Embed Size (px)
Citation preview
1
An Automated Immunoblot Method for Detection of IgG Antibodies to 1
Hepatitis C Virus: a Potential Supplemental Antibody Confirmatory Assay 2
3
Running title: Anti-HCV Confirmatory assay 4
5
Maja Kodani#, Miranda Martin, Vivianne Landgraf de Castro, Jan Drobeniuc and Saleem Kamili 6
7
Division of Viral Hepatitis, National Center for HIV, Hepatitis, STD and Tuberculosis Prevention, Centers 8
for Disease Control and Prevention, Atlanta, GA 30329 9
10
11
12
Author for Correspondence: 13
Maja Kodani, Ph.D. 14
Centers for Disease Control and Prevention 15
1600 Clifton Road 16
Atlanta, GA 30329 17
404-639-1015 18
20
JCM Accepted Manuscript Posted Online 16 January 2019J. Clin. Microbiol. doi:10.1128/JCM.01567-18This is a work of the U.S. Government and is not subject to copyright protection in the United States. Foreign copyrights may apply.
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
2
ABSTRACT 21
An estimated 41,200 people were newly infected with hepatitis C virus (HCV) in 2016 in the United 22
States. Screening tests for antibodies to HCV may generate up to 32% false positivity in low-risk 23
populations. Current Centers for Disease Control and Prevention (CDC) screening recommendations do 24
not require confirmatory testing of a screening anti-HCV positive test, however confirmation is 25
valuable for surveillance in the absence of HCV RNA testing. Recombinant Immunoblot Assay (RIBA) 26
was used as a confirmatory assay for anti-HCV reactive samples but was discontinued in 2013. Another 27
anti-HCV confirmatory assay, INNO-LIA, is commercially available in Europe but not approved by the 28
Food and Drug Administration (FDA) in the United States. We report the development of an anti-HCV 29
assay performed on an automated immunoblot platform using a fourth generation HCV recombinant 30
fusion protein. Based on testing of 70 well characterized samples of which 40 were HCV RNA and anti-31
HCV positive, 15 HCV RNA positive/anti-HCV negative and 15 HCV RNA and anti-HCV negative, the 32
specificity and sensitivity of the HCV-WES assay was 100% and 95%, respectively. Concordance 33
between INNO-LIA and HCV WES, was determined by testing 205 HCV RNA negative/anti-HCV positive 34
samples, of which 149 (72.7%) were positive by HCV-WES, while 146 (71.2%) were positive by INNO-35
LIA. We have shown proof of concept for the use of this test for confirmation of screening anti-HCV 36
results. The HCV-WES assay is advantageous over manual western blot assays and INNO-LIA including 37
ease of use, low cost and reduced hands-on time. 38
39
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
3
INTRODUCTION 40
Hepatitis C virus (HCV) is a major public health problem worldwide with an estimated 71 million 41
individuals living with chronic HCV infection in 2015 (1). In the United States (US) from 2003 to 2010, 42
there were an estimated 4.6 million Americans infected with HCV, 3.5 million of whom were estimated 43
to be current cases (2). An estimated 41,200 people were newly infected with HCV in 2016 in the US 44
(3). Furthermore, it is estimated that more than half of the people infected with HCV may not be 45
aware of their infection status (4). Testing data from a large US commercial laboratory suggest that an 46
estimated one in four HCV-infected people in the US have significant liver disease and could benefit 47
from treatment (5). 48
The Centers for Disease Control and Prevention (CDC) recommends determining current HCV 49
infection status by screening for HCV antibodies (anti-HCV), followed by testing for HCV RNA if the HCV 50
antibody test is reactive (6) to facilitate linkage to care and treatment with currently available highly 51
efficacious direct acting anti-viral agents (DAAs). Anti-HCV assays have a lower positive predictive value 52
in low prevalence populations. A recent study showed up to 32% anti-HCV false-positivity in a national 53
US based surveillance study (7). Although positive results for anti-HCV and HCV RNA test indicate 54
current HCV infection, anti-HCV positive and HCV RNA negative results indicate past resolved infection 55
or no infection, i.e., a false-positive anti-HCV test result. 56
In population studies of the true prevalence of HCV infection, a second anti-HCV test is 57
necessary to confirm the first anti-HCV positive test result. Currently there are no FDA-approved 58
supplemental anti-HCV confirmatory assays commercially available in the United States. Supplemental 59
anti-HCV confirmatory tests, such as INNO-LIA, a Line Immuno Assay (LIA®) (Fujirebio, Sweden) or HCV 60
blot 3.0 (MP Biomedicals, L.L.C., San Diego, CA), are commercially available in Europe but not in the 61
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
4
United States. Furthermore, INNO-LIA test requires hours of hands-on time to results and complicated 62
analysis of test results. In this study, we used a recently automated blotting technology, the Simple 63
WesternTM (ProteinSimple, San Jose, CA), to develop a confirmatory anti-HCV assay (HCV-WES) using a 64
commercially available recombinant HCV fourth generation antigen containing core, and non-structural 65
proteins NS3, NS4 and NS5. This assay was evaluated using a set of well characterized 275 66
serum/plasma samples previously tested for anti-HCV and HCV RNA with other tests. 67
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
5
RESULTS 68
Relative Range and Reproducibility of the HCV-WES Assay. A well-characterized anti-HCV positive 69
human serum sample diluted in four-fold dilutions (neat, 1:16, 1:64, and 1:256) and tested in triplicate 70
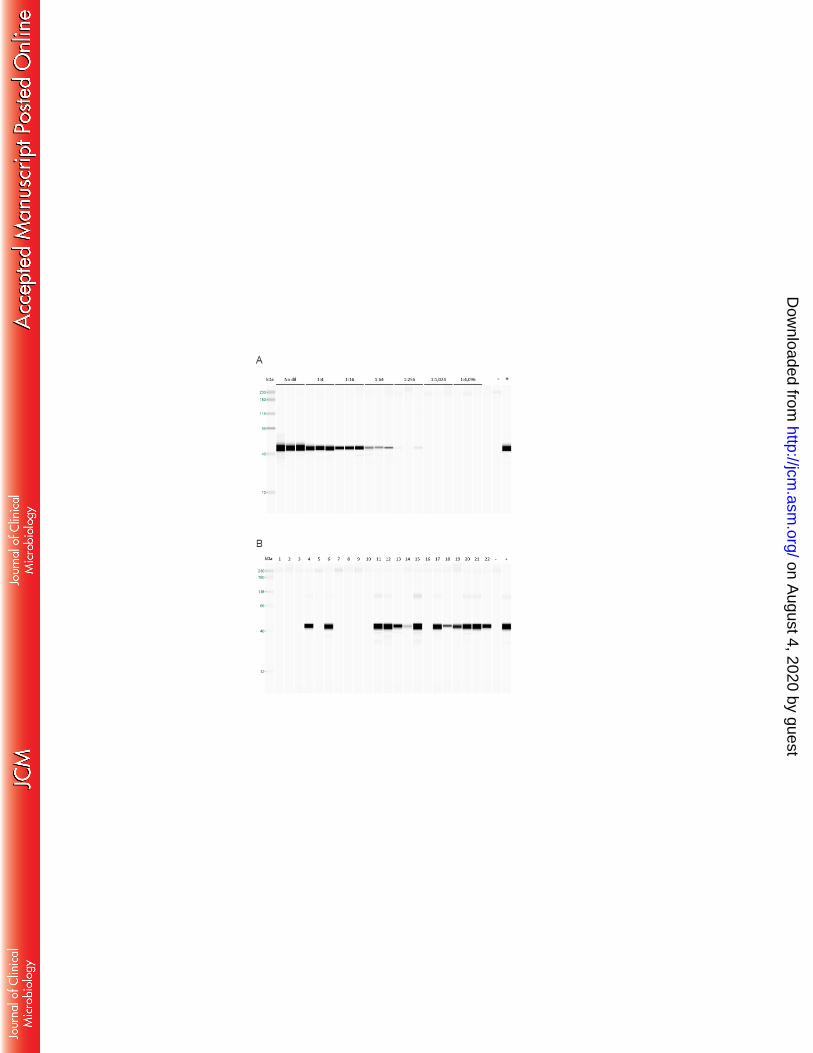
was used to evaluate the dynamic range and reproducibility of the HCV-WES assay (Figure 1). All 71
triplicate dilutions less than the 1:256 dilution produced positive bands, while two of the three 1:256 72
dilution were positive (Figure 1a). All other dilutions were negative. Twenty two serum/plasma 73
samples including negatives, and a range of signal from positives are shown in Figure 1b. Anti-HCV 74
negative specimens tested negative by HCV-WES while screening anti-HCV positive samples tested 75
positive. 76
Performance of HCV-WES in Clinical Specimens. The specificity of the HCV WES assay was determined 77
by testing 30 anti-HCV negative serum/plasma samples from patients which included equal number of 78
HCV RNA negative and HCV RNA positive samples (window period of infection). All 30 samples tested 79
negative by HCV-WES, suggesting the specificity to be 100% compared to VITROS anti-HCV IgG 80
chemiluminescence assay (Ortho Clinical Diagnostics, Raritan, NJ) (Figure 2). 81
The sensitivity of HCV-WES was determined with 40 anti-HCV positive/RNA positive 82
serum/plasma samples; 38 (95%) were confirmed positive by HCV-WES, while 39 (97.5%) were 83
confirmed positive by INNO-LIA compared with RNA positivity test as the gold standard. One anti-HCV 84
and HCV RNA positive sample was missed by HCV-WES only, and this may have occurred due to 85
sensitivity of the test or antigen incompatibility. Concordance between HCV-WES and INNO-LIA was 86
determined using an additional equivocal panel of 205 samples which were anti-HCV positive but HCV 87
RNA negative: 149 (72.7%) were confirmed anti-HCV positive using HCV-WES, while 146 (71.2%) were 88
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
6
confirmed with INNO-LIA (Figure 2). Almost 15% (30) samples were determined to be indeterminate 89
using the INNO-LIA, while HCV-WES scored 16 of these samples as anti-HCV positive. 90
Performance of HCV-WES using Seroconversion Panels. Eight commercially available seroconversion 91
panels were used to evaluate the performance of HCV-WES. Twenty anti-HCV negative samples in 92
three panels (PHV 929, PHV 928, and PHV 927) also tested negative by HCV-WES (data not shown), 93
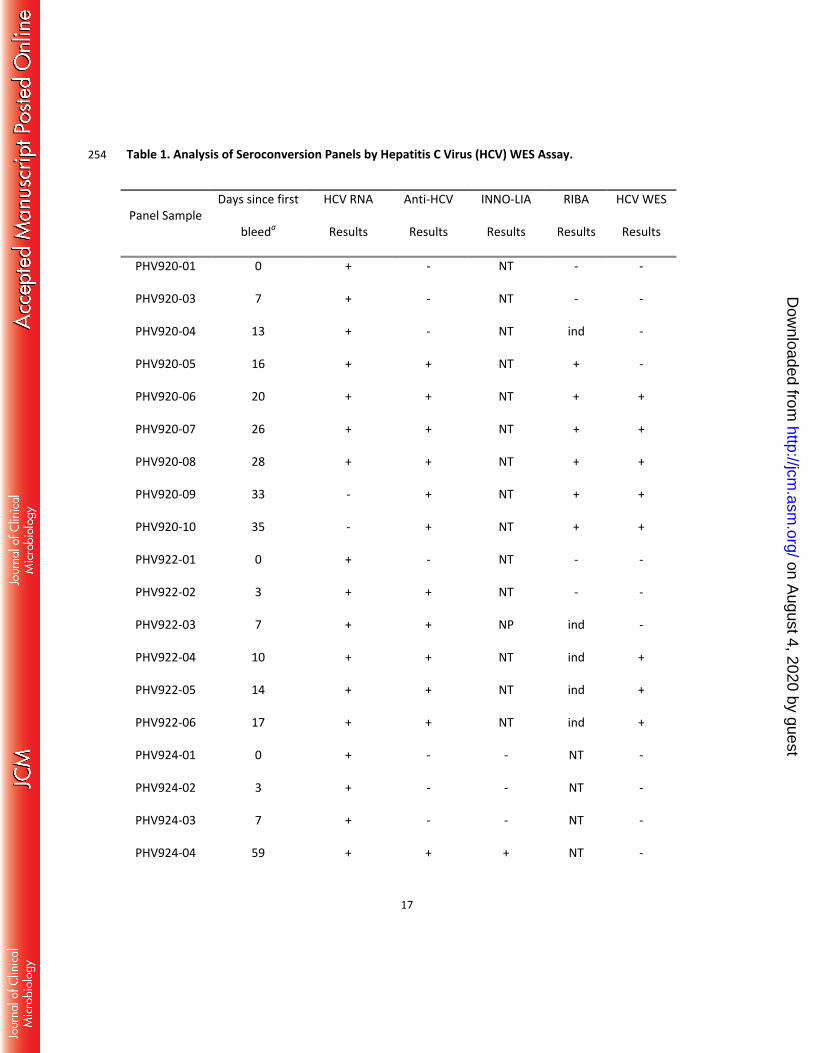
suggesting 100% specificity on this set of panels. Timing of the confirmation of anti-HCV of HCV-WES 94
occurred one week later than the confirmation by INNO-LIA as shown in Table 1 in panels PHV 920(M), 95
PHV 922, PHV 913, and PHV 926. 96
97
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
7
DISCUSSION 98
This study describes the development of a novel serologic assay using, for the first time Simple 99
WesternTM technology for detection and confirmation of anti-HCV in clinical samples. The system has 100
previously been used for detection of serum antibodies in Salmonella infected chicken (8), in vaccine 101
development (9) and utilized in place of traditional Western blots in numerous applications (10-14). 102
Simple WesternTM offers such advantages as standardization, higher reproducibility, elimination of 103
human error due to automation, and substantial savings of time relative to traditional Western blot 104
(15). WES workflow consists of about 30-60 minutes of hands on time to prepare up to 25 samples for 105
immunoblot analysis, which is followed by a three hour run on the instrument. The results are 106
available immediately upon the completion of the run. This is substantial improvement from a 107
traditional Western blot or INNO-LIA, which both require multiple steps, such as washes and 108
incubations, usually requiring more than one working day from sample to results. 109
In clinical setting, the CDC recommends determining current HCV infection status by screening 110
for HCV antibodies (anti-HCV), followed by testing for HCV RNA if the HCV antibody test is reactive (6). 111
However, in population studies where HCV RNA test is often not feasible, false positivity by anti-HCV 112
assays has been demonstrated, and it can inflate the estimated prevalence rate of HCV infection (7). 113
Anti-HCV assays have a lower positive predictive value in low prevalence populations. Previously, all 114
anti-HCV reactive samples were either confirmed by a signal-to-cutoff threshold or RIBA (17) and all 115
previous estimates have been established based on that antibody confirmation. There is no alternative 116
FDA approved confirmatory anti-HCV assay commercially available in the United States since the 117
discontinuation of RIBA. Although positive results for anti-HCV and HCV RNA test indicate current HCV 118
infection, anti-HCV positive and HCV RNA negative results indicate past resolved infection or no 119
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

8
infection, i.e., a false-positive anti-HCV test result. In population studies of the true prevalence of HCV 120
infection, a second anti-HCV test is necessary to confirm the first anti-HCV positive test result. 121
Based on testing of a panel of 70 well characterized samples, the specificity and sensitivity of 122
the HCV-WES assay was 100% and 95%, respectively. Confirmation of true positivity was similar 123
between HCV-WES and INNO-LIA, with HCV-WES discriminating 16 samples that were indeterminate by 124
INNO-LIA. Although WES comes with an initial instrument purchase cost, the HCV-WES assay costs 125
approximately one-third as much per sample as the INNO-LIA assay excluding the costs of importing 126
the INNO-LIA kits into the United States. The HCV-WES assay has other significant attractive features 127
compared to commercial immunoblot assay; these include ease of use, less labor-intensive, faster turn-128
around time of results and a read-out in a digital format that is easily interpretable as positive or 129
negative. 130
In summary, we provided empirical evidence of the accuracy (high sensitivity and specificity) of 131
the HCV-WES assay compared with INNO-LIA test as the gold standards of anti-HCV positivity and 132
negativity. The HCV-WES assay has the potential for use as supplementary anti-HCV confirmatory 133
assay for epidemiologic, surveillance and other population studies of anti-HCV prevalence. 134
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
9
MATERIALS AND METHODS 135
Clinical samples. Human serum or plasma samples used in this study were selected from collections of 136
de-identified convenient specimens archived in our laboratory. All samples used in this study had anti-137
HCV and HCV RNA test results available; anti-HCV status was determined using the VITROS anti-HCV 138
IgG chemiluminescence assay (Ortho Clinical Diagnostics, Raritan, NJ). HCV RNA testing was previously 139
performed using the COBAS Ampliprep/COBAS TaqMan HCV version 2.0 (Roche, Indianapolis, IN). Anti-140
HCV confirmatory testing was performed using the INNO-LIA HCV Score (Fujirebio, Sweden). A total of 141
245 samples were tested which included 205 anti-HCV positive/HCV RNA negative samples, 40 anti-142
HCV positive/HCV RNA positive samples, 15 anti-HCV negative/HCV RNA positive samples, and 15 anti-143
HCV negative/HCV RNA negative samples. In addition, eight commercial HCV seroconversion panels 144
(PHV 913, PHV 920(M), PHV922, PHV 924, and PHV 926, PHV 927, PHV 928 and PHV 929 (SeraCare, 145
Milford, MA)) were also tested by HCW-WES. For these samples, the anti-HCV and confirmatory 146
results were used as reported by the manufacturer. 147
HCV-WES Procedure. A commercially available 4th generation recombinant HCV antigen (46 kDa) 148
(ProSpec Bio, Israel) containing medium size core (55 amino acids), non-structural protein 3 (NS3) (226 149
amino acids), three epitopes from the NS4 protein and three epitopes from the NS5 protein, 150
respectively, was used to detect IgG antibodies to HCV. Prior to loading the samples on the WES 151
Separation Module cartridge (ProteinSimple, San Jose, CA), antigen was diluted 1:500 in 0.1 X sample 152
Dilution Buffer (ProteinSimple, San Jose, CA), and the secondary antibody and plasma samples were 153
diluted 1:2000 and 1:20 in the Antibody Diluent (ProteinSimple, San Jose, CA), respectively. The 154
cartridges were loaded according to the manufacturer’s instructions, with the following modifications: 155
diluted antigen was run in the capillaries as the “sample”, diluted human serum was run as the 156
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
10
“primary antibody,” and the 1:2000 dilution of the goat anti-human IgG labeled with HRP (SeraCare, 157
Milford, MA) replaced the secondary antibody from the Anti-Rabbit Detection Module (ProteinSimple, 158
San Jose, CA). All reagents were loaded into a sample cartridge placed into the automated 159
immunoblotter, WES with the capillary cartridge. The 4th generation antigen was separated in the 160
proprietary separation matrix in the capillaries by size. The binding of the anti-HCV antibodies from 161
the serum or plasma samples are captured/bound to the cross-linked HCV antigen, and a signal is 162
produced from the HRP labeled secondary antibody (Figure 3), which is digitally recorded upon a 163
chemiluminescent reaction. The anti-HCV antibodies from the diluted serum or plasma samples are 164
run over the cross-linked HCV antigen, and the capillary is washed. HRP-labelled secondary antibody is 165
then applied over the bound antibodies, and washed again. The signal, produced upon the primary 166
antibody from human serum or plasma binding to the anti-HCV antigen, is measured and digitally 167
recorded after a five second exposure. Compass software, supplied by ProteinSimple, captures data as 168
a chemiluminescent image of the capillary. The software determines when the signal is higher than the 169
noise and records it in the form of peaks or bands (both views are available). The background 170
determination is based on a “dark” image where the loaded capillaries (i.e. immobilized proteins and 171
antibodies) is taken just prior to substrate loading (e.g. luminol/peroxide). This will capture any 172
artifacts derived from sources not induced by the enzymatic reaction. Next, the substrate is loaded and 173
a subsequent image is captured with emission from the luminol. Compass will then subtract the 174
emission image with the dark image “pixel for pixel” to determine corrected signal responses. A system 175
control, provided in the running buffer, is used with every sample to monitor uniformity of separation 176
between different cappilaries. In the case of HCV-WES, if a band of 42 kDa is detected by the 177
instrument, the sample is considered anti-HCV positive regardless of the band intensity value. 178
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
11
HCV INNO-LIA Procedure. Seroconversion panels and a subset of samples used in the evaluation 179
panels were previously tested by RIBA and/or INNO-LIA by the panel manufacturer (SeraCare, Milford, 180
MA); however confirmatory anti-HCV results were not available for 40 samples. These samples were 181
tested using the INNO-LIA HCV Score (Fujirebio, Belgium), according to the manufacturer’s 182
recommendations. 183
184
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
12
DISCLAIMER 185
The findings and conclusions in this paper are those of the authors and do not necessarily represent 186
the views of the Centers for Disease Control and Prevention. Use of trade names is for identification 187
only and does not imply endorsement by the U.S. Department of Health and Human Services, the 188
Public Health Service, or the Centers for Disease Control and Prevention. 189
190
ACKNOWLEDGEMENTS 191
The authors would like to thank Laurie Barker and Tonya Hayden for critically reading the manuscript 192
and help with editing, as well as David Sloan from ProteinSimple for clarifying how the background is 193
subtracted by the instrument. 194
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
13
FIGURE AND TABLE LEGENDS 195
Figure 1. Anti-HCV Results Using HCV-WES Assay. This figure represents two different runs on the 196
WES instrument in the form of gels. The first lane of every gel is a dedicated molecular marker lane 197
while the last two were a positive (+) and a negative (-) control. (A) Serial dilution of an anti-HCV 198
positive control sample tested in triplicate to demonstrate the range and reproducibility of the assay. 199
(B) A random selection of a variety of clinical specimens shows anti-HCV negative (lane 1–3, 5, 7–10, 200
and 16) and positive (lanes 4, 6, 11–15, and 17–22) samples, ranging from weak (lane 14) to strong 201
positives (lane 15). 202
Figure 2. Clinical Sample Testing Results. 245 serum/plasma samples were chosen for this study 203
based on their anti-HCV and HCV RNA status, as shown in the second row of boxes. The results 204
obtained by HCV-WES and INNO-LIA, including both the number of samples and percent from the total 205
for that category are shown in the third row. NT, not tested. 206
207
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
14
REFERENCES 208
1. Global hepatitis report 2017. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 209
IGO. 210
2. Edlin BR, Eckhardt BJ, Shu MA, Holmberg SD, Swan T. 2015. Toward a more accurate estimate of 211
prevalence of hepatitis C in the United States. Hepatology 62(5):1353-63. 212
3. CDC. Surveillance for Viral Hepatitis – United States, 2016. Accessed April 17, 2018.4. Holmberg SD, 213
Spradling PR, Moorman AC, Denniston MM. 2013. Hepatitis C in the United States. N Engl J Med 214
368(20):1859-61. 215
5. Kleveens RM, Canary L, Huang X, Denniston MM, Yeo AE, Pesano RL, Ward JW, Holmberg, S. 2016. 216
The burden of hepatitis C infection-related liver fibrosis in the United States. Clin Infect Dis 63(8):1049-217
55. 218
6. Getchell JP, Wroblewski KE, DeMaria Jr A, Bean CL, Parker MM, Pandori, M, Dufour DR, Busch MP, 219
Meyer WA, Pesano RL, Teo C-G, Beckett GA, Araujo AC, Branson, BM, Drobeniuc J, Hatia R, Holmberg 220
SD, Kamili S, Ward JW. 2013. Testing for HCV infection: an update of guidance for clinicians and 221
laboratorians. MMWR 62:May 7. 222
7. Moorman AC, Drobeniuc J, Kamili S. 2017. Prevalence of false-positive hepatitis C antibody results, 223
National Health and Nutrition Examination Study (NHANES) 2007-2012. J Clin Virol 89:1-4. 224
8. Yeh HY, Serrano KV, Acosta AS, Buhr RJ. 2016. Production of recombinant Salmonella flagellas 225
protein, FlgK, and its uses in detection of anti-Salmonella antibodies in chickens by automated capillary 226
immunoassay. J Microbiol Methods 122:27-32. 227
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
15
9. Rustandi RR, Loughney JW, Hamm M, Hamm C, Lancaster C, Mach A, Ha S. 2012. Qualitative and 228
quantitative evaluation of SimonTM, a new CE-based automated Western blot system as applied to 229
vaccine development. Electrophoresis 33(17):2790-7. 230
10. Rustandi RR, Hamm M, Lounghney JW, Ha S. 2015. Detection of ADP ribosylation in PARP-1 and 231
bacterial toxins using capillary-based western system. Electrophoresis 36(21-22):2798-2804. 232
11. Wang J, Valdez A, Chen Y. 2017. Evaluation of automated Wes system as an analytical and 233
characterization tool to support monoclonal antibody drug product development. J Pharm Biomed 234
Anal 139:263-268. 235
12. Serrano MJ, Ortega FG, Alvarez-Cubero MJ, Nadal R, Sanchez-Rovira P, Salido M, Rodriquez M, 236
Garcia-Puche JL, Delgado-Rodriguez M, Sole F, Garcia MA, Peran M, Rosell, R, Marchal JA, Lorente JA. 237
2014. EMT and EGFR in CTCs cytokeratin negative non-metastatic breast cancer. Oncotarget 238
5(17):7486-97. 239
13. Stentzel S, Sundaramoorthy N, Michalik S, Nordengrun M, Schulz S, Kolata J, Kloppot P, Engelmann 240
S, Steil L, Hecker M, Schmidt F, Volker U, Roghmann M, Broker BM. 2015. Specific serum IgG at 241
diagnosis of Staphylococcus aureus bloodstream invasion is correlated with disease progression. 242
128:1-7. 243
14. Li Q, Sodroski C, Lowey B, Schweitzer CJ, Cha H, Zhang F, Liang TJ. 2016. Hepatitis C virus depends 244
on E-cadherin as an entry factor and regulates its expression in epithelial-tomesenchymal transition. 245
Proc. Natl Acad. Sci U S A 113(27):7620-5. 246
15. Nguyen U, Squaglia N, Boge A, Fung PA. 2011. The Simple Western: a gel-free, blot-free, hands-free 247
Western blotting reinvention. Nature Methods Application Note v-v1. 248
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
16
16. Harding A. 2013. Not Your PI’s Western Blot. Science 339:1100-1103. 249
17. Alter MJ, Kuhnert WL, Finelli L. 2003. Guidelines for laboratory testing and result reporting of 250
antibody to hepatitis C virus. Centers for Disease Control and Prevention. MMWR Recomm Rep. 251
75(Rr-3):1-13. 252
253
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
17
Table 1. Analysis of Seroconversion Panels by Hepatitis C Virus (HCV) WES Assay. 254
Panel Sample Days since first
bleeda
HCV RNA
Results
Anti-HCV
Results
INNO-LIA
Results
RIBA
Results
HCV WES
Results
PHV920-01 0 + - NT - -
PHV920-03 7 + - NT - -
PHV920-04 13 + - NT ind -
PHV920-05 16 + + NT + -
PHV920-06 20 + + NT + +
PHV920-07 26 + + NT + +
PHV920-08 28 + + NT + +
PHV920-09 33 - + NT + +
PHV920-10 35 - + NT + +
PHV922-01 0 + - NT - -
PHV922-02 3 + + NT - -
PHV922-03 7 + + NP ind -
PHV922-04 10 + + NT ind +
PHV922-05 14 + + NT ind +
PHV922-06 17 + + NT ind +
PHV924-01 0 + - - NT -
PHV924-02 3 + - - NT -
PHV924-03 7 + - - NT -
PHV924-04 59 + + + NT -
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
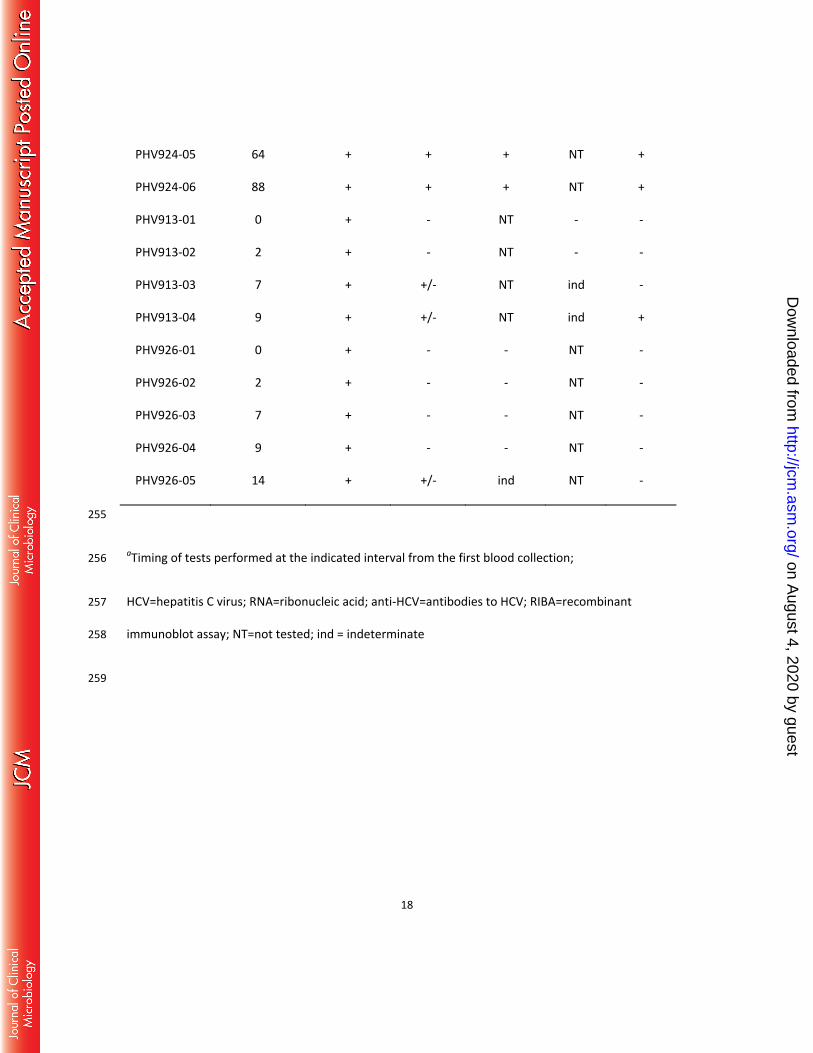
18
PHV924-05 64 + + + NT +
PHV924-06 88 + + + NT +
PHV913-01 0 + - NT - -
PHV913-02 2 + - NT - -
PHV913-03 7 + +/- NT ind -
PHV913-04 9 + +/- NT ind +
PHV926-01 0 + - - NT -
PHV926-02 2 + - - NT -
PHV926-03 7 + - - NT -
PHV926-04 9 + - - NT -
PHV926-05 14 + +/- ind NT -
255
aTiming of tests performed at the indicated interval from the first blood collection; 256
HCV=hepatitis C virus; RNA=ribonucleic acid; anti-HCV=antibodies to HCV; RIBA=recombinant 257
immunoblot assay; NT=not tested; ind = indeterminate 258
259
on August 4, 2020 by guest
http://jcm.asm
.org/D
ownloaded from