Embed Size (px)
Citation preview

Antimicrobial resistance in Africa1 |
AMR in AFRICA
Dr Marc SprengerDirector
AMR Secretariat
Antimicrobial resistance in Africa2 |
AMR in AFRICA
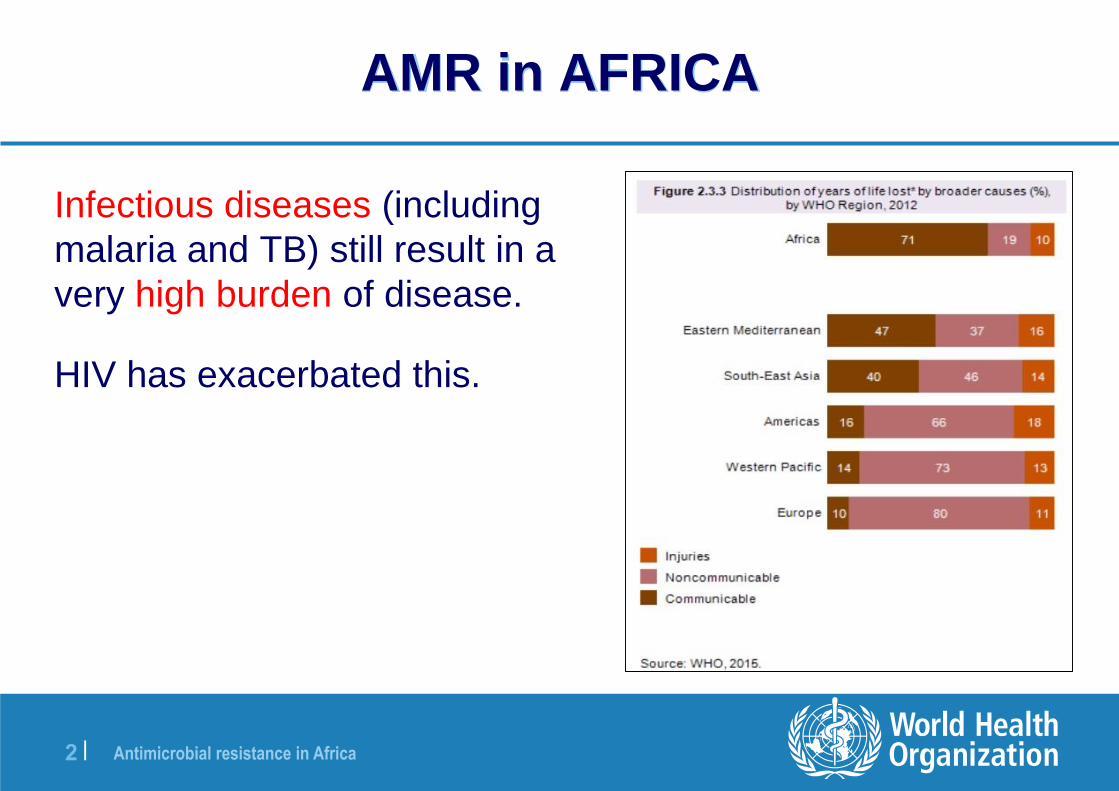
Infectious diseases (including
malaria and TB) still result in a
very high burden of disease.
HIV has exacerbated this.

Antimicrobial resistance in Africa3 |
Why AMR is an issue in Africa
Massive progress against
the MDG
Africa has made huge gains
against priority health
problems
Access to cheap, effective
antibiotics has supported all
of this
These gains are vulnerable
if antibiotics less effective
Av % Reduction Africa 1990-2013
54.2% Child mortality
40.7% Maternal mortality ratio
42% Malaria incidence
57% HIV prevalence
31%TB mortality
Antimicrobial resistance in Africa4 |
Why AMR is a challenge in AfricaWeak health systems
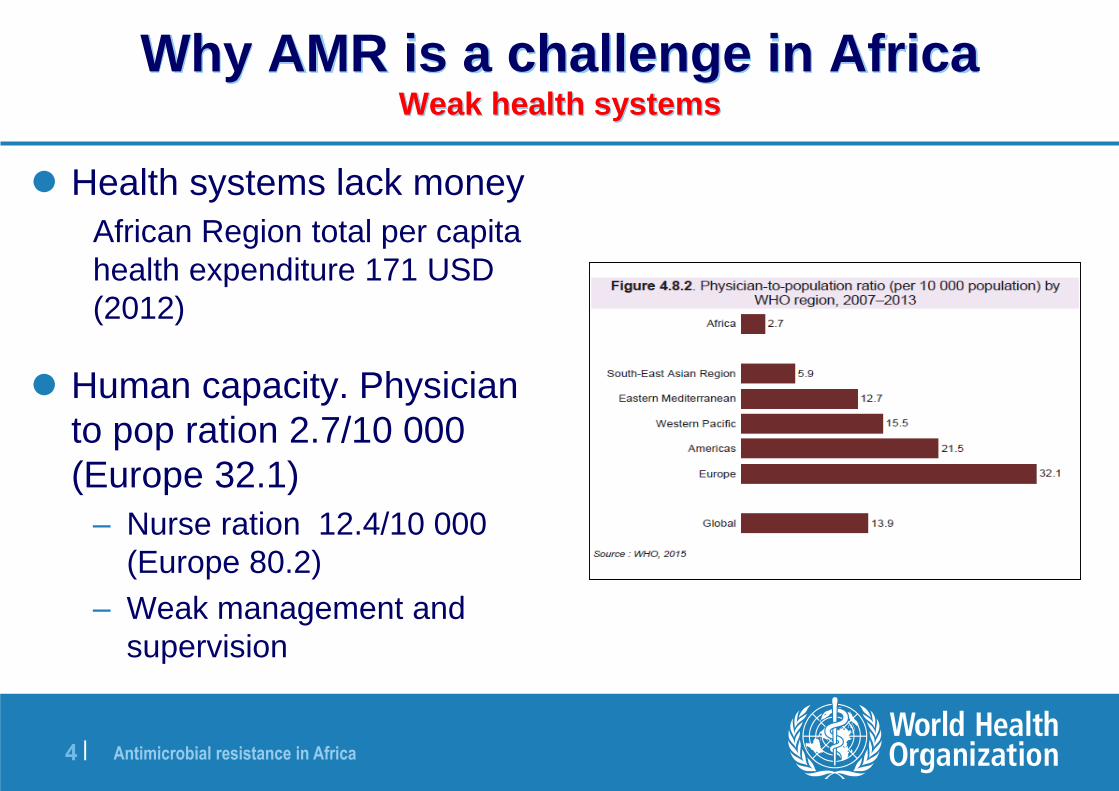
Health systems lack money
African Region total per capita
health expenditure 171 USD
(2012)
Human capacity. Physician
to pop ration 2.7/10 000
(Europe 32.1)
– Nurse ration 12.4/10 000
(Europe 80.2)
– Weak management and
supervision
Antimicrobial resistance in Africa5 |
Why AMR is a challenge in AfricaWeak health systems
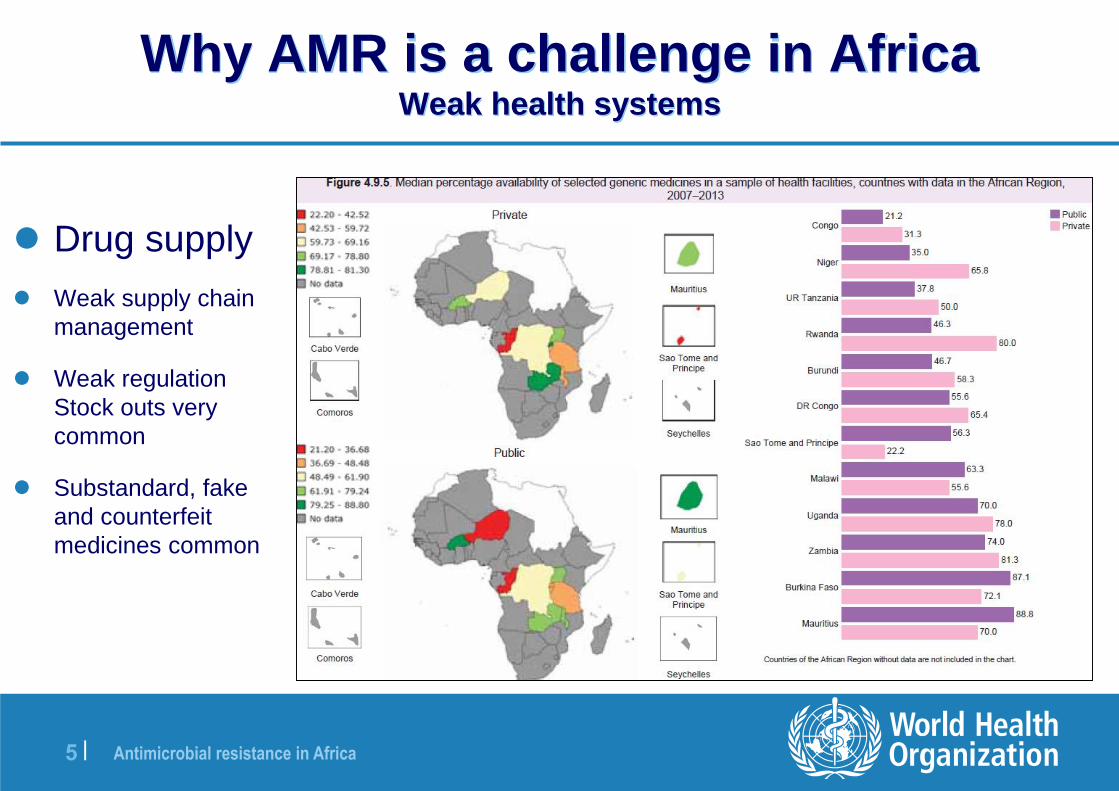
Drug supply
Weak supply chain
management
Weak regulation
Stock outs very
common
Substandard, fake
and counterfeit
medicines common

Antimicrobial resistance in Africa6 |
Why AMR is an issue in Africa
People more vulnerable to infection (Malnutrition, HIV)
People have a huge appetite for antibiotics
• Belief in antibiotics as ‘strong medicine`
• High consumption rates (although still much unmet need)
• % Respondents that have consumed antibiotics in the last month
(WHO 2015): Egypt 54%; Sudan 49%; Nigeria 40%; S Africa 31%

Antimicrobial resistance in Africa7 |
Antibiotics – A substitute for better care
Cheap Accessible antibiotics have allowed progress,
despite very weak systems and poor care.
(50% hospital births are in a facility without basic water, sanitation and hygiene)
– Poor diagnosis (unskilled staff, weak labs)
– Very weak Infection prevention and control
– Treatment very variable, non standard.
But if the bugs become resistant and the drugs more
resistant, health care becomes much more risky, and
universal coverage much harder to achieve.

Antimicrobial resistance in Africa8 |
Why AMR is an issue in Africa
High rates, and total disease burden

Antimicrobial resistance in Africa9 |
Why AMR is NOT an issue in Africa
Other Priorities
Ebola, Yellow Fever, political instability, drought etc. etc.
Lack of Awareness
Little data on AMR in Africa
Lots of other reasons for treatment failure
First Steps not Clear
Doing something about it is perceived to be difficult and
costly

Antimicrobial resistance in Africa10 |
DATA is PATCHY
Available National Data* on Resistance for Nine
Selected Bacteria/Antibacterial Drug Combinations, 2013

Antimicrobial resistance in Africa11 |
What we do know
Available data suggests major problem, although published
studies may not be representative of general population
– 59% of Central African children under 5 years, are asymptomatic
carriers of extended-spectrum β-lactamase-producing
Enterobacteriaceae (ESBL-E); one of the highest prevalence
ever described in the world.
– Ecoli resistance to Aminopenicillins 80% S Africa, 88% Kenya
– Tanzania Resistance of Strep Pneumoniae, to Trimethoprim
Sulphamethexazole in children under 5 increased from 25% in
2006 to 80% in 2012
– High rates of resistance seen by MSF in rural Niger

Antimicrobial resistance in Africa12 |
Trends and Drivers
Prosperity and urbanisation
• Increasing reliance on the largely unregulated private
market (quacks and traditional healers to hospitals)
• Increasing use of poor quality drugs and diagnostics.
• Very poor environmental sanitation
• Increasing demand for cheap meat and more intensive
agriculture

Antimicrobial resistance in Africa13 |
What needs to happen : GAP in AFRICA
1. Awareness
Political commitment to act
Change of mind-set (Population & HCW)
2. EvidenceBetter surveillance data to inform prescribing and advocacy
3. Infection prevention and control
Improve WASH in communities and health facilities
Increase Immunisation (esp Pneumoccocus, rotavirus etc)
Hand washing, cleaning and IPC practices

Antimicrobial resistance in Africa14 |
What needs to happen : GAP in AFRICA
4. Responsible Use
Improve adherence to (local) treatment guidelines
Improve Drug supply of first line drugs
Improve Regulation systems
Phase out use in agriculture for growth promotion and mass prophylaxis
5. Investment and New Products
Mainstream AMR into Health and agriculture sector development
programmes
African needs reflected in New product development and TPP

Antimicrobial resistance in Africa15 |
Progress :
National Action Plans
NAPS Developed
S Africa, Ethiopia, Ghana, Kenya, Zambia, Guinea-Bissau
Under development
Tanzania, Mozambique, Zimbabwe, Liberia, Swaziland, Cote
d'Ivoire

Antimicrobial resistance in Africa16 |
Progress : Surveillance
19 countries trained in methodology for assessing total
consumption
8 countries attending GLASS workshop
7 expressed interest for GLASS
Antimicrobial resistance in Africa17 |
WHO Response
• Close collaboration between AFRO and HQ
• Joint programming health systems & security teams
• Ali Yahaya is focal point, working closely with Jean Bosco
• Additional resource via Fleming fund (primarily for NAPs)
• 20 Countries have national focal points essential medicines
• Incorporated into Country assessments for emergency
preparedness (GHSA and JEE)
Antimicrobial resistance in Africa18 |
Take Home Message
Political support & engagement needed for the fight against
AMR
Developing a NAP is going through a multisectoral process
and should result in implementation
Without good health systems no AMR control

Antimicrobial resistance in Africa19 |
THANK YOUTHANK YOU