cellsacross which neural communicationtakes place, Dr. Brunken says.
The connections between the light-sensitive cells in the retina and the cellsthat convey visual signals to the brainare held together by laminins, “which arethe chief organizers of one of the retina’sand one of the body’s, most importantstructures: the basement membrane.”
In a series of papers published inNeuron and the Journal of Neuroscience,Dr. Brunken and his group were the firstto demonstrate the presence of nativelaminins in the central nervous system.
Basement membranes in the retina,and elsewhere, serve as platforms ontowhich cells attach themselves. They alsoorient tissue development, “telling cellswhat is top and what is bottom, andtherefore how cells should organizethemselves,” Dr. Brunken notes. “Theseproperties make them critical for retinaldevelopment. If the basement mem-brane doesn’t form properly, then theattachment of cells is irregular and theretina’s columnar organization, and itsability to transmit visual signals, is lost.”
Dr. Brunken’s lab has identified fourof the approximately forty laminin vari-ants that are active in retinal tissue.Mutations in one of the genes that pro-duces the laminin beta-2 protein, a genecalled LAMB2, “completely disrupts vas-cularization of the retina during fetaldevelopment,” Dr. Brunken notes. “What
William J. Brunken, PhD
results is a very altered pattern of vascu-larization, much like one sees in childrenwith retinopathy of prematurity, whereinflammation and, eventually, the deathof retinal tissue, disrupts the visual field.”
Other laminin mutations lead to rarebut complex diseases that involve the eyealong with other bodily systems. These dis-eases include Pierson syndrome, Merosin-dependent muscular dystrophy, and Herlitzjunctional epidermolysis bullosa.
Dr. Brunken has created a mousemodel in which two laminin genes havebeen removed. These mice have all thesymptoms of eye-brain-muscle disease,a complex neurodevelopmental disorder.
Of particular interest to Dr. Brunkenis the role netrins play in the retina’sorganizing structure. “A netrin is noth-ing more than a small piece of alaminin,” he explains. “Laminins arecross-shaped molecules and netrins arethe ends of the arms of the cross.”
Working with Manuel Koch, PhD, of theUniversity of Cologne, in Germany, Dr.Brunken’s lab discovered that a noveltype of netrin, called netrin-4, regulatesaxon guidance in the retina.
“Netrin-4 helps bundle axons in theretina together, enabling communica-
tion between the retina and the rest ofthe brain’s visual apparatus,” Dr.Brunken says. Perhaps, most important-ly, netrin-4 regulates the branching ofthe retina’s deepest capillaries.
Understanding the basic functionsof these proteins may lead to new treat-ments for a number of eye diseases, Dr.Brunken says. “If we can separate out
the cell-binding domains — the partsthat interact with receptors on cellmembranes of molecules — we can usethose pieces for drug development.”
Dr. Brunken’s investigations mayalso lead to a new way of treating visionloss from retinal defects. “Given that
laminins and netrins are guidance mol-ecules and stabilize synapses,” Dr.Brunken explains, “we hope we canincorporate them into a microchip-based neuroprosthesis that would pro-mote a kind of synapse between theprosthesis and the retina. The hopewould be to fool neurons into thinking asilicon chip is a photoreceptor.”
Members of Dr. Brunken’s lab: (left to right) Aarti Kuver, PhD student; Zeng-Xiu Liu, MSc, research associate;Dr. Brunken; Germán Pinzón-Duarte, MD, research associate; Gopalan Gnanaguru, PhD student.
Dow
nst
ate
Res
earc
h2008
18
RETINOPATHY RESEARCH William J. Brunken, PhDD
own
stateR
esearch2008
19
FIG 1
Dr. Brunken’s investigations may also lead to anew way of treating vision loss from retinaldefects. “The hope would be to fool neuronsinto thinking a silicon chip is a photoreceptor.”
The Exquisite Beauty ofOcular Architecture
FIG 3
FIG 2
Fig 1. A section of the mouse retina stained with fluorescent proteinmarkers. Support cells, Müller glia (green), span the whole retina and adhere tothe retinal basement membrane (red line at bottom of the figures); the adhesionpoints are yellow. Some genetic deletions of laminins (B and D but not C) causealterations in Müller cell and, secondarily, in retinal anatomy.
Fig 2. The development of retinal blood supply is dependenton laminin synthesis. Blood vessels spread over the normal reti-na (left side, overview) forming three different capillaries networksat the surface, in the middle, and deep within the retina. In animalswith laminin gene deletions (right column) the development ofblood vessels is altered dramatically. The entire surface of the reti-na is not covered with blood vessels (overview) and the branching ofall three levels of the capillaries are disrupted. These effects mimic ahuman disease called retinopathy of prematurity, a blinding disorderfound in some premature children.
Fig 3. Blood vessels are under-developed in laminin mutants.

20
Dow
nst
ate
Res
earc
h2008
RETINOPATHY RESEARCH Brahim Chaqour, PhD
blood sugar levels), plays a crucial rolein all phases of diabetic retinopathy.Working in tissue culture and with lab-oratory animals, he has documentedhow these genes, normally active onlyduring embryonic and fetal develop-ment, initiate the weakening of healthyretinal blood vessels and promote theformation of new, leaky ones.
On a fundamental level, Dr.Chaqour is interested in the ways thatcellular environment affects cellbehavior. In the hyperglycemic milieuof the diabetic retina, the pericytes,the smooth muscle cells forming theouter layer of capillaries, begin to die.That process further deprives the reti-nal tissues of oxygen. Dr. Chaqourand his colleagues discovered thatwhen this oxygen deprivation occurs,two long-dormant genes, Cyr61 andCTGF, from the family Dr. Chaqourhas identified begin to express them-selves in the retina. Their proteinsaccumulate in the space surroundingblood vessel cells, further exacerbatingpericyte death.
That’s not the only role Cyr61 andCTGF play in diabetic retinopathy.During the most advanced stage of dia-betic retinopathy, their over-expressioncontributes to the uncontrolled prolif-eration of new, leaky blood vessels, Dr.Chaqour has concluded. “The proteinsthese genes express even cause bloodvessels to grow into the eye’s vitreousgel, which, under normal conditions,is completely free of blood vessels.There’s no control mechanism inthese newly activated genes that allowsthem to stop.”
Dr. Chaquour ’s lab discovered thatvasculogenesis, the creation of entirelynew blood vessels from stem cells, ispromoted by the Cyr61 protein as well.Until recently, scientists believed thatangiogenesis — the branching off of
new blood vessels from existing ones— was the only blood vessel-formationmechanism involved in the disease. Infact, “scientists believed vasculogene-sis took place only during embryonicdevelopment and then stopped alto-
gether,” he says. By exposing stem cellsto Cyr61 in tissue culture, Dr.Chaqour and his colleagues demon-strated “this protein promotes theprocess of vasculogenesis involved indiabetic retinopathy.”
Another of his important discoveriesis a protein called MMP-2. “In the normalretina,” Dr. Chaqour explains, “there’salmost no MMP-2. But in diabetic ani-mals, Cyr61 and CTGF induce expres-sion of MMP-2.” The protein destroys theextracellular matrix, the biological scaf-folding that stabilizes and connects cells.“This further degrades the pericytes.”
Dr. Chaqour is using these discover-ies to develop pharmacological treat-ments that may derail diabetic retinopa-thy, even in the absence of tight bloodsugar control. “We’re trying,” he says,“to put together recombinant peptidesthat will interrupt the growth of abnor-mal blood vessels and allow healthy reti-nal activity to occur.”
Already, Dr. Chaqour and his col-leagues developed several compounds,still unnamed, that block the destruc-tive action of MMP-2. “That’s not
enough to stop diabetic retinopathy,yet,” Dr. Chaqour says. “But it’s astart. One day, we may discover apharmacological treatment thatenables patients to avoid the currentsurgical one.”
Dow
nstate
Research
2008
21
B etween 12,000 and 24,000Americans go blind each yearas a result of diabetic retinopathy.
Diabetic retinopathy usually devel-ops over several years and has its originsin the body’s poor control of blood sugarlevels. At the onset, the tiny blood ves-sels in the retina begin to swell and leak.Next, some of these vessels close off.Then, as more of them are blocked, theretina sends molecular signals that initi-ate a frenzied formation of new and frag-ile blood vessels. In the advanced stages,called proliferative retinopathy, theseweakened vessels invade the vitreous gelthat fills the eye; when they leak, severevision loss or blindness results.
To date, a high-tech vision-savingtechnique called scatter laser surgerycan, when administered early, improvethe vision of people with diabeticretinopathy. But the procedure has limi-tations. Often, it can lead to the loss ofperipheral vision, and, because newblood vessels continue to grow, the pro-cedure must be repeated.
To develop better treatments forthis vision-impairing disease, BrahimChaqour, PhD, an assistant professorof anatomy and cell biology at SUNYDownstate, is decoding the molecularprocesses that underlie diabeticretinopathy. “My goal is to understanda number of mechanisms that affect
blood vessel growth and degeneration,”he says. These include the role ofangiogenic factors, which lead to theproliferation of new blood vesselbranches, and the role of anti-angio-genic factors, which lead to thedestruction of pre-existing blood ves-sels and the formation of new bloodvessel branches.
“A better understanding at themolecular level will help us learn how tocontrol the process, both in the earlyand later stages of the disease,” he says.
Dr. Chaqour has made greatprogress towards this goal. He has iden-tified a “small family of genes,” that, inthe presence of hyperglycemia (high
Image 1: A well-organized and functional network of blood vessels in the retina of an adult rat.Image 2: A disorganized and dysfunctional network of blood vessels in the retina of an adult diabetic rat.Image 3: An extensive degradation of blood vessels in the retina of a diabetic rat. Diabetes activates specific proteases responsible for the destruction ofretinal vessels during diabetes.
Members of Dr. Chaqour’s lab: (from left to right) Jorge Espinoza, PhD student; Dr. Chaqour; Haibo Liu, PhD, postdoctoral fellow; and Hunter Collegeinterns Michelle Lee and Tyesha Williams.
Decoding DiabeticRetinopathy
Image 1 Image 2 Image 3
Dr. Chaqour has identified a “small family ofgenes,” that, in the presence of hyperglycemia,plays a crucial role in all phases of diabeticretinopathy.
Brahim Chaqour, PhD

22
W hoever said the “eyes are thewindow to the soul” nevermet Daniel Rosenbaum, MD,
chairman of neurology at SUNYDownstate.Given the nature of Dr.
Rosenbaum’s research into the retina,the light-sensitive inner layer of the eye,the phrase might be slightly amendedto: “the eyes are the window to the souland the gateway to the brain.”
The retinas are actually outcrop-pings of brain tissue. For Dr.Rosenbaum, intent on better under-standing the causes of major strokesand developing treatments that mayone day ameliorate or even preventthem, the eye has proven to be anideal, if unanticipated, area of study.“Originally, I began my research in thebrain itself,” says Dr. Rosenbaum.“But, because of the eye’s accessibility,there are certain topics that are much
more readily researched there than inthe brain itself.”
Among those topics are the types ofdamage that occur in neural tissue
when it’s deprived of oxygen and glu-cose, as happens during a stroke.Using rodent models, Dr. Rosenbaumis making important breakthroughs,discovering that some stroke-inducedbrain damage can be limited throughthe use of strategies that interrupt celldeath. In addition, his research sug-gests the body’s own protective mech-anisms may be mobilized to protectthose at highest risk for strokes.
What type of death do brain cellsundergo during a stroke? Researchersassumed it was necrosis, a passiveform of cell death “in which the cellssimply explode,” Dr. Rosenbaumexplains.
In the early 1990s, however, Dr.Rosenbaum demonstrated that necro-sis was far from the only type ofcell death involved. “In cerebralischemia,” a consequence of a strokeor other condition causing inadequateblood supply, “the brain area that’smost significantly ischemic, the core,will undergo necrotic cell death,” Dr.Rosenbaum notes. “But there’s aregion surrounding the core, thepenumbra, where the damage may notbe severe enough to actually kill thecells immediately.”
However, many of those cellseventually die off. Why? Because ofapoptosis, or so-called programmedcell death.
Dr. Rosenbaum was among thefirst to demonstrate this phenomenonin neurons outside a stroke’s core areaof impact. Apoptosis is the body’s“systematic and planned dismantlingof cells,” Dr. Rosenbaum explains. (Inthe study that led to this discovery, asin many others, Dr. Rosenbauminduced ischemia in his laboratoryanimals by restricting blood flow tothe retina.)
“The distinction between apoptosisand necrosis is a vitally important one,”Dr. Rosenbaum continues, “because ifit’s an active form of cell death, we can
Daniel Rosenbaum, MD
Frank Barone, PhD, director, basic research in cerebrovascular disease; Joel David, lab technician;and Dr. Rosenbaum.
Dow
nst
ate
Res
earc
h2008
RETINOPATHY RESEARCH Daniel Rosenbaum, MD
intervene and prevent cells from dying.With necrosis, we can’t.”
Indeed, in a study published in1997 in the journal Vision Research,Dr. Rosenbaum was the first todemonstrate that during an ischemicevent in the retina, the application of acompound called aurintricarboxylicacid halted apoptosis and thus pre-served retinal function.
Ultimately and unfortunately, aur-intricarboxylic acid proved to presentserious life-risk when used systemical-ly. But Dr. Rosenbaum’s finding wasimportant because it was proof of prin-ciple. “We now know for sure that ifyou find the right strategy, you canlimit some of the apoptosis that occursafter stroke,” he says.
Dr. Rosenbaum’s research has ledto a major discovery: Yet another typeof cell death that occurs duringstroke. Called necroptosis, this typeof cell death shares characteristicswith both apoptosis and necrosis.(The study of cell death involves theuse of an inflammatory cytokinecalled TNF. In the presence ofinhibitors of programmed cell death,or apoptosis, a TNF variant calledTNF-alpha activates and exposesnecroptosis for detailed analysis.) It isa finding that may increase the arse-nal of stroke-fighting drugs becausethe agents that will one day blocknecroptosis “are going to be differentthan the agents that block apoptosisand necrosis.”
In fact, future stroke-blockingagents may be based on molecules pro-duced by the body itself, Dr.Rosenbaum has begun to learn. “One
of the most exciting ways to limitapoptosis is with a compound callederythropoietin (EPO), which the retinabegins to express when it becomesischemic, as if to protect itself,” heexplains. Dr. Rosenbaum hopes EPO,
or a modified version of it, will play aclinical role in limiting cell damageafter stroke.
Similarly, his lab is exploring aphenomenon known as remote pre-conditioning, in which minor ischemicevents protect brain cells from damageduring later, more severe strokes. “Inour animals, we found that if we makethe hind legs ischemic for a short timeand then come back 24 hours later
with a severe insult, we see much lessstroke injury.”
This finding may eventually helpprevent strokes in cardiac bypasspatients, who are at high risk forischemic events. “Perhaps 24 hours
before surgery, we could mimic precon-ditioning, and thereby increase protec-tion against major strokes,” Dr.Rosenbaum explains.
These discoveries could potentiallychange the course of stroke treatmentand the lives of millions of stroke suf-ferers. They have been enabled as muchby Dr. Rosenbaum’s keen, observing eyeas by the eye itself — window to thesoul and gateway to the brain.
Dow
nstate
Research
2008
23
Ampl
itude
(uV
)
-200
200
0 125 250
Time (ms)
Normal Baseline Vehicle TNF-alpha Ab
125125 250250
Time (ms)Time (ms)
TheEye:Gateway to theBrain
Using rodent models, Dr. Rosenbaum is makingimportant breakthroughs, discovering thatsome stroke-induced brain damage can belimited through the use of strategies thatinterrupt cell death.
Cryosections of rat retina at different time points subsequent to 60 minutes of retinal ischemia. One can see that TNF-alpha is expressed following ischemicinjury to the retina. By blocking TNF-alpha activity, one may be able to protect the retina against cell death.
Electroretinography (ERG) tests retinal function. By blocking TNF-alpha activity before and even afterthe ischemic insult, one can see protection of retinal function following the ischemic insult.

Dow
nst
ate
Res
earc
h2008
24
RETINOPATHY RESEARCH Gladys Teitelman, PhD
including connective tissue growthfactor (CTGF), cystein-rich protein(Cyr61), and nephroblastoma overex-pressed gene (NOV), which play a rolein new blood vessel formulation andappear to be involved in the initiation ofretinopathy’s pathological changes (see,Brahim Chaquor, “Decoding DiabeticRetinopathy,” p.20, for more informa-tion on CCN proteins).
Dr. Teitelman and her team are specif-ically focusing on the action of CTGF.“We’re making progress in understandinghow we might be able to interrupt itsdestructive action in the eye,” she says.
Under normal conditions, CTGF isinvolved in a host of healthy biologicalprocesses that include wound healing,cell division, and nerve conduction. Inthe diabetic eye, however, its action canbe life altering.
“Because CTGF is involved in somany important biological processes,
it’s not a good target for a systemic ther-apy,” observes Ms. Winkler. “But theeye is encapsulated. Which means wecan block the action of CTGF in the eyewithout concern for the treatment’s
Dow
nstate
Research
2008
25
I n the United States, almost 21 mil-lion people — 7 percent of the popu-lation — are diabetic. Of these 21
million, an estimated 40 to 45 percentwill eventually suffer from diabeticretinopathy, the leading cause of blindnessamong American adults.
Diabetic retinopathy has its originsin poor control of blood sugar levels. Inthe eye, high levels of circulating bloodsugar, a condition called hyperglycemia,set off a years-long reaction that resultsin the formation of new, fragile bloodvessels that grow along the retina and
into the eye’s clear vitreous gel. Ideally,people with diabetes can slow or evenhalt the advance of diabetic retinopathyby keeping their blood sugar levels undertight control. Such control, however, isdifficult to achieve for the large majorityof people with diabetes.
But what if unrestrained blood ves-sel growth, called proliferative retinopa-thy, could be kept in check with arecombinant molecule administered byinjection or through eye drops?
That’s the possibility being investi-gated by Gladys Teitelman, PhD, profes-
sor of anatomy and cell biology, and thetwo members of her lab, graduate stu-dent Jennifer Winkler and research sci-entist Mamdouh Kedees, PhD.
Dr. Teitelman is a diabetes researcherwhose primary focus is the regenerationof insulin-producing B-cells in the pan-creas (see Profiles in Innovation, 2007).Yet, she finds this new avenue of diabetesresearch and “the possibility that wemight be able to intervene in diabeticretinopathy” compelling.
One promising focus involvesproteins belonging to the CCN family,
Restraining AbnormalBlood Vessel Growth in the Retina
When blood vessels of the retina are infused with a red dye, leakage of the dye is found in retina of diabetic rats, but not in retina of rats with normalblood glucose levels. Arrow indicates area of leakage in the diabetic retina.
impact on the rest of the body.”Working first in tissue culture and
then in diabetic laboratory rats, Dr.Teitelman and her team have devel-oped recombinant molecules that bindto CTGF and prohibit its production.In their first experiment, the team useda bioengineered virus that reduced
CTGF expression by 70 percent in cellsin culture. Now, Dr. Teitelman’s lab isusing a small interfering RNA (sIRNA)to accomplish the same task in labora-tory rats with induced diabetes.
“One of sIRNA’s benefits is that it’svery small — about a tenth of the size ofthe virus we engineered,” says Dr.Kedees. The smaller size means anytreatment that involves sIRNAs will beless likely to provoke immune orinflammatory responses.
Moreover, using sIRNAs rather thanviruses will facilitate a treatment’sentrance into involved cells, since virus-es enter cells through receptors on thecells’ surfaces. During this process,viruses’ relatively large size can hindertheir entrance. “sIRNA, on the otherhand,” Dr. Teitelman says, “is smallenough to enter the cell simply throughdiffusion,” by the natural movement ofmolecules in the body.
Dr. Teitelman is hopeful the team’sresearch will result in an effective treat-ment for what is becoming, in theUnited States and around the world, anincreasingly common illness. “With thefirst sign of diabetic retinopathy — thepresence of leaky blood vessels, forinstance — we may be able to interveneand prevent further complications of thedisease,” she explains.
Of course, Dr. Teitelman notes,“glycemic control is always importantin preventing diabetic retinopathy. Butgiven how hard that is to achieve, wemust also pursue research that canlead to effective, minimally invasivetreatments.”
Dr. Teitelman and Jennifer Winkler, PhD student.
Mamdouh Kedees, PhD
But what if unrestrained blood vessel growth,called proliferative retinopathy, could be kept incheck with a recombinant molecule administeredby injection or through eye drops?