Embed Size (px)
Citation preview
AMI Virtual Learning Collaborative
Building on LS1-B
Atlantic Node
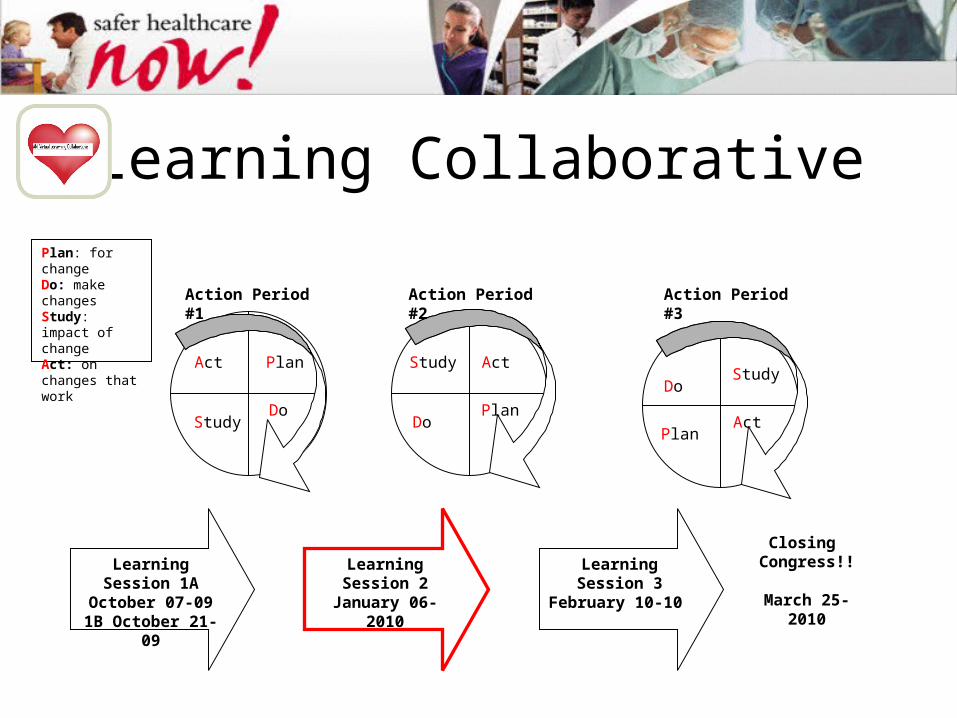
Learning Collaborative
Learning Session 1A October 07-091B October 21-09
Learning Session 2
January 06-2010
Learning Session 3
February 10-10
Closing Congress!!
March 25-2010
Act Act
Act
Plan
Plan
Plan
DoDo
Do
Study
StudyStudy
Plan: for changeDo: make changesStudy: impact of changeAct: on changes that work
Action Period #1 Action Period #2 Action Period #3
Atlantic Node
Team Self Evaluation
LS1-B Re-Cap
• Measures, data collection, worksheets and submission
• Model for Improvement: Team, AIM, Measures, Changes
• PDSA Cycles
Atlantic Node
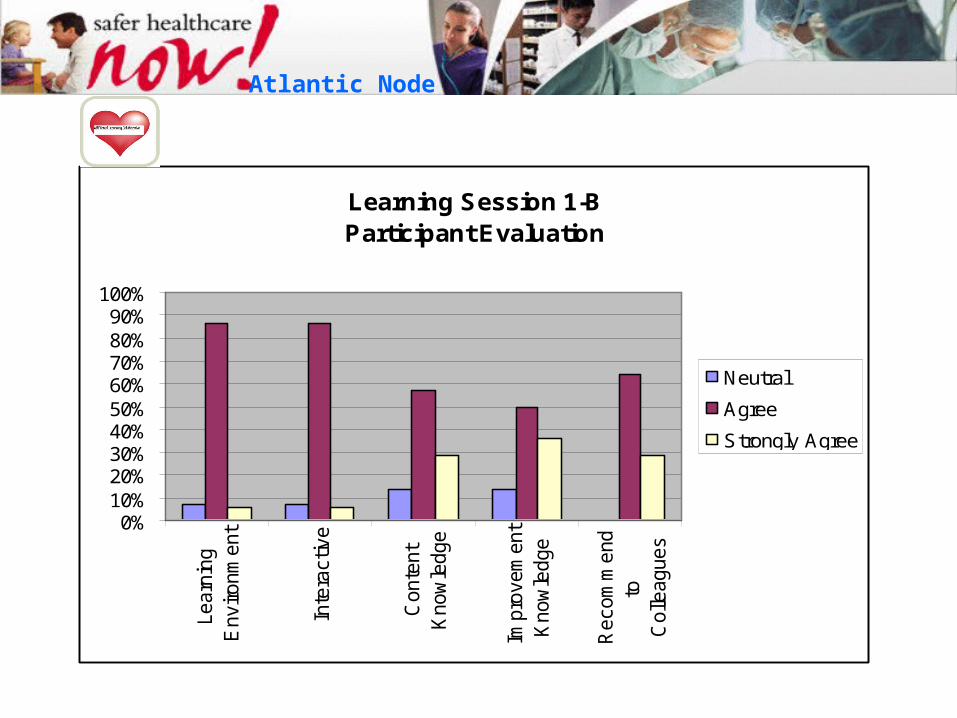
Learning Session 1-BParticipant Evaluation
0%10%20%30%40%50%60%70%80%90%
100%
Learn
ing
Environm
ent
Inte
ractive
Conte
nt
Know
ledge
Impro
vem
ent
Know
ledge
Recom
mend
toC
olle
agues
Neutral
Agree
Strongly Agree
Atlantic Node
What Worked Well
• The interactive aspect and the examples
• Use to this format & it is easy to use!
• This was a new format for me so the process is slow enough to follow
Atlantic Node
What Worked Well
• Convenient and a good use of my time
• Slide info together with handouts • People sharing their work from today. The
brave ones!
Atlantic Node
Improvement Opportunities
• More sharing by all and more questions.
• Keep things moving along at a faster pace, less breaks.
Atlantic Node
Comments/Questions
Atlantic Node
IMPROVING DOOR TO NEEDLE TIMESTRH STEPHENVILLE
EXPERIENCE
AMER QURESHI MD, FRCPC
DISCLOSURE
I have no relevant financial relationships to disclose.
OBJECTIVES
FIBRINOLYTICS IN STEMI
DOOR TO NEEDLE TIME
STRH – EXPERIENCE & EFFORTS TO IMPROVE DOOR TO NEEDLE TIME
CVD - MORTALITY
CVD : 32.3% MEN
34.1% WOMEN
18.0% HOSPITALISATION
HEART ATTACKS 49,220 - 2007-08
1678 (3.4%) 2nd MI
HEART ATTACKS ~ 18000 DEATHS
Canadian Institute for Health Information: Health Indicators 2009
ACUTE MYOCARDIAL INFARCTION 30 DAY – MORTALITY
2003-2004 10.2%
2007-2008 9.1%
MORTALITY ↓ - 11%
20 - 44 YRS. 41%
> 65YRS. 11%
Canadian Institute for Health Information: Health Indicators 2009
ACUTE MYOCARDIAL INFARCTION
↓ MORTALITY
♂ > ♀ 4 TIMES AGE 20 - 44 YRS
♂ > ♀ 1.5 TIMES AGE > 65 YRS
Canadian Institute for Health Information: Health Indicators 2009
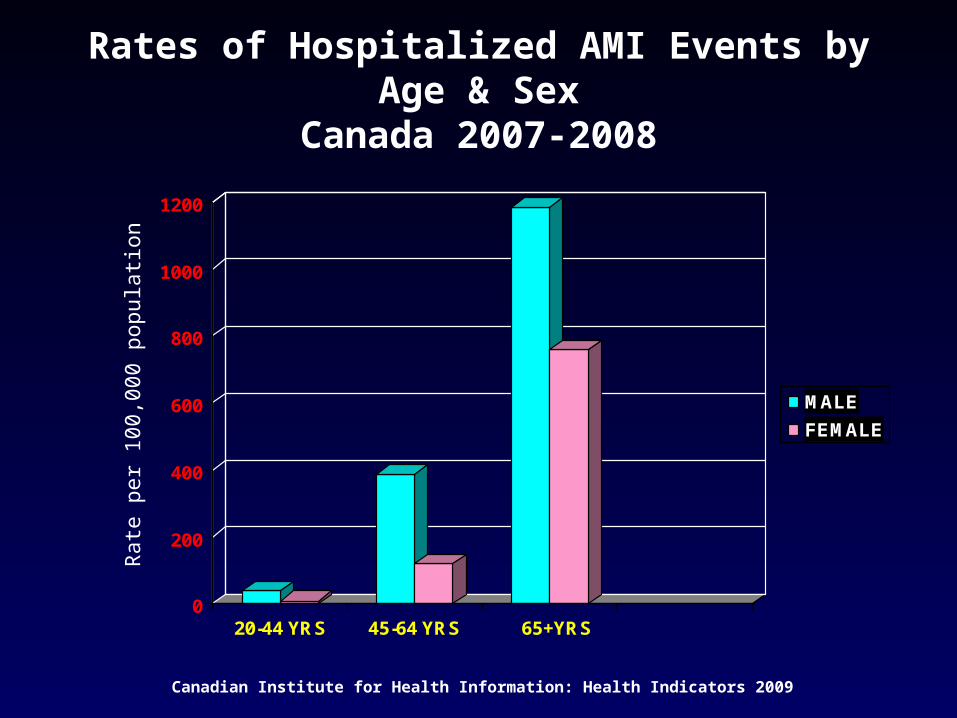
Rates of Hospitalized AMI Events by Age & SexCanada 2007-2008
0
200
400
600
800
1000
1200
20-44 YRS 45-64 YRS 65+YRS
MALE
FEMALE
Rat
e pe
r 10
0,00
0 po
pula
tion
Canadian Institute for Health Information: Health Indicators 2009
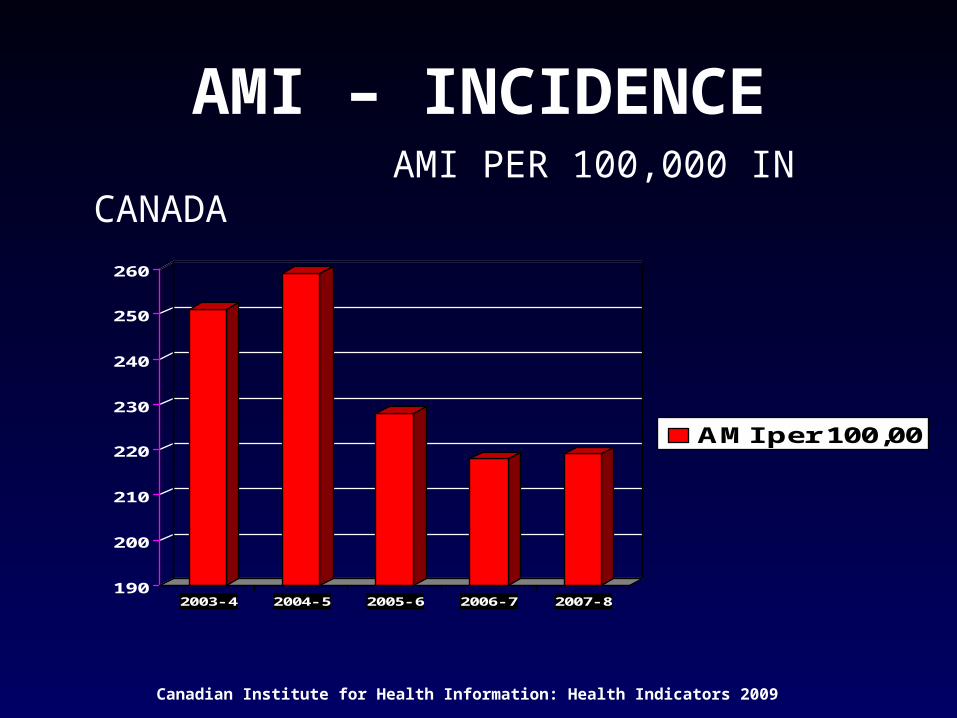
AMI – INCIDENCE AMI PER 100,000 IN CANADA
190
200
210
220
230
240
250
260
2003- 4 2004- 5 2005- 6 2006- 7 2007- 8
AMI per 100,00
Canadian Institute for Health Information: Health Indicators 2009
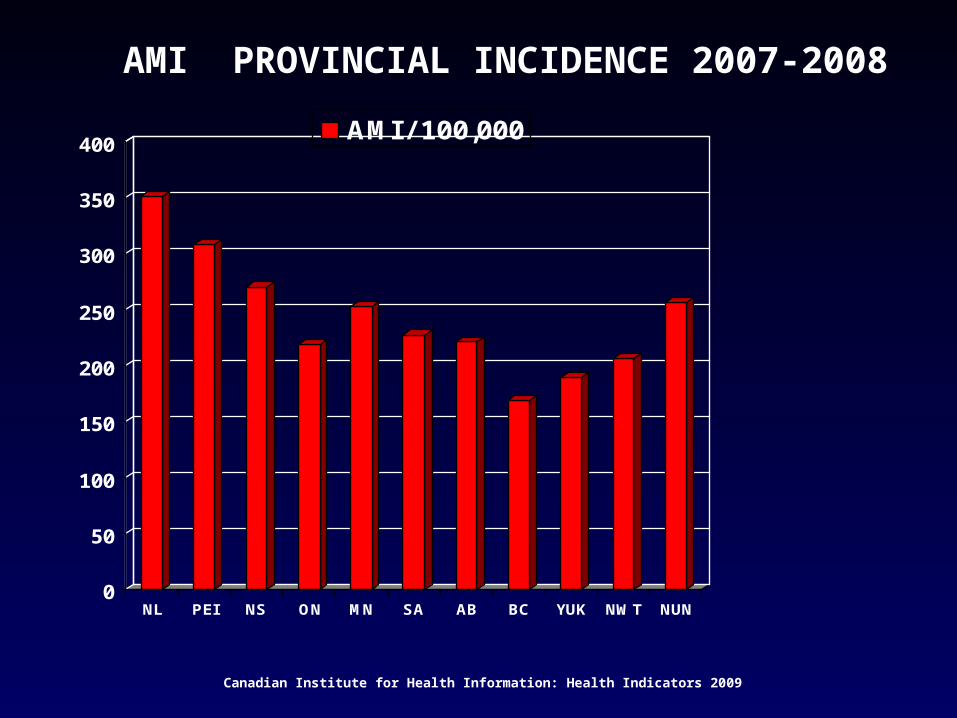
AMI PROVINCIAL INCIDENCE 2007-2008
0
50
100
150
200
250
300
350
400
NL PEI NS ON MN SA AB BC YUK NWT NUN
AMI / 100,000
Canadian Institute for Health Information: Health Indicators 2009
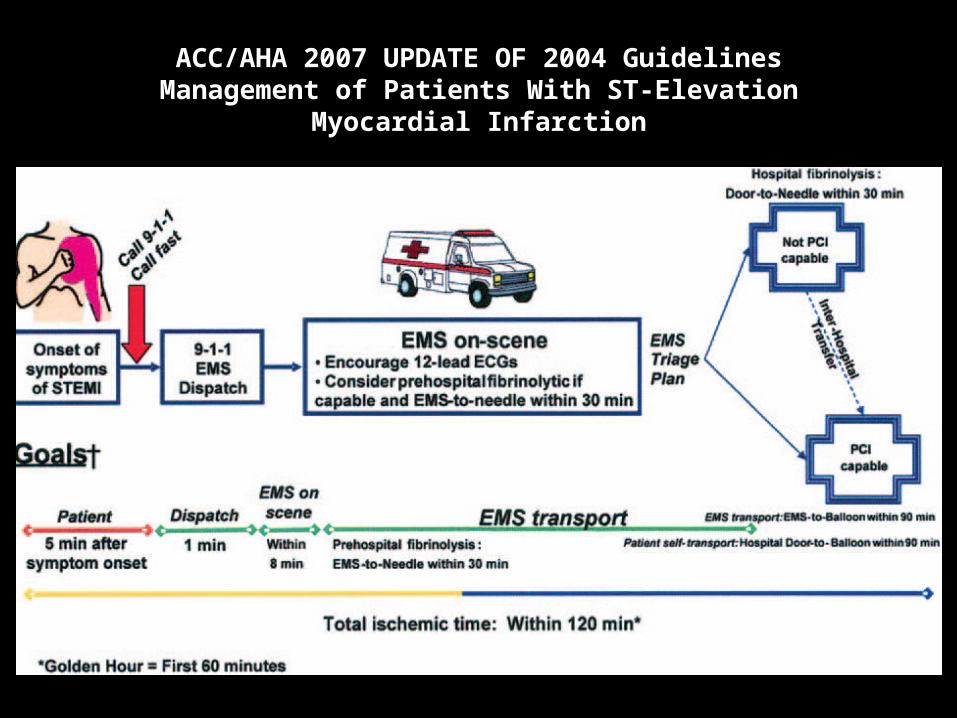
ACC/AHA 2007 UPDATE OF 2004 GuidelinesManagement of Patients With ST-Elevation
Myocardial Infarction
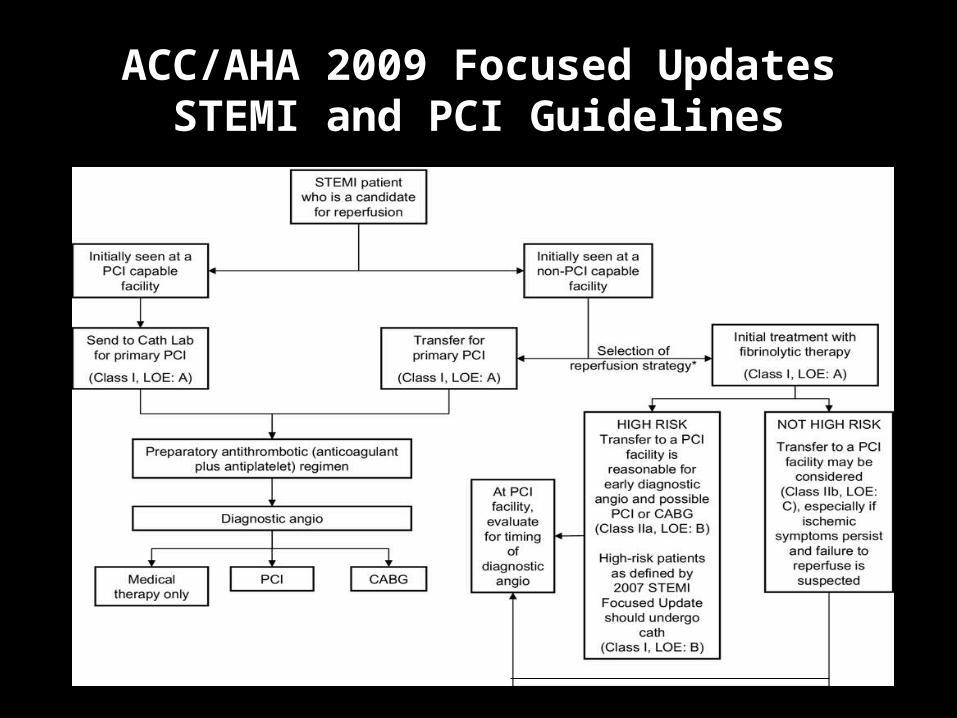
ACC/AHA 2009 Focused UpdatesSTEMI and PCI Guidelines
AMI – CARE INITIATIVE
ASPIRIN ON PRESENTATION FIBRINOLYTIC BETABLOCKER ACEI / ARB STATIN ASPIRIN AT DISCHARGE SMOKING CESSATION COUNSELLING
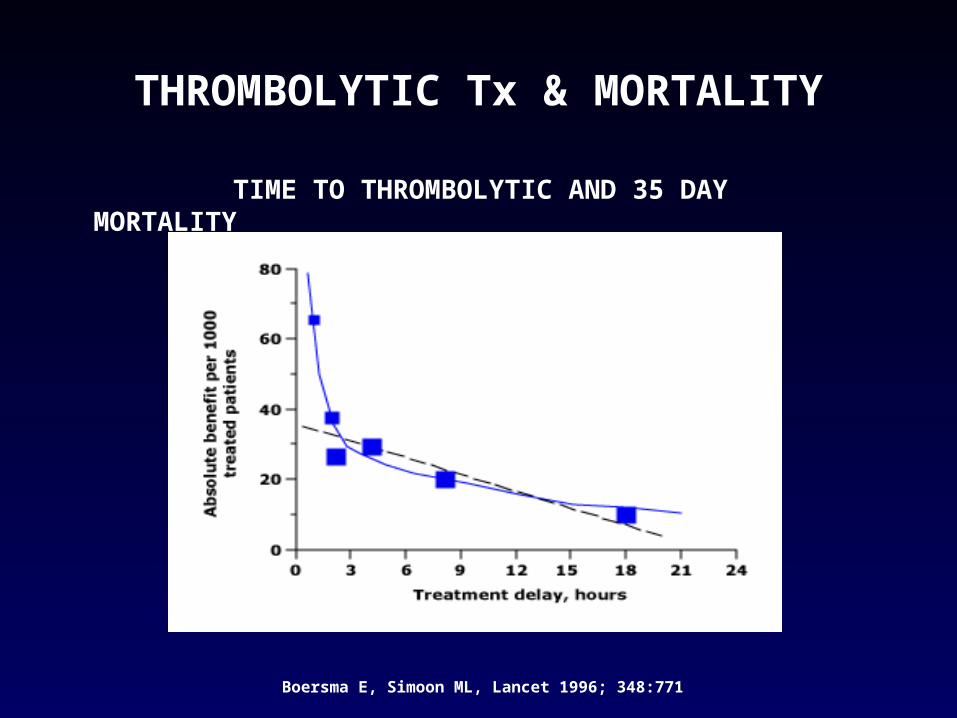
THROMBOLYTIC Tx & MORTALITY
TIME TO THROMBOLYTIC AND 35 DAY MORTALITY
Boersma E, Simoon ML, Lancet 1996; 348:771
TIME IS MYOCARDIUM
TIMELY FIBRINOLYTIC Tx:
LIMIT INARCT SIZE PRESERVE LV FUNCTION IMPROVE SURVIVAL
DOOR TO NEEDLE TIME
ACC/AHA 2004 TASK FORCE ON STEMIREC. - DNT < 30min.ACC/AHA 2007 REC. WAS NOT CHANGED
NRMI eval. >1000 US Hospitals 1999-2002 68,000 pts given Fibrinolytic Tx
46% < 30 min 33% ↓ DNT by >1 min
32% ↑ DNT by >1 min
National Registry of Myocardial Infarction, McNamara RL; Herrin J; J Am Coll Cardiol. 2006 Jan 3;47(1):45-51
FIBRINOLYTIC Tx
ABSOLUTE CONTRAINDICATIONS:
o ICHo Cerebral Vascular lesiono Malignant I/C Neoplasmo CVA within last 3 monthso Suspected Aortic Dissectiono Active Bleeding or Bleed. Diathesiso Severe closed head/facial trauma
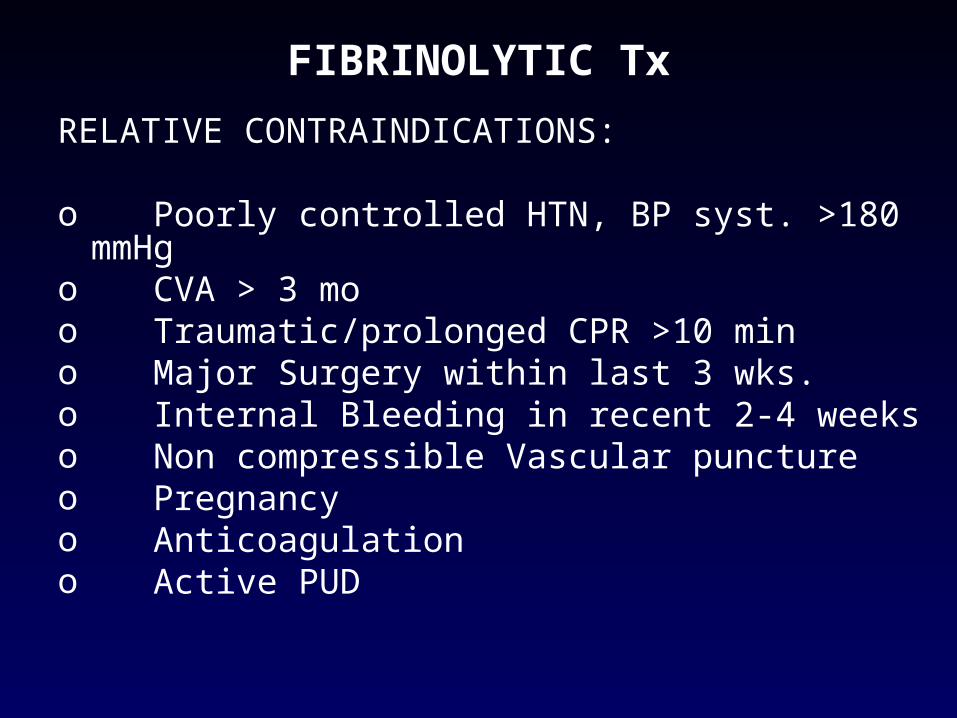
FIBRINOLYTIC Tx
RELATIVE CONTRAINDICATIONS:
o Poorly controlled HTN, BP syst. >180 mmHg o CVA > 3 moo Traumatic/prolonged CPR >10 mino Major Surgery within last 3 wks.o Internal Bleeding in recent 2-4 weeks o Non compressible Vascular punctureo Pregnancyo Anticoagulation o Active PUD
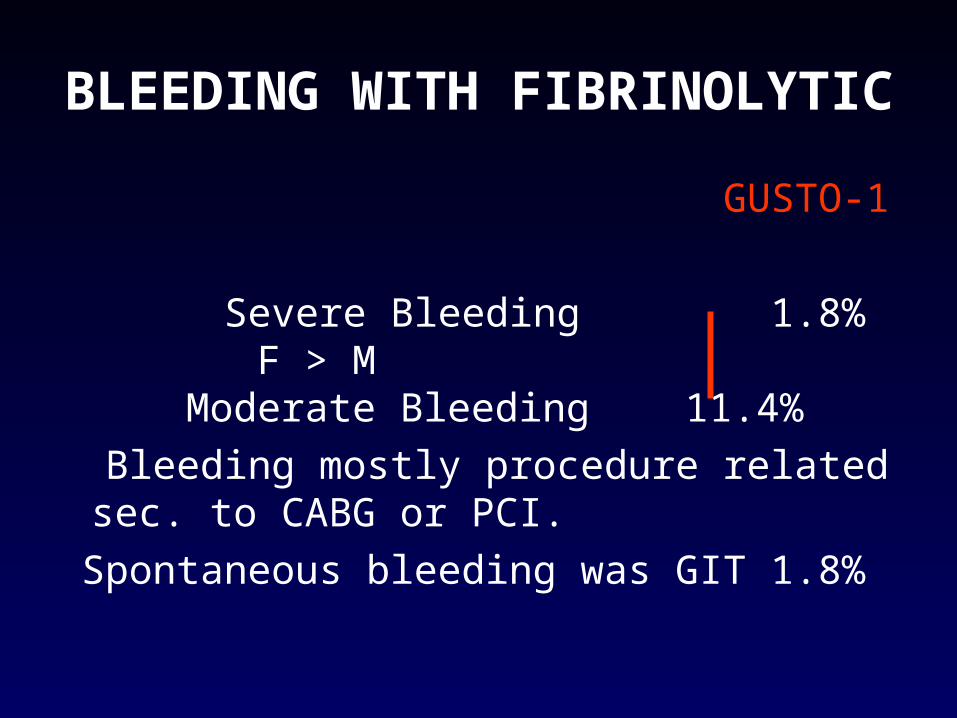
BLEEDING WITH FIBRINOLYTIC
GUSTO-1
Severe Bleeding 1.8% F > M Moderate Bleeding 11.4%
Bleeding mostly procedure related sec. to CABG or PCI.
Spontaneous bleeding was GIT 1.8%
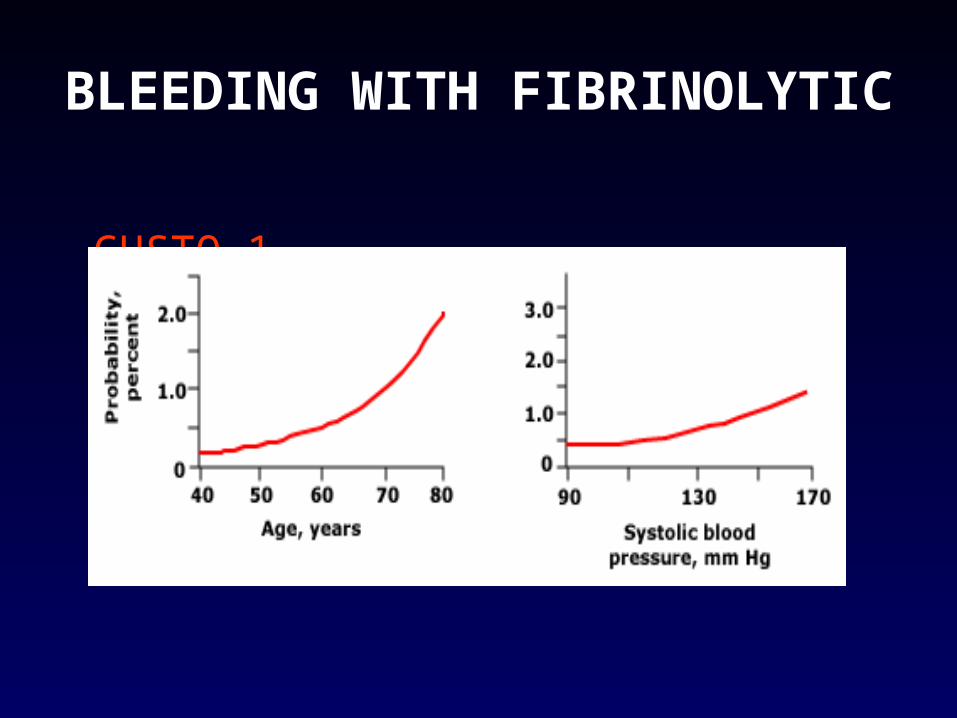
BLEEDING WITH FIBRINOLYTIC
GUSTO-1
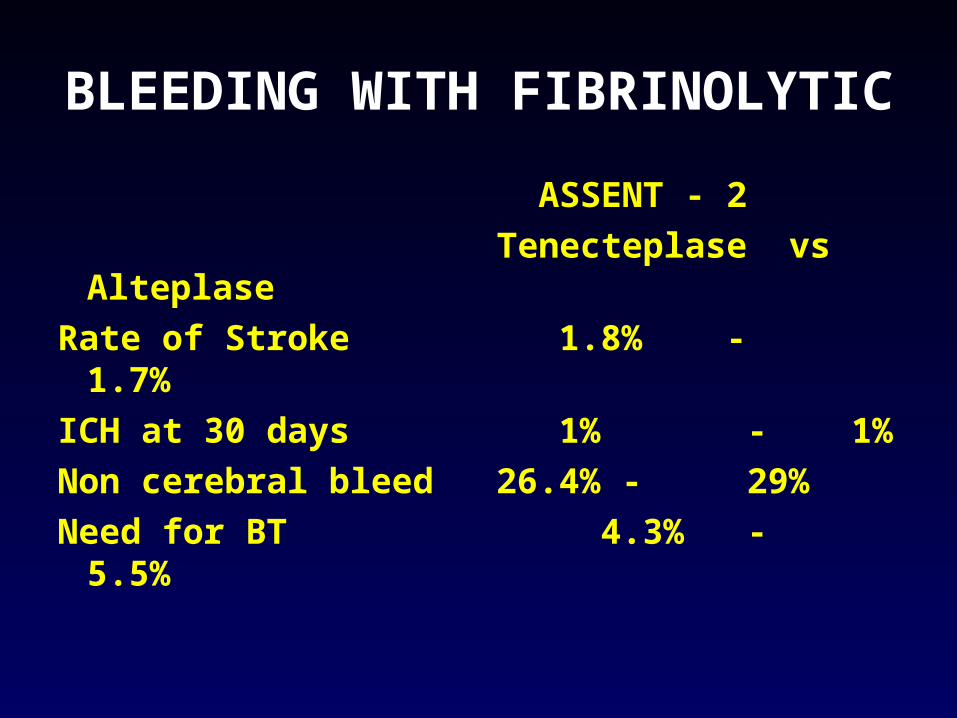
BLEEDING WITH FIBRINOLYTIC
ASSENT - 2
Tenecteplase vs Alteplase
Rate of Stroke 1.8% - 1.7%
ICH at 30 days 1% - 1%
Non cerebral bleed 26.4% - 29%
Need for BT 4.3% - 5.5%
BLEEDING WITH FIBRINOLYTIC
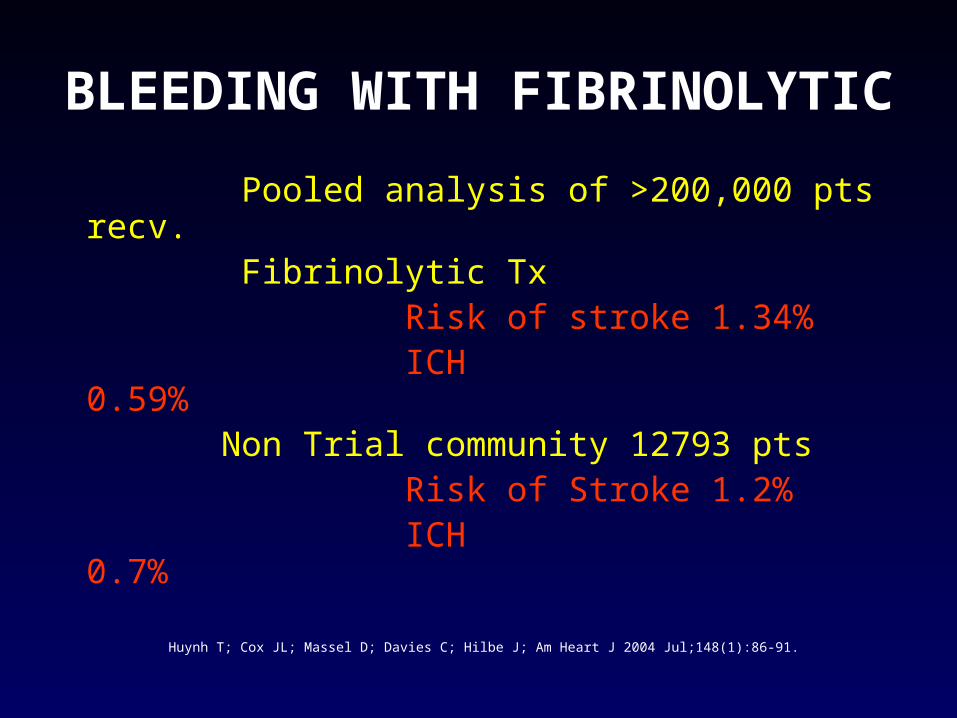
Pooled analysis of >200,000 pts recv. Fibrinolytic Tx Risk of stroke 1.34% ICH 0.59% Non Trial community 12793 pts Risk of Stroke 1.2% ICH 0.7%
Huynh T; Cox JL; Massel D; Davies C; Hilbe J; Am Heart J 2004 Jul;148(1):86-91.
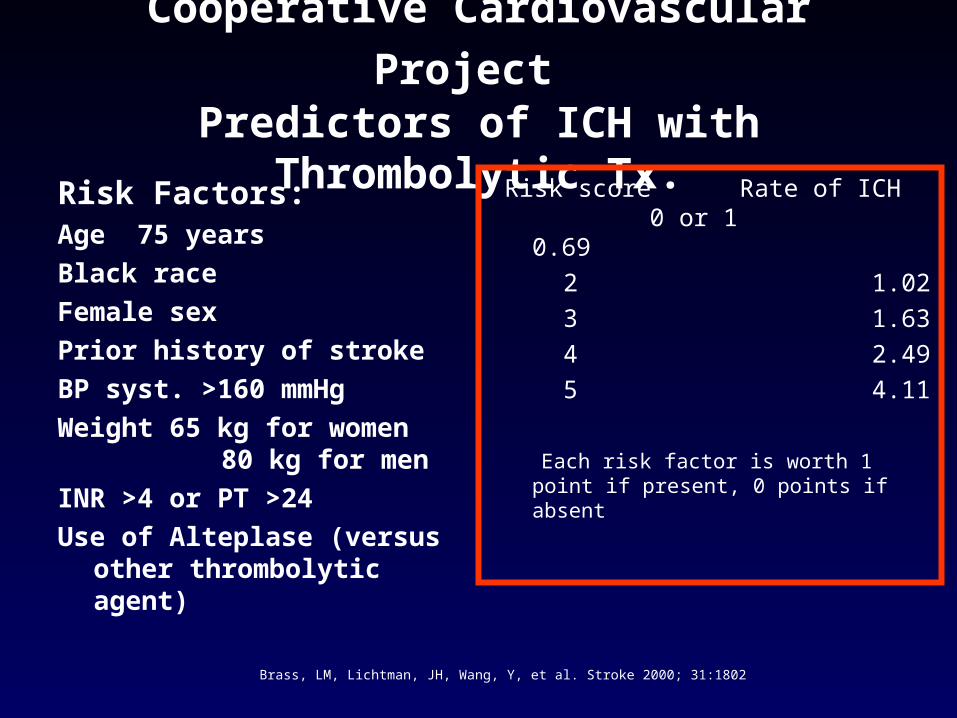
Cooperative Cardiovascular Project Predictors of ICH with Thrombolytic Tx.
Risk Factors:Age 75 years
Black race
Female sex
Prior history of stroke
BP syst. >160 mmHg
Weight 65 kg for women 80 kg for men
INR >4 or PT >24
Use of Alteplase (versus other thrombolytic agent)
Risk score Rate of ICH 0 or 1 0.69
2 1.02
3 1.63
4 2.49
5 4.11
Each risk factor is worth 1 point if present, 0 points if absent
Brass, LM, Lichtman, JH, Wang, Y, et al. Stroke 2000; 31:1802
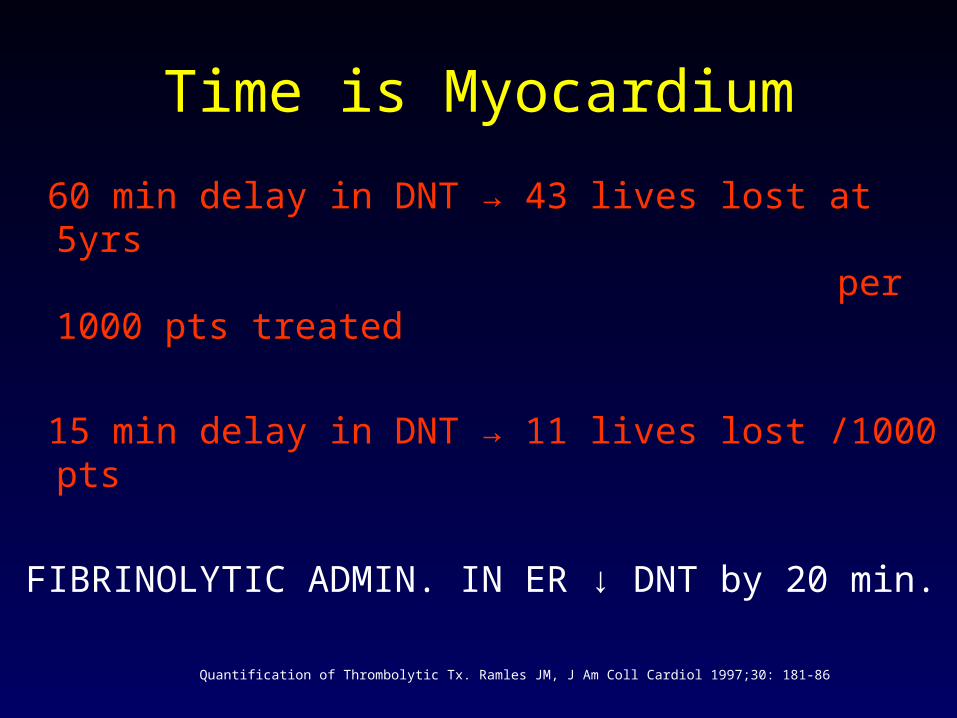
Time is Myocardium
60 min delay in DNT → 43 lives lost at 5yrs per 1000 pts treated
15 min delay in DNT → 11 lives lost /1000 pts
FIBRINOLYTIC ADMIN. IN ER ↓ DNT by 20 min.
Quantification of Thrombolytic Tx. Ramles JM, J Am Coll Cardiol 1997;30: 181-86
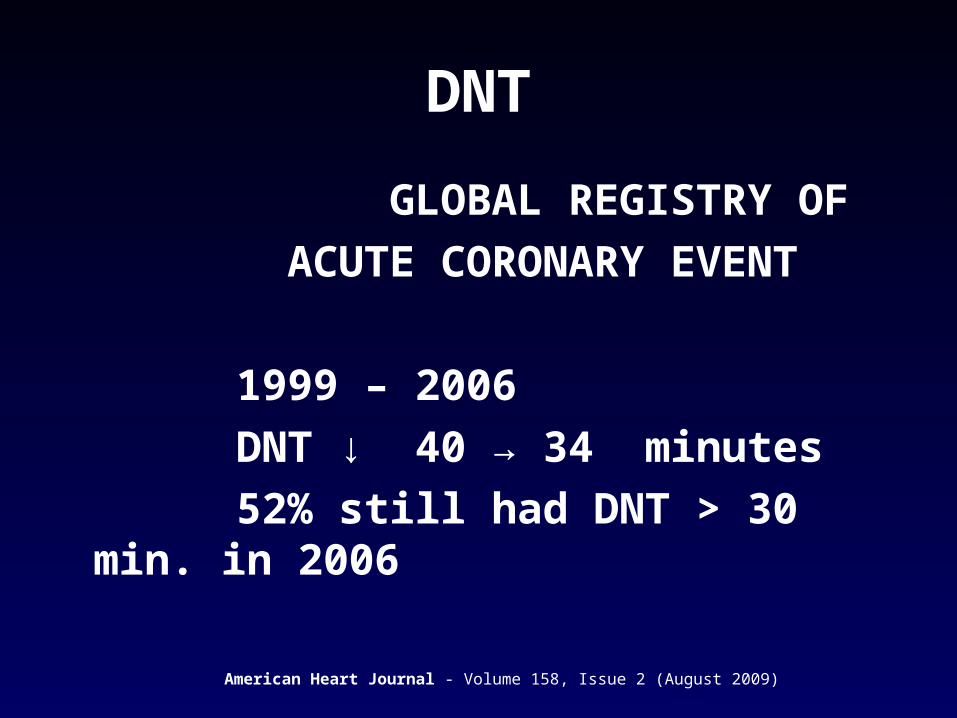
DNT
GLOBAL REGISTRY OF
ACUTE CORONARY EVENT
1999 – 2006
DNT ↓ 40 → 34 minutes
52% still had DNT > 30 min. in 2006
American Heart Journal - Volume 158, Issue 2 (August 2009)
Causes of delay in DNT
Pre – Hospital/ER presentation Patient related factors Transport
After Presentation to Hospital / ER Registration Triage EKG Physician Evaluation - Diagnosis Decision to give drug
Time to presentation to ER
Patient’s failure to recognize symptoms and seek evaluation accounts for up to 2/3 of the time delay in DNT.
Insufficient knowledge/awareness
Poor coping mechanism
Attributing symptoms to other cause
Hesitation to go to ER and being wrong about the cause of symptoms
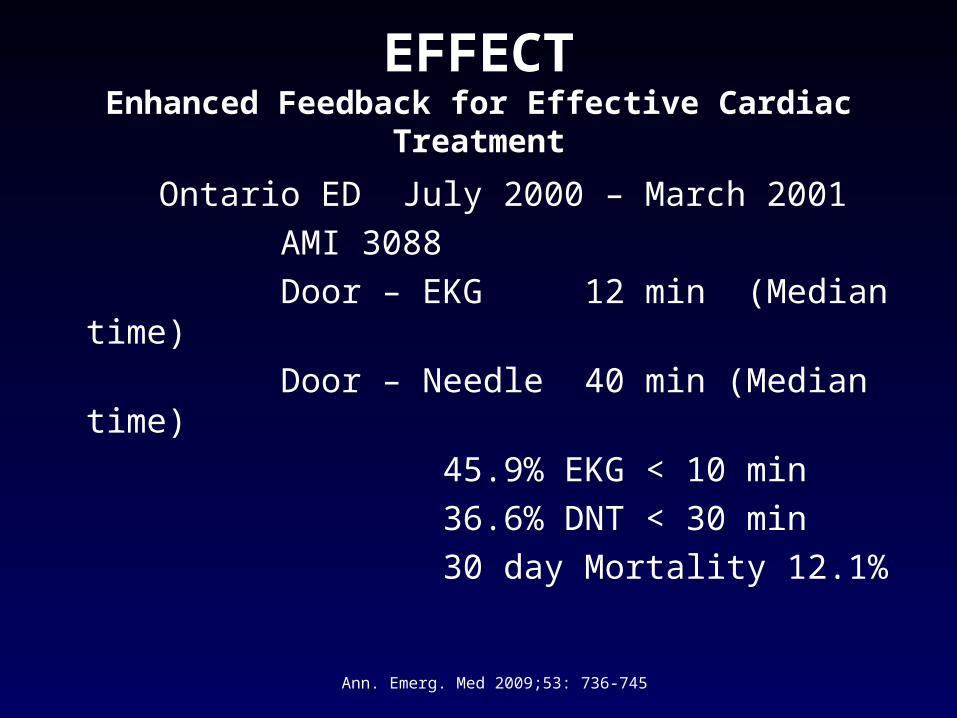
EFFECTEnhanced Feedback for Effective Cardiac Treatment
Ontario ED July 2000 – March 2001
AMI 3088
Door – EKG 12 min (Median time)
Door – Needle 40 min (Median time)
45.9% EKG < 10 min
36.6% DNT < 30 min
30 day Mortality 12.1%
Ann. Emerg. Med 2009;53: 736-745
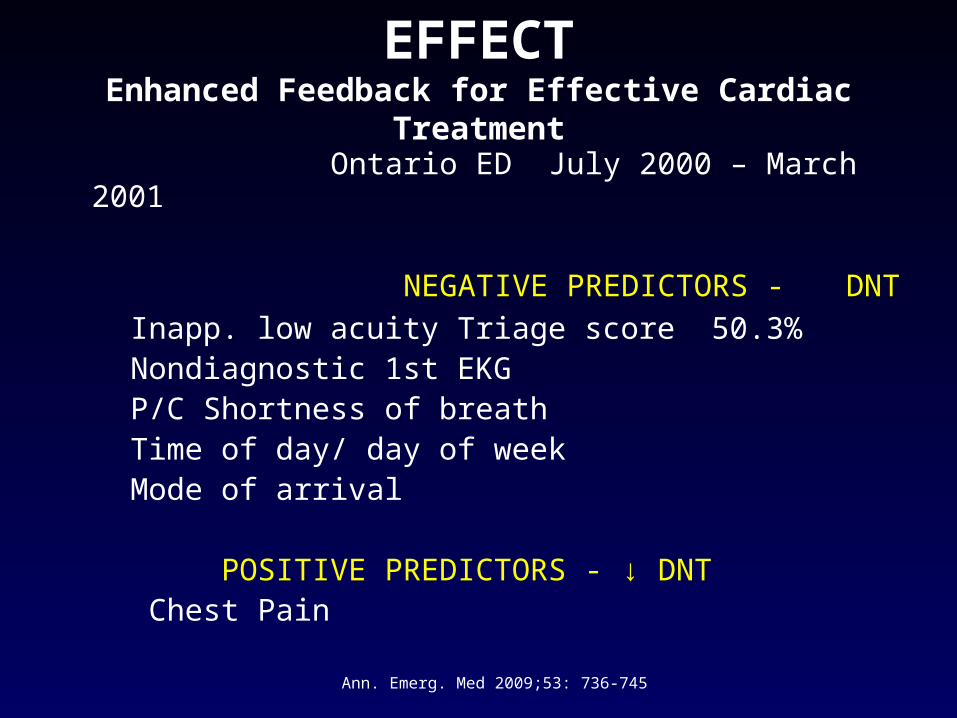
EFFECTEnhanced Feedback for Effective Cardiac Treatment
Ontario ED July 2000 – March 2001
NEGATIVE PREDICTORS - DNT
Inapp. low acuity Triage score 50.3% Nondiagnostic 1st EKG P/C Shortness of breath Time of day/ day of week Mode of arrival POSITIVE PREDICTORS - ↓ DNT Chest Pain
Ann. Emerg. Med 2009;53: 736-745
EFFECTEnhanced Feedback for Effective Cardiac Treatment
NEGATIVE PREDICTORS - DNT Inappropriately low CTAS 44% with criteria for STEMI – low CTAS ↓ 15 min ↑ median DNT
Odds of getting bench mark time for EKG & Fibrinolytic were about half as good for the Pts.with inapp. CTAS, when compared with appropriately triaged score AMI Pts.
Ann. Emerg. Med 2009;53: 736-745
STRH - EXPERIENCE
ASPIRIN ON PRESENTATION FIBRINOLYTIC BETABLOCKER ACEI / ARB STATIN ASPIRIN AT DISCHARGE SMOKING CESSATION COUNSELLING
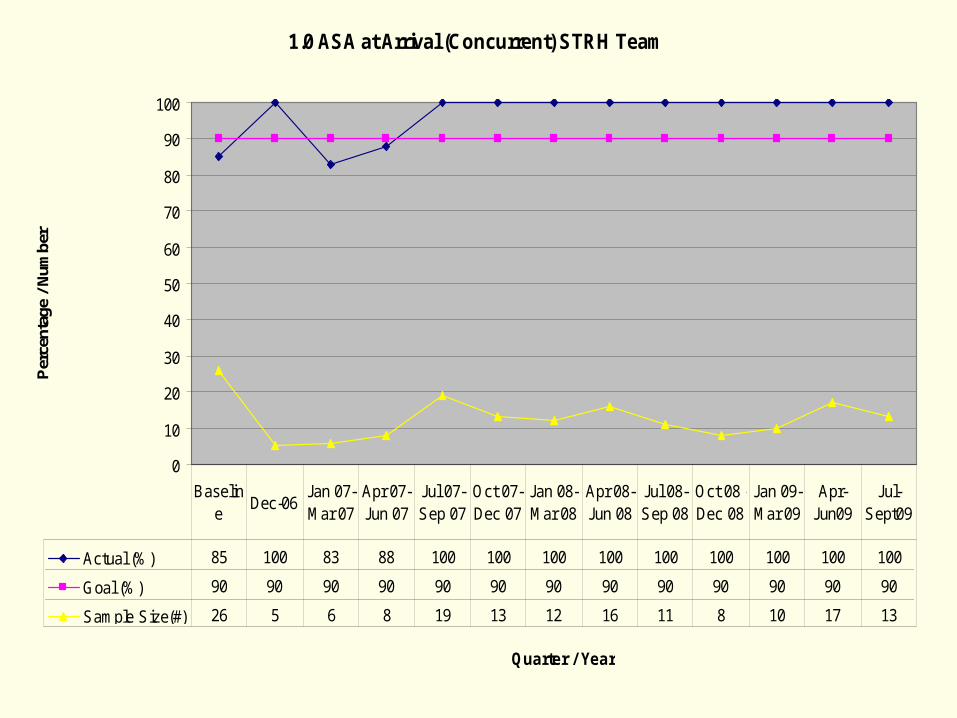
1.0 ASA at Arrival (Concurrent) STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 85 100 83 88 100 100 100 100 100 100 100 100 100
Goal (%) 90 90 90 90 90 90 90 90 90 90 90 90 90
Sample Size(#) 26 5 6 8 19 13 12 16 11 8 10 17 13
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
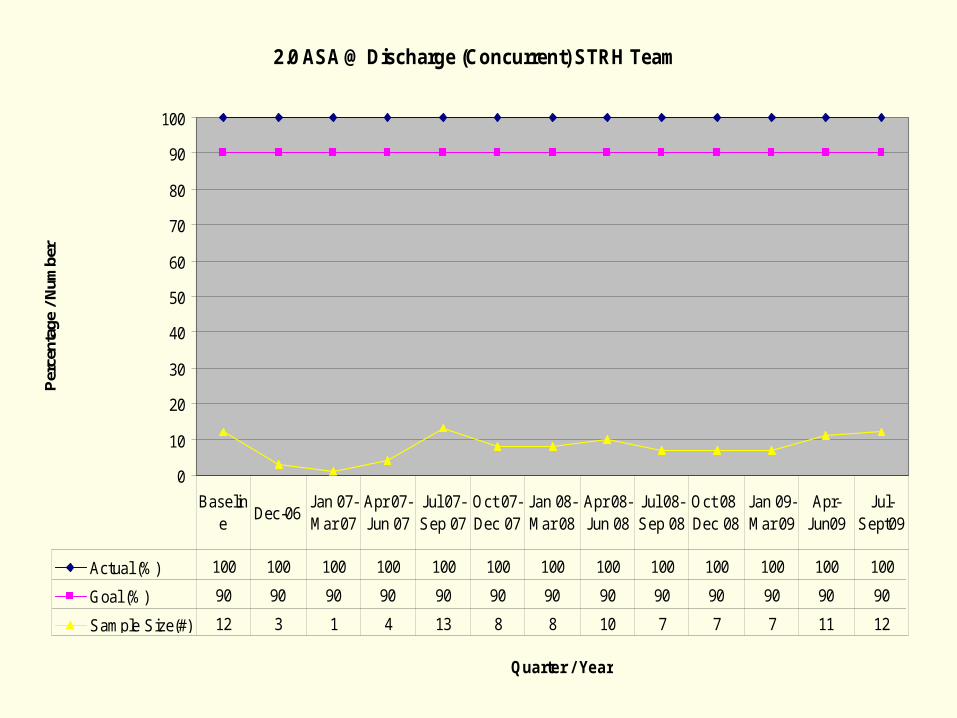
2.0 ASA @ Discharge (Concurrent) STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 100 100 100 100 100 100 100 100 100 100 100 100 100
Goal (%) 90 90 90 90 90 90 90 90 90 90 90 90 90
Sample Size(#) 12 3 1 4 13 8 8 10 7 7 7 11 12
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
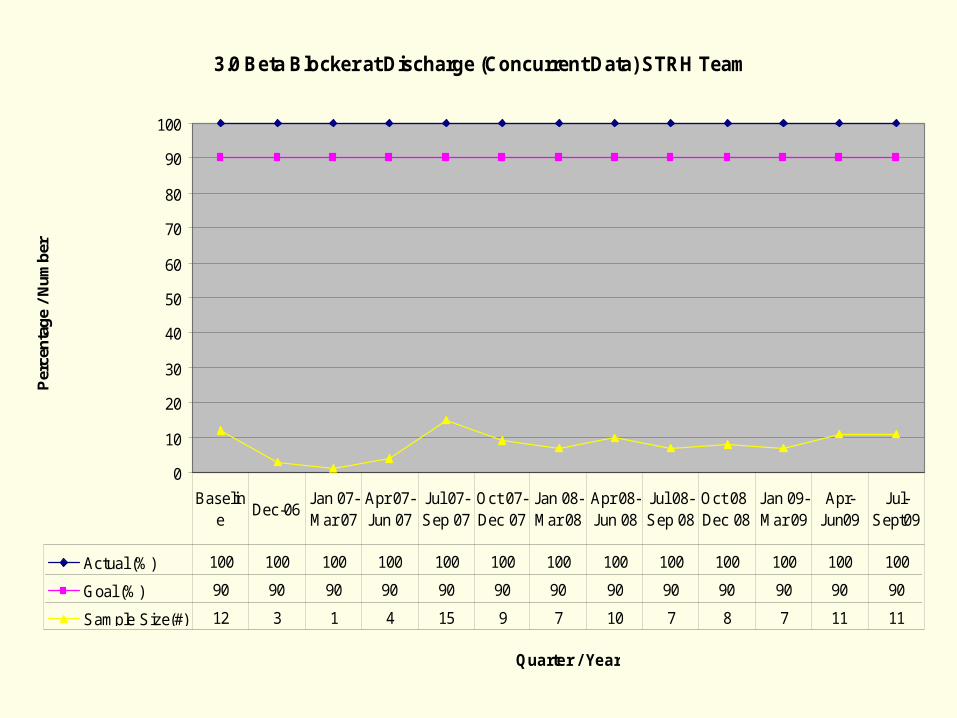
3.0 Beta Blocker at Discharge (Concurrent Data) STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cen
tag
e /
Nu
mb
er
Actual (%) 100 100 100 100 100 100 100 100 100 100 100 100 100
Goal (%) 90 90 90 90 90 90 90 90 90 90 90 90 90
Sample Size(#) 12 3 1 4 15 9 7 10 7 8 7 11 11
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
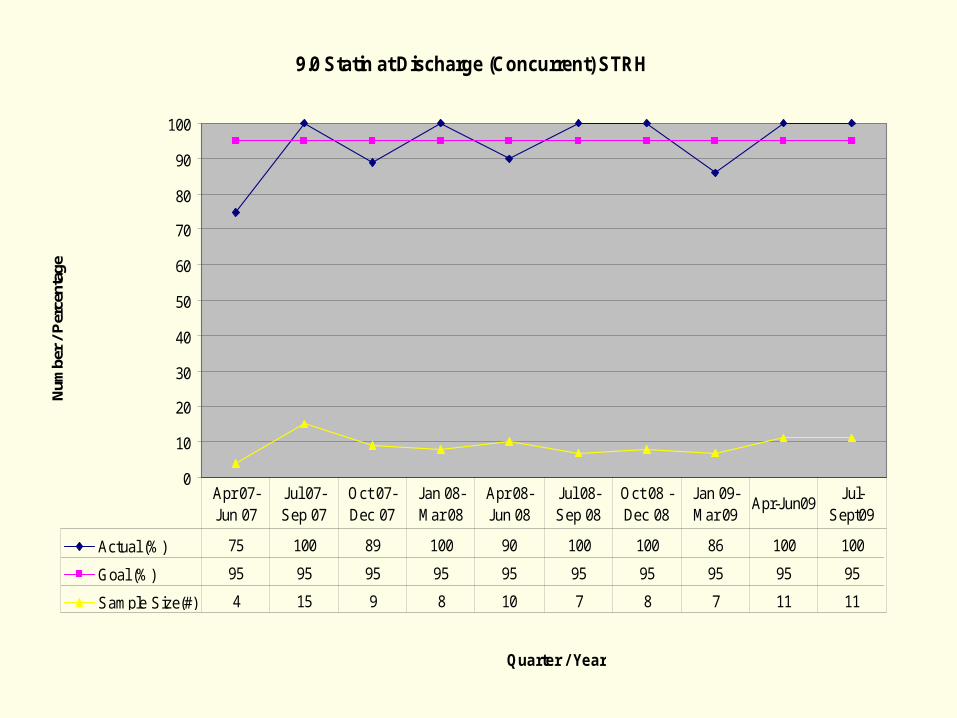
9.0 Statin at Discharge (Concurrent) STRH
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Num
ber
/ Per
cent
age
Actual (%) 75 100 89 100 90 100 100 86 100 100
Goal (%) 95 95 95 95 95 95 95 95 95 95
Sample Size(#) 4 15 9 8 10 7 8 7 11 11
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09Jul-
Sept09
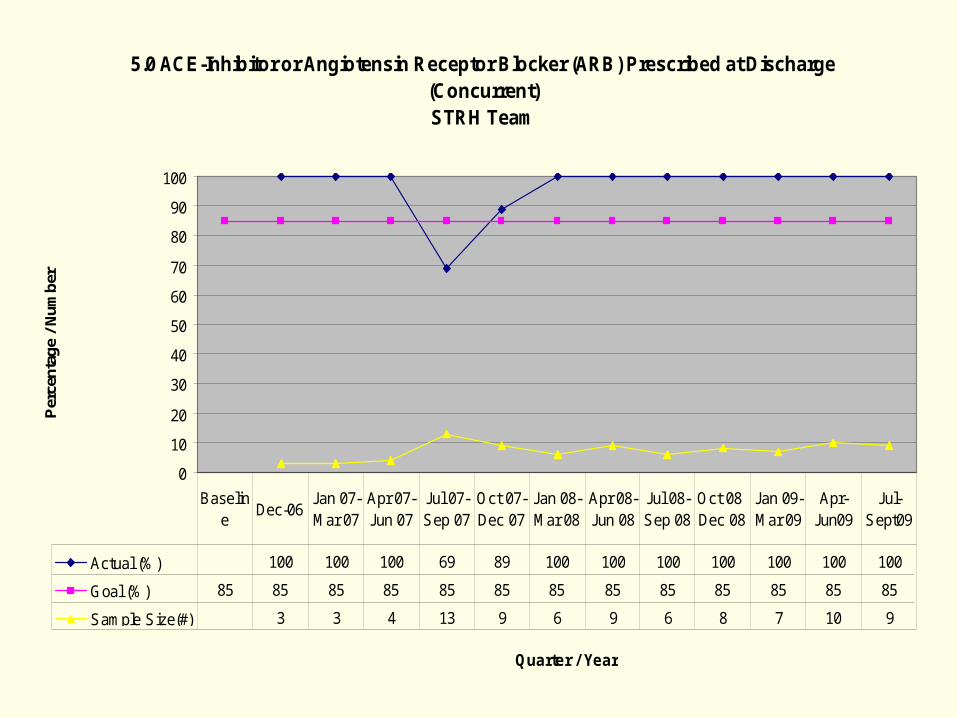
5.0 ACE-Inhibitor or Angiotensin Receptor Blocker (ARB) Prescribed at Discharge (Concurrent)STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 100 100 100 69 89 100 100 100 100 100 100 100
Goal (%) 85 85 85 85 85 85 85 85 85 85 85 85 85
Sample Size(#) 3 3 4 13 9 6 9 6 8 7 10 9
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
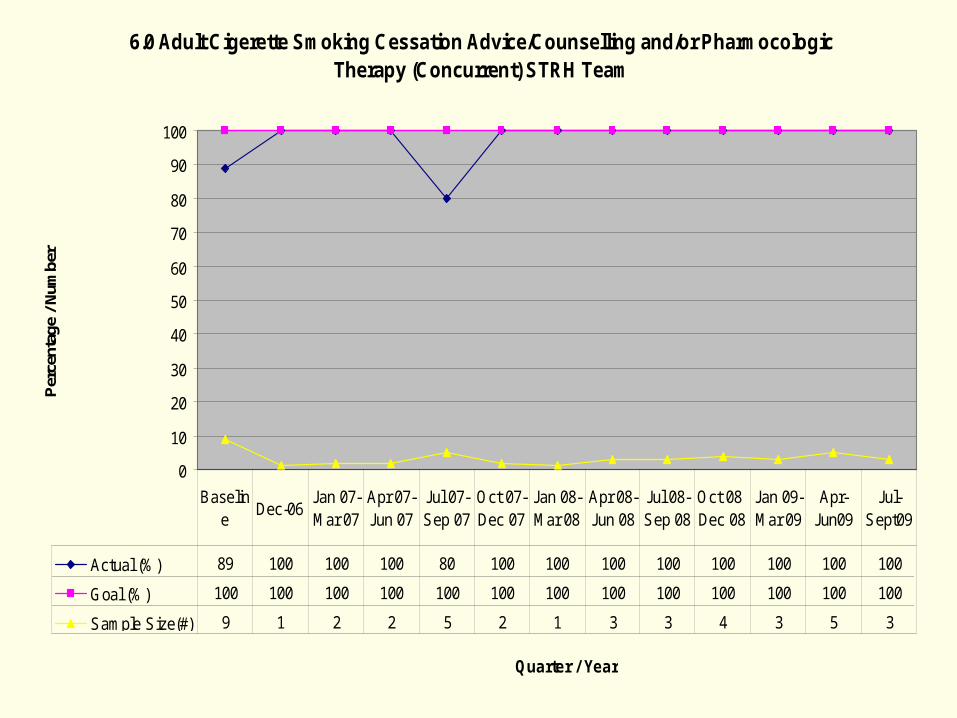
6.0 Adult Cigerette Smoking Cessation Advice/Counselling and/or Pharmocologic Therapy (Concurrent) STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 89 100 100 100 80 100 100 100 100 100 100 100 100
Goal (%) 100 100 100 100 100 100 100 100 100 100 100 100 100
Sample Size(#) 9 1 2 2 5 2 1 3 3 4 3 5 3
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
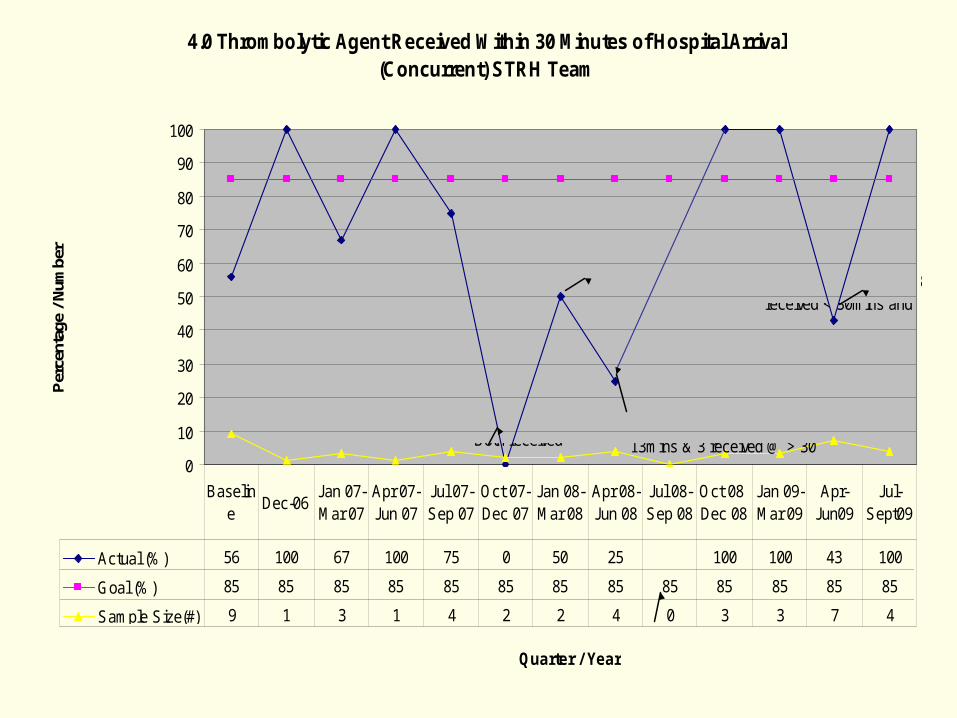
4.0 Thrombolytic Agent Received Within 30 Minutes of Hospital Arrival (Concurrent) STRH Team
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 56 100 67 100 75 0 50 25 100 100 43 100
Goal (%) 85 85 85 85 85 85 85 85 85 85 85 85 85
Sample Size(#) 9 1 3 1 4 2 2 4 0 3 3 7 4
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
There were 2 of 13 patients that qualified for inclusion for ST elevation MI.Both received
2 of 12 patients qualified for inclusion for STEMI.
4 of 17 patientsqualified for STEMI. Of the 4 in sample 1 received < 30mins @ 13mins & 3 received @ > 30
None qualified for sample July-Sept 08
8 of 18 patientsqualified for STEMI. 1 pt.refused (terminal) leaving a sample of 7. Of the 7 in the sample,3 received < 30mins and
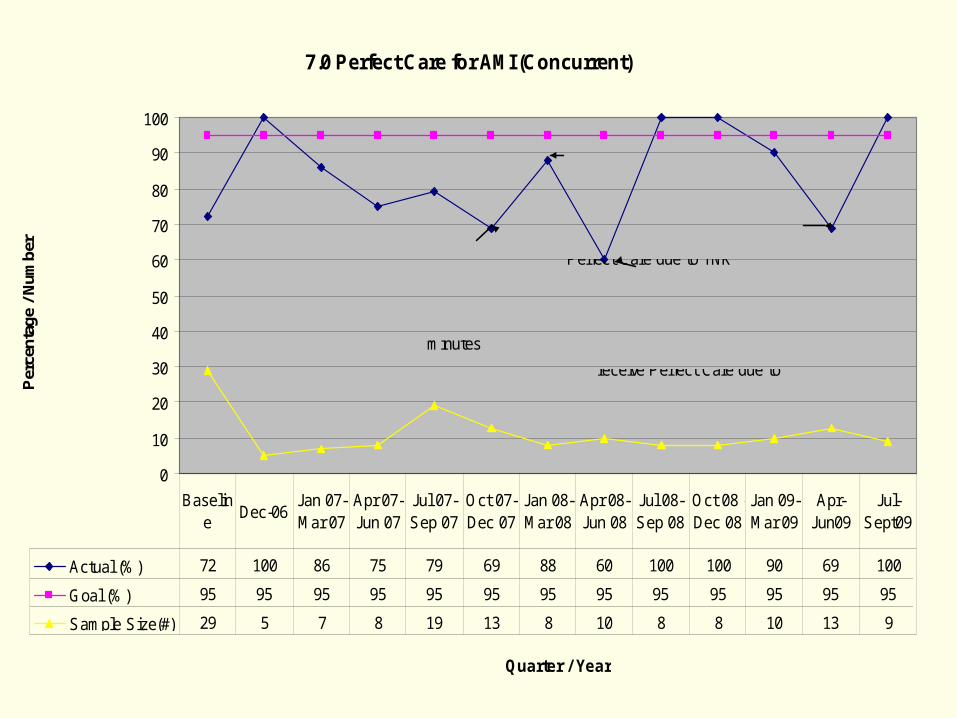
7.0 Perfect Care for AMI (Concurrent)
0
10
20
30
40
50
60
70
80
90
100
Quarter / Year
Per
cent
age
/ Num
ber
Actual (%) 72 100 86 75 79 69 88 60 100 100 90 69 100
Goal (%) 95 95 95 95 95 95 95 95 95 95 95 95 95
Sample Size(#) 29 5 7 8 19 13 8 10 8 8 10 13 9
Baseline
Dec-06Jan 07- Mar 07
Apr 07- Jun 07
Jul 07- Sep 07
Oct 07- Dec 07
Jan 08- Mar 08
Apr 08- Jun 08
Jul 08- Sep 08
Oct 08 - Dec 08
Jan 09- Mar 09
Apr-Jun09
Jul-Sept09
Of the 13 sample, 4 did not receive perfect care:2 no TPA within 30 minutes
Of the 12 sample 4 were transferred to HSC, so excluded. Of 8 remaining 1 did not receive Perfect Care due to TNK
Of the 17 sample 7 were transferred to HSC or WMH, so excluded. Of 10 remaining 4 did not receive Perfect Care due to
Of the 18 sample 5 were transferred to HSC or WMH, so excluded. Of 13 remaining 4 did not receive Perfect Care
CHALLENGES AT STRH
DELAYED PRESENTATION MODE OF ARRIVAL TRIAGE EKG AVAILIBILITY CLOCK ASYNCHRONY ER PHYSICIAN REQUIRING CONSULTATION PT. RELUCTANCE TO HAVE TNK ALTERNATIVE DIAGNOSIS W/U PROPER DOCUMENTATION
STRH efforts to decrease DNT
LONG TERM: PUBLIC EDUCATION ↑ AWARENESS RECOGNITION OF SYMPTOMS NEED TO SEEK EVAL ASAP UTILISE EMS APPROPRITELY
EMS SERVICES: ASPIRIN ASAP WHEN INDICATED EKG FIBRINOLYTIC AFTER DIAGNOSTIC EKG
STRH EFFORTS TO DECREASE DOOR TO NEEDLE TIME
EXPEDITIOUS TRIAGE LOW THRESHOLD FOR ACS EKG ASAP < 5 MIN ASPIRIN ASAP CLOCKS SYNCHRONISATION PROPER DOCUMENTATION MEDICAL STAFF CME SESSIONS TNK ASAP PATIENT EDUCATION
SUMMARY
DNT < 30 min. still not attained in significant percentage of the patients
Triage, first EKG and review ASAP
Continued comprehensive effort is required to improve the DNT
Site specific contributing factors should be identified and improved to meet the bench marks
THANKS
QUESTIONS ?
Cape Breton Regional Hospital
Anne Buchanan & Sharon MacLeod
• Cape Breton Regional Hospital is part of the Cape Breton District Health Authority in Nova Scotia. District 8
• CBRH is the Level 2 trauma center for the island.
• The District provides primary, secondary and tertiary care to about 130,000 people. Each year the District has more than 15,000 patient admissions, more than 125,000 Emergency Room visits and approximately 24,000 Ambulatory Care Visits.
• In total, the District has 466 Acute Care beds and 207 Veteran and Continuing care beds.
Who We Are
The CBRH AMI Collaborative
AIM Door to Thrombolytic within 30mins for 90% of
patients presenting with AMI by
March 30th 2010
AIM
Sponsor
Martha McLean Nursing Director for Critical Care Services
Co-Leads
Anne Buchanan Nursing Unit Manager ED
Sharon MacLeod Clinical Leader ED
Members
EKG dept ( Mgr & tech),Frontline ED Nursing Staff member, Medical Director Emergency Medicine,
Representative from EHS,NUM Coronary Care, Patient Safety Coordinator & Ward Clerk ( data entry)
Team Members
PDSA Cycles Tested • Education re collaborative ( posters, email, in-service)• Syncing of Clocks to EKG machine• Data collection form (staff involvement…FUN initiative)• Recommendations from CBDHA industrial engineer re process
improvement • Alert EKG of room location (board marked with room #)• Consistent person calling EKG tech (triage nurse)• Patient Labeling of EHS EKGs for chart ( to improve data
collection)• Revision to data collection form ( improvement to data)• EKG machine ‘Homed’ in department **(for EKG use only)• Lytic boxes # (ease to track use for data collection)
Change Ideas
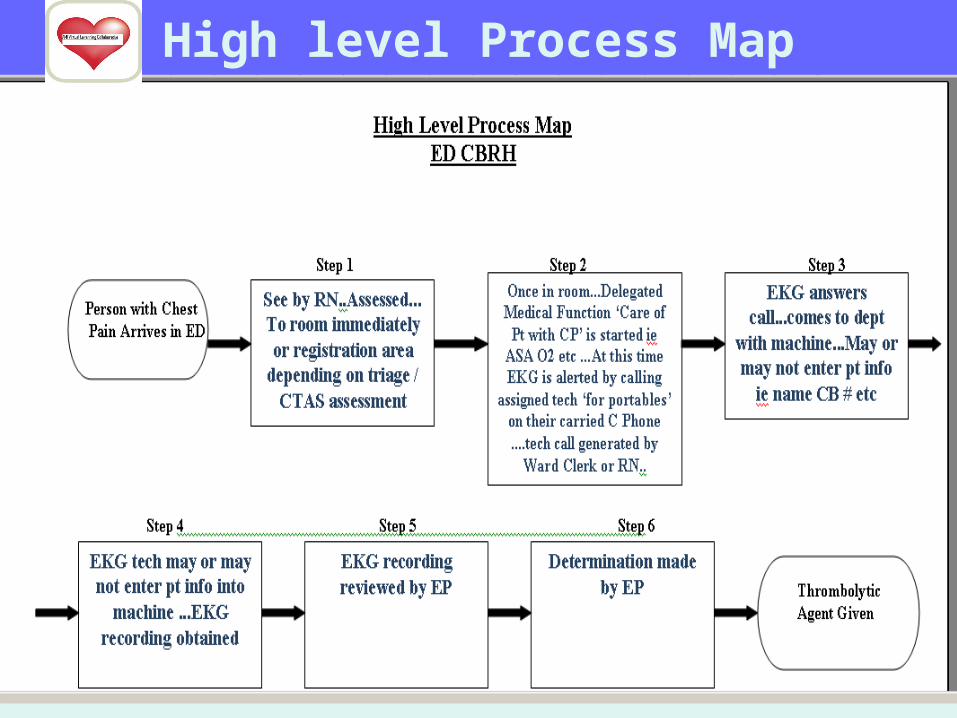
High level Process Map
Recommendations to another team
• Give an incentive to collect data ( $$ talks…gift card)
• Involve all stake holders in education in-service regarding change from the beginning (nurses, EKG techs , ward clerks etc)
• Keep staff updated on data• Need a MD who supports the standards!!!
Change Ideas
October..........34%
November……45%
December……49%
Measures (EKG)
What advice would you give to other teams?• Persistence, Patience and Prayer• Stay Motivated
What are your key insights?• Always keep going back to the patient and time is muscle. • Keep your AIM always in mind.• That sometimes change is difficult • With change there is not always improvement but with
improvement change is required.
Lessons Learned
What are some things we will be working
on in Action Period #2
Improving time to EKG…Data collection
Continuing to work toward or AIM of 90%
Next Steps
A Peak at our Dept
When All Else Fails
Eastern Health: HSC SiteSt. John’s, NL
AMI team

• Location of Facility• Number of ER Visits• Demographics
Who We Are
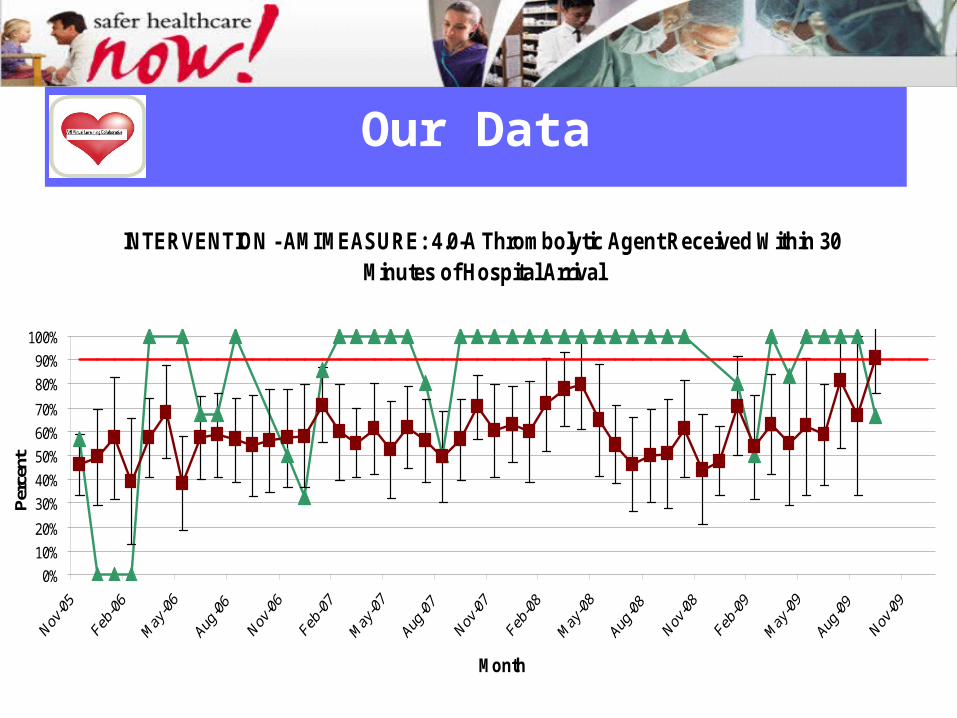
Our Data
INTERVENTION - AMI MEASURE: 4.0-A Thrombolytic Agent Received Within 30 Minutes of Hospital Arrival
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Month
Per
cent
• We are doing GOOD!
• Successful most months for timely administration of lytics
• Room for improvement
How the Data Informs our Work
• Not a lot of changes implemented• Our Process (What Works)
– Present to ER with CP • Triage first-2 paths
– 1. previous HX» Suspect cardiac pain
– 2. No HX» RAS (Risk assessment score)» Score > 11 put patient in monitored bed in ER
• ECG• TX plan Lytics/no lytics
• Staff pride in meeting benchmarks• Review charts and meet with ER Manager and educator
when not above or at goal
Change Ideas
• Need for improvement
• Why are we not consistently at or above goal?– Multifactorial
• Clock issues• Documentation (if not why not)• Improve Door to ECG time• Review process
– Where can we improve
Why take part in VLC
• Staff buy in – Executive - frontline– Importance of door to needle time (Time is muscle)– Poll staff on how to improve
• Review process map– How and where can we improve
• Complete and finalize Team Charter
Change Ideas
• Review clock issue
• ECG from bedside vs ECG technician
• Staff Education– Staff engagement and ownership
• Chart reviews for documentation
Next Steps
Break & Networking
Please be back at 1045 AST or 1115 NL
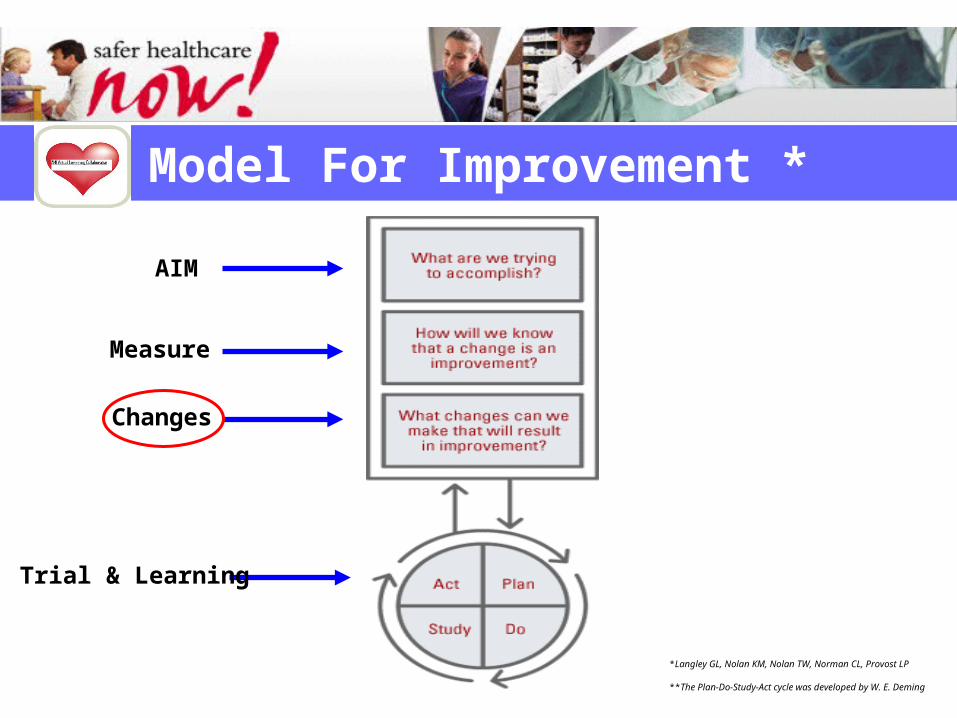
Model For Improvement *
*Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP
**The Plan-Do-Study-Act cycle was developed by W. E. Deming
AIM
Measure
Changes
Trial & Learning

Harvesting Ideas for Change
Making a Plan
Atlantic Node
1. Small GroupWrite list of changes that could lead to an improvement (10 minutes)
2. Large GroupRound Robin listing (white board)
Atlantic Node
Small Group: (5 minutes)
Select 1 change you are willing to test by next Tuesday• What: describe the change• Who?• When?• Where?• How?• What do you predict will happen?
Atlantic Node
Large Group:
Volunteer to share a change they will test by Next Tuesday.
Atlantic Node
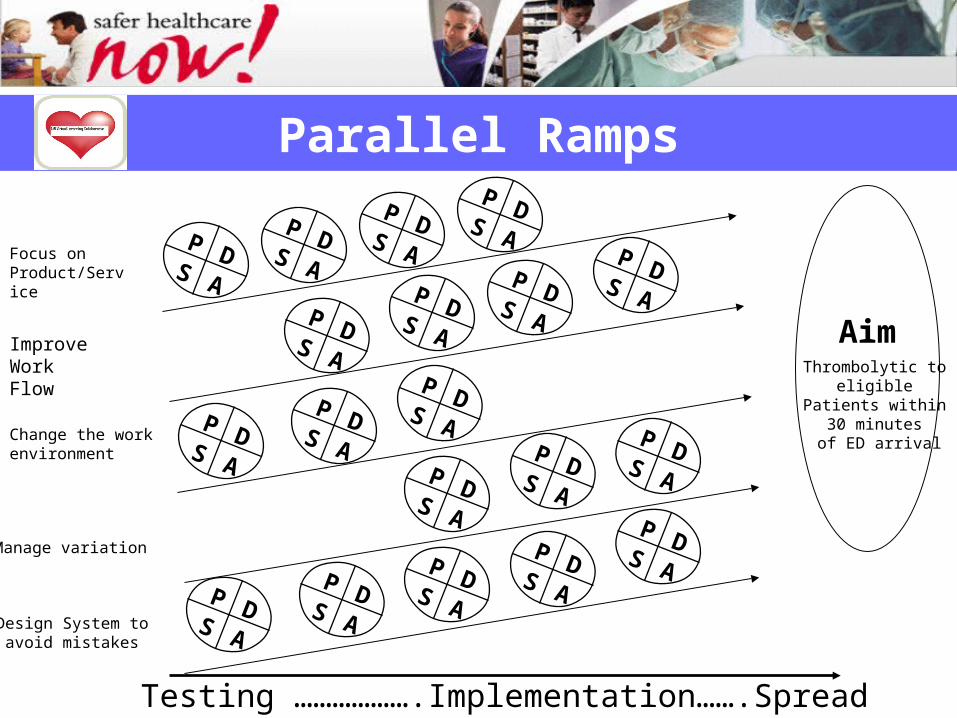
Parallel Ramps
Testing ……………….Implementation…….Spread
Aim
P DS A
Improve Work Flow
Focus on Product/Service
Change the work environment
Manage variation
Design System to avoid mistakes
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A P D
S A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
P DS A
Thrombolytic to eligible
Patients within 30 minutes
of ED arrival
Team Charter
Process Map
Baseline Data
PDSA Cycles
Monthly Reports
Community of Practice
Atlantic Node
Expectations

Atlantic Node
Q&A
Atlantic Node
Session Evaluation