Embed Size (px)
Citation preview
Approach to Syncope
VIC VYAS, MD
STAFF ELECTROPHYSIOLOGIST
SOUTH LOUISIANA MEDICAL ASSOCIATES
Disclosures
No financial disclosures to report
No off-label uses of medications or devices will be discussed
2
Definition
A transient loss of consciousness (T-LOC) due to transient cerebral
hypoperfusion characterized by:
Rapid onset
Short duration
Spontaneous complete resolution
Syncope is a symptom, not a diagnosis
Determination of etiology allows for diagnosis
Brignole et al. Europace, 2004;6:467-537
3
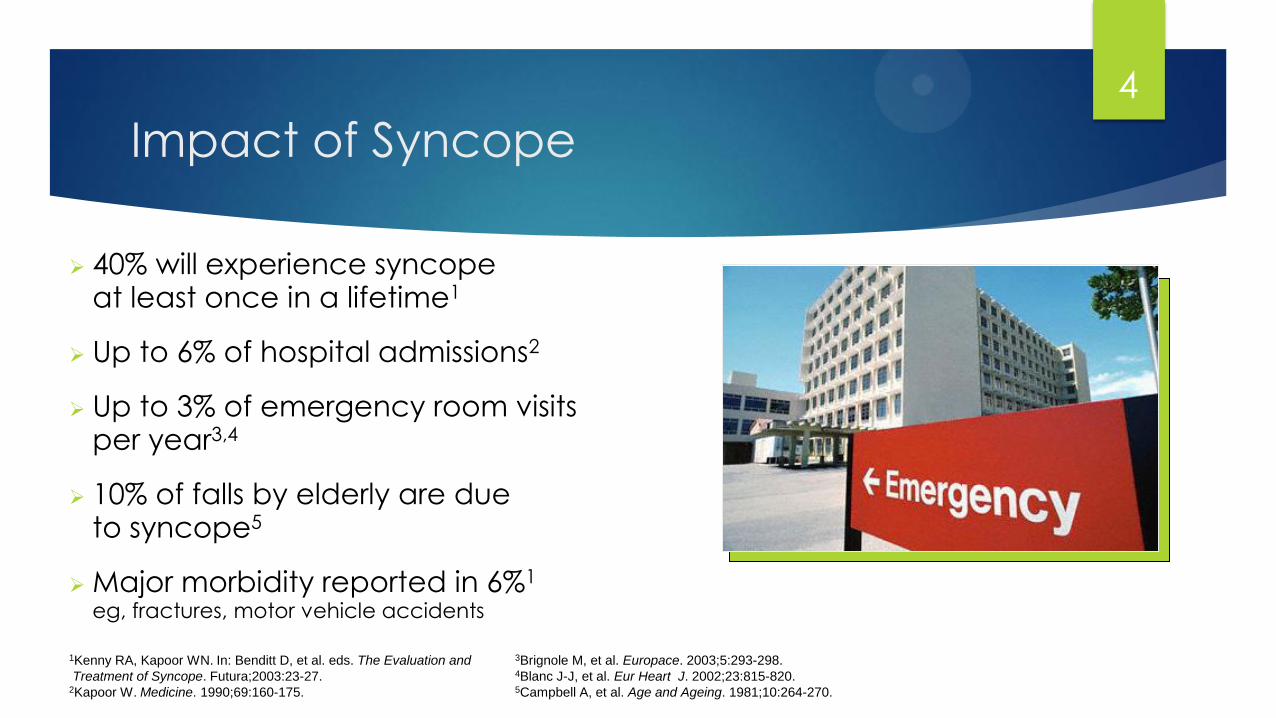
Impact of Syncope
1Kenny RA, Kapoor WN. In: Benditt D, et al. eds. The Evaluation and
Treatment of Syncope. Futura;2003:23-27. 2Kapoor W. Medicine. 1990;69:160-175.
3Brignole M, et al. Europace. 2003;5:293-298. 4Blanc J-J, et al. Eur Heart J. 2002;23:815-820. 5Campbell A, et al. Age and Ageing. 1981;10:264-270.
40% will experience syncope at least once in a lifetime1
Up to 6% of hospital admissions2
Up to 3% of emergency room visits per year3,4
10% of falls by elderly are due to syncope5
Major morbidity reported in 6%1 eg, fractures, motor vehicle accidents
4
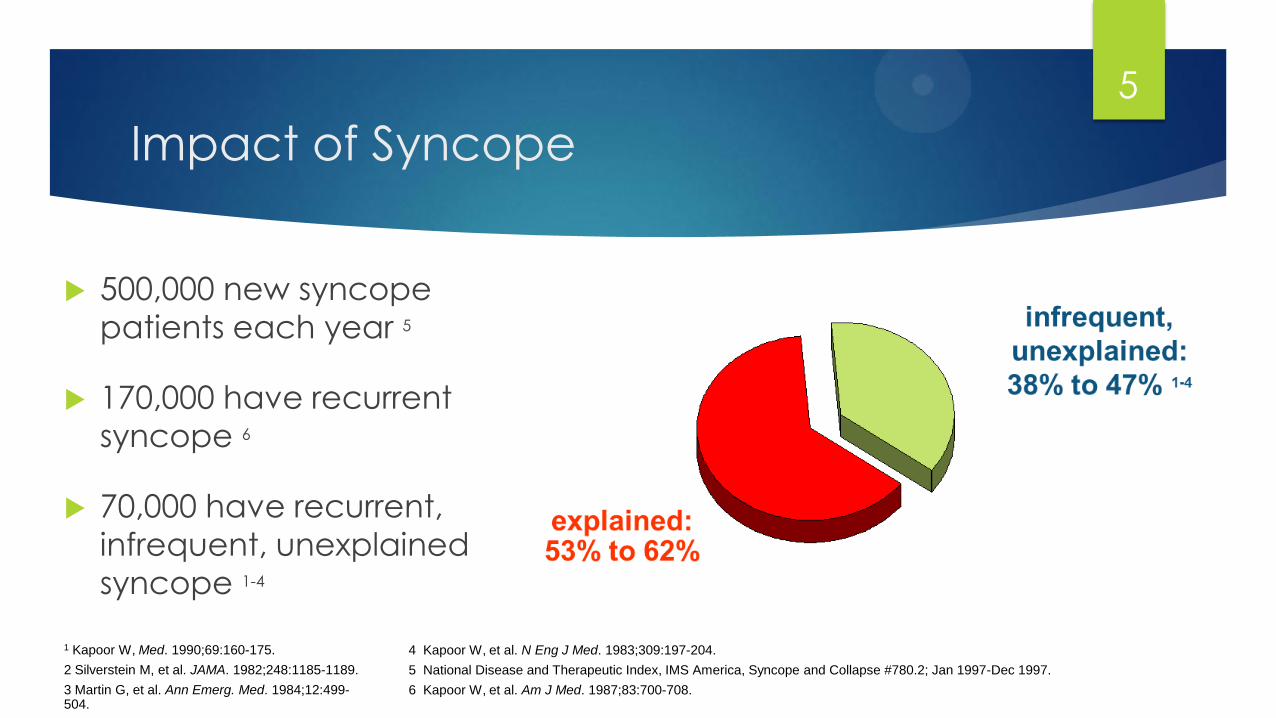
Impact of Syncope
500,000 new syncope
patients each year 5
170,000 have recurrent
syncope 6
70,000 have recurrent,
infrequent, unexplained
syncope 1-4
1 Kapoor W, Med. 1990;69:160-175.
2 Silverstein M, et al. JAMA. 1982;248:1185-1189.
3 Martin G, et al. Ann Emerg. Med. 1984;12:499-504.
4 Kapoor W, et al. N Eng J Med. 1983;309:197-204.
5 National Disease and Therapeutic Index, IMS America, Syncope and Collapse #780.2; Jan 1997-Dec 1997.
6 Kapoor W, et al. Am J Med. 1987;83:700-708.
5
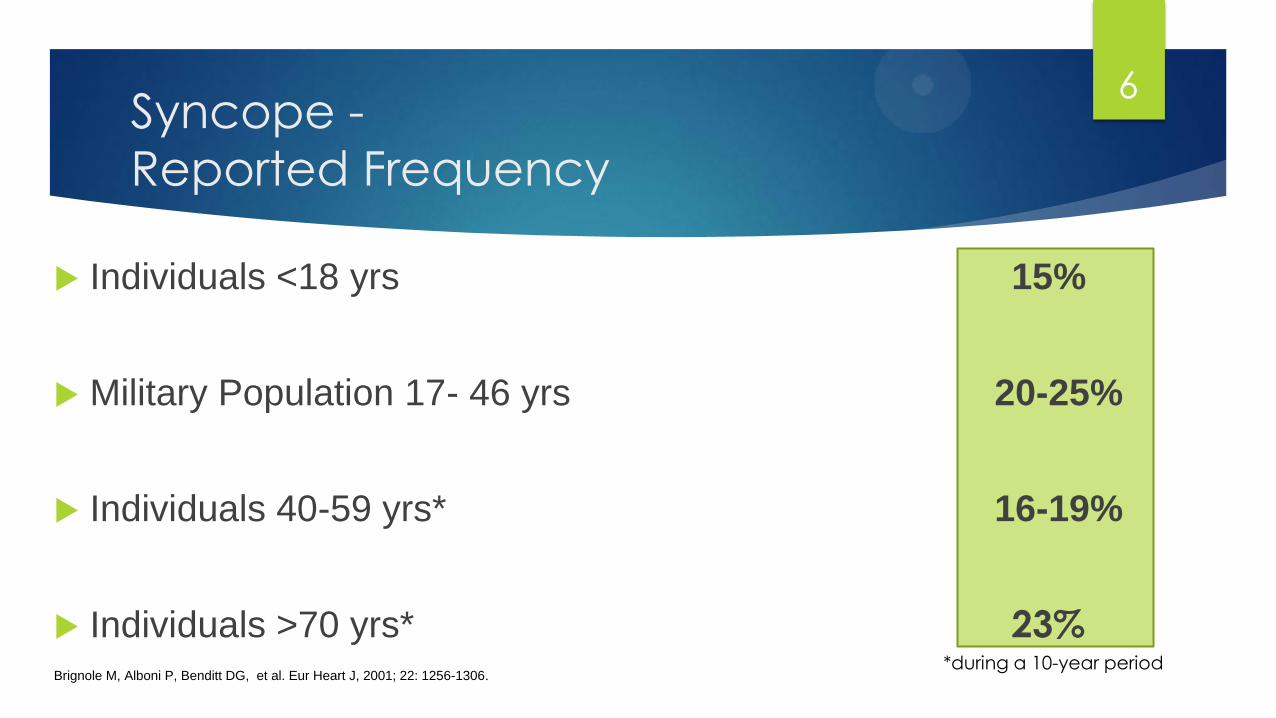
Syncope -
Reported Frequency
Individuals <18 yrs 15%
Military Population 17- 46 yrs 20-25%
Individuals 40-59 yrs* 16-19%
Individuals >70 yrs* 23% *during a 10-year period
Brignole M, Alboni P, Benditt DG, et al. Eur Heart J, 2001; 22: 1256-1306.
6
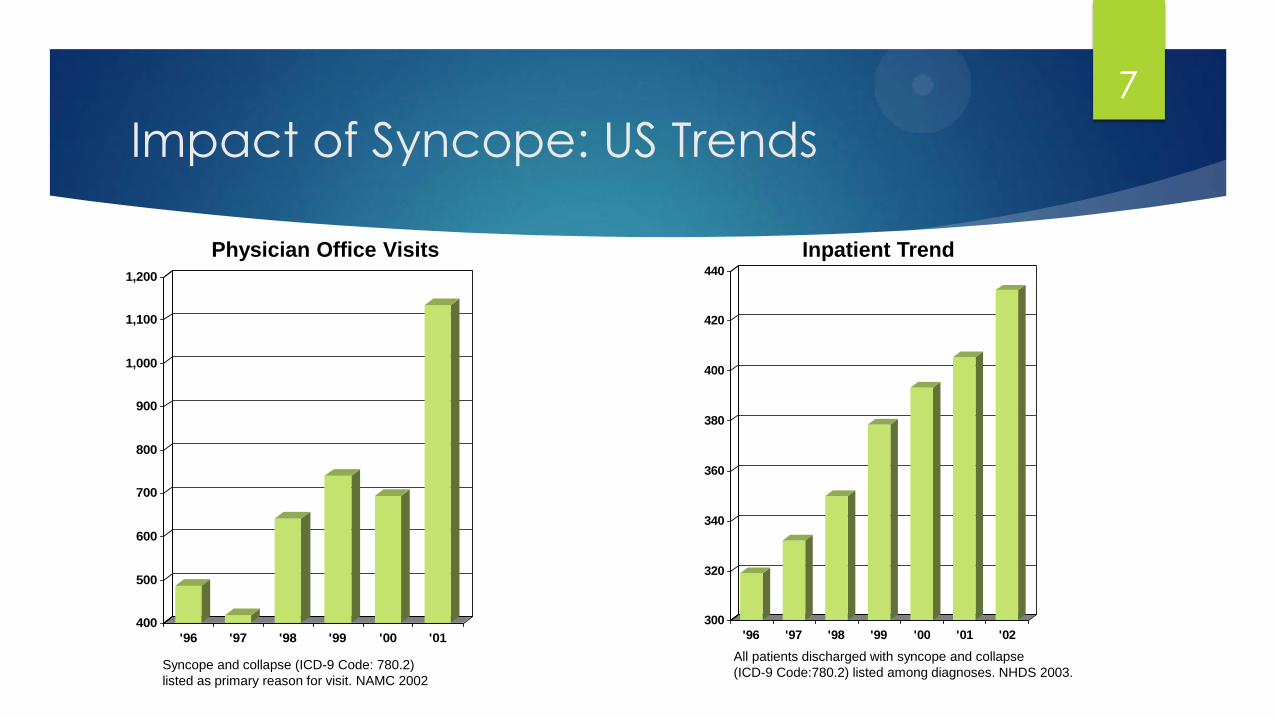
Impact of Syncope: US Trends
400
500
600
700
800
900
1,000
1,100
1,200
'96 '97 '98 '99 '00 '01
300
320
340
360
380
400
420
440
'96 '97 '98 '99 '00 '01 '02
All patients discharged with syncope and collapse
(ICD-9 Code:780.2) listed among diagnoses. NHDS 2003.
Inpatient Trend
Physician Office Visits
Syncope and collapse (ICD-9 Code: 780.2)
listed as primary reason for visit. NAMC 2002
7

Impact of Syncope: Quality of Life
1Linzer M. Journal of Clinical Epidemiology, 1991;44:1037. 2Linzer M. Journal of General Internal Medicine, 1994;9:181.
0
20
40
60
80
100
Anxiety/
Depression
Alter Daily
Activities
Restricted
Driving
Change
Employment
73%1 71%2 60%2 37%2
8
Impact of Syncope: Cost
Mean cost - $5,400 per hospitalization
Estimated total annual costs for syncope-related hospitalizations - $2.4
billion
Sun et al. American Journal of Cardiology, 2005:95;668-671
9
Syncope… or something else?
High likelihood of T-LOC due to global cerebral hypoperfusion (syncope) if:
Complete LOC
Loss of postural tone
Transient LOC with rapid onset and short duration
Spontaneous, complete recovery
10

Mimics
Consider disorders that present
without impairment of consciousness Cataplexy Drop Attacks
Falls TIA of Carotid
Origin
Pseudsyncope
11
Mimics
Consider disorders that can present
with LOC but are not due to global
cerebral hypoperfusion
Epilepsy Metabolic disorders
Intoxication Vertebrobasilar
TIA
Trauma
12
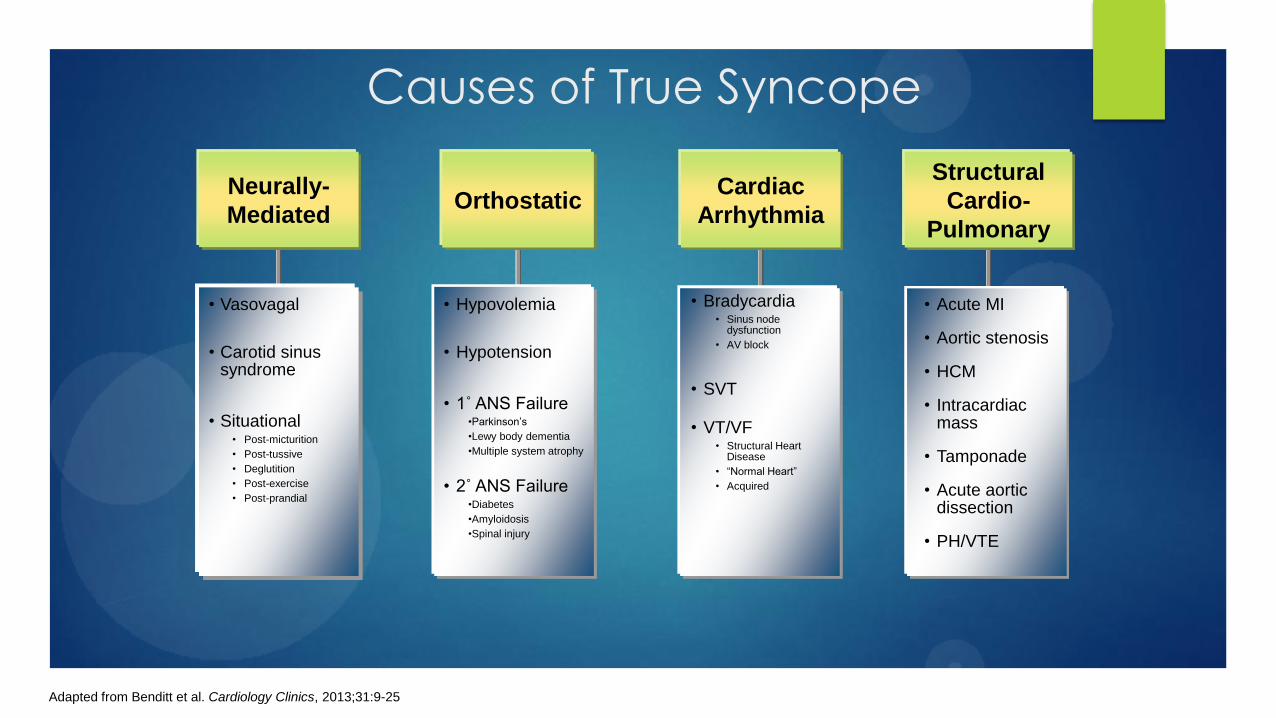
Causes of True Syncope
Orthostatic Cardiac
Arrhythmia
Structural
Cardio-
Pulmonary
• Vasovagal
• Carotid sinus syndrome
• Situational • Post-micturition
• Post-tussive
• Deglutition
• Post-exercise
• Post-prandial
• Hypovolemia
• Hypotension
• 1˚ ANS Failure •Parkinson’s
•Lewy body dementia
•Multiple system atrophy
• 2˚ ANS Failure •Diabetes
•Amyloidosis
•Spinal injury
• Bradycardia • Sinus node
dysfunction
• AV block
• SVT
• VT/VF • Structural Heart
Disease
• “Normal Heart”
• Acquired
• Acute MI
• Aortic stenosis
• HCM
• Intracardiac mass
• Tamponade
• Acute aortic dissection
• PH/VTE
Neurally-
Mediated
Adapted from Benditt et al. Cardiology Clinics, 2013;31:9-25
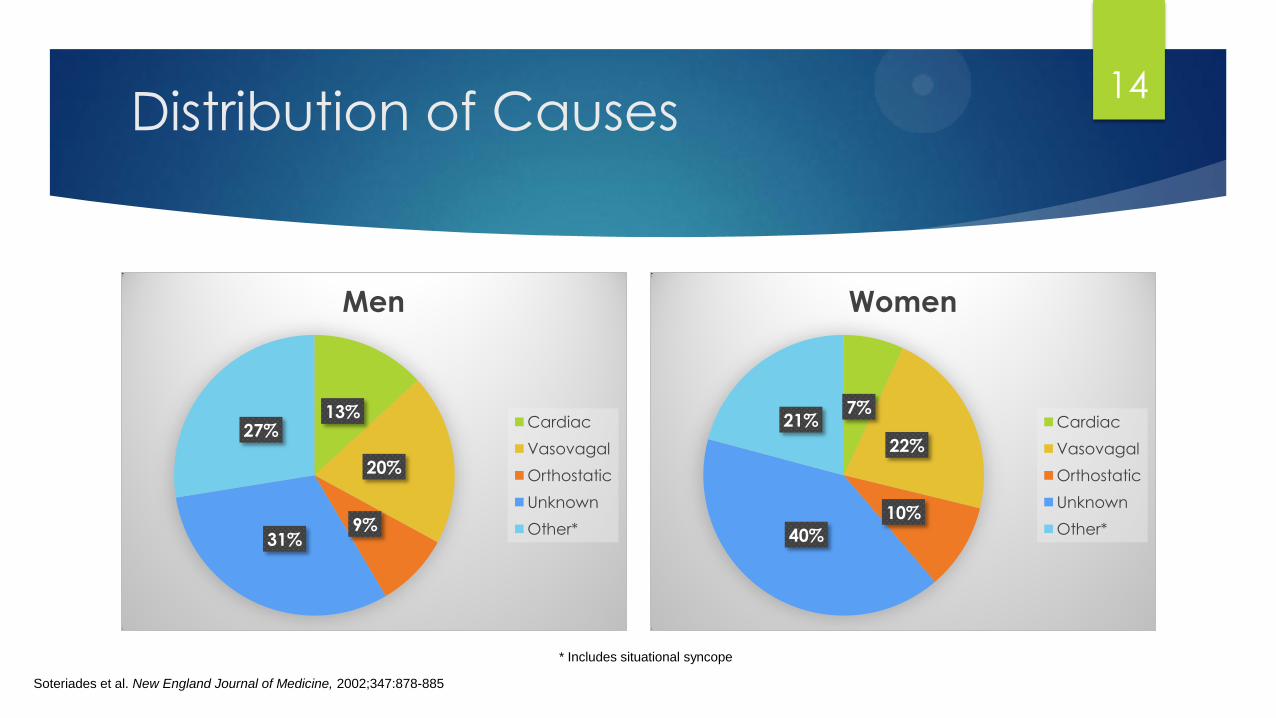
Distribution of Causes
13%
20%
9% 31%
27%
Men
Cardiac
Vasovagal
Orthostatic
Unknown
Other*
Soteriades et al. New England Journal of Medicine, 2002;347:878-885
7%
22%
10%
40%
21%
Women
Cardiac
Vasovagal
Orthostatic
Unknown
Other*
* Includes situational syncope
14
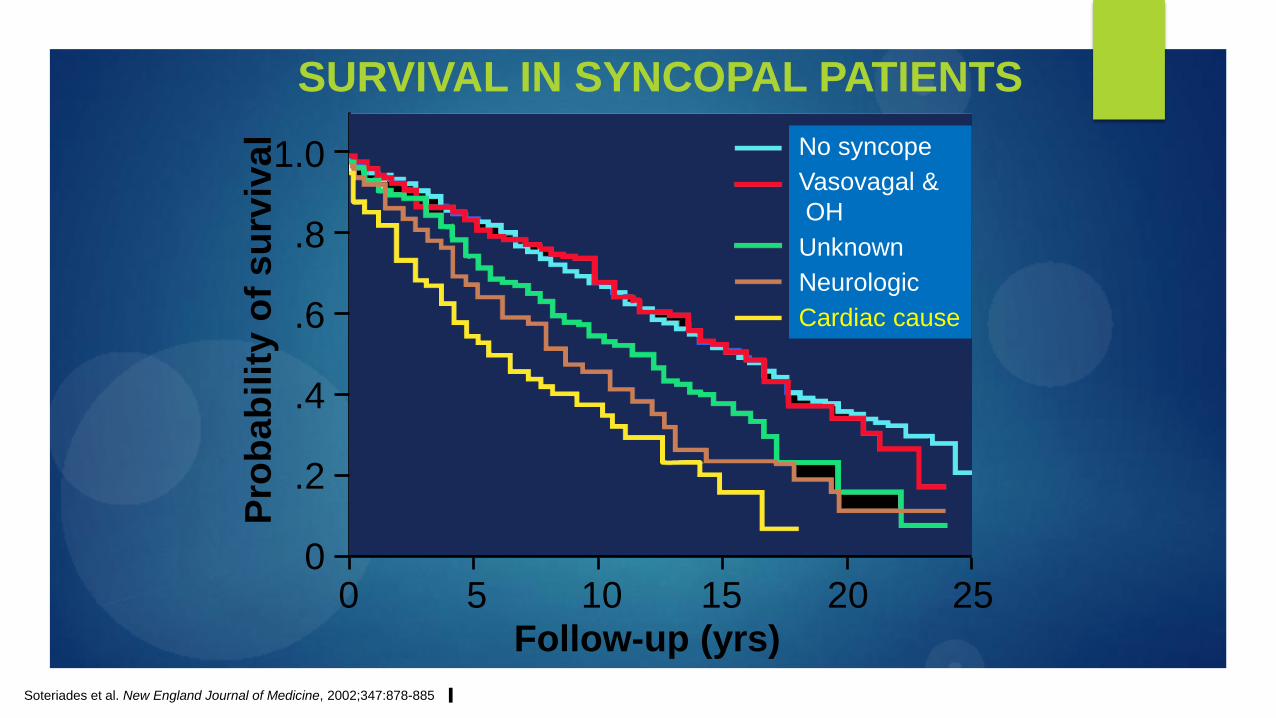
SURVIVAL IN SYNCOPAL PATIENTS
Follow-up (yrs)
Soteriades et al. New England Journal of Medicine, 2002;347:878-885
0 5 10 15 20 25
Pro
bab
ilit
y o
f s
urv
ival
1.0
.8
.6
.4
.2
0
No syncope
Vasovagal &
OH
Unknown
Neurologic
Cardiac cause
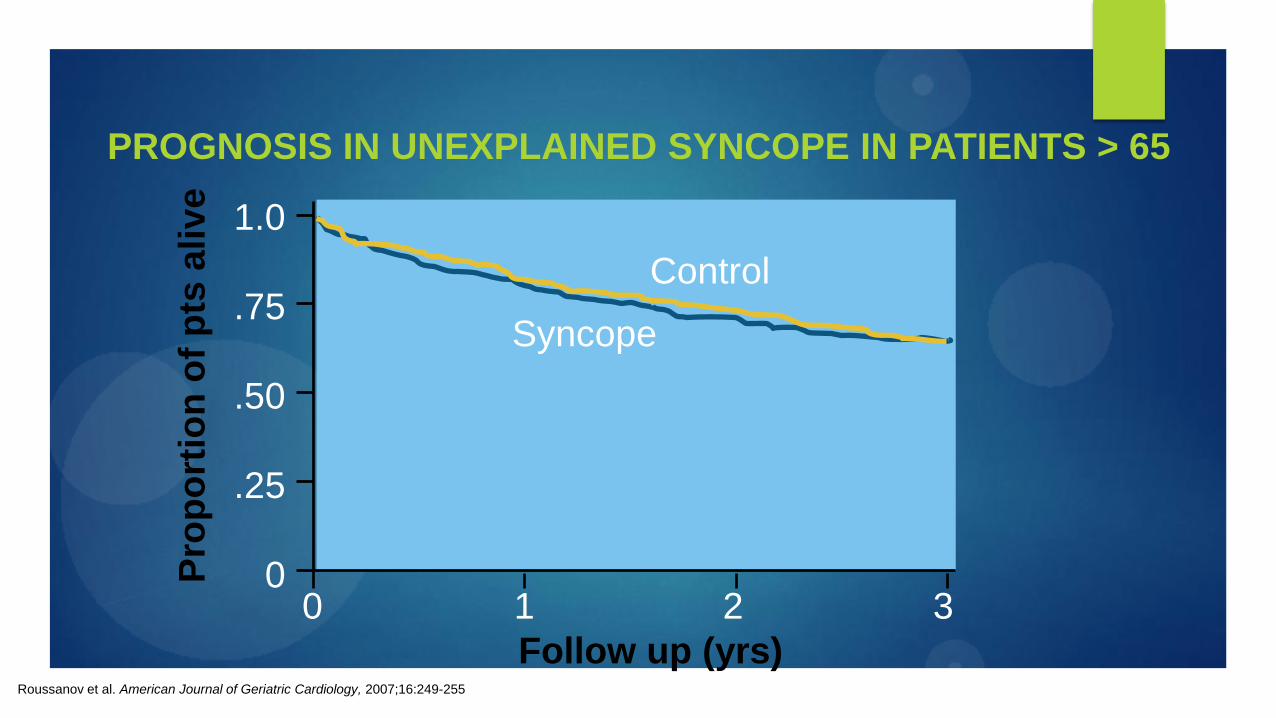
PROGNOSIS IN UNEXPLAINED SYNCOPE IN PATIENTS > 65
Pro
po
rtio
n o
f p
ts a
live
1.0
.75
.50
.25
0 0 1 2 3
Follow up (yrs) Roussanov et al. American Journal of Geriatric Cardiology, 2007;16:249-255
Control
Syncope
Determining Etiology
Step 1: Detailed History
Number, frequency and duration of episodes
Episodes scattered over many years tend to be benign
Frequent episodes over short period of time suggests a more ominous etiology (i.e. intermittent AVB or paroxysmal tachyarrhythmias)
Onset
An extended prodrome suggests vasovagal process whereas abrupt LOC without prodrome is more common in cardiac syncope
Body position
Supine erect positional change preceding event suggests orthostatic process
Reflex syncope usually occurs in upright position
Syncope while supine is worrisome for arrhythmia
17
Determining Etiology
Step 1: Detailed History (cont.)
Provocative factors
During/immediately after exercise,
During/immediately after urination, coughing, defecation or swallowing
While standing in warm/crowded place
During prolonged standing
In association with emotional stress, fear or intense pain
Immediately after turning neck
Associated symptoms preceding the event
Nausea, vomiting, feeling cold/clammy
Palpitations
Chest pain
Dyspnea
18
Determining Etiology
Step 1: Detailed History (cont.)
Associated symptoms following the event
Persistent nausea, diaphoresis or pallor suggests vasovagal process
Profound resultant fatigue is also characteristic of a vasovagal process
Significant neurological changes or confusion during the recovery period suggests a primary CNS process (CVA, seizure)
Bystander report
Abrupt loss of postural tone?
Total duration of LOC
Physical signs (tonic/clonic movements, tongue biting)? Before or after collapse?
19
Determining Etiology
Step 1: Detailed History (cont.)
Past Medical History
CAD or structural heart disease?
Risk factors for ASCVD or structural heart disease?
Seizure disorder or other neurological conditions?
Social History
Use of intoxicants?
20

Determining Etiology
Step 1: Detailed History (cont.)
Family History
Sudden cardiac death in family members <40
Any known hereditary disorders that would predispose to SCD?
Familial cardiomyopathy (HCM, ARVC)
Familial channelopathy (Brugada, LQTS, CPVT)
Medications
Diuretics hypovolemia, electrolyte derangements predisposing to arrhythmia
Antihypertensives hypotension
Acquired LQTs www.crediblemeds.org
21
Determining Etiology
Step 2: Physical Exam
Orthostatic vital signs
Supine, seated, standing
3-5 minutes in each position with serial VS measurements throughout
Real time telemetry monitoring preferred
Non-invasive BP monitoring (i.e. “beat to beat”
measurement) is ideal but not universally available
22
Determining Etiology
23

Determining Etiology
Step 2: Physical Exam (cont.)
Comprehensive cardiovascular exam
Evidence of acute cardiopulmonary process?
Evidence of structural heart disease?
Neuro exam
Focal deficits?
Stigmata of Parkinson’s?
24
Determining Etiology
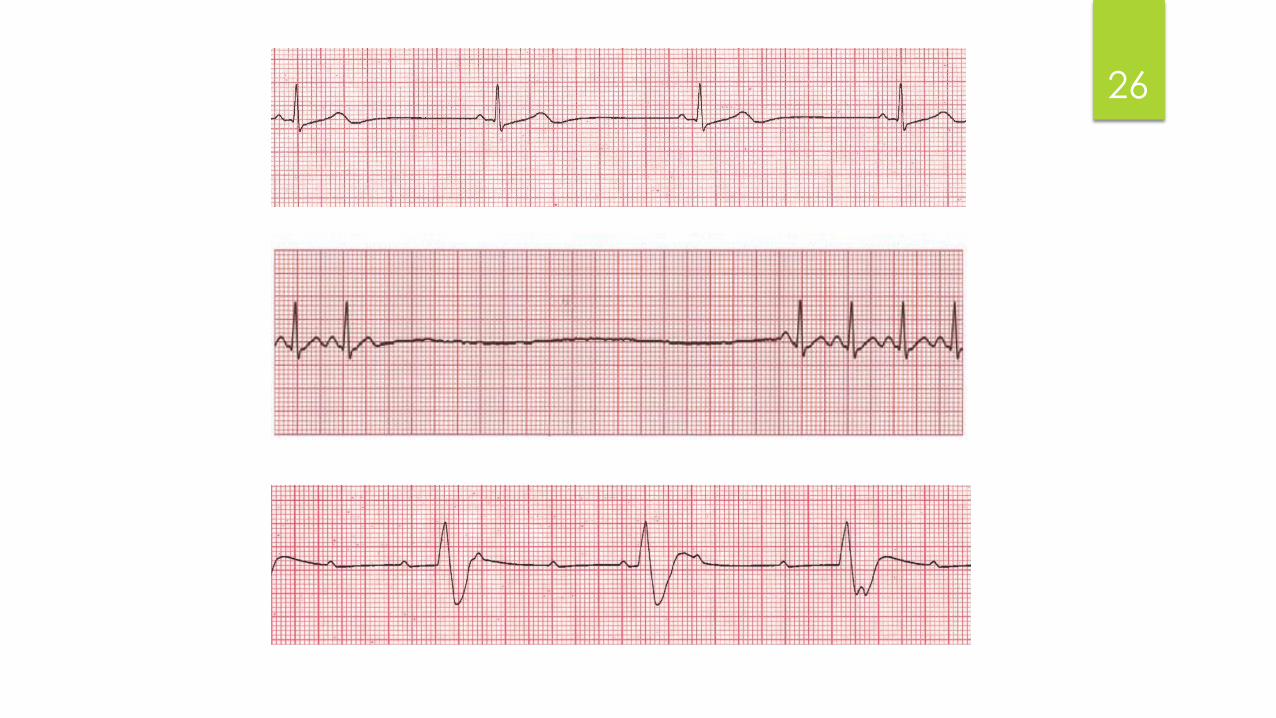
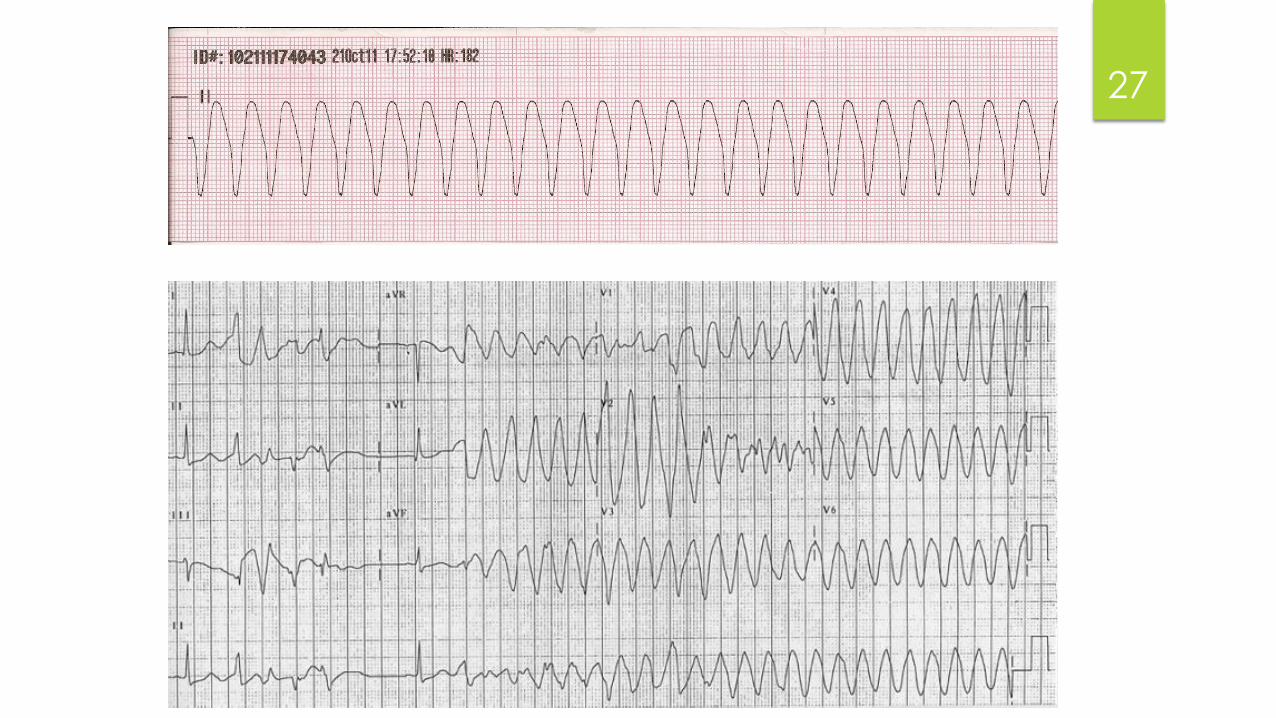
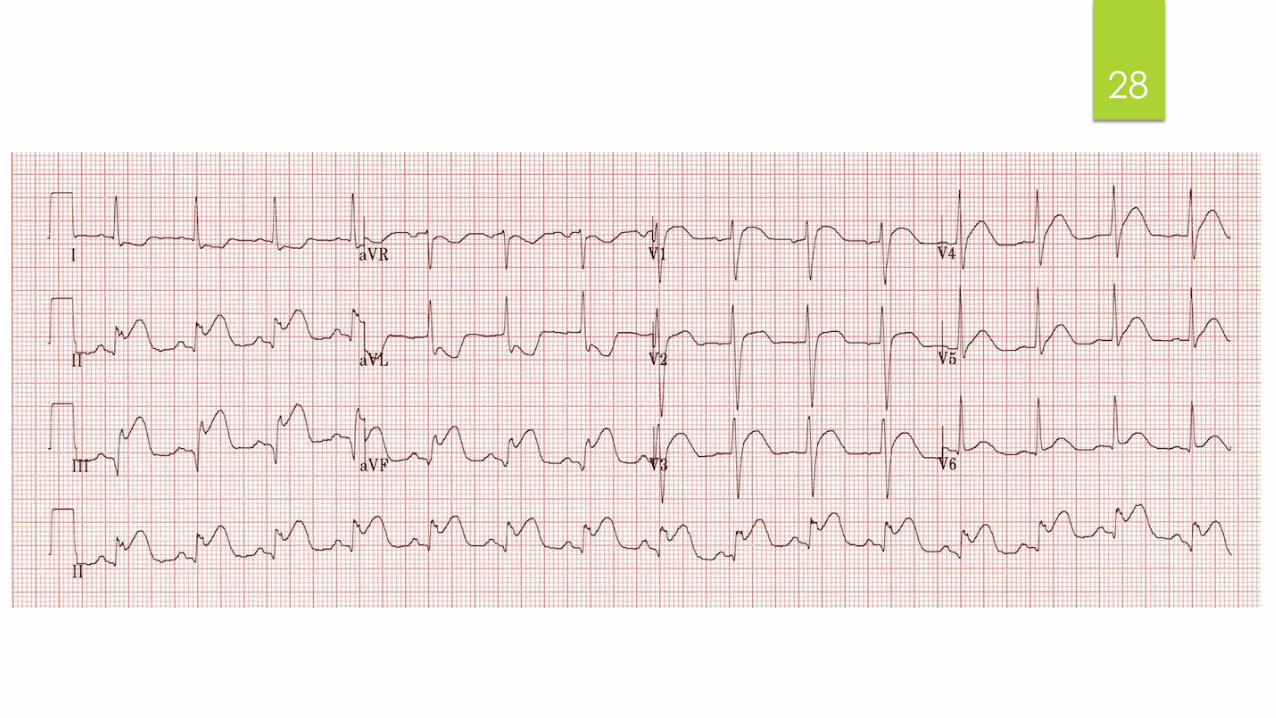
Step 3: Telemetry & ECG
Indicated in ALL patients with syncope
Limited yield but diagnostic if any of the
following are present:
Persistent sinus bradycardia (<40bpm) while
awake
Repetitive SA pauses >3 secs while awake
Mobitz II AVB
3rd degree AVB
Alternating LBBB/RBBB
Sustained tachyarrhythmia
Ischemic changes, particularly ST elevation
25
26
27
28
Determining Etiology
Step 3: ECG (cont.)
Suggestive of CV pathology (EP consultation recommended):
Bifascular block
LBBB or IVCD with QRSd >120ms
LVH
Q waves
Sinus bradycardia >40bpm
Ventricular pre-excitation
Long/short QT interval
Brugada pattern
Epsilon waves suggesting ARVC
29
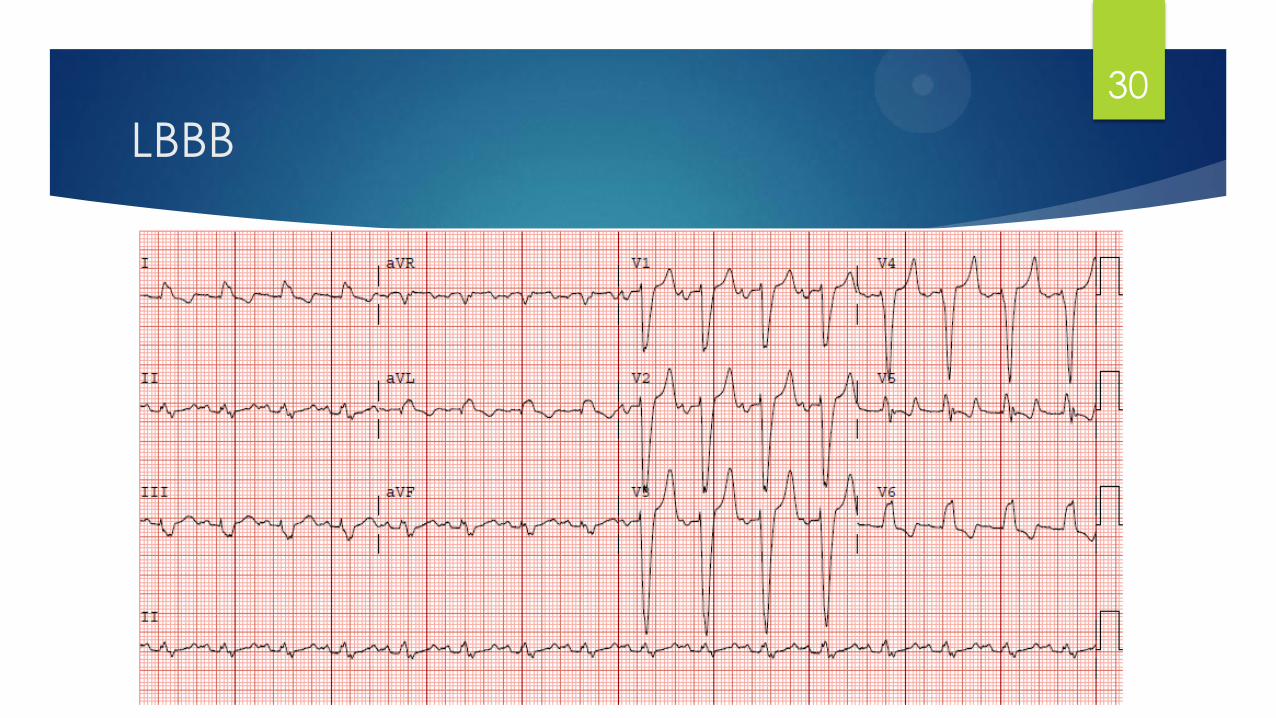
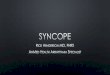
LBBB
30

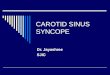
LVH
31
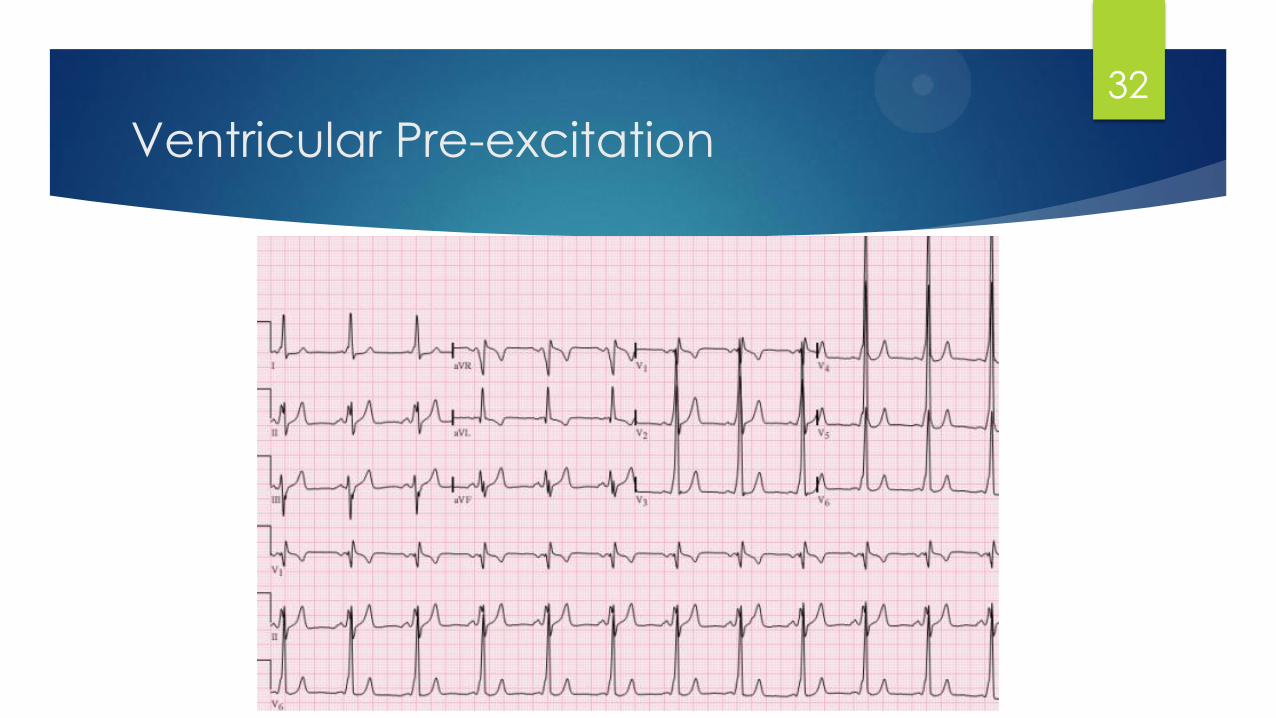
Ventricular Pre-excitation
32
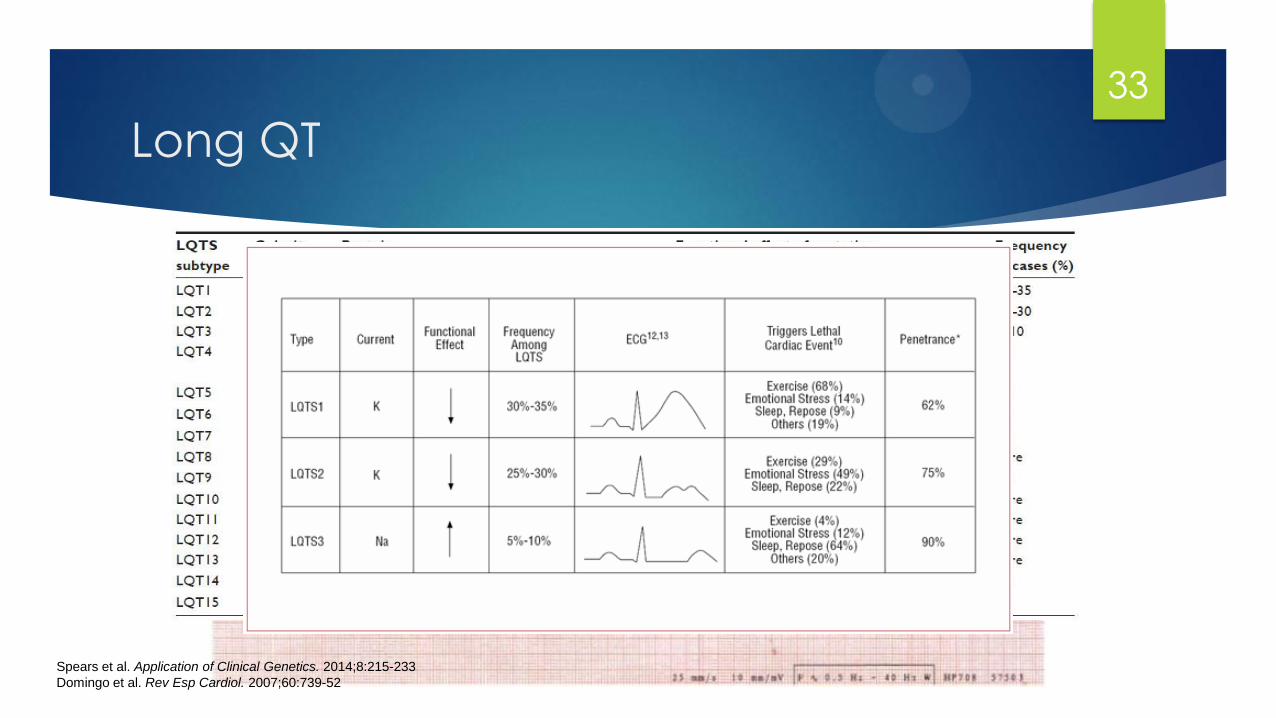
Spears et al. Application of Clinical Genetics. 2014;8:215-233
Domingo et al. Rev Esp Cardiol. 2007;60:739-52
Long QT
33
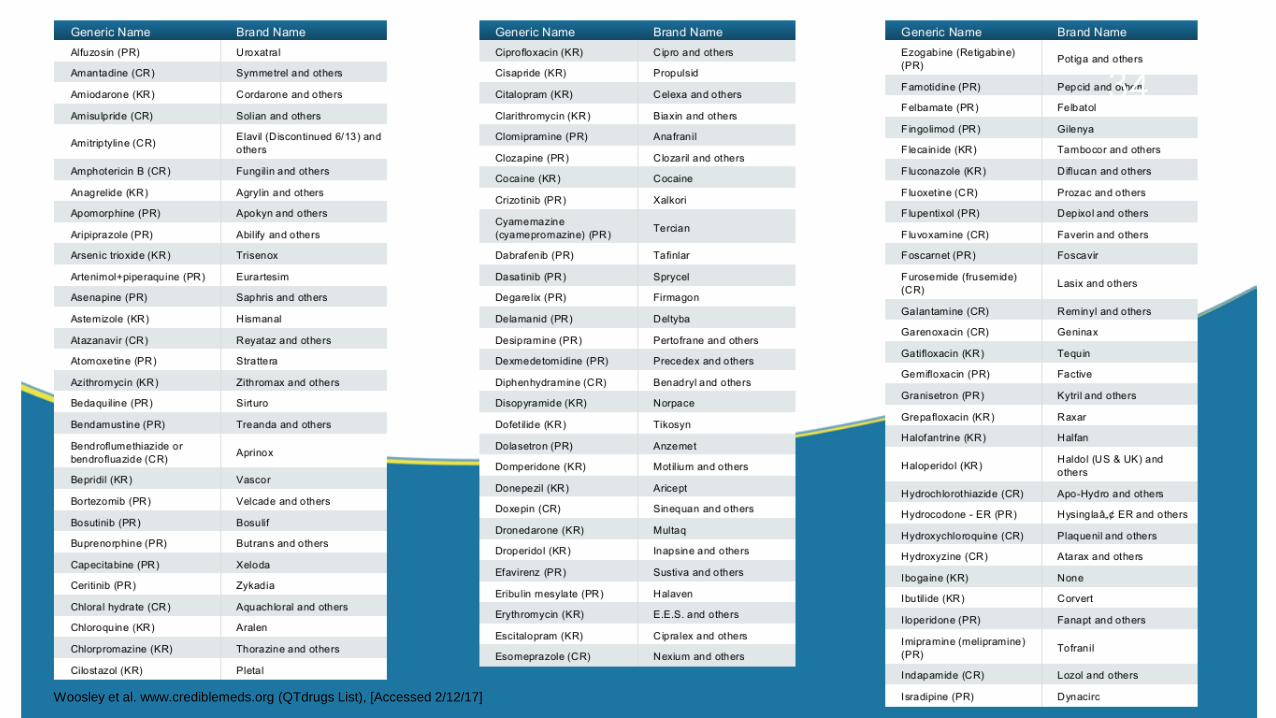
Woosley et al. www.crediblemeds.org (QTdrugs List), [Accessed 2/12/17]
34
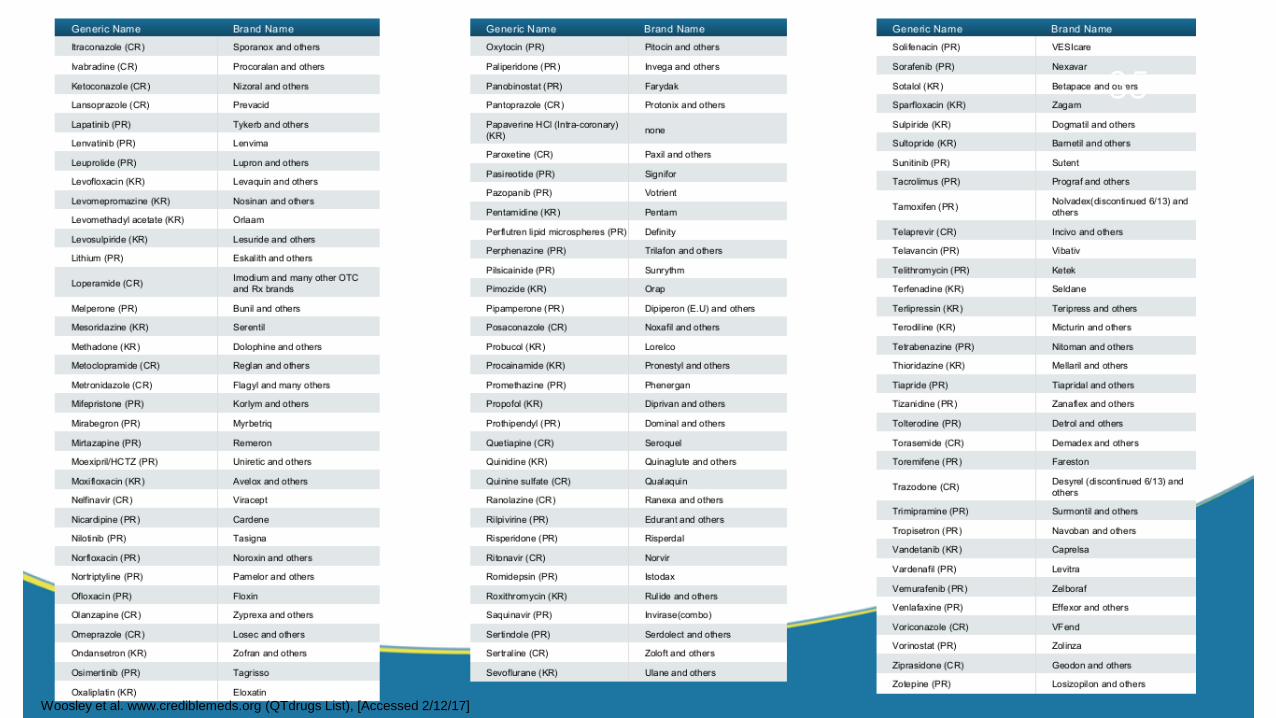
Woosley et al. www.crediblemeds.org (QTdrugs List), [Accessed 2/12/17]
35
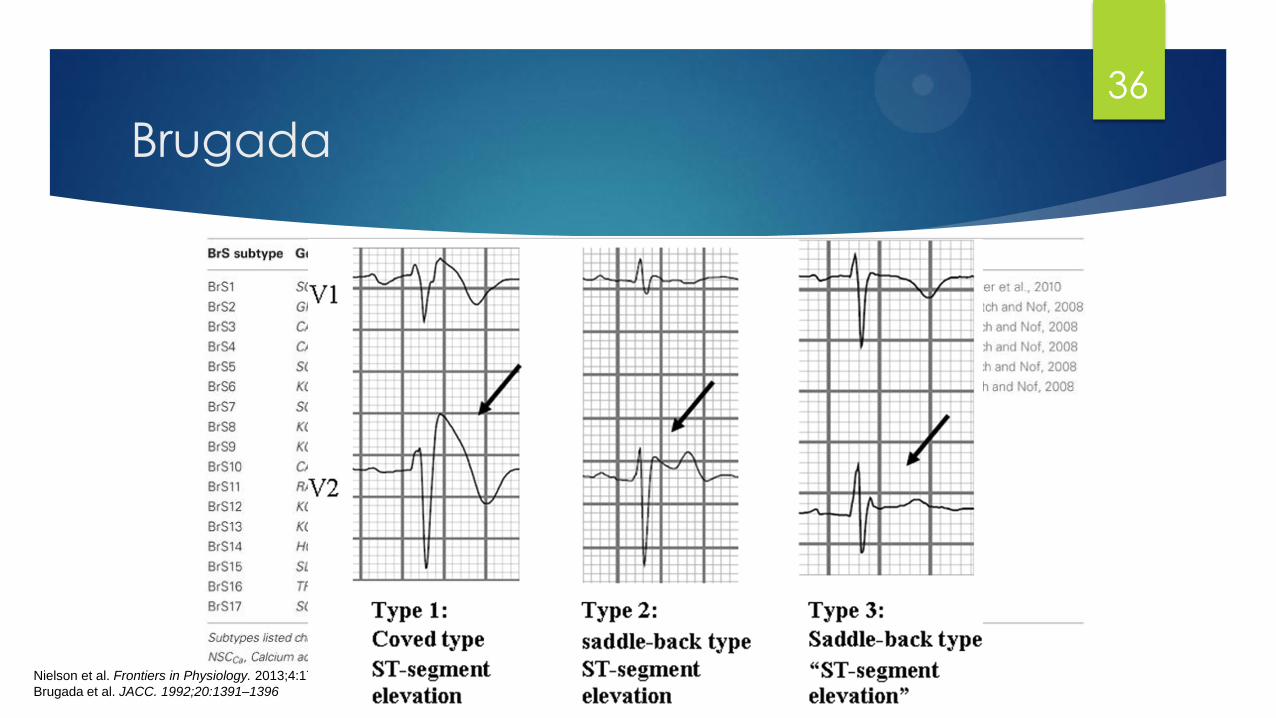
Nielson et al. Frontiers in Physiology. 2013;4:179
Brugada et al. JACC. 1992;20:1391–1396
Brugada
36

ARVC
Lang et al. Encyclopedia of Molecular Mechanisms of Disease; 2009:155
37
Determining Etiology
Step 4: Echocardiography
IF structural heart disease is evident or suggested by history,
exam or ECG.
Usually normal
Can reveal:
HFrEF
HCM
Valvulopathy
Intracardiac mass
Pericardial effusion
Acute right heart failure
38
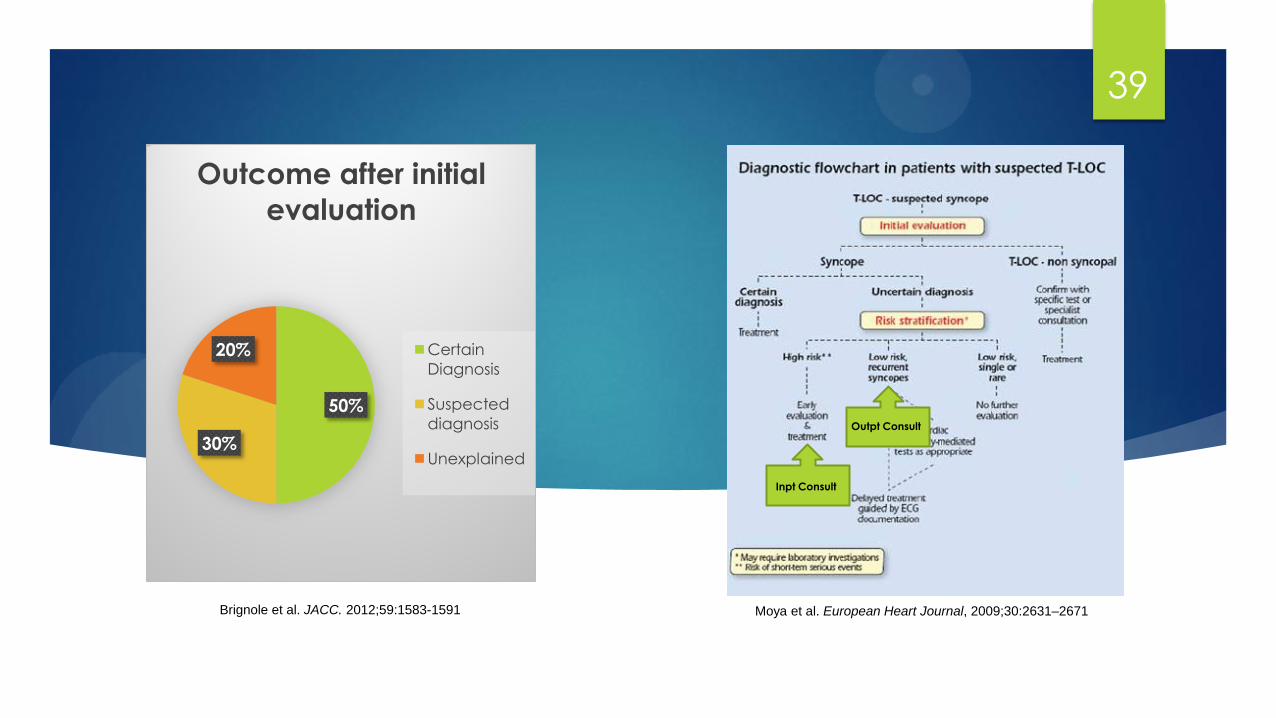
50%
30%
20%
Outcome after initial
evaluation
Certain
Diagnosis
Suspected
diagnosis
Unexplained
Brignole et al. JACC. 2012;59:1583-1591
Inpt Consult
Outpt Consult
39
Moya et al. European Heart Journal, 2009;30:2631–2671
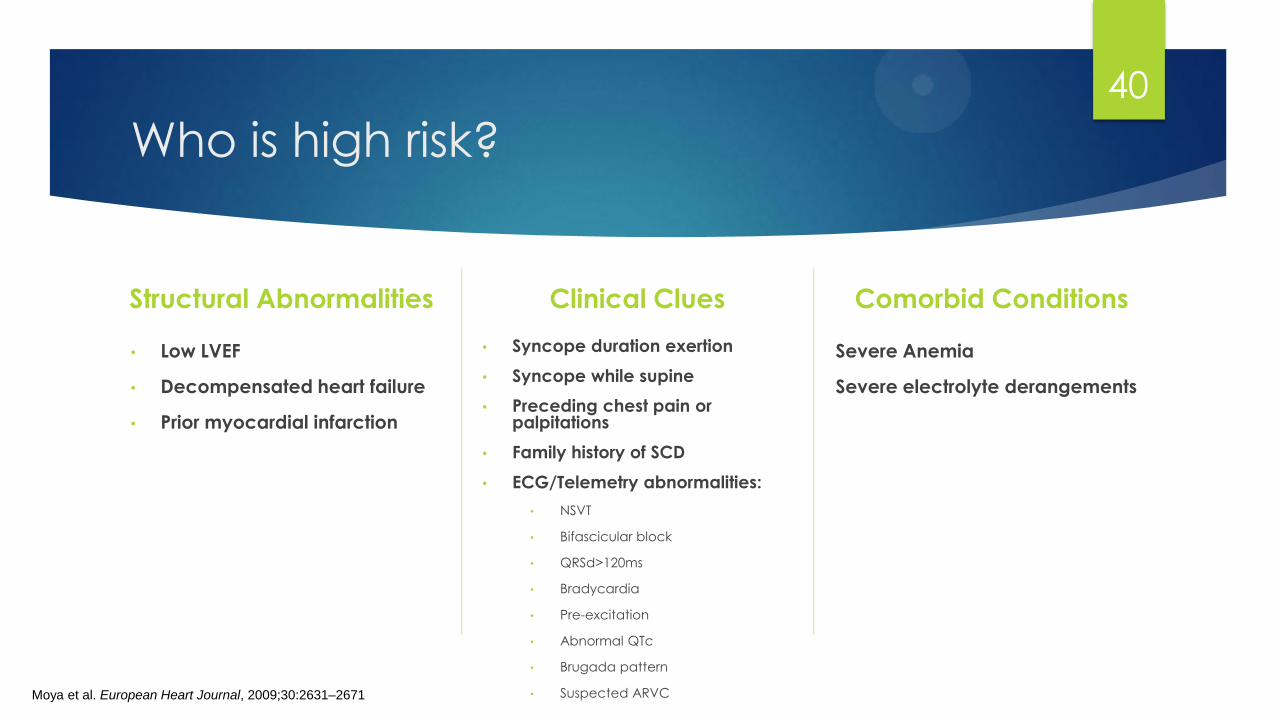
Who is high risk?
Structural Abnormalities
• Low LVEF
• Decompensated heart failure
• Prior myocardial infarction
Clinical Clues
• Syncope duration exertion
• Syncope while supine
• Preceding chest pain or palpitations
• Family history of SCD
• ECG/Telemetry abnormalities:
• NSVT
• Bifascicular block
• QRSd>120ms
• Bradycardia
• Pre-excitation
• Abnormal QTc
• Brugada pattern
• Suspected ARVC
Comorbid Conditions
Severe Anemia
Severe electrolyte derangements
Moya et al. European Heart Journal, 2009;30:2631–2671
40
Testing Performed By The Consultant
Carotid Sinus Massage
Exercise Test
Ambulatory ECG
Holter monitoring
Event recorder
Implantable Loop Recorder
Head-Up Tilt
Electrophysiology Study (EPS)
Brignole M, et al. Europace, 2004;6:467-537.
41
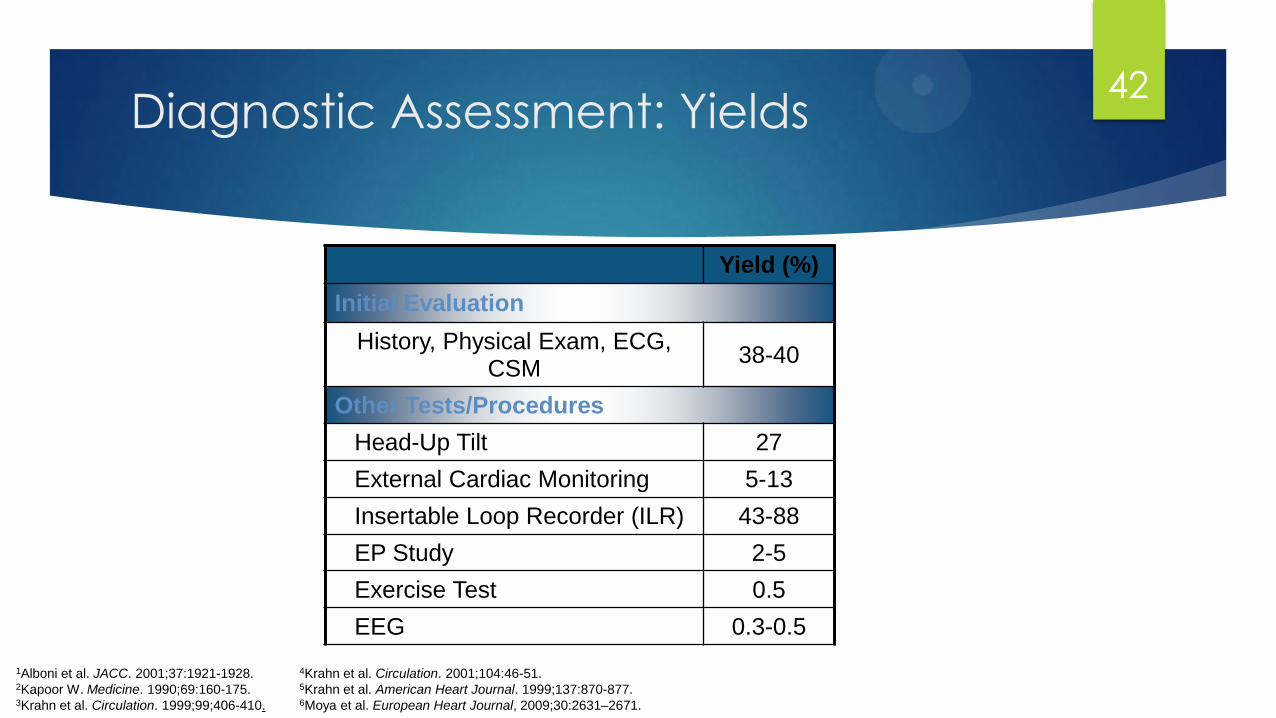
Diagnostic Assessment: Yields
1Alboni et al. JACC. 2001;37:1921-1928. 2Kapoor W. Medicine. 1990;69:160-175. 3Krahn et al. Circulation. 1999;99;406-410.
Yield (%)
Initial Evaluation
History, Physical Exam, ECG, CSM
38-40
Other Tests/Procedures
Head-Up Tilt 27
External Cardiac Monitoring 5-13
Insertable Loop Recorder (ILR) 43-88
EP Study 2-5
Exercise Test 0.5
EEG 0.3-0.5
4Krahn et al. Circulation. 2001;104:46-51. 5Krahn et al. American Heart Journal. 1999;137:870-877. 6Moya et al. European Heart Journal, 2009;30:2631–2671.
42

Carotid Sinus Massage
Indications:
Age >40 with syncope of unknown etiology
after initial evaluation or when CSS is
suspected
Stimulates carotid baroreceptor reflex
(vagally-mediated bradycardia/asystole)
1Kenny RA. Heart. 2000;83:564
43
Carotid Sinus
Method1
Usually performed in conjunction with
tilt (supine and upright)
Massage, 5-10 seconds
Don’t occlude!
Outcome
3 second asystole and/or 50 mmHg fall
in systolic BP with reproduction of
symptoms = Carotid Sinus Syndrome
Absolute contraindications2
Carotid bruit, known significant carotid
arterial disease, previous CVA, MI last 3
months
Complications
Primarily neurological
Less than 0.2%3
Usually transient
1Kenny RA. Heart. 2000;83:564. 2Linzer M. Annnals of Internal Medicine. 1997;126:989. 3Munro N, et al. Journal American Geriatric Society. 1994;42:1248-1251.
44
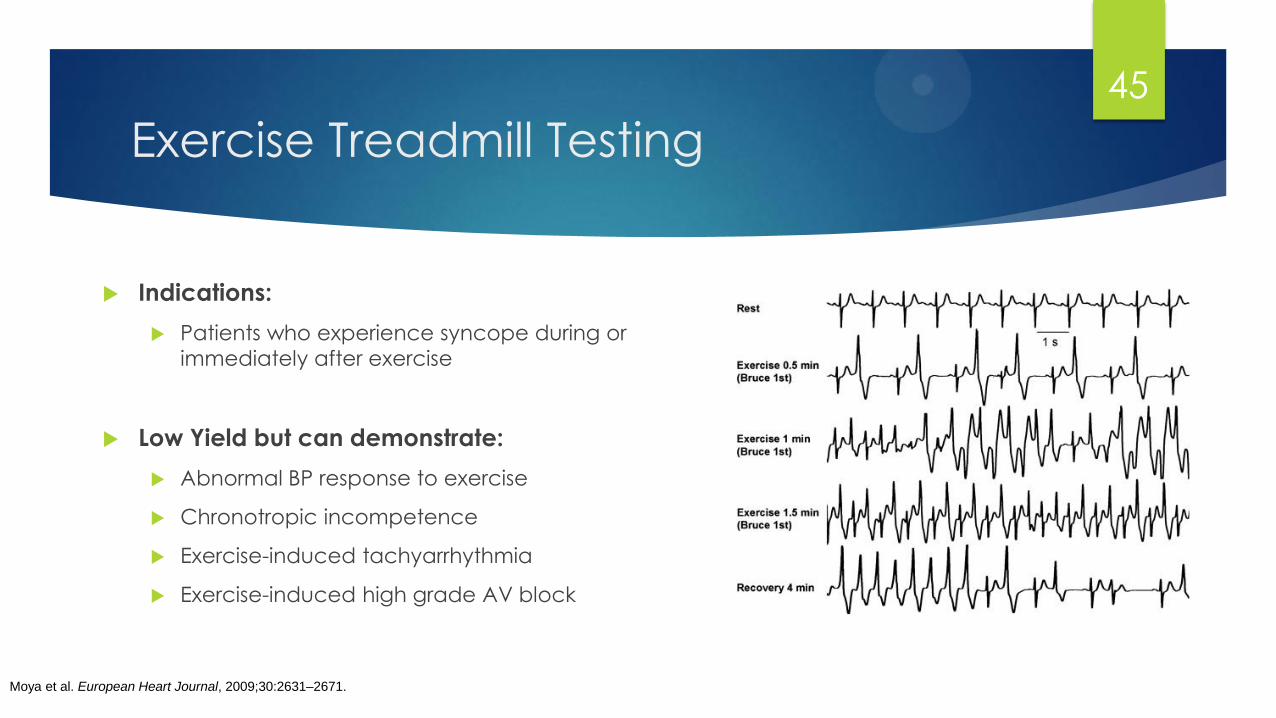
Exercise Treadmill Testing
Indications:
Patients who experience syncope during or
immediately after exercise
Low Yield but can demonstrate:
Abnormal BP response to exercise
Chronotropic incompetence
Exercise-induced tachyarrhythmia
Exercise-induced high grade AV block
Moya et al. European Heart Journal, 2009;30:2631–2671.
45
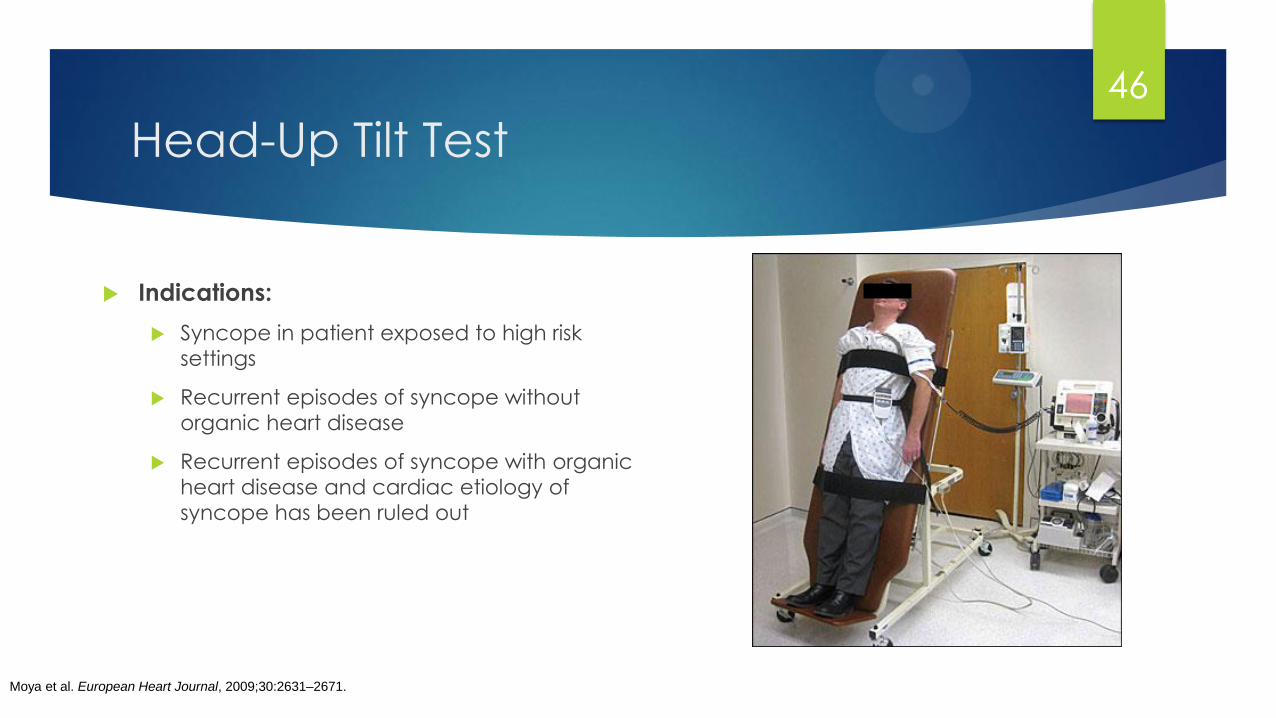
Head-Up Tilt Test
Indications:
Syncope in patient exposed to high risk
settings
Recurrent episodes of syncope without
organic heart disease
Recurrent episodes of syncope with organic
heart disease and cardiac etiology of
syncope has been ruled out
Moya et al. European Heart Journal, 2009;30:2631–2671.
46
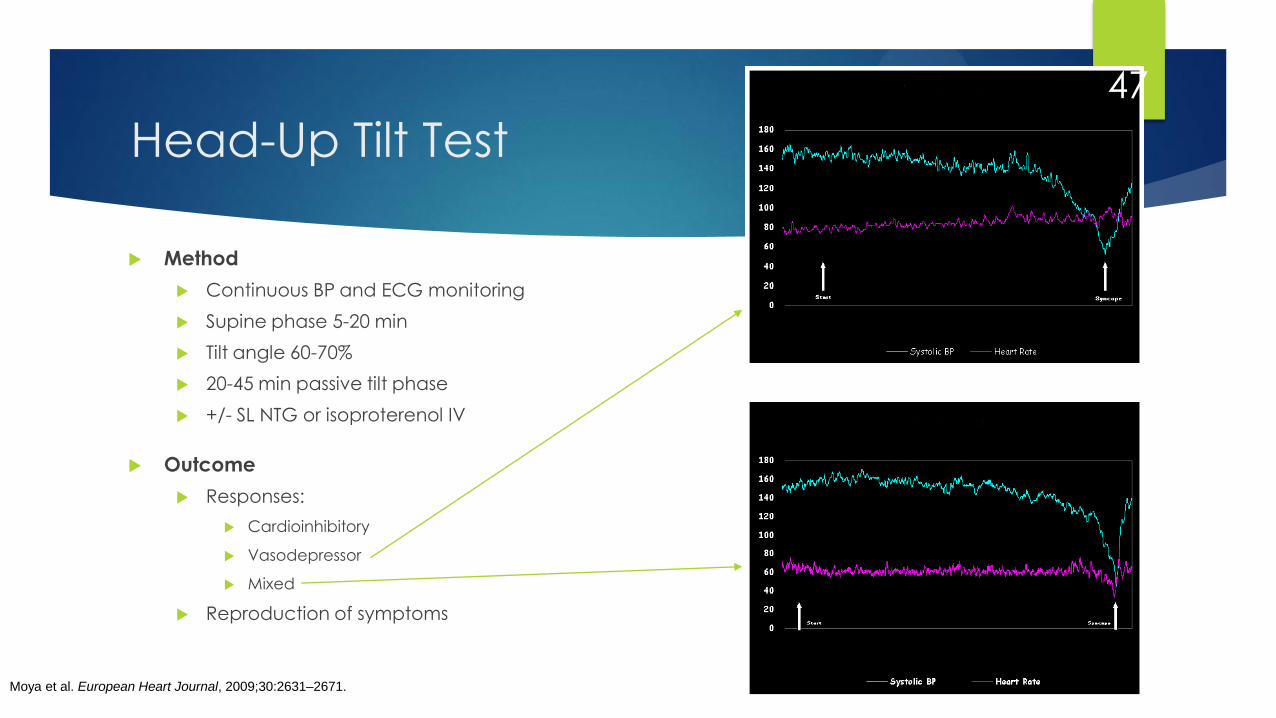
Head-Up Tilt Test
Method
Continuous BP and ECG monitoring
Supine phase 5-20 min
Tilt angle 60-70%
20-45 min passive tilt phase
+/- SL NTG or isoproterenol IV
Outcome
Responses:
Cardioinhibitory
Vasodepressor
Mixed
Reproduction of symptoms
Moya et al. European Heart Journal, 2009;30:2631–2671.
47
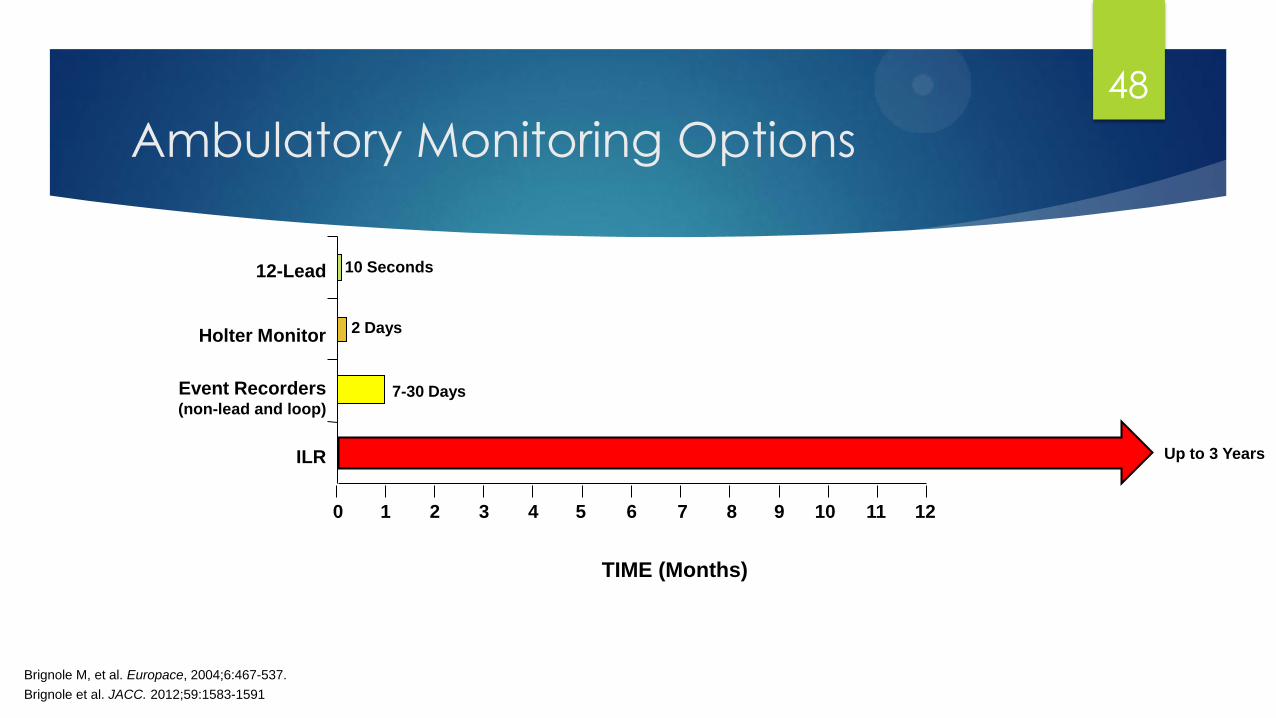
Ambulatory Monitoring Options
ILR
Event Recorders (non-lead and loop)
Holter Monitor
12-Lead
2 Days
7-30 Days
10 Seconds
TIME (Months)
0 1 2 3 4 5 6 7 8 9 10 11 12
Brignole M, et al. Europace, 2004;6:467-537.
Up to 3 Years
Brignole et al. JACC. 2012;59:1583-1591
48
Ambulatory Monitoring
Indications
Patients who have clinical or ECG features suggesting arrhythmic syncope
Type of testing
Inpatient telemetry – high risk patients
Holter monitor – low risk, very frequent symptoms
Event monitor – low risk, expected to have symptoms within 4 weeks
Remote telemetry – emerging technology
ILR
Late implant – high risk patients with negative comprehensive evaluation thus far
Early implant – recurrent syncope, unknown cause, no events during external monitoring
Moya et al. European Heart Journal, 2009;30:2631–2671.
49
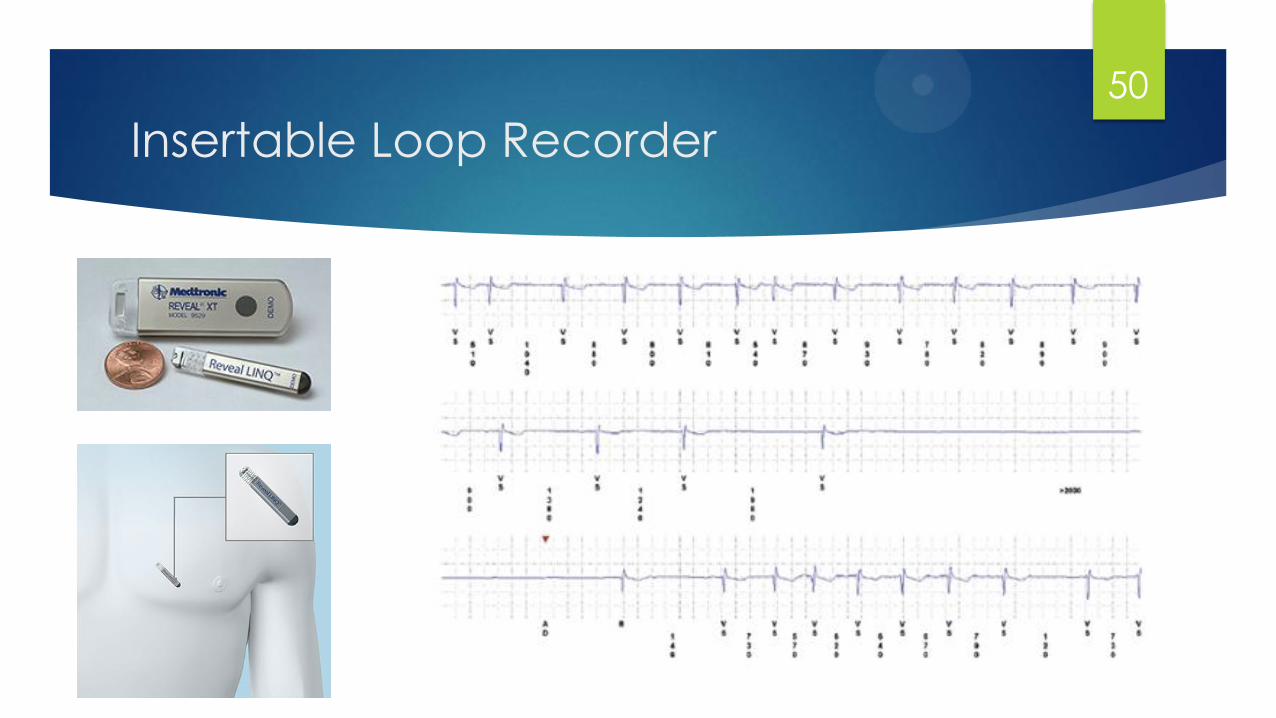
Insertable Loop Recorder
50
Electrophysiological Study (EPS)
Indications for evaluation of syncope:
Ischemic heart disease without standard indication for ICD
Presence of BBB; negative non-invasive testing
Syncope preceded by palpitations; negative non-invasive testing
High risk occupations (every effort to exclude arrhythmic etiology is warranted)
Generally not indicated in patients with normal ECG, normal echo & no
history of palpitations
51
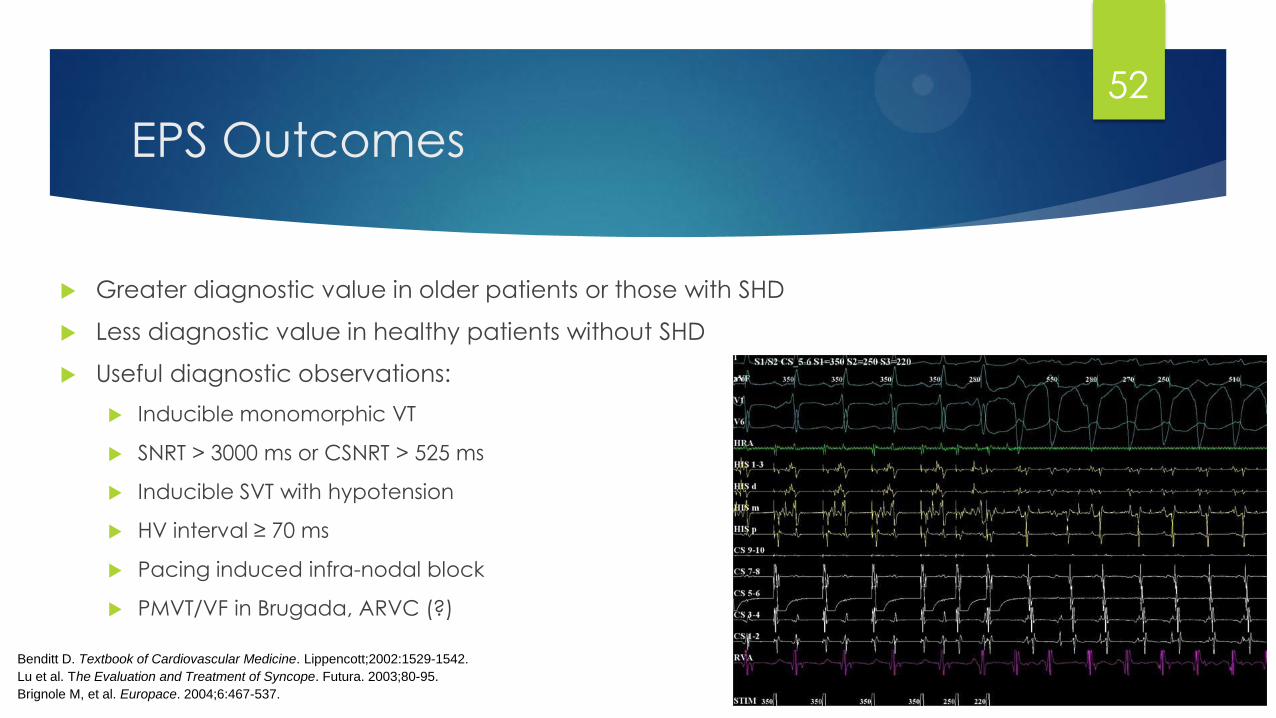
EPS Outcomes
Greater diagnostic value in older patients or those with SHD
Less diagnostic value in healthy patients without SHD
Useful diagnostic observations:
Inducible monomorphic VT
SNRT > 3000 ms or CSNRT > 525 ms
Inducible SVT with hypotension
HV interval ≥ 70 ms
Pacing induced infra-nodal block
PMVT/VF in Brugada, ARVC (?)
Benditt D. Textbook of Cardiovascular Medicine. Lippencott;2002:1529-1542.
Lu et al. The Evaluation and Treatment of Syncope. Futura. 2003;80-95.
Brignole M, et al. Europace. 2004;6:467-537.
52
Diagnostic Limitations of EPS
Difficult to correlate spontaneous events and
laboratory findings
Positive findings1
Without SHD: 6-17%
With SHD: 25-71%
Less effective in assessing bradyarrhythmias
than tachyarrhythmias2
EPS findings must be consistent with clinical history
Beware of false positive
1Linzer M, et al. Annals of Internal Medicine. 1997;127:76-86. 2Lu F, et al. In: Benditt D, et al. The Evaluation and Treatment of Syncope. Futura. 2003;80-95.
53
54
Questions?
(225)610-0993
ISSUE
International Study of Syncope of Uncertain Etiology
Multicenter, international, prospective study
Analyzed the diagnostic contribution of an ILR in
three predefined groups of patients with syncope of
uncertain origin:
1) Isolated syncope: No SHD, Normal ECG1
• Negative tilt
• Positive tilt
2) Patients with heart disease and negative EP test2
3) Patients with bundle branch block and negative EP test3
1Moya A. Circulation. 2001; 104:1261-1267. 2Menozzi C, et al. Circulation. 2002;105:2741-2745. 3Brignole M, et al. Circulation. 2001;104:2045-2050.
56

ISSUE - Patients with Isolated Syncope and Tilt-Positive
Syncope
Moya A. Circulation. 2001;104:1261-1267.
Follow-Up to Recurrent
Spontaneous Episode
111 Patients with Syncope
No SHD, Normal ECG
29: Tilt-Positive 82: Tilt-Negative
“Isolated Syncope”
Tilt Test Followed by
Insertable Loop Recorder
57
Isolated Syncope vs. Tilt-Positive Syncope
Conclusions
Results similar in the two arms, including syncope
recurrence and ECG correlation
Tilt-negative patients had as many bradycardias (18%) as
tilt-positive patients (21%)
Most frequent finding was asystole secondary to progressive
sinus bradycardia, suggesting a neuro-mediated origin
Homogeneous findings from tilt-negative and tilt-positive
infer low sensitivity of tilt-testing
Moya A. Circulation. 2001;104:1261-1267.
58

ISSUE - Patients with Heart Disease and a Negative EPS
Menozzi C, et al. Circulation. 2002;105:2741-2745.
35 Pts with Heart Disease
and Insertable Loop Recorder
Syncope: 6 Pts (17%)
ECG-Documented: 6 Pts (17%)
Pre-Syncope: 13 Pts (37%)
ECG-Documented: 8 Pts (23%)
AV block + asystole: 1
A.Fib + asystole: 1
Sinus arrest: 1
Sinus tachycardia: 1
Rapid A.Fib: 2
Sustained VT: 1
Parox. A.Fib/AT: 1
Post tachycardia pause: 1
No rhythm variations: 4
Sinus tachycardia: 1
59
ISSUE - Patients with Heart Disease and a Negative EP Test
Conclusions
Patients with unexplained syncope, overt heart disease, and negative
EP study had a favorable medium-term outcome
Mechanism of syncope was heterogeneous
Ventricular tachyarrhythmia was unlikely
“ILR-guided strategy seems reasonable, with specific therapy safely
delayed until a definite diagnosis is made.”
Menozzi C, et al. Circulation. 2002;105:2741-2745.
60
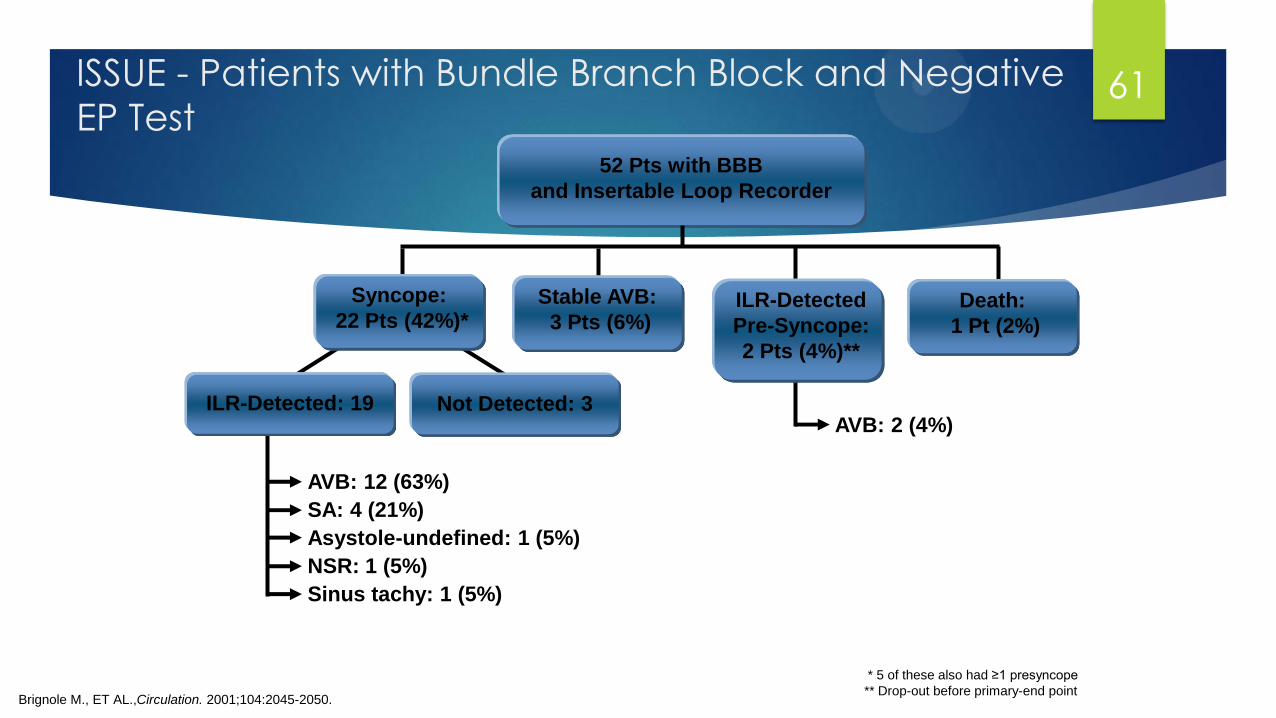
ISSUE - Patients with Bundle Branch Block and Negative
EP Test
Brignole M., ET AL.,Circulation. 2001;104:2045-2050.
* 5 of these also had ≥1 presyncope
** Drop-out before primary-end point
52 Pts with BBB
and Insertable Loop Recorder
Syncope:
22 Pts (42%)*
ILR-Detected: 19
AVB: 12 (63%)
SA: 4 (21%)
Asystole-undefined: 1 (5%)
NSR: 1 (5%)
Sinus tachy: 1 (5%)
Not Detected: 3
Stable AVB:
3 Pts (6%) ILR-Detected
Pre-Syncope:
2 Pts (4%)**
Death:
1 Pt (2%)
AVB: 2 (4%)
61
Patients with Bundle Branch Block and
Negative EP Test
Conclusion:
In patients with BBB and negative EP study, most syncopal
recurrences have a homogeneous mechanism that is characterized by
prolonged asystolic pauses mainly attributable to sudden-onset
paroxysmal AV block
Brignole M. Circulation. 2001;104:2045-2050.
62






















![Syncope AHD[1]](https://img.pdfslide.us/doc/110x75/577d36611a28ab3a6b92ec10/syncope-ahd1.jpg)
