Embed Size (px)
Citation preview

AMOEBIASISAMOEBIASIS

HISTORYHISTORY 2yr 10mo girl2yr 10mo girl Main Complaint:Main Complaint:
7 days of loose, bloody diarrhoea and vomiting7 days of loose, bloody diarrhoea and vomiting Lethargic and doesn’t feed wellLethargic and doesn’t feed well
Previous history:Previous history: Uneventful perinatal historyUneventful perinatal history No previous admissions to hospitalNo previous admissions to hospital Numerous clinic visits in preceding months for diarrhoeaNumerous clinic visits in preceding months for diarrhoea RVD status unknownRVD status unknown No TB or other infectious contactsNo TB or other infectious contacts No recent travel history / No significant family historyNo recent travel history / No significant family history DIETDIET: Never breastfed , Feeds on a family diet that includes : Never breastfed , Feeds on a family diet that includes
mainly veg protein and carbohydrates. Denies traditional mainly veg protein and carbohydrates. Denies traditional medicine ingestion. medicine ingestion.

EXAMINATIONEXAMINATION
Growth paramoetersGrowth paramoeters:: WeightWeight: 11kg - : 11kg - 73%73% of expected for age of expected for age LengthLength: 86cm – Below 3: 86cm – Below 3rdrd centile centile Head CircHead Circ: 48cm – On 50: 48cm – On 50thth centile centile Weight for heightWeight for height: Just below 3: Just below 3rdrd centile centile
TempTemp: 37.1 : 37.1 HRHR:135bpm :135bpm RRRR:42/m :42/m BPBP:70mmHg syst:70mmHg syst Distressed, ill-looking, pale, 7.5% dehydratedDistressed, ill-looking, pale, 7.5% dehydrated Chest, CVS & CNS: NormalChest, CVS & CNS: Normal

EXAMINATIONEXAMINATION
Abdomen:Abdomen: Soft, distended abdomen with decreased bowel soundsSoft, distended abdomen with decreased bowel sounds 3cm hepatomegaly – Firm, sharp edge, smooth surface 3cm hepatomegaly – Firm, sharp edge, smooth surface
non-displaced and not tender. non-displaced and not tender. Fullness possibly a mass lesion extending from R flank Fullness possibly a mass lesion extending from R flank
across midline & tender to touch.across midline & tender to touch. Normal hernial orifices and female genitaliaNormal hernial orifices and female genitalia
PRPR:: No exterior abnormalities notedNo exterior abnormalities noted
Irregular rectal mucosaIrregular rectal mucosa
Bloody, foul-smelling diarrhoea mixed with pus notedBloody, foul-smelling diarrhoea mixed with pus noted

SPECIAL SPECIAL INVESTIGATIONSINVESTIGATIONS
FBC:FBC: WCC: 3.12WCC: 3.12 Hb: 9.5Hb: 9.5 MCV: 80.1MCV: 80.1 Platelets: 127Platelets: 127 DiffDiff: Neut: 42.7%: Neut: 42.7%
Mono: 17.8%Mono: 17.8%
Lymph: 35.7%Lymph: 35.7%
Eosino: 1.8%Eosino: 1.8%
SmearSmear: Left shift + toxic : Left shift + toxic granulation.granulation.
CRP:CRP: 337 337
U&E:U&E: 129 / 2.6 / 91 / 24 / 3.4 / 38129 / 2.6 / 91 / 24 / 3.4 / 38
LFT:LFT: Tbili: 13 Cbili: 1Tbili: 13 Cbili: 1 TP: 46 Alb: 17 Glob: 29TP: 46 Alb: 17 Glob: 29 ALP: 54 GGT: 32ALP: 54 GGT: 32 ALT: 68 AST:81ALT: 68 AST:81
Urine culture: Urine culture: Negative Negative Stool culture:Stool culture: Negative Negative Blood culture:Blood culture: Negative Negative RVD Elisa:RVD Elisa: Positive Positive CD4:CD4: 188 (4.62%) 188 (4.62%) TB W/Up:TB W/Up: Negative Negative

SPECIAL SPECIAL INVESTIGATIONSINVESTIGATIONS
AXR:AXR: Distended loops of large Distended loops of large
bowel with air fluid levelsbowel with air fluid levels No free air notedNo free air noted
Abd. Sonar:Abd. Sonar: Aperistaltic thickened loops Aperistaltic thickened loops
of bowel in RFIof bowel in RFI No mass seenNo mass seen
CT Abdomen:CT Abdomen: Fluid-filled large & small Fluid-filled large & small
bowel loopsbowel loops Closely related bowel loops Closely related bowel loops
in RFI – bowel wall in RFI – bowel wall thickeningthickening
No definite mass seenNo definite mass seen
Sigmoidoscopy:Sigmoidoscopy: Mass seen at recto-sigmoid Mass seen at recto-sigmoid
junction – biopsy takenjunction – biopsy taken
Histology:Histology: Rectal biopsy with extensive Rectal biopsy with extensive
mucosal ulceration.mucosal ulceration. Marked inflammatory cell Marked inflammatory cell
infiltrate composed infiltrate composed predominantly of chronic predominantly of chronic inflamm. cells and fibrin inflamm. cells and fibrin depositiondeposition
Amoebae noted and Amoebae noted and confirmed with PAS confirmed with PAS stainstain..

SUMMARY & MANAGEMENTSUMMARY & MANAGEMENT
2yr 10mo girl with2yr 10mo girl with ImmunosuppressionImmunosuppression Amoebic proctitis and a chronic Amoebic proctitis and a chronic
inflammatory mass at the recto-sigmoid inflammatory mass at the recto-sigmoid junction consistent with an amoebomajunction consistent with an amoeboma. .
Treated with oral MetronidazoleTreated with oral Metronidazole Optimized general condition in terms of Optimized general condition in terms of
nutritionnutrition Referred for initiation of HAARTReferred for initiation of HAART

AMOEBIASISAMOEBIASIS

The OrganismThe Organism
4 species of Entamoeba:4 species of Entamoeba: Nonpathogenic: E. dispar, E. coli, E. hartmanniNonpathogenic: E. dispar, E. coli, E. hartmanni Pathogenic: E. histolytica Pathogenic: E. histolytica
amoebiasis = A Parasitic infection caused by the protozoon amoebiasis = A Parasitic infection caused by the protozoon Entamoeba histolyticaEntamoeba histolytica
22ndnd to Malaria as protozoan cause of death worldwide to Malaria as protozoan cause of death worldwide
10% of world’s population infected – Increased prevalence in 10% of world’s population infected – Increased prevalence in developing countries (up to 25%)developing countries (up to 25%)
In SA – More common in KZNIn SA – More common in KZN
Factors contributing to faecal-oral spread:Factors contributing to faecal-oral spread: Poor educationPoor education Poverty and overcrowdingPoverty and overcrowding Unsanitary conditionsUnsanitary conditions HIV infection HIV infection

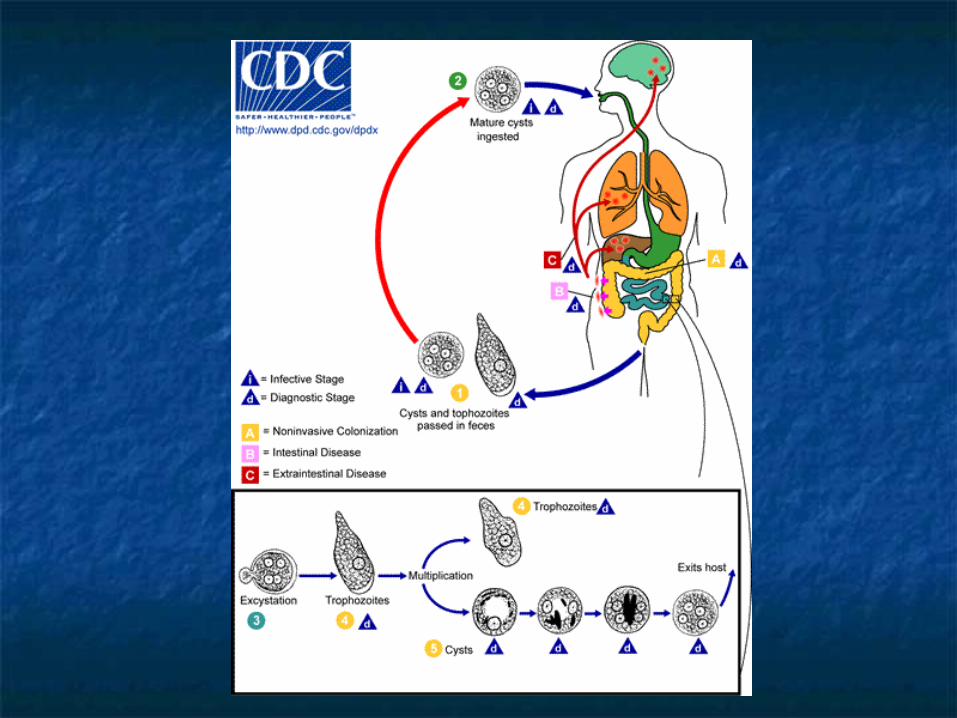
The Life CycleThe Life Cycle
1. Cyst Stage1. Cyst Stage Infective stageInfective stage Survive from –4 to 40 CelciusSurvive from –4 to 40 Celcius Size – 12mmSize – 12mm Quadrinucleated Quadrinucleated Ingested by contact with Ingested by contact with
fecally contaminated foodfecally contaminated food Passes through stomach, Passes through stomach,
excysts in lower small bowel.excysts in lower small bowel. Metacystic amoeba with four Metacystic amoeba with four
cystic nuclei from each cystcystic nuclei from each cyst 8 Small trophozoites from 8 Small trophozoites from
each metacystic amoebaeach metacystic amoeba Trophozoites carried to Trophozoites carried to
cecumcecum

The Life CycleThe Life Cycle The Trophozoite Stage:The Trophozoite Stage: 10-40 qm, fragile10-40 qm, fragile UninucleateUninucleate ErythrophagocytosisErythrophagocytosis Reside, feed and multiply by Reside, feed and multiply by
binary fissionbinary fission in lumen of in lumen of coloncolon
May May invadeinvade – Lytic & – Lytic & physical mechanisms and physical mechanisms and metastasize to liver and metastasize to liver and other extra-intestinal sitesother extra-intestinal sites
Galactose-containing Galactose-containing molecules & receptors molecules & receptors regulate cyst formationregulate cyst formation
Precyst – Cyst – Uninucleate Precyst – Cyst – Uninucleate to Quadrinucleate and to Quadrinucleate and passed in stoolpassed in stool

The PathogenesisThe Pathogenesis
10%10% of infected individuals develop of infected individuals develop invasive diseaseinvasive disease
Factors contributing to developing invasive disease:Factors contributing to developing invasive disease: Pathogenicity Pathogenicity of infecting Entamoeba speciesof infecting Entamoeba species Dose of inoculumDose of inoculum Host factorsHost factors: Impaired cell-mediated immunity, on steroids: Impaired cell-mediated immunity, on steroids Virulence of infecting speciesVirulence of infecting species::
Presence of surface adhesion factorsPresence of surface adhesion factors Release of proteolytic enzymesRelease of proteolytic enzymes Release of cytotoxins and inflicting of cytolysisRelease of cytotoxins and inflicting of cytolysis

The PathogenesisThe Pathogenesis
Trophozoites adhere to colonic mucosal glycoproteins via a Trophozoites adhere to colonic mucosal glycoproteins via a galactose and galactose and N-acetyl-D-galactosamine-specific lectinN-acetyl-D-galactosamine-specific lectin..
(Gal/GalNac) (Gal/GalNac) – Lectin is 260kD-surface protein consisting of a 225kD – Lectin is 260kD-surface protein consisting of a 225kD subunit and a 35kD subunit.subunit and a 35kD subunit.
Adherence results in cell lysis (apoptosis) and PMN invasionAdherence results in cell lysis (apoptosis) and PMN invasion PMN’s are then lysed releasing lytic enzymes, causing more tissue destructionPMN’s are then lysed releasing lytic enzymes, causing more tissue destruction Small foci of necrosis in the intestinal wall coalesce to form ulcers Small foci of necrosis in the intestinal wall coalesce to form ulcers (Flask-(Flask-
shaped ulcers)shaped ulcers)
Parasites Parasites resist resist destruction by complement armdestruction by complement arm of immune system via of immune system via Gal/GalNac mediated inhibition of the membrane attack complexGal/GalNac mediated inhibition of the membrane attack complex
Cell-mediated immunityCell-mediated immunity is important in clearing infection through is important in clearing infection through generating generating Ұ-INFҰ-INF and and TNF-αTNF-α to activate macrophages and neutrophils to kill to activate macrophages and neutrophils to kill the trophozoitethe trophozoite

The PathogenesisThe Pathogenesis
Area most commonly Area most commonly involved = involved = CecumCecum, then , then Recto-sigmoidRecto-sigmoid area area
May invade blood vessels May invade blood vessels causing thrombosis, causing thrombosis, infarction and infarction and disseminationdissemination via portal via portal circulation to circulation to liverliver and and extra-intestinal sitesextra-intestinal sites eg. eg. brain, pleura, pericardium brain, pleura, pericardium and genito-urinary system.and genito-urinary system.
Flask-shaped Flask-shaped ulcersulcers

The Clinical FeaturesThe Clinical Features Many infections = Many infections = AsymptomaticAsymptomatic ‘cyst passers’ ‘cyst passers’ SymptomaticSymptomatic infections may have a gradual, acute or rapid, infections may have a gradual, acute or rapid,
fulminant course.fulminant course.
Clinical incubation period = 4 days to several monthsClinical incubation period = 4 days to several months OftenOften gradual developmentgradual development of symptoms = Irregular bouts of of symptoms = Irregular bouts of
diarrhoea, abdominal pain, weight loss, nausea, loss of diarrhoea, abdominal pain, weight loss, nausea, loss of appetiteappetite(amoebic proctocolitis)(amoebic proctocolitis)
Less oftenLess often sudden onset of copious diarrhoea containing sudden onset of copious diarrhoea containing mucus and blood. mucus and blood.
FindingsFindings may include low-grade fever, tenderness on may include low-grade fever, tenderness on palpation of the abdominal wall overlying involved large palpation of the abdominal wall overlying involved large bowel.bowel.

The ComplicationsThe Complications
Complications of Intestinal amoebiasis:Complications of Intestinal amoebiasis: Fulminant Amoebic Colitis with PerforationFulminant Amoebic Colitis with Perforation
May have a mortality rate of up to 50%May have a mortality rate of up to 50% Children less than 2 yrs at increased risk of perforationChildren less than 2 yrs at increased risk of perforation
Massive HaemorrhageMassive Haemorrhage Due to vasculitis of large arteries or multiple ulcers leading Due to vasculitis of large arteries or multiple ulcers leading
to small arterial leaksto small arterial leaks amoebomasamoebomas
A A granulomatous thickening of the colongranulomatous thickening of the colon resulting from lytic resulting from lytic necrosis followed by secondary pyogenic inflammation, necrosis followed by secondary pyogenic inflammation, leading to fibrosis and proliferative granulation tissue. leading to fibrosis and proliferative granulation tissue. Lesions are firm, hard, may resemble a carcinoma.Lesions are firm, hard, may resemble a carcinoma.
amoebic Strictureamoebic Stricture Resulting from fibrosis of intestinal wall. Can involve Resulting from fibrosis of intestinal wall. Can involve
rectum, anus or sigmoid.rectum, anus or sigmoid.

The ComplicationsThe Complications
Complications of Extra-Intestinal Complications of Extra-Intestinal Amoebiasis:Amoebiasis: Amoebic Liver AbcessAmoebic Liver Abcess
Most frequentMost frequent complication of amoebiasis complication of amoebiasis Male:Female Ratio = 1 in Children and infantsMale:Female Ratio = 1 in Children and infants In adulthood = More common in young malesIn adulthood = More common in young males Third to Half may have no history of diarrhoeaThird to Half may have no history of diarrhoea Commonly found in Commonly found in Right LobeRight Lobe of liver of liver Presents acutely with high fever, RUQ tendernessPresents acutely with high fever, RUQ tenderness Jaundice an unusual findingJaundice an unusual finding Have marked Have marked leucocytosisleucocytosis and may have and may have XR XR
abnormalitiesabnormalities in 25 to 90% of patients in 25 to 90% of patients

The ComplicationsThe Complications
Complications of Extra-Intestinal amoebiasis:Complications of Extra-Intestinal amoebiasis: amoebic Peritonitisamoebic Peritonitis
As a complication of a ruptured hepatic abcessAs a complication of a ruptured hepatic abcess Pleuropulmonary amoebiasisPleuropulmonary amoebiasis
Caused by rupture of Caused by rupture of Rt. LobeRt. Lobe Liver abcess in 10% of patients Liver abcess in 10% of patients Has cough, pleuritic chest pain & dyspnoeaHas cough, pleuritic chest pain & dyspnoea
amoebic Pericarditisamoebic Pericarditis Rare, but most serious complication in 3% of pts. with liver Rare, but most serious complication in 3% of pts. with liver
involvementinvolvement Rupture of Rupture of Left LobeLeft Lobe liver abcess liver abcess
Cerebral amoebiasisCerebral amoebiasis Rare, has altered consciousness and focal neuro signsRare, has altered consciousness and focal neuro signs CT – Irregular lesions CT – Irregular lesions withoutwithout surrounding capsule or enhancement surrounding capsule or enhancement
Genito-Urinary InvolvementGenito-Urinary Involvement Painful genital ulcers – Punched out appearance & profuse Painful genital ulcers – Punched out appearance & profuse
dischargedischarge
The DiagnosisThe Diagnosis Light Microscopy of StoolLight Microscopy of Stool
Identification of trophozoites / cysts in fresh stoolIdentification of trophozoites / cysts in fresh stool Disadvantages:Disadvantages:
Not sensitive (miss up to two thirds of infections)Not sensitive (miss up to two thirds of infections) Cannot distinguish between E.histolytica and E. disparCannot distinguish between E.histolytica and E. dispar
Serology:Serology: Anti-amoebic antibodies (IgM) Anti-amoebic antibodies (IgM) 70%70% sensitive for sensitive for amoebicamoebic colitis colitis and and 90%90% sensitive for sensitive for amoebic amoebic
liver abcessliver abcess
Stool antigen-detection test or PCRStool antigen-detection test or PCR Sensitive and SpecificSensitive and Specific Disadvantages:Disadvantages:
Antigen detection test (EIA) only available from Blacksburg VAAntigen detection test (EIA) only available from Blacksburg VA

The DiagnosisThe Diagnosis
Colonoscopy / Colonoscopy / SigmoidoscopySigmoidoscopy ColonoscopyColonoscopy preferable preferable Wet preps of material from Wet preps of material from
ulcer-base can show ulcer-base can show trophozoitestrophozoites
BiopsiesBiopsies should be taken should be taken from edge of ulcersfrom edge of ulcers
Recommended to evaluate Recommended to evaluate for amoebic colitis even for amoebic colitis even when when Ulcerative ColitisUlcerative Colitis consideredconsidered

The DiagnosisThe Diagnosis
amoebic Liver Abcess:amoebic Liver Abcess: Diagnosis relies on:Diagnosis relies on:
Detection of Detection of risk factorsrisk factors for E.histolytica infection for E.histolytica infection Positive SerologyPositive Serology Lesion in LiverLesion in Liver : :
Abdominal USSAbdominal USS Abdominal CT: Well-rounded, wall enhancesAbdominal CT: Well-rounded, wall enhances
Aspiration may yield “anchovy-paste” materialAspiration may yield “anchovy-paste” material More often yellow / gray-greenMore often yellow / gray-green Often odourless and sterile – Often odourless and sterile – Highly suggestive of Highly suggestive of
amoebicamoebic abcessabcess
The ManagementThe Management Asymptomatic infectionsAsymptomatic infections
Luminal agent only recommended but ?not available in SALuminal agent only recommended but ?not available in SA In general, not treated in endemic areasIn general, not treated in endemic areas
Symptomatic infectionsSymptomatic infections Oral MetronidazoleOral Metronidazole for 10 days for 10 days Effective in eradicating amoebae in bowel lumen and wallEffective in eradicating amoebae in bowel lumen and wall Effective in eradicating extra-intestinal diseaseEffective in eradicating extra-intestinal disease Additional luminal agent not necessaryAdditional luminal agent not necessary
E. dispar infection doesn’t require treatmentE. dispar infection doesn’t require treatment

PreventionPrevention
Improved sanitationImproved sanitation andand clean water supplyclean water supply reducereduce fecal-oral transmissionfecal-oral transmission
Boiling water, Washing veg with vinegarBoiling water, Washing veg with vinegar
Vaccination:Vaccination: None available currentlyNone available currently Prototype subunit vaccines based on the Prototype subunit vaccines based on the
Gal/GalNAc-lectin under studyGal/GalNAc-lectin under study