An A- Z Guide for Working with Patients with Memory Loss and
Dementia
Slide 2
Objectives 1.Gain proficiency in brief cognitive screening to
help improve detection of memory loss among older patients
2.Describe evidence-based medication and non- medication
interventions known to improve outcomes among patients with
dementia and their care partners 3.Learn how to best support
patients and care partners in accessing services throughout the
continuum of the disease 4.Identify common health risks associated
with caregiving and address the unique needs of dementia caregivers
5.Recognize how to incorporate health equity principles into
dementia assessment, diagnosis and care 2
Slide 3
Introduction to ACT on Alzheimers
Slide 4
What is ACT on Alzheimers? statewide collaborative volunteer
driven 60+ ORGANIZATIONS 500+ INDIVIDUALS IMPACTS OF ALZHEIMERS
BUDGETARYSOCIAL PERSONAL
Slide 5
Collaborative Goals/Common Agenda 5 shared goals with a Health
Equity perspective 5
Slide 6
ACT Tool Kit Evidence- and consensus- based best practice
standards for Alzheimers care Tools and resources for: Primary care
providers Care coordinators Community agencies Patients and care
partners 6 www.actonalz.org/provider-practice-tools
Slide 7
Health Care Settings: Care Coordination
www.actonalz.org/provider-practice-tools
Slide 8
Dementia and Alzheimers 8
Slide 9
FAQ What is the difference between dementia and Alzheimers
disease?
Slide 10
Dementia Diagnoses Alzheimers disease: 60-80 % Includes mixed
AD + VD Lewy Body Dementia: 10-25 % Parkinson spectrum Vascular
Dementia: 6-10 % Stroke related Frontotemporal Dementia: 2-5 %
Personality or language disturbance
Slide 11
Alzheimers Disease: Challenges and Opportunities
Slide 12
Alzheimers: A Public Health Crisis Scope of the problem 5.3M
Americans with AD in 2015 Growing epidemic expected to impact 13.8M
Americans by 2050 and consume 1.1 trillion in healthcare spending
Almost 2/3 are women (longer life expectancy) If disease could be
detected earlier incidence would be much higher Pre-clinical stage
1-2 decades Some populations at higher risk Older African Americans
(2x as whites) Older Hispanics (1.5x as whites) 12 Alzheimers
Association Facts and Figures 2015
Slide 13
The Lens of Health Equity Take into consideration health
disparities and inequities Seek the attainment of the highest level
of health for all people Help create a new style of curb cut by
promoting cultural competence 13
Slide 14
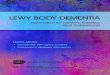
Base Rates 1 in 9 people 65+ (11%) 1 in 3 people 85+ (32%) 14
Age RangePercent with Alzheimers < 654%4% 65 -7413% 75 -8444% 85
+38% Alzheimers Association Facts and Figures 2014
Slide 15
Challenges & Opportunities AD under-recognized by providers
Only 50% of patients receive formal diagnosis Millions unaware they
have dementia Diagnosis often delayed on average by 6+ years after
symptom onset Significant impairment in function by time it is
recognized Poor timing: diagnosis frequently at time of crises,
hospitalization, failure to thrive, urgent need for
institutionalization 15 Boise et al., 2004; Boustani et al., 2003;
Boustani et al., 2005; Silverstein & Maslow, 2006
Slide 16
A population with complex care needs Indisputable correlation
between chronic conditions and costs Patients with Dementia 16 2.5
chronic conditions (average) 5+ medications (average) 3 times more
likely to be hospitalized Many admissions from preventable
conditions, with higher per person costs Alzheimers Association
Facts and Figures 2014
Slide 17
Cognitive Impairment ID
Slide 18
Practice Tips Unfortunately, most of us do not recognize signs
and symptoms until they are quite pronounced Attribution error:
What do you expect? She is 80 years old. Subjective impressions
FAIL to detect dementia in early stages Clinical interview Let
patient answer questions without help Remember: Social skills
remain intact until late stage dementia Easy to be fooled by a
sense of humor, reliance on old memories, or quiet/affable
demeanor
Slide 19
Practice Tips Red flags Chart Review: memory concerns,
forgetfulness, memory complaints; emergency contact is main
contact; Aricept / Donepezil or other ACHI in record Ask How are
you xxx? instead of Are you xxx? Repetition (not normal in 7-10 min
conversation) Tangential, circumstantial responses Losing track of
conversation Frequently deferring answers to family member Over
reliance on old information/memories Inattentive to appearance
Unexplained weight loss or failure to thrive
Slide 20
Practice Tips Family observations: ANY instances whatsoever of
getting lost while driving, trouble following a recipe, asking same
questions repeatedly, mistakes paying bills Take these concerns
seriously: by the time family report problems, symptoms have
typically been present for quite a while and are getting worse
Raise your expectation of older adults: If this patient was alone
on a domestic flight across the country and the trip required a
layover with a gate change, would he/she be able to manage that
kind of mental task on his/her own? If answer is not likely for a
patient of any age: RED FLAG
Slide 21
Practice Tips Intact older adult should be able to: Describe at
least 2 current events in adequate detail (who, what, when, why,
how) Describe events of national significance 9/11, New Orleans
disaster, etc. Name or describe the current President and an
immediate predecessor Describe their own recent medical history and
report the conditions for which they take medication
Slide 22
Cognitive Screening 22
Slide 23
Provider Perspective Avoiding detection of a serious and life
changing medical condition just because there is no cure or ideal
medication therapy seems, at worst, incredibly unethical, and, at
best, just bad medicine. George Schoephoerster, MD Family Practice
Physician 23
Slide 24
Screening Measures Wide range of options Mini-Cog (MC)
Mini-Mental State Exam (MMSE) St. Louis University Mental Status
Exam (SLUMS) Montreal Cognitive Assessment (MoCA) All but MMSE
free, in public domain, and online Borson et al., 2000; Folstein et
al., 1975; Nasreddine 2005; Tariq et al., 2006
Slide 25
Alternative Screening Tools Virtually all screening tools based
upon a euro-centric cultural and educational model Consider:
country and language of origin, type/quality/length of education,
disabilities (visual, auditory, motor) Alternative tools my be less
biased 25
Slide 26
Screening Administration Try not to: Use the words test or
memory Instead: Were going to do something next that requires some
concentration Allow patient to give up prematurely or skip
questions Deviate from standardized instructions Offer multiple
choice answers Be soft on scoring Score ranges already padded for
normal errors Deduct points where necessary be strict
Slide 27
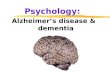
Mini-Cog Contents Verbal Recall (3 points) Clock Draw (2
points) Advantages Quick (2-3 min) Easy High yield (executive fx,
memory, visuospatial) Subject asked to recall 3 words Leader,
Season, Table Subject asked to draw clock, set hands to 10 past 11
+3 +2 Borson et al., 2000
Slide 28
28
Slide 29
29
Slide 30
Mini-Cog Pass > 4 Fail 3 or less Borson et al., 2000
Slide 31
Mini-Cog Research Performance unaffected by education or
language Borson Int J Geriatr Psychiatry 2000 Sensitivity and
specificity similar to MMSE (76% vs. 79%; 89% vs. 88%) Borson JAGS
2003 Does not disrupt workflow & increases rate of diagnosis in
primary care Borson JGIM 2007 Failure associated with inability to
fill pillbox Anderson et al Am Soc Consult Pharmacists 2008
Slide 32
Case Study: Colleen 66 y/o presents to primary care with memory
complaints Daughter c/o short-term memory is poor Began 1-2 years
ago, getting worse Hx Low blood sugar, history of heart attack,
repeat hospitalizations for atrial flutter Frequent medication
changes, managing independently Patient is a retired accountant for
family business Lives with husband who is still running the family
business Referred to Care Coordination
Slide 33
Mini-Cog: Colleen 33 http://youtu.be/DeCFtuD41WY
Slide 34
Colleens Clock
Slide 35
Colleens Score
Slide 36
Mini-Cog Exercise Form groups of 2 Administer MiniCog to each
other Score sample clocks 36
Slide 37
Clock #1
Slide 38
Clock #2
Slide 39
Clock #3
Slide 40
Clock #4
Slide 41
Clock #5
Slide 42
Clock #6
Slide 43
Clock #7
Slide 44
SLUMS Tariq et al., 2006
Slide 45
SLUMS High School DiplomaLess than 12 yrs education Pass>
27> 25 Fail26 or less24 or less 45 Tariq SH, Tumosa N, Chibnall
et al. Comparison of the Saint Louis University mental status
examination and the mini-mental state examination for detecting
dementia and mild neurocognitive disorder--a pilot study. Am J
Geriatr Psychiatry. 2006 Nov;14(11):900-10.
MoCA: Sam 52
http://youtu.be/ryf8SG0NQLQ?list=UUOPv8U5bHcdDCm4edmQDY9g
Slide 53
MoCA Scoring: Sam Interactive scoring exercise 53
Slide 54
MoCA Scoring: Sam 54
Slide 55
MoCA Scoring: Sam 55
Slide 56
MoCA Scoring: Sam 56
Slide 57
MoCA Scoring: Sam 57
Slide 58
Screening Tool Selection Montreal Cognitive Assessment (MoCA)
Sensitivity: 90% for MCI, 100% for dementia Specificity: 87% St.
Louis University Mental Status (SLUMS) Sensitivity: 92% for MCI,
100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE)
Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner
2012; Nasreddine et all, 2005; Tariq et al., 2006; Ismail et al.,
2010
Slide 59
Family Questionnaire
www.actonalz.org/pdf/Family-Questionnaire.pd f
Care and Treatment The care for patients with Alzheimers has
very little to do with pharmacology and much to do with
psychosocial interventions Care Coordination 65
Slide 66
Dementia Care Coordination 66
Slide 67
Care Coordination What are some of the challenges you face when
working with people with dementia and their families? 67
Slide 68
ACT Practice Tool
Slide 69
Dementia Care Plan Checklist
Slide 70
Identify Care Partner(s) Inform the patient that this disease
requires a team approach Ask the patient to identify team members
or care partners Be task specific (e.g., doctor visits, medication
management) Think outside the box / family (e.g., friends,
neighbors, religious congregation members, colleagues, community
organization volunteers or workers) 70
Care Plan Tool Highlights Disease Education Medication Therapy
and Management Maximize Abilities Health, Wellness and Engagement
Home & Personal Safety Legal Planning Advance Care Planning
76
Slide 77
Disease Education ASK the patient / care partner: What the
doctor told them about their memory loss / diagnosis What they know
about the disease / questions about the diagnosis / disease Biggest
concerns; barriers to care / health 77
Slide 78
Education Resources for Patients & Caregivers 78
Slide 79
Disease Education: Print Materials 79
Slide 80
After A Diagnosis -Partner with doctors -Understand the disease
-Use team approach -Plan ahead -Ask for help -Use community
resources -Role of care coordinator
http://www.actonalz.org/sites/default/file
s/documents/ACT-AfterDiagnosis.pdf
Slide 81
Disease Education 81 http://youtu.be/zEst_VxwA4U
Slide 82
Taking Action Workbook -Understanding the disease -Partnering
with doctors -Telling others about the diagnosis -Strategies for
managing symptoms & coping -Safety -Legal / financial issues
http://www.alz.org/documents/mndak/taki ng_action_workbook.pdf
Disease Education: What is AD? 86
http://youtu.be/ECbjK4Ra-Ys
Slide 87
Maximize Abilities 87 Identify / treat conditions that may
worsen symptoms or lead to poor outcomes Diabetes, HTN, sleep
dysregulation Encourage patient to stop smoking / limit alcohol
Refer to OT to maximize independence (e.g., simplify environment,
maximize independence & self-care abilities) Educate families
on communication and approach to prevent or reduce dementia-related
behavioral symptoms
Slide 88
Medication Therapy & Management 88 Discuss prescribed and
OTC medications simplify medication regimen reduce / eliminate
anticholinergics, benzodiazepines, hypnotics, narcotics Create plan
with care team Family plan for managing meds Med management aids
(pill boxes, alarms) Create & review medication log
Slide 89
Medication Therapy & Management 89
Slide 90
Health, Wellness & Engagement 90 Encourage lifestyle
changes that may reduce disease symptoms or slow progression
-Exercise -Nutrition -Stress reduction -Meaning & purpose
-Relationships -Health management -Routine
http://www.alz.org/documents/mndak/alz_living_well_workbook_2011v2_web.pdf
Slide 91
Maximize Abilities: Routine 91
Slide 92
Patient Engagement: Research Participation Alzheimers
Association Trial Match Free, easy-to-use clinical studies matching
service that connects individuals with Alzheimer's, caregivers,
healthy volunteers and physicians with current studies.
http://www.alz.org/research/clinical_trials/find
_clinical_trials_trialmatch.asp
http://www.alz.org/research/clinical_trials/find
_clinical_trials_trialmatch.asp National Institute of Health (NIH)
http://clinicaltrials.gov http://clinicaltrials.gov 92
Slide 93
Home & Personal Safety 93 Educate & develop a plan for
5 Fs: fire, falls, firearms, finances, freeways Refer to OT or PT
Fall risk assessment Sensory / mobility aids Home safety inspection
/ modifications Driving evaluation Encourage emergency plans (phone
numbers, hospital, fire, POLST/med list by bed, etc.) Encourage
enrollment in Medic Alert Safe Return
Slide 94
Role of Hospitalization More preventable hospitalizations
Higher rates of delirium, falls, new incontinence, indwelling
urinary catheters, pressure ulcers, functional decline & new
feeding tubes Significantly less likely to regain preadmission
functional abilities at 1 month, 3 months, or 1 year after
discharge 3-7 times more likely to be living in a nursing home 3
months after discharge. 94
Slide 95
Role of Hospitalization Reduce Unnecessary Hospitalization
Falls UTI / other medical conditions Medications / medication
mismanagement Dementia-related behavior Hospitalization
alternatives Hospitalization Pre-Planning
http://www.nia.nih.gov/alzheimers/publication/hosp
italization-happens
http://www.nia.nih.gov/alzheimers/publication/hosp
italization-happens
http://www.aaa1c.org/docs/healthtips/Hospital_Visi
ts_for_People_with_ALZ.pdf
http://www.aaa1c.org/docs/healthtips/Hospital_Visi
ts_for_People_with_ALZ.pdf 95
Slide 96
Legal & Advance Care Planning 96 Encourage patient / care
partner to assign health care and durable POA Refer to elderlaw
attorney Encourage patient to discuss / document preferences for
care Honoring Choices MN Healthcare Directive POLST In mid-stage,
discuss palliative and hospice options
Slide 97
Visit Frequency & Communication 97 Schedule regular
check-ins Educate patient / care partner WHEN to contact you
Changes in condition Assistance with med management Before / after
hospitalization Change in living environment New needs
Slide 98
Visit Frequency & Communication 98 Facilitate physician
appointments Reminders, transportation Educate on physician
engagement strategies Encourage care partner(s) to attend medical
appointments Educate about HIPAA, as needed Educate on use of
appointment log, medication log
Slide 99
Appointment Log
Slide 100
HIPAA Q & A HIPAA (Health Insurance Portability and
Accountability Act) Federal law that protects medical information
Allows only certain people to see information Doctors, nurses,
therapists and other health care professionals on the patients
medical team Family caregivers and others directly involved with a
patients care (unless the patient says he/she does not want this
information shared with others) 100
www.nextstepincare.org/Caregiver_Home/HIPAA/ United Hospital Fund,
2002
Slide 101
HIPAA: Sharing Patient Information If the patient is present
and has the capacity to make health care decisions, a health care
provider may discuss the patients health information with a family
member, friend, or other person if the patient agrees or, when
given the opportunity, does not object. If the patient is not
present or is incapacitated, a health care provider may share the
patients information with family, friends or others as long as the
health care provider determines, based on professional judgment,
that it is in the best interest of the patient. 101
www.nextstepincare.org/Caregiver_Home/HIPAA/ United Hospital Fund,
2002
Slide 102
Caregiver Support 102
Slide 103
Dementia Caregiving Risks Physical risks: caregiving increases
the risk of health problems Social risks: caregivers frequently
suffer from feelings of social isolation Psychological risks:
caregivers are at increased risk of depression and burden Financial
risks: caregiving places significant financial burdens on
caregivers due to lost wages and cost of care
Slide 104
Care Plan: Caregiver Support Providing support for dementia
caregivers is a societal imperative 70% of individuals with
Alzheimers disease live at home In 2012, an estimated 15 million
unpaid caregivers provided an estimated 17.5 billion hours of
unpaid care The health care system could not sustain the cost of
care without unpaid caregivers
Slide 105
Common Caregiver Challenges 105 Lack of disease knowledge /
education Emotional stress, burden Need for support and respite
Role changes Challenging family dynamics Communication difficulties
Neglected health Putting patient needs first Challenging patient
behaviors Planning for the future
Slide 106
Caregiver Support There is a strong correlation between the
health and well-being of a care partner and the quality of care
that she can provide. A care partner with a balanced outlook and
good self-care practices can provide care for longer periods of
time while maintaining his own health and well-being.
#5Connect to Resources 112 Alzheimers Association 24/7 Helpline
| 800.272.3900 www.alz.org/mnnd www.alz.org/mnnd Senior LinkAge
Line 800-333-2433 www.minnesotahelp.info
www.minnesotahelp.info
Slide 113
Case Studies 113
Slide 114
Case Study: Colleen 66 y/o presents to primary care with memory
complaints Daughter c/o short-term memory is poor Began 1-2 years
ago, getting worse Hx Low blood sugar, history of heart attack,
repeat hospitalizations for atrial flutter Frequent medication
changes, managing independently Patient is a retired accountant for
family business Lives with husband who is still running the family
business Referred to Care Coordination
Slide 115
Case Example: Medications 115 https://youtu.be/3lp0n9DOEWQ
Slide 116
Care Coordination: Colleen Discussion Observations? What did
you notice? What was done well? What could have been done
differently, better? What might you incorporate into your practice?
What recommendations / referrals would you make to Colleen? What
might you do differently if Colleen was not a native English
speaker or was from a diverse cultural community? 116
Slide 117
Case Example: Legal Planning 117
https://youtu.be/a-gIojhzGOY
Slide 118
Care Coordination: Colleen Discussion Observations? What did
you notice? What was done well? What could have been done
differently, better? What might you incorporate into your practice?
What recommendations / referrals would you make to Colleen? What
might you do differently if Colleen was not a native English
speaker or was from a diverse cultural community? 118
Slide 119
Watch the Complete Session: 119
https://youtu.be/5Kxj-5Ezlzw?list=PLGu3PyEblnIKVrTqVj9NzR5f_fcCbTd9T
Slide 120
Care Plan Exercise In small groups, develop a 3-5 step care
plan for Colleen and her family. Consider: Which areas of the care
plan tool should be incorporated in the plan? What educational
materials would you give? What referrals would you make? When would
you like to see the patient again? How would you communicate the
plan to the care team (physicians, family, patient, etc.)
Slide 121
Questions? Download ACT on Alzheimers practice tools at:
www.ACTonALZ.org/provider-practice-tools
www.ACTonALZ.org/provider-practice-tools For more information
email: [email protected]@ACTonALZ.org Web:
www.ACTonALZ.orgwww.ACTonALZ.org 121
Slide 122
Questions 122
Slide 123
Evaluation 123
Slide 124
ACKNOWLEDGEMENTS This project is/was supported by funds from
the Bureau of Health Professions (BHPr), Health Resources and
Services Administration (HRSA), Department of Health and Human
Services (DHHS) under Grant Number UB4HP19196 to the Minnesota Area
Geriatric Education Center (MAGEC) for $2,192,192
(7/1/20106/30/2015). This information or content and conclusions
are those of the author and should not be construed as the official
position or policy of, nor should any endorsements be inferred by
the BHPr, HRSA, DHHS or the U.S. Government. Minnesota Area
Geriatric Education Center (MAGEC) Grant #UB4HP19196 Director:
Robert L. Kane, MD Associate Director: Patricia A. Schommer,
MA
Slide 125
References & Resources 2012 Updated AGS Beers Criteria:
http://www.americangeriatrics.org/files/documents/beers/2012BeersCriteria_JAGS.pdf
http://www.americangeriatrics.org/files/documents/beers/2012BeersCriteria_JAGS.pdf
After a Diagnosis (ACT):
http://www.actonalz.org/sites/default/files/documents/ACT-AfterDiagnosis.pdfhttp://www.actonalz.org/sites/default/files/documents/ACT-AfterDiagnosis.pdf
Alzheimers Association Basics of Alzheimers Disease:
https://www.alz.org/national/documents/brochure_basicsofalz_low.pdfhttps://www.alz.org/national/documents/brochure_basicsofalz_low.pdf
Caregiver Notebook -
http://www.alz.org/care/alzheimers-dementia-caregiver-notebook.asphttp://www.alz.org/care/alzheimers-dementia-caregiver-notebook.asp
Driving Center:
www.alz.org/care/alzheimers-dementia-and-driving.aspwww.alz.org/care/alzheimers-dementia-and-driving.asp
Facts & Figures video:
http://youtu.be/waeuks1-3Z4http://youtu.be/waeuks1-3Z4 Facts &
Figures Report:
https://www.alz.org/facts/downloads/facts_figures_2015.pdfhttps://www.alz.org/facts/downloads/facts_figures_2015.pdf
Family Questionnaire:
http://www.alz.org/mnnd/documents/Family_Questionnaire.pdfhttp://www.alz.org/mnnd/documents/Family_Questionnaire.pdf
Know the 10 Signs.
http://www.alz.org/national/documents/checklist_10signs.pdfhttp://www.alz.org/national/documents/checklist_10signs.pdf
Living with Alzheimers Mid Stage:
https://www.alz.org/documents_custom/middle-stage-caregiver-tips.pdfhttps://www.alz.org/documents_custom/middle-stage-caregiver-tips.pdf
Living with Alzheimers Late Stage:
https://www.alz.org/documents_custom/late-stage-caregiver-tips.pdfhttps://www.alz.org/documents_custom/late-stage-caregiver-tips.pdf
Living Well
workbook:http://www.alz.org/documents/mndak/alz_living_well_workbook_2011v2_web.pdfhttp://www.alz.org/documents/mndak/alz_living_well_workbook_2011v2_web.pdf
Taking Action Workbook:
http://www.alz.org/mnnd/documents/2010_taking_action_e-book(1).pdfhttp://www.alz.org/mnnd/documents/2010_taking_action_e-book(1).pdf
Trial Match:
http://www.alz.org/research/clinical_trials/find_clinical_trials_trialmatch.asphttp://www.alz.org/research/clinical_trials/find_clinical_trials_trialmatch.asp
125
Slide 126
References & Resources AD8 Dementia Screening Interview:
http://knightadrc.wustl.edu/About_Us/PDFs/AD8form2005.pdfhttp://knightadrc.wustl.edu/About_Us/PDFs/AD8form2005.pdf
At the Crossroads:
http://www.thehartford.com/sites/thehartford/files/at-the-crossroads-2012.pdfhttp://www.thehartford.com/sites/thehartford/files/at-the-crossroads-2012.pdf
Caring for a Person with Alzheimers Disease:
http://www.nia.nih.gov/sites/default/files/caring_for_a_person_with_alzheimers_disease_0.pdf
http://www.nia.nih.gov/sites/default/files/caring_for_a_person_with_alzheimers_disease_0.pdf
Coach Broyles Playbook on Alzheimers:
http://www.caregiversunited.comhttp://www.caregiversunited.com
Honoring Choices Minnesota:
http://www.honoringchoices.orghttp://www.honoringchoices.org Health
Care Directive (MN):
http://www.ag.state.mn.us/pdf/consumer/healtcaredir.pdfhttp://www.ag.state.mn.us/pdf/consumer/healtcaredir.pdf
Hospitalization Happens:
http://www.nia.nih.gov/sites/default/files/hospitalization_happens_0.pdfhttp://www.nia.nih.gov/sites/default/files/hospitalization_happens_0.pdf
Medicare Annual Wellness Visit:
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/downloads/MM7079.pdfhttp://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/downloads/MM7079.pdf MiniCog
http://www.alz.org/documents_custom/minicog.pdfhttp://www.alz.org/documents_custom/minicog.pdf
MN Health Care Home Care Coordination Tool Kit:
http://www.health.state.mn.us/healthreform/homes/collaborative/lcdocs/cliniccarecoordtoolkit.pdf
http://www.health.state.mn.us/healthreform/homes/collaborative/lcdocs/cliniccarecoordtoolkit.pdf
Montreal Cognitive Assessment
(MoCA)http://www.mocatest.orghttp://www.mocatest.org National
Alzheimers Project Act:
http://aspe.hhs.gov/daltcp/napa/NatlPlan.pdfhttp://aspe.hhs.gov/daltcp/napa/NatlPlan.pdf
Next Step in Care:
http://www.nextstepincare.orghttp://www.nextstepincare.org
Physician Orders for Life Sustaining Treatment (POLST):
http://www.polst.orghttp://www.polst.org 126
Slide 127
References & Resources St. Louis University Mental Status
(SLUMS) examination
http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf
http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf
The Alzheimers Action
Plan:http://www.amazon.com/The-Alzheimers-Action-Plan-Know/dp/0312538715http://www.amazon.com/The-Alzheimers-Action-Plan-Know/dp/0312538715
Understanding Difficult
Behaviors:http://www.amazon.com/Understanding-Difficult-Behaviors-suggestions-
Alzheimers/dp/0978902009http://www.amazon.com/Understanding-Difficult-Behaviors-suggestions-
Alzheimers/dp/0978902009 Zarit Caregiver Burden Interview:
http://www.uconn-
aging.uchc.edu/patientcare/memory/pdfs/zarit_burden_interview.pdfhttp://www.uconn-
aging.uchc.edu/patientcare/memory/pdfs/zarit_burden_interview.pdf
127
Slide 128
References & Resources Alzheimers Association (2014).
Alzheimers Disease Facts and Figures, Alzheimers & Dementia,
Volume 10, Issue 2. Anderson K, Jue S & Madaras-Kelly K 2008.
Identifying Patients at Risk for Medication Mismanagement: Using
Cognitive Screens to Predict a Patient's Accuracy in Filling a
Pillbox. The Consultant Pharmacist, 6(14), 459-72. Barry PJ,
Gallagher P, Ryan C, & Omahony D. (2007). START (screening tool
to alert doctors to the right treatment)--an evidence-based
screening tool to detect prescribing omissions in elderly patients.
Age and Ageing, 36(6): 632-8. Blendon RJ, Benson JM, Wikler, EM,
Weldon, KJ, Georges, J, Baumgart, M, Kallmyer B. (2012). The impact
of experience with a family member with Alzheimers disease on views
about the disease across five countries. International Journal of
Alzheimers Disease, 1-9. Boise L, Neal MB, & Kaye J (2004).
Dementia assessment in primary care: Results from a study in three
managed care systems. Journals of Gerontology: Series A; Vol 59(6),
M621-26. Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A.
(2000). The mini-cog: a cognitive vital signs measure for dementia
screening in multi-lingual elderly. Int J Geriatr Psychiatry,
15(11):1021-1027. Borson S, Scanlan JM, Chen P, Ganguli M. (2003).
The Mini-Cog as a screen for dementia: validation in a
population-based sample. J Am Geriatr Soc;51(10):1451-1454. Borson
S, Scanlan J, Hummel J, Gibbs K, Lessig M, & Zuhr E (2007).
Implementing Routine Cognitive Screening of Older Adults in Primary
Care: Process and Impact on Physician Behavior. J Gen Intern Med;
22(6): 811817. Boustani M, Peterson B, Hanson L, et al. (2003).
Systematic evidence review. Agency for Healthcare Research and
Quality; Rockville, MD: Screening for dementia. Boustani M,
Callahan CM, Unverzagt FW, Austrom MG, Perkins AJ, Fultz BA, Hui
SL, Hendrie HC (2005). Implementing a screening and diagnosis
program for dementia in primary care. J Gen Intern Med. Jul;
20(7):572-7. Ferri CP, Prince M, Brayne C, et al. (2005).
Alzheimers Disease International Global prevalence of dementia: A
Delphi consensus study. Lancet, 366: 21122117. 128
Slide 129
References & Resources Finkel, SI (Ed.) (1996). Behavioral
and Psychological Signs of Dementia: Implications for Research and
Treatment. International Psychogeriatrics, 8(3). Folstein MF,
Folstein SE, & McHugh PR (1975). "Mini-mental state". A
practical method for grading the cognitive state of patients for
the clinician. J Psychiatr Res, Nov 12(3):189-98. Gallagher P &
OMahony D (2008). STOPP (Screening Tool of Older Persons
potentially inappropriate Prescriptions): Application to acutely
ill elderly patients and comparison with Beers criteria. Age and
Ageing, 37(6): 673-9. Gitlin LN, Kales HC, Lyketsos CG, & Plank
Althouse E (2012). Managing Behavioral Symptoms in Dementia Using
Nonpharmacologic Approaches: An Overview. JAMA, 308(19): 2020-29.
Holroyd S, Turnbull Q, & Wolf AM (2002). What are patients and
their families told about the diagnosis of dementia? Results of a
family survey. Int J Geriatr Psychiatry, Mar;17(3):218-21. Ismail
Z, Rajji TK, & Shulman KI (2010). Brief cognitive screening
instruments: An update. Int J Geriatr Psychiatry, 25:11120. Jeste
DV, Blazer D, Casey D et al. (2008). ACNP White Paper: Update on
Use of Antipsychotic Drugs in Elderly Persons with Dementia.
Neuropsychopharmacology, 33(5): 957-70. Larner AJ (2012). Screening
utility of the Montreal Cognitive Assessment (MoCA): In place of or
as well as the MMSE? Intern Psychogeriatrics, 24, 391396. Lin JS,
OConnor E, Rossom RC, Perdue LA, Burda BU, Thompson M, &
Eckstrom E (2014). Screening for Cognitive Impairment in Older
Adults: An Evidence Update for the U.S. Preventive Services Task
Force. Agency for Healthcare Research and Quality, Evidence
Syntheses, 107. Long KH, Moriarty JP, Mittelman MS, & Foldes SS
(2014). Estimating The Potential Cost Savings From The New York
University Caregiver Intervention In Minnesota. Health Affairs,
33(4), 596-604. McCarten JR, Anderson P Kuskowski MA et al. (2012).
Finding dementia in primary care: The results of a clinical
demonstration project. J Am Geritr Soc;60(2):210-217. 129
Slide 130
Mittelman MS, Haley WE, Clay OJ, & Roth DL (2006).
Improving caregiver well-being delays nursing home placement of
patients with Alzheimer disease. Neurology, November 14(67 no. 9),
1592-1599. Nasreddine ZS, Phillips NA, Bdirian V, Charbonneau S,
Whitehead V, Collin I, Cummings JL, & Chertkow H. (2005). The
Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For
Mild Cognitive Impairment. J Amer Ger Soc, 53(4), 695- 99. National
Chronic Care Consortium and the Alzheimers Association. 1998.
Family Questionnaire. Revised 2003. Silverstein NM & Maslow K
(Eds.) (2006). Improving Hospital Care for Persons with Dementia.
New York: Springer Publishing CO. Tariq SH, Tumosa N, Chibnall JT,
Perry MH, & Morley E. (2006). Comparison of the Saint Louis
University mental status examination and the mini-mental state
examination for detecting dementia and mild neurocognitive
disorder: A pilot study. Am J Geriatr Psychiatry,
Nov;14(11):900-10. Turnbull Q, Wolf AM, & Holroyd S (2003).
Attitudes of elderly subjects toward truth telling for the
diagnosis of Alzheimers disease. J Geriatr Psychiatry Neurol,
Jun;16(2):90-3. Zaleta AK & Carpenter BD (2010).
Patient-Centered Communication During the Disclosure of a Dementia
Diagnosis. Am J Alzheimers Dis Other Demen, 25, 513. 130 References
& Resources