Embed Size (px)
Citation preview

O
O
Awa
J
a
b
S
R
S
1h
besity Research & Clinical Practice (2014) 8, e1—e15
RIGINAL ARTICLE
n assessment of the relationships between over-eight, obesity, related chronic health conditionsnd worker absenteeism
effrey T. Howarda,∗, Lloyd B. Potterb
Department of Demography, University of Texas at San Antonio, United StatesDepartment of Demography, University of Texas at San Antonio and Institute for Demographic andocioeconomic Research, United States
eceived 22 July 2012; received in revised form 8 September 2012; accepted 9 September 2012
KEYWORDSObesity;Overweight;Obesity relatedchronic healthconditions;Worker absenteeism
SummaryIntroduction: Worker absenteeism is an important area of study within the fieldof occupational health. Prior studies have linked the presence of obesity to higherrates of absenteeism, but have not examined whether or not the relationship ismoderated by the presence of other chronic health conditions or whether or not therelationships have been stable over time.Methods: Data from the 2000 and 2010 National Health Interview Survey, a nationallyrepresentative sample of the US population, were analyzed to determine the extentto which the presence of 5 obesity-related chronic health conditions moderatesthe relationship between overweight/obesity and worker absenteeism, and whetheror not these relationships are stable over time. Logistic regression was used toexamine the relationships between overweight/obesity, the obesity-related chronichealth conditions and worker absenteeism, while controlling for demographic, socio-economic, occupational, health related and behavioral variables.Results: The findings suggest that obesity (p < 0.01) is related to higher rates of
worker illness absence, and that the presence of diabetes positively moderates thisrelationship (p < 0.05) within the severely obese population (class III — BMI ≥ 40).Other health conditions, including hypertension, coronary heart disease, other heartdisease and stroke, were not found to have significant moderating effects.Conclusion: The evidence suggests that obesity is associated with a higher likelihood of worker illness absenteeism, and that the effect is doubled for those with both∗ Corresponding author at: Department of Demography, University of Texas at San Antonio, 501W. Cesar E. Chavez Blvd.,an Antonio, TX 78207-4415, United States. Tel.: +1 210 458 3163.
E-mail address: [email protected] (J.T. Howard).
871-403X/$ — see front matter © 2012 Asian Oceanian Association for the Study of Obesity. Published by Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.orcp.2012.09.002

e2 J.T. Howard, L.B. Potter
) and diabetes. The moderating effect between class III obe-served only in 2010, indicating that this may be a relatively
ssociation for the Study of Obesity. Published by Elsevier Ltd.
CB
ahcohctdoio[caass$
btOhoqt[Ba[cmAsfroarfsented about 21% of the obesity-attributable costs[12].
class III obesity (BMI ≥ 40sity and diabetes was obnew phenomenon.© 2012 Asian Oceanian AAll rights reserved.
Introduction
An important area in occupational health researchis the study of the risk factors associated with directand indirect health care costs. Direct health carecosts are those related to the actual treatmentof an illness or disease, such as doctor’s visits,hospital admissions, treatments, procedures andprescription drug medication. One key componentof indirect costs that has received much attention isabsenteeism. Absenteeism is defined as an absencefrom work due to illness or an underlying healthcondition [1]. Absenteeism is one of the primarycomponents that make up the indirect costs of ill-ness that are absorbed by employers, both privatebusiness and government. The scale of the eco-nomic impact of absenteeism in the workplace isenormous. The overall costs of worker productiv-ity loss from absenteeism to businesses in the USwere recently estimated at $118 billion [2]. Asidefrom the economic consequences of absenteeism,measures of worker absence are also general indi-cators of occupational health and wellbeing in theirown right, and are, therefore, important areas ofstudy regardless of their potential financial impli-cations. Absenteeism has been associated withboth acute and chronic illnesses, such as allergies,influenza, acute gastrointestinal diseases, acuteand chronic pain conditions, pulmonary diseases,anxiety, depression, stress, alcohol and drug abuse,and obesity [1,3—6].
Based on research conducted in both the USand internationally, obesity has emerged as animportant risk factor for absenteeism as researchin this area has increased over the last 15—20 years[7]. Obesity is typically defined as one’s Body MassIndex (BMI) exceeding 30 [7—10]. The BMI is abiometric measure of one’s weight in relation toheight, and is measured as weight in kilogramsdivided by height in square meters [11]. Clinicianshave developed a classification system basedon BMI that establishes ranges for underweight,normal weight, overweight and obese. The BMIthresholds for these categories are: (1) BMI < 20is underweight, (2) BMI of 20—24.99 is normal
weight, (3) BMI of 25—29.99 is overweight and (4)BMI ≥ 30 is considered obese [11]. Additionally, theobese category is further divided into 3 classes.pl
lass I obesity is BMI 30—34.99, Class II obesity isMI 35—39.99 and Class III obesity is BMI ≥ 40 [11].
In addition to establishing links between obesitynd other chronic disease conditions, researchersave linked obesity to increased direct health careosts [7,12—15]. The general conclusion is thatbese individuals are more likely to have otherealth conditions, such as diabetes, hypertension,oronary heart disease and stroke, and thereforeend to be less healthy on average. One Cana-ian study conducted in the mid-1990s found thatbesity-attributable direct health care costs weren the range of $1.8 billion, which equated to 2.4%f all health expenditures in Canada at that time15]. Additionally, the researchers found that 3hronic health conditions, hypertension, diabetesnd coronary heart/artery disease, accounted forpproximately 80% of these costs. In a similar UStudy, direct health care costs attributable to obe-ity in the United States were estimated to be75 billion in 2003 [13].
However, research examining the relationshipetween obesity and the prevalence and dura-ion of absenteeism specifically remains limited.besity has been found to be associated withigher levels of absenteeism in several early studiesf the subject in the 1990s [9,16—20]. Subse-uent studies over the last 10 years have reinforcedhese earlier findings in a variety of settings7,8,10,12,17,21—23]. For example, data from aelgian study published in 1999 showed significantssociations between obesity and worker absence8]. BMI was also found to be positively asso-iated with increased rates of absenteeism forale employees at Oklahoma State University [17].
larger US study of a nationally representativeample of full-time employees conducted in 2005ound that overweight and all 3 classes of obesityesulted in increased absenteeism for women, butnly classes II and III obesity resulted in increasedbsenteeism for men [12]. The same research alsoeported that, although class III obesity accountedor only about 3% of the sample, this group repre-
More recently, researchers at Shell Oil Com-any found that obese employees were 80% moreikely to have a work absence, and missed 3.7

O
mmo$webawordwaTwHoa
tpaedcttriaamoi
tobofrodaimtmr[tzttt
ocrnpaasc(cewobtpiotbet
D
S
DHCwoNatTarcgora(
M
Sd
besity and worker absenteeism
ore days of work per year than employees of nor-al weight [21]. They also estimated the costs of
besity-related absenteeism to be approximately11 million per year for their 25,000 employeeorkforce [21]. Another study of 10,026 employ-es conducted across multiple worksites in the USetween 2005 and 2007 found evidence for thessociation between obesity and absenteeism, asell as the number of doctor’s visits, the numberf emergency room visits, hospital admissions andates of presenteeism, the term given to the pro-uctivity losses associated with continuing to workhile ill [22]. Obese employees were found to bebsent 14.7% more than normal weight employees.his study did not find any evidence that being over-eight, but not obese, was related to absenteeism.owever, being overweight was found to be relatednly to increased incidence of hospital admissionsnd presenteeism [22].
Yet, research specifically examining the rela-ionship between obesity, with and without theresence of other disease conditions, and workerbsence is even more limited [7]. Since the pres-nce and severity of obesity is related to otherisease conditions, such as diabetes, hypertension,oronary heart disease and stroke, it is logical thathe presence of one or more of these health condi-ions in combination with overweight/obesity couldesult in a moderating effect on absenteeism. Thats, that the combined effect of overweight/obesitynd another comorbid condition could actu-lly amplify the likelihood of worker absenceore so than the presence of overweight/obesity
r an additional chronic health condition insolation.
However, only two studies have been identifiedhat specifically address the potential mediatingr moderating effects of the presence of comor-id disease conditions on the relationship betweenverweight/obesity and absenteeism. Diabetes wasound to significantly increase the absenteeismelated health costs within obese and morbidlybese individuals [24]. A more recent study con-ucted in 2010 analyzing the effects of obesitynd several chronic health conditions, includ-ng cardiovascular disease, hypertension, diabetes,usculoskeletal and psychiatric disorders, found
hat the inclusion of comorbid conditions in aultivariate model reduced the magnitude of the
elationship between obesity and worker absence25]. However, this study only considered indica-ors of the presence of comorbid conditions as
ero-order covariates and did not explicitly testhe extent to which these conditions moderatehe relationship between obesity and absen-eeism by examining interaction terms betweenwcna
e3
verweight/obesity and selected chronic healthonditions. Furthermore, no research has beeneported that specifically addresses whether orot these relationships have been stable over aeriod of time. The purpose of this study is toddress the following research hypotheses, whichre: (1) that the presence of overweight and obe-ity, regardless of the presence of any other healthondition, is positively related to worker absence,2) that the presence of each of the five otherhronic health conditions, regardless of the pres-nce of overweight/obesity, is positively related toorker absence, (3) that the relationship betweenverweight/obesity and absenteeism is moderatedy the presence of other chronic health condi-ions when they are comorbid, specifically that theresence of comorbid health conditions will signif-cantly increase the effect of overweight/obesityver and above its effect when other health condi-ions are not present, and (4) that the relationshipsetween overweight/obesity and any moderatingffects of chronic health conditions are stable overime.
ata and methods
ample
ata compiled from the 2000 and 2010 Nationalealth Interview Survey (NHIS) conducted by theenters for Disease Control and Prevention (CDC)ere used to analyze the relationships betweenverweight/obesity and absenteeism [26,27]. TheHIS is a nationally representative, continuouslydministered survey with annual data releases fromhe National Center for Health Statistics (NCHS).he NHIS asks respondents many health-relatednd occupational questions, as well as questionselated to various socio-economic and demographicharacteristics. Moreover, the survey responses areathered for both adults and children. For this studynly the adult sample of the NHIS, defined as thoseespondents 18 years of age or older, was utilized,nd these data were analyzed using SAS softwareversion 9.2 for Linux).
easures
tandard statistical procedures were used toetermine the relationships between the over-
eight/obese measures, obesity-related healthonditions, including diabetes, hypertension, coro-ary heart disease, other heart disease and stroke,nd absenteeism for those who were employed
fcdoihaitaeeec
etahvav(tbadstvpgtttopretrrroi
atpewo
e4
during the past year, while controlling for other rel-evant demographic, socio-economic, occupationaland health behavior variables. Absenteeism wasmeasured as the number of missed days of workdue to illness. Due to the fact that close to half ofthe respondents in the survey reported that theyhad not missed any days of work, and that thosewho did miss work tended to be tightly groupedbetween 2 and 6 days, absenteeism was convertedto a dichotomous variable, where 1, missed 1 ormore days of work and 0, did not miss a day ofwork in the last year. This type of dichotomousmeasurement of worker illness absence is consis-tent with several prior studies on the subject ofworker absenteeism [17,24,25]. The interpretationof this analysis of absenteeism is therefore in termsof the likelihood to miss work as the result of ill-ness, rather than on the specific duration of workdays missed.
Overweight and obesity were measured usingthe BMI score available in the NHIS sample.BMI is calculated based on responses to ques-tions that ask the respondents their height andweight. Four dichotomous variables were createdusing standard BMI score cut-off thresholds toplace each respondent into the categories of over-weight (25 ≤ BMI < 30), obese class I (30 ≤ BMI < 35),obese class II (35 ≤ BMI < 40) and obese class III(BMI ≥ 40). Each of these overweight/obese cat-egories was used to compare the likelihood ofabsence to the reference group of individualswith BMI < 25, which are typically characterizedas normal weight (18.5 < BMI < 25) and underweight(BMI ≤ 18.5) [11].
Similar to the obesity measures, five dichoto-mous variables were created in order to measurethe presence of obesity-related health conditions,including diabetes, hypertension, coronary heartdisease, other heart disease and stroke. The NHISasks each respondent whether or not they haveever been told by a doctor that they have oneof these five conditions. For each of the con-ditions, affirmative responses were coded as 1,and all other responses were coded as 0. Eachof these chronic health condition indicators werethen compared to the reference group consistingof all respondents without the presence of thesefive conditions. In addition to analyzing the effectsof overweight/obesity and the other chronic healthcondition variables individually, another goal of thisstudy is to evaluate whether or not the effectsof overweight/obesity on absenteeism are moder-
ated by the presence of the five health conditionswhen they are comorbid. In order to measure anymoderating effects of these disease conditions,a set of interaction variables were constructedh1qm
J.T. Howard, L.B. Potter
or each combination of the overweight/obesityategories and the presence of each additionalisease condition. Each 1/0 indicator variable forverweight/obesity was multiplied by each 1/0ndicator variable for the presence of chronicealth conditions [28—30]. This resulted in the cre-tion of an additional 20 variables, representingnteraction terms between overweight/obesity andhe presence of each disease condition, that weressessed in the analysis. The interpretation of theffects of these variables is that they represent theffect of overweight/obesity in conjunction withach additional health condition, when they areomorbid.
While the primary explanatory variables of inter-st in this study are related to overweight/obesity,he five obesity-related chronic health conditions,nd the interactions between obesity and chronicealth conditions, a number of additional controlariables were also analyzed. The control vari-bles used in this analysis constitute four majorariable types: (1) demographic characteristics,2) socio-economic characteristics, (3) occupa-ional characteristics and (4) health related andehavioral characteristics. Age, sex, race/ethnicitynd geographic region of residence comprise theemographic variables used in the analysis. Theocio-economic variables consist of income, educa-ional attainment and marital status. Occupationalariables include type of employer (private com-any, federal government, state government, localovernment or self), size of employer in terms ofhe number of employees, the number of yearshe respondent has worked in his or her occupa-ion, type of occupation (white collar, blue colorr service), whether or not the respondent isaid hourly or salaried and whether or not theespondent has paid sick leave provided by themployer. Health related and behavioral charac-eristics include indicators for whether or not theespondent is currently an alcohol drinker, cur-ent or former cigarette smoker, has pro-activelyeceived a flu shot in the last year, and whetherr not the respondent currently has health carensurance.
The total NHIS adult sample size was 32,374nd 27,157 for the years 2000 and 2010, respec-ively. However, several other data exclusions wereerformed in order to focus the analysis on the rel-vant population actually at risk of absence fromork. First, the sample was reduced to includenly those respondents who indicated that they
ad been employed at some point within the past2 months. Respondents were asked the followinguestion in the NHIS in order to determine employ-ent status, ‘‘Did you have a job or business at
Obesity and worker absenteeism e5
Table 1 Overall prevalence rates of chronic health conditions, BMI categories and worker illness absenteeism forNHIS year 2000 and 2010 with �2 significance tests for the difference in prevalence rates.
Variable Year 2000 Year 2010 % change
N Prevalencerate as %
N Prevalencerate as %
Chronic health conditionsDiagnosed with diabetes 18,860 3.6 16,626 6.1 71.2**
Diagnosed with coronary heart disease 18,860 1.4 16,626 2.5 78.6**
Diagnosed with other heart disease 18,860 4.8 16,626 5.6 16.7**
Diagnosed with hypertension 18,860 16.1 16,626 24.6 52.8**
Diagnosed with stroke 18,860 0.6 16,626 1.1 93.9**
BMI categoriesUnderweight — BMI < 18.5 18,860 1.9 16,626 1.4 −26.3**
Normal — BMI 18.5—24.99 18,860 40.8 16,626 35.6 −12.7**
Overweight — BMI 25—29.99 18,860 36.0 16,626 35.4 −1.7Obese class I — BMI 30—34.99 18,860 14.2 16,626 17.3 21.8**
Obese class II — BMI 35—39.99 18,860 4.8 16,626 6.4 33.3**
Obese class III — BMI ≥ 40 18,860 2.3 16,626 4.0 73.9**
AbsenteeismWorker illness absence 18,860 47.9 16,626 41.6 −13.2**
aAdjusted for NHIS cluster, weight and stratum variables [26,27].*p < 0.05, **p < 0.01.
actff2owtrBf1fqepfftwosiwaoids
ss
S
Tsrpdttviatceslr2rcth
ny time in the past 12 months?’’ Respondents indi-ating that they had no job or business at anyime in the past 12 months were then excludedrom the analysis. This reduced the sample in 2000rom 32,374 to 22,505 and the sample in 2010 from7,157 to 17,524. Second, any respondents with-ut a valid BMI score were also excluded, alongith any female respondents who indicated that
hey were currently pregnant, as this fact wouldesult in those individuals having artificially highMI scores. This step reduced the 2000 samplerom 22,505 to 21,338 and the 2010 sample from7,524 to 16,757. Third, those respondents whoailed to answer the number of work days misseduestion or any of the explanatory variables werexcluded. This step further reduced the 2000 sam-le from 21,328 to 18,860 and the 2010 samplerom 16,757 to 16,626. While previous studies haveurther limited samples of the working populationo those individuals aged 18—64, those individualsho did work in the last year but happen to bever age 64 were not excluded from the currenttudy provided they met the other conditions fornclusion described above [12]. The exclusion oforking individuals over age 64 seems arbitrarynd unnecessary given the increasing prevalence
f workers over age 64 and the fact that ages included explicitly in the multivariate analysisescribed below. This process resulted in a finalample size of 18,860 (58.3% of total) for the 2000coaa
urvey and 16,626 (61.2% of total) for the 2010urvey.
tatistical procedures
he data from the 2000 and 2010 surveys were usedpecifically to assess the extent to which observedelationships between overweight/obesity, theresence of diabetes, hypertension, coronary heartisease, other heart disease, stroke and absen-eeism have been stable over time, at least overhe last decade. The cluster, weight and stratumariables provided in the NHIS datasets were usedn order to control for the complex stratificationnd sampling design of the survey. Table 1 con-ains prevalence rates for the five chronic healthonditions of interest, the 4 overweight/obese cat-gories and for worker absences, along with �2
ignificance test results for the difference in preva-ence rates from 2000 to 2010. Multivariate logisticegression models were fit separately for both the000 and 2010 datasets in order to quantify theelationships between the key overweight/obesity,hronic health condition variables, the interac-ions between overweight/obesity and chronicealth conditions and worker absenteeism, while
ontrolling for the demographic, socio-economic,ccupation and health behavior variables describedbove. Results of the logistic regression analysesre reported in Table 2 .
e6
J.T. H
oward,
L.B. Potter
Table 2 Results of multiple logistic regression analysis of worker illness absenteeism for chronic health conditions, overweight/obesity categories and interactionsusing the 2000 and 2010 NHIS samples.
Chronic health conditions andoverweight/obesityvariables
2000 2010
Logit coefficient Odds ratios Logit coefficient Odds ratios
Estimate L95% CI U95% CI Estimate L95% CI U95% CI
Chronic health conditionsDiagnosed with diabetes 0.318 1.374 0.860 2.194 0.159 1.173 0.773 1.780Diagnosed with coronary
heart disease0.138 1.148 0.668 1.973 0.486 1.625 0.889 2.973
Diagnosed with other heartdisease
0.201 1.223 0.937 1.596 0.212 1.236 0.880 1.736
Diagnosed withhypertension
0.155 1.168 0.970 1.406 0.260** 1.297 1.068 1.574
Diagnosed with stroke 0.165 1.180 0.573 2.430 0.858* 2.359 1.120 4.967Overweight/obesity categories
Overweight — BMI 25—30 0.003 1.003 0.919 1.094 0.095 1.099 0.984 1.228Obese class I — BMI 30—35 0.204 1.226 1.083 1.388 0.192** 1.211 1.048 1.400Obese class II — BMI 35—40 0.601** 1.825 1.499 2.221 0.452** 1.572 1.268 1.949Obese class III — BMI 40+ 0.663** 1.941 1.425 2.644 0.297* 1.346 1.004 1.806
InteractionsOverweight w/diabetes 0.227 1.254 0.707 2.225 0.159 1.172 0.684 2.008Obesity class I w/diabetes −0.156 0.856 0.483 1.516 0.118 1.125 0.677 1.869Obesity class II w/diabetes −0.234 0.791 0.388 1.613 −0.089 0.915 0.515 1.624Obesity class III w/diabetes −0.073 0.929 0.396 2.182 0.974* 2.649 1.334 5.261Overweight w/coronary
heart disease0.413 1.512 0.743 3.076 −0.638 0.528 0.248 1.128
Obesity class I w/coronaryheart disease
0.171 1.187 0.532 2.650 −0.355 0.701 0.300 1.639
Obesity class II w/coronaryheart disease
0.986 2.680 0.565 12.723 −0.598 0.550 0.203 1.495
Obesity class III w/coronaryheart disease
0.832 2.297 0.555 9.511 −0.499 0.607 0.188 1.959

Obesity
and w
orker absenteeism
e7
Table 2 (Continued )
Chronic health conditions andoverweight/obesityvariables
2000 2010
Logit coefficient Odds ratios Logit coefficient Odds ratios
Estimate L95% CI U95% CI Estimate L95% CI U95% CI
Overweight w/other heartdisease
−0.114 0.893 0.592 1.345 0.316 1.372 0.874 2.151
Obesity class I w/otherheart disease
0.054 1.056 0.630 1.769 −0.080 0.923 0.544 1.566
Obesity class II w/otherheart disease
−0.307 0.736 0.311 1.741 −0.033 0.968 0.437 2.142
Obesity class III w/otherheart disease
0.198 1.219 0.343 4.336 0.085 1.089 0.523 2.269
Overweightw/hypertension
0.025 1.026 0.801 1.314 0.064 1.066 0.830 1.369
Obesity class Iw/hypertension
0.113 1.120 0.844 1.487 −0.036 0.965 0.735 1.265
Obesity class IIw/hypertension
0.000 1.000 0.673 1.486 0.010 1.010 0.710 1.438
Obesity class IIIw/hypertension
−0.224 0.799 0.490 1.304 −0.176 0.839 0.538 1.309
Overweight w/stroke 0.271 1.312 0.462 3.725 −0.490 0.613 0.226 1.662Obesity class I w/stroke 0.830 2.293 0.674 7.804 −0.452 0.636 0.206 1.966Obesity class II w/stroke 1.068 2.908 0.225 37.633 0.233 1.262 0.307 5.197Obesity class III w/stroke −2.523 0.080 0.010 0.644 −1.221 0.295 0.081 1.080
Fit statistics 2000 2010
Log likelihood 107,432,482 143,665,195Likelihood ratio �2 5,882,046.12** 9,549,329.29**
N 18,860 16,626aEstimates are adjusted for age, gender, race/ethnicity, region, educational attainment, marital status, income, smoking and drinking status, occupational variables, uninsured status,type of employer and employment sector.bAdjusted for NHIS cluster, weight and stratum variables [26,27].*p < 0.05, **p < 0.01.

do
M
Asml9tctvatfhlomotaswrcfpdTra
asccwosdbsslbootr
e8
Results
Prevalence of chronic health conditions,overweight, obesity and absenteeism
Prevalence rates for each of the five chronic healthconditions of interest, including diabetes (p < 0.01),coronary heart disease (p < 0.01), other heart dis-ease (p < 0.01), hypertension (p < 0.01) and stroke(p < 0.01), have increased significantly over the lastdecade within the non-pregnant adult, workingpopulation. As Table 1 illustrates, the prevalencerate of diabetes increased from 3.6% in 2000 to6.1% in 2010, an increase of 71.2%. The preva-lence rate of coronary heart disease increased from1.4% to 2.5%, a 78.6% increase, while the rate forother heart disease increased 16.7% from 4.8% to5.6% over the same time period. Prevalence ratesfor hypertension and stroke increased 52.8%, from16.1% to 24.6%, and 93.9%, from 0.6% to 1.1%,respectively.
Similarly, the prevalence of all 3 classes of obe-sity also significantly increased between 2000 and2010 (p < 0.01 for all 3 classes). While there wasa slight decrease in the percentage of individualsoverweight but not obese, with BMI between 25and 30, the difference was not statistically signif-icant, falling from 36.0% to 35.4% during this timeperiod. Class I obesity, where BMI is between 30and 35, increased from 14.2% in 2000 to 17.3% in2010, an increase of 21.8%. Class II obesity, whereBMI is between 35 and 40, increased from 4.8% to6.4%, an increase of 33.3%. Class III obesity, themost severe where BMI is 40 or more, increasedfrom 2.3% to 4.0%, an increase of 73.9%, the largestrate of increase of any of the overweight/obesecategories.
In contrast to the large increases in prevalence ofthe obesity and chronic health condition measures,worker absenteeism actually declined significantlyfrom 2000 to 2010, from 47.9% to 41.6%, a decreaseof 13.2%. The fact that each of the chronic healthconditions as well as each of the obesity cate-gories have all increased substantially over the lastdecade would suggest that the overall health ofthe working population is decreasing over time.One would expect absenteeism to be increasing asthese other health issues are increasing, yet thisis not the case. While the decrease in rates ofabsenteeism is an interesting finding, evaluatingthe change from 2000 to 2010 is not the primaryobjective of this study, and a full analysis of the
reasons for this decline is beyond its scope. Never-theless, several possible contributing factors to thedecline in absenteeism will be discussed in moresria
J.T. Howard, L.B. Potter
etail later, along with some suggestions for areasf future research.
ultivariate analysis
s the results from the multivariate logistic regres-ion procedure in Table 2 suggest, the overallodels for each year are significant, with a like-
ihood ratio �2 of 5,882,046.12 (p < 0.01) and,549,329.29 (p < 0.01), for 2000 and 2010 respec-ively. This indicates that the models with allovariates provide a better fit of the data thanhe intercept alone. Additionally, the indicatorariables for the 3 classes of obesity (p < 0.05)re all statistically significant, indicating thathey are related to absenteeism, while controllingor demographic, socio-economic, occupational,ealth related and behavioral covariates. The like-ihood of absence was not found to differ forverweight individuals as compared to the nor-al/underweight reference group. An assessment
f the cross-correlation matrix and variance infla-ion measures (not shown) suggests that therere statistically significant correlations betweenome independent variables, but these correlationsere not found to be of sufficient strength to
esult in estimation problems associated with multi-ollinearity [28,30,31]. The regression coefficientsor overweight and the obesity indicators are allositive, indicating that being overweight or obeseoes result in a higher likelihood of worker absence.hese data provide evidence in support of the firstesearch hypothesis, that overweight and obesityre positively related to absenteeism.
Hypertension (p < 0.01) and stroke (p < 0.05)re the two chronic health conditions that haveignificant associations with absenteeism, whenontrolling for other covariates. The effects oforonary heart disease and other heart diseaseere each found to be non-significant. Diabetes,n the other hand, has a more complex relation-hip with absenteeism. The interaction betweeniabetes and class III obesity is significant (p < 0.05),ut the diabetes indicator on its own is not. Thisuggests that diabetes without the presence ofevere obesity (class III) does not impact the like-ihood of a worker to be absent due to illness,ut that the combination of diabetes and class IIIbesity does significantly increase the likelihoodf worker absence. This finding also indicates thathe presence of diabetes does play an importantole in positively moderating the effect of obe-
ity on absenteeism. Interestingly, the observedelationships between hypertension, stroke and thenteraction between diabetes and class II obesityppear to be significant only in the 2010 data.
O
Thsas
aaiAtrttcap
ioromyrao
bief1Tttemltt
Iiooca1ndwej2c
hw1tiqcwiwaddaat
stidoowbparbo1t2teris(t1oDoTidat
rs
besity and worker absenteeism
hese results provide evidence that of the 5 chronicealth conditions of interest, only hypertension andtroke have significant positive main effects onbsenteeism, and, therefore, provide only partialupport of the second research hypothesis.
Likewise, the only significant interaction vari-ble between the overweight/obesity indicatorsnd the 5 chronic health conditions of interest is thenteraction between class III obesity and diabetes.gain, these results provide only partial support forhe third hypothesis, that the overweight/obesityelationships with absenteeism are moderated byhe presence of each of the chronic health condi-ions. These results suggest that diabetes is the onlyhronic health condition that acts as a moderator,nd that it only exerts a moderating effect in theresence of class III obesity.
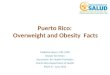
The bar graph in Fig. 1 provides a visualllustration of the effects of overweight/obesityn absenteeism. Each bar in this graph rep-esents the odds ratio for the correspondingverweight/obesity category compared to the nor-al/underweight, reference population for the
ears 2000 and 2010. These data suggest a dose-esponse pattern of increasing odds of absenteeisms one moves from overweight to obese to severelybese.
Specifically, the overweight group was found toe no more likely to have a work absence due tollness than the normal/underweight group. How-ver, the odds of absence are significantly higheror the class I obesity group, with odds ratios of.211 and 1.226 for 2000 and 2010, respectively.his means that in 2010, class I obesity increaseshe odds of worker absence by 22.6% compared tohe normal/underweight category. Similarly, work-rs with class II obesity were 1.825 times (82.5%)ore likely in 2000, and 1.572 times (57.2%) more
ikely in 2010 to miss work due to illness thanheir normal/underweight counterparts in thoseime periods.
Perhaps most interesting is the effect of classII obesity because of the interaction with diabetesn the 2010 data. In 2000, class III obesity with-ut the presence of diabetes increased the oddsf absenteeism by 1.941 times, or 94.1%. In 2010,lass III obesity without the presence of diabetesppears to increase the odds of absenteeism by only.346 times, or 34.6% (p < 0.05). In 2000, there waso evidence of a significant interaction betweeniabetes and class III obesity. In 2010, however,hen class III obesity is coupled with the pres-
nce of diabetes the odds of absence due to illnessump by 2.649 times, or 164.9%. This means that in010, all other things being equal, a worker withlass III obesity who is not diabetic has a 34.6%oip2
e9
igher likelihood of absenteeism, while a workerith class III obesity who is diabetic has roughly a64.9% higher likelihood of absenteeism comparedo the normal/underweight worker population. Thiss an important finding for several reasons: (1) ituantifies a moderating effect of a chronic healthondition on the relationship between obesity andorker absenteeism previously undocumented, (2)
t provides evidence that the underlying health oforkers is worsening as the rate of class III obesitynd diabetes has been rising rapidly over the pastecade even though the overall rate of absenteeismecreased over this time and (3) it suggests that thelready high indirect costs attributable to workerbsence may continue to increase if the currentrends of obesity and diabetes continue.
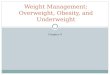
In addition to the overweight/obesity relation-hips already discussed, the odds ratios for each ofhe chronic health conditions of interest are listedn Fig. 2. As previously mentioned, the presence ofiabetes is related to an increase in absenteeismnly for those with class III obesity. When class IIIbesity is not present the odds ratio for diabetesas estimated at 1.374 in 2000 and 1.173 in 2010,ut it is not statistically significant in either timeeriod. Hypertension, on the other hand, does have
significant relationship to absenteeism (p < 0.01),egardless of the presence of overweight or obesity,ut the relationship is significant only in 2010. Thedds ratios for hypertension are 1.168 in 2000 and.297 in 2010. While hypertension was not foundo be significantly associated with absenteeism in000, in 2010 workers with hypertension were foundo be 1.297 times, or 29.7%, more likely to experi-nce absenteeism than those without hypertension,egardless of overweight/obesity status. The find-ngs for stroke are similar, where the effect oftroke on absenteeism in 2000 is non-significantOR = 1.18; p > 0.05), but in 2010 stroke was foundo be associated with an increase in absenteeism of35.9% (p < 0.05) as compared to those with nonef the five chronic health conditions of interest.iabetes was found to be related to absenteeismnly through the interaction with class III obesity.he remaining chronic health conditions examined,
ncluding coronary heart disease and other heartisease, had non-significant regression coefficientsnd were not observed to have significant interac-ions with overweight/obesity indicators.
The 4th and final set of research hypotheseselates to the relative stability of the relation-hips between overweight/obesity and absenteeism
ver time. Odds ratios with 95% confidencentervals, obtained from the logistic regressionrocedures performed for both the 2000 and010 samples, were compared, in order to assess
e10 J.T. Howard, L.B. Potter
Figure 1 Odds ratios of absenteeism for overweight and obesity levels compared to normal/underweight group with
st9l
corresponding �2 p values.
whether or not the relationship between each over-weight/obesity category and worker absenteeismhave changed over the last decade. There are 3criteria that must be met in order to concludethat the observed relationships between over-
weight/obesity and absenteeism have been stableover time: (1) the odds ratios must be greater than1 in both years, indicating the relationship is in the(9e
Figure 2 Odds ratios of absenteeism for chronic health condchronic health conditions along with corresponding �2 p value
ame direction, (2) the relationship must be statis-ically significant in both years (p < 0.05) and (3) the5% confidence intervals for both years should over-ap for each of the overweight/obesity categories.
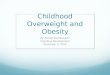
Fig. 3 displays the odds ratio point estimates
OR) as diamond-shaped coordinates, with the5% confidence interval (95% CI) error bars onither side of the estimate. These results suggestitions of interest compared to reference group withouts.

Obesity and worker absenteeism
Figure 3 Odds ratios describing the effects ofomc
tbIog2mfiosdatThwt
D
Wwo2cieItsctbicd
oiataac
tepoil5Itdctoapththod
dtecatIedbaiinabiibcmo
verweight/obese categories compared to the nor-al/underweight group for 2000 and 2010 with 95%
onfidence intervals.
hat there has been stability in the relationshipsetween class I obesity, class II obesity and classII obesity without diabetes, and absenteeism. Thedds ratios for each of these three obesity cate-ories is statistically significant (p < 0.05) in both000 and 2010, the relationships are all positive,eaning the direction is the same, and the 95% con-dence intervals around the odds ratio estimates allverlap. Thus, the conclusion is that, class 1 obe-ity, class II obesity and class III obesity withoutiabetes are related to increased odds of workerbsenteeism, and that these relationships appearo have been present for at least the past 10 years.his does provide at least partial support for theypothesis that the relationships between over-eight/obesity and absenteeism are stable over
ime.
iscussion
hile the observed relationships between over-eight/obesity and absenteeism, regardless ofther health conditions, have remained stable from000 to 2010, the interaction between diabetes andlass III obesity has changed significantly. The find-ngs from this study suggest that the moderatingffect of diabetes on the relationship between classII obesity, when they are comorbid, and absen-eeism were not present in 2000, but have emergedometime within the last decade. While the specificlinical mechanisms explaining the emergence ofhese relationships over the last 10 years have not
een documented, it seems plausible that, at leastn the case of class III obesity with diabetes, the pre-ipitous rise in the prevalence of both conditionsuring this time has given rise to a critical levelmaw
e11
f comorbidity. The increased level of comorbidity,n turn potentially results in higher rates of illnessnd/or increased severity of illness, which has ledo the expression of the observed moderating inter-ction effect. Of course, this is only speculative,nd more research is needed to determine the spe-ific causal components of these observed patterns.
Results from the multivariate analysis suggesthat there is support for the first research hypoth-sis that overweight and obesity have a direct,ositive effect on work absenteeism, regardless ofther health conditions. The findings suggest thatn 2010 workers with class I obesity are 21.1% moreikely to be absent, workers with class II obesity are7.2% more likely to be absent, workers with classII obesity without diabetes are 34.6% more likelyo be absent, and workers with class III obesity andiabetes are 164.9% more likely to be absent, asompared to their under and normal weight coun-erparts. The second research hypothesis, that eachf five obesity-related chronic health conditions islso directly related to worker absenteeism is onlyartially supported. In the case of hypertensionhere is support that the presence of this chronicealth condition is directly related to worker absen-eeism, but there was no evidence to support theypotheses that diabetes, coronary heart disease,ther heart disease and stroke, on their own, areirectly related to worker absence.
In the case of diabetes, however, there is evi-ence supporting the third research hypothesishat the effects of overweight/obesity are mod-rated by the presence of the five obesity-relatedhronic health conditions. This means that there is
relationship between diabetes and worker absen-eeism, but only when it is coupled with classII obesity. This is an important finding for sev-ral reasons: (1) because prior research has notocumented a significant moderating effect of dia-etes on the relationship between obesity andbsenteeism, (2) because the presence of diabetesncreases the odds of worker absence by approx-mately 100% over those with class III obesity buto diabetes, (3) because of the implications for
significant increase in the prevalence of dia-etes and class III obesity if current trends continuento the future and (4) because of the clinicalmplications for prevention and treatment of dia-etes and obesity. None of the other obesity-relatedhronic health conditions were found to haveoderating effects on the relationship between
verweight/obesity and absenteeism.
Finally, the fourth research hypothesis, that theeasured effects between overweight/obesity andbsenteeism would be found to be stable over time,as only partially supported. For class I and class

e12 J.T. Howard, L.B. Potter
Table 3 Changes in medical insurance status, paid sick leave and pay type variables between 2000 and 2010.
Variable Year 2000 Year 2010 % change
N % N %
Employment variablesNo medical insurance indicator 18,860 16.6 16,626 21.1 27.1**
Current employer offers paid sick leave 18,860 56.3 16,626 52.5 −6.8**
Paid on hourly basis 18,860 57.3 16,626 59.6 4.0**
7].
icetcewa
iilni2rh[e5daece
obfwtfyhltta(c
aAdjusted for NHIS cluster, weight and stratum variables [26,2*p < 0.05, **p < 0.01.
II obesity there is evidence that the relationship toabsenteeism has remained stable, at least over thepast 10 years. However, this is not the case for theoverweight and class III obesity categories. In 2000there was no evidence that workers who were sim-ply overweight were any more likely to be absent,but in 2010 there is evidence that overweight work-ers have a higher likelihood of absence. Similarly,there was no evidence of the moderating effect ofdiabetes on the relationship between class III obe-sity and absenteeism in 2000, but there is strongstatistical evidence for the presence of this effectin 2010. This suggests that the underlying dynamicsof overweight/obesity, related chronic health con-dition and worker absence is complex and changingover time. This also suggests that if the prevalenceof obesity, especially severe obesity (class III), dia-betes and other chronic health conditions continueto increase as dramatically as they have in the past10 years, the presence of other moderating effectsmay also emerge, along with potential increases inthe rate of worker absences.
Even with the significant increases in the preva-lence of obesity and other chronic health conditionsover the last 10 years, the rate of worker absen-teeism actually declined by roughly 13% between2000 and 2010. The obvious question is, why? Onepossible reason for this decline is that in 2010 theeconomy had just emerged from a severe recession,and with high unemployment, many workers maysimply have been reluctant to take time away fromwork even when ill [32,33]. If this is true, then onewould expect to see higher levels of worker presen-teeism in 2010 than in 2000. This would mean thatmore workers were electing to continue to workwhile ill, rather than take sick leave. Unfortunately,the NHIS does not address the issue of worker pre-senteeism, and this study, therefore, cannot assesswhether or not there has been an increase in pre-senteeism during this timeframe.
Of course, it may be the case that workers donot have much choice in the matter. For example,over the past 10 years there have been reductions
frl
n employer provided benefits [33], such as medi-al insurance and paid sick leave, which may helpxplain some of the observed difference in absen-eeism rates. While such associations may not beausal, they could point to a general employmentnvironment in which there is lower tolerance fororker absence, or at least the perception of suchn environment [32,33].
As Table 3 illustrates, there has been a signif-cant shift in several key employment variables,ncluding uninsured status, availability of paid sickeave and pay type. The percentage of workersot covered by some form medical insurance hasncreased by 27.1%, from 16.6% in 2000 to 21.1% in010. This finding is consistent with other recenteports, which have examined the decrease inealth insurance coverage over the last decade33]. Over the same period the percentage of work-rs with paid sick leave declined by 6.8%, from6.3% to 52.5%. Other studies have reported evi-ence that, in addition to reduction in benefits suchs employer provided health insurance, many work-rs have delayed utilization of medical care for bothhronic and acute illnesses as a result of the 2008conomic downturn [34].
A simple cross-tabular examination of thebserved differences in rates of absenteeismetween 2000 and 2010 was conducted in orderurther explore the possibility that reduction inorker benefits may have contributed to a reduc-
ion in worker absenteeism. Table 4 contains resultsrom bivariate �2 tests of association between theear and absenteeism rates, while controlling forealth insurance status, availability of paid sickeave and pay type. The differences in absen-eeism rates between 2000 and 2010 were foundo be significant even when controlling for the vari-bles measuring the availability of paid sick leavep < 0.01) and pay type (p < 0.01). However, whenontrolling for health insurance status, specifically
or lack of health insurance, the difference in theate of absenteeism between 2000 and 2010 is noonger significant (p > 0.05). These findings suggest
Obesity and worker absenteeism e13
Table 4 Bivariate associations between health insurance status, paid sick leave, hourly pay and differences inworker absenteeism rates between 2000 and 2010.
Variable % of workers with illness absence
Year 2000 Year 2010 Diffa
Employment variablesHealth insurance status
Has health insurance 49.5 43.1 −6.4**
Uninsured 37.4 34.6 −2.8Current employer offers paid sick leave
Yes 54.1 49.5 −4.6**
No 39.6 32.7 −6.9**
Paid on hourly basisYes 49.7 42.6 −7.1**
No 45.6 40.2 −5.4**
Sample size 18,860 16,626aAdjusted for NHIS cluster, weight and stratum variables [26,27].b�2 was used to test for differences in worker absenteeism rates between 2000 and 2010.*p < 0.05, **p < 0.01.
thsorc
rthtctarWtaim
tsfsmcrmaloss
ap
ytwato1d
itcwatlcagh
waaprwa
hat the observed reductions in employer providedealth insurance coverage may account for at leastome of the decrease in overall worker absencebserved between 2000 and 2010, although moreesearch is clearly needed to fully explain thehanges in overall absence rates over time.
Another possible explanation for the change inates of absenteeism between 2000 and 2010 ishat the treatment and maintenance of chronicealth conditions may have improved over thisimeframe. It could be that those who have varioushronic health conditions are better able to manageheir health in 2010 compared to 2000. This couldccount for some of the change in absenteeismates observed between the two time periods.hile the data used in this study are not sufficient
o address this question, the efficacy of treatmentnd maintenance of chronic health conditions is anmportant component of occupational health anderits more focused study in future research.Although this study has shed light on some impor-
ant aspects of workplace absenteeism, there areome limitations to consider. First, the data usedor this study were compiled from self-reportedurvey measurements only, and no direct measure-ents of absence from employers or measures of
hronic health condition diagnoses from medicalecords were used. This is a limitation in that theeasurements of the variables under consideration
re potentially subject to recall bias, which mayead to under or over estimation of key variables
f interest by respondents. Although this is con-idered a limitation, the use of self-report data intudies of occupational health in general, as wellflh
s worker absenteeism specifically, is a standardractice [1,35].
Second, only two time periods, covering a 10-ear period, were analyzed in order to assesshe stability of the observed effects of over-eight/obesity and chronic health condition onbsenteeism. It is possible that other differences inhese effects may be apparent if a broader periodf time is considered, such as 3 time periods from990 to 2000 to 2010, or perhaps examination ofifferences over 5-year increments.
Third, the samples used in this study arendependent, cross-sectional samples, ratherhan longitudinal. Therefore, any within-subjecthanges for variables of interest, such as over-eight/obesity, chronic health condition andbsence, over time are not accounted for inhis analysis. However, the inclusion of suchongitudinal measurements within-subjects wouldontribute to knowledge of how individual workerbsenteeism is affected over time by the pro-ression of overweight/obesity and other chronicealth conditions from onset to the present.
Finally, this study is limited to measures oforker absenteeism only and does not include anyssessment of the effects of overweight/obesitynd other chronic health conditions on workerresenteeism, which is economic loss due toeduced productivity of workers who continue toork while ill. The fact that there has been
reduction in the overall worker absence rate
rom 2000 to 2010, even though the preva-ence of overweight/obesity and the other chronicealth conditions has increased, suggests that more
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
e14
workers in 2010 are either choosing to work whileill or are forced to work while ill due to thereduction of employer benefits, such as paid sickleave, and perhaps out of fear of losing theirjob in a difficult economic environment. Futurestudies on this topic would thus benefit from (1)the examination of additional sources of directmeasures of overweight/obesity, chronic healthcondition and absenteeism from employer andmedical records, (2) the examination of longi-tudinal data, (3) the examination of additionaltime periods, (4) the integration of measures ofworker presenteeism in addition to absenteeism,and (5) examination of the extent to which changesin economic conditions, employer-provided healthbenefits, and improvements in the treatment andmaintenance of chronic health conditions has ledto decreased rates of work absenteeism overtime.
References
[1] Howard K, Howard J, Smyth A. The problem of absenteeismand presenteeism in the workplace. In: Gatchel R, SchultzI, editors. Handbook of Occupational Health and Wellness.Springer; 2012.
[2] Prater T, Smith K. Underlying factors contributing to pre-senteeism and absenteeism. J Bus Econ Res 2011;9(6):1—14.
[3] Loeppke R, Taitel M, Richling D, Parry T, Kessler RC, HymelP, et al. Health and productivity as a business strategy. JOccup Environ Med 2007;49(7):712—21.
[4] Palmer KT, Calnan M, Wainwright D, Poole J, O’Neill C, Win-terbottom A, et al. Disabling musculoskeletal pain and itsrelation to somatization: a community-based postal survey.Occup Med 2005;55(8):612—7.
[5] Burton W, Morrison A, Yuan Y, Li T, Marioni R, MacleanR. Productivity cost model of the treatment of rheuma-toid arthritis with abatacept. J Med Econ 2008;11:3—21.
[6] Roche A, Pidd K, Berry J, Harrison J. Workers’ drinkingpatterns: the impact on absenteeism in the Australian work-place. Addiction 2008;103:738—48.
[7] van Duijvenbode D, Hoozemans M, vanPoppel M, ProperK. The relationship between overweight and obesity, andsick leave: a systematic review. Int J Obes 2009;33:807—16.
[8] Moens G, Van Gaal L, Muls E, Viaene B, Jacques P. Bodymass index and health among the working population. EurJ Public Health 1999;9:119—23.
[9] Thompson D, Edelsberg J, Kinsey J, Oster G. Estimated eco-nomic costs of obesity to US business. Am J Health Promot1998;5(2):120—7.
[10] Neovius K, Johansson K, Kark M, Neovius M. Obesitystatus and sick leave: a systematic review. Obes Rev2009;10:17—27.
[11] WHO. BMI Classification. World Health Organization; 2012.[12] Finkelstein E, Fiebelkorn I, Wang G. The costs of obe-
sity among full-time employees. Am J Health Promot2005;20(1):45—51.
[
[
J.T. Howard, L.B. Potter
13] Finkelstein E, Fiebelkorn I, Wang G. State-level estimates ofannual medical expenditures attributable to obesity. ObesRes 2004;12:18—24.
14] Thompson D, Wolfe A. The medical-care cost burden ofobesity. Obes Rev 2001;2:189—97.
15] Birmingham C, Muller J, Palepu A, Spinelli J, AnisA. The cost of obesity in Canada. Can Med Assoc J1999;160(4):483—8.
16] Aldana S. Financial impact of health promotion programs:a comprehensive review of the literature. Am J Health Pro-mot 2001;15(5):296—320.
17] Adams T, Cowen V. Health risk factors and absen-teeism among university employees. Am J Health Stud2004;19(3):129—37.
18] Burton W, Chen C, Schultz A, Edington D. The economiccosts associated with body mass index in a workplace. JOccup Environ Med 1998;40(9):786—92.
19] Narbro K, Johsson E, Larsson B, Waaler H, Wedel H,Sjostron L. Economic consequences of sick leave andearly retirement in obese Swedish women. Int J Obes1998;20:895—903.
20] Tucker L, Friedman G. Obesity and absenteeism: an epi-demiologic study of 10,825 employed adults. Am J HealthPromot 1998;12(3):202—7.
21] Tsai S, Ahmed F, Wendt J, Bhojani F, Donnelly R. The impactof obesity on illness absence and productivity in an indus-trial population of petrochemical workers. Ann Epidemiol2008;18:8—14.
22] Goetzel R, Gibson T, Short M, Chu B, Waddell J, BowenJ, et al. A Multi-worksite analysis of the relation-ships among body mass index, medical utilization, andworker productivity. J Occup Environ Med 2010;52(1):52—8.
23] Pronk N, Martinson B, Kessler R, Beck A, Simon G, WangP. The association between work performance and physi-cal activity, cardiorespiratory fitness, and obesity. J OccupEnviron Med 2004;46:19—25.
24] Cawley J, Rizzo J, Haas K. The association of dia-betes with job absenteeism costs among obese andmorbidly obese workers. J Occup Environ Med 2008;50(5):527—34.
25] Harvey S, Glozier N, Carlton O, Mykletun A, Hender-son M, Hotopf M, et al. Obesity and sickness absence:results from the CHAP study. Occup Med 2010;60:362—8.
26] National Center for Health Statistics. Data File Documen-tation, National Health Interview Survey, 2010 (machinereadable data file and documentation). Hyattsville, MD:National Center for Health Statistics, Centers for DiseaseControl and Prevention; 2011.
27] National Center for Health Statistics. Data File Documen-tation, National Health Interview Survey, 2000 (machinereadable data file and documentation). Hyattsville, MD:National Center for Health Statistics, Centers for DiseaseControl and Prevention; 2001.
28] Cohen J, Cohen P. Applied multiple regression/correlationanalysis for the behavioral sciences. 2nd ed. Mahwah, NJ:Lawrence Erlbaum Associates, Inc; 1983.
29] Hanushek E, Jackson J. Statistical methods for social scien-tists. San Diego, CA: Academic Press, Inc; 1977.
30] Ott R, Longnecker M. An introduction to statistical methodsand data analysis. 6th ed Brooks/Cole, Cengage Learning;2010.
31] Tabachnick B, Fidell L. Using multivariate statistics. 5th ed.Boston, MA: Pearson Education; 2007.
32] Catalano R. Health, medical care, and economic crisis. NEngl J Med 2009;360(8):749—51.

O
[
[
[
besity and worker absenteeism
33] Fronstin P. The impact of the 2007—2009 recession on work-ers’ health coverage. In: EBRI issue brief, no. 356. Employee
Benefit Research Institute; 2011. p. 1—20.34] Bernstein J. Impact of the economy on health care. In:Changes in health care financing and organization. RobertWood Johnson Foundation; 2011.
Available online at www
e15
35] Kivimaki M, Head J, Ferrie J, Shipley M, Vahtera J, MarmotM. Sickness absence as a global measure of health: evidence
from mortality in the Whitehall II prospective cohort study.Br Med J 2003;237:364—9..sciencedirect.com