Embed Size (px)
Citation preview
National Council on Ageing and Older People
An Chomhairle Náisiúnta um Aosú agus Daoine Aosta
An Age Friendly Society
A Position Statement

National Council on Ageing and Older People
An Chomhairle Náisiúnta um Aosú agus Daoine Aosta
An Age Friendly Society
A Position Statement

National Council on Ageing and Older People
22 Clanwilliam Square
Grand Canal Quay
Dublin 2
Report no. 88
© National Council on Ageing and Older People, 2005
ISBN 1 900378 39 6
Cover image kindly provided by West Cork Arts Centre in association with Skibbereen Day Care Centre.

An Age Friendly Society
Chapter One: Introduction 7
1.1 Irish society 8
1.2 The place of older people in Irish society 8
1.3 The ageing of the population 8
1.4 Addressing the ageing of the population 9
Chapter Two: A Profile of Older People in Ireland Today 11
2.1 Introduction 12
2.2 Demographic profile 12
2.3 Incomes and poverty 13
2.4 Employment, retirement and education 14
2.5 Health and lifestyle 14
2.6 Health service usage 16
2.7 Community services 17
2.8 Long-stay care 17
2.9 Problems facing older people 17
2.10 Older people’s information needs 18
2.11 Conclusion 18
Chapter Three: An Outline of International Developments 19
3.1 Introduction 20
3.2 International events and publications 20
3.3 Principles and concepts 21
3.4 From principles to policy 23
3.5 Conclusion 24
Chapter Four: What Is an Age Friendly Society? 25
4.1 A society for all ages 26
4.2 An age friendly society 26
4.3 Conclusion 27
Contents

Chapter Five: Barriers to the Development of an Age Friendly Society in Ireland 29
5.1 Introduction 30
5.2 Ageism in Irish society 31
5.3 Equating old age with dependence 31
5.4 Confusion regarding the meaning of dependency 31
5.5 Inappropriate models of old age 31
5.6 Negative perspectives on the ageing of the population 31
5.7 Limitations in current national policy in ageing and older people 32
5.8 Inadequacies in information for planning purposes 34
5.9 Limitations in quality standards development 34
5.10 Agreement on roles and responsibilities in building
and maintaining an age friendly society 35
Chapter Six: Towards an Age Friendly Society in Ireland 37
6.1 Defining an age friendly society in Ireland 38
6.2 Implementing an age friendly society in Ireland 41
6.3 Conclusion 42
Appendix One: References 44
Appendix Two: UN Principles for Older Persons 47
Appendix Three: Terms of Reference and Membership 48

An Age Friendly Society
Only in this century has human civilisation
made it possible for most people in western
societies to reach the age of 70 and over.
Therefore, the shaping of what is possible
in old age does not have a long tradition.
As a society, we are only at the beginning
of a learning process about old age.
In this sense, old age is still young, its
potential is not fully realised, and institutions,
norms and resources advantageous for
old age still need to be developed.– Baltes and Mayer, 1999


An Age Friendly Society
7
CHAPTER ONE
Introduction

8
1.1 Irish society
For the first time since 1871, the Irish population now exceeds four million and the CSO projects that it will rise
to five million people over the next 15 years.
According to the United Nations (UN) Human Development Index 2004, Ireland ranks among the top ten countries
across a range of socio-economic indicators including life expectancy, education, literacy and adjusted real income.
In 2004, Ireland recorded the third highest GDP per capita in the world. Between 1999 and 2004, unemployment
rates decreased from 5.5 per cent to 4.4 per cent.
Ireland performs less well, however, across a range of social indicators. For example, even though the rate of
consistent poverty fell from 15 per cent to 5 per cent between 1994 and 2001, Ireland is still ranked sixteenth out
of the seventeen countries reviewed in the Index. In addition, Irish people with an illness or disability, households
headed by a retired person, people living alone, people living in rural areas and women are at a greater risk of poverty
than the general population.
Rates of ‘excellent’ or ‘very good’ self-reported general health have increased from 48.2 per cent to 53.8 per cent for
males and from 49.1 per cent to 56.5 per cent for females between 1997 and 2002. However, the 4.9 per cent of GDP
spent on public healthcare by the Irish Government compares unfavourably to Germany, Sweden, France, Denmark,
Belgium, Holland and the UK.1
Life expectancy at birth has also improved, rising from 73.0 to 75.1 years for males and from 78.5 to 80.3 years
for females between 1996 and 2002. Nevertheless, life expectancy at age 65 in Ireland still compares unfavourably
with our EU partners. In 1999, Ireland ranked lowest among seventeen European countries in life expectancy at age
65, with a gap of 2.11 years between Ireland and the EU average.
1.2 The place of older people in Irish society
As indicated in Section 1.1, Irish society has changed significantly and become more prosperous in recent years.
Older people’s circumstances have changed too and they have shared, to varying degrees, in the prosperity.
However, our society still has some serious questions to answer about the place it accords to its oldest citizens
and how this place is determined. Like other countries around the world, we must face up to the ageing of our
population and identify the strategies we need to adopt and the provisions we must make to create an age friendly
society, both now and in the future.
1.3 The ageing of the population
Population ageing is an international phenomenon. However, the experience of the phenomenon varies from one
country to another. One of the reasons for this is the variation in national demographic structures, which means that
countries find themselves at different points in the population ageing cycle. Though Ireland’s population is ageing,
in comparative terms it remains relatively young.
In 2002, the proportion of Ireland’s population aged 65 years and over was 11.1 per cent. According to population
projections prepared for the National Council on Ageing and Older People (NCAOP), this proportion will rise to
between 14. 8 per cent and 15.3 per cent by 2021. The number of Irish people aged 80 and over is projected
to increase quite steeply; from 100,583 in 2002 to 137,305 in 2021.
CHAPTER ONE
Introduction
1 The average healthcare expenditure for these countries is 6.9 per cent of GDP.

An Age Friendly Society
9
Though Ireland’s old age dependency ratio will rise over the next twenty years in line with other developed countries,
the expectation is that it will remain relatively low by international standards. A projected old age dependency ratio
of 17.9 per cent in 2011 will be below current levels in all other developed countries. Fortunately, therefore, Ireland
has some time to plan how to meet the needs – including the long-term care needs – of an ageing population.
1.4 Addressing the ageing of the population
A wide-ranging public debate on the place of older people in Irish society is needed to inform thinking and
decision-making on matters critical to the welfare of older people in Ireland. The NCAOP believes that such
a debate is long overdue for a range of reasons, including:
• The need to consider and agree as a society the respective roles of the State, the family, the community and the
individual in maintaining and developing the independence, self-fulfilment and participation of older people in society
while assuring the care and dignity of those older people who are most frail and vulnerable.
• The limitations and inadequacies of some current national policies on ageing and older people.
• The frequent inconsistencies between policies on services for older people and their implementation.
• The urgent need to address health and social care deficits affecting older people in particular.
• The need to plan and provide adequately for an ageing population and the ageing of the population.
The planning, development and implementation of long-term care policy and practice, for example, will pose
significant challenges in the Irish setting. This is not unique to Ireland. Processes of reform and innovation in respect
of this issue in other countries, such as Australia, England, Germany, Japan and Scotland, have been accompanied
by widespread public debate and discussion.
A national debate on older people in Irish society will include discussion about the long-term care of older people.
Inevitably, dilemmas in decision-making about the financing of long-term care raise important questions for society:
who is primarily responsible for providing care for older people, the State or their families? Should publicly-funded
support be universally available or available to older people with low incomes/assets? The Council believes that it
would be healthy for our society if these and other questions were discussed thoroughly, frankly and openly in
advance of any decision-making.
If we, as a society, do not debate these questions and reach positive conclusions about the place of older people in
society, we will not make appropriate legislative and financial provisions for them. Such provisions are required to
promote the independence and dignity of older people in the face of ageist attitudes on the one hand, and failing
health or reduced capacity on the other.
As a society, we would not intentionally want to make inadequate provision for older people; that would mean
making inadequate provision for our own future. However, unless we understand and engage with the issues of
ageing and the issues faced by older people, we will not create – or eventually enjoy – an age friendly society.

10
An Age Friendly Society
11
CHAPTER TWO
A Profile of Older People in Ireland Today

12
2.1 Introduction2
Ireland’s older people are a diverse group, whose lives have been shaped by a variety of events, experiences and
circumstances. It is difficult to compose a vignette that adequately captures this diversity and the information in
this chapter is purely intended to provide an overview of Ireland’s older population.3
2.2 Demographic profile
2.2.1 Age profile
According to Census 2002, there are 436,000 people aged 65 and over in Ireland; this constitutes 11.1 per cent of the
Irish population. 44 per cent of older people are aged 75 and over. 56 per cent of the older people in Ireland are women.
By 2021, projections prepared for the Council predict that the percentage of Irish people aged 65 and over will rise
to between 14.8 per cent and 15.3 per cent, with the numbers of those aged 75 and over rising as high as 285,000.
Currently, on average, women in Ireland live longer than men. A man who has reached the age of 60 can expect
to live for a further 19.2 years, while his female counterpart can expect to live for an additional 22.9 years.
2.2.2 Marital status
According to Census 2002, 47 per cent of all older Irish people are married, while 33 per cent are widowed.
There are four times as many widows as widowers.
66 per cent of older women and 36 per cent of older men living in rural communities are either single or widowed,
while in urban communities the numbers are 62 per cent and 31 per cent respectively.
CHAPTER TWO
A Profile of Older People in Ireland Today
2 The data used in this chapt�in Ireland is available from the NCAOP website (www.ncaop.ie). A guide to the work of the Council, which includes a catalogue of its publications, is also available on request.
3 For the purpose of this document, older people are defined as people aged 65 years and over, unless otherwise stated.
��
���
���
���
���������
��������
������� �
�������������������
Figure 2.1: Marital status of older people

An Age Friendly Society
13
2.2.3 Living arrangements
The majority of Ireland’s older population (55 per cent) live in urban communities of 1,500 people or more.
In 2002, more than 25 per cent of people aged 65 and over lived alone, with older people comprising 41 per cent
of all Irish people living alone. Council projections forecast that by 2021, 211,000 older people (30 per cent) will
be living alone.
2.2.4 Home ownership
According to the Irish National Survey of Housing Quality 2001-2002, 81 per cent of older adults living alone and
87 per cent of older adults living with another own their own homes. Between 4 per cent and 6 per cent of older adults
are on a purchasing scheme from a local authority. Of those living alone, 9 per cent rent their accommodation from
a local authority. Between 1 and 2 per cent of older people live in the private rented sector.
2.3 Incomes and poverty
2.3.1 Income
Council research has shown that 84 per cent of income in households with one or more older people resident
derives from pensions. In 2003, the Department of Social and Family Affairs (DoSFA) reported that 26 per cent
of older people were in receipt of the Old Age Contributory Pension, 19.8 per cent were in receipt of the Retirement
Pension and 19.9 per cent were in receipt of the Old Age Non-Contributory Pension.
2.3.2 Poverty
According to the results of the 2004 EU Survey on Income and Living Conditions (EU-SILC), 36.4 per cent of
those aged 65 years and over are ‘at risk of poverty’ at the 60 per cent threshold (after social transfers). Furthermore,
7 per cent of those aged 65 years and over are considered as being in ‘consistent poverty’ at the 60 per cent level
using basic lifestyle deprivation indices.
According to Council research, the sub-groups of the older population whose incomes are particularly low when
compared to others are those on the Non-Contributory Widows Pension, the Old Age Non-Contributory Pension
and the Contributory Widows Pension.
2.3.3 Fuel poverty
The inability to afford adequate home heating can result in premature mortality among older people. Ireland has
the highest levels of fuel poverty in northern Europe for the category of lone pensioner households. The Irish National
Survey of Housing Quality found that older households are more likely to be characterised by having an open fire,
with 25 per cent of older households having no central heating.
14
2.4 Employment, retirement and education
2.4.1 Employment and retirement
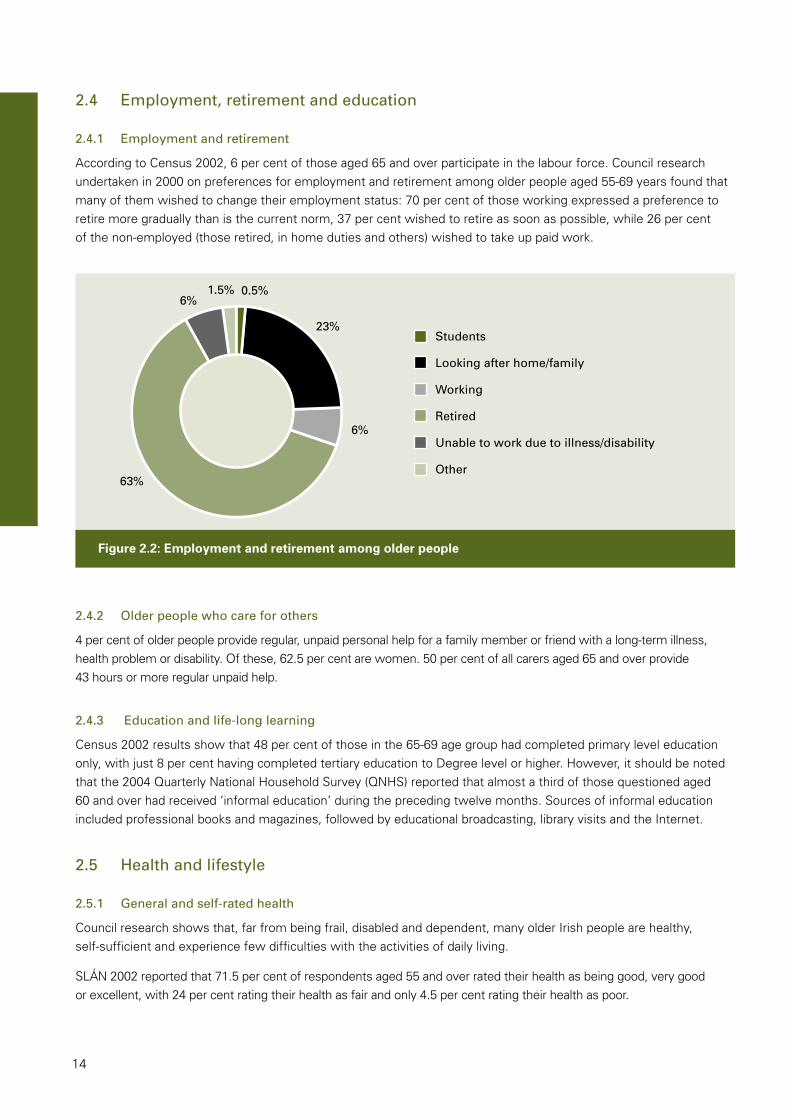
According to Census 2002, 6 per cent of those aged 65 and over participate in the labour force. Council research
undertaken in 2000 on preferences for employment and retirement among older people aged 55-69 years found that
many of them wished to change their employment status: 70 per cent of those working expressed a preference to
retire more gradually than is the current norm, 37 per cent wished to retire as soon as possible, while 26 per cent
of the non-employed (those retired, in home duties and others) wished to take up paid work.
2.4.2 Older people who care for others
4 per cent of older people provide regular, unpaid personal help for a family member or friend with a long-term illness,
health problem or disability. Of these, 62.5 per cent are women. 50 per cent of all carers aged 65 and over provide
43 hours or more regular unpaid help.
2.4.3 Education and life-long learning
Census 2002 results show that 48 per cent of those in the 65-69 age group had completed primary level education
only, with just 8 per cent having completed tertiary education to Degree level or higher. However, it should be noted
that the 2004 Quarterly National Household Survey (QNHS) reported that almost a third of those questioned aged
60 and over had received ‘informal education’ during the preceding twelve months. Sources of informal education
included professional books and magazines, followed by educational broadcasting, library visits and the Internet.
2.5 Health and lifestyle
2.5.1 General and self-rated health
Council research shows that, far from being frail, disabled and dependent, many older Irish people are healthy,
self-sufficient and experience few difficulties with the activities of daily living.
SLÁN 2002 reported that 71.5 per cent of respondents aged 55 and over rated their health as being good, very good
or excellent, with 24 per cent rating their health as fair and only 4.5 per cent rating their health as poor.
��
��
��������
���
���
���������
�������������������������
�������
��������������
����������������������������������������
�����
�
Figure 2.2: Employment and retirement among older people

An Age Friendly Society
15
2.5.2 Diet and exercise
Recent Council research reported that one third of people aged 55 and over do not consume the recommended
daily servings of dairy, fruit and vegetables, or meat, fish and alternatives. In addition, 54 per cent of those consulted
felt that they could be eating more healthily. 45 per cent of those surveyed reported having taken food supplements
in the previous twelve months.
Lack of exercise is one of the primary risk factors for heart disease. In this regard, the research found that 78 per cent
of those aged 55 and over felt that they exercised sufficiently. It also reported that between 1998 and 2002, there
had been an increase in the numbers of older people taking regular moderate and regular strenuous exercise, but
that there had been a decrease in those taking mild exercise.
2.5.3 Chronic health problems and disability
While acknowledging that many older Irish people are healthy and self-sufficient, it must also be recognised that
substantial numbers of older people experience chronic physical or mental health problems. Among those who
have a chronic illness, more than 46 per cent experience mobility problems; this is particularly prominent among
older women.
According to Census 2002, 135,696 older people have a disability. This comprises 32.2 per cent of the total older
population. The average older person affected by disability has 2.8 disabilities, compared with 1.9 for the rest of
the population.
SLÁN 1998 reported that 43 per cent of people aged 55 and over experience some difficulty following a conversation
if there is background noise; it was also found that these difficulties increase significantly with age. The same survey
reported that almost 86 per cent of respondents wear glasses or contact lenses some or all of the time.
2.5.4 Specific disorders
Cardiovascular disease is the major cause of death in Ireland, and the commonest cause in those aged 65 and over.
In 2002, cardiovascular diseases, including heart disease and stroke, accounted for 36 per cent of all deaths in the
65-74 age group and 40 per cent for those aged 75 and over.
For those aged 65 and over, cancer is the second most common cause of death, and the majority of colon cancer,
lung cancer and skin cancer cases are recorded among older Irish adults. In 2002, cancers accounted for 36 per cent
of all deaths among those aged 65-74 years and 16.5 per cent for those aged 75 and over.
���������������
��������������������������
������������������������
������������������������
���
��
��
��
Figure 2.3: Levels of difficulty with activities of daily living

16
2.5.5 Unintentional injury and falls
Admissions to hospital for unintentional injury are highest among older people, and there is a higher rate of admission
among females aged 65 and over. The number of accidents that involve older people are unknown, however external
causes accounted for 3.2 per cent of all deaths among those aged 65-74 years and 2.8 per cent among those aged
75 and over in 2002.
In 2001, 6,905 older people were admitted to hospital due to a fall. One third of those aged 65 and over will fall this
year; more than half of these will be aged 80+ years.
2.5.6 Suicide
There has been a steady increase in suicide in Ireland since the 1970s. In 2003, 13 males and 2 females per 100,000
of the population in the 65+ age group committed suicide. Council research has shown that factors associated with
suicide in older people include loss of independence, chronic pain, the loss of a loved one, alcohol problems, and
social isolation and loneliness. In this regard, recent Council research found that 11 per cent of older people have
minimal social contacts and a limited social network.
2.5.7 Mental disorders
Between 20 per cent and 25 per cent of older Irish people have a mental disorder of some severity at any one time.
Roughly 5 per cent of people aged 65 and over suffer from some form of dementia, while between 15 per cent
and 20 per cent suffer from other mental problems, such as depression and anxiety.
There were just over 30,000 people with dementia in Ireland in 1999, of whom 88.9 per cent were 65 years and
over. It is estimated that the number of people with dementia will grow to 35,116 in 2006 and to 41,125 in 2016.
The level of alcohol problems among older people is unknown as they often go unrecognised, however 11.5 per cent
of those in the 64-74 age group and 4.8 per cent of those aged 75 and over who were admitted to psychiatric
hospitals in 2000 suffered from alcoholic disorders. The misuse of alcohol by older people gives rise to dependence
and an increased risk of unintentional injury.
2.5.8 Elder abuse
Between 12,000 and 20,000 older Irish people are estimated to be victimised in Ireland on an annual basis.
These figures probably represent an underestimate given the hidden nature of this problem.
2.6 Health service usage
2.6.1 Check-ups
Council analysis of the 2002 SLÁN survey results revealed that 79.8 per cent of the older people interviewed had
a general health check-up during the previous three years. Over half the older people questioned regularly attended
their GP’s surgery or health centre for a check-up.
2.6.2 Hospital service usage in previous year
Research published by the Council in 2001 reported that 12 per cent of the older people interviewed had visited
A&E in the previous twelve months, while 16 per cent had scheduled in-patient appointments and 24 per cent
had scheduled out-patient appointments.
2.6.3 Acute hospital stays
In 1999, the average length of hospital stay for all ages and all conditions was 5.1 days. For older people, it was
7.9 days.

An Age Friendly Society
17
2.7 Community services
Council research has repeatedly found that older people wish to live independently in their own homes for as long
as possible. To this end, a continuum of services that caters for the entire range of dependence levels is essential.
The Council has found that the most used community care services include optician services, dental services,
chiropody and the Public Health Nurse (PHN) service. Research published by the Council in 2001 reported that
chiropody services were used by 16 per cent of the older people interviewed, with a further 12 per cent saying
that they would like to avail of the service. 15 per cent of the older people interviewed reported having been visited
by a PHN during the course of the previous year, with a further 3 per cent saying they would have liked to receive
the service.
2.8 Long-stay care
In 2003, 4.8 per cent of older Irish people were in long-stay care. The principal reasons for admission to long-stay
care include chronic illness, mental infirmity, physical disability and social reasons.
When questioned about their preferences for care, research published by the Council found that 87 per cent of
older people would prefer to remain in their own homes with family members taking care of all needs and health
services providing respite care.
2.9 Problems facing older people
A recent survey of older people’s perceptions of the problems facing them highlighted a number of issues: 82.5 per
cent of the older people interviewed identified crime as a major problem, while 51 per cent identified ‘making ends
meet’. Other problems highlighted included transport, loneliness and keeping warm in winter.4
Older people were also asked about how they felt they were treated by others: 33 per cent reported perceiving that they
were treated better than the general population, while 27.5 per cent reported the opposite. 61.5 per cent of the older
people interviewed also felt that older people are treated less favourably by the financial sector because of their age.
Finally, 86 per cent of those interviewed felt that society does not recognise the contribution made by older people.
4 This was one of� The ESRI conducted t� based on interviews with a nationally representative sample of the population aged 18 years and over.
Figure 2.4: Reasons for admission to long-stay care
� � �� �� �� �� �� ��
�����
�������������
�������������������
�����������������
����������������������
�����
�����
�����
�����
�����
18
2.10 Older people’s information needs
Council research has found that there are four significant transition times in older age that require the availability
of timely, accessible and accurate information to facilitate adjustment. These are retirement, onset of illness
and disability, moving from home for increased care and bereavement.
2.11 Conclusion
Heterogeneity is a key attribute of any age group in Irish society and this is no less true for older people. This is
reflected in the data in this chapter. However, by its nature, a profile of a population can only reflect key trends.
It cannot fully present the wide diversity of people’s experiences and needs.
Ageist attitudes include stereotypical views of older people, such as poor health, despite data showing that many
older Irish people enjoy good health. The challenge for Ireland and its policy-makers is to change perceptions of
ageing in order to reflect the diversity of Ireland’s older population, and to modify policies and practices in all
sectors of society to respond flexibly to the needs of all our older people.

An Age Friendly Society
19
CHAPTER THREE
An Outline of International Developments

20
3.1 Introduction
In April 2002, the Second World Assembly on Ageing was convened by the UN in Madrid. The Assembly, in which
Ireland participated, adopted the Madrid International Plan of Action on Ageing. The Madrid Plan is one of a number
of key international documents, endorsed by Ireland, which have been developed to guide and inform national and
international policy implementation in response to the challenge of population ageing. These international documents
indicate the changes in attitudes, policies and practices that are necessary to enable the emergence of an age
friendly society.
3.2 International events and publications
The development of international thinking on population ageing leading to the Madrid Plan is marked by a series
of events and publications (Figure 3.1). The Vienna International Plan of Action was adopted by the First World
Assembly on Ageing in 1982. Nine years later in 1991, the UN General Assembly adopted the UN Principles
for Older Persons.
In 1999, the UN celebrated the International Year of Older Persons. In keeping with further developments in
thinking about a society for all at the Copenhagen World Summit on Social Development in 1995, the theme
of the International Year was ‘a society for all ages’. A number of other bodies made specific contributions to the
International Year of Older Persons: the World Health Organisation (WHO) marked World Health Day with the theme
‘active ageing makes the difference’, while the European Commission published Towards a Europe for All Ages:
Promoting Prosperity and Intergenerational Solidarity.
CHAPTER THREE
An Outline of International Developments
1982 Vienna International Plan of Action on Ageing
1991 UN Principles for Older Persons
1995 Copenhagen World Summit on Social Development
1999 International Year of Older Persons
World Health Day on Active Ageing
Towards a Europe for All Ages: Promoting Prosperity and Intergenerational Solidarity
2002 Active Ageing: A Policy Framework
Madrid International Plan of Action on Ageing
Regional Implementation Strategy
Figure 3.1: International developments

An Age Friendly Society
21
As a contribution to the Second World Assembly on Ageing, the WHO published Active Ageing: A Policy Framework.
Following the adoption of the Madrid Plan, UN regional commissions became responsible for translating the Plan
into regional action plans. In this context, the United Nations Economic Commission for Europe (UNECE) organised
a ministerial conference on ageing in Berlin in September 2002. This event culminated in the adoption of the Regional
Implementation Strategy of the Madrid Plan. This Strategy specified ten commitments, nationally and regionally,
in pursuit of a society for all ages. Ministerial representatives of UNECE member states, including Ireland, declared
their support for these commitments.
3.3 Principles and concepts
Each of these events and publications formulated specific sets of recommendations in respect of population ageing.
Nonetheless, considered as a whole, there is a commonality at the heart of their thinking. In terms of the emergence
of a positive societal approach to population ageing, they highlight the significance of the UN Principles for Older Persons,
ideas of an age-integrated society, and affirmative concepts and images of ageing and older people, as outlined below.
3.3.1 UN Principles for Older Persons
The UN Principles address the independence, participation, care, self-fulfilment and dignity of older people. They follow
in the footsteps of the Universal Declaration of Human Rights and subsequent UN documents concerning the rights of
older people. In adopting these Principles, the UN urged governments to incorporate them into their national programmes
whenever possible.
3.3.2 A society for all ages
According to the operational framework for the International Year of Older Persons, a society for all ages is an
age-integrated society, which ‘adjusts its structures and functioning, as well as its policies and plans, to the needs
and capabilities of all, thereby releasing the potential of all, for the benefit of all’.
Such a society enables the participation of all citizens and also functions to the benefit of all citizens, regardless
of their age. An age-integrated society is characterised by relationships of reciprocity, solidarity and equity between
the generations.
3.3.3 Active ageing
Active ageing is, as the WHO explains, the process of optimising opportunities for health, participation and security
in order to enhance quality of life as people age. This approach aims to recognise factors or ‘determinants’ that affect
how people and populations age.
Culture and gender are considered cross-cutting determinants of active ageing. Culture shapes the way we age
because it influences all the other determinants of active ageing. Gender is a ‘lens’ through which we consider the
appropriateness of various policy options and how they affect the well-being of both men and women. The other
determinants of active ageing to be taken into account are shown in Figure 3.2. These determinants are embodied
in the WHO’s own policy proposals for societies committed to the goal of active ageing.

22
In order to promote active ageing, health systems need to adopt a life course perspective that focuses on health promotion, disease prevention and equitable access to quality primary healthcare and long-term care. This perspective recognises that older people are not one homogeneous group and that individual diversity increases with age. Interventions that create supportive environments and foster healthy choices are important at all stages of life, regardless of age. They confer benefits in terms of healthy living at any point in the life course and also in terms of healthy population ageing.
3.3.4 Productive ageing
Older people contribute to society in many different ways. As the Madrid International Plan of Action on Ageing (para. 23) says:
The social and economic contribution of older persons reaches beyond their economic activities. They often play crucial roles in families and in the community. They make many valuable contributions that are not measured in economic terms: care for family members, productive subsistence work, household maintenance and voluntary activities in the community. Moreover, these roles contribute to the preparation of the future labour force. All these contributions, including those made through unpaid work in all sectors by persons of all ages, particularly women, should be recognised.
3.3.5 Positive ageing
Positive ageing has been defined by the Office of an Ageing Australia as ‘an individual, community, public and private sector approach to ageing that aims to maintain and improve the physical, emotional and mental well-being of older people. It extends beyond the health and community service sectors, as the well-being of older people is affected by many different factors including socio-economic status, family and broader social interactions, employment, housing and transport. Social attitudes and perceptions of ageing can also strongly influence the well-being of older people, whether through direct discrimination or through negative attitudes and images.’
3.3.6 Successful ageing
Successful ageing has been described both in terms of its benefits to the individual and in terms of ‘the “strategies or the how” of achieving a successful old age’. The benefits of successful ageing to the individual include: autonomy; tolerance, optimism and courage; capacity for self-care; the reaching of one’s potential; generativity; the avoidance of disease, the maintenance of high physical and cognitive functioning and an active social life; and being happy, remaining hopeful, and developing (one’s) sense of self and (one’s) connections with others.
�������������
������
��������������������
������������������
�������������������
��������������������
�����������������������
�������������������������
�����������
Figure 3.2: Determinants of active ageing

An Age Friendly Society
23
The ‘strategies or the how’ description of successful ageing refers to the ability to adapt to the transitions and
diminishments experienced by the ageing person. The best known model of successful ageing is the selection,
optimisation and compensation (SOC) model developed by Baltes and Baltes, which proposes that as people
experience losses of function in older age, a parallel deterioration in their quality of life is prevented through a
process of adaptation. Individuals become more selective in their goals and expectations, use their resources to
optimise their functioning in these selected goal areas, and compensate for whatever losses they have experienced
with available resources.
3.4 From principles to policy
3.4.1 Policy framework for active ageing
The policy framework for active ageing devised by the WHO incorporated three strands: the UN Principles for Older
Persons; an understanding of how the determinants of active ageing influence the way that people and populations
age; and specific proposals in relation to each of the three pillars of the policy framework, i.e., participation, health
and security (Figure 3.3).
3.4.2 Towards a Europe for All Ages
In Towards a Europe for All Ages, the European Commission identified the implications of population ageing in
employment, social protection, and health and social services. Policy responses in each of these areas were proposed.
Those challenges, summarised, are:
• the relative decline of the population of working age and the ageing of the workforce;
• the growing numbers of retired people;
• the implications for health and care systems of population ageing;
• the requirement for differentiated policy responses in recognition of the increasing diversity of the older population;
• the gender balance of the ageing population which includes a higher proportion of women.
�������������
����������������� �������� ��������
�������������������������������������������
�����������������������������
Figure 3.3: Policy framework for active ageing

24
3.4.3 Madrid International Plan of Action on Ageing
The Madrid Plan identified three priority directions: older persons and development; advancing health and well-being
into old age; and ensuring enabling and supportive environments. In terms of over-arching themes and core content,
the Madrid Plan overlaps with the content of the WHO’s policy framework for active ageing. Both documents share
an identification of policy and practice objectives related to participation, health and security for the older population
as fundamental to the successful management of population ageing.
3.4.4 Regional Implementation Strategy
Following on from the Madrid Plan, member states of the UNECE, including Ireland, adopted the Regional
Implementation Strategy in Berlin in 2002. In adopting the Strategy, they made ten commitments:
1 To mainstream ageing in all policy fields with the aim of bringing societies and economies into harmony
with demographic change to achieve a society for all ages.
2 To ensure full integration and participation of older persons in society.
3 To promote equitable and sustainable economic growth in response to population ageing.
4 To adjust social protection systems in response to demographic changes and their social and economic consequences.
5 To enable labour markets to respond to the economic and social consequences of population ageing.
6 To promote life-long learning and adapt the educational system in order to meet changing economic, social
and demographic conditions.
7 To strive to ensure quality of life at all ages and maintain independent living including health and well-being.
8 To mainstream a gender approach in an ageing society.
9 To support families that provide care for older persons and promote intergenerational and intra-generational
solidarity among their members.
10 To promote the implementation and follow-up of the Strategy through regional co-operation.
3.5 Conclusion
Since 1982, developments in international thinking relating to population ageing have been reflected in a series
of UN, WHO and other documents and events, culminating in the 2002 Regional Implementation Strategy of the
Madrid International Plan of Action on Ageing. This indicates significant evolution in international awareness and
understanding of the issue of population ageing, as well as suggesting an orientation and first steps for societies
wishing to become age friendly societies. Ireland has been a participant in the international processes described in
this chapter. The challenge now is for Ireland to follow international participation with national implementation of
positive policy and practice, building on and extending the thinking already encapsulated in UN and other publications.

An Age Friendly Society
25
CHAPTER FOUR
What Is an Age Friendly Society?

26
4.1 A society for all ages
A society for all ages is the foundation of an age friendly society. In such a society the interdependence of
generations and of individuals is emphasised; diversity is recognised; the identity, values and beliefs of the individual
are protected; and social cohesion is fostered through the adoption of socially inclusive policies and priorities. In a
society for all ages, the generations are valued equally and intergenerational solidarity is part of the social contract.
In such a society, a life course perspective is adopted by all authorities; there is consistency and equity in the
treatment of all citizens; and risks are pooled between and within generations.
4.2 An age friendly society
When thinking about an age friendly society, it is important to be aware that there are two distinct perspectives on
ageing and older people. The first is that of the observer looking in. The second is that of the individual-who-is-ageing
looking out. For the observer looking in, concerns about demographic changes may be added to traditional concerns
about policies, practices and services. The individual-who-is-ageing looking out may see things differently. For
example, how often do we hear people say ‘I don’t feel old’, when they mean ‘I don’t feel any different to other
people’ or ‘I don’t feel different to when I was younger’?
However we feel about ageing, we are all increasingly concerned about the social construction of later life. We have
coined terms and developed concepts to give expression to what we, looking in, consider particularly worthwhile
aspirations for older people. Many of these concepts are valuable tools to help us build the foundation for an age
friendly society, but we must also see beyond them lest they limit the possibilities and opportunities for the
individual-who-is-ageing looking out.
4.2.1 Active ageing
In keeping with the WHO’s policy framework on active ageing, an age friendly society will seek to enhance
the quality of life of its citizens as they age by optimising their opportunities for health, participation and security.
An age friendly society will take account of all of the determinants of active ageing in its national, regional and local
policies and strategies.
4.2.2 Productive, positive and successful ageing
In addition to facilitating active ageing, an age friendly society will enable the achievement of productive, positive
and successful ageing, while acknowledging those who have other aspirations or visions. The policies of an age
friendly society will address inequalities in health and well-being over the life course to maximise the opportunities
for its older citizens. Older people will be the key stakeholders in determining the supports they need to enhance
their potential for active, productive, positive and successful ageing. These will include the financial, physical,
psychological, moral and spiritual supports needed at key transition times in later life, such as retirement, the
onset of illness, moving from home for increased care and bereavement.
4.2.3 Accommodating the perspective of the individual
An age friendly society is therefore a society which is receptive to positive constructs of ageing and rejects negative
ones. It is informed by and comes from ideas of active ageing, healthy ageing, positive ageing and successful ageing.
An age friendly society seeks to provide the conditions for the growth of positive attitudes to ageing among all
citizens, but particularly among older people themselves.
CHAPTER FOUR
What Is an Age Friendly Society?

An Age Friendly Society
27
However, a truly age friendly society will not impose any social construct of ageing on its individual older citizens.
To do so would be to risk alienating those for whom these constructs have no resonance, relevance or meaning,
those who may feel threatened by a perceived moral selectivity or burdened by norms set by others. In contrast,
an age friendly society will be person-centred, and will seek to accommodate the perspective of the individual older
person insofar as it can be ascertained, as well as respecting the older person’s lived experience of ageing.
4.3 Conclusion
An age friendly society is one that takes a positive approach to population ageing. On the one hand, it will address
the needs of older people as a distinct group in society. On the other hand, it will seek to remove the barriers that
segregate older people from the rest of society. Key to such an approach is timely identification of the tools required
for successful planning and a clear understanding of critical concepts including independence, dependence and
interdependence in a society for all ages. Most important of all, perhaps, is the need to identify the values and
aspirations we wish to adopt in determining the place older people will have in our society and the provisions that
will be made to ensure those values are realised.

28

An Age Friendly Society
29
CHAPTER FIVE
Barriers to the Development of an Age Friendly Society in Ireland

30
A positive view of ageing is an integral aspect of the International Plan of Action on Ageing, 2002.
Recognition of the authority, wisdom, dignity and restraint that comes with a lifetime of experience has
been a normal feature of the respect accorded to the old throughout history. These values are often neglected
in some societies and older persons are disproportionately portrayed as a drain on the economy, with their
escalating need for health and support services. Although healthy ageing is naturally an increasingly important
issue for older persons, public focus on the scale and cost of healthcare, pensions and other services have
sometimes fostered a negative image of ageing. Images of older persons as attractive, diverse and creative
individuals making vital contributions should compete for the public’s attention. Older women are particularly
affected by misleading and negative stereotypes: instead of being portrayed in ways that reflect their
contributions, strengths, resourcefulness and humanity, they are often depicted as weak and dependent.
This reinforces exclusionary practices at the local and national levels.
– Madrid International Plan of Action on Ageing (para. 102)
5.1 Introduction
The NCAOP has identified a number of barriers to the development of an age friendly society in Ireland. In the
first instance these relate to our attitudes to and understanding of ageing and older people; in the second, to policy,
planning and standard setting deficiencies leading to inadequate provision for the ageing of the population and for
our oldest citizens.
The attitudinal and conceptual barriers relate to:
• endemic ageism in Irish society;
• equating old age with dependence;
• confusion regarding the meaning of dependency;
• inappropriate models of old age;
• negative perspectives on the ageing of the population.
The policy, planning and standard setting limitations relate to:
• current national policy on ageing and older people;
• inadequacies in information for planning purposes;
• lack of quality standards development;
• lack of agreement on the respective roles and responsibilities of all sectors in building and maintaining
an age friendly society. 5
CHAPTER FIVE
Barriers to the Development of an Age Friendly Society in Ireland
5 Including the State, the community, the family, the individual and the Social Partners.
An Age Friendly Society
31
5.2 Ageism in Irish society
A critical barometer of how age friendly a society is relates to prevailing thinking, attitudes and behaviour towards its older
citizens individually and its older population in general. When these are negative, we call it ageism.
Ageism incorporates:
• negative thinking which leads to stereotyping of older people;
• negative attitudes which lead to prejudice against older people;
• negative behaviour which leads to discrimination against older people.
Ageism promotes the idea that older people are a burden and this can lead to neglect and social exclusion. It can also
diminish older people’s self-esteem, reduce their participation in society, and restrict the types and quality of services
available to them.
5.3 Equating old age with dependence
Dependence is part of the human condition experienced by all those who need support and assistance from others
because of frailty, illness, impairment or poverty. It is not specific to old people. Equating old age with dependence
has become self-fulfilling as society denies its older citizens the opportunity to continue to participate in economic
and other activities on the grounds of their age, and provides inadequate financial, health, social and physical supports
to those whose independence may be compromised for want of them. Understandably under these circumstances,
many older people have succumbed to the prevailing negative circumstances and have internalised a view of
themselves as dependent on others for all their needs.
5.4 Confusion regarding the meaning of dependency
As highlighted by the National Disability Authority (NDA), there has been a failure to distinguish between ‘necessary’
dependency flowing from individual life situations and ‘socially created dependency’ which results from those
structures and systems in our society that restrict optimal independence for the individual. The prevalent attitudes
in a society, the physical environment it builds and the services it provides can make all the difference between
a situation of independence for an older person and a situation of dependence.
5.5 Inappropriate models of old age
The older population is a diverse population: each person experiencing life and growing old differently to the next;
each coming from a different family and background, living in different circumstances with different aspirations and
beliefs. Why then do we treat all older people the same? Why do we adopt extreme models of old age: the ‘deficit’
model, which sees old age as an illness without cure; or the ‘heroic’ model which suggests that to age successfully
you must maintain the appearance, capacities and perspectives of youth and middle age.
5.6 Negative perspectives on the ageing of the population
In common with most developed countries our population is ageing. Is that a good thing or a bad thing? Many
emphasise projected deteriorating old age dependency ratios and resulting strains on the public system and the
working age population. Many predict, on the basis of certain calculations, that the ageing of the population will
impose an unsustainable burden at some time in the future. Others do not do any calculations at all in the hope that
the issues surrounding the ageing of the population will go away. These are static positions, ultimately ageist, leading
to discrimination against older people.

32
The prospective ageing of the population, and selective interpretations of its impacts, are being used as leverage for
changes that are not in the best interests of older people today or in the future. This approach is neither responsive
nor responsible. Terminology such as ‘the demographic time bomb’, ‘the ageing crisis’ and ‘the burden of ageing’
quickly projects onto older people and facilitates negatively differential treatment in health and other services.
5.7 Limitations on current national policy on ageing and older people
In recent years, the NCAOP has published recommendations on a wide range of issues relating to ageing and the
welfare of older people (see www.ncaop.ie). While these reports have served to increase our understanding of
ageing and older people in Ireland and have had some success in influencing policy development, it is clear that they
have had limited impact in generating a national debate on the place of older people in Irish society. In consequence,
national policy remains limited and is open to the challenge that it is driven as much by administrative expediency
as by national consensus.
5.7.1 The Years Ahead: A Policy for the Elderly (1988)
The Years Ahead: A Policy for the Elderly remains the most significant national policy exclusively dedicated to older
people. It states:
In the light of our obligations towards our elderly citizens as they are perceived today, we consider that the following
should be the objectives of public policy in regard to them.
• To maintain elderly people in dignity and independence in their own home.
• To restore those elderly people who become ill or dependent to independence at home.
• To encourage and support the care of the elderly in their own community by family, neighbours
and voluntary bodies in every way possible.
• To provide a high quality of hospital and residential care for elderly people when they can no longer
be maintained in dignity and independence at home.
As a public policy, its perspective is therefore on ‘our obligations to our elderly citizens’, not on older people’s place
in Irish society or on their rights and entitlements to equal citizenship. Even within its relatively narrow parameters,
The Years Ahead was to prove to have limited success in achieving its objectives. The 1997 review by the NCAOP
of the implementation of the recommendations of The Years Ahead noted that it remained a highly significant
influence on the care of older people in this country. However, it also identified obstacles to its implementation.
Co-ordination
While the policy emphasised interdepartmental co-ordination (between the Departments of Health, Social Welfare,
and the Environment particularly) and co-ordination at local level (between health boards and local authorities), this
did not happen in any systematic way such as to achieve policy objectives. In consequence, many of the practical
problems in developing alternative services to help older people to continue living at home in the community for
as long as possible remain as intractable today as in 1988.
Statutory basis
The Years Ahead has no statutory basis and the recommendations it made for the legal underpinning of certain
services were not implemented. The review states that ‘while acknowledging the danger of rigidity in legislating for
all aspects of care, the absence of a legislative framework for a certain standard of care, with obligatory provision
of core services, is an issue which has to be addressed’.
An Age Friendly Society
33
Funding
The legislative status of The Years Ahead resulted in significant weaknesses in national provisions for older people in
Ireland, which contrasts with progress in other areas. While additional revenue funding has been allocated to services
for older people in recent years and while it is also expected that significant resources will be provided to subvent
home care in the near future, it remains the case that there is a very significant inconsistency between the objectives
of The Years Ahead and current care provisions.
Provision of core community care services
While The Years Ahead communicated excellent principles and objectives for health and welfare services for older people,
the core services required to translate these principles into practice were not provided in a consistent and equitable basis
across the country. There is still no requirement to fund services such as home help, day care or respite care. They are,
therefore, provided on a discretionary basis.
Eligibility vs entitlement
In keeping with the objectives of The Years Ahead, older people may be eligible to receive core home care services
enabling them to live in dignity and independence at home. However, because they are not entitled to these services,
they may not receive them due to budgetary constraints.
In consequence, there arises an inconsistency between the objectives of public policy for older people in Ireland and the
service provision required to ensure implementation. It appears that the criterion of affordability takes precedence over
commitment to the provision of services to the standard required to meet national policy objectives for older people.
5.7.2 Quality and Fairness: A Health System for You (2001)
Consultation
During the consultation process preceding the development of the National Health Strategy, Quality and Fairness:
A Health System for You, the needs of older people were particularly prominent; the emphasis being largely on improving
their quality of life.
Supporting their carers, especially family carers, was also an important concern. Providing improved assessment,
community support services and rehabilitation in order to enable older people to remain in their own homes or
communities for as long as possible was also mentioned, as well as proposals on the availability, cost and quality
of long-stay care.
Responding to older people’s needs
With regard to services for older people, Chapter 6 of the Strategy (‘Responding to people’s needs’) states:
Older people often experience a poor level of health accompanied by pain, discomfort, anxiety and depression.
There is a need to develop a comprehensive approach to meeting the needs of ageing and older people if the
problems in the care and quality of life of older people are to be addressed and the increased demands over the
next 20-30 years are to be met. This must include both acute healthcare provisions for the sick elderly and active
health maintenance programmes for continuance of health in the elderly.
The Strategy identified the main gaps in current service provision relating to:
• community-support services (e.g. paramedic services, community nursing services, health promotion,
home help service, day care);
• acute hospitals (e.g. shortages in assessment and rehabilitation beds and day hospital facilities);
• long-stay places (e.g. need for additional community nursing units).

34
Key actions
The Strategy then identified the following key actions for ageing and older people:
• A co-ordinated action plan to meet the needs of ageing and older people will be developed by the Department
of Health and Children in conjunction with the Departments of the Environment and Local Government; Social,
Community and Family Affairs; and Public Enterprise.
• Community groups will be funded to facilitate volunteers in providing support services, such as shopping, visiting
and transport for older people.
• Health boards will continue to take the lead role in implementing Adding Years to Life and Life to Years:
A Health Promotion Strategy for Older People.
• An action plan for dementia, based on the recommendations of the NCAOP, will be implemented.
• Legislation to include provision for a clear framework for financing long-stay care for older people and funding
options to meet the cost of care would be outlined for public debate prior to the preparation of legislation.
• National standards and protocols for quality care for all health and personal social services will be developed.
While these key actions are welcomed, the absence of an implementation framework to support their delivery
is a significant deficiency.
5.8 Inadequacies in information for planning purposes
In order to plan effectively for an age friendly society, policy-makers require accurate and timely information about
the older population. Existing information systems are unable to provide this data. Typically, datasets operate on a
stand-alone basis and it is not possible to link and integrate data from a range of datasets, either to create a more
holistic profile of the older population or to identify more vulnerable sub-groups of that population.
In terms of a national framework of information about the older population, there are significant issues and deficits.
Notably, these relate to social determinants, including the quality of life and social contribution of older people;
determinants related to the physical environment, including housing and transport; and to the health and social
services where datasets are stronger in the provision of institutional than of community-based data, though the
majority of older people live in community settings.
There are particular concerns about the lack of person-centred data, of population-based morbidity data, of a
national psychiatric out-patient database and of data on the prevalence and incidence of different forms of impairment
and disability in the population. There is an urgent need for information systems to capture and analyse such data
for Ireland.
5.9 Limitations in quality standards development
Currently, the absence of legally enforceable standards of care provision results in an lack of rights for the patient
and a lack of responsibility on the part of the care provider for quality care provision. As a result, the quality of
services received and the dignity of the patient may suffer.
In many cases, this is inadvertent and symptomatic of limited and limiting resources. However, in some cases,
it is related to the manner in which the services are provided at a personal level. For example, Council research
has demonstrated that ageist attitudes among health and social care providers can result in the provision of poor
quality services at an individual level.

An Age Friendly Society
35
The absence of systems necessary to agree standards and to establish whether these standards are being met
is notable. In addition, authoritative statements of policy on prevention, assessment, rehabilitation, standards of
care, and the maintenance of independence and dignity in various care settings are limited. Finally, quality assurance
policy statements and service plans are virtually absent.
The Working Group on Elder Abuse starkly highlighted the implications of an absence of quality standards in its report
Protecting Our Future:
Elder abuse is something that happens culturally and corporately as well as on an individual basis … a lot of the
abuse that goes on is purely unintentional abuse that is institutionalised. It comes from the structures of health and
social care that we have in place at the moment … some people are being looked after in impoverished environments
… being treated and cared for by overworked, stressed, burnt-out staff who are too small in number to be able to
cater for their needs properly … the wider definition of what abuse is needs to be highlighted very quickly and
emphatically as well.
5.10 Agreement on roles and responsibilities in building and maintaining an age friendly society
Good policy should operate in tandem with the social reality within which it operates. Current policy with respect
to older people, which promotes home and community-based care as its primary aim, relies on the availability and
willingness of families to accept a certain level of responsibility for the care of their older relatives. There are two
divergent views with regard to responsibility for the care of older people: one maintains that families do not have any
responsibilities and that comprehensive services provided by the State are required to fulfill long-term care needs; the
other that the family has primary responsibility for care and the State should only support those without family.
There is an urgent need to ascertain and understand the values that Irish society holds about family responsibilities
for the support and care of older people. Therefore, further research and debate is required to identify conditions under
which it is considered appropriate for families to provide care and support, and to ascertain the ways in which this type
of support can be assisted.
This has been echoed by the WHO, which noted in 2000 that it is important to pursue a national consensus that
encompasses the following goals:
• creating public programmes that provide the foundation for private sector support and co-operation;
• assuring the development of measures to provide the necessary supply of supportive resources for older people
in need of long-term care and similar support for their family caregivers by the public and private sectors;
• identifying and assigning specific responsibilities for assuring quality of care.

36

An Age Friendly Society
37
CHAPTER SIX
Towards an Age Friendly Society in Ireland

38
We the representatives of Governments, meeting at the Second World Assembly on Ageing in Madrid,
have decided to adopt an International Plan of Action on Ageing to respond to the opportunities and challenges
of population ageing in the twenty-first century and to promote the development of a society for all ages.
– Article 1 of the political declaration accompanying the Madrid International Plan of Action on Ageing
The Madrid Plan promotes a new vision of population ageing as both challenge and opportunity. It promotes
a new image of older persons with their potential to be a powerful basis for future development.
– Alexandre Sidorenko, UN Programme on Ageing, Address to Positive Ageing Conference, Farmleigh, 30 September 2004
6.1 Defining an age friendly society in Ireland
As outlined in Chapter Three, the UN and the WHO have recommended common policy and practice objectives
related to the participation, security and health of older people. The Council strongly recommends that a broad
intersectoral and cross-departmental approach be adopted to the application of these policy and practice objectives
in Ireland in order to facilitate the successful development of an age friendly society.
Our society is shaped significantly by an economic imperative which makes it very difficult to re-shape notions of
contribution, participation and human value, so it is crucial to the successful development of an age friendly society
that our core values and aspirations for older people and ourselves are adequately defined.
6.1.1 Defining values
In this regard, the Council proposes that an age friendly society should:
• promote an anti-ageist philosophy;
• be integrated;
• be needs-focused;
• be person-focused;
• be holistic;
• be flexible;
• build self-esteem and self-respect;
• facilitate choice;
• facilitate empowerment;
• promote partnership;
• aim to maximise the well-being of all.
CHAPTER SIX
Towards an Age Friendly Society in Ireland
An Age Friendly Society
39
Building on these core values, the Council proposes that the development of public policy should:
• prioritise the needs and preferences as expressed by older people themselves;
• recognise the desire of the majority of older people to remain in their own homes;
• promote the primacy of the independence of older people and of partnership approaches in planning
to meet their needs.
6.1.2 Participation
An age friendly society in Ireland will encourage the full participation and integration of all older people in our society.
In this context, the effectiveness of our policies and practices will be judged on the basis of how well they meet the
needs of our older population.
An age friendly society in Ireland will adopt a democratic approach to consumer consultation; older people will
take an active role in all decision-making processes, including how services are developed, structured or provided.
In addition, recognising the divergence of life expectancy between the sexes and the fact that the ratio of women
to men increases dramatically in the older population, an age friendly society will develop policies and practices that
are both age and gender aware.
Our age friendly society will also be a disability friendly society, given the numbers of older people who have a
disability and the numbers of people with a disability who are old. Our age and disability friendly society will do
all in its power to reduce the social and physical isolation of both older people and disabled people of all ages.
An age friendly society will only be achieved in Ireland when we subject our laws, policies, strategies and service
plans to scrutiny to ensure that the welfare of older people is taken into account before measures likely to affect
them are adopted at national, regional or local levels. The Council recommends using the UN Principles for Older
Persons to inform these age-proofing exercises.
6.1.3 Security
As part of a strategic response to population ageing in Ireland, both equitable and sustainable economic growth
and a commitment to distributive outcomes that protect older people against poverty will be required.
Social protection systems
In an age friendly society, social protection systems will adjust in response to the economic and social consequences
of demographic change. Our social protection systems must provide our older citizens with sufficient income to
maintain their self-respect and dignity.
Furthermore, given the high levels of poverty among the older population in Ireland identified in Section 2.3.2, social
welfare pensions must be indexed to net average industrial earnings and at such a rate that income poverty for those
dependent on social welfare pensions does not become institutionalised.
In addition, our age friendly society must adopt active policies to encourage people to plan for retirement in order
to avoid an unexpected drop in living standards upon ceasing paid employment.
Labour market policy
To become age friendly, our labour market must respond to the economic and social consequences of population
ageing. This will entail improving the employability of older workers, and facilitating gradual retirement through
adjustment of pension and employment systems allowing those who wish to work after age 65 to do so without
being penalised.

40
To become age friendly, our society must implement a dual strategy for tackling age discrimination in the workplace
by informing older people of their rights as workers and by making employers aware of their legal obligations.
Finally, in our age friendly society, the right to work and the right to pensions must co-exist and an older person’s
right to work will not be seen as compensation for the loss or reduction of pensions.
Life-long learning and education
In our age friendly society, the promotion of literacy and numeracy skills for older people and the provision of life-long
learning will be priorities.
In our age friendly society, information about public and private pensions, taxation and benefits, life-long learning,
training and education, healthy and active ageing will be readily available so that older people can make informed
choices about how they want to live in their third age and beyond.
6.1.4 Health
An age friendly society in Ireland will provide a continuum of care with appropriate services to meet the diverse
care needs and preferences of older people in a holistic and person-centred way. It will provide for adequate and
sustainable resourcing of the four elements in the continuum of care: self-care; community-based care; care and
case management; and long-stay care.
An age friendly society in Ireland will allocate responsibilities for providing and meeting the costs of long-term care,
whether residential or community. It will value the importance of consulting older people in the development and
implementation of new systems to plan and fund long-term care, so that their views and perspectives are heard
both nationally and locally.
Self-care
Our age friendly society will make provision for preventative and anticipatory care in the form of health promotion
and health information. In this regard, the continuation and monitoring of the implementation of Adding Years to Life
and Life to Years: A Health Promotion Strategy for Older People will be prioritised.
In addition, our age friendly society will fulfil the health, social care and welfare services information needs of older people
at the important transition times of older age: retirement; onset of illness and disability; moving from home for increased
care; and bereavement.
Community-based care
With time, older people’s ability to care for themselves at home may decline and community-based networks and
services may be required to maintain them in their own homes. To become age friendly, our society must ensure that
critical components of community-based care (health and social care assessment, support for carers, community care
services including community paramedical services, home helps, meals-on-wheels, day services, housing and transport)
are be provided.
In order to address the needs of each older person effectively, a structured assessment is necessary to both identify
a person’s difficulties or problem areas, to identify their strengths and supports, and to determine service provision that
will effectively accommodate their needs and preferences. An age friendly society in Ireland will be supported by a national
framework for the multi-disciplinary assessment of older people in acute and community care settings, to ensure that the
assessment process is standardised.

An Age Friendly Society
41
Care and case management
Frail and vulnerable older people at the margins of home and residential care require more intense assistance to remain
at home. Our age friendly society will ensure that national, regional and local policies on health and social care services for
older people embrace a care and case management approach to co-ordinated service delivery. In particular, this approach
will be introduced to co-ordinate services for people with dementia and their carers. In our age friendly society, carers
will also have a greater input into decision-making and service delivery issues.
Long-stay care
Although maintaining older people at home is in accord with the preferences of older people, it is not always feasible,
and some older people require long-stay care services. In our age friendly society, attention will be unequivocally
placed on the quality and effectiveness of long-stay care services while ensuring that older people experience both
health and social gain from these services, rather than on the provision of such services to a minimum standard.
6.2 Implementing an age friendly society in Ireland
In the Madrid Plan, the UN reminds us that implementation will require sustained action at all levels in order
to respond to the demographic changes ahead, and to mobilise the skills and energies of the older population
(para. 114). It says that implementation of the Plan also requires a political, economic, ethical and spiritual vision for
the social development of older persons and states that governments have primary responsibility for implementing
its broad recommendations (paras. 115 and 116). The Plan also highlights the fact that a necessary first step in this
regard is to mainstream ageing and the concerns of older people into national development frameworks and poverty
eradication strategies (para. 116).
6.2.1 Inclusion of ageing issues in national partnership agreements
The NCAOP therefore strongly recommends that ageing and the concerns of older people be included as a priority
in our country’s social partnership process and in future national partnership agreements. Only in this way, we
believe, will the critical issues of ageing be adequately addressed and the possibility of an age friendly society
in Ireland be secured.
6.2.2 A national strategy on ageing and older people
In addition to including ageing and the concerns of older people in the social partnership process, there is an urgent
need to develop a national co-ordinated strategy on ageing and older people to ensure the full implementation of UN,
WHO and national aspirations for the participation, security and health of older people in our society. This strategy
should address itself to the ten commitments adopted by the UNECE in 2002, as outlined in Chapter Three, and
should be grounded in informed national debate about the place of older people in our society.
To inform this debate and the development of the strategy, a national research and consultation agenda building on
the work of the Council and others must be developed. This would provide a comprehensive view of older people
in Ireland today, establish more clearly their needs and preferences, and provide all the information required to plan
properly for an ageing population.
It is advocated that the strategy adopt a life course perspective and an inter-generational approach. It is further
recommended that the strategy articulate the values and principles underpinning an age friendly society, and address
itself to overcoming the barriers to the development of an age friendly society set out in Chapter Five.
As highlighted in Chapter Five, the absence of a legislative framework can jeopardise the successful implementation
of strategic objectives. The Council, therefore, strongly recommends that the national strategy for older people be
underpinned by legislation to ensure the allocation of the resources necessary to realise strategic aims.

42
6.2.3 An age friendly health and social care framework
Within the context of a comprehensive national strategy on ageing and older people, there is a particular need to
develop a new framework for the provision of high quality, person-centred, integrated and age friendly health and
social care services for older people. This framework should maintain the same objectives for services for older
people articulated in The Years Ahead: A Policy for the Elderly as outlined in Chapter Five.
The framework should provide a clear statement of policy on health and social care services provision for our
older population, together with statements of policy on prevention, rehabilitation and standards of care. It should
also include a planning model based on the provision of a comprehensive continuum of care to ensure that
appropriate health and social care services are available to older people as required on the basis of assessed
need. The framework should provide for a single assessment process to ensure the equity, consistency and
appropriateness of services provided. A care and case management approach should be adopted throughout the
country and those core community care services required to enable older people to remain living at home for as
long as possible should be provided.
Over many years, the Council has advocated the development of a legislative framework governing the provision of
these essential services to older people as entitlements rather than – as at present – on a discretionary and unequal
basis. This legislation is required to underpin the health and social care framework, and to ensure that the requisite
funding is available to ensure successful implementation of the policy.
6.3 Conclusion
In calling for an age friendly society in Ireland, the Council does not seek preferential treatment for older people.
Rather it reiterates the UN call for a society for all ages. In such a society, parity of esteem with other citizens will be
accorded to older people. They will be treated with equal dignity and respect by the organs of the State, as well as by
their fellow citizens. Their independence will not be compromised by inequality of opportunity and their participation
in the activities of society will not be denied by differential conditions of access based on age.
Finally, in calling for an age friendly society, the Council is calling on all of us – Government, social partners, policy-
makers, service providers, family, friends, neighbours and strangers – to consider, discuss, debate and build the
sort of society we want to live in as we age. We all have a role to play in this endeavour: the creation of a truly
age friendly society in Ireland.
An Age Friendly Society
43
APPENDICES
44
Note: A full list of NCAOP publications is available from the Council’s website www.ncaop.ie. A catalogue is also available from the Council upon request.
Balanda, K. and Wilde, J., 2001. Inequalities in Mortality 1989-1998, A Report on All-Ireland Mortality Data. Dublin:
Institute of Public Health in Ireland.
Baltes, P.B. and Baltes, M., 1990. ‘Psychological perspectives on successful aging: the model of selective
optimization with compensation’ in P.B. Baltes and M. Baltes (eds) Successful Ageing: Perspectives From the
Behavioural Sciences. Cambridge: Cambridge University Press.
Baltes, P.B. and Mayer, K.U., 1999. The Berlin Aging Study: Aging From 70 to 100. Cambridge: Cambridge University
Press.
Biggs, S., 2004. ‘New ageism: age imperialism, personal experience and ageing policy’ in S. Daatland and S. Biggs
(eds) Ageing and Diversity: Multiple Pathways and Cultural Migration. Bristol: The Policy Press.
Brenner, H. and Shelley, E., 1998. Adding Years to Life and Life to Years: A Health Promotion Strategy for Older
People. Dublin: NCAOP.
Browne, C., Daly, A. and Walsh, D., 2001. Activities of Irish Psychiatric Services 2000. Dublin: Health Research Board.
Central Statistics Office, 2001. Regional Population Projections 2001-2031. Dublin: Stationery Office.
Central Statistics Office, 2002. Quarterly National Household Survey. Dublin: Stationery Office.
Central Statistics Office, 2002. Report on Vital Statistics. Dublin: Stationery Office.
Central Statistics Office, 2004. Census 2002. Dublin: Stationery Office.
Central Statistics Office, 2005. EU Survey on Income and Living Conditions (EU-SILC): First Results. Dublin:
Stationery Office.
Commission of the European Communities, 1999. Towards a Europe for All Ages: Promoting Prosperity
and Intergenerational Solidarity. Brussels: Commission of the European Communities.
Connell, P. and Pringle, D., 2004. Population Ageing in Ireland: Projections 2002-2021. Dublin: NCAOP.
Department of Health, 1988. The Years Ahead: A Policy for the Elderly. Dublin: Stationery Office.
Department of Health and Children, 2001. Quality and Fairness: A Health System for You. Dublin: Stationery Office.
Department of Health and Children, 2003. Long-Stay Activity Statistics 2002. Dublin: Stationery Office.
Department of Social and Family Affairs, 2003. Annual Report 2003. Dublin: Stationery Office.
Economic and Social Council, 2002. Berlin Ministerial Declaration: A Society for All Ages in the UNECE Region.
New York: UN.
Economic and Social Council, 2002. Regional Implementation Strategy for the Madrid International Plan of Action
on Ageing 2002. New York: UN.
ESRI, 2002. Activity in Acute Public Hospitals in Ireland 1990-1999. Dublin: ESRI.
Fahey, T. and Russell H., 2001. Older People’s Preferences for Employment and Retirement. Dublin: NCAOP.
APPENDIX ONE
References

An Age Friendly Society
45
Garavan, R., Winder, R. and McGee, H., 2001. Health and Social Services for Older People (HeSSOP).
Dublin: NCAOP.
Glendinning, C., Davies, B., Pickard, L. and Comas-Herrera, A., 2004. Funding Long-Term Care for Older People:
Lessons From Other Countries. York: Joseph Rowntree Foundation.
Government of Ireland, 2003. Sustaining Progress, Social Partnership Agreement 2003-2005.
Dublin: Stationery Office.
Jacobzone, S., 1999. Ageing and Care for Frail Elderly Persons: An Overview of International Perspectives. Labour
Market and Social Policy, Occasional Papers No. 38. Paris: OECD.
Kelleher, C., NicGabhainn, S. and Friel, S., 1998. The National Health and Lifestyle Surveys: Survey of Lifestyle,
Attitudes and Nutrition (SLÁN). Dublin: Stationery Office.
Kelleher, C., NicGabhainn, S. and Friel, S., 2002. The National Health and Lifestyle Surveys: Survey of Lifestyle,
Attitudes and Nutrition (SLÁN). Dublin: Stationery Office.
Keogh, F. and Roche, A., 1996. Mental Disorders Among Older Irish People. Dublin: NCAOP.
Layte, R., Fahey, T. and Whelan, C., 1999. Income, Deprivation and Well-Being Among Older Irish People.
Dublin: NCAOP.
McGivern, Y., 2005. From Ageism to Age Equality: Addressing the Challenges. Dublin: NCAOP.
McGlone, E. and Fitzgerald, F., 2005. Perceptions of Ageism in Health and Social Services in Ireland. Dublin: NCAOP.
Mercer Ltd, 2002. Study to Examine the Future Financing of Long-Term Care in Ireland, Undertaken by Mercer Ltd
on Behalf of the Department of Social and Family Affairs. Dublin: Stationery Office.
National Cancer Registry, 1999. Cancer in Ireland 1994-1999 With Estimates to 2002. Dublin: NCRI.
Newberger, J., 2005. The Moral State We’re In: A Manifesto for a 21st Century Society. London: HarperCollins.
Office for Social Inclusion, 2004. National Action Plan Against Poverty and Social Exclusion, First Annual Report,
Implementation of Plan 2003-2004. Dublin: Stationery Office.
O’Loughlin, A. and Duggan, J., 1998. Abuse, Neglect and Mistreatment of Older People: An Exploratory Study.
Dublin: NCAOP.
O’Shea, E. and O’Reilly, S., 1999. An Action Plan for Dementia. Dublin: NCAOP.
O’Shea, E., 2000. The Costs of Caring for People with Dementia and Related Cognitive Impairments. Dublin: NCAOP.
O’Shea, E. and Conboy, P., 2005. Planning for an Ageing Population: Strategic Considerations. Dublin: NCAOP.
Rowe, J.W. and Kahn, R.L., 1998. Successful Aging. New York: Pantheon Books.
Ruddle, H., Donoghue, F. and Mulvihill, R., 1997. The Years Ahead Report: A Review of the Implementation
of its Recommendations. Dublin: NCAOP.
Shiely, F. and Kelleher, C., 2004. Older People in Ireland: A Profile of Health Status, Lifestyle and Socio-Economic
Factors From SLÁN. Dublin: NCAOP.
The Equality Authority, 2002. Implementing Equality for Older People. Dublin: The Equality Authority.
Torres, S., 2004. ‘Making sense of the construct of successful ageing: the migrant experience’ in S. Daatland
and S. Biggs (eds) Ageing and Diversity: Multiple Pathways and Cultural Migration. Bristol: The Policy Press.
46
Treacy, P., Butler, M., Byrne, A., Drennan, J., Fealy, G., Frazer, K. and Irving, K., 2005. Loneliness and Social Isolation
Among Older Irish People. Dublin: NCAOP.
United Nations, 1948. Universal Declaration of Human Rights. New York: UN.
United Nations, 1982. Vienna International Plan of Action on Ageing. New York: UN.
United Nations, 1991. United Nations Principles for Older Persons. New York: UN.
United Nations, 1999. International Year of Older Persons Operational Framework. New York: UN.
United Nations, 2002. Madrid International Plan of Action on Ageing. New York: UN
United Nations, 2002. Report of the Second World Assembly on Ageing, Madrid, 8-12 April 2002. New York: UN.
United Nations, 2004. Human Development Report 2004 – Cultural Liberty in Today’s World. New York: UN.
Watson, D. and Williams, J., 2003. Irish National Survey of Household Quality 2001-2002. Dublin: Stationery Office.
Wistow, G., Waddington, E. and Godfrey, M., 2003. Living Well in Later Life: From Prevention to Promotion.
Leeds: University of Leeds.
Working Group on Elder Abuse, 2002. Protecting Our Future. Dublin: Stationery Office.
World Health Organisation, 2002. Active Ageing: A Policy Framework. Geneva: WHO.

An Age Friendly Society
47
Independence
1 Older persons should have access to adequate food, water, shelter, clothing and healthcare through
the provision of income, family and community support and self-help.
2 Older persons should have the opportunity to work or to have access to other income-generating
opportunities.
3 Older persons should be able to participate in determining when and at what pace withdrawal from
the labour force takes place.
4 Older persons should have access to appropriate educational and training programmes.
5 Older persons should be able to live in environments that are safe and adaptable to personal preferences
and changing capacities.
6 Older persons should be able to reside at home for as long as possible.
Participation
7 Older persons should remain integrated in society, participate actively in the formulation and implementation
of policies that directly affect their well-being and share their knowledge and skills with younger generations.
8 Older persons should be able to seek and develop opportunities for service to the community and to serve
as volunteers in positions appropriate to their interests and capabilities.
9 Older persons should be able to form movements or associations of older persons.
Care
10 Older persons should benefit from family and community care and protection in accordance with each society’s
system of cultural values.
11 Older persons should have access to healthcare to help them to maintain or regain the optimum level of physical,
mental and emotional well-being and to prevent or delay the onset of illness.
12 Older persons should have access to social and legal services to enhance their autonomy, protection and care.
13 Older persons should be able to utilise appropriate levels of institutional care providing protection, rehabilitation
and social and mental stimulation in a humane and secure environment.
14 Older persons should be able to enjoy human rights and fundamental freedoms when residing in any shelter,
care or treatment facility, including full respect for their dignity, beliefs, needs and privacy and for the right
to make decisions about their care and the quality of their lives.
Self-fulfilment
15 Older persons should be able to pursue opportunities for the full development of their potential.
16 Older persons should have access to the educational, cultural, spiritual and recreational resources of society.
Dignity
17 Older persons should be able to live in dignity and security and to be free of exploitation and physical or mental
abuse.
18 Older persons should be treated fairly regardless of age, gender, racial or ethnic background, disability or other status,
and be valued independently of their economic contribution.
APPENDIX TWO
UN Principles for Older Persons

48
The National Council on Ageing and Older People was established on 19th March 1997 in succession to the National
Council for the Elderly (January 1990 to March 1997) and the National Council for the Aged (June 1981 to January 1990).
The functions of the Council are as follows:
1 To advise the Minister for Health on all aspects of ageing and the welfare of older people, either at its own initiative
or at the request of the Minister and in particular on:
a) measures to promote the health of older people;
b) measures to promote the social inclusion of older people;
c) the implementation of the recommendations contained in policy reports commissioned by the Minister for Health;
d) methods of ensuring co-ordination between public bodies at national and local level in the planning and provision
of services for older people;
e) methods of encouraging greater partnership between statutory and voluntary bodies in providing services
for older people;
f) meeting the needs of the most vulnerable older people;
g) means of encouraging positive attitudes to life after 65 years and the process of ageing;
h) means of encouraging greater participation by older people;
i) whatever action, based on research, is required to plan and develop services for older people.
2 To assist the development of national and regional policies and strategies designed to produce health gain
and social gain for older people by:
a) undertaking research on the lifestyle and the needs of older people in Ireland;
b) identifying and promoting models of good practice in the care of older people and service delivery to them;
c) providing information and advice based on research findings to those involved in the development and/ or
implementation of policies and services pertaining to the health, well-being and autonomy of older people;
d) liaising with statutory, voluntary and professional bodies involved in the development and/or implementation
of national and regional policies which have as their object health gain or social gain for older people.
3 To promote the health, welfare and autonomy of older people.
4 To promote a better understanding of ageing and older people in Ireland.
5 To liaise with international bodies which have functions similar to the functions of the Council.
The Council may also advise other Ministers, at their request, on aspects of ageing and the welfare of older people
which are within the functions of the Council.
APPENDIX THREE
Terms of Reference
An Age Friendly Society
49
Chairperson Cllr Éibhlin Byrne
Mr Bernard Thompson Ms Mary O’Neill
Mr Eddie Wade Cllr Jim Cousins
Mr Michael Dineen Dr Ciaran Donegan
Fr Peter Finnerty Mr James Flanagan
Mr Eamon Kane Dr Michael Loftus
Mr Michael Murphy Ms Mary Nally
Mr Pat O’Toole Ms Rosemary Smith
Ms Pauline Clancy-Seymour Mr John Brady
Mr Noel Byrne Ms Kit Carolan
Dr Davida de la Harpe Mr John Grant
Dr Ruth Loane Ms Sylvia Meehan
Mr Paddy O’Brien Ms Martina Queally
Mr Bernard Thompson Mr Oliver R Cleary
Ms Annette Kelly Ms Eileen O’Dolan
Mr Paul O’Donoghue Ms Elaine Soffe
Director Bob Carroll
Membership

50
Notes

An Age Friendly Society
51
Notes

52
Notes

An Chomhairle Náisiúnta um Aosú agus Daoine Aosta
22 Cearnóg Chlann Liam Cé na Mórchanálach Baile Átha Cliath 2
Fax: 01 676 5754 website: www.ncaop.ie
National Council on Ageing and Older People
22 Clanwilliam Square Grand Canal Quay Dublin 2
Tel: 01 676 6484/5 email: [email protected]