An Analysis of the ACUITY Trial Lincoff AM, JACC Intv 2008;1:639–48 Influence of Timing of...
If you can't read please download the document
An Analysis of the ACUITY Trial Lincoff AM, JACC Intv 2008;1:639–48 Influence of Timing of Clopidogrel Treatment on the Efficacy and Safety of Bivalirudin
An Analysis of the ACUITY Trial Lincoff AM, JACC Intv
2008;1:63948 Influence of Timing of Clopidogrel Treatment on the
Efficacy and Safety of Bivalirudin in Patients With NSTE-ACS
Undergoing PCI
Slide 2
Background In REPLACE-2 (elective or urgent PCI), bivalirudin
was not inferior to heparin plus a GP IIb/IIIa inhibitor in
reducing ischemic events and the efficacy of bivalirudin was not
influenced by the timing of clopidogrel administration 1 In
contrast, preliminary analysis of the ACUITY trial found an
interaction of borderline significance (p= 0.054) between
clopidogrel exposure and randomized therapy on 30-day composite
ischemia, 2 leading to the suggestion that the use of bivalirudin
monotherapy should be limited to NSTE ACS patients in whom
clopidogrel pre- treatment is given. This post-hoc analysis of the
ACUITY trial, evaluated the timing of the initiation of clopidogrel
treatment in patients undergoing PCI to determine whether
clopidogrel pre-treatment is especially beneficial or necessary in
patients not receiving a GP IIb/IIIa antagonist. 1: Saw et al 2.
Stone GW. NEJM Lincoff AM, JACC Intv 2008;1:63948 PCI Subgroup
Slide 3
Method of analysis for clopidogrel timing study Timing for the
initiation of clopidogrel was a priori designated as:
Pre-angiography if initiated at any time prior to the angiography
Peri-PCI if initiated after angiography and within 30 minutes of
the end of PCI Post-PCI if initiated > 30 minutes after PCI No
clopidogrel. Patients who did not receive clopidogrel (or
ticlopidine) at any time before or after PCI. Lincoff AM, JACC Intv
2008;1:63948 PCI Subgroup
Slide 4
Underwent PCI and received clopidogrel at some time prior to or
during hospitalization N= 7517 Clopidogrel pre-hospital N=1820
Clopidogrel at hospital pre- randomization N= 2383 No clopidogrel
N= 129 Clopidogrel study population All ACUITY patients N= 13,518
Lincoff AM, JACC Intv 2008;1:63948 Medical management N= 4491 CABG
N= 1539 PCI patients N= 7789 Missing data N=47 Clopidogrel pre-
angiography N= 928 Clopidogrel peri-PCI N=1572 Clopidogrel post-PCI
N=814 Known dose and duration Pre-angiography cohort Peri-PCI
cohort Post-PCI cohort No clopidogrel PCI Subgroup Ticlopidine
N=96
Slide 5
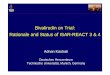
GPIIb/IIIa plus heparin GPIIb/IIIa plus bivalirudin Bivalirudin
alone 8.8 6.9 8.5 8.9 9.5 10.8 19.5 8.1 8.6 12.6 23.3 0 10 20
Pre-procedure N=5131 Peri-PCI N=1572 Post-PCI N=814 None N=129
Timing of Clopidogrel Exposure % Composite Ischemia 30-Day Ischemic
Outcomes P=0.46 P=0.29 P=0.13 P=0.08 Lincoff AM, JACC Intv
2008;1:63948 PCI Subgroup Analysis by clopidogrel timing and
randomized treatment arm
Slide 6
Timing of Clopidogrel Exposure Composite Ischemia % 8.8 9.7
14.0 8.1 8.6 12.6 23.3 8.2 0 10 20 Pre-PCI N=5131 Peri-PCI N=1572
Post-PCI N=814 None N=129 GPIIb/IIIa antagonist + any anticoagulant
Bivalirudin alone P=0.36 P=0.77 P=0.22 P=0.18 30-Day Ischemic
Outcomes 8.8 Lincoff AM, JACC Intv 2008;1:63948 PCI Subgroup
Analysis by clopidogrel timing and randomization to bivalirudin
alone vs combined heparin or bivalirudin plus GPIIb/IIIa
Slide 7
9.0 9.1 19.6 8.4 8.3 13.7 23.1 8.2 0 10 20 Timing of
Clopidogrel Exposure Composite Ischemia % Pre-PCI N=2824 Peri-PCI
N=950 Post-PCI N=471 None N=77 GPIIb/IIIa antagonist + any
anticoagulant Bivalirudin alone P=0.60 P=0.72 P=0.13 P=0.97 30-Day
Ischemic Outcomes in Troponin+ PCI Patients Lincoff AM, JACC Intv
2008;1:63948 PCI Subgroup Analysis by clopidogrel timing and
randomization to bivalirudin alone vs combined heparin or
bivalirudin plus GPIIb/IIIa
Slide 8
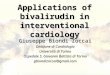
Estimated Spline Transformation and 95% C.I. Log Odds for
Composite Ischemia (30-Days) Duration of Clopidogrel Treatment
Prior to PCI (hours) -4 -3 -2 0 1 2 024681012141618202224
GPIIb/IIIa antagonist + any anticoagulant Bivalirudin alone 30-Day
Ischemic Outcomes Lincoff AM, JACC Intv 2008;1:63948 Patients with
known time of clopidogrel administration (n=928) Analysis by
duration of cloplidogrel treatment pre-PCI and randomization to
bivalirudin alone vs combined heparin or bivalirudin plus
GPIIb/IIIa PCI Subgroup
Slide 9
Outcomes and clopidogrel administration Pre* - or Peri -PCI PCI
patientsRisk Ratio 95% CIRR (95% CI) p-value Bivalirudin
monotherapy better (N=2284) UFH/enoxaparin + GP IIb/IIIa better
(N=2189) 30-day composite ischemia 0.98 (0.811.20) 0.88 30-day
major bleeding 0.53 (0.410.69)
Outcomes and clopidogrel administration Post-PCI or None PCI
patientsRR 95% CIRR (95% CI) p-value Bivalirudin monotherapy better
(N=290) UFH/enoxaparin + GP IIb/IIIa better (N=317) 30-day
composite ischemia 1.66 (1.052.63) 0.03 30-day major bleeding 0.48
(0.230.98) 0.04 1-year composite ischemia 1.21 (0.881.67) 0.25
1-year death 0.61 (0.281.37) 0.23 PCI Subgroup Groups based on
first exposure to clopidogrel; excludes patients who received
ticlopidine. Postprocedure = patients who received clopidogrel any
time >30 minutes after PCI within the index hospitalization. No
clopidogrel = patients who had no documentation of receiving
clopidogrel at any time before or after the PCI procedure. Lincoff
AM, JACC Intv 2008;1:63948
Slide 11
In ACUITY, patients who received clopidogrel either prior to,
or at the time of PCI achieved similar ischemic event rates and
significantly less bleeding when randomized to bivalirudin alone vs
a GPIIb/IIIa antagonist, irrespective of troponin status. Among
patients for whom clopidogrel will be given more than 30 min or not
at all after PCI, an antithrombotic regimen that includes GP
IIb/IIIa inhibition may provide better protection against ischemic
events than does bivalirudin alone. These data are reassuring for
the treatment of patients with NSTE-ACS who undergo diagnostic
catheterization and PCI with bivalirudin alone without clopidogrel
pre-loading Conclusions Lincoff AM, JACC Intv 2008;1:63948 PCI
Subgroup