Embed Size (px)
Citation preview

1320
BRIEF REPORT
AMYLOID ARTHROPATHY IN A PATIENT WITH PSORIASIS AND AMY LOIDOSIS
ROBERT FRIEDMAN, BERTRAM AGUS, and ELIZABETH AMES
Amyloid is a homogeneous extracellular eosin- ophilic material that deposits in joints and displays fibrillar structure when examined in the electron mi- croscope. A variety of different proteins may form amyloid fibrils. In multiple myeloma, immunoglobulin light chains deposited as amyloid may be seen in synovial tissue ( 1 ) . In rheumatoid arthritis and other chronic inflammatory diseases, amyloid is composed of a unique protein termed AA (2). While AA amyloid is widely deposited in blood vessels, it is not usually found outside blood vessels in the joints of patients with amyloidosis and rheumatoid arthritis (3).
We have recently studied an unusual patient who developed arthritis and amyloidosis after having suffered from psoriasis for 20 years. Her knee effu- sions were examined for amyloid by means of electron microscopy. No fibrils were seen. A synovial biopsy subsequently demonstrated AA amyloid deposited in the connective tissue, as well as in blood vessels of the synovium revealed by immunohistochemical examina- tion. We believe this is the first report of amyloid arthropathy complicating psoriatic arthritis.
Case Report. The patient, a 58-year-old white woman, was admitted to the Dermatology Service
From the Departments of Medicine and Pathology and the Division of Rheumatology, New York University Medical Center, 550 First Avenue, New York, N Y 10016.
Supported by grant #AM07176 from the National Institutes of Health.
Robert Friedman, MD: formerly a Fellow in the Division of Rheumatology; Bertram Agus, MD; Elizabeth Ames, MD.
Address reprint requests to Robert Friedman, MD, Palm Beach Medical Group, 705 North Olive Avenue, West Palm Beach, FL 33402.
Submitted for publication October 27, 1980; accepted in revised form April 9, 1981.
for treatment of psoriasis, psoriatric arthritis, and diarrhea. She developed psoriasis in her 20s and was treated briefly with corticosteroids and then with topical tar applications. Four years before admission, she noted morning stiffness in her hands, knees, and ankles lasting about an hour which improved when she took 6-10 aspirin a day. Within 2 years, she required a cane because of her knee pain. She noted increasing stsness in her hands. Her psoriasis also appeared more frequently and extensively. A year prior to admission, she was treated for her arthritis with 6 gm of aspirin a day and with indomethacin (50 mg a day) but developed loose stools alternating with constipa- tion. The psoriasis remained unimproved despite ste- roids and tar. Indomethacin was stopped, but her diarrhea persisted. She was admitted for treatment.
Physical examination revealed a chronically ill white woman with extensive psoriatic plaques on her legs and arms and with pitting of her nails. On abdomi- nal examination, the liver measured 15 cm in span and the spleen was enlarged. Synovial thickening of her wrists, metacarpophalangeal and proximal interpha- langeal joints of her hands, and knees was noted. Shoulders showed limited range of motion. No synovi- a1 thickening was apparent on examination of the shoulders, and no shoulder pad sign was present. A small effusion of the right knee was present.
Laboratory results showed a hematocrit of 30%, mean corpuscular volume of 66, and an erythro- cyte sedimentation rate of 80. White blood cell count, differential, and platelet count were normal. The pe- ripheral blood smear revealed a significant microcyto- sis and hypochromia. Stool exam was positive for occult blood. A urinalysis showed a trace of protein. A 24-hour urine specimen contained 2.5 gm of protein,
Arthritis and Rheumatism, Vol. 24, No. 10 (October 1981)

BRIEF REPORTS 1321
none of which had the characteristics of Bence-Jones protein. Serum creatinine was 0.8 mg/dl, albumin was 3.1, and cholesterol was 180 mg/dl. Serum protein electrophoresis revealed no monoclonal peak. and o n immunoelectrophoresis there was only a slight in- crease of IgM levels. Antinuclear antibody. latex fixation test, and complement levels were normal. A bone marrow examination showed a slight increase in plasma cells.
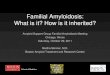
Chest roentgenograms showed cardiomegaly. X-ray films of her feet and hands exhibited character- istic changes of psoriatic arthritis; knee roentgeno- grams were normal. A diffuse ulcerative process in- volving the ceciim and the ascending and transverse Figure 1 . Paraffin section of synovial tissue denionstrating green
birefringence of amyloid deposits in the interstitiuni (arrows) C o n p ~ colon was demonstrated by barium enema. Multiple red staining pol:iriied light (magnification x 5 0 0 ) . biopsies of the colon from ulcerated and non-ulcerated
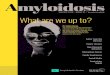
A B Figure 2. A, Frozen section of synovial tisstie denionstrating metachromasia of amyloid deposits in the interstitiuni (arrows). Crystal violet stain (magnification x 650). R. I’arallel section reacted with anti-AA antiserum depicting fluorescence of amyloid deposils (arrows) (magnification x 530).

1322 BRIEF REPORTS
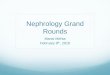
A B Figure 3. A, Frozen section showing rnetachromasia of deposits in the wall of an arteriole (arrows). Crystal violet stain (magnification x 1,700). B, Parallel section reacted with anti-AA antiserum demonstrating fluorescence of amyloid deposits (arrows) (magnification x 2.250).
areas in the hepatic flexure, sigmoid colon, and rectum revealed a pale eosinophilic material deposited in the interstitium and the vessel walls of the lamina propria and submucosa when stained with hemotoxylin and eosin. The material exhibited crystal violet metachro- masia consistent with amyloid. A punch biopsy from abdominal skin not affected by psoriasis revealed aniyloid in the papillary dermis.
The right knee was then examined for amyloid. Aspirated fluid from the knee was cloudy, with a good mucin clot. The fluid contained 800/mm3 white blood cells, all of which were polymorphonuclear leuko- cytes. The fluid did not stain with Congo red. Paraffin sections of synovial tissue showed, in addition to predominantly plasmacytic infiltrate in the intersti- tium, amorphous deposits in vessels and in the intersti- tiurn which demonstrated green birefringence on po- larization of Congo red-stained sections (Figure l ) and were metachromatic with crystal violet stain. Parallel frozen sections of synovial tissue were examined for amyloid proteins by immunofluorescence and crystal violet stain. Deposits in the interstitiurn and arteriolar
walls, which showed crystal violet metachromasia (Figures 2A and 3A), also demonstrated strong fluo- rescent staining when incubated with rabbit anti-AA protein antiserum (kindly provided by Dr. Edward Franklin) and fluorescein-conjugated goat anti-rabbit Ig (Behring) (Figures 2B and 3B). Additional parallel sections incubated with fluorescein-conjugated goat anti-human kappa and lambda light chains (Rehring) did not fluoresce.
Discussion. Amyloidosis is an unusual compli- cation of psoriasis. In a large series of psoriatic patients, the incidence was found to be 0.4% (4). Four other patients described with amyloidosis developed gastrointestinal symptoms and arthritis after pro- longed therapy with systemic and topical corticoste- roids for their psoriasis. Their arthritis was symmetric, seronegative, and polyarticular (5-7). One of these patient’s joints was examined post mortem, but the details of histologic examination were not reported ( 5 ) . Diarrhea and gastrointestinal involvement are uncom- mon in secondary amyloidosis but were the presenting features of patients with psoriatic arthritis and amy-

BRIEF REPORTS 1323
loidosis. I t cannot be determined from the other re- ported cases if amyloid arthropathy was present.
Amyloid arthropathy, an unusual complication of multiple myeloma, may also occur in patients with long-standing psoriasis. Differentiating amyloid ar- thropathy from psoriatic arthritis is difficult without performing a synovial biopsy. l h i s difference, as we learned from this patient, is important. Her arthritis was unimproved despite treatment with aspirin or indomethacin. Her diarrhea and arthritis symptoms responded well to small doses of codeine. Thus , the recognition of amyloid arthropathy in patients with psoriasis may help determine optimal therapy.
ACKNOWLEDGMENTS
The authors wish to thank Drs. Edward Franklin, Gloria Gallo, and Gerald Weissmann for their constructive criticism.
REFERENCES 1. White GC, 11, Jacobson RJ, Binder KA, Linke ZP,
Glenner GG: Immunoglobulin D myeloma and amyloid- osis: immunochemical and structural studies of Bence Jones and amyloid fibrillar proteins. Blood 46:713-722, 1975
2. Levin M, Franklin EC, Frangione €3: The amino acid sequence of a major non-immunoglobulin component of some amyloid fibrils. J Clin Invest 51:2773-2776, 1972
3. Cohen AS: Amyloidosis, Arthritis and Allied Conditions. Edited by DJ McCarty. Philadelphia, Lea & Febiger, 1979, pp 906-919
4. Larnbert JR, Ansell BM. Sephenson E, Wright V: Clinics in rheumatic diseases. Philadelphia, W.B. Saunders. 1976, p 339
5 . Berger P: Amyloidosis complicating pustular psoriasis. Br Med J 2:351-353, 1969
6. Ferguson A, Downie WW: Gastrointestinal amyloidosis in psoriatic arthritis. Ann Rheum Dis 27:245-247. 1968
7. Qureshi MS, Sandle GI, Kell JK, Fox H: Amyloidosis complicating psoriatic arthritis. Br Med J 2:302, 1977