Endoscopic appearance: Early cancers: superficial plaque,
nodule, or ulceration Advanced lesions: strictures, ulcerated
masses, circumferential masses, or large ulcerations
Slide 4
Preoperative staging is warranted in patients who are
considered to be surgical candidates (can help to take someone off
the table). If distant metastases are not demonstrated by CT or
PET, upper EUS allows a more detailed evaluation of locoregional
disease extent (T and N stage).
Slide 5
Modified from AJCC Cancer Staging Manual. 7 th ed. 2010.
Distant metastases including extraregional lymph node spread
(including paraaortic or mesenteric) Malignant celiac nodes*
Unresectable primary disease including invasion of the aorta,
trachea, heart, great vessels, or presence of TE fistula Cervical
esophageal tumors with infiltration into prevertebral fascia or
posterior larynx, invasion of the membranous trachea to the level
of the carina, or significant bilateral encasement of major
neurovascular structures
Slide 9
In a meta-analysis of 2558 patients, pooled sensitivity and
specificity of EUS to diagnose T4 were 92.4% and 97.4%. FNA
increases sensitivity of EUS to diagnose N stage from 84.7% to
96.7%. (World J Gastroenterol 2008; 14(10): 1479-1490.)
Slide 10
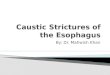
Endosonographic criteria suggestive of malignant involvement of
lymph nodes include: Width greater than 10 mm Round shape Smooth
border Echo-poor pattern When all four suspicious features are
present in a lymph node, there is an 80-100% chance of metastatic
involvement. Only 25% of malignant nodes have all four features.
Lymph node involvement supports the selection of induction
chemoradiotherapy over surgery alone, particularly in T2 disease.
EUS-FNA appears to improve accuracy of N staging as long as the
primary tumor is not in the pathway of the aspiration needle.
Slide 11
Instrument cannot traverse a tumor- induced stenosis (affects
30% of patients), leading to understaging because the entire lesion
and the celiac axis are not seen Lymph node assessment in the
immediate vicinity of the tumor is restricted
Slide 12
Among expert endosonographers (>75 esophageal cancer
examinations): Overstaging occurs in 8-14% of patients, more often
with T2 lesions (peritumoral inflammation leading to overestimation
of mural penetration?) Understaging in 3-15% of cases, more often
with T3 tumors with microscopic infiltration of the adventitia
beyond resolution capability of the echoendoscope Gatrointest
Endosc 1996; 7: 162. Surg Endosc 1999; 13: 894. Endoscopy 1992; 24
Suppl 1: 324.
Slide 13
Accuracy of EUS for restaging after chemoradiation is poor
Thought to be due to inability to differentiate between residual
tumor and post-treatment inflammation and fibrosis Detection of
locoregional recurrence EUS has sensitivity and specificity >92%
and >96% for detecting locoregional relapse in patients with
worrisome signs or symptoms that have a negative endoscopic and
radiographic evaluation EUS surveillance of resected patients every
6 months for 2 years has been shown to have a strong positive
predictive value (92%) for tumor recurrence, and two-thirds with
EUS-shown relapse were asymptomatic at the time. BUT, has not been
shown that early detection of tumor recurrence improves
survival.