Embed Size (px)
Citation preview

An Approach for Artificial Pancreas to Control the Type-I DiabetesMellitus
Submitted by
Muhammad FarmanRegistration No: DMAT 0 1 143004
SESSION: 2014-2018
Supervisor
Prof. Dr. Muhammad Ozair Ahmad
Department of Mathematics and Statistics
The University of Lahore, Lahore.
Co-Supervisor
Dr. Muhammad Umer Saleem
Department of Mathematics (DS & T)
University of Education, Lahore
DEPARTMENT OF MATHEMATICS AND STATISTICSTHE T.IhIIVERSTTY OF LAHORE,
LAHORE-PAKISTAN2019

An Approach for Artificial Pancreas to Control the Type-IDiabetes Mellitus
This dissertation is submitted to the Department of Mathematics andStatistics, University of Lahore, Lahore, Pakistan, for the partial fulfillment of the
requirements for the award of the degree of
Submitted byMuhammad Farman
Registration No: DMAT 0 1 143004
APProved on )' t? ' c' ('* L-" r \
" --#Sign: . i ,', ;'" . I Sigr' \id 2l: -
Prof. Dr. Muhammad Ozair AhmadInternal Examiner (Thesis Supervisor)Deparhnent of Mathematics & Statistics
Intemal Examiner (Thesis Co-Supervisor)Department of Mathematics
University of Education, Lahore
Dr. Aziz-tr-Rehman (Extemal Examiner)Deparhnent of Mathematics
University of Engineering & Technology,
Lahore
Sign:
Prof. Dr. Muhammad Ozair AhmadHead of Departrnent of Mathematics and StatisticsThe University of Lahore, Lahore
DEPARTMENT OF MATHEMATICS AND STATISTICSTHE UNIVERSITY OF LAHORE,
LAHORE.PAKISTAl\2019
The University of Lahgre
Dr. Muhammadtlmer Saleem Dr. Anjum yrydtz (Extemal Examiner)



Acknowledgments
My highest praise is for Almighty Allah, the most Gracious and most Merciful
who guides me in difficulties all respect to Holy Prophet Muhammad (PBUH)
enlightening a conscience with essence of faith in Allah. With His grace and
guidance I have reached this stage of my academic carrier. With His blessing and
kindness, I plan, visualize and execute my dreams into reality.
I am indebted to all my teachers for the great cooperations through out the aca-
demic program. It is a matter of great pleasure to express our sincere regards to my
honorable supervisor Prof. Dr muhammad Ozair Ahmad and Dr Muhammad Umer
Saleem for affectionate supervision and masterly advice. His able guidance, valuable
suggestions and continuous encouragement helped me at every stage in completion
of my work. I am very thankful to both of you for this love, kindness and cooperation.
I wish to express my thanks to Head of Department DR. Muhammad Ozair
Ahmad, PhD coordinator Dr Maqbool Ahmad Chadury , Dr Deba Afzal and other
faculty members of department of mathematics and Statistics who were always
there to facilitate me in my research work and taught me during the course of my
study. I also very thankful to Dr Nouman Raza and Dr Muhammad Rizwan for
their piece of advice during research work. Thanks to all authors who I mentioned
in bibliography, their work enable me to step forward in the field of mathematical
biology,
I offer my gratitude to my dear parents, father in law, wife, my brothers and
sisters , whose prayers and good wishes made it possible for me to carry out this
work progressively. The immeasurable sacrifices of my parents and family led to
what I am today. Bundle of thanks to my family members specially Sara Farman
, and the little stars Huda Rameen , Noriaz Haider, Ammara, Khansa who helped
me morally and emotionally to accomplish my task. I Love you all.
I am very grateful to all my friends specially Aqeel Ahmad, Ehsan-ul Haq,
Muhammad Abdullah, Farhan and my Ph.D fellows who always encouraged and
helped me during my completion of all work.
Muhammad Farman
UOL, Pakistan, 2018

List of Publications Related Thesis
1. Saleem M.U., Muhammad Farman, Meraj M.A., Stability Analysis of
Sorensen’s Model for controllability and observability, B. Life and Environ-
mental Sciences, 54 (2): 133145, (2017) .
2. M.U Saleem, Muhammad Farman, M.O. Ahmad, Rizwan M., A Control of
Artificial Human Pancreas, Chines journal of Physics.55(6)2273-2282,(2017).
3. Muhammad Farman, M.U Saleem, M.O. Ahmad, An Approach for Artificial
Pancreas to Control the Type-1 Diabetes Mellitus, Journal of Applied Envi-
ronmental and Biological Sciences, 93-102, (2017).
4. Muhammad Farman, Muhammad Umer Saleem, M. O Ahmad, Aqeel Ahmad,
Stability Analysis and Control of Glucose Insulin Glucagon System in human,
Chines Journal of Physics, 56, 1362-1369, (2018).
5. Muhammad Farman, Muhammad Umer Saleem, Control of Augmented mini-
mal model for glucose insulin pump, Current Research in Diabetes and Obesity
Journal, DOI: 10.19080/CRDOJ.2018.08.555742 (2018).
6. M.U Saleem, Muhammad Farman, Rizwan M., M.O. Ahmad, Aqeel ahmad,
Controllability and Observability of Glucose Insulin Glucagon systems in Hu-
man, Chines journal of Physics, ,56(5), 1909-1916, (2018).
7. M.U Saleem, Muhammad Farman, Aqeel Ahmad, M. Naeem, M. O Ahmad,
Stability Analysis and Control of Fractional Order Diabetes Mellitus Model
for Artificial Pancreas, Punjab University mathematics journal, 51(4),97-113,
(2019)..

List of others Publications
1. Saleem M.U., Muhammad Farman, Meraj M.A., A linear control of Hovorka
Model, Sci. Int. (Lahore),28(1),15-18, (2016).
2. Aqeel, Muhammad Farman, M. O Ahmad, N. Raza, Abdullah, Dynamical
behavior of SIR epidemic model with non-integer time fractional derivatives: A
mathematical analysis, International journal of Advance and Applied sciences,
123-129 (2018).
3. Aqeel, Muhammad Farman, Faisal yaseen, M. O Ahmad, Dynamical trans-
mission and effect of smoking in society, International journal of Advance and
Applied sciences, 5(2),71-75, (2018).
4. Farah Ashraf, Aqeel Ahmad, Muhammad Umer Saleem, Muhammad Farman,
M.O. Ahmad, Dynamical behavior of HIV immunology model with non-integer
time fractional derivatives, International journal of Advance and Applied sci-
ences, 5(3), 39-45, (2018).
5. Muhammad Farman, Muhammad Umer Saleem, Aqeel Ahmad, M. O Ahmad,
Analysis and Numerical Solution of SEIR Epidemic Model of Measles with Non-
integer Time Fractional Derivatives by using Laplace Adomian Decomposition
Method, Ain Shams Engineering Journal, 9(4), 3391-3397 ( 2018).
6. Saleem M.U., Muhammad Farman, Aqeel Ahmad, Meraj M.A, Mathematical
model based assessment of the cancer control by Chemo-Immunotherapy, Pure
and Applied Biology vol 7, 678-683, (2018).
7. Abdullah, Aqeel, N. Raza, Muhammad Farman, M. O Ahmad, Approximate
solution and analysis of smoking epidemic model with Caputo fractional deriva-
tives, Int. J. Appl. Comput. Math 4:112 (2018).
8. Muhammad Farman, Zafer, Aqeel Ahmad, Ali Raza, Ehsan ul Haq, Numeri-
cal Simulation and Analysis of Acute and Chronic Hepatitis B, International
journal of Analysis and Application, 16(6), 842-855, (2018).
9. Aqeel Ahmad, Nouman, Muhammad Farman, M. O Ahmad, A. Hafeez, Ali,
Dynamical Behavior of Fractional Order Epidemic Model, International journal
of Analysis and Application, (accepted).

ABSTRACT
Currently diabetes mellitus is worldwide issue and challenges for diabetes com-
munity for healthy life. An effort is made to develop the idea of getting a fully
automated artificial pancreas. The artificial pancreas is a developing technology
to help patients with diabetes of type 1 diabetes mellitus (T1DM) to control au-
tomatically their blood glucose level by making available the alternative endocrine
functionality of a healthy pancreas. The concept of controllability and observability
for the linearized control system of human glucose insulin system is used so that we
can have a feedback control for artificial pancreas. For the purpose of automatic
artificial pancreas in the glucose regulatory system, we consider the Glucose Insulin
(GI) Systems and Glucose Insulin Glucagon (GIG) systems. These models includes
Augmented Meal Model (AMM), Reduced Meal Model (RMM), fractional order glu-
cose insulin system, a composite model of Glucagon-Glucose Dynamics Model and
Sorenson model being comprehensive model for Type-1 Diabetes Mellitus (T1DM).
These models can be used to simulate a glucose insulin system for the treatment of
T1DM. The Lyapunov Equation is used to check the stability analysis of the model.
A fractional-order time derivatives model is presented for comprehensive glucose
insulin regulatory model. A fractional-order state observer is designed for approx-
imating the structure of a blood glucose-insulin with glucose rate disorder to show
the complete dynamics of the glucose-insulin system with the fractional-order at
α ∈ (0 < a < 1]. The developed method provides the observer estimation algo-
rithm for a glucose-insulin system with unknown time-varying glucose rate distur-
bance. Numerical simulations are carried out to demonstrate our proposed results
and show the nonlinear fractional-order glucose-insulin systems are at least stable
as their integer-order counterpart in the existence of exogenous glucose infusion or
meal disturbance.
Controllability and observability of the linearized model are calculated under two
different cases,for case 1 insulin is taken as an input and case 2, insulin and glucagon
are taken as an input for the system. This played an important role in the devel-
opment of fully automatic artificial pancreas by stabilizing the control loop system
for the glucose-insulin glucagon pump. Proportional Integral Derivative (PID) con-
troller is designed for an artificial pancreas by using the transfer function. According
to the desire value, the algorithm of an artificial pancreas measures the glucose level
in the blood of a patient by using glucose sensor that sends a signal to an insulin

glucagon pump to adjust the basal insulin. A closed-loop system is tested in simulink
environment and simulation results show the performance of the designed controller.
We convert the Sorenson model to Sorenson model type 1 diabetes mellitus because
this is the most comprehensive model in the Glucose Insulin Glucagon dynamics for
human. This may play an important role in the development of fully automatic arti-
ficial pancreas and stabilize the control loop system for the Glucose Insulin Glucagon
pump. It would be helpful for type 1 diabetic patients to control their diseases.
The thesis is also review the state of art in hypoglycemia prevention and detection
technique in the closed-loop artificial pancreas. Hypoglycemia is the major adverse
effect of insulin therapy and therefore minimizing the risk of hypoglycemia, by apply-
ing different control and detection techniques is often considered in the development
of artificial pancreas.

Contents
Abstract 1
Table of Contents 3
List of Tables 6
List of Figures 7
1 Introduction 9
1.1 Physiology of Glucose Insulin System . . . . . . . . . . . . . . . . . . 11
1.1.1 Pancreas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.1.2 Insulin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.1.3 Glucose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1.1.4 Glucagon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1.2 Diabetes Mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1.2.1 Type 1 Diabetes Mellitus . . . . . . . . . . . . . . . . . . . . . 14
1.2.2 Type 2 Diabetes Mellitus . . . . . . . . . . . . . . . . . . . . . 14
1.3 Treatment of Type 1 Diabetes Mellitus . . . . . . . . . . . . . . . . . 14
1.3.1 Insulin Administration . . . . . . . . . . . . . . . . . . . . . . 15
1.3.2 Blood Glucose Measurements . . . . . . . . . . . . . . . . . . 15
1.4 Diabetes Treatment Methods . . . . . . . . . . . . . . . . . . . . . . 16
1.4.1 Standard Therapy . . . . . . . . . . . . . . . . . . . . . . . . 16
1.4.2 Basal Insulin . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.4.3 Bolus Insulin . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.4.4 Introduction to Systems and Control . . . . . . . . . . . . . . 17
1.4.5 Open-Loop Control . . . . . . . . . . . . . . . . . . . . . . . . 17
1.4.6 Closed-Loop Control . . . . . . . . . . . . . . . . . . . . . . . 18
1.5 Motivation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3

1.6 Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1.7 Organization of Thesis . . . . . . . . . . . . . . . . . . . . . . . . . . 20
2 Controllability and Observability 23
2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2.1.1 Linear Control System . . . . . . . . . . . . . . . . . . . . . . 23
2.1.2 Linear Singular Control System . . . . . . . . . . . . . . . . . 25
2.2 Controllability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
2.2.1 Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
2.2.2 Linear, time-invariant control system . . . . . . . . . . . . . . 28
2.3 Observability (Reconstructibility) . . . . . . . . . . . . . . . . . . . . 29
2.3.1 Observability of Linear, time-invariant control system . . . . . 31
3 Glucose Insulin System 34
3.1 Augmented Minimal Model . . . . . . . . . . . . . . . . . . . . . . . 34
3.1.1 Linear Control System: . . . . . . . . . . . . . . . . . . . . . . 36
3.2 Reduced Meal Model . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
3.3 Linear Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
3.3.1 Controllability and Observability . . . . . . . . . . . . . . . . 42
3.4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
4 Fractional Order Glucose Insulin Model 44
4.1 Fractional Order Glucose Insulin Model . . . . . . . . . . . . . . . . . 44
4.1.1 Stability Analysis and Equilibria . . . . . . . . . . . . . . . . 45
4.2 Laplace Adomian Decomposition Method . . . . . . . . . . . . . . . . 47
4.3 Case I for Normal Person . . . . . . . . . . . . . . . . . . . . . . . . . 48
4.4 Case II for Type 1 Diabetes . . . . . . . . . . . . . . . . . . . . . . . 50
4.5 Numerical Results and Discussion . . . . . . . . . . . . . . . . . . . . 51
4.6 Input and Output Stability . . . . . . . . . . . . . . . . . . . . . . . 55
4.6.1 Controllability and Observability . . . . . . . . . . . . . . . . 56
4.7 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
5 Stability Analysis and Control of GIG System 58
5.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
5.2 Mathematical Model . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
5.3 Stability Theorem: . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
5.4 Linear Control System . . . . . . . . . . . . . . . . . . . . . . . . . . 62

5.4.1 Controllability and Observability . . . . . . . . . . . . . . . . 62
5.5 Controller Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
5.6 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
6 Sorenson Model for Type 1 Diabetes Mellitus 71
6.1 Sorensen’s Model For Type 1 Diabetes . . . . . . . . . . . . . . . . . 71
6.1.1 Description of Variables . . . . . . . . . . . . . . . . . . . . . 74
6.1.2 First Subscript: Physiological Compartment . . . . . . . . . . 75
6.1.3 Second Subscript: Physiological Compartment . . . . . . . . . 75
6.1.4 Metabolic source and sink . . . . . . . . . . . . . . . . . . . . 76
6.2 Modified Form of Model in Type 1 Diabetes Mellitus . . . . . . . . . 79
6.2.1 Linearised Model . . . . . . . . . . . . . . . . . . . . . . . . . 81
6.2.2 Stability Analysis . . . . . . . . . . . . . . . . . . . . . . . . . 82
6.3 Results and Discussions . . . . . . . . . . . . . . . . . . . . . . . . . 83
6.3.1 Case I: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
6.3.2 Case II: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
6.4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
7 Control of Composite Model 86
7.1 Material and Method . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
7.1.1 Composite Model Glucagon-Glucose Dynamics . . . . . . . . . 87
7.2 Extended Form of Composite Model . . . . . . . . . . . . . . . . . . 89
7.2.1 Gastrointestinal Absorption Model . . . . . . . . . . . . . . . 90
7.2.2 Subcutaneous Insulin Absorption Model . . . . . . . . . . . . 90
7.2.3 Subcutaneous Glucagon Absorption Model . . . . . . . . . . . 91
7.2.4 Linearized System . . . . . . . . . . . . . . . . . . . . . . . . 94
7.3 Stability Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
7.4 Linear Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
7.4.1 Results and Discussion . . . . . . . . . . . . . . . . . . . . . . 95
7.5 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
8 Conclusion and Future Work 99
Bibliography 102

List of Tables
3.1 Table of Parameter’s used in the Augmented Minimal Model . . . . . 35
3.2 Table of Parameters used in the Reduced Meal Model . . . . . . . . . 39
4.1 Table of Parameter’s used in Sandhya Model . . . . . . . . . . . . . . 45
5.1 Table of parameter’s value used in the model . . . . . . . . . . . . . . 60
6.1 Description of variables . . . . . . . . . . . . . . . . . . . . . . . . . . 74
6.2 Physiological Compartment . . . . . . . . . . . . . . . . . . . . . . . 75
6.3 Physiological Compartment . . . . . . . . . . . . . . . . . . . . . . . 75
6.4 Table of parameter’s and constant value of the model . . . . . . . . . 76
7.1 Table of parameters and constant value of the model . . . . . . . . . 92
6

List of Figures
1.1 Physiology of Diabetes Mellitus . . . . . . . . . . . . . . . . . . . . . 11
1.2 Illustration of open-loop control for T1DM treatment. . . . . . . . . . 18
1.3 Illustration of closed-loop control for T1DM treatment . . . . . . . . 18
2.1 Idealized diagram of a control system . . . . . . . . . . . . . . . . . . 24
2.2 control system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
3.1 Controllability and observability Graph . . . . . . . . . . . . . . . . . 37
3.2 Controllability and observability Graph . . . . . . . . . . . . . . . . . 38
4.1 Numerical solution of Glucose level of normal person . . . . . . . . . 52
4.2 Numerical solution of Glucose level of type 1 diabetes . . . . . . . . . 53
4.3 Behavior of insulin in normal person . . . . . . . . . . . . . . . . . . 53
4.4 Behavior of insulin in type 1 diabetes . . . . . . . . . . . . . . . . . . 54
4.5 Numerical solution of insulin concentration in plasma of normal person 54
4.6 Numerical solution of insulin concentration in plasma of type 1 diabetes 55
5.1 Controllable and observable state of model, when insulin is an input
at initial condition (80,21,900, 300,0.16) . . . . . . . . . . . . . . . . 64
5.2 Controllable and observable steady state of model, when insulin is an
input at initial condition (120,10,5, 3,0.1) . . . . . . . . . . . . . . . . 64
5.3 Controllable and observable state of model, when insulin and glucagon
are an input at initial condition (120,21,900, 300,0) . . . . . . . . . . 66
5.4 Controllable and observable state of model, when insulin and glucagon
are an input at initial condition (80,0,900, 300,0.16) . . . . . . . . . . 66
5.5 Simulink to measure Glucose, insulin and glucagon with effect of β-
cell, α-cell mass . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
5.6 Pole zero diagram of transfer function G(s) . . . . . . . . . . . . . . . 69
5.7 Frequency response transfer function G(s) . . . . . . . . . . . . . . . 69
7

6.1 Schematic representation of the Glucose Model . . . . . . . . . . . . . 72
6.2 Schematic representation of the Insulin Model . . . . . . . . . . . . . 72
6.3 Schematic representation of the Glucagon Model . . . . . . . . . . . . 73
7.1 The glucagon extended Minimal model . . . . . . . . . . . . . . . . . 87

Chapter 1
Introduction
Go down deep enough into anything and you will
find mathematics.(D Schlicter)
Mathematics is the supreme judge; from its decisions
there is no appeal.(Tobias Dantzig)
God does not care about our mathematical difficulties;
He integrates empirically.(Albert Einstein)
Mathematics has always advantages from its participation with developing sci-
ences. Each consecutive interface invigorates and improves the field. Biomedical
science is obviously the premier science of the expected future. For the health of
their subjects mathematicians have to be concerned with biology. Mathematical
biology is a fast-growing, well-known, albeit not evidently defined, subject and for
my mind, the most thrilling modern application of Mathematics. The rising use of
Mathematics in biology is predictable as biology becomes more quantitative. The
best models show how a method works and then forecast what may follow. If these
are not previously clear to the biologists and the predictions turn out to be right,
then you will have the biologist’s attention. Authentic interdisciplinary research and
the exploit of models can produce thrilling results, many of which are described [1]
The group of metabolic disorders which is caused by high blood sugar level that is
due to defects in insulin secretion, action or both. Normally, insulin controles glucose
and blood sugar level is lowered by insulin. Insulin is released from the pancreas,
when glucose level elevates from the normal level. There is no cure of diabetes but it
can be manageable. After cardiovascular and cancer, diabetes is the third fatal dis-
ease. In diabetes, insulin is not properly produced or not properly done its function.
A lack of insulin secretion or lack in its function causes impaired carbohydrate, fat
9

CHAPTER 1. INTRODUCTION 10
and glucose known as diabetes mellitus. Diabetes mellitus has two types. Insulin
dependent diabetes mellitus (IDDM) is commonly known as type 1 diabetes melli-
tus, in this deficiency of insulin secretion is present. Noninsulin dependent diabetes
mellitus (NIDDM) is commonly known as type 2 diabetes mellitus, in this insulin
is properly produced but not properly work. Type 1 diabetes is caused by impair
insulin in beta cells of pancreas [2, 3]. This insufficient level of insulin is unable
to regulate the blood glucose level to normalize the body’s hormonal system: when
someone intakes food the blood glucose level rises even more. This type of diabetes
appears with the symptoms of urination, tiredness, thirst, hunger and weight loss.
The treatment of this type is done by injecting insulin into the body, exercising and
by taking healthy food. Patients suffering from type 1 diabetes are totally dependent
on insulin injections, and, if not treated on the initial stage patients will die, because
the body cannot handle high level of glucose by itself. Type 2 diabetes is not as
common as type 1 diabetes. Patients of this type are known as insulin resistant.
Symptoms of this type appear to be same as type 1 diabetes. With the passage of
time, in patients suffering from this type of diabetes cells start to decrease and the
patients are treated like type 1 diabetes by using insulin injections. It is a condition
of diabetic patients when the blood glucose level rises above 270mg/dL and it can be
increased by eating a heavy meal or having a very low amount of insulin in the blood
to regulate the system. This serious condition is very dangerous for the patient’s
survival. A diabetic patient with a very low amount of glucose in their blood (up
to 60 mg/dL or below) causes a condition called hypoglycemia. It is caused when
the patient taking insulin treatment skips their proper meal or has laborious work
or heavy exercise and it is also very dangerous for the patients [4, 5].
In the 1970’s, the first experiment with an artificial pancreas (AP) was made with
a large device with beneficial limitations. Over the last decade, several clinical studies
were made. Insulin pumps have been used to administrate subcutaneous (SC) insulin
and subcutaneous continuous glucose monitoring (CGM) with enzymatic technology.
An artificial pancreas in glucose measurement and insulin infusion occurring in the
peritoneal cavity [6]. The artificial pancreas (AP) or automated control system has
been developed by researchers during the last decades [7]. Continuous insulin dose is
allowed by a continuous subcutaneous insulin infusion systems (CSII). The missing
feedback of glucose sensing has a fundamental drawback for closed loop control. The
idea of closed loop control is practically achieved by the development of continu-
ous glucose monitoring (CGM). Many plans were made with the available feedback
among others, proportional integral design control [8], adaptive control and fuzzy

CHAPTER 1. INTRODUCTION 11
logic control. The model predictive control is the most widely used control approach,
because of its ability to elegantly handle a broad range of scheme constraints. It is
still challenging to overcome the problems of insulin regulation in artificial pancreas
research. The main goal of an artificial pancreas system is the prevention of and
safe recovery from hypoglycemia episodes [9], Insulin-glucose dynamics of healthy
subjects as well T1DM and T2DM, with appropriate adjustment in its parameters
for glycaemia control [3, 10].
1.1 Physiology of Glucose Insulin System
This section presents the elements involved in the glucose regulation system in dia-
betes. First, the mechanism of glucose regulation in healthy person is summarized
then difference between healthy person and diabetic person explained in order to
indicate impermanence of required control scheme. Blood sugar level is balanced by
insulin and glucagon in the human body. Insulin and glucagon is known as pancre-
atic endocrine hormones because they are secreted by pancreas. The relationship of
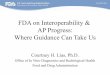
insulin and glucagon is shown in the below figure. Diabetes, hypoglycemia and other
sugar problems are due to imbalanced pancreatic hormones.
Figure 1.1: Physiology of Diabetes Mellitus

CHAPTER 1. INTRODUCTION 12
Insulin and glucagon are hormones secreted by islet cells within the pancreas.
They are both secreted in response to blood sugar levels, but in opposite fashion.
Insulin is normally secreted by the beta cells (a type of islet cell) of the pancreas.
The stimulus for insulin secretion is a high blood glucose. Although there is always
a low level of insulin secreted by the pancreas, the amount secreted into the blood
increases as the blood glucose rises. Similarly, as blood glucose falls, the amount of
insulin secreted by the pancreatic islets goes down. As shown in figure 1.1, insulin
has an effect on a number of cells, including muscle, red blood cells, and fat cells. In
response to insulin, these cells absorb glucose out of the blood, having the net effect
of lowering the high blood glucose levels into the normal range. Glucagon is secreted
by the alpha cells of the pancreatic islets in the same manner as insulin but in the
opposite direction. If blood glucose is high, then no glucagon is secreted. When
blood glucose goes low, (such as between meals, and during exercise) more glucagon
is secreted. Like insulin, glucagon has an effect on many cells of the body, but most
notably the liver [11] .
1.1.1 Pancreas
The pancreas is present near the stomach, help in absorption of the food by making
different enzymes which work on large particles of the food and break it into smaller
particles. The main enzymes are lipase, amylase and trypsin. These enzymes are
made into small glands within pancreas. These enzymes reach into main pancreatic
tube after traveling through large tubes. Pancreatic tube connects gland and bowel.
Thus food from the stomach and enzymes from the pancreas meet with each other
through pancreatic tube. Stomach juices activate pancreatic enzymes. Gastric juice
helps lipase in fat digestion.
1.1.2 Insulin
In 1922, first time insulin separated from pancreas by Banting and Beast. Insulin
is related to blood sugar. Insulin effects carbohydrate mechanism. Beta cells of
pancreas made hormone insulin that helps glucose to enter in cells and help body to
use glucose. Insulin has two types of function. One is normal function and other is
impaired function. Normal function of insulin helps in clearing of glucose. Glycogen
is made by glucose and store in liver and muscle cells with the help of insulin. But
in impaired function blood stream is not cleared from glucose and glycogen is not
formed by glucose [2].

CHAPTER 1. INTRODUCTION 13
1.1.3 Glucose
Energy is provided by glucose (sugar) to the whole body including brain cells. Com-
mon sources of glucose is fruit, bread, pasta and cereals. Food is converted into
glucose in stomach then glucose enters into bloodstream. The value of glucose of
fasting glucose level is 100 mm per deciliter. The value of random glucose level is
140 mm per deciliter. Increase in normal level of glucose is regulated by insulin.
Decrease in normal level of glucose is regulated by glucagon [12].
1.1.4 Glucagon
Glycogen is a form of stored carbohydrate which is released from the liver by the
hormone named glucagon and so the blood glucose rises in the body. The glucagon
called the life saver as it control the blood sugar level of the blood. The function
of glycogen is to produce glucose in the blood. The main producer is comprise on
pancreas, liver and kidney. The glycogen hormone generated by pancreas secrete
glycogen that is accumulated in the form of glucose in liver. When the glucagon
receptors of liver cells binds with glucagon they change glucagon to glucose molecule
and then liver allow them to enter in the blood stream. When the concentration
of the glucose decrease into the body, glucagon encourage the liver and kidney to
synthesize more glucose in the blood to maintain the glucose level in it [12].
1.2 Diabetes Mellitus
Diabetes mellitus is a Greek word which means the excess of sugar. Diabetes mean
run through and mellitus mean honey. Mostly it can be diagnosed from the blood test
or urine test as the urine of patient become sweet, but sometime it gets difficult to
diagnose. Where diagnostic complexity exists, the accurate diagnosis can be created
with an oral glucose tolerance test (OGTT) using a 75 g anhydrous glucose load
melted in water a 2 hour value ≥ 200mg/dl instituted the analysis of diabetes. A
positive test utilizing one or other of the three method should be utilized [14].
Main diabetes is of two types
1. Type 1 Diabetes Mellitus(insulin dependent)
2. Type 2 Diabetes Mellitus(insulin independent)
Approximately 10% patient of type I. In type I hyperglycemia is at low level of
insulin and type II it is the resistance of insulin. In both cases the food stuff alters

CHAPTER 1. INTRODUCTION 14
most of the cells except brain stop using glucose and the glucose level increases in
the body and cells use fats and protein instead of glucose.
1.2.1 Type 1 Diabetes Mellitus
It is autoimmune disease in which the immune system attacks the pancreas and
destroys its cells thus pancreas stops producing insulin or its production decreases.
In T1DM, the immune system attacks the insulin-producing beta (β) cells in the
pancreas and obliterates them. The pancreas then creates little or no insulin. Ev-
erybody who is a patient of type, I need to take insulin regular basis. Scientist is
stir helpless to find the real cause of the body’s immune system to attack the beta
cells (β). They believe that this may be because of specific virus or genetic system.
The destruction of beta cells starts very earlier before the symptoms type 1 diabetes
start. This kind of diabetes mostly attack in old age. The causes of type 1 diabetes
have inherent, obesity , previous history of gestational diabetes, physical inactivity
and eating [2, 13].
1.2.2 Type 2 Diabetes Mellitus
It is common form of diabetes in which the production of insulin is normal but the role
is not effective. As body is not able to utilize the insulin due to unknown reasons.
After many years, the production of insulin in the body decreases, and person is
effected by the diabetes of T1DM and the some symptoms start appearing in the
body. It is seen that the diabetes II is caused by the genetic disorder, still the exact
reason is not known. Concordance rate in identical twins in more than non-identical
twins and it is noticed that those who have no diabetic history in their family are
much secure of this disease. The development of symptoms of T2DM are fatigue,
nausea, unusual thirst, weight loss, blurred or weak vision, frequent infection. Some
time its symptoms are not mark able even in patient [13]
1.3 Treatment of Type 1 Diabetes Mellitus
Artificial pancreas is a innovation to preserve the typical blood glucose level in dia-
betes with a substitute endocrine work to pancreas. The task is lacking to oversee
physically the blood glucose level with alone that is why the current treatment of
affront substitution (Artificial Pancreas) is appreciated for its life sparing capability.

CHAPTER 1. INTRODUCTION 15
This treatment can offer assistance in the hyperglycaemia state by catapulting more
affront by the affront pump but in case of hypoglycaemia state this treatment will
not work. Hypoglycaemia leads to neuroglycopenia and impacts can run from gentle
dysphoria to more serious issues such as seizures, obviousness, harmful for brain cells
and death.
1.3.1 Insulin Administration
Affront can be managed by several implies. In spite of the fact that syringes have
been utilized for a long time for injecting insulin boluses (single doses), they are
broadly supplanted by affront pens. For the final decades, the utilize of affront
pumps has ended up more and more widespread. These gadgets permit nearly
persistent affront implantation by giving boluses up to each miniature. Affront may
be managed (i) subcutaneously, i.e. underneath the skin, (ii) intraperitoneally,i.e.
into the membrane of the stomach depression, or (iii) intravenously, i.e directly into
the veins. The SC course is the standard for commercial affront pumps because of
the moo hazard of contaminations, but has the downside of relatively slow affront
take-up times. Since quick affront activity decreases the amplitude postprandial BG
trips (as will be shown later), speedier IP conveyance is being inquired about and
appears promising out comes, but with the complications [15]. (iv) mixture is the
speediest as it is to closest.
1.3.2 Blood Glucose Measurements
Exact blood glucose measurements are key for fitting treatment and shirking of
hypoglycemia. Two fundamental strategies are commonly being utilized: Self
Checking of Blood Glucose (SMBG) and Nonstop Glucose Observing. SMBG
comprises in measuring the glucose concentration in a little drop of blood gotten
by pricking the finger with a lancet. This strategy is by distant the most common
since of its relatively great precision at sensible fetched. The greatest disadvantage
of this method is that for each estimation, the persistent needs to extricate a blood
drop - a excruciating method. As come about most patients do not take blood
glucose estimations exceptionally habitually. Persistent Glucose Observing (CGM)
devices are an elective that gives nearly nonstop BG concentrations with less finger
pricks, at the cost of decreased precision and reliability. Also, these gadgets are

CHAPTER 1. INTRODUCTION 16
generally costly and have a time-lag that can be dangerous. These impediments
clarify its moderate movement on the advertise. This work considers both types of
measurements.
1.4 Diabetes Treatment Methods
Different approaches used for T1DM treatment, ranging from currently applied
methods to active research fields, are introduced in literature. Followings are
1.4.1 Standard Therapy
Currently, standard therapy as it will be called in this thesis is the norm when it
comes to T1DM treatment. This therapy is also referred to as basal/bolus therapy
or Multiple Daily Injections (MDI), if performed using insulin pens or syringes.
1.4.2 Basal Insulin
Basal insulin is insulin that acts relatively uniformly throughout the day and
should keep patients fasting BG concentration close to the optimum. Patients using
syringes or pens inject long-acting insulin once or twice a day while CSII-treated
patients use the insulin pump to adjust the basal rate in an ”optimal” manner. A
good overview of CSII treatment is given in [16].
1.4.3 Bolus Insulin
Bolus affront is affront that is injected in arrange to check the impact of dinners. The
carbohydrates contained in dinners are handled by the stomach related framework
and discharge glucose into the bloodstream. In arrange to dodge hyperglycemia, this
major unsettling influence needs to be checked by infusing a well-chosen amount of
fast-acting insulin using a syringe, write, or affront pump. This amount is based
on the quantity of ingested carbohydrates and the pre-meal BG concentration. To
compute the correct insulin sum, the understanding has to take an SMBG estimation
some time recently each meal [17].

CHAPTER 1. INTRODUCTION 17
1.4.4 Introduction to Systems and Control
In the setting of control, a framework, spoken to in figure 1.1, is an object of intrigued
(it can be numerous diverse things) upon which diverse actions can be taken - the
inputs u and that appears or gives diverse responses - the yields y. The inputs
are characterized by the reality that they can be manipulated from exterior the
framework, while the yields are characterized by the property that they can be
watched from exterior the framework. Additionally, disturbances may apply to the
frameworks. These are for the most part obscure, but have a quantifiable impact on
the yields. For case, in this proposal, the system is portion of the human endocrine
framework, the inputs are basically insulin injection and supper admissions, the yield
is BG concentration, and the disturbance is the estimation clamor or other obscure
excitations that have an impact on BG concentration.
Often, the behavior of a system is studied and described mathematically. This
description is called a model, and it should reproduce the outputs of a system,
based on the inputs, as accurately as possible. However, quite often, models are
not capable of capturing the whole behavior of a system, either because it is too
complex, or disturbances are too important. A system is called static if its outputs at
a given time are influenced by the inputs at that time, only. In a dynamical system,
however, the outputs are determined by current and past inputs. A controller is
used to adjust a systems inputs, in order to obtain desired outputs. This system is
called controlled system. A controller itself can be considered as a system, whose
output is the controlled systems input. If the controllers inputs depend directly on
the controlled systems outputs, then the controller is called a closed-loop controller,
otherwise it is called an open-loop controller. The output value that a closed-loop
control algorithm is intended to reach is called a set point [18].
1.4.5 Open-Loop Control
Open-loop control In control theory, an open-loop controller is a controller that com-
putes system inputs based on the current system state and a model in control theory.
In the context of T1DM treatment, open-loop control means that future insulin in-
fusions are computed using current BG measurements. Hence, standard therapy is
a good example of open-loop control applied at every SMBG measurement and us-
ing a simple static model for BG prediction. However, other implementations than
standard therapy exist for open-loop control and the use of different BG prediction
and state estimation methods may improve treatment. These improvements should

CHAPTER 1. INTRODUCTION 18
result in reduced hypo- and hyperglycemia. Open-loop control is currently not a very
active field of research, despite its potential improvements over standard therapy.
Figure 1.2: Illustration of open-loop control for T1DM treatment.
1.4.6 Closed-Loop Control
In closed-loop control, a nonstop or habitually inspected estimation is used to com-
pute the framework input ceaselessly or at the same inspecting rate, respectively.
For closed-loop T1DM treatment, persistent estimations, i.e. a CGM gadget, is re-
quired. The coming about criticism structure, appeared in figure 1.2, possibly leads
to sensational execution enhancements and better disturbance dismissal, in spite
of the fact that ensuring quiet security is still an open issue. The objective of a
closed-loop treatment is to replicate the behavior of a healthy pancreas as near as
conceivable while minimizing quiet involvement. Therefore, it is too alluded to as
the Fake Pancreas (AP) [19].
Figure 1.3: Illustration of closed-loop control for T1DM treatment
1.5 Motivation
Diabetes is a disease with an enormous human and economic impact, but its current
treatment is suboptimal, as it does not fully embrace the possibilities offered by
insulin pumps and CGM devices. Thus, research to improve the treatment has a lot of

CHAPTER 1. INTRODUCTION 19
potential to positively affect patient’s life while reducing the health care burden. For
these reasons, this thesis aims at making the treatment of patients with T1DM more
successful. An adequate control calculation must be competent of dealing with these
physiological and specialized challenges while still giving satisfactory performance.
Currently, the fundamental challenges is that the advance of manufactured pancreas
faces are the advancement of a solid closed-loop control calculation and availability
of a strong and exact glucose sensor [20].
The issue is to discover a criticism control for the framework so that it can work
automatically. The address is that can we control states of the framework so that
we can impact the framework by choosing a criticism control. For the purpose we
require to check the property, controllability, of the mathematical models for the
GIG frameworks. At that point the next address is to know that what kind of data
we can have from the yield of the framework. The property to answer this address
is the discernible of the framework. With respect to a control system there are two
questions one ordinarily came over. To begin with one is that in what way can we
impact the framework by choosing a fitting control? Second is what data almost the
framework can we get from the yield of the framework? The concept of controllability
answer the first question where as the observability concept answer the second one.
Controllability and observability are main issues in the analysis of a system before
deciding the best control strategy to be applied, or whether it is even possible to
control or stabilize the system. Controllability is related to the possibility of forcing
the system into a particular state by using an appropriate control signal. If a state is
not controllable, then no signal will ever be able to control the state. Observability
instead is related to the possibility of observing, through output measurements, the
state of a system. If a state is not observable, the controller will never be able to
determine the behaviour of an unobservable state and hence cannot use it to stabilize
the system [21, 22, 23, 13].
Refinements in calculations (relative indispensably subordinate, show predictive
control, fluffy rationale), stages (manufactured pancreas framework, Diabetes Assis-
tant), nonstop glucose screens (CGMs) and affront pumps, along with continuing
miniaturization and movability of these gadgets, have enhanced the common sense
and convenience of modern close-loop control frameworks by adults and teenagers
with sort 1 diabetes mellitus [24]. Furthermore, recent studies [25] incorporating
both insulin and glucagon infusions have extended the entire concept from an arti-
ficial β-cell closer to an artificial endocrine pancreas system [26].

CHAPTER 1. INTRODUCTION 20
1.6 Objectives
The goal of the present work is to get the answer of the question that why we still
can not have a fully automated artificial pancreas? In this work we tried to find the
reason of the problem of having no fully automatic artificial pancreas. The first step
in this direction is to find that do we have a controllable and observable system for
GIG. For the purpose some of the well known GIG systems are treated. If a linear
system is controllable then the nonlinear system is locally controllable but if the
linear system is not controllable then in general no conclusion can be drawn for the
nonlinear system. The most of the systems for GIG are nonlinear due to the action
of glucose, insulin and glucagon thus the systems treated here are linearised about
the equilibrium point. If system is controllable and observable then we can design a
feedback control. For an uncontrollable systems an attempt is made to answer the
reason on the basis of our results.
The aims of this research project are to implement and assess several differential
methods, with emphasis on procedures that do not require gradient information.
These techniques are referred to as derivative the mathematical solution of glucose
insulin-glucagon system and fully automatic artificial pancreas for diabetic patients.
Because other way of treatment like transparent of pancreas or liver is the chance
of infection, costly and very difficult process. The existing artificial pancreas is very
expensive and not reliable for every patient because it is not fully controllable. Imple-
ment the model of differential equation and Model of non-liner ordinary differential
equations for possible solutions.
1.7 Organization of Thesis
The thesis is organized as follows
Chapter 1: This chapter is an introductory chapter. The physiological background
is provided to familiarize the reader with subject. The general background of the
work, the research motivation, thesis objective and outline are given in this chapter.
Chapter 2: This chapter contains the basics about the linear control systems for
linear, continuous time control systems and linear time invariant control systems.
Chapter 3: This chapter contains the glucose insulin models. Controllability and
observability are discussed the Augmented minimal model and Reduced meal model
for type 1 diabetes mellitus for an artificial pancreas. These models can be used to
simulate a glucose insulin system for the treatment of type 1 diabetes and stabilizes

CHAPTER 1. INTRODUCTION 21
the control loop system for the glucose insulin pump.
Muhammad Farman, M.U Saleem, Control of Augmented minimal model
for glucose insulin pump, Current Research in Diabetes and Obesity
Journal, DOI: 10.19080/CRDOJ.2018.08.555742 (2018).
Chapter 4: In this chapter, we proposed the fractional order glucose insulin model
for healthy and type 1 diabetes and numerical simulations are carried out to support
the analytical results. Also discussed the controllability and observability of the
linearized system to design the close loop for automatic artificial pancreas.
M.U Saleem, M. Farman, Aqeel Ahmad, M.A Meraj Stability Analysis
and Control of Fractional Order Diabetes Mellitus Model for Artificial
Pancreas, Punjab University mathematics journal, 51(4),97-113, (2019)..
Chapter 5: Stability analysis of the model of glucose-insulin and glucagon system
in humans is made which is one of the important factors of study for healthy life.
We show the numerical simulation of the model for type 1 diabetes mellitus for
the controllability and observability matrix according to different initials conditions
on state vector. Model is used for this purpose and consists of glucose, insulin
and glucagon function in human body. Equilibrium points for different levels of
concentration of glucose are calculated. Proportional-Integral-Derivative (PID)
controller designed for an artificial pancreas. This paper is published
Muhammad Farman, Muhammad Umer Saleem, M. O Ahmad, Aqeel
Ahmad, Stability Analysis and Control of Glucose Insulin Glucagon
System in human, Chines Journal of Physics, 56 (4), 1362-1369, (2018).
Chapter 6: chapter 6 includes the Glucose insulin glucagon model like Sorensons
model for type 1 diabetes mellitus. Models are used for this purpose and consists
of glucose, insulin and glucagon function in human body. Equilibrium points for
different case of concentration of glucose are calculated by using Mathematica
software for stability of the system. Results are refined by using Jacobean linearized
method to check the stability of the model to design feedback control for artificial
pancreas. Publication include in this chapter are
Saleem M.U., Muhammad Farman, Meraj M.A., Stability Analysis
of Sorensen’s Model for controllability and observability, B. Life and
Environmental Sciences, 54 (2): 133145, (2017).
Muhammad Farman, M.U Saleem, M.O. Ahmad, An Approach for

CHAPTER 1. INTRODUCTION 22
Artificial Pancreas to Control the Type-1 Diabetes Mellitus, Journal of
Applied Environmental and Biological Sciences, 93-102, (2017).
Chapter 7: In this chapter composite model and its extension is treated for
type 1 diabetes. Equilibrium points for different case of concentration of glucose
are calculated and check the stability analysis of the system by using Lyapunov
function. Also checked the controllability and observability of the linearized system
to design the close loop for automatic artificial pancreas.
M.U Saleem, Muhammad Farman, Rizwan M., M.O. Ahmad, Aqeel
ahmad, Controllability and Observability of Glucose Insulin Glucagon
systems in Human , Chines journal of Physics, ,56(5), 1909-1916, (2018).
Chapter 8: Finally, a conclusion is drawn in chapter 7 and an outlook on possible
future work is given.

Chapter 2
Controllability and Observability
2.1 Introduction
A control system design deals with the problem of making a concrete physical system
behave according to certain desired specifications. The ultimate product of a control
system design problem is a physical device that, if connected to the to be controlled
physical system, makes it behave according to the specifications. This device is
called a controller. To get from a concrete to be controlled physical system to a
concrete physical device to control the system, the following intermediate steps are
often taken. First, a mathematical model of the physical system is made. Such a
mathematical model can take many forms. For example, the model could be in the
form of a system of ordinary and/or partial differential equations, together with a
number of algebraic equations, relating the relevant variables of the system. The
model could also involve difference equations, some of the variables could be related
by transfer functions, etc. The usual way to get a model of an actual system is
to apply the basic laws that the system satisfies. Often, this method is called first
principles modeling [27].
2.1.1 Linear Control System
Mathematically a linear control system is written in the form of following two equa-
tions,
x(t) = D(t)x(t) + E(t)u(t), t ∈ I (2.1)
y(t) = F (t)x(t), t ∈ I (2.2)
23

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 24
Where x(t) ∈ Rn, u(t) ∈ Rp and y(t) ∈ Rk for t ∈ I. The matrices D(t) ,
E(t) and F (t) are defined on I and have correct dimensions (i.e., D(t)) is n × n, E(t) is n × p and F (t) is k × nmatrix) . I is closed interval, I = [to, te],
t0 < te < ∞ , respectively. I = [t0,∞). We suppose the elements of the matrices
D(.), E(.) and F (.) are in L2(I;R).
The function u(.) is also suppose to be in L2(I;Rp) is called the input respectively
the control of the system. For given initial value x0 ∈ Rn and input u(.) ∈ L2(I;Rp)
of equation x(t) = D(t)x(t)+E(t)u(t), t ∈ I also called the state equation of system.
This system has a unique solution of x(.),in the sense of Caratheodory, i.e., x(.) is
absolutely continuous on I with x(t0) = x0 and the derivative x(.) is exist almost
every where on I. Furthermore equation (2.1) is satisfied on I , x(t) , t ∈ I is called
state of system at time t. If we have the solution of x(.) of equation (2.1) with initial
value xo and equation (2.2) establish y(.) ∈ L2(I;Rk) is called output of the system.
Figure 2.1: Idealized diagram of a control system
Figure 2.2: control system
In general we have not access the state x(.) itself but only some function of
the state. We can think the coordinate y(.) as those quantities of the system we
can measure. The diagram given in Figure (2.1)and (2.2) represents an idealized

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 25
situation. In reality we have distinguish between the system (or plant) and model
for the system, which is given by equation (2.1) and (2.2) for instance. The real
situation is representation in Figure 3.2. Usually one expects that the model for the
system describe the dynamics of the system sufficiently well, so that input-output
behavior of the model is sufficiently close to that of the system.
The output-equation (2.2) can also have the more general form
y(t) = F (t)x(t) +G(t)u(t), t ∈ I,
Which reflects a situation where the input influences the output also directly.
2.1.2 Linear Singular Control System
The equation
H(t)x(t) = D(t)x(t) + E(t)u(t), t ∈ I,
Where H(t) is an n × n matrix which is not invertible everywhere on I. such
system are called linear descriptor or linear singular control system.
In the system equation (2.1), (2.2) is called linear continues time system or (con-
trol system). The time set for such a system is an bounded or unbounded close
interval in R. A class of system are discrete time systems, where time set is finite
and infinite sequence t0 < t1 ... < te respectively t0 < t1 ... < te , and instead of
equation (2.1) and (2.2) we have
x(tk+1) = D(tk)x(tk) + E(tk)u(tk), k = 1, 2, 3, ...,
y(tk) = F (tk)x(tk), k = 0, 1, 2, 3, ...,
The main part of this work will be concerned with time-invariant , continuous-
time systems.This class of system is the special case of class characterized by
equation (2.1) and (2.2) where the matrices are constant in time:
x(t) = Dx(t) + Eu(t), t ∈ R (2.3)
y(t) = Fx(t), t ∈ R (2.4)
Lemma 1. a) Let X be a subspace of Rn. Then we have
Rn = X ⊕ X⊥.

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 26
b) For a subspace X1, X2 of Rn the following is true:
(X1 ∩X2)⊥ = X⊥1 +X⊥2 .
Let S be a real m× n matrix. Then we have
ker S = (range S>)⊥
(and consequently Rn = rangeS> ⊕ kerS).
2.2 Controllability
We denote x(.; t0, x0, u(.)) is the solution of equation (2.1) with initial data (t0, x0)
and input function u(.). Let φ(t, s) t, s ∈ I, denote the matrix solution of the
homogenous equation
x = D(t)x(t)
Then we have
x(t; t0, x0, u(.)) = φ(t, t0) +∫ t
t0φ(t, τ)dτ t ∈ I (2.5)
2.2.1 Definition
Assume that the control system is given by equations (2.1) and (2.2)
a) Let x0, x1 ∈ Rn and t0 ∈ I be given. The state x0 is at time t0 controllable
to x1, if and only if there exit t1 > t0 and a u ∈ L2([t0, t1];Rp) such that
x(t; t0, x0, u(.)) = x1
b) System (2.1) and (2.2) is completely controllable at t0, iff every state x0 ∈ Rn is
at time t0 ∈ I controllable to any state x1.
A state x1 is at t1 ∈ I reachable from x0 if and only if t0 < t1 ∈ I and a
u ∈ L2([t0, t1];Rp) such that x(t; t0, x0, u(.)) = x1. The System (2.1) and (2.2) is
completely reachable at time t1 ∈ I if and only if there exist a t0 < t1, t0 ∈ I, such
that every x1 ∈ Rn ia at time t1 reachable from every other state x0 ∈ Rn.
Using equation (2.3), x0 is controllable to x1 at time t0 iff t1 > t0 and a
u ∈ L2([t0, t1];Rp) such that
φ(t1, t0)x0 +∫ t
t0φ(t1, τ)E(τ)u(τ)dτ = x1

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 27
or equivalently
−x0 + φ(t0, t1)x1 =∫ t
t0φ(t0, τ)E(τ)u(τ)dτ.
Theorem 1. a) A State x0 is at time t0 controllable to the state x1 iff there exists
a t1 > t0x0 − φ(t0, t1)x1 ∈ range W (t0, t1),
where
W (t0, t1) =∫ t1
t0φ(t0, τ)E(τ)E(τ)>φ(t0, τ)>dτ
b) System (2.1) and (2.2) is completely controllable at some time t0 iff there exists
t1 > t0 such that
rangeW (t0, t1) = n (orequivalently range(t0, t1) = Rn).
Proof: The proof for a) follows directly from the previous lemma and the con-
sideration stated above that lemma. For the proof of b) let us first assume that
rankW (t0, t1) = n i.e., rangeW (t0, t1) = Rn. Then it follows immediately from a)
that any state x0 is at time t0 controllable to any x1 and in particular to 0. This
proves that the system is completely controllable at t0. We should remark that any
x0 can be controlled to any x1 on the fixed time interval [t0, t1].
If any x0 is at time t0 controllable to 0, then this is true for the elements b1, ..., bnof a basis for Rn, i.e., there exist ti > t0 and u ∈ L2([t0, ti];R
p) such that
bi = rangeW (t0, ti), i = 1, 2, ..., n,
If we can prove that rangeW (t0, s) ⊂ rangeW (t0, t) for t > s > t0, then
bi ∈ rangeW (t0, t1), i = 1, 2, ..., n. This implies rankW (t0, t1) = n. Now let
x ∈ rangeW (t0, s) and t > s. According to previous lemma this means that there
exists a u ∈ L2(t0, s;Rp) such that
x =∫ s
t0φ(t0, τ)E(τ)u(τ)d(τ) =
∫ t1
t0φ(t0, τ)E(τ)u(τ)d(τ)
Here u(τ) = u(τ) for t0 ≤ τ ≤ s and u(τ) = for s < τ ≤ t. Since u ∈ L2(t0, t;Rp)
we see, again using previous lemma, that x ∈ rangeW (t0, t) [30, 22, 13].

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 28
2.2.2 Linear, time-invariant control system
We consider controllability for a system given by the equation (2.3) and (2.4). The
fundamental matrix solution of the homogenous equation x(t) = Dx(t) + Eu(t), is
given by
φ(t, s) = eD(t−s) =∞∑k=0
1
k!Dk(t− s)k
If we take t0 = 0, Then controllability Grammian is given by
W (0, t) =∫ t
t0e−DτEE>e−D
>τdτ (2.6)
In view of Theorem 1 we are interested in range W (0.t)) for t > 0. Accord-
ing to (Lemma 1, c), we have range W (0.t) = (kerW (0, t))⊥. We first inves-
tigate kerW (0, t). Since W (0, t) is symmetric,x ∈ kerW (0, t) is equivalent to
x>W (0.t)x = 0. Using this and (2.2) we see that x ∈ kerW (0, t) if and only if
x>W (0, t)x =∫ t
t0x>e−DτEE>e−D
>τdτ =∫ t
t0‖E>e−D>τx‖2
2dτ
i.e.if and only if E>e−D>τx ≡ 0. by analyticity of τ → e−D
>τ this in turn is equivalent
to
E>(D>)kx = 0, k = 0, 1, ...
By Cayley-Hamilton theorem we can restrict k to k = 0, 1, 2, ..., n− 1 and get
kerW (0, t) =n−1⋂k=0
kerE>(D>)k for all t ∈ R.
Using Lemma 1 this implies
rangW (0, t) =n−1∑k=0
(kerE>(D>)k)⊥ =n−1∑k=0
rangeDkE for all t ∈ R.
From Theorem 1 we get
Theorem 2: Let control system be given by equation (2.3) and (2.4)
a) A State x0 is at time 0 (equivalently at any time t0 ∈ R)controllable to zero
if and only if
x0 ∈ range(E,DE, ..., Dn−1E)

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 29
b) System (2.3) and (2.4) is completely reconstructible at some time 0 (equivalently
at any time t0 ∈ R) if and only if
rank(E,DE, ..., Dn−1E) = n
Proof: We only have to verify that range
(E,DE, ..., Dn−1E) =n−1∑k=0
rangeDkE.
But this is clear, because range AkB is generated by the columns of AkB and if
a1, ..., ar, b1, ..., br generate X + Y .
If the rank condition in statement b) of the theorem is satisfied for the matrices
D and E, then we say that the pair (D;E) is controllable. Since the condition given
in statement b) of Theorem 2 is independent of t0 and t1, completely controllability
for a time-invariant linear system is equivalent to the following property: For any
x0, x1 ∈ R and any times t0 < t1 there exists a control u(.) such that the solution
of (2.3) with initial values (t0, x0) and control function u(.) reaches x1 at time t1.
Note that the the difference t1 − t0 can be arbitrary small. Of course, if t1 − t0is small, then the values of u(t) and also x(t) on the interval (t0, t1) can become large.
Since the conditions in Theorem 2 are independent of t0 and t1, it can be expected
that in this theorem we can replace ’controllable’ respectively ’completely control-
lable’ by ’reachable’ respectively ’completely reachable’. It is indeed an easy exercise
to prove the analogous results for ’reachable at time t1 from x0’ and ’completely
reachable’. The subspace
(E,DE, ..., Dn−1E) =n−1∑j=0
rangeDjE.
is called the controllable subspace for system (2.3), (2.4) [30, 22, 23].
2.3 Observability (Reconstructibility)
Let the control system is given by equations (2.1) and (2.2)

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 30
a) Let x0 ∈ Rn non-observable and t0 ε I if and only if there exit t1 < t0 ∈ I,
such that
F (t)x(t; t0, x0, u(.)) = F (t)x(t; t1, x0, u(.)) (2.7)
for all t ∈ [t1, t0 and u ∈ L2([t1, t0];Rp).
b) System (2.1) and (2.2) is completely observable at time t0 ∈ I, if and only if
0 is the only state which at time t0 non-observable.
A state x0 is non-observable at t0 ∈ I iff t1 > t0 , t1 ∈ I such that
F (t)x(t; t0, x0, u(.)) = F (t)x(t; t1, x0, u(.)) for all t ε [t0, t1] and a u ∈ L2([t0, t1];Rp).
The System (2.1) and (2.2) is completely observable at time t0 εI if and only if 0 is
the only state which at time t0 is non-observable.
Using the representation (2.5) then equation (2.6) equivalent to
F (t)φ(t; t0)x0 = 0, t ∈ [t1, t0] (2.8)
For t0, t1 ∈ I t1 < t0, we define the mapping Ft0,t1 : Rn → L2([t1, t0];Rk) by
Ft0,t1x = F (.)φ(., t0)x, x ∈ Rn (2.9)
Then condition (2.5) is equivalent to
x0 ∈ KerFt0,t1 (2.10)
If we choose complementary subspace X of KerFt0,t1 , i.e.,
Rn = X ⊕KerFt0,t1
, then any state x0 ∈ Rn has a unique representation as
x0 = x01 + x02, x01 ∈ X, x02KerFt0,t1
The component x01 is reconstructible at t0 (equivalently any time) in the following
sense: If, for some t∗ < t0, we have yt = Fx(t; t0, x01, 0) = 0 on [t∗, t0], then x01 =
0. Note, that by linearity of the system this is equivalent to Fx(t; t0, x0, u(.) =
Fx(t; t0, 0, u(.)), t ∈ [t∗, t0] for all u ∈ L2([t∗, t0];Rp). By linearity of the system
we could phrase this also as follow: Let x0, x1 be two states of the system. If,
for some t∗ < t0, we have Fx(t; t0, x0, u(.) = Fx(t; t0, 0, u(.)), t ∈ [t∗, t0] for all
u ∈ L2([t∗, t0];Rp), then x1 − x0 ∈ kerFt0,t1 . A special complementary subspace
forkerFt0,t1 is (kerFt0,t1)⊥. The consideration from above motivate the following

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 31
definition: we call a state x0 ∈ Rn observable at time t0 ∈ I if and only if there
exit a t1 < t0,t0 ∈ I, such that
x0 ∈ (KerFt0,t1)⊥
. Observe that ’reconstructible’ is not the negation of ’non-reconstructible’
Using lemma , equation (2.7) is equivalent to
x0 ∈∫ t0
t1φ(τ, t0)>F (τ)>F (τ)φ(τ, t0)dτ
With
N(t0, t1) =∫ t0
t1φ(τ, t0)>F (τ)>F (τ)φ(τ, t0)dτ, t1 < t0, (2.11)
Theorem 3. Let control system be given by equation (2.3) and (2.4)
a) A State x0 ∈ Rn is at t0 ∈ I non-reconstructible iff there exits such that
t1 < t0, t1 ∈ I, such that
x ∈ ker N(t0, t1).
b) The linear system (2.1) and (2.2) is completely reconstructible at t1 ∈ I iff there
exists a t1 < t0, t1 ∈ I, such that
rank N(t0, t1) = n
Proof:
We only have to prove statement b). Using a) and the definition of complete
reconstructibility. We immediately get that for any x ∈ Rn there exists a t1 < t0such that x ∈ kerN(t0, t1). Let e1, ..., en be a basis for Rn. Then there exist si < t0such that ei ∈ kerN(t0; si), i = 1, ..., n. Since, for s < t0, x ∈ kerN(t0; s) is
equivalent to x ∈ kerFt0;s, i.e., to F (τ)Φ(τ, t0)x = 0 i.e. on [s, t0], we easily see
that kerN(t0, s) ⊂ kerN(t0; t) for s < t. Therefore we get ei ∈ kerN(t0, t1), i =
1, ..., n, with t1 = min(s1, ..., sn) < t0. The matrix N(t0, t1) is usually called the
reconstructibility Grammian of system (2.1), (2.2). The same remarks apply to this
matrix as the ones given for the controllability Grammian [31, 21, 23].
2.3.1 Observability of Linear, time-invariant control system
In this subsection we consider observability for linear , time-invariant control sys-
tem given by equation (2.3) and (2.4). Since most of the consideration concerning
observability for linear , time-invariant control system.

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 32
Equation (2.7) for a system (2.5) and (2.6) which is equivalent to
FeDτx0 ≡ 0. (2.12)
By analyticity of τ → eDτ , equation (3.3.6) is equivalent to
FDjx0 = 0, j = 0, ..., n− 1
respectively to
x0 ∈ kerF, (2.13)
where F =
F
FD
.
.
.
FDn−1
which in view lemma 1 is equivalent to
x0 ∈ (range(F>, D>F>, ..., (D>)n−1F>)⊥
The condition rankN(t0, t1) = n is equivalent to kerN(t0, t1) = 0 which in turn for
arbitrary t0, t1 is equivalent to rankF = n
Thus we have established the following results:
Theorem 4. Let control system be given by equation (2.3) and (2.4)
a) A State x0 ∈ Rn is non-reconstructible at time t0 (or, equivalently , at any
time) if and only if
x0 ∈ ker F, (2.14)
b) System (2.3) and (2.4) is completely reconstructible at some time t0 (or, equiva-
lently , at any time) if and only if
rank F = n, (2.15)
Proof: It is easily seen that for linear, time-invariant systems the notions ’non-
reconstructible’ respectively ’completely reconstructible’ are equivalent to ’observ-
able’ respectively ’completely observable’. For linear, time-invariant systems one
usually uses the latter terms. We call the pair (F,A) observable if and only if
condition rankF = n is satisfied. The subspace kerF is called the unobservable
subspace for system (3.1.3), (3.1.4). If we compare conditions rankF = n and

CHAPTER 2. CONTROLLABILITY AND OBSERVABILITY 33
rank(E,DE, ..., Dn−1E) = n we see that complete reconstructibility of the system
(2.3), (2.4) is equivalent to complete controllability of the system
˙x(t) = −DTx(t)− F Tv(t)
z(t) = ETx(t), t ∈ R,
and that complete observability of the above system is equivalent to the complete
observability of the system (2.5), (2.6). This follows immediately from rankC =
rank(F T , DTF T , ..., (DT )n−1F T )
rank(E,DE, ..., Dn−1E) = rank
ET
ETDT
.
.
.
ET (DT )n−1
.
This indicates that there exists a relation between control systems such that a
system property like reconstructibility is equivalent to another system property, as
for instance controllability, for the related systems [22, 23, 13, 21].

Chapter 3
Glucose Insulin System
In this chapter, Augmented Minimal model and Reduced meal model for type 1
diabetes mellitus are discussed. Controllability and observability of these system are
treated for control purpose for close loop feedback design.
3.1 Augmented Minimal Model
First time, augmented minimal model glucose kinetics was described for type 1 di-
abetes mellitus. In human homeostasis augmented minimal model is most accurate
and most useful model. Transfer of insulin from the injected site to the central
circulation and glucose from the stomach to the central circulation is described in
augmented minimal model [28].
G = −Sg(G−Gb)−XG+Ra(t)
Vg(3.1)
Gi = −1
τ(Gi −G) (3.2)
X = −p2X + p3(Ip − IPbasal) (3.3)
I = −nI +ka1ISQ1 + ka2ISQ2
Vi(3.4)
ISQ1 = −(ka1 + kd)ISQ1 + J(t) (3.5)
ISQ2 = −ka2ISQ2 + kdISQ2 (3.6)
Ra = − 1
τmeal(Ra−D(t)) (3.7)
34

CHAPTER 3. GLUCOSE INSULIN SYSTEM 35
In these equations, t is the independent model variable time, G(t) is the plasma
glucose concentration [mg/dL], I(t) is the plasma insulin level [U/mL] and X(t) is
the interstitial insulin activity. Gb is the basal plasma glucose concentration [mg/dL]
and Ipbasal is the basal plasma insulin concentration [µU/mL]. Basal plasma con-
centrations of glucose and insulin are typically measured before administration of
glucose (or sometimes 180 minutes after).ISQ1 and ISQ2 are the subcutaneous insulin
transport after injection (J), Ra is the glucose rate appearance from a meal D. These
are unknown parameters in this model: Sg, Vg, p2, p3, ka1, ka2, kd and n [28].
Parameter value Parameters values
n 0.2 Vi 0.125
Sg 0.0094 J(t) 0.690656
Vg 96000000 D(t) 247.76
p2 0.0265 ka1 0.002
p3 0.00005 ka2 0.0211
Ip 15 kd 0.0166
IPbasal 2.7648 τmeal 0.055
τ 0.2 Gb 142
Table 3.1: Table of Parameter’s used in the Augmented Minimal Model
Model after substitution parameter value becomes
G = −0.0094(G− 142)−XG+Ra(t)
2.5(3.8)
Gi = − 1
0.2(Gi −G) (3.9)
X = −0.0265X + 0.00005(15− 2.7648) (3.10)
I = −0.2I +0.002ISQ1 + 0.02ISQ2
0.125(3.11)
ISQ1 = −(0.002 + 0.0166)ISQ1 + 0.690656 (3.12)

CHAPTER 3. GLUCOSE INSULIN SYSTEM 36
ISQ2 = −0.0211ISQ2 + 0.0166ISQ2 (3.13)
Ra = − 1
0.055(Ra− 247.76) (3.14)
Put left hand side of the system (3.8− 3.14) equal to zero and get the Equilibrium
point of the model is
(G,Gi, X, I, ISQ1, ISQ2, Ra) = (3091.85, 3091.85, 0.023085, 2.97056, 37.132, 0, 247.76)
Hence, the linearized model according to the equilibrium point is
G = −0.032465G− 3091.81X + 0.4Ra (3.15)
Gi = 5G− 5Gi (3.16)
X = −0.0265X (3.17)
I = −0.2I − 0.016ISQ1 + 0.1688ISQ2 (3.18)
ISQ1 = −0.0186ISQ1 (3.19)
ISQ2 = −0.0045ISQ2 (3.20)
Ra = −18.18Ra (3.21)
3.1.1 Linear Control System:
Consider the linear system
x(t) = Ax(t) +Bu(t) (3.22)
y(t) = Cx(t) (3.23)
In this case we have
x = [G Gi X I ISQ1 ISQ2 Ra]T
Where
A =
−0.032485 0 −3091.85 0 0 0 0.4
5 −5 0 0 0 0 0
0 0 −0.0265 0 0 0 0
0 0 0 −0.2 −0.016 0.1688 0
0 0 0 0 −0.0186 0 0
0 0 0 0 0 −0.0045 0
0 0 0 0 0 −18.18

CHAPTER 3. GLUCOSE INSULIN SYSTEM 37
If we consider the glucose concentration in plasma is the only measured output and
the insulin concentration in plasma is only input then B = [0 0 1 0 0 0]T and
C = [1 0 0 0 0 0 0 ]. The controllability matrix is R = [B AB A2B ... A6B] and
its rank is 1.So the system is not controllable. The observability matrix is O =
[C;CA;CA2;CA3; ...;CA6]T and its rank is 3. So the system is not observable. At
equilibrium point (3091.85; 3091.85; 0.023085; 2.97056; 37.132; 0; 247.76) and at dif-
ferent initial conditions like (100; 0; 11.01; 0; 0; 0; 0), (100; 0; 11.01; 11.01; 11.01; 0; 0),
(110; 0; 15.01; 0; 0; 0; 0), (130; 0; 20.01; 0; 0; 0; 0) the controllability and observability
of the graph is approaches to zero, so system not work like close loop for feedback
design are shown in figures 3.1 to 3.3.
Figure 3.1: Controllability and observability Graph

CHAPTER 3. GLUCOSE INSULIN SYSTEM 38
Figure 3.2: Controllability and observability Graph
3.2 Reduced Meal Model
This model is designed to tell about control glucose on insulin and insulin on glucose
and also about their subsystems. Glucose and insulin subsystems are the part of
this model. Insulin dependent utilization and insulin independent utilization in the
glucose kinetics model is the subsystem of glucose. Plasma and fat equilibrating tis-
sue is represented by insulin independent. Peripheral tissue is represented by insulin
dependent partition. Plasma and liver is described in inulin subsystem [29]. This
departs from the initial model, which included a strongly nonlinear modeling of the
rate of appearance of glucose. The model is consists of 11 nonlinear differential equa-
tions, different parameters and constants their values given in [29, 28]. Followings
are the equation of the model

CHAPTER 3. GLUCOSE INSULIN SYSTEM 39
Gp = −(k2 + kp2)Gp + k1Gt − Uii − kp3Id +Ra(t) + kp1 (3.24)
Gt = −k1Gt + k2Gp −Vm0 + VmX
X
Kmo +Gt
Gt (3.25)
Gi = − 1
τIG(Gi −
Gp
Vg) (3.26)
Id = −ki(Id − I1) (3.27)
I1 = −ki(I1 −IpVi
) (3.28)
Ip = −(m2 +m4)Ip +m1Il + ka1ISQ1 + ka2ISQ2 (3.29)
Il = −(m1 +m3)Ip +m2Ip (3.30)
X = −p2u(X −IpVi
+ Ib) (3.31)
ISQ1 = −(ka1 + kd)ISQ1 + J(t) (3.32)
ISQ2 = −ka2ISQ2 + kdISQ2 (3.33)
Ra = − 1
τmeal(Ra −D(t)) (3.34)
Following is the table of parameter’s value
Parameter value Parameter value Parameter value
k1 0.0702 k2 0.1151 Vg 1.834
kp1 5.1207 kp2 0.0061 kp3 0.0087
Ib 104 Uii 1 τIG 0.2
J(t) 0.690656 D(t) 247.76 Vi 0.0503
ka1 0.002 ka2 0.0211 kd 0.0166
Vmo 5.3263 VmX0.0417 τmeal 0.055
Km0 234.0043 m1 0.0312 m2 0.3616
m4 0.1446 ki 0.0075 m3 0.306
p2u 0.0276
Table 3.2: Table of Parameters used in the Reduced Meal Model

CHAPTER 3. GLUCOSE INSULIN SYSTEM 40
After Substitution parameter values, we get
Gp = −0.1212Gp + 0.0702Gt − 0.0087Id +Ra(t) + 4.1207 (3.35)
Gt = −0.0702Gt + 0.1151Gp −5.3263 + 0.0417X
234.0043 +Gt
Gt (3.36)
Gi = −5Gi + 2.7262Gp (3.37)
Id = −0.0075Id + 0.0075I1 (3.38)
I1 = −0.0075Id + 0.1491I1 (3.39)
Ip = −0.5062Ip + 0.0312Il + 0.002ISQ1 + 0.0211ISQ2 (3.40)
Il = 0.0244Ip (3.41)
X = −0.0276X + 0.5487Ip − 2.8704 (3.42)
ISQ1 = −0.0638ISQ1 + 0.690656 (3.43)
ISQ2 = −0.00449ISQ2 (3.44)
Ra = −18.1818Ra + 4504.7272 (3.45)
Substitute left hand side of the system equal to zero, we find equilibrium points of
(Gp, Gt, Gi, Id, I1, Ip, Il, X, ISQ1 , ISQ2 , Ra) are
(41197.8, 67539.4, 22462.7, 0, 0, 0,−0.69391,−104, 10.8253, 0, 247.787) and
(1947.56,−225.976.04, 1061.89, 0, 0, 0,−0.69391,−104, 10.8253, 0, 247.787)
In this model both the equilibrium point includes two negative values one for
Il and other for X. Il is the insulin kinetics of glucose production. X insulin
concentration in plasma are taken in units so it cannot have a negative value. This
is the most comprehensive model in the glucose insulin system dynamics for human
but the result show that this model has some deficiency in it since the equilibrium
point is not in feasible region.
Gp = −0.1212Gp + 0.0702Gt − 0.0087Id +Ra(t) (3.46)
Gt = −0.7145Gt + 0.1151Gp − 6.15× 10−7X (3.47)
Gi = −5Gi + 2.7262Gp (3.48)
Id = −0.0075Id + 0.0075I1 (3.49)
I1 = −0.0075Id + 0.1491I1 (3.50)
Ip = −0.5062Ip + 0.0312Il + 0.002ISQ1 + 0.0211ISQ2 (3.51)

CHAPTER 3. GLUCOSE INSULIN SYSTEM 41
Il = 0.0244Ip (3.52)
X = −0.0276X + 0.5487Ip (3.53)
˙ISQ1 = −0.0638ISQ1 (3.54)
˙ISQ2 = −0.00449ISQ2 (3.55)
Ra = −18.1818Ra (3.56)
Theorem 3.1: The linear x(t) = Ax(t), where A continuous and bounded for t ≥ t0, is uniformly asymptotically stable if and only if given a positive definite real matrix
A, there exists a symmetric positive definite real matrix P , which satisfies
P (t) + AT (t)P (t) + P (t)A(t) = −Q(t), t ≥ t0
The linear time invariant system x(t) = Ax(t)the corresponding equation to be used
as ATP + PA+Q = 0 this is called Lyapunov equation [32, 33, 34].
Proof: By using Lyapunov equation ATP + PA+Q = 0 , then we have A =
−0.12 0.07 0 −0.0087 0 0 0 0 0 0 0
0.11 −0.71 0 0 0 0 0 −6.15× 10−7 0 0 0
2.72 0 −5 0 0 0 0 0 0 0 0
0 0 0 −0.0075 0.0075 0 0 0 0 0 0
0 0 0 −0.0075 0.1491 0 0 0 0 0 0
0 0 0 0 0 −0.50 0.03 0 0.002 0.02 0
0 0 0 0 0 0.02 0 0 0 0 0
0 0 0 0 0 0.54 0 −0.0276 0 0 0
0 0 0 0 0 0 0 0 −0.063 0 0
0 0 0 0 0 0 0 0 0 −0.004 0
0 0 0 0 0 0 0 0 0 0 −18.18
and substitute Q = I11×11 in Lyapunov equation ATP + PA + Q = 0, and by
using matlab we find matrix P but P is not symmetric positive-definite solution P so

CHAPTER 3. GLUCOSE INSULIN SYSTEM 42
system is not asymptotically and uniformly stable. In other technique eigne values of A are
(−5.0000,−0.7228,−0.1072,−0.0071, 0.1487,−0.5012, 0.0012,−0.0276,−0.0630,−0.0040,−18.1800),
so the system is not again asymptotically and uniformly stable.
3.3 Linear Control
Consider the linear system
x(t) = Ax+Bu (3.57)
y(t) = Cx (3.58)
In this case we have
x = [Gp, Gt, Gi, Id, I1, Ip, Il, X, ISQ1 , ISQ2 , Ra]T
andA =
−0.12 0.07 0 −0.008 0 0 0 0 0 0 0
0.11 −0.71 0 0 0 0 0 −6.15× 10−7 0 0 0
2.72 0 −5 0 0 0 0 0 0 0 0
0 0 0 −0.007 0.0075 0 0 0 0 0 0
0 0 0 −0.007 0.1491 0 0 0 0 0 0
0 0 0 0 0 −0.50 0.03 0 0.002 0.02 0
0 0 0 0 0 0.02 0 0 0 0 0
0 0 0 0 0 0.54 0 −0.0276 0 0 0
0 0 0 0 0 0 0 0 −0.063 0 0
0 0 0 0 0 0 0 0 0 −0.004 0
0 0 0 0 0 0 0 0 0 0 −18.18
3.3.1 Controllability and Observability
Here we take the only measured output of glucose and the only input is insulin then
B = [0, 0, 0, 0, 0, 0, 0, 1, 0, 0, 0]T and C = [1, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0]
R = [B,AB,A2B,A3B ... A10B]

CHAPTER 3. GLUCOSE INSULIN SYSTEM 43
The system is not controllable because its rank (i.e.rank(R) 6= 11). The observability
matrix is given by
O = [C,CA,CA2, CA3 ... CA10]T
The system is not observable because its rank (i.e.rank(R) 6= 11). By using the Matlab
function found that system is not controllable nor observable. At equilibrium point the
controllability and observability of the graph is approaches to zero, so system not work
like close loop for feedback design.
3.4 Conclusion
Consider Augmented Minimal model of Glucose Kinetics and reduced meal model which
had a simple but comprehensive models. The controllability and observability for linearized
system are treated. In first model,we consider that only measured output is concentration
of glucose in plasma that we can measure easily. The system is not controllable neither
observable. The controllability and observability of the graph is approaches to zero, so
system not work like close loop for feedback design. Reduced meal model which had
a simple but comprehensive models are also treated for glucose insulin pump. For this
purpose, In the model the equilibrium point includes two negative values one for Il and
other for X. Il is the insulin kinetics of glucose production. X insulin concentration in
plasma are taken in units so it cannot have a negative value. The system is not stable at
these points results are also verified with Lyapunov function for stability analysis. Consider
that only measured output is concentration of glucose in plasma that we can measured
easily. The system is not controllable neither observable.

Chapter 4
Fractional Order Glucose InsulinModel
4.1 Fractional Order Glucose Insulin Model
We determine a model for all plasma glucose concentration, generalized insulin and plasma
insulin. Diabetes dynamics is a mathematical model. There are two other models of
glucose/insulin used to explain interaction. These are valid to predict blood glucose because
these are inherent requirement of frequently updated information. In this model we take
glucose level G, glucose uptake X, insulin level I. This model also include the basal values
Gband Ib [4]. The model is given in the followings equations
G(t) = −m1G+m2I +m1Gb (4.1)
X(t) = −m2X +m3I −m3Ib +m6Ib (4.2)
I(t) = −m3I +m4G+m4m5 −m6I +m6Ib (4.3)
with initial conditions
G(0) = p1 = 100, X(0) = p2 = 0, I(t) = p3 = Ib (4.4)
Where G(t) is plasma glucose concentration, X(t) is plasma insulin variable for remote
compartment, I(t) is plasma insulin concentration, Gb is the basal preinjection value of
44

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 45
plasma glucose, Ib is basal preinjection value of plasma insulin, m1 is the insulin indepen-
dent rate uptake in liver, muscle and adipose tissue, m2 is the rate of decrease in tissue
glucose uptake ability, m3 is the insulin independent increase in glucose uptake ability in
Ib, m4 is the rate of pancreatic cells which are released after the glucose injection and
glucose concentration above system, m5 is the threshold value of glucose, m6 is the decay
rate for insulin in plasma [4]. The values of parameter are given as follows.
Parameter Normal person Type 1 Diabetes Units
m1 0.0317 0 min−1
m2 0.0123 0.017 min−1
m3 4.92× 10−6 5.3× 10−6 min−2(µU/ml)
m4 0.0039 0.0042 (µU/ml)min−2(mg/dl)−2
m5 79.053 80.25 mg/dl
m6 0.2659 0.264 min−1
Gb 80 80 mg/dl
Ib 7 15 µU/ml
Table 4.1: Table of Parameter’s used in Sandhya Model
4.1.1 Stability Analysis and Equilibria
Model after substituting parameter values given in table 4.1, we get
G(t) = −0.0317000G+ 0.0123I + 2.536 (4.5)
X(t) = −0.0123X + 0.00000492I − 0.00000492 + 1.8613 (4.6)
I(t) = −0.26590492I + 0.0039G+ 2.1695 (4.7)

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 46
Substituting the left hand side of the system equal to zero and we get the values of G, X
and I . Hence the equilibrium points are
(83.6417, 151.3288, 9.3817)
Theorem 4.1: The linear x(t) = Ax, where A continuous and bounded for t ≥ t0 , is
uniformly asymptotically stable if and only if given a positive definite real matrix A, there
exists a symmetric positive definite real matrix P , which satisfies
P (t) +AT (t)P (t) + P (t)A(t) = −Q(t), t ≥ t0
The linear time invariant system x(t) = Ax the corresponding equation to be used as
ATP + PA+Q = 0 this is called Lyapunov equation [32, 33].
Proof:
Here
A =
−0.0317 0.0123 0
0 −0.0123 1.1876
0.0039 −0.2659 0
and substitute Q = I3×3 in ATP + PA+Q = 0, get P
P =
16.0010 0.5880 −2.2467
0.5880 219.0273 1.8475
−2.2467 1.8475 49.0567
The Lyapunov equation has symmetric positive-definite solution P , then the eigen
values of A are (−0.0315,−0.0062 + 0.5619i,−0.0062 − 0.5619i) has negative real parts,
so the system is asymptotically and uniformly stable. Now, we give some fundamental
results and definitions from fractional calculus. For detailed over view of the topic readers
are referred to [35, 36, 37, 38].

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 47
Definition 4.1 The definitions of Laplace transform of Caputo’s derivative and Mittag-
Leffler function in two arguments is written as
L {Dαf(t), s} = sαF (s)− Σn−1i=0 s
α−i−1f (i)(0), (n− 1 < α ≤ n); n ∈ N.
The fractional order extension of this model have been first studied in [40, 39] and show
the realistic biphasic decline behavior of infection of diseases but at a slower rate. The new
diabetes mellitus model described in the form of fractional differential equations (FDEs)
given as
Dα1G(t) = −m1G+m2I +m1Gb (4.8)
Dα2G(t) = −m2X +m3I −m3Ib +m6Ib (4.9)
Dα3I(t) = −m3I +m4G+m4m5 −m6I +m6Ib (4.10)
with initial conditions G(0) = p1 = 100, p2 = X(0) = 0, I(0) = p3 = Ib.
4.2 Laplace Adomian Decomposition Method
Consider the fractional-order epidemic model (4.8 − 4.10) subject to the initial condition
(4.4). For α1 = α2 = α3 = 1 the fractional order model converts to the classical diabase
model. Applying the Laplace transform on equation (4.8− 4.10), we get
L {Dα1t G(t)} = −m1L {G(t)}+m2L {I(t)}+ L {m1Gb} (4.11)
L {Dα2t X(t)} = −m2L {X(t)}+m3L {I(t)} −L {(m3Ib −m6Ib)} (4.12)
L {Dα3t I(t)} = −(m3 +m6)L {I(t)}+m4L {G(t)}+ L {(m6Ib +m4m5)} (4.13)
By applying the rule of Laplace transform, we get
Sα1L {G} − Sα1−1G(0) = −m1L {G(t)}+m2L {I(t)}+ L {m1Gb} (4.14)

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 48
Sα2L {X} − Sα1−1X(0) = −m2L {X(t)}+m3L {I(t)} −L {m3Ib −m6Ib} (4.15)
Sα3L {I} − Sα1−1I(0) = −(m3 +m6)L {I(t)}+m4L {G(t)}+ L {m6Ib +m4m5}(4.16)
Sα1L {G} = Sα1−1G(0)−m1L {G(t)}+m2L {I(t)}+ L {m1Gb} (4.17)
Sα2L {X} = Sα1−1X(0)−m2L {X(t)}+m3L {I(t)} −L {m3Ib −m6Ib} (4.18)
Sα3L {I} = Sα1−1I(0)− (m3 +m6)L {I(t)}+m4L {G(t)}+ L {m6Ib +m4m5} (4.19)
by using the initial conditions (4.4), we get
L {G} =p1
S+m1GbSα1+1
+m2
Sα1L {I(t)} − m1
Sα1L {G(t)} (4.20)
L {X} =p2
S− m3Ib −m6Ib
Sα2+1− m2
Sα2L {X(t)}+
m3
Sα2L {I(t)} (4.21)
L {I} =p3
S+m6Ib +m4m5
Sα3+1− m3 +m6
Sα3L {I(t)}+
m4
Sα3L {G(t)} (4.22)
4.3 Case I for Normal Person
First of all we study the glucose, plasma concentration and insulin for non-diabetic person
for the period of 10 hours. The model show that when we give glucose to normal man then
the level of glucose concentration is very high but after time passing it become stable [4].
The model after substituting the parameters values for case I.
L {G} =p1
S+
2.536
Sα1+1+
0.0123
Sα1L {I(t)} − 0.0317
Sα1L {G(t)} (4.23)
L {X} =p2
S+
1.861
Sα2+1− 0.0123
Sα2L {X(t)}+
4.92× 10−6
Sα2L {I(t)} (4.24)

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 49
L {I} =p3
S+
2.1696
Sα3+1− 0.2659
Sα3L {I(t)}+
0.0039
Sα3L {G(t)} (4.25)
with initial conditions G(0) = p1 = 100, p2 = X(0) = 0, I(0) = p3 = 7.
It should be assumed that method gives the solution as an infinite series
G =∞∑k=0
Gk, X =∞∑k=0
Xk, I =∞∑k=0
Ik (4.26)
Substitute equations (4.26) in (4.23− 4.25), we have the followings results
L {G0} =p1
S+
2.536
Sα1+1, L {X0} =
p2
S+
1.861
Sα2+1, L {I0} =
p3
S+
2.1696
Sα3+1(4.27)
Similarly we have
L {G1} =0.0123
Sα1L {I0} −
0.0317
Sα1L {G0}, ..., L {Gk+1} =
0.0123
Sα1L {Ik}−
0.0317
Sα1L {Gk} (4.28)
L {X1} =−0.0123
Sα2L {X0}+
0.00000492
Sα2L {I0}, ...,
L {Xk+1} =−0.0123
Sα2L {Xk}+
0.00000492
Sα2L {Ik} (4.29)
L {I1} =−0.2659
Sα3L {I0}+
0.0039
Sα3L {G0}, ...,L {Ik+1} =
−0.2659
Sα3L {Ik}+
0.0039
Sα3L {Gk} (4.30)
The purpose of the work is to analysis the mathematical behaviour of the solution
G(t), X(t), I(t) for the different values of α. By applying the inverse laplace transform
to both sides of the equation (4.27), we get the values of G0, X0, I0 and used for further
process. Putting the values of G0, X0, I0 into the equations (4.28 − 4.30) and get the

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 50
values of G1, X1, I1. Similarly we find the remaining term G2, G3, G4, ...., X2, X3, X4, ....
and I2, I3, I4, .... in the same manners. Solution can be written as
G(t) = G0 +G1 +G2 +G3 +G4, ... (4.31)
X(t) = X0 +X1 +X2 +X3 +X4, ... (4.32)
I(t) = I0 + I1 + I2 + I3 + I4, ... (4.33)
by substituting the values of G0, X0, I0, G1, X1, I1 and G2, G3, G4, .... we get
G(t) = 100− 0.547tα1
α1!+ 0.0267
tα3
α3!+ 0.0174
t2α1
2α1!− 0.0190
tα1+α3
(α1 + α3)!− 0.0071
tα1+2α3
(α1 + 2α3)!
+ 0.00012t2α1+α3
(2α1 + α3)!+ 0.0025
t3α1
3α1!(4.34)
X(t) = 1.86103tα2
α2!− 1.92× 10−9 t
2α2
2α2!+ 3.5× 10−6 tα2+α3
(α2 + α3)!+ 0.00028
t3α2
3α2!+
1.3× 10−7 t2α2+α3
(2α2 + α3)!− 2.8× 10−6 tα2+2α3
(α2 + 2α3)!+ 4.87× 10−8 tα1+α2+α3
(α1 + α2 + α3)!(4.35)
I(t) = 7 + 0.6983tα3
α3!− 0.1856
t2α3
2α3!− 0.0021
tα1+α3
(α1 + α3)!− 0.1539
t3α3
3α3!−
0.0026tα1+2α3
(α1 + 2α3)!− 0.00031
t2α1+α3
(2α1 + α3)!(4.36)
4.4 Case II for Type 1 Diabetes
Now we study the model for diabetic patient for the period of 10 hours. The model show
that at start time the level of glucose is very high but when we give glucose then his level
of glucose does not fall. After time passing from 250mg/dl it fall only about 275mg/dl [4].
The fractional model after substituting the parameters values for case II.
L {G} =p1
S+
0.017
Sα1L {I(t)} (4.37)

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 51
L {X} =p2
S+
3.9599
Sα2+1− 0.017
Sα2L {X(t)}+
5.3× 10−6
Sα2L {I(t)} (4.38)
L {I} =p3
S+
4.297
Sα3+1− 0.264
Sα3L {I(t)}+
0.0042
Sα3L {G(t)} (4.39)
with initial conditions G(0) = p1 = 240, p2 = X(0) = 0, I(0) = p3 = 15. We computed
first three terms by using the L-ADM for the equations (4.37− 4.39) . We have followings
series solution
G(t) = 240 + 0.255tα1α1!
+ 0.0228tα1+α3
(α1 + α3)!− 0.0193
tα1+2α3
(α1 + 2α3)!, (4.40)
X(t) = 3.9606tα2
α2!− 0.067314
t2α2
(2α2)!+ 6.8× 10−5 tα2+α3
(α2 + α3)!+ 0.0011
t3α2
3α2!
−0.0000039t2α2+α3
(2α2 + α3)!− 0.00006
tα2+2α3
(α2 + 2α3)!, (4.41)
I(t) = 15 + 1.645tα3
α3!− 0.3551
t2α3
2α3!+ 0.2994
t3α3
3α3!+ 0.0011
tα1+α3
(α1 + α3)!+
0.00031tα1+2α3
(α1 + 2α3)!(4.42)
4.5 Numerical Results and Discussion
The analytical solution of fractional order model consist of nonlinear system of fractional
differential equation has been presented by using Laplace Adomian decomposition method.
To observe the effects of the parameter on the dynamics of the fractional-order model
for Case I and Case II, we conclude several numerical simulations varying the value of
parameter given in table 4.1 with time 20 to 40 minutes. These simulations reveals that a
change of the value affects the dynamics of the model . In figures 4.1 and 4.2 clearly shows
the bounded solution according to normal values of glucose level for normal person and

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 52
type 1 diabetes. In figures 4.3 and 4.4 basal values of insulin properly rise and bounded
according to inial conditions and approach to zero when no insulin injected nor produced
in human body. Figure 4.5 represent the insulin concentration in plasma with effect of
glucose level. Figure 4.6 represents no insulin produce in human body caused by type 1
diabetes with passage of time. The system gives the solution at fractional derivative on non
integer values which are more appropriate and accurate values in given domain. Glucose
level increase in figure 4.4 due to cause of type 1 diabetes which control with suitable input
values of insulin to normalize the glucose level.
0 5 10 15 20 2580
85
90
95
100
105
110
115
120Glucose Level measured for normal person
Time (min)
G(t)
Gluc
oaw
Leve
l
Glucose level at α
1= 0.9,α
3= 0.8
Glucose level at α1=α
3=0.75
Glucose level at α1= α
3=0.5
Figure 4.1: Numerical solution of Glucose level of normal person

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 53
0 5 10 15 20 25 30 35 400
50
100
150
200
250
300
350Gluocse Level measured for Type 1 Diabetes person
Time (min)
G(t)
Gluc
ose
Leve
l
Glucose level at α
1= α
3=0.7
Glucose level at α1= α
3=0.8
Glucose level at α1= α
3=0.5
Figure 4.2: Numerical solution of Glucose level of type 1 diabetes
0 5 10 15 20 250
2
4
6
8
10
12
14
16
18
20 Monitoring of insulin basal values for normal person
Time (min)
I(t)I
nsuli
n Le
vel
Insulin level at α
1=α
3=0.15
Insulin level at α1=α
3=0.09
Insulin level at α1=α
3=0.05
Figure 4.3: Behavior of insulin in normal person

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 54
0 5 10 150
5
10
15
20
25
30Monitoring of insulin basal values for Type 1
Time (min)
I(t)
Insu
lin L
evel
Insulin level at α
1=α
3=0.3
Insulin level at α1=α
3=0.6
Insulin level at α1=α
3=0.2
Figure 4.4: Behavior of insulin in type 1 diabetes
0 5 10 15 20 250
5
10
15
20
25
30
35
40Monitoring of Insulin concentration in plasma for normal person
Time (min)
X(t)
Insu
lin co
ncen
tratio
n in
plasm
a
Insulin level at α
1=0.6,α
2=0.4,α
3=0.5
Insulin level at α1=α
2=α
3=0.6
Insuline level at α1=α
2=α
3=0.5
Figure 4.5: Numerical solution of insulin concentration in plasma of normal person

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 55
0 2 4 6 8 100
1
2
3
4
5
6
7
8
9
10Monitoring of Insulin concentration in plasma for Type 1
Time (min)
X(t)
Insu
lin C
once
ntra
tion
in pla
sma
Insulin level at α
2= 0.02α
3=0.1
Insulin level at α2=α
3=0.006
Insulin level at α2=α
3=0.01
Figure 4.6: Numerical solution of insulin concentration in plasma of type 1 diabetes
4.6 Input and Output Stability
Stability is a main anxiety in feedback control design in engineering for automatic control
systems because a feedback control law can stabilize a and also destabilize a system. We use
Lyapunov’s indirect method [33] to examine the system stability (4.1)-(4.3). The system
equilibrium points depends on the steady state of glucose and insulin concentration in
plasma. The blood glucose level has the steady state 100(mg/dl) and the steady state
of insulin in the system (4.1)-(4.3) with the feedback infusion rates and the values of
parameters are given in Tables 4.1 . We find the following equilibrium points by using
Matlab as (83.6417, 151.3288, 9.3857). The linear control system is
x(t) = Ax+B, y(t) = Cx (4.43)
where x = [G, I,X]T B = [0, 0, 1]T and C = [1, 0, 0]. A is the Jacobian matrix at the
equilibrium. We find the following eigenvalues of A by using the MATLAB are as follows

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 56
(−0.0315,−0.0062 + 0.5619i,−0.0062 − 0.5619i), since the eigen values of the system are
negative real parts, it satisfied the inputoutput stability theorem.
4.6.1 Controllability and Observability
The dynamical system has physical properties Controllability and observability and rep-
resents the effect of regulatory system of blood glucose in human. The system (4.43) is
controllable if for any initial state x0 and any desired state xf , there exists a control
of insulin such that x(T ) = xf for some T > 0. The system (4.43) is observable if any
initial state can be uniquely determined by the output Glucose (blood glucose) over (0, T )
for some T > 0. To check the controllability of (4.43), it suffices to examine the rank
of the Kalman controllability matrix [41, 42]. C = [B|AB|A2B]. Here we take the only
measured output of glucose and the only input is insulin. we compute the determinant of
the matrix det(C) = 0.0245. Therefore C has the full rank of 3 and then the system 4.43
is controllable. In the same way, O = [CT |ATCT |(AT )2C] and det(O) = −2.3574e005. We
can have the full rank of 3 and then the system (4.43) is observable. Hence the system is
controllable and observable. For case II type 1 diabetes mellitus, the system is controllable
but not observable.
4.7 Conclusions
In this chapter a theoretical and numerical investigation of the bio-medical glucose insulin
model is presented. It shows the controllability and applicability of the model for the
control of the blood glucose concentration in normal person and T1DM. For the purpose
of automatic artificial pancreas in the glucose regulatory system, we discuss fractional
order glucose insulin model. The model is stable by using the lyapunov equation and
input/output stability is also satisfied for automatic control. Hence the model is stable

CHAPTER 4. FRACTIONAL ORDER GLUCOSE INSULIN MODEL 57
in each case to design the close loop for artificial pancreas. System is controllable and
observable for case 1. For case II, the system is controllable but not observable according
to the given parameters values.
It is important to note that Laplace adomian decomposition method for mathemat-
ical models based on system of fractional order differential equations are more powerful
approach to compute the convergent solutions. The convergence analysis is provided to
demonstrate the efficiency of the method. The model provide the continues glucose mea-
suring in limited time and solutions are bounded in normal values for healthy person and
type 1 diabetes. This is perhaps due to development in the biological approach for the new
model; e.g the hypothesis associated to internal insulin creation through a time dependent
model. Our results show that the fractional-order models can give enhanced turns to the
data than integer-order models in some cases, it is clear that for the satisfactory turns, the
models need additional improvement and insertion of these changes should greatly improve
future models [58].

Chapter 5
Stability Analysis and Control ofGIG System
5.1 Introduction
The goal for treatment of type-1 diabetes mellitus is the development of an artificial pan-
creas to regulate the blood glucose level in the closed loop design. A system of nonlinear
differential equations having five variables (glucose, insulin, β-cell mass, α-cell mass, and
glucagon) with seventeen parameters is considered. The Lyapunov function is used to
check the stability analysis of the model. Controllability and observability of the linearized
model are discussed under two different cases, in case 1 insulin is taken as an input and in
case 2, insulin and glucagon are taken as an input for the system. This played an impor-
tant role in the development of fully automatic artificial pancreas by stabilizing the control
loop system for the glucose-insulin glucagon pump. Proportional Integral Derivative (PID)
controller is designed for an artificial pancreas by using the transfer function. According
to the desire value, the algorithm of an artificial pancreas measures the glucose level in the
blood of a patient by using glucose sensor that sends a signal to an insulin glucagon pump
to adjust the basal insulin. A closed-loop system is tested in Simulink environment and
simulation results show the performance of the designed controller.
58

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 59
5.2 Mathematical Model
The level of blood glucose is mainly controlled by two hormones having opposite effects.
While insulin clears out blood glucose by stimulating its uptake by muscles and adipose
tissues and storing it as glycogen in the liver, glucagon supplies bloodstream by glucose
produced through liver gluconeogensis and glycogenolysis. Consequently, any dysfunction
in the secretion of insulin or glucagon will lead to problems in the control of glycaemia.
Despite the important of glucagon in the control of glycaemia,the literature on glucagon and
α-cells is less important than the available information on insulin and β-cells [43]. Based
on two existing mathematical models by Boutayeb et al. [44] described the dynamics
of glucose, insulin and β-cell mass in presence and absence of genetic predisposition to
diabetes and Ruby Celecte et al. who studied the role of glucagon in the regulation of
blood glucose [45]. A mathematical model considering the dynamics of glucose, insulin ,
β-cells mass, α-cells mass and glucagon. We assumed that the glucagon is released by the
α-cells at low glucose concentrations (Gl = 80mg/dl) in order to stimulate hepatic glucose
production that raises the concentration of glucose in the blood. Where as the insulin is
secreted by the α-cells to reduce the elevation of glucose levels in the blood [46].
dG
dt= a− bG− cIG
αG+ 1+ cjJ (5.1)
dI
dt=
dβG2
e+G2− fI (5.2)
dβ
dt= rβ(1− β
K) (5.3)
dα
dt= rjα(1− α
Kj) (5.4)
dJ
dt= −djα(G−Gt)− fjJ (5.5)
Following is table of parameter’s value used in model

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 60
Parameter value Units Description
a 864 mg/(dId) glucose production rate by liver when G=0
b 1.44 d−1 glucose clearance rate independent of insulin
c 0.85 mI/(mUd) insulin induced glucose production rate
cj 1350 d−1 glucagon induced glucose production rate
d 43.2 mU/(mIdmg) β − cell maximum insulin secretory rate
dj 0.05 1/(mgd) α− cell maximum glucagon secretory rate
e 20000 mg2/dI2 gives inflection point of sigmoid function
f 432 d−1 whole body insulin clearance rate
fj 0.3 d−1 whole body glucagon clearance rate
K 900 mg environmental capacity of β − cell mass
Kj 300 mg inverse of half saturation constant
Gt 80 mg/dI minimum level of glycaemia
r 0.01 mg growth rate of β − cell
rj 0.001 mg growth rate of α− cell
Table 5.1: Table of parameter’s value used in the model
The mathematical model given in [46], after substituting the values of parameter, we get
the following system of equations
dG
dt= 854− 1.44G− 0.85IG
αG+ 1+ 1350J (5.6)
dI
dt=
43.2βG2
20000 +G2− 432I (5.7)
dβ
dt= 0.01β(1− β
900) (5.8)

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 61
dα
dt= 0.001α(1− α
300) (5.9)
dJ
dt= −0.05α(G− 80)− 0.3J (5.10)
For equilibrium point, set left hand side of the system (5.6−5.10) equal to zero; we get
values of the variables (G, I, β, α, J) are P1(600, 0, 0, 0, 0), P2(80, 21, 900, 300, 0.16). The
first point is an unstable point describing a severe hyperglycaemia with zero levels of β-cell
mass and α-cell mass leading to zero levels of insulin and glucagon and hence raising the
level of glucose. The second point is a stable point corresponding to a normal state with
normal values of glucose, insulin, β-cell mass, α-cell mass and glucagon. By using the
Jacobian technique, the linearized model about the stable equilibrium point is
dG
dt= −1.44G− 0.002833I + 0.000198α+ 1350J (5.11)
dI
dt= 178.512G− 432I + 10.4727β (5.12)
dβ
dt= −0.01β (5.13)
dα
dt= −0.001α (5.14)
dJ
dt= −15G− 0.3J (5.15)
5.3 Stability Theorem:
The linear x(t) = Ax(t), where A(t) continuous and bounded for t ≥ t0 , is uniformly
asymptotically stable if and only if given a positive definite real matrix A, there exists a
symmetric positive definite real matrix P , which satisfies
P (t) +AT (t)P (t) + P (t)A(t) = −Q(t), t ≥ t0
The linear time invariant system x(t) = A(t)x(t)the corresponding equation to be used as
ATP + PA+Q = 0 this is called Lyapunov equation [32, 33].

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 62
Here A =
−1.44 −0.002833 0 0.0001983 1350
178.512 −432 10.4727 0 0
0 0 −0.01 0 0
0 0 0 −0.001 0
−15 0 0 0 −0.3
and Q = I5×5 By using this Lyapunov equation ATP + PA+Q = 0 on matlab, we get
P =
26.1330 9.7451 −5.25664× 10−7 1.4737536× 10−5 0.0275
9.7451 4.0574 1.2121 6.089863× 10−6 −0.3268
−5.25664× 10−7 1.2121 50.0000 0 2.5435368× 10−5
1.4737536× 10−5 6.089863× 10−6 0 500.0000 −0.0001
0.0275 −0.3268 2.5435368× 10−4 −0.0001 0.2904
The eigen values of P are (0.0012, 0.6342, 29.8105, 50.0350, 500.0000) and which shows
that P is symmetric positive definite real matrix P. Hence prove that the system is
uniformly asymptotically stable. Similarly at point (600,0,0,0,0), eigne values of A, is
(−1.44,−4320.0100,−0.300, 0.001) so, system is not stable at that point.
5.4 Linear Control System
A linear control system is
x(t) = Ax(t) +Bu(t), y(t) = Cx(t) (5.16)
5.4.1 Controllability and Observability
We have two cases, for case I: Insulin as the input only and glucose as an output and in
case II: insulin and glucagon as an input and glucose as output only.

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 63
Case1: Here we take the only measured output of glucose and the only input is insulin
then
B = [0, 1, 0, 0, 0]T C = [1, 0, 0, 0, 0]
where
A =
−1.44 −0.002833 0 0.0001983 1350
178.512 −432 10.4727 0 0
0 0 −0.01 0 0
0 0 0 −0.001 0
−15 0 0 0 −0.3
The controllability matrix is
R = [B; AB; A2B; A3B; A4B]
rank(R) = rank([B; AB; A2B; A3B; A4B]) = 2
The observability matrix is
O = [C; CA; CA2; CA3; CA4]
rank(O) = rank([C; CA; CA2; CA3; CA4]) = 5
Hence the system is observable but not controllable. Figures 5.1 and 5.2 represent the
controllable and observable state at the equilibrium point and for different initial conditions
on the state variable values, when insulin is an input and the glucose level for that state
system is observable but not controllable. Note that our given requirements are not met,
specifically, the steady-state error is much too large.

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 64
Figure 5.1: Controllable and observable state of model, when insulin is an input at
initial condition (80,21,900, 300,0.16)
Figure 5.2: Controllable and observable steady state of model, when insulin is an
input at initial condition (120,10,5, 3,0.1)

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 65
For Case 2:Here we take the only measured output of glucose and the only input is
insulin and α− cellthen
B = [0, 1, 0, 1, 0]T C = [1, 0, 0, 0, 0]
where
A =
−1.44 −510 0 0 1350
0 −432 40.926 0 0
0 0 0.01 0 0
0 0 0 0.001 0
0 0 0 4 −0.3
The controllability matrix is
R = [B; AB; A2B; A3B; A4B]
rank(R) = rank([B; AB; A2B; A3B; A4B]) = 4
The observability matrix is
O = [C; CA; CA2; CA3; CA4]
rank(O) = rank([C; CA; CA2; CA3; CA4]) = 5
The rank of controllability matrix and observability matrix is 4 and 5 respectively. Hence
the system is observable but not controllable. Figures 5.3 and 5.4 represents the controllable
and observable state with different initial conditions of state variables, when glucagon is
an input with insulin its form close loop to stabilize the glucose level.

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 66
Figure 5.3: Controllable and observable state of model, when insulin and glucagon
are an input at initial condition (120,21,900, 300,0)
Figure 5.4: Controllable and observable state of model, when insulin and glucagon
are an input at initial condition (80,0,900, 300,0.16)

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 67
5.5 Controller Design
Tracking step reference signal with zero steady state error is possible if and only if loop
transfer function contain one transfer function contains at least one integral. Figure 5.5
represents the simulink constructed on linear model (5.11− 5.15), which shows the contin-
uous measuring of glucose, insulin and glucagon with effect of β-cell, α-cell mass. Glucose,
insulin and glucagon show the positive behaviour in measurement on its approaching val-
ues.
Figure 5.5: Simulink to measure Glucose, insulin and glucagon with effect of β-cell,
α-cell mass
The transfer function can be determined by the system identification in the MATLAB

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 68
after importing these signals into identifying the Graphical User Interface (GUI) in the
MATLAB workspace. Also, the design control for this transfer function will be easy and
accurate. S−function in this paper shows artificial pancreas [47, 48]. The transfer function
of this linear system thus will be a rational function
G(s) =c(s)
d(s)
where
c(s) = c0sn + c1s
n−1 + ...+ cn−1s+ cn
and
d(s) = sn + d1sn−1 + ...+ dn−1s+ dn
are polynomials function. In facts we obtain results for control system
x(s) = (sI −A)−1(B(u(s) + x0))
y(s) = C(sI −A)−1Bu(s) + C(sI −A)−1x0) +Du(s)
where matrix
G(s) = C(sI −A)−1B +D
is the system of transfer matrix. We have used MATLAB symbolic math toolbox, following
transfer functions are obtained, when insulin is input only We have
G(s) =−1.705e−13s2 − 0.04045s− 0.01213
s3 + 433.6s2 − 1.954e4s− 8.748e6
continuous-time transfer function. When insulin and glucagon are input
G1(s) =1.705e−13s2 + 1350s+ 5.832e5
s3 + 433.6s2 − 1.954e4s− 8.748e6
continuous-time transfer function. Pole-zero diagram of these transfer functions and fre-
quency response are shown in Figures 5.6 and 5.7 for open loop.

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 69
Figure 5.6: Pole zero diagram of transfer function G(s)
Figure 5.7: Frequency response transfer function G(s)

CHAPTER 5. STABILITY ANALYSIS AND CONTROL OF GIG SYSTEM 70
5.6 Conclusions
The obtained results will have some impact on attempts to construct an artificial pancreas.
Until now primarily one tries to implement a feedback control by taking glucose as the only
input providing information on the system state and by using administration of insulin as
the only control input. The use of insulin as the only control input may be insufficient
in case of hypoglycemia because a low glucose level cannot be raised by insulin action.
It seems to be that in order to restore the desired glucose level that one has to include
administration of glucagon as another control input. For instance, in this model, we can
see that the system improves its controllability when we consider glucagon as second input
along with insulin. In our opinion, one has to develop models for the glucose-insulin-
glucagon system which pay special attention to the control mechanisms of the systems
first for the health system in order to understand the working of the control loops in the
health system which should be restored by the artificial pancreas. Our results indicate
that such a feedback control will have to use administration of insulin and glucagon by
a combined insulin-glucagon pump. An algorithm for an artificial pancreas in simulink
and used the transfer function of the model for Proportional-Integral-Derivative (PID)
controller is designed. Controllability and observability of linear system are discussed for
this purpose. The system is not controllable but observable for case 1 and 2. When we
considered a glucagon as input with insulin rank of controllability matrix is improved and
its rank is 4. Only one variable is not controllable. To overcome that problem we discussed
the state of the model where the model is completely controllable. A control system can
only be used in the form of closed-loop control to stabilize the system [49].

Chapter 6
Sorenson Model for Type 1Diabetes Mellitus
In this chapter, convert the Sorenson’s model for T1DM because this is the most compre-
hensive model in the Glucose Insulin Glucagon dynamics for human but the result show
that this model has some deficiency in original model since the equilibrium point is not in
feasible region. We treated Sorensen’s Model for T1DM to check the linear controllability
and observability.
6.1 Sorensen’s Model For Type 1 Diabetes
The physiological compartments of the human body are classified in six category: brain,
heart, periphery, gut, liver and kidney. Arrows joining the physiological compartments
represent the direction of blood flow. The heart and lungs compartment serves to close
the circulatory loop, representing simply the blood volume of the cardiopulmonary system
and the major arteries. Figure 6.1, which represents the mass balance of 8 ODE’s in
each compartment results with linear and nonlinear terms that are related to each specific
metabolic rate. In Insulin model, the mass balance in each compartment results in 7 ODE’s
with linear and nonlinear terms represents in figure 6.2, which are related to each specific
71

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 72
metabolic rate and glucagon mode is 1 ODE with linear and nonlinear terms, which are
related to each specific metabolic rate represents in figure 6.3.
Figure 6.1: Schematic representation of the Glucose Model
Figure 6.2: Schematic representation of the Insulin Model

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 73
Figure 6.3: Schematic representation of the Glucagon Model
Followings are the equations of the model
V GBV GBV = QGB(GH −GBV )− VBI
TB(GBV −GBI) (6.1)
VBIGBI =VBITB
(GBV −GBI)− rBGU (6.2)
V HG GH = QGBGBV +QGLGL +QGKGK +QGPGPV +QGHGH − rRBGU (6.3)
V GG GG = QGG(GH −GG)− rGGU (6.4)
V GL GL = QGAGH +QGGGG −QGLGL + rHGP − rHGU (6.5)
V GK GK = QGK(GH −GK)− rKGE (6.6)
V GPV GPV = QGP (GH −GPV )− VPI
TGP(GPV −GPI) (6.7)
VPIGPI =VPITGP
(GPV −GPI)− rPGU (6.8)

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 74
V IB IB = QIB(IH − IB) (6.9)
V IH IH = QIBIB +QILIL +QIKIK +QIP IPV +QIHIH (6.10)
V IGIG = QIG(IH − IG) (6.11)
V IL IL = QIAIH +QIGIG −QILIL − rPIR − rLIC (6.12)
V IK IK = QIK(IH − IK)− rKIC (6.13)
V IPV IPV = QIP (IH − IPV )− VPI
T IP(IPV − IPI) (6.14)
VPI IPI =VPIT IP
(IPV − IPI)− rPIC (6.15)
V ΓΓ = rPΓR − rPΓC (6.16)
6.1.1 Description of Variables
G Glucose concentration (mg/dl) T Diffusion rate (min)
Q Vascular Plasma flow rate (dl/min) V Volume (dl)
r Metabolic source and sink rate (mg/min) M Multiplier of basal MR
τ Time constant (min) I Insulin concentration (mg/dl)
F Fractional clearance (dimensionless) t Time constant (min)
Γ Glucagon concentration (pg/ml) B Brain
Table 6.1: Description of variables

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 75
6.1.2 First Subscript: Physiological Compartment
G Gut H Heart and Lung
L Liver K Kidney
P Periphery A Hepatic artery
G Glucose I Insulin
Γ Glucagon B Basal value
I Interstitial fluid space V Vascular plasma space
N Normalized value B Brain
Table 6.2: Physiological Compartment
6.1.3 Second Subscript: Physiological Compartment
BGU Brain glucose uptake GGU Gut glucose utilization
HGP Hepatic glucose production HGU Hepatic glucose uptake
KGE Kidney glucose excretion PGU Peripheral glucose uptake
RBCU Red blood cell glucose uptake KIC Kidney Insulin clearance
LIC Liver insulin clearance PIR Peripheral insulin release
PIC Peripheral insulin clearance PΓC Plasma glucagon clearance
MΓC Metabolic glucagon clearance PΓR Pancreatic glucagon release
Table 6.3: Physiological Compartment
Following is the table of parameter’s and constant values given in [50, 13] used in model

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 76
Table 6.4: Table of parameter’s and constant value of the model
Parameter Value Parameter Value
QGR 5.9dlmin−1 QG
H 43.7dlmin−1
QGA 2.5dlmin−1 QG
L 12.6dlmin−1
QGG 10.1dlmin−1 QG
K 10.1dlmin−1
QGP 15.1dlmin−1 QG
BV 3.5dl
V GH 13.8dl V G
L 25.1dl
V GG 11.2dl V G
K 6.6dl
V GPV 10.4dl VPI 67.7dl
VBI 4.5dl TGP 5.0min
TR 2.1min V Γ 11310ml
V IB 0.26l QI
A 0.18l/min
T IP 20min V IH 0.99l
QIR 0.45l/min V I
G 0.94l
QIH 3.12l/min V I
L 1.14l
QII 0.90l/min V I
K 0.51l
QIK 0.72l/min V I
PV 0.74l/min
V IPI 6.74l V I
G 0.72min−1
QIP 1.05l/min α 0.00482min−1
β 0.931lmin−1 K 0.00794min−1
M1 0.00747l/min M2 0.0958U
γ 0.575l/min Q0 6.33dlmin−1
6.1.4 Metabolic source and sink
rBGU = 70mg/min(Constant), rRBCU = 10mg/min(Constant),
rGGU = 20mg/min(Constant), rPGU = M IPGUM
GPGUτ
BPGU ,

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 77
τBPGU = 35mg/min, τBHGP = 155mg/min, τΓ = 65min, FLIC = 0.40, FKIC = 0.30,
FPIC = 0.415, rBPIR = 4mU/min, rMΓC = 9.10,MGPGU = GNPI
M IPGU = 7.03 + 6.52tanh[0.338(INPI − 5.82)]
rHGP = M IHGPM
ΓHGPM
GHGP τ
BHGP
M IHGP =
1
τI(M I∞
HGP −MIHGP ) (6.17)
M I∞HGP = 1.21− 1.14tanh[0.62(GLN − 0.89)]
MΓHGP = MΓ0
HGP − f2
MΓ0HGP = 2.7tanh[0.39ΓN ]
f2 =1
τΓ[(MΓ0HGP − 1
2)− f2] (6.18)
MGHGP = 1.42− 1.41tanh[1.66(INL − 0.497)]
rHGU = M IHGUM
GHGUτ
BHGU
τBHGU = 20mg/min
M IHGU =
1
τI[M I∞
GHU −MIGHU ] (6.19)
M I∞HGU = 2.0tanh[0.55INL ]

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 78
MGHGU = 5.66 + 5.66tanh[2.44(GNL )− 1.48]
rKGE = {71 + 71tanh[0.11(GK − 460)], 0 < GK < 460mg/min
−330 + 0.83GK , GK > 460mg/min
rLIC = FLIC [QIAIH +QIGIG + rPIR]
rKIC = FKIC [QIKIK ]
rPIC =IIP
[(1−FPICFPIC
)( 1QI
P
− T IP
VPI)]
rPIR =S(GH)
S(GBH)rBPIR
P = α[P∞ − P ] (6.20)
I = β[X − I] (6.21)
Q = K[Q−Q0] + [γP − S] (6.22)
S = [M1Y +M2(X − I)0+]Q
S =(GH)3.27
(132)3.27 + 5.93(GH)3.02
P∞ = Y = (X)1.11
rPΓC = rMΓCΓ
rPΓR = MGPΓRM
IPΓRτ
BPΓR
τBPΓR = rMTCΓB
MGPΓR = 2.93− 2.10tanh[4.18(GNH − 0.61)]
M IPΓR = 1.31− 0.61tanh[1.06(INH − 0.47)][6]

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 79
6.2 Modified Form of Model in Type 1 Diabetes
Mellitus
In this section model (6.1− 6.22), convert Sorenson’s model into Type 1 Diabetes Mellitus
[51]. The nomenclature, basal values, parameters values and metabolic rates are same like
non diabetic model. After eliminating pancreatic insulin released model and rPIR due to
type 1 diabetes mellitus and substitution of parameters and basal values given in table 6.1,
the model ends up 19 ordinary differential equations and takes the form
GBV = 1.685GH − 2.297GBV + 0.612GBI (6.23)
GBI = 0.476GBV − 0.476GBI − 15.555 (6.24)
GH = 0.427GBV + 0.913GL + 0.731GK + 1.094GPV − 3.166GH − 0.724 (6.25)
GBI = 0.901(GH −GG)− 1.785 (6.26)
GL = 0.099GH + 0.402GG − 0.501GL + 6.175M IHGP (2.7tanh(0.389Γ)− f2) (6.27)
(1.42− 141tanh((0.006GL − 0.31))− 4.5M IHGU (1 + tanh(0.024GL − 3.61)))
GK = 1.53GH − 1.53GK − 10.721− 10.721(0.11GK − 50.6) (6.28)
GPV = 1.451GH − 2.748GPV + 1.296GPI (6.29)
GPI = 0.2GPV − 0.2GPI − 0.005GPI(7.03 + 6.52tanh(0.015IPI − 1.967)) (6.30)
M IHGP = −0.04M I
HGP + 0.048− 0.045tanh(0.077IL − 1.477) (6.31)

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 80
M IHGU = −0.04M I
HGU + 0.08tanh(0.025IL) (6.32)
f2 = −0.015f2 − 0.007 + 0.02tanh(0.389Γ) (6.33)
IB = 1.73IH − 1.73IB (6.34)
IB = 0.454IB + 0.909IL + 0.727IK + 1.06IPV − 3.151IH (6.35)
IG = 0.765IH − 0.765IG (6.36)
IL = 0.094 + 0.378IG − 0.789IL (6.37)
IK = 1.411IH − 1.835IK (6.38)
IPV = 1.418IH − 1.874IPV + 0.455IPI (6.39)
IPI = 0.05IPV − 0.111IPI (6.40)
Γ = −0.08Γ + 0.08(2.93− 2.10tanh(0.041GH − 2.55))
(1.31− 0.61tanh(1.31− 0.61tanh(0.049IH − 0.429) (6.41)
For equilibrium the left hand side of the equations (6.23− 6.41) are substituted zero. By
algebraic manipulations we can represent all the equations as a function of either GK or IB
separately. The model represent a type 1 diabetes mellitus subject so it is not surprising to
take insulin concentration in all compartments zero. The equation for kidney compartment
provides GK = 197.10mg/d1. The uniqueness of values provide in [52]. Hence we get a
unique point of equilibrium for the Sorenson Model in type 1 diabetes mellitus.
(185.2, 152.5, 197.1, 195.1, 207.7, 197.1, 193.6, 189.9, 2.33, 0, 0.1, 0, 0, 0, 0, 0, 0, 0, 1.3).

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 81
6.2.1 Linearised Model
Linearized model is given as
GBV = 1.685GH − 2.297GBV + 0.612GBI
GBI = 0.476GBV − 0.476GBI
GH = 0.427GBV + 0.913GL + 0.731GK + 1.094GPV − 3.166GH
GBI = 0.901(GH −GG)
GL = 0.099GH + 0.402GG − 0.563GL + 2.755M IHGP − 8.467M I
HGU − 5.299f2 + 4.354Γ
GK = 1.53GH − 1.53GK
GPV = 1.451GH − 2.748GPV + 1.296GPI
GPI = 0.2GPV − 0.204GPI − 0.007IPI
M IHGP = −0.04M I
HGP + 0.007IL
M IHGU = −0.04M I
HGU + 0.002IL
f2 = −0.015f2 − 0.006Γ
IB = 1.73IH − 1.73IB
IB = 0.454IB + 0.909IL + 0.727IK + 1.06IPV − 3.151IH

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 82
IG = 0.765IH − 0.765IG
IL = 0.094IH + 0.378IG − 0.789IL
IK = 1.411IH − 1.835IK
IPV = 1.411IH − 1.874IPV + 0.455IPI
IPI = 0.05IPV − 0.111IPI
Γ = −0.08Γ + 0.0016IH − 0.00000069GH
6.2.2 Stability Analysis
The linear x(t) = A(t)x(t), where A(t) continuous and bounded for t ≥ t0, is uniformly
asymptotically stable if and only if given a positive definite real matrix A(t), there exists a
symmetric positive definite real matrix P (t), which satisfies P (t)+Aτ (t)P (t)+P (t)A(t) =
−Q(t),t ≥ t0. The linear time invariant system x(t) = A(t)x(t) the corresponding equation
to be used as AτP + PA+Q = 0. This is called Lyapunov equation [32, 33].
Here A is matrix of coefficients of above linearized model and Q = I, where I is an
identity matrix with the same order of A. By using the equation AτP + PA + Q = 0 on
Matlab. We find matrix P and its det(P ) = 4.8878e11 which shows that P is symmetric
positive definite real matrix P . The eigen values of A are
(-4.6799,-2.5946,-2.0129,-1.0195 + 0.3193i,-1.0195 - 0.3193i,-0.3518,-0.1949, -0.0118,-
0.0152,-0.0800,-0.0400,-4.4302,-1.7618,-1.8580,-0.9559 + 0.3134,-0.9559 - 0.3134i,-0.2154,-
0.0779,-0.0400) negative real roots. Hence prove that the system is uniformly asymptoti-
cally stable.

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 83
6.3 Results and Discussions
Achieving and maintaining normal blood glucose concentrations are critical issues for suc-
cessful long term care of patients with diabetes mellitus. Serious attention is needed to
maintain blood glucose level as close to the nondiabetic range as possible in individuals
with T1DM to reduce the development and progression of micro-vascular and cardiovascu-
lar complications. Till now we don’t have a fully automated artificial pancreas. An effort
is made to answer the hurdles of having a fully automated artificial pancreas, since we need
to have a feedback control for the system. First step in this direction is to check if we can
stabilize the system by choosing an appropriate feedback control.
A mathematically linear control system is given by the following two equations
x = Ax+Bu,
y = Cx,
Here x = [GBV GBI GH GG GL GK GPV GPI MIHGP M
IHGU F2 IB IB IH IL IK IPV IPI Γ]τ
and B = [0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0] and C = [0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0].
The n × np controllability matrix is given by R = [B,AB,A2B,A3B, ..., An−1B]. The
rank(i.e. rank(R)=n), so the system is said to be controllable. The nk×np the observability
matrix is given by O = [C,ACA;CA2;CAn − 1]τ . The rank (i.e. rank(R)=n) , so the
system is said to be observable [13, 21, 53].
6.3.1 Case I:
If we consider the insulin concentration in periphery vascular blood space as in-
puts and glucose concentration in extracellular fluid as the only output than B =
[0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0] and C = [0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0]. R is
the controllability matrix, where R = [B,AB,A2B,A3B, ..., A18B] and its rank is 12. The

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 84
observability matrix is O = [C,CA;CA2;CA3;CA4, ..., CA18] and its rank is 11. Hence
the linear system is neither controllable nor observable.
6.3.2 Case II:
If we consider the insulin concentration in periphery vascular blood space and glucagon
concentration as inputs and glucagon concentration in extracellular fluid as the only output
than B = [0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0] and C = [0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0].
In this case rank of controllability and observability matrix is 13 and 11 respectively.
Stability analysis of A is checked by using Lyapunov equation and found that the system
is stable because P is definite positive matrix and eigen values of A are negative real roots.
So the system is uniformly asymptotically stable. Two cases are discussed according to
input value, for case 1, insulin is an input only and glucose is output. For case 2, insulin
and glucagon are input and glucose as an output only.
6.4 Conclusion
The results obtained in this paper will have some impact on attempts to construct the
artificial pancreas. Until now primarily one tries to implement a feedback control by
taking glucose as the only input providing information on the system state and by using
administration of insulin as the only control input. The use of insulin as the only control
input may be insufficient in case of hypoglycemia, because a low glucose level cannot be
raised by insulin action. In our opinion one has to develop models for the glucose-insulin-
glucagon system which pay special attention to the control mechanisms of the systems
first for the healthy system in order to understand the working of the control loops in the
healthy system which should be restored by the artificial pancreas. Our results indicate
that such a feedback control will have to use administration of insulin and glucagon by a

CHAPTER 6. SORENSON MODEL FOR TYPE 1 DIABETES MELLITUS 85
combined insulin-glucagon pump.
The system is uniformly asymptotically stable by using the Lyapunov equation because
eigen values of A are all negative real roots. We treat the linear system because if a
linear system is controllable and observable, then a nonlinear system may or may not be
controllable and observable. If a nonlinear system is neither controllable nor observable
then linear may or may not be. This is the most comprehensive model in the history of
Glucose Insulin Glucagon systems. Results show that the deficiency of the model can be
improved if glucagon is used as input along with insulin. For this purpose, we check the
controllability and observability of the system which further can be treated to design the
feedback control for fully automatic artificial pancreas. It was concluded that controllability
and observability is improved by considering glucagon as another input since glucagon plays
an important role in glucose regulatory systems. The system is neither controllable nor
observable in both cases. The situation is improved when we consider insulin and glucagon
as inputs than only insulin but still system is not controllable and observable thus we
cannot design the feedback control for fully automatic artificial pancreas.
The discussion in the conclusion show that the following tasks should be considered for
future research. Development and validation of a comprehensive model for the system
including the important control mechanisms involving insulin and glucagon for the healthy
system [54].

Chapter 7
Control of Composite Model
Man may be the captain of his fate, but he is also
the victim of his blood sugar.(Wilfrid Oakley)
Artificial pancreas is one of the solutions to control the type1 diabetes mellitus now a day.
Effort is being made to develop the desired artificial pancreas for this purpose. Article
presents the controllability and observability of the glucose insulin glucagon dynamical
model which is the modified form of composite model of glucose insulin glucagon dynam-
ics for type 1 diabetes mellitus. The concept of controllability and observability for the
linearized control system of human glucose insulin systems is used so that we can have
a feedback control. This model completely describes the glucagon effect in the safety of
artificial pancreas to overcome the risk of hyperglycemia. Composite model of glucagon-
glucose dynamics and its extension is treated for type 1 diabetes mellitus to check the
linear controllability and observability. Two cases discussed in system according to the
input. For case I, insulin as the input only and glucose as an output and in case II insulin
and glucagon as an input and glucose as output only.
86

CHAPTER 7. CONTROL OF COMPOSITE MODEL 87
7.1 Material and Method
7.1.1 Composite Model Glucagon-Glucose Dynamics
Consider the composite model having combined form of minimal model, Hovorka model
and glucagon sub model. Figure 7.1 graphically shows the structure of proposed glucagon-
extended minimal model in composite model [55].
Figure 7.1: The glucagon extended Minimal model
Pharmacodynamics on the net endogenous glucose production, insulin absorption
model to add the effects of subcutaneous glucagon, insulin delivery on plasma insulin
and glucagon concentration is described in glucagon glucose composite model. The model
describe in following equations
G(t) = −[SG +X(t)− Y (t)]G(t) + SGGb +RaV
(7.1)

CHAPTER 7. CONTROL OF COMPOSITE MODEL 88
Y (t) = −p3Y (t) + p3SN [N(t)−Nb] (7.2)
X(t) = −p2X(t) + p2S1[I(t)− Ib] (7.3)
F (t) =1
tmaxG(−F (t) +AGDG) (7.4)
Ra(t) =1
tmaxG(−Ra(t) + F (t)) (7.5)
I(t) = −keI(t) +S2(t)
V1tmax1(7.6)
S1(t) = u(t)− S1(t)
tmax1(7.7)
S2(t) =S1(t)− S2(t)
tmax1(7.8)
N(t) = −kNN(t) +Z2(t)
VN tmaxN(7.9)
Z1(t) = w(t)− Z2(t)
tmaxN(7.10)
Z2(t) =Z1(t)− Z2(t)
tmaxN(7.11)
Where G, I,N,X and Y represents the plasma glucose concentration, plasma insulin
and plasma glucagon concentration, insulin and glucagon action on glucose production
respectively with time t. Where P3 = k8 , SN = k7/k8k9 are constant parameters
in the model. Where Ra and F are the plasma appearance of glucose and glucose
appearance in the first compartment respectively. Where V is measure as the glucose
distribution volume (dI/kg). ke, u1(t), VI and tmaxI represent the insulin clearance in

CHAPTER 7. CONTROL OF COMPOSITE MODEL 89
the plasma, subcutaneous insulin infusion rate, the distribution volume of plasma insulin
and absorption time constant of insulin. S1 and S2 represents the two compartments
subcutaneously administrated insulin. Where KN is the first order decay for glucagon
in plasma, w is glucagon infusion rate, VN is the distribution volume of plasma, Z1 and
Z2 are two-compartment resented absorption of subcutaneously administered glucagon [55].
The data is classified into three subjects 117-1, 126-1, and 128-1 according to different
parameters values in each case. In each subject we have two cases, for case I: Insulin as the
input only and glucose as an output and in case II: insulin and glucagon as an input and
glucose as output only. The only measured output is concentration of glucose in plasma
that we can easily measure. The system is neither controllable nor observable in both
cases for every subject. But the rank of the matrix is improved in each subject when we
consider insulin and glucagon as inputs than only insulin but still system is not controllable
and observable thus we cannot design the feedback control for fully automatic artificial
pancreas. Now considering the modified form of that composite model for controllability
and observability of the model for artificial pancreas.
7.2 Extended Form of Composite Model
The glucose kinetics is described by a system of differential equation in the form
G(t) = −[SG +X(t)− Y (t)]G(t) + SGGb +D2(t)
tmaxGV(7.12)
X(t) = −p2X(t) + p2SI [I(t)− Ib] (7.13)
Y (t) = −p3Y (t) + p3SN [N(t)−Nb] (7.14)

CHAPTER 7. CONTROL OF COMPOSITE MODEL 90
Where G, I,N,X and Y represent the plasma glucose concentration, plasma insulin
and plasma glucagon concentration, insulin and glucagon action on glucose production
respectively with time t. SG represents the fractional glucose effectiveness, SI and SN are
insulin and glucagon sensitivities. p2, p3 are the constant parameters describing the insulin
and glucagon action. Ib and Nb are basal values of insulin and glucagon. V is the volume
of glucose distribution and tmaxG rate appearance in glucose plasma [56].
7.2.1 Gastrointestinal Absorption Model
The glucose rate of appearance into systematic circulation after meal is described by gas-
trointestinal absorption model as well as glucagon extended minimal model [57]. The
equation representing such a model is
D1(t) =1
tmaxG(−D1(t) +AGDG) (7.15)
D2(t) =1
tmaxG(−D2(t) +D1(t)) (7.16)
Where D1(t) and D2(t) represent the first and second compartment of glucose. AG
and DG show the carbohydrate bioavailability and intake of carbohydrates per kg of body
weight respectively.
7.2.2 Subcutaneous Insulin Absorption Model
The equations of such a model are
I(t) = −keI(t) +S2(t)
V1tmaxI(7.17)
S1(t) = u1(t)− S1(t)
VItmaxI(7.18)

CHAPTER 7. CONTROL OF COMPOSITE MODEL 91
S2(t) =S1(t)− S2(t)
VItmaxI(7.19)
Where ke represent the insulin clearance in the plasma, u1(t) is subcutaneous insulin
infusion rate, VI describes the distribution volume of plasma insulin and tmaxI absorption
time constant of insulin. S1 and S2 represents the two compartments subcutaneously
administrated insulin [56].
7.2.3 Subcutaneous Glucagon Absorption Model
Pharmacokinetics of subcutaneous glucagon absorption has same structure as Hovarka and
coauthors proposed in the subcutaneous insulin absorption. Plasma glucagon concentration
N was estimated as
N(t) = −kNN(t) +Z2(t)
VN tmaxN(7.20)
Z1(t) = u2(t)− Z1(t)
tmaxN(7.21)
Z2(t) =Z1(t)− Z2(t)
tmaxN(7.22)
Where KN is the first order decay for glucagon in plasma, u2 is glucagon infusion
rate, VN is the distribution volume of plasma, Z1 and Z2 are two-compartment resented
absorption of subcutaneously administered glucagon [55]. Hence the model takes the form
in the following equations
G(t) = −[SG +X(t)− Y (t)]G(t) + SGGb +D2(t)
tmaxGV(7.23)
X(t) = −p2X(t) + p2SI [I(t)− Ib] (7.24)
Y (t) = −p3Y (t) + p3SN [N(t)−Nb] (7.25)

CHAPTER 7. CONTROL OF COMPOSITE MODEL 92
D1(t) =1
tmaxG(−D1(t) +AGDG) (7.26)
D2(t) =1
tmaxG(−D2(t) +D1(t)) (7.27)
I(t) = −keI(t) +S2(t)
V1tmaxI(7.28)
S1(t) = u1(t)− S1(t)
VItmaxI(7.29)
S2(t) =S1(t)− S2(t)
VItmaxI(7.30)
N(t) = −kNN(t) +Z2(t)
VN tmaxN(7.31)
Z1(t) = u2(t)− Z1(t)
tmaxN(7.32)
Z2(t) =Z1(t)− Z2(t)
tmaxN(7.33)
This is the table of parameters use in each subject data for close loop artificial pancreas
are given in [56, 55].
Table 7.1: Table of parameters and constant value of the model
Parameter Value Parameter Value
Ke 0.1381/min VI 0.12ml/kg
p2 0.0283441/min SN 0.02179min−1/pg/ml
tmaxI 55Min p3 0.000051/min
Ib 11.01U/ml tmaxG 69.6Min
KN 0.621/min u2(t) 70ng/kg
VN 16.06ml/kg u1(t) 4U/kg
tmaxN 32.46Min DG 20Mg
Nb 46.30pg/ml AG 0.8unitless
SI 6.40e−4min− 1/U/ml V 1.7dl/kg
Gb 100mg/dl SG 0.0141/min

CHAPTER 7. CONTROL OF COMPOSITE MODEL 93
After Substitution Parameter value, we have
G(t) = −0.0896G− 6.4XG+ 6.4Y G+D2 + 8.96 (7.34)
X(t) = −0.028344X + 0.003324I − 0.036589 (7.35)
Y (t) = −0.00005Y + 1.0895× 10−7N − 5.044385× 10−5 (7.36)
D1(t) =1
69.6(−D1 + 16) (7.37)
D2(t) =1
69.6(−D2(t) +D1) (7.38)
I(t) = −0.138I +S2
6.6(7.39)
S1(t) = 4− S1
55(7.40)
S2(t) =S1 − S2
55(7.41)
N(t) = −0.62N +Z2
520.0092(7.42)
Z1(t) = 70− Z1
32.46(7.43)
Z2(t) =Z1 − Z2
32.46(7.44)
For equilibrium points are in the above system (7.34− 7.44) put L.H.S. equal to zero
G(t) = X(t) = Y (t) = D1(t) = D2(t) = I(t) = S1(t) = S2(t) = N(t) = Z1(t) = Z2(t) = 0
By using the Mathematica software tools find the equilibrium points. Hence the equilibrium
point is
(G,X, Y,D1, D2, I, S1, S2, Z1, Z2, N) = (0.1398, 27.0273,−0.855691, 16, 16,
241.546, 220, 220, 2272.2, 2272.24, 7.0301)
In equilibrium point glucose, insulin and glucagon are concentrations in plasma are positive,
so the system is stable and feasible for controllability and observability.

CHAPTER 7. CONTROL OF COMPOSITE MODEL 94
7.2.4 Linearized System
The linearized system about equilibrium point is
G(t) = −178.5407G− 0.89472X + 0.8947Y +D2
X(t) = −0.028344X + 0.003324I
Y (t) = −0.00005Y + 1.0895× 10−7N−
D1(t) =D1
69.6
D2(t) =1
69.6(−D2(t) +D1)
I(t) = −0.138I +S2
6.6
S1(t) = −S1
55
S2(t) =S1 − S2
55
N(t) = −0.62N +Z2
520.0092
Z1(t) = − Z1
32.46
Z2(t) =Z1 − Z2
32.46
7.3 Stability Analysis
Theorem 7.1: The linear x(t) = Ax, where A continuous and bounded for t ≥ t0 , is
uniformly asymptotically stable if and only if given a positive definite real matrix A, there
exists a symmetric positive definite real matrix P (t), which satisfies
P (t) +AT (t)P (t) + P (t)A(t) = −Q(t), t ≥ t0
The linear time invariant system x(t) = Ax the corresponding equation to be used as
ATP + PA+Q = 0 this is called Lyapunov equation [32, 33].

CHAPTER 7. CONTROL OF COMPOSITE MODEL 95
Proof:
Here A =
178.58 −0.8947 0.8972 0 1 0 0 0 0 0 0
0 −0.028 0 0 0 0.0033 0 0 0 0 0
0 0 .00005 0 0 0 0 0 1.089× 10−7 0 0
0 0 0 −0.014 0 0 0 0 0 0 0
0 0 0 0.014 −0.0144 0 0 0 0 0 0
0 0 0 0 0 −0.138 0 0.1515 0 0 0
0 0 0 0 0 0 −0.0181 0 0 0 0
0 0 0 0 0 0 0.0181 −0.0181 0 0 0
0 0 0 0 0 0 0 0 −0.62 0 0.00192
0 0 0 0 0 0 0 0 0 −0.0308 0
0 0 0 0 0 0 0 0 0 0.0308 −0.0308
coefficients of above linearized model and Q = I, where I is an identity ma-
trix with the same order of A. By using the equation ATP + PA + Q = 0
on Matlab, compute matrix P and det(P ) = 1.4221e10 which shows that
P is symmetric positive definite real matrix. The eigen values of A are
(−178.5400,−0.0283,−0.0001,−0.1430,−0.1430,−0.1380,−0.0181,−0.0181,−0.6200,−0.0308,−0.0308)
negative real roots. Hence prove that the system is uniformly asymptotically stable.
7.4 Linear Control
7.4.1 Results and Discussion
Achieving and maintaining normal blood glucose concentrations are critical issues for
successful long term care of patients with diabetes mellitus. Serious attention is needed to
maintain blood glucose level as close to the non-diabetic range as possible in individuals
with type 1 diabetes mellitus to reduce the development and progression of micro-vascular
and cardiovascular complications. Till now we don’t have a fully automated artificial

CHAPTER 7. CONTROL OF COMPOSITE MODEL 96
pancreas. An effort is made to answer the hurdles of having a fully automated artificial
pancreas, since we need to have a feedback control for the system. First step in this
direction is to check if we can stabilize the system by choosing an appropriate feedback
control. A mathematically linear control system is given by the following two equations
x = Ax+Bu
y = Cx
Here x = [G,X, Y,D1, D2, I, S1, S2, Z1, Z2, N ]T and B = [00000100000]T
and C = [100000000000]. The n × np controllability matrix is given by
R = [BABA2BA3B...An−1B]. The rank (i.e. rank(R) = n), so the system
is said to be controllable. The nk × n is the observability matrix is given by
O = [C;CA;CA2;CA3;CA(n− 1)]T . The rank (i.e. rank(R) = n) , so the system is said
to be observable [21, 22, 53].
Theorem 7.2: let ρ(B) = p, The pair (A,B) are said to be controllable if
Gcn−p+1 = [BABA2BA3B...An−pB] has full row rank. This is equivalent to
Gcn−p+1.G(n−p+1)c being nonsingular and G(n−p+1)c.G(n−p+1)c > 0 (positive definite).
Theorem 7.3: let ρ(C) = p, The pair (A,C) are said to be observable if
Gcn−p+1 = [CCACA2CA3BCA(n − p)C]T has full row rank. This is equivalent to
Gcn−p+1.Gcn−p+1 being nonsingular and Gcn−p+1.G(n−p+ 1)c > 0 (positive definite)[21, 53]
We have two cases in the system, for case I: Insulin as the input only and glucose as
an output and in case II: insulin and glucagon as an input and glucose as output only.
For Case I: If we consider the insulin concentration in periphery vascular

CHAPTER 7. CONTROL OF COMPOSITE MODEL 97
blood space as inputs and glucose concentration in extracellular fluid as the
only output than B = [00100000000]T and C = [100000000000] The control-
lability matrix is R = [BABA2BA3BA4B...A10B] and the observability matrix
is O = [C;CA;CA2;CA3;CA4; ..., CA10]. By using the property of controlla-
bility Det(R × R) = 0, so the controllability matrix is not controllable and
det(O × O) = 1.76614e−019, matrix is nonsingular so the observability matrix is
observable. Hence the system is observable but not controllable.
For case II: If we consider the insulin concentration in periphery vascular blood space
and glucagon concentration as inputs and glucagon concentration in extracellular fluid as
the only output than B = [00100000100]T and C = [100000000000]. By using theorem
7.3 of observability Det(O × O) = 0, so the controllability matrix is not controllable and
det(O×O) = 1.76614e−019, matrix is nonsingular so the observability matrix is observable.
Hence the system is observable but not controllable.
7.5 Conclusion
For instance, in case of extended form of composite model for type 1diabetes mellitus, we
can see that the system improves its controllability when we consider glucagon as second
input along with insulin. In our opinion one has to develop models for the glucose-insulin-
glucagon system which pay special attention to the control mechanisms of the systems
first for the healthy system in order to understand the working of the control loops in the
healthy system which should be restored by the artificial pancreas. The system is uniformly
asymptotically stable by using the lyapunov equation because eigen values of matrix A are
all negative real roots. In each subject we have two cases, for case I: Insulin as the input
only and glucose as an output and in case II: insulin and glucagon as an input and glucose

CHAPTER 7. CONTROL OF COMPOSITE MODEL 98
as output only. First model is neither controllable nor observable in both cases. But the
second modified from of the composite model is observable but not controllable. The only
measured output is concentration of glucose in plasma that we can easily measure. But the
rank of the matrix is improved in model when we consider insulin and glucagon as inputs.
It means glucagon play an important role in the development of an artificial pancreas for
peoples types 1 diabetes. Our results indicate that such a feedback control will have to use
administration of insulin and glucagon by a combined insulin-glucagon pump.

Chapter 8
Conclusion and Future Work
Long term treatment plan of diabetic patient for regulation of blood glucose level is
critical. To overcome the complications of T1DM, blood sugar level must be maintained.
Unfortunately, therapy to overcome the complications is difficult to handle by patients
because it includes self-monitoring of BGL, multiple daily injections of insulin and use
of insulin pump. Hyperglycemia and hypoglycemia is most common complications in
type 1 diabetes patients even after insulin bolus therapy or continuous delivery of insulin
throughout the day. Hypoglycemia is dangerous condition. Artificial pancreas is used to
regulate BGL and have no negative consequences in T1DM patients.
The results of our calculations strongly indicate that it will not be possible to design a
stabilization feedback control if insulin is the only one input variable and glucose the only
output variable. Since the controllability and observability are sufficient conditions for the
existence of a stabilizing feedback control (obtained as a solution linear-quadratic regulator
problem), further investigations should be also the lowest detectability and stabilizability
properties for the models, which provide a set of necessary and sufficient conditions exis-
tence of a stabilizing control.
The results obtained in this thesis will have some impact on attempts to construct
99

CHAPTER 8. CONCLUSION AND FUTURE WORK 100
the artificial pancreas. Until now primarily one tries to implement a feedback control by
taking glucose as the only output providing information on the system state and by using
administration of insulin as the only control input. Glucose concentration is measured
subcutaneously by an implanted sensor which measures glucose concentration in the inter-
stitial fluid and not directly in blood. Therefore one will need a submodel describing the
relation between glucose concentrations in blood and in interstitial fluid. The use of in-
sulin as the only control input may be insufficient in case of hypoglycaemia, because a low
glucose level cannot be raised by insulin action. It seems to be that in order to restore the
desired glucose level that one has to include administration of glucagon as another control
input. For instance, in case of Sorensen’s model, GIG model for T1DM we can see that the
system improves its controllability when we consider glucagon as second input along with
insulin. In our opinion one has to develop models for the glucose-insulin-glucagon system
which pay special attention to the control mechanisms of the systems first for the healthy
system in order to understand the working of the control loops in the healthy system which
should be restored by the artificial pancreas. This means that in a second step one has
to reduce such a model to the case of T1DM in order to construct a stabilizing feedback
control for the model which presumably also works for the patient. Our results indicate
that such a feedback control will have to use administration of insulin and glucagon by
a combined insulin-glucagon pump. Despite the increased complexity of such a system
we see that this approach is already pursued by some groups as for instance at Boston
University and Massachusetts General Hospital and at Pancreum, The Wearable Artificial
Pancreas Company.
Framework provided by biologist in the field of mathematics for understand complex
phenomena. While the inclusion of delays but one approach among many, the theory
behind it should be continue to developed, with a particular eye towards practical results
and the ability to draw applicable conclusions.

CHAPTER 8. CONCLUSION AND FUTURE WORK 101
The discussion in the previous section shows that the following tasks should be con-
sidered for future research: (i) Development and validation of a comprehensive model for
the system including the important control mechanisms involving insulin and glucagon for
the healthy system. (ii) Adapting the model developed according to (i) to the case of
T1DM and investigation of the T1DM-model with respect to its control properties. Of
particular interest are the properties of the model obtained by linearisation around the
equilibrium state which should be preserved. The linearised model with glucose as the ob-
servable output and both, insulin and glucagon, as the control input should be controllable
and observable. (iii) Proportional integral controller design can be developed for Sorenson
Model and Composite model for type 1 diabetes mellitus to monitoring the glucose insulin
and glucagon measurement because these are the comprehensive model for physiology of
diabetes mellitus.

Bibliography
[1] J.D Murray: Mathematical Biology I. An Introduction,USA , Springer , Verlag Berlin
Heidelberg.(2002).
[2] A. C. Guyton and J. E. Hall, Text Book of Medical Physiology, Elsevier Saunders, St.
Louis, edition 11, 972 (2012).ISBN 0-7216-0240-1.
[3] M.U. Saleem, M. Farman , M.O. Ahmad and M. Rizwan, A Control of Artificial
Pancreas in Human, Chines journal of Physics. 55, 6, 2273-2282, 2017.
[4] S. Sandhya S. and D. Kumar, Mathematical model for glucose-insulin regulatory sys-
tem of diabetes mellitus, Advances in Applied Mathematical Biosciences, 2(1) 39-46,
(2011).
[5] Y. Kuang, A. Markroglou and J. Li, Mathematical models and software tools for
the glucose-insulin regulatory system and diabetes: an overview. Applied numerical
mathematics, 56, 559-573 (2006).
[6] C. Cobelli, E. Renard, and B. Kovatchev, Artificial Pancreas: Past, Present, Future.
Diabetes, 60(11) 2672-2682 (2011).
[7] K. Turksoy, L. Quinn, E. Littlejohn and A. Cinar, Multivariable adaptive identifi-
cation and control for artificial pancreas systems, IEEE Transactions on Biomedical
Engineering, 61(3),883-891, (2014).
102

BIBLIOGRAPHY 103
[8] S. Schmidt, D. Boiroux, A. Ranjan, J.B. Jrgensen, H. Madsen and K. Nrgaard. An ar-
tificial pancreas for automated blood glucose control in patients with Type 1 diabetes.
Therapeutics Delivery, 6(5),609-619, (2015).
[9] D. Boiroux, A. K. Duun-Henriksen, S. Schmidt, K. Nrgaard, N. K. Poulsen, H. Mad-
sen, and J. B. Jrgensen, Assessment of model predictive and adaptive glucose control
strategies for people with type 1 diabetes, 19th IFAC World Congress, Cape Town,
South Africa, 24 (2014).
[10] M. G. Markakis, G. D. Mitsis and V.Z. Marmarelis, Computational Study of an Aug-
mented Minimal Model for Glycaemia Control, 30th Ann. Intern. Conf. IEEE EMBS,
5445 (2008).
[11] J. Norman, The Important Roles of Insulin and Glucagon: Diabetes and Hy-
poglycemia, https://www.endocrineweb.com/conditions/diabetes/normal-regulation-
blood-glucose, april 2018.
[12] J. E. Gerich ,Physiology of Glucose Homeostasis, Diabetes, Obesity and
Metabolism,(2000).
[13] M. U. Saleem,Controllability and Observability in glucose insulin system in human,
Ph.D Thesis, Karl-Franzens University, Graz, Austria (2011).
[14] J. Li, Y. Kuang and A. Makroglou, Mathematical models and software tools for the
glucose-insulin regulatory system and diabetes, U.K. Applied numerical mathematics
56,559-573, (2005).
[15] A. Liebl, R. Hoogma, E. Renard, P. G. Duijvestijn, E. Klein, J. Diglas, L. Kessler,
V. Melki, P. Diem, J. M. Brun, P. Schaepelynck-Blicar and T. Frei, A reduction in
severe hypoglycaemia in type 1 diabetes in a randomized crossover study of continuous

BIBLIOGRAPHY 104
intraperitoneal compared with subcutaneous insulin infusion. Diabetes. Obes.Metab.,
11(11):10018, (2009).
[16] A. O. Marcus, Continuous Subcutaneous Insulin Infusion Therapy with Rapid-Acting
Insulin Analogs in Insulin Pumps: Does it Work, How Does it Work, and what Ther-
apies Work Better than Others? Open Diabetes J., 6(1):819, (2013).
[17] T. Prudhomme, A. Bock, G. Francois and D. Gillet, Preclinically assessed optimal
control of postprandial glucose excursions for type 1 patients with diabetes. IEEE Int.
Conf. Autom. Sci. Eng., 702-707, (2011).
[18] A. Bock, Modeling and Control for the Treatment of Type 1 Diabetes: An Approach
Based on Therapy Parameters, Ph.D Thesis, Institute of Electrical Engineering, Lau-
sanne, Switzerland, DOI10.5075/epfl-thesis-6084
[19] A. Bock, G. Franois, D. Gillet, A Therapy Parameter-based Model for Predicting
Blood Glucose Concentrations in Patients with Type 1 Diabetes. Comput. Methods
Programs Biomed,118(2),107-123, (2013).
[20] K. Kumareswaran, M. L. Evans and R. K Hovorka, Artificial pancreas: an emerging
aproach to treat type 1 diabetes, Expert reviews of medical devices, 6(4), 401-410,
(2009)
[21] J. M. Coron, Control and nonlinearity, American Mathematical society, 136, (2007).
ISBN: 978-0-8218-4918-7
[22] R. E. Kalman, P.L. Falb, M.A. Arbib, Topics in Mathematical Systems Theory, Mc-
Graw Hill, New York, (1969).
[23] F. Kappel, G. Peichl, Preservation of Controllability Under Approximation for Delay
Systems, Mat. Aplid. Comp., 8(1),23- 47, (1989).

BIBLIOGRAPHY 105
[24] F.J. Doyle, L.M. Huyett, J. B. Lee, H. C. Zisser and E. Dassau, Closed-loop artificial
pancreas systems: engineering the algorithms. Diabetes Care 37:1191-1197, (2014)
[25] S. J. Russell, F. H. El-Khatib, D. M. Nathan, K. L. Magyar, J. Jiang and E. R.
Damiano, Blood glucose control in type 1 diabetes with a bihormonal bionic endocrine
pancreas. Diabetes Care 35:2148-2155, (2012).
[26] C. Yogish, Kudva, E. Rickey, Carter, C. Cobelli and R. Basu, Closed-Loop Artificial
Pancreas Systems: Physiological Input to Enhance Next-Generation Devices, Diabetes
Care, 37(5): 1184-1190, (2014).
[27] H. L. Trentelman, A.A. Stoorvogel and M. Hautus, Control theory for linear
systems,Springer-Verlag London, (2001)
[28] S.D. Patek and M. D. Breton, LQG Artificial Pancreas Control System and Related
Method Vol. 6(5),609-619 , (2008).
[29] C. DallaMan, R.A. Rizza and C. Cobelli, Meal simulation model of the glucose-insulin
system, IEEE Transactions on Biomedical Engineering, 54(10),1740-1749, (2007).
[30] M. L. J. Hautus, Controllability and Observability Conditions for Linear Autonomous
Systems, Akad. Wet. Proc., A72, 443-448, (1969).
[31] A. Manitius and R. Triggiani, Function Space Controllability of Linear Retarded Sys-
tems: A derivative from abstract operator conditions, SIAM J. Control Optimiza-
tion, 23, 928-951, (1985).
[32] P.A. Hokayem and E. Gallestey, Lyapunov Stability Theory, non-linear systems and
control, (2015).
[33] H.K. Khalil, Nonlinear systems, Prentice hall, 3rd edition, (2002).

BIBLIOGRAPHY 106
[34] R. Morgan, linearization and stability analysis of non-linear problems, Rose-Hulman
Un- dergraduate Mathematics Journal , 16(2), 65-91, (2015).
[35] F. Haq, K. Shah, G. Rahman and M. Shahzad, Numerical solution of fractional order
smoking model via laplace Adomian decomposition method, Alexandria Engineering
Journal, February (2017).
[36] H. Jafari, Khalique and M. Nazari, Application of the Laplace decomposition method
for solving linear and nonlinear fractional diffusion-wave equations, Appl. Math. Lett.
24, 1799-1805, (2011).
[37] H. Jafari, C.M. Khalique, M. Khan and M. Ghasemi, A two-step Laplace decompo-
sition method for solving nonlinear partial differential equations, Int. J. Phys. Sci. 6,
4102-4109, (2011).
[38] S.J. Johnston, H. Jafari, S.P. Moshokoa, V.M. Ariyan and D. Baleanu, Laplace homo-
topy perturbation method for Burgers equation with space and time-fractional order,
Open Phys. 14, 247-252, (2016) .
[39] I. Podlubny, Fractional Differential Equations, Academic Press, San Diego-New York-
London, (1999).
[40] O.A. Arqub, A. El-Ajou, Solution of the fractional epidemic model by homotopy
analysis method, J king saud univ sci, 25, 73-81, (2013).
[41] K.A Morris, Introduction to Feedback Control. Academic Press, San Diego (2001).
[42] K. Ogata, Mordern Control Engineering, Fourth ed. Prentice-Hall, Upper Saddle
River, NJ (2002).

BIBLIOGRAPHY 107
[43] W. Boutayeb, M. Lamlili, A. Boutayeb and M. Derouich, Mathematical modeling and
simulation of -cell mass, insulin and glucose dynamics: Effect of genetic predisposition
to diabetes. Journal of Biomedical Science and Engineering 7 330 (2014).
[44] R. Celeste, E. Ackerman, L. C. Gatewood, Reynolds and G. D. Molnar, The role
of glucagon in the regulation of blood glucose: mathematical studies. Bulletin of
Mathematical Biology 40(1) 59 (1978).
[45] W. Boutayeb, A Mathematical Model of Glucose, Insulin, beta-Cells, alpha-Cells and
Glucagon, BAOJ Diabet, 1: 001 (2015).
[46] H. K. Khalil, Nonlinear systems, Prentice hall, 3rd edition, (2002).
[47] D. Boiroux, A. D. Henriksen, S. Schmidt, K. Norgaard and N. K. Poulsen, Adaptive
control in an artificial pancreas for people with type-1 diabetes, Control Engineering
Practice 58(1) 332-340 (2017).
[48] A. Algaddafi and A. Ali, Proposed procedure to improve performance of an artificial
pancreas and pancreas transplant: Review, Journal of diabetes and metabolism 8:
731 (2017).
[49] M. Farman, M. U. Saleem, M. O Ahmad and Aqeel Ahmad, Stability Analysis and
Control of Glucose Insulin Glucagon System in human, Chines Journal of Physics, 56,
1362-1369, (2018).
[50] J. T. Sorensen, A Physiological Model of Glucose Metabolism in Man and its Use
to Design and Assess Improved Insulin Therapies for Diabetes, Ph.D. Thesis, MIT,
USA, (1985).



BIBLIOGRAPHY 108
[51] M. U. Saleem, M. Farman and M.A Meraj, Stability Analysis of Sorensen’s Model for
Controllability and Observability, B. Life and Environmental Sciences 54 (2),133-145
(2017).
[52] G. Quiroz and R. Femat, On Hyperglycemic Glucose Basal Levels in Type 1 Diabetes
Mellitus from Dynamic Analysis, Math. Biosci., 210(2), 554-575, (2007).
[53] M.K. Camlibel and H. Heemels, Controllability of Linear Systems with Input and
State Constraints, Proceedings of the 46th IEEE Conference on Decision and Control
New Orleans, LA, USA. (2007).
[54] M. Farman, M.U Saleem and M.O. Ahmad, An Approach for Artificial Pancreas to
Control the Type-1 Diabetes Mellitus, Journal of Applied Environmental and Biolog-
ical Sciences, 11(5), 93-102, (2017).
[55] P. Herrero, G. Pantelis, N. Oliver, M. Reddy, D. Johnston and C. Toumazou, Com-
posite model of Glucagon-Glucose Dynamics for in silico testing of bihormonal glucose
controllers, Journal of diabetes science and technology, 7(4),941-951, (2013).
[56] S. Schmidt and B. Vladimir et all, The Contribution of Glucagon in an Artificial
Pancreas for People with Type 1 Diabetes 2015 American Control Conference Palmer
House Hilton. 1-3, (2015).
[57] R. Hovorka, V. Canonico, L. J. Chassin, U. Haueter, M. Massi- Benedetti, M. O.
Federici, T. R. Pieber, H. C. Schaller, L. Schaupp, T. Vering, and M. E. Wilinska,
Nonlinear model predictive control of glucose concentration in subjects with type 1
diabetes, Physiological Measurement,25(4), 905-920, (2004).
[58] M.U Saleem, Muhammad Farman, Aqeel Ahmad, M. Naeem, M. O Ahmad, Stabil-
ity Analysis and Control of Fractional Order Diabetes Mellitus Model for Artificial
Pancreas, Punjab University journal of mathematics, 51(4),97-113, (2019).