Embed Size (px)
Citation preview
Journal of Vimlogical Methods, 16 (1987) 39-44 Elsevier
39
JVM 00578
An assessment of the sensitivity of three methods for the detection of rotavirus
A. L. Martin and E. A. C. Follett
Regional Virus Laboratory, Ruchill Hospital, Glasgow, UK
(Accepted 15 December 1986)
Summary
A comparison was made of the sensitivity of a current commercial ELISA for detecting rotavirus in faecal specimens with the more complex, technically de- manding systems of electron microscopy and polyacrylamide gel electrophoresis. Even after modification, the ELISA failed to detect 22% of specimens with par- ticles identifiable by electron microscopy. Polyacrylamide gel electrophoresis failed to identify 2 out of 50 specimens with particles present but did distinguish 2 group C rotaviruses.
ELISA; EM; PAGE; Rotavirus
Introduction
Rotaviruses are a major cause of nonbacterial gastroenteritis, especially in the young (Bishop et al., 1974). As the human virus cannot be grown readily in tissue culture, a diagnosis of its presence in faeces is usually achieved by either electron microscopy (EM) or immunological assays (Middleton et al., 1977; Yolken et al., 1977; Birch et al., 1979). Diagnosis may also be achieved by demonstration of a unique pattern of double-stranded ribonucleic acid (RNA) in virus particles by po- lyacrylamide gel electrophoresis (PAGE) (Herring et al., 1982; Moosai et al., 1984). Both EM and PAGE require expensive equipment and are technically demanding. Few diagnostic laboratories are so equipped and many have utilised commercial ELISA which require no special equipment or expertise.
In this laboratory, a commercial enzyme-linked immunosorbent assay (ELISA)
Correspondence to: A.L. Martin, Regional Virus Laboratory, Ruchill Hospital, Glasgow G20 9NB, UK.
0166-0934/87~$03.50 0 1987 Elsevier Science Publishers B.V. (Biomedical Division)

40
(Rotazyme I, Abbott Laboratories) has been used in conjunction with EM. The ELISA was used to screen stool samples for the presence of rotavirus, and any positive findings further investigated by EM. When a new test Rotazyme II was
introduced, discrepancies were noticed between Rotazyme and EM positivity. As a result, it was decided to compare the sensitivity of ELISA to EM. In addition, PAGE was carried out on stool extracts where virus was detectable by EM.
Materials and Methods
Specimens
Faecal samples routinely sent to this laboratory for investigation of diarrhoea between April and June 1985, and which were positive for rotavirus by EM were included in the study.
Processing of the specimens and EM
Stools were made to 10% in phosphate-buffered saline (PBS, Dulbecco). After clarification at 1200 x g for 20 min in a bench-top centrifuge, the supernatant was then centrifuged at 200000 x g for 60 min in a SW50 rotor in a Beckman L2 ul- tracentrifuge. The resulting pellet was resuspended in 2-3 drops of a 10% (v/v) Bacitracin solution. One drop of this was mixed with one drop of 3% phospho- tungstic acid (pH 7), placed on a Formvar carbon-coated grid, blotted dry and ex- amined in a Philips 301 electron microscope at a magnification of 57000. The quantity of virus present was scored on a scale of occasional to 4+.
ELISA
Clarified supernatant samples, prior to ultracentrifugation, were used in the Ro- tazyme II (Abbott Laboratories) test system according to the manufacturer’s pro- tocol. Subsequently, the incubation times and temperatures were adjusted as set out in Table 1. In addition, stool slurries in Rotazyme buffer were prepared from
TABLE 1
Incubation time and temperature conditions for the Rotazyme assay.
Sample incubation time and temperature
Conjugate incubation time and temperature
Substrate incubation time and temperature
Rotazyme I Rotazyme II
3h 45°C lh 37°C
lh 45°C Ih 37°C
30 min rt 30 min rt
Overnight Rotazyme
overnight rt
lh 45°C
30 min rt
41
36 stools as described in the manufacturer’s protocol and tested under the condi- tions outlined in Table I.
PAGE
The extraction of viral nucleic acid, its resolution and staining was a slight mod- ification of that described by Herring et al. (1982) (N.F. Inglis, pers. comm.).
Briefly, the stool specimens were diluted 1:4 with TNE buffer (Tris 10 mM, NaCl 0.1 m, EDTA l%, pH 7.5) with I% SDS, and vortexed for 30 s. An equal volume of phenol/chloroform (3:2, v/v) was added to the mixture and vortexed for 1 min. The suspension was centrifuged at 1200 X g and the aqueous phase removed and stored. For electrophoresis, 40 t~_l of the aqueous phase was mixed with 10 JJJ of a marker (Bromphenol Blue O.l%, EDTA 15 mM, sucrose 25% in TNE buffer) and loaded onto a gel. A 7.5% polyacrylamide gel was used in a continuous buffer sys- tem, with a 25 mA running current and constant voltage overnight.
Silver staining of the gel was as described by Herring et al. (1982) with the ‘sil- ver soak’ reduced from 1 h to 20 min and the sodium borohydride omitted from the developer.
Results
EM
The 56 stools positive for rotavirus ranged in concentration from occasional (- 1 x 10h particles/ml) to 4+ (>lO”’ particles/ml). Forty-one of these stools had an EM score of 2+ or less. In 13 stools, all the virus particles had their inner cores penetrated by PTA stain. Twenty-three stools had the majority of viruses with a complete outer virus shell, the smooth form of rotavirus.
PA GE
PAGE of 50 stools where sufficient sample remained showed 46 stools with typ- ical group A rotavirus pattern. Two stools contained ‘atypical’ rotavirus of group C (McNulty et al., 1981). This is the first time rotaviruses of this group have been detected in the west of Scotland. Two samples, both containing occasional rota- virus particles, had no apparent RNA.
Twenty-seven stools were found to be negative in Rotazyme II using the clari- fied extract (Table 2). Twenty-two of these had an EM score of 2+ or less. One had an EM score of 4+ but fell within the lO%-negative retest zone described in the test protocol. Two were the ‘atypical’ rotaviruses which would not be expected to be detected in the current ELISAs.
42
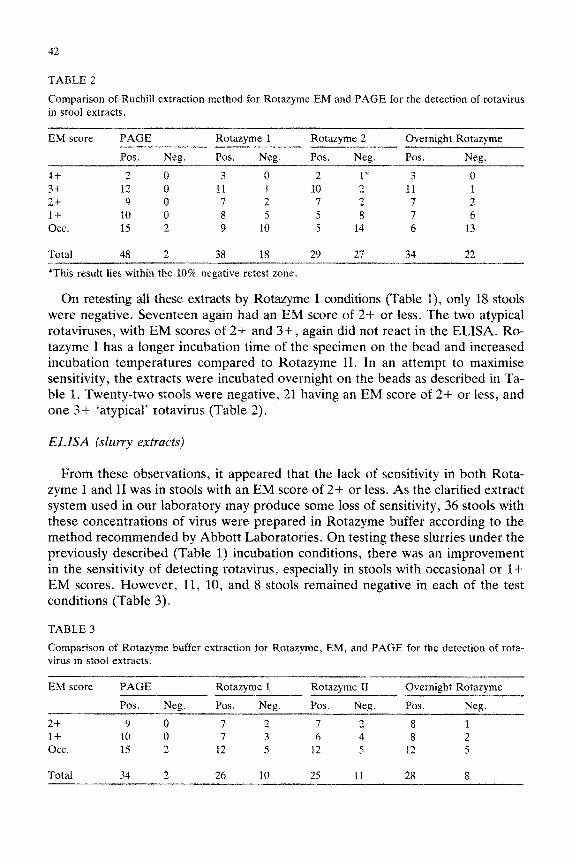
TABLE 2
Comparison of Ruchill extraction method for Rotazyme EM and PAGE for the detection of rotavirus in stool extracts.
EM score PAGE Rotazyme 1 Rotazyme 2 Overnight Rotazyme
Pos. Neg. POS. Neg. Pas. Neg. Pos. Neg.
4-t 2 0 3 0 2 1* 3 0 3+ 12 a 11 1 10 2 11 1 2t 9 0 7 2 7 2 7 2 l-4- 10 0 8 5 5 8 7 6 occ. 15 2 9 10 5 14 6 13
Total 48 2 38 18 29 27 34 22
*This result lies within the 10% negative retest zone
On retesting all these extracts by Rotazyme I conditions (Table 1). only 18 stools were negative. Seventeen again had an EM score of 2-t or less. The two atypicaf rotaviruses, with EM scores of 2+ and 3+, again did not react in the ELISA. Ro- tazyme I has a longer incubation time of the specimen on the bead and increased incubation temperatures compared to Rotazyme II. In an attempt to maximise sensitivity, the extracts were incubated overnight on the beads as described in Ta- ble 1. Twenty-two stools were negative, 21 having an EM score of 2+ or less, and one 3+ ‘atypical’ rotavirus (Table 2).
ELBA (slurry extracts)
From these observations, it appeared that the lack of sensitivity in both Rota- zyme I and II was in stools with an EM score of 2-t or less. As the clarified extract system used in our laboratory may produce some loss of sensitivity, 36 stools with these concentrations of virus were prepared in Rotazyme buffer according to the method recommended by Abbott Laboratories. On testing these slurries under the previously described (Table 1) incubation conditions, there was an improvement in the sensitivity of detecting rotavirus, especially in stools with occasional or l-t- EM scores. However, 11, 10, and 8 stools remained negative in each of the test conditions (Table 3).
TABLE 3
Comparison of Rotazyme buffer extraction for Kotazyme, EM, and PAGE for the detection of rota- virus in stool extracts.
EM score PAGE Rotazyme I Rotazyme II Overnight Rotazyme
Pos. Neg. Pos. Neg. Pos. Neg. Pos. Neg.
2+ 9 0 7 2 7 2 8 1 1+ 10 0 7 3 6 4 8 2 0% 15 2 12 5 12 5 12 5
Total 34 2 26 10 25 11 28 8
43
It was clear that the rotavirus positive stools did not react consistently in the ELISA. Only 11 of the 36 stools examined by all ELISA methods were positive for rotavirus in all methods. The overnight incubation of stool slurry was the only ELISA positive for rotavirus in 3 stools. With 1 stool, the overnight incubation with both the clarified extract and slurry were the only ELISAs positive for rota- virus.
Discussion
Commercial ELISAs are being used increasingly to detect rotavirus in stool specimens. Concern has been expressed at the number of ‘false-positives’ found in such systems and clarification of the stool extract suggested as a means to reduce the problem (Christie et al., 1983). Unfortunately, this problem persists. Out of 82 specimens submitted to the Regional Virus Laboratory in 1985 by other testing laboratories as rotavirus positive by ELISA, only 57 were confirmed by EM or PAGE. It would seem prudent that laboratories using ELISAs should either sub- mit ‘positive’ specimens to a specialist laboratory for confirmation by another technique or confirm the result by neutralisation with specific antibody.
The recently reported atypical or pararotavirus (Dimitrov et al., 1983; Hung et al., 1984; Chan et al., 1985) present another problem in that they do not cross- react serologically with normal rotaviruses and, therefore, will not be detected by the ELISAs. This study detected 2 atypical rotaviruses in children by EM and PAGE but not by ELBA which was to be expected as they do not possess the same group antigen (A) of the typical strains. These were similar to those found in Scotland by Hargreaves et al. (1984).
It is clear from this small study that using our normal stool extract in the Abbott Rotazyme II ELISA results in false-negatives. This situation is improved slightly if the conditions ate changed to that of the previous Rotazyme I system or incu- bation is overnight at room temperature. However, at best, 32% of the stools po- sitive by EM and PAGE are still negative by Abbott ELBA. This problem seems to be one of sensitivity in that the majority of negatives occur in stools with low numbers of virus particles as seen by EM. The slurry extraction method, as de- scribed in the Rotazyme II protocol, improves the detection rate slightly but 30% of stools positive by EM and PAGE are still clearly negative using the standard incubation times. Only when the incubation times are modified, does the false- negative number fall significantly to 22%. This study therefore indicates that at best this ELBA will miss 1 in 5 positive specimens where particles are readily detect- able by EM but not present in large numbers. There is no simple way of overcom- ing this deficiency in the test system.
PAGE has the best agreement with EM in that it gave negative results in only two of the 50 stools examined. It has the advantage over EM in that the electro- pherotype of the virus and any atypical rotaviruses may be determined in the sys- tem. However, PAGE may miss some rotavirus positive stools towards the end of infection due to a lack of RNA in the viruses.
44
Requests for the laboratory diagnosis of rotavirus are increasing and a positive finding can influence patient management and have implications for cross-infection and control of infection policy within a hospital. The results of this study indicate that a much greater awareness of the deficiencies of this test system is required. Other ELISAs may be better but perhaps virologists and the many others now us- ing test kits for diagnosing virus infections should be more critical of the results.
References
Birch, C.J., Lehman, N.I., Hawker, A.J., Marshall, J.A. and Gaust, J.D. (1979) J. Clin. Path. 32,
700. Bishop, R.J., Davidson, G.P., Holmes, I.H. and Ruck, B.J. (1974) Lancet i, 149.
Chan, C.-M., Hung, T., Bridger, J.C. and McCrae, N.A. (1985) Lancet ii, 1123.
Chrystie, I.L., Totterdell, B.M. and Banatvala, J.E. (1983) Lancet ii, 1028.
Dimitrov, D.H., Estes, M.K., Rangelova, S.M., Shindarov, L.M., Melnick, J.L. and Graham, D.Y.
(1983) Infect. Immun. 41, 523. Hargreaves, F.D., Inglis, J.M. and Herring, A.J. (1984) Communicable Diseases Scotland Weekly Re-
port 8415.
Herring, A. J., Inglis, N.F., Ojele, C.K., Snodgrass, D.R. and Menzies, J.D. (1982) J. Clin. Microbial.
16, 473.
Hung, T., Wang, C., Fang, Z., Chou, Z., Chang, X., Laing, X., Chen, C., Yao, H., Chaeo, T., Ye,
W., Den, S. and Chang, W. (1984) Lancet i, 1139.
Middleton, J.P., Petri, M., Hewitt, C.M., Szymanski, N.T. and Tam, J.S. (1977) Infect. Immun. 16,
439.
Moosai, R.B., Carter, M.J. and Madeley, C.R. (1984) J. Clin. Pathol. 37. 1404.
McNulty, M.S., Allan, G.M., Todd, D., McFerran, J.B. and McCracken, R.M. (1981) J. Gen. Virol.
55, 405. Yolken, R.H., Kim, H.W., Chem, T., Wyatt, R.G., Kalici, A.R., Chanock, R.M. and Kapikian, A.Z.
(1977) Lancet ii, 263.





























