Embed Size (px)
Citation preview

AMERICAN THORACIC SOCIETYDOCUMENTS
Diagnosis of Primary Ciliary DyskinesiaAn Official American Thoracic Society Clinical Practice GuidelineAdam J. Shapiro, Stephanie D. Davis, Deepika Polineni, Michele Manion, Margaret Rosenfeld, Sharon D. Dell,Mark A. Chilvers, Thomas W. Ferkol, Maimoona A. Zariwala, Scott D. Sagel, Maureen Josephson, Lucy Morgan,Ozge Yilmaz, Kenneth N. Olivier, Carlos Milla, Jessica E. Pittman, M. Leigh Anne Daniels, Marcus Herbert Jones,Ibrahim A. Janahi, Stephanie M. Ware, Sam J. Daniel, Matthew L. Cooper, Lawrence M. Nogee, Billy Anton,Tori Eastvold, Lynn Ehrne, Elena Guadagno, Michael R. Knowles, Margaret W. Leigh, and Valery Lavergne; on behalf ofthe American Thoracic Society Assembly on Pediatrics
THIS OFFICIAL CLINICAL PRACTICE GUIDELINE OF THE AMERICAN THORACIC SOCIETY WAS APPROVED MAY 2018
Background: This document presents the American ThoracicSociety clinical practice guidelines for the diagnosis of primary ciliarydyskinesia (PCD).
Target Audience: Clinicians investigating adult and pediatricpatients for possible PCD.
Methods: Systematic reviews and, when appropriate, meta-analyseswere conducted to summarize all available evidence pertinent to ourclinical questions. Evidence was assessed using the GRADE (Gradingof Recommendations, Assessment, Development and Evaluation)approach for diagnosis and discussed by amultidisciplinary panel withexpertise in PCD. Predetermined conflict-of-interest managementstrategies were applied, and recommendations were formulated,written, and graded exclusively by the nonconflicted panelists. Threeconflicted individuals were also prohibited from writing, editing, orproviding feedback on the relevant sections of the manuscript.
Results: After considering diagnostic test accuracy, confidence inthe estimates for each diagnostic test, relative importance of testresults studied, desirable and undesirable direct consequences ofeach diagnostic test, downstream consequences of each diagnostictest result, patient values and preferences, costs, feasibility,acceptability, and implications for health equity, the panel maderecommendations for or against the use of specific diagnostictests as compared with using the current reference standard(transmission electron microscopy and/or genetic testing) for thediagnosis of PCD.
Conclusions:The panel formulated and provided a rationale for thedirection as well as for the strength of each recommendation toestablish the diagnosis of PCD.
Keywords: primary ciliary dyskinesia; Kartagener syndrome; situsinversus; nitric oxide; diagnosis
ContentsGoals of This GuidelineIntroductionMethods
Committee Composition
Confidentiality Agreement andConflict-of-InterestManagement
Meetings and Conference CallsFormulating Clinical QuestionsLiterature Search
Evidence Review andDevelopment of ClinicalRecommendations
Manuscript PreparationRecommendations for SpecificDiagnostic Questions
Supported by a pediatric assembly grant through the American Thoracic Society, as well as in part by the Division of Intramural Research, NHLBI, NIH (K.N.O.).
An Executive Summary of this document is available at http://www.atsjournals.org/doi/suppl/10.1164/rccm.201805-0819ST.
ORCID IDs: 0000-0001-6066-6750 (A.J.S.); 0000-0002-9390-0651 (S. D. Davis); 0000-0003-2169-9407 (S. D. Dell); 0000-0003-1619-1393 (M.A.Z.);0000-0001-6051-5020 (O.Y.); 0000-0001-5515-3053 (C.M.); 0000-0001-6979-2681 (M.L.A.D.); 0000-0002-8263-1265 (M.H.J.).
Correspondence and requests for reprints should be addressed to Adam J. Shapiro, M.D., Pediatrics, Montreal Children’s Hospital, 1001 Boulevard Decarie,BRC.5016, Montreal, QC, H4A 3J1 Canada. E-mail: [email protected].
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Am J Respir Crit Care Med Vol 197, Iss 12, pp e24–e39, Jun 15, 2018
Copyright © 2018 by the American Thoracic Society
DOI: 10.1164/rccm.201805-0819ST
Internet address: www.atsjournals.org
e24 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

Question 1: Should an ExtendedGenetic Panel (Testing >12Genes) Be Used as aDiagnostic Test in Adult andPediatric Patients with a HighProbability (At Least Two ofFour Key Clinical Features) ofHaving PCD (as a Replacementof Reference Standards ofClassic TEM Structural CiliaryDefect and/or StandardGenetic Panel Testing forMutations in <12 GenesAssociated with PCD)?
Question 2: Should a Low nNOLevel (Detected withChemiluminescenceTechnology), after ExcludingCF, Be Used as a Diagnostic
Test for PCD in Adult andPediatric Patients 5 Years ofAge or Older with a HighProbability (At Least Two ofFour Key Clinical Features) ofHaving PCD (as Replacementof Reference Standards ofClassic TEM Structural CiliaryDefect and/or BiallelicCausative Mutations in PCDGenes)?
Question 3: Should HSVM AloneBe Used as a PCD DiagnosticTest in Adult and PediatricPatients with a High Probability(At Least Two of Four KeyClinical Features) of HavingPCD (as a Replacement ofReference Standards of
Classic TEM Structural CiliaryDefect and/or Biallelic CausativeMutations in PCD Genes)?
Question 4: Should CBF or CiliaryWaveform Analysis Using LightMicroscopy without High-Speed Recording Be Used as aPCD Diagnostic Test in Adultand Pediatric Patients with aHigh Probability (At Least Twoof Four Key Clinical Features)of Having PCD (asReplacement of ReferenceStandards of Classic TEMStructural Ciliary Defect and/orBiallelic Causative Mutations inPCD Genes)?
Conclusions: Proposed DiagnosticAlgorithm
Goals of This Guideline
The purpose of this guideline is toanalyze evidence and present diagnosticrecommendations for primary ciliarydyskinesia (PCD). The guideline shouldempower clinicians to interpret theserecommendations in the context of theindividual patient and make appropriateclinical decisions about diagnostic tests. Foreach recommendation, it is important toconsider both the summary of evidencereviewed and discussed by members ofthe committee, especially patient valuesand preferences, before applying theserecommendations to specific clinicalsituations or policy decisions.
Clinicians, patients, and otherstakeholders should never view theserecommendations as dictates. No guidelinecan account for all clinical circumstances.The implications of the strength of therecommendations are described in Table 1.
This guideline applies the samereference standard for all clinical questions,but it does not necessarily providerecommendations for one diagnostic testover another or advocate for or againstcombinations or sequential tests. However, asuggested diagnostic algorithm for PCD isprovided as part of this document. Strong orconditional ratings for each recommendationmust be weighed individually (i.e., tworecommendations with the same strong orconditional rating should not by default beconsidered equivalent recommendations),
factoring in all components used todetermine the grade of the recommendation,including the confidence in accuracyestimates of each diagnostic test; the relativeimportance of test results studied; desirableand undesirable consequences of eachdiagnostic test; and the cost, feasibility,acceptability, and implications of eachdiagnostic test. The methods used byguideline panels to appraise the evidenceare different from those employed duringregulatory agency reviews of applicationsseeking market approval.
From the outset of guidelinedevelopment, the workgroup made certainassumptions. First, with PCD being aheterogeneous disease, no referencediagnostic standard is universally accepted.Thus, the workgroup proposed thecombination of transmission electronmicroscopy (TEM) ultrastructural ciliarydefect and/or genetic panel testing formutations in known PCD genes as the mostaccurate “reference standard” for diagnosingPCD. Second, per the GRADE (Gradingof Recommendations, Assessment,Development and Evaluation) approach,the effects of diagnostic test results onpatient-important clinical outcomes mustbe assessed to develop recommendations.With PCD being a rare disease, frequentlymisdiagnosed in past cohorts, and managedwith a wide range of unproven therapies,the workgroup considered that long-termeffects of appropriate/inappropriatediagnostic decisions would make modeling
of diagnostic results imprecise. Thus, theworkgroup decided to rank the importanceof the test results, patient-importantoutcomes, and overall certainty in theevidence of effect of the test separately fromthe certainty in diagnostic test accuracy.
Introduction
PCD is a genetically heterogeneous,autosomal recessive disorder characterizedby motile cilia dysfunction. Clinicalmanifestations of PCD include chronicupper and lower airway disease, left–rightlaterality defects, and infertility (1–4). Thediagnosis is often delayed, even in childrenwho have characteristic clinical features ofPCD, in part related to limitations ofavailable diagnostic tests. For over fourdecades, the diagnosis of PCD has beenbased on the presence of ultrastructuraldefects in the ciliary axoneme using TEManalysis, which can have serious drawbacks.Nonspecific ciliary changes, which can beinduced by exposure to environmentalpollutants or infection, may appear similaras visualized by TEM to findings seen inPCD. Also, the absence of axonemal defectsdoes not exclude PCD, because 30% of allaffected individuals have normal ciliaryultrastructure (5). Other diagnostic testshave emerged, including nasal nitric oxide(nNO) measurement, genetic testing, digitalhigh-speed video microscopy with ciliarybeat pattern analysis (HSVM), andimmunofluorescence imaging for specific
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e25

axonemal proteins. However, there is nouniversally agreed-upon “gold standard” fordiagnosis, and no single modality hassufficient diagnostic sensitivity andspecificity when applied to the generalpopulation (1, 6).
Some clinical features of PCD canoverlap with other conditions, such as cysticfibrosis (CF), immunodeficiency, pulmonaryaspiration, asthma, and recurrent viralrespiratory infections. However, PCD is not adiagnosis of exclusion. Recently, investigatorsidentified four key clinical featurescharacteristic of PCD (7). 1) Year-round,daily, productive (wet) cough and 2) year-round, daily, nonseasonal rhinosinusitis beginin early childhood, often shortly after birth,and are almost universally present by6 months of age. These respiratory symptomsmay vary but never fully resolve, evenafter systemic antibiotic therapy (6).Approximately 80% of children with PCDhave a history of 3) neonatal respiratorydistress syndrome as term newborns, definedas the need for supplemental oxygen orpositive pressure ventilation support for morethan 24 hours without clear explanation(6–9). Roughly 40–55% of patients with PCDhave 4) laterality defects (e.g., situs inversustotalis), whereas other situs anomalies (e.g.,situs ambiguus), with or without congenitalheart defects, are found in roughly 12% ofaffected individuals (4, 10). If two of thesedistinguishing features are present, thesensitivity and specificity for PCD are 80%and 72%, respectively. If all four are present,the sensitivity and specificity are 21% and99%, respectively (7). Chronic otitis mediawith effusion is also common in children withPCD, and many require tympanostomy tubeplacement before 5 years of age (8), but this
feature does not distinguish children withPCD from those who do not have PCD. Interm newborns, the combination of situsinversus totalis and unexplained neonatalrespiratory distress is highly suggestive ofPCD, even in infants who have not yetdeveloped chronic respiratory symptoms.Without at least two of these key features,patients are unlikely to have PCD, andfurther testing is usually unwarranted. Thus,clinicians should consider diagnostic testingfor PCD only in those patients who truly fitthe clinical phenotype.
Other diagnoses should be consideredon the basis of a detailed clinical history. Theotosinopulmonary features of PCD overlapwith symptoms of CF, another geneticdisorder of mucociliary clearance. Childrenwith CF typically do not have neonatalrespiratory distress or chronic otitis media,nor do they have daily cough until lungdisease has significantly progressed.Nonetheless, children being evaluated forPCD should undergo sweat chloride testingat a laboratory certified to perform sweatchloride measurements. Similarly, variousimmunodeficiencies may also present withchronic upper and lower respiratory tractinfections, though not typically with daily,year-round symptoms. Depending on theclinical manifestations, a complete bloodcount with leukocyte differential, serumquantitative immunoglobulin levels,serological assays for specific antibodies asa measure of vaccine response, and totalserum complement levels should bemeasured. Although this testing does notfully exclude immune dysfunction, majordeficiencies will usually be identified.Further evaluation by an immunologist maybe required in some cases. Chronic
aspiration may also manifest as chroniccough and recurrent pulmonary disease.Asthma and bronchial hyperreactivity maycoexist with PCD, but they can be furtherexplored with bronchial provocation testingor bronchodilator response testing.
Methods
Committee CompositionThis guideline committee consisted of 2cochairs (A.J.S. and V.L.), 2 co–vice-chairs(S. D. Davis and M.M.), 12 additionalpediatric pulmonologists with PCDexpertise, 5 adult pulmonologists with PCDexpertise, and 1 of each of the followingexperts: PCD genetics, cardiology/genetics,pediatric radiology, pediatric otolaryngology,and neonatology. There were fourrepresentatives from PCD advocacy groups,including two adult patients with PCD andtwo parents of pediatric patients with PCD.The committee worked with a health researchmethodologist (V.L.) who has expertise inevidence synthesis and the guidelinedevelopment process. This methodologist,who is a clinician and also has expertise inclinical diagnostic laboratory tests, conductedsystematic reviews and prepared the evidencesummaries following the GRADE approach asdescribed previously (11).
Confidentiality Agreement andConflict-of-Interest ManagementCommittee members signed aconfidentiality agreement and disclosedpotential conflicts of interest according toAmerican Thoracic Society (ATS) policy. Allconflicts were successfully managed. At least50% of the committee chairs, vice-chairs, and
Table 1. Interpretation of Strong and Conditional Recommendations for Stakeholders (Patients, Clinicians, and Healthcare PolicyMakers)
Implications for Strong Recommendation Conditional Recommendation
Patients Most individuals in this situation would want therecommended course of action and only a smallproportion would not.
The majority of individuals in this situation would want thesuggested course of action, but many would not.
Clinicians Most individuals should receive the intervention.Adherence to this recommendation according to theguideline could be used as a quality criterion orperformance indicator. Formal decision aids are notlikely to be needed to help individuals make decisionsconsistent with their values and preferences.
Recognize that different choices will be appropriate forindividual patients and that you must help each patientarrive at a management decision consistent with his or hervalues and preferences. Decision aids may be useful inhelping individuals to make decisions consistent with theirvalues and preferences.
Policy makers The recommendation can be adopted as policy in mostsituations.
Policy making will require substantial debate andinvolvement of various stakeholders.
AMERICAN THORACIC SOCIETY DOCUMENTS
e26 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

members were free from industry ties. Twelveof 30 members with recognized expertise inPCD (A.J.S., S. D. Davis, S. D. Dell, M.R.,T.W.F., D.P., M.J., M.R.K., C.M., S.D.S.,M.W.L., and L.M.) reported ties to industry-sponsored research as primary investigatorsin PCD therapeutic trials; however, theserelationships were easily managed for thisdiagnostic guideline, which does not evaluatePCD therapies. Three members (M.W.L.,S. D. Davis, and T.W.F.) reportedinvolvement in clinical trials with a novelnitric oxide measurement device, and thesemembers participated in the discussion of theevidence with the rest of the committee butwere recused from discussions related to theevidence-to-decision framework as well asfrom formulating, writing, and gradingrecommendations related to nNO testing.The conflicted members were allowed to stayin the same room to provide expert inputwhile discussions among nonconflictedmembers took place; however, the memberscould do so only when specifically requestedby nonconflicted members. Adherenceto the rules was strict, with one of thecochairs (A.J.S.) responsible for monitoringthe discussions for adherence to these rules. Themethodologist also participated in discussionsbut was a nonvoting participant.
Meetings and Conference CallsFace-to-face committee meetings were heldat the ATS annual conferences in Denver,Colorado (May 2015), and in San Francisco,California (May 2016), and at the PCDFoundation conference in Minneapolis,Minnesota (August 2017). Members whocould not attend were invited to participate viateleconference. Additional planning meetingswere held regularly over the telephone betweenA.J.S. and S. D. Davis. Conference calls ande-mail correspondence were used to discussspecific issues requiring input from others.
At the Denver meeting, a group ofcommittee members (n = 18) discussed thescope and objectives of the project andformulated clinically relevant questions,each dealing with a different diagnostic test.This process was monitored and approvedby the lead ATS methodologist (J. Brozek).For each of the four proposed clinicalquestions, a subcommittee was responsiblefor all remaining steps of the process.After various editing done via e-mailcommunications, the four questions werefinalized during a conference call inOctober 2015. At the San Franciscomeeting, committee members (n = 19) met,
evidence summaries were presented anddiscussed, and the recommendations wereformulated for three of the four clinicalquestions. All meetings were attended bystaff from the ATS documents committee.One member (D.P.) took detailed notes onall conversations and decision makingconducted at the meetings. Members whocould not attend were invited to participatevia teleconference (M.L.C. in 2016, fivemembers in 2017). The first clinicalquestion, regarding genetic testing, wasrevised under the guidance of thecommittee methodologist and the lead ATSmethodologist (see FORMULATING CLINICAL
QUESTIONS subsection below). A follow-upconference call was held in January 2017,and e-mail communications were finishedby July 2017 to complete the guidelinedevelopment for this remaining question.The final committee meeting inMinneapolis (n = 19) was held to discussthe strength of final recommendations,and greater than 70% agreement throughanonymous online voting was required tomake a strong recommendation. The ATSprovided financial and logistical support formeetings and conference calls. The viewsand interests of the ATS had no influence onthe topics discussed and recommendationsmade.
Formulating Clinical QuestionsThe committee created four questions withdirect relevance to clinical challengescommonly faced by physicians and patientssurrounding PCD diagnosis. Specificattention was paid to creating questions thatwere relevant to centers without expertise inPCD, which commonly encounter diagnosticdifficulties with PCD. The committeeidentified possible results for each testevaluated with each question and explicitlyrated their relative importance (from theperspective of a patient suspected of havingPCD) from not important to critical,following the approach suggested by theGRADEworking group for diagnosis (11–14).Despite providing an indirect link to clinicaloutcomes, ranking test results by theirrelative importance helps focus attentionon those that are most relevant to patientsand helps resolve or clarify potentialdisagreements in decision making. Criticaltest results uniformly selected for all fourquestions include maximizing true-positiveresults as well as limiting false-negativeresults, thus favoring tests with highsensitivity. To this end, the committee
reasoned that delays in diagnosis andtreatment of PCD may be harmful but thatstarting nontoxic therapies (such as dailyairway clearance and aggressive antibiotics)in patients who may not have PCD(i.e., false-positive results) would be beneficial(and not harmful) in any chronic suppurativelung disease, regardless of the underlyingcause. Rankings of all outcomes were agreedon through consensus of the committee.
The clinical question regarding genetictesting for diagnosis of PCD was initiallycreated with three separate subquestions.These questions were formulated whencommercial genetic testing was notcomprehensive, with panels investigatingonly 12 to 19 PCD genes, providing PCDmutation detection rates estimated at only50%. However, midway through the firstyear of this guideline process, access toextended genetic panel PCD testing becamecommercially available when one companyintroduced a 32–PCD gene next-generationsequencing (NGS) panel, includingdeletion/duplication analysis. The new32-gene panel was estimated to detect atleast 70% of PCD mutations, which iscomparable to properly performed TEMstudies. With the increased access toextended genetic panel testing, thecommittee decided that the question ongenetic diagnosis of PCD should bereformatted to address the possible benefitsof extended genetic PCD panels becausethis would be most useful to cliniciansattempting to diagnose PCD. In January2017, this genetic testing question wasslightly reformatted to reflect this new goal,and subquestions were removed. Initially,this question included scenarios in whichgenetic testing would be pursued dependingon nNO testing results. Ultimately, thesubcommittee believed that this pathwaywas not clinically relevant, because accessto nNO testing is often not available toclinicians investigating PCD, and the stand-alone diagnostic accuracy for PCD genetictesting is much more relevant to clinicians.
Literature SearchA senior medical librarian (E.G.) designeda search strategy using medical subjectheadings and text words from the title,abstract, and keyword fields, limited tohuman studies and articles in any language.The following databases were searched frominception forward: MEDLINE (PubMed),PubMed (National Library of Medicine),Embase (Ovid), BIOSIS (Ovid), Web of
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e27

Science (Thomson Reuters), Scopus(Elsevier), Cochrane (Wiley), Africa-WideInformation (EBSCO), AMED (Ovid), andGlobal Health (Ovid) (see the onlinesupplement). Two updates were made,in September 2015 and in July 2016.Additional publications not included inthe search were added individually fromcommittee members’ personal libraries.Reviewers evaluated previous meta-analysesfor additional articles. Two reviewers (A.J.S.and D.P.) screened titles and abstractsto identify articles for full review andevaluated the full text of articles deemedpotentially relevant by either reviewer usingpredefined inclusion and exclusion criteria.Articles identified for full-text review wereregrouped by topicality and furtherevaluated by each subcommittee accordingto inclusion/exclusion criteria specific totheir question. These specific criteria wereagreed on a priori by each subcommitteeand varied between questions.Disagreement was resolved by groupdiscussion with the chairs and cochairs.
Evidence Review and Development ofClinical RecommendationsFirst, data abstraction occurred independentlyand in duplicate (by one subcommitteemember and one chair) for all included studiesfor each diagnostic question using predesigneddata abstraction forms that had been pilotedbefore being used. Disagreements wereresolved through discussion with a thirdmember. In addition to accuracy, individualstudy risk of bias and applicability wereassessed independently by two reviewers(V.L. and A.J.S.), using the revised QualityAssessment of Diagnostic Accuracy Studies(QUADAS-2) tool (15). During the dataextraction phase, authors of accepted articleswere contacted via e-mail if inconsistencies inthe article text or data were found. Authorcontact was established to investigatemethods that were unclear; to quantifyreference diagnostic data when not included;and to clarify contentious issues in PCDdiagnosis, such as inclusion of isolated innerdynein arm (IDA) defects in the referencestandard of diagnosed PCD. If authors didnot respond to several e-mail attempts or theimprecision was not resolved, their articleswere excluded from further analysis.
Subsequently, diagnostic test accuracyestimates were pooled and meta-analysesperformed for each test using ReviewManager version 5.3 (The CochraneCollaboration) and STATA version IC 14
(StataCorp) software. For this guideline, weliberally used the term “diagnostic testaccuracy” when referring to the differentmeasures used to evaluate the ability of atest to discriminate between the targetcondition and health (such as sensitivityand specificity or negative and positivepredictive values) rather than the formalstatistical meaning. Pooling and meta-analyses of study data were performed bythe methodologist (V.L.) when appropriate.Of note, pooled analysis presented inthis document may at times differ fromother published meta-analyses, owing todifferences in inclusion and exclusioncriteria. The meta-analysis for the clinicalquestion on the diagnostic accuracy of nNOwas published before finalization of therelated recommendation provided in thisguideline (16).
Evidence tables for each question wereprepared by the methodologist, followingthe GRADE approach for diagnosis (11, 13,17) and using the GRADEpro GuidelineDevelopment Tool online software (18).The certainty in test accuracy (also knownas confidence in accuracy estimates)was first assessed as per the GRADErecommendation for diagnosis—that is,after evaluating the five domains (risk ofbias, precision, consistency, directness ofthe evidence, and other considerations)—and graded into one of four levels: high,moderate, low, or very low. All committeemembers reviewed the evidence profiletables, and modifications and additionswere made when appropriate.
Development of recommendations foreach question was based on the GRADEevidence-to-decision frameworks fordiagnosis using the GRADEpro GuidelineDevelopment Tool online software (18).This framework helped organize discussionaround each recommendation and ensuredthat each of the following factors wasconsidered: the test accuracy with itsassociated certainty, the balance of desirableand undesirable consequences of compareddiagnostic options, the link between testresults and management decisions, theeffects of the management guided bythe tests results, the overall certainty of theevidence of effects of the test, the patients’values and preferences, the implicationsfor resource use and health equity, theacceptability of the test to stakeholders, andthe feasibility of implementation (19). Theoverall certainty of evidence for eachrecommendation (i.e., the certainty of
the effect of testing and subsequentmanagement decisions on patient-important outcomes) was assessedfollowing the GRADE approach fordiagnosis and categorized into one of fourlevels: high, moderate, low, or very low(19). Recommendations and their strengthwere decided by consensus throughanonymous online voting by committeemembers. The committee agreed on thefinal wording of recommendations andremarks with further qualifications foreach recommendation (e.g., subgroupconsiderations, justification, implementationconsiderations), and a unified diagnosticalgorithm was created and accepted by thecommittee. The recommendations wereeither “strong” or “conditional” according tothe GRADE approach (20, 21). As suggestedby GRADE, we used the phrasing “werecommend” for strong recommendationsand “we suggest” for conditionalrecommendations. Table 1 providessuggested interpretation of theserecommendations by intended stakeholders,including patients, clinicians, and healthpolicy makers.
The committee encountered challengesin adopting strengths of recommendation,notably for the questions on nNO andextended genetic panel testing asreplacements of the reference standard. Theanalysis for these tests provided moderatecertainty of evidence in diagnostic testaccuracy, and over 70% of committeemembers initially voted for “strong”recommendations in this diagnosticguideline. However, long-term, patient-important outcome data are lacking inPCD, and there is major uncertaintyregarding the impact of PCD diagnosis onlong-term patient health (i.e., very lowcertainty in the overall evidence). This ledto the final strengths of recommendationfor nNO and extended genetic panel testingbeing downgraded to “conditional”recommendations, despite the committee’s(including all PCD stakeholders) opinionthat diagnostic test accuracy should be ofprimary importance in the decision-makingprocess of a diagnostic guideline. Thisdiscrepancy highlights the challenges ofmaking strong diagnostic recommendationsfor rare diseases, because even perfectdiagnostic accuracy will often result in aconditional recommendation withoutlong-term outcome data, which doesnot exist for many rare diseases. Thecommittee believed that novel approaches
AMERICAN THORACIC SOCIETY DOCUMENTS
e28 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

to this challenge should be investigatedby the GRADE consortium and otherregulatory bodies overseeing diagnosticclinical practice guidelines.
Manuscript PreparationThe writing committee (A.J.S., S. D. Davis,D.P., V.L, J.E.P., and T.W.F.) drafted theguideline document. The manuscript wasthen reviewed by the entire committee.Feedback was provided primarily throughelectronic communication and telephoneconference calls, which included some of thecommittee members. The entire committee(both conflicted and nonconflictedmembers) had the opportunity to correctfactual errors, clarify the presentation ofbackground information or evidencesummaries, and suggest changes to therationale sections if they improperlycaptured the discussion from the face-to-facemeetings. The wording of recommendations(including strength and direction) was notaltered once recommendations were finalizedduring the face-to-face meetings andteleconferences. The chairs (A.J.S., S. D.Davis, M.M., and V.L.) confirmed that thewritten version of the guideline reflected therecommendations made by the committeemembers. The same process was followed foreach version of the document. The finalapproved version was submitted to the ATSfor peer review.
Recommendations forSpecific DiagnosticQuestions
Question 1: Should an ExtendedGenetic Panel (Testing >12 Genes) BeUsed as a Diagnostic Test in Adultand Pediatric Patients with a HighProbability (At Least Two of Four KeyClinical Features) of Having PCD (as aReplacement of Reference Standardsof Classic TEM Structural CiliaryDefect and/or Standard Genetic PanelTesting for Mutations in <12 GenesAssociated with PCD)?
Background. PCD is a geneticallyheterogeneous and predominantlyautosomal recessive disorder caused bybiallelic pathogenic mutations in one of themany identified PCD causative genes (39 todate). Each PCD diagnostic test carrieslimitations, and those tests dependent onrespiratory mucosal (ciliary) biopsy (TEM,
ciliary beat frequency [CBF], and HSVM)are encumbered by the need for on-sitehigh-quality specimen sampling, processing,and analysis. The widespread lack of localexpertise and resources in ciliary biopsytesting has made molecular genetic testingan attractive alternative. Genetic testing fora Mendelian disease has the added valueof procuring inherently high specificity;however, sensitivity may be expected tobe lacking in a genetically heterogeneousdisease such as PCD. In a comprehensivereview of the PCD literature in 2015,Zariwala and colleagues demonstrated thatmore than 50% of patients with PCD possesstwo pathogenic mutations in trans in aknown PCD causative gene (22). However,the sensitivity of genetic testing isanticipated to increase as commercialdiagnostic panels incorporate novelidentified PCD genes. Because genetictesting for PCD is already available inClinical Laboratory ImprovementAmendment–certified laboratories andcosts have been decreasing, the impetusto consider molecular genetic testing as afirst-line diagnostic test for PCD isincreasing.
Specific methodology. Studies usingmultigene panels, with sample sizes of 10 ormore subjects, for diagnostic assessment ofPCD were evaluated. After the initial reviewof titles and abstracts (see the onlinesupplement), 91 records were identified forfull-text review to determine their eligibilityfor inclusion in the analysis. The genetictesting subcommittee members (S. D. Dell,D.P., M.A.Z., and S.D.S.) agreed oninclusion and exclusion criteria for full-textreview of all 91 articles (see Figure E1.1 inthe online supplement). The committeeexcluded 86 articles from the analysis onthe basis of lack of multigene analysis,sample size of less than 10 patients, articleaddressing only disease carrier frequency,or lack of genetic testing information (seeSection E1 of the online supplement). Fivearticles were eligible for evidence synthesis(7, 23–26); however, two of these articlesused the same patient cohort (25, 26). Fourstudies included only PCD cases and thuscould not provide complete diagnosticaccuracy information (23–26). One cohortstudy that evaluated genetic and TEMtesting in a population of patients referredfor suspected PCD was included in thedata analysis (7). When necessary, weobtained additional data from authors tocompare genetic testing results with our
prespecified reference standard for thisquestion.
Summary of evidence. In the singleanalyzed article, Leigh and colleaguesprospectively evaluated 534 pediatric subjectsreferred to a multicenter consortium for highclinical suspicion of PCD (7). Subjectsinvariably had chronic otosinopulmonarydisease symptoms, with CF already ruled outin most cases. All subjects underwent TEMand NGS genetic testing of 26 known PCD-causing genes. Two hundred five participantswere diagnosed as “definite PCD” per ourreference standard of classic TEM structuralciliary defect and/or standard genetic paneltesting for mutations in up to 12 genesassociated with PCD. Among this cohort of205 patients with definite PCD, 164 patientscarried two pathogenic variants in a PCDgene (138 detected with the standard geneticpanel, 26 additional ones detected withextended genetic panel testing), and 41patients showed classic TEM defects withnegative extended genetic panel testing. Onehundred eighty-seven were categorized as“other diagnosis or undefined” (i.e., absenceof classic TEM structural ciliary defectand/or absence of standard genetic paneltesting for mutations in <12 genesassociated with PCD), among whom 186participants had a negative 26-gene panel.The remaining 142 participants with acompatible PCD clinical phenotype and lownNO measurements, but no identified TEMdefect or disease-causing gene, were labeledas “probable/possible PCD.”
The sensitivity for the diagnosis of“definite PCD” by an extended geneticpanel (.12 genes) in this study was 80%,indicating that 20% of patients werediagnosed by TEM alone (without acausative PCD gene found). Despite the factthat 142 patients with “possible/probablePCD” could have been considered to havetrue negative results according to ourreference standard, the panel membersbelieved that these patients probably hadPCD and thus had potential false-negativeresults. However, without a clear referencestandard diagnosis, these patients wereexcluded from our analysis, and the risk ofbias was increased according to QUADAS-2(Figures E1.2 and E1.3 and Table E1.1). In aworst-case scenario, if we were to assumethat all of these patients had false-negativeresults, the sensitivity of the extended geneticpanel would considerably decrease to 47%.
The specificity for PCD diagnosis was99.5% in the analyzed study, indicating that
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e29

0.5% of patients were identified by theextended panel alone without being detectedby TEM and/or a standard panel of up to 12genes (our reference standard). Specifically,one case was considered a “false-positiveresult” owing to a positive SPAG1 generesult on the extended gene panel whenthe TEM result was nondiagnostic.Importantly, nearly all cases of PCDdetected by the extended gene panel, butmissed on the standard panel, were alreadydetected by TEM defects.
Although we were unable to analyze thespecificity of PCD diagnosis in the four case-series studies, we were able to calculatesensitivities of each published extendedgenetic panel compared with ourprespecified reference standard. Largely, thesensitivity of the genetic panel test improvedwith the increasing number of genes testedfor PCD. Sensitivities were 71.9% whentesting 12 genes (25), 73.3% when testing 19genes (23), 54.8% when testing 24 genes(24), 80% when testing 26 genes (7),and 93.9% when testing 32 genes withdeletion/duplication analysis (26). Thelower sensitivity of 54.8% with the 24-genepanel (24) may be due to differences inpopulation stratification, because PCDgenes included in this panel were similar tothose in other studies. Importantly, twostudies conducted genetic testing in thesame patient population (n = 45 families)and directly demonstrated increasingsensitivity as the number of analyzed PCDgenes increased (sensitivity of 71.9% with12-gene panel increased to sensitivity of93.9% with 32-gene panel includingdeletion/duplication analysis) (25, 26).
Recommendation. In patientspresenting with a strong clinical phenotypefor PCD, we suggest using an extendedgenetic panel as a diagnostic test over TEMciliary testing and/or standard (<12 genes)genetic panel testing (conditionalrecommendation, moderate certainty ofevidence in test accuracy but very lowcertainty in the overall evidence). Amajority of committee members initiallyendorsed a strong recommendation forextended genetic panel testing, based on itsdiagnostic accuracy, the benefit of geneticfamily planning, and the potential toidentify more rapid pulmonary functiondecline and poorer clinical outcomes incertain genotypes (8). However, withoutrobust, long-term, patient-importantoutcome data, the committee felt compelledto limit this recommendation to a
conditional recommendation to adhere tothe GRADE approach.
Justification and implementationconsiderations. This recommendationencourages the use of extended geneticpanel testing for diagnosis of PCD (TableE1.2 [evidence-to-decision table]) as areplacement for standard genetic panels (<12genes) and/or TEM ciliary testing. With thisrecommendation, it is noteworthy that TEManalyses in the cohort-type study wereprocessed by one expert technician andreviewed by blinded investigators at aspecialized PCD research center, where TEMspecimens were suitable for interpretation in88% of cases (27). Conversely, one tertiaryacademic care center reported only 63%feasibility in clinical TEM testing for PCD(28), with 37% of clinical cases failing tohave biopsy specimens adequate for TEManalysis. This report is congruent with otherpublications showing poor feasibility forciliary TEM testing (ranges of 60–80%feasibility) at international PCD centers ofexcellence (5, 29–31). In addition, theseexpert PCD centers require repeat ciliarybiopsies for successful TEM analysis in11–22% of patients, providing additionaltravel and medical costs to tested patients(29, 30, 32). Furthermore, the potentialfor broad variability in the handling,preparation, and interpretation of even thosespecimens that are adequate for TEManalysis raises concerns that many of thepatients with PCD diagnosed by TEMdefects alone in Leigh and colleagues’ study(7) would be missed in other clinical centers.This has been confirmed through TEMtesting in the same multicenter consortiumas Leigh and colleagues, whereapproximately 20% of patients diagnosedby TEM defects at their local clinicalcenters lacked the same diagnostic findingupon repeat TEM testing in the expertconsortium (33). Thus, the actual sensitivityof extended panel genetic testing is likelyhigher than 80% in clinical centers, whereTEM testing for PCD is often fraughtwith false-positive, false-negative, andnondiagnostic specimens. In contrast,routine phlebotomy for genetic testing ishighly feasible in all clinical centers, doesnot require patient travel over longdistances, and should not require repeatsample acquisition.
In the past several years, exomesequencing of well-characterized PCDpopulations has revealed many PCD-causing genes (CCNO, MCIDAS, DNAH11,
CCDC65, CCDC164, GAS8, HYDIN, RPGR,and RSPH1) resulting in normal, near-normal, or nondiagnostic TEM studies ofrespiratory cilia (34–41). However, the26-gene panel used by Leigh and colleagues(7) did not include most of these newlydiscovered PCD-causing genes associatedwith normal TEM studies. The inclusion ofthese genes, which are now routinely foundon most commercial PCD genetic panels,would further increase the sensitivity ofPCD genetic testing over that seen by Leighand colleagues. Last, Leigh and colleagues’study did not include deletion/duplicationanalysis of the 26 PCD genes tested.One study of PCD diagnosis bymolecular genetic testing indicates that8% of cases may be diagnosed by reflexdeletion/duplication analysis on a 32-genepanel (26). Thus, the sensitivity of theextended panel used by Leigh andcolleagues should be considerably higherwith deletion/duplication analysis included.Currently, some commercially availableNGS genetic panels for PCD diagnosisinclude deletion/duplication analysis.
This recommendation to use extendedgenetic panel testing rather than TEM ciliarytesting and/or standard (<12 genes) geneticpanel testing was voted by consensus, basedon a very low certainty in the overallevidence for improved long-term, patient-important outcomes. The committeeconsidered the aforementioned variables,resulting in higher test sensitivity in actualclinical practice (increasing sensitivity withnewer panels and overestimation of TEMperformance in research), as criticallyimportant for this recommendation. Inaddition, PCD stakeholders believed thatthis recommendation for extended geneticpanel testing will directly benefit patientsthrough improved diagnostic success. PCDstakeholders also appreciated the benefitsthat early and accurate genetic PCDdiagnosis may have for long-term clinicaland psychosocial outcomes.
Extended genetic panel testing doeshave clinical limitations. First, a negativepanel does not rule out PCD, because someadditional PCD genes are likely yet to bediscovered. Next, only biallelic mutations inthe same PCD gene are disease causing, andparental gene carrier testingmay be requiredto verify that mutations arise in trans.Variants of unknown significance canprovide nondiagnostic results, andincorrect interpretation of genetic variantsmay result in false-positive or false-negative
AMERICAN THORACIC SOCIETY DOCUMENTS
e30 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

diagnoses. Some regions of PCD-causinggenes are not screened by standard genetictesting and may result in false-negativeresults. Thus, consultation with localgenetic specialists may be required forinterpretation of extended genetic paneltesting. Last, North American, European,and international health plans will need toadopt payment policies for PCD genetictesting in their populations.
Future research opportunities. Furtherinvestigation of possible/probable PCDcases through genetic sequencing is essentialto finding new PCD-causing genes andnew pathogenic variants in known genes(including possible intronic or regulatoryregion mutations). With the increasingnumber of PCD-causing genes includedin commercially available genetic testingpanels, the sensitivity of the accessiblegenetic testing will continue to improve.However, genetic panels must be routinelyand frequently updated to include all newlydiscovered PCD-causative genes. Last,databases listing and explaining thepresenting phenotypes associated withvariants of unknown significance in PCDgenes will be necessary to further elucidategenotype–phenotype relationships inpeople with PCD.
Question 2: Should a Low nNO Level(Detected with ChemiluminescenceTechnology), after Excluding CF, BeUsed as a Diagnostic Test for PCD inAdult and Pediatric Patients 5 Yearsof Age or Older with a High Probability(At Least Two of Four Key ClinicalFeatures) of Having PCD (asReplacement of Reference Standardsof Classic TEM Structural CiliaryDefect and/or Biallelic CausativeMutations in PCD Genes)?
Background. nNO levels are reproduciblyreduced (,77 nl/min) in PCD (42), andgiven that nNO results are immediatelyavailable at certain centers, thesemeasurements are often used as a screeningtool for PCD before proceeding to TEMand/or genetic analysis for confirmatorydiagnostic testing. These latter tests areexpensive, can take weeks to monthsto complete, and frequently yieldnondiagnostic results (22, 28). Inexperiencein obtaining biopsy samples can lead toinsufficient cilia for TEM analysis, andinexperience in processing andinterpretation can lead to false-positive or
false-negative TEM results (28, 43). Finally,current genetic testing cannot detectbiallelic mutations in all cases of PCD (22).
Specific methodology. Studies wereincluded if they evaluated, in cooperativepatients (generally >5 yr old) who weredeemed to have a high probability of havingPCD (based on a compatible clinicalphenotype), the accuracy of nNO testing(index test) compared with the referencestandards of classic TEM ultrastructuralciliary defect (outer dynein arm defect,outer dynein arm plus IDA defect, IDAdefect with microtubule disorganization,radial spoke or central apparatus defect)and/or biallelic mutations in known PCDgenes. Studies were excluded if any of thefollowing were present:
1. Fewer than 10 patients with PCD wereincluded in the recruited population.
2. The index test was inadequate: nNOmeasurement used electrochemicaltechnology (NIOX MINO; CircassiaPharmaceuticals), only nonvelumclosure techniques were used (tidalbreathing), and/or nasal sampling flowrates outside the ATS/EuropeanRespiratory Society recommended rangewere used (44).
3. The reference standard relied on only asingle HSVM for PCD confirmation(without a second positive PCD diagnostictest result or without HSVM after cellularregrowth in culture) or greater than orequal to 30% of subjects had nonstandardTEM defects (unrepeated, isolated IDAdefects without MTD) (43).
4. Diagnostic testing accuracy was either notprovided, not accurate, or not calculable.
5. Index testing was incorporated into thereference standard.
nNO data from patients with CF wereexcluded from the analysis because nearlyone-third of patients with CF can have nNOlevels below the PCD diagnostic cutoff of77 nl/min (45).
After initial review of 6,204 referencesby title and abstract, 76 full-text articleswere assessed for eligibility, of which 65were excluded (Figure E2.1). Twelve studypopulations derived from 11 articles wereincluded in the quantitative synthesis (4,42, 46–54) and underwent full-text reviewby the subcommittee (M.J., M.R., O.Y.,A.J.S., and V.L.) (Tables E2.1 and E2.2).A meta-analysis provided a summaryestimate for sensitivity and specificity anda hierarchical summary receiver operating
characteristic curve. The QUADAS-2tool was used to assess study quality,and the GRADE approach was used toassess the diagnostic test accuracy ofstudies to evaluate the certainty ofevidence (Figures E2.2 and E2.5). Furtherdetails on methodology can be foundelsewhere (16).
Summary of evidence. In 12 studypopulations (1,432 patients comprising 524PCD, 908 non-PCD), with use of a referencestandard of TEM alone or TEM and/orgenetic testing, summary sensitivity was97.5% (95% confidence interval [CI],92.8–99.2%), and specificity was 96.4%(95% CI, 88.6–98.9%) (Figures E2.3 andE2.4). Excluding studies using TEM aloneas the reference standard, the seven studiesusing an extended reference standard ofTEM and/or genetic testing showed asummary sensitivity of 96.4% (95% CI,89.4–98.8%) and specificity of 96.2% (95%CI, 84.2–99.2%) (Figure E2.6 and TableE2.3). Successful measurements wereobtained in more than 90% of subjects inthis meta-analysis, making this test highlyfeasible.
Recommendation. In cooperativepatients 5 years of age or older with aclinical phenotype consistent with PCDand with CF excluded, we suggest usingnNO testing for the diagnosis of PCD overTEM and/or genetic testing (conditionalrecommendation, moderate certainty intest accuracy but very low certainty in theoverall evidence). A majority of committeemembers initially endorsed a strongrecommendation for nNO testing, based onits excellent diagnostic accuracy. However,without long-term, patient-importantoutcome data, the committee revisedthis recommendation to a conditionalrecommendation.
Comment. Because nNO values maybe transiently decreased with acute viralrespiratory infections or sinusitis, establishinga low nNO on two separate occasions isindicated. In patients with a compatibleclinical phenotype and low nNO on twooccasions, a presumptive diagnosis of PCDmay be established; TEM and/or genetictesting are indicated for clinical prognosisand to enhance understanding of PCD.
Justification and implementationconsiderations. Our recently publishedmeta-analysis of 12 study populations showsexcellent diagnostic accuracy for nNO as aPCD diagnostic test, in comparison with theextended reference standard of TEM and/or
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e31

genetic testing (16). Two prior meta-analyses have come to similar conclusions(55, 56). Both TEM and genetic analysis areimperfect reference standard PCD tests,with currently estimated sensitivities at 70%(5, 22, 57); each of these tests detects PCDcases that can be missed by the other test.In addition, these reference standard testscan frequently provide nondiagnosticresults, with up to 40% of clinical biopsiesshowing inadequate cilia for TEM analysis(28–30) and up to 43% of genetic testingdetecting no mutations, monoallelicmutations, or variants of unknownsignificance (24). Conversely, nNOmeasurement is a highly feasible testin cooperative patients (generally >5 yrold), with successful measurementsaccomplished in more than 90% of patientsin this meta-analysis. Failure to obtainreliable nNO values were secondary tonasal obstruction, equipment malfunction,high ambient nitric oxide values, or lack ofpatient cooperation. A recent multicentercohort study of PCD diagnostic referralsfurther suggested that nNO testing is moreaccurate than both TEM and/or genetictesting for a PCD diagnosis because nearlyone-fourth of the referred populationhad compatible PCD clinical phenotypesand low nNO values (after ruling outCF) but negative extended genetic paneltesting and normal or nondiagnostic TEMstudies (7).
Although nNO testing has been largelyconsidered a PCD screening test, theseanalyses show that nNO has diagnosticaccuracy similar to (and possibly betterthan) that of the accepted confirmatoryPCD tests of TEM and/or genetic analysis(Table E2.4 [evidence-to-decision table])when used in a population with a highprobability of having PCD (at least two keyclinical PCD features). The use of nNO as aPCD screening test in general populationswithout key clinical PCD features will resultin reduced positive predictive value and isstrongly discouraged. The direct desirableconsequences of using nNO testing insteadof TEM and/or genetic testing outweigh theundesirable consequences, and the overallimpact of avoiding direct costs andcomplications justifies using nNO testing asa replacement for the reference standards.The overall rates of false-negative results(which were considered critical) and falsepositive results were small (when usingestablished, standardized protocols withchemiluminescence devices), and thus the
downstream consequences were consideredsimilar between nNO, TEM, and genetictesting. Nevertheless, despite the reportedhigh accuracy of nNO in comparison withthe reference standards, nNO might be evenmore sensitive than TEM and/or currentgenetic testing, thus potentially reducingfalse-negative results and their downstreamconsequences. Because nNO values may bedecreased with acute viral respiratoryinfections or sinusitis, verification of lownNO values on at least two separateoccasions seems prudent when using thisas a PCD diagnostic test. In cases ofstrongly suspected PCD with normalTEM studies and negative genetic testing,repeatedly low nNO values may be theonly positive PCD diagnostic test resultand should be verified on at least twooccasions.
Therefore, in individuals 5 years ofage or older, with an appropriate clinicalphenotype for PCD, and when CF isexcluded, the diagnostic accuracy ofnNO measurement (performed withchemiluminescence devices usingestablished, standardized protocols) iscomparable to that of TEM and/or genetictesting. nNO testing is noninvasive,relatively inexpensive for patients(after institutions purchase a costlychemiluminescence analyzer), and providesimmediate results. However, there arelimitations, including the need to travel tospecialized centers that perform the testing,training of device operators, lack of U.S.Food and Drug Administration approvalfor devices in the United States (andthus the inability of institutions to gainreimbursement for clinical testing), and thelack of test standards for children under5 years old.
Even with low nNO measures, patientsshould still progress to further corroborativePCD diagnostic studies, including geneticand/or TEM testing, which may providelong-term prognostic information (8, 41);improve the general understanding of PCD;and account for other respiratory tractillnesses, including acute sinusitis or viralinfection, which may lead to reduced nNOvalues (58–60). PCD stakeholders agreedon the critical importance of confirminggenetic and/or TEM defects after adiagnosis is made with nNO measurements.Patients with biallelic disease-causingmutations in some genes (e.g., RSPH1) canhave nondiagnostic nNO results. Genetictesting may also inform family planning.
Finally, defining the PCD genotype mayallow development future mutation-specifictherapies, as occurred in CF (61).
Future research opportunities. Furtherresearch is needed on nNO measurements inchildren younger than 5 years of age, whocannot cooperate with velum closuremaneuvers and therefore perform thistechnique through tidal breathing. Additionalresearch needs include determination of age-specific distributions of nNO levels in diseasecontrol populations and determination ofappropriate diagnostic cutoffs for tidalbreathing nNO measurements. A majorlimitation of nNO measurement is the highcost of chemiluminescence devices, becausethis is the only technology currentlyrecommended for nNO measurement inPCD diagnosis (44). Further researchexamining the diagnostic accuracy ofportable electrochemical nNO devicescould potentially validate less expensivealternatives for PCD diagnosis. Last,further standardization of nNO devicemeasurement software is required, becausesignificant differences can occur withautomated online measurement programscompared with offline operator-drivenprotocols (62).
Question 3: Should HSVM Alone BeUsed as a PCD Diagnostic Test inAdult and Pediatric Patients with aHigh Probability (At Least Two of FourKey Clinical Features) of Having PCD(as a Replacement of ReferenceStandards of Classic TEM StructuralCiliary Defect and/or Biallelic CausativeMutations in PCD Genes)?
Background. HSVM is used in a numberof specialized laboratories to diagnosePCD (50, 63–65). With use of a digitalhigh-speed video camera attached to amicroscope, beating ciliated epithelial edgesare recorded at frame rates of between 120and 500 frames per second and are thenreplayed at slower rates to view ciliarymotion. Samples can then be evaluated toassess ciliary function by measuring CBFand/or ciliary beat pattern (CBP). Recentexpert consensus recommended HSVMciliary functional assessment of both CBFand CBP coupled with TEM as a means ofdiagnosing PCD (66). However, conductingHSVM proves challenging, requiringsignificant expertise and training.Furthermore, this expertise is limitedto a few laboratories in Europe and
AMERICAN THORACIC SOCIETY DOCUMENTS
e32 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

Canada; therefore, clinical applicability isrestricted.
Specific methodology. For this analysis,studies using HSVM (>120 frames persecond recording) were reviewed. After theinitial appraisal of titles and abstracts,35 articles were identified for full-text reviewby the subcommittee (S. D. Davis, C.M.,and M.A.C.) (Section 3 of the onlinesupplement). Agreed-upon exclusion criteriaused for full-text review were 1) fewerthan 10 patients with PCD in the studiedpopulation, 2) index test of HSVM includedin the reference diagnostic standard,3) HSVM with CBP analysis technique notused, and 4) unable to calculate sensitivityor specificity (Figure E3.1). Authors werecontacted via e-mail if exclusion criteriawere unclear. Upon further review by thecommittee cochairs (A.J.S. and V.L.), fourarticles are included in the quantitativemeta-analysis (50, 63–65).
Summary of evidence. Four cross-sectional, cohort-type studies consecutivelyrecruited participants and evaluated theability of HSVM to diagnose PCD by CBPanalysis. Two studies were prospective, withsample sizes of 371 (63) and 34 (50)participants with suspected PCD. Two wereretrospective, with sample sizes of 231 (65)and 158 (64) participants. None of theincluded studies examined PCD diagnosisby genetic testing in the reference standard.
Stannard and colleagues (63) evaluatedCBP using nasal ciliated epithelial samplesin 371 participants, with TEM as thereference standard for PCD diagnosis. Ofthe 371 participants, 70 were diagnosedwith PCD on the basis of electronmicroscopy. The Stannard group evaluatedCBF, ciliary dyskinesia score, percentageof dyskinetic edges, and immotility indexto determine abnormal CBP. A ciliarydyskinesia score greater than 2 was themost accurate of these HSVM measures,resulting in sensitivity of 92.5%, specificityof 97.6%, positive predictive value of 91.2%,and negative predictive value of 98%.
Papon and colleagues (50) evaluatedHSVM in 34 participants with suspectedPCD, using a reference diagnostic standardof nNO measurement coupled with TEMfor PCD diagnosis. This group conductedboth qualitative and quantitative analysisusing 12 different HSVM measures. Of the34 participants, 15 were deemed non-PCD,10 were diagnosed with definite PCD byreference standard, and 9 received aninconclusive diagnosis. On the basis of this
small sample size, the investigators reportedthat the use of quantitative HSVM CBPanalysis diagnosed 9 of the 10 patients withPCD and improved diagnostic accuracy,whereas qualitative measurementsidentified only 7 patients with PCD. Inthe inconclusive group of nine patients,quantitative ciliary analysis identified afurther four and qualitative analysis afurther two with abnormal HSVM who hadlow nNO levels. However, on reviewing thediscordant nNO and TEM findings withinindividual subjects in this group, genetictesting would be required to accuratelyidentify PCD in this group of patients. Ofnote, the methodology required to performthis quantitative analysis is complex andmay not be feasible in a clinical setting.
Using a retrospective cohort of 231patients referred for PCD in Leicester,England, Hirst and colleagues (65)evaluated the utility of HSVM in improvingthe diagnosis of PCD after epithelial biopsysamples were grown under air–liquidinterface tissue culture conditions. Thisgroup used TEM as the diagnostic referencestandard with qualitative HSVM analysis asthe index test. HSVM was performed inboth fresh ciliated samples and later aftercellular regrowth to allow for assessment ofany ciliary functional gain after cell culture.The results revealed that 28 participantshad definite PCD with diagnostic TEMdefects, and all showed 100% dyskinesiawithin biopsy samples on HSVM in thefresh specimens. However, only 12 of 28(43%) PCD biopsy samples successfullyregrew in culture, but postculture HSVMand TEM studies were consistent with thepreculture results. In a separate study, Hirstand colleagues (64) retrospectively analyzedHSVM after culture regrowth in 158participants referred for PCD diagnosis,using a reference diagnostic standard ofTEM defects, clinical history, or abnormalciliary function. However, 73 participantsfrom one site were excluded from ouranalysis because the index test of HSVMwas also incorporated into the referencediagnostic standard. The investigatorsreported that the CBP analyses postcultureconfirmed the ciliary phenotype in 100% ofPCD cases, and in some cases, they werebetter at identifying abnormal CBP versuspreculture fresh analyses.
The selected studies reported data(Figure E3.3) for two qualitative parameters ofCBP analysis: either by describing thepercentage of dyskinetic beating cilia on the
epithelial edge (64, 65) or by reporting aciliary dyskinesia score for the edge (50, 63).Overall, the pooled sensitivity and specificityfor all four studies were 97.3% (95% CI,59.8–99.9%) and 96.5% (95% CI,63.7–99.8%), respectively. However, the 95%CI of these diagnostic accuracy results wasextremely large, signifying great variationin the certainty of these results. This isillustrated by the summary receiver operatingcharacteristic curve and 95% CIs (FigureE3.4)
Because genetic PCD testing was notperformed in any of the studies, it is possiblethat the reported accuracy may beoverestimated (Figures E3.2–E3.4 and TableE3.1). Three of the four studies wereconducted by the same research group inthe United Kingdom; these investigatorsare expert at using HSVM as well as theair–liquid interface tissue culture technique.The single analyzed study done outside ofthe United Kingdom was conducted in asmall sample of patients and demonstratedmuch worse diagnostic accuracy. Ofnote in this study, the accuracy of thereference standard used for diagnosisappeared to vary in PCD and inconclusivecases.
Recommendation. We suggest notusing CBP analysis by HSVM as areplacement diagnostic test in patientswith a high probability of having PCD(conditional recommendation, lowcertainty in the diagnostic accuracy of thetest but very low certainty in the overallevidence).
Justification and implementationconsiderations. Ciliary functionalassessment (CBF and CBP) by HSVM isoften used as a primary PCD diagnostic toolin some countries. Experts now recommendHSVM analysis after cellular regrowth oftissue samples, but CBP may still be affectedby the manipulation of fresh tissue, leadingto a different functional phenotype afterculture (66–68). Significant technicalexpertise and equipment are required tosuccessfully grow ciliated epithelialcultures, which often fail to regrow, even atexpert centers (65). If cellular regrowthcannot be achieved, families must travelrepeatedly to centers of expertise formultiple biopsies and repeat HSVManalyses.
There is also a lack of standardizationin HSVM interpretation techniques, withsome centers using various quantitativefunctional measures based on qualitative
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e33

assessments, such as immotility index,percentage of dyskinetic edges, and distanceof ciliary tip traveled, whereas other centersuse mainly qualitative descriptions of beatpattern, including “stiffness” of cilia and“failure of bending” along the entireaxoneme. With this lack of standardizationin both sample preparation and CBPinterpretation, the HSVM technique itself isnot easily transferred to other centers (poorfeasibility), and the applicability of thetechnique across centers remains poor(Table E3.2 [evidence-to-decision table]).Only a few international centers have thenecessary expertise to conduct ciliaryfunctional analysis with HSVM. Last,interrater agreement of HSVM beat patternanalysis is quite poor, even in samplesfrom healthy control subjects (69). Giventhese limitations and the potential forfalse-positive and false-negative resultsfor PCD diagnosis, we suggest notusing CBP assessment with HSVM as aroutine diagnostic tool (Table E3.2).Despite this, CBP analysis may still havea role in the assessment of patients withPCD, because currently there is no“gold standard” PCD test, and both TEMand genetic testing have significantdiagnostic limitations. Currently,HSVM is more appropriate for PCDdiagnosis in expert research settingsuntil investigators offer significantclinical advancements in HSVMfeasibility and test standardization.PCD stakeholders strongly support thisrecommendation until such standardizationis achieved.
Future research opportunities.Conducting genotype–phenotyperelationships using HSVM may helpinvestigators elucidate the underlyingmechanisms leading to progressive lungdisease in PCD. However, this will requirestandardization of protocols (includingtissue culture conditions) and developmentof robust, validated CBP measurements.Studies comparing HSVM analysis withTEM defects and PCD-causing genemutations may delineate diseasemechanisms and aid PCD diagnosis;however, this would require participationby multiple centers to achieve adequatesample size. To improve generalapplicability of HSVM, further research isindicated which demonstrates that multiplecenters can successfully use this tool whenfollowing validated standard operatingprotocols.
Question 4: Should CBF or CiliaryWaveform Analysis Using LightMicroscopy without High-SpeedRecording Be Used as a PCDDiagnostic Test in Adult and PediatricPatients with a High Probability (AtLeast Two of Four Key ClinicalFeatures) of Having PCD (asReplacement of Reference Standardsof Classic TEM Structural CiliaryDefect and/or Biallelic CausativeMutations in PCD Genes)?
Background. Calculation of CBF hashistorically been suggested as a PCDdiagnostic method that can be used withinexpensive bright-field microscopy andstraightforward recording technology (70, 71).In addition, some clinicians employ ciliarywaveform analysis without high-speedrecording to diagnose PCD (72–74). Someacademic centers even suggest these tests asfirst-line screening, and if results are normal,further PCD diagnostic testing (such as TEMor genetic testing) may not be necessary(75, 76). However, most expert NorthAmerican PCD centers avoid CBFmeasurement or waveform analysis withouthigh-speed video recording in PCD, becauseseveral recently discovered genetic forms ofPCD result in normal CBF with only subtlechanges in CBP (77). In addition, most PCDresearchers have migrated from standard-speed video recording to HSVM because thismethod provides more detailed ciliarywaveform information for analysis (seeQUESTION 3 above).
Specific methodology. Studies usingstandard-speed video microscopy andHSVM were evaluated in this analysis, butwhen HSVM was used, the analyzed datawere limited to only CBF values, and ciliarywaveform analysis was excluded altogetherif HSVM was used. After the initial reviewof titles and abstracts, 51 articles wereidentified for full-text review by the questionsubcommittee (A.J.S., M.W.L., L.M.). Afteragreeing on specific inclusion and exclusioncriteria for the full-text review, thesubcommittee completed a full-text reviewof all 51 articles (Figure E4.1). Upon furtherreview by the committee cochairs (A.J.S.,V.L.), three articles examining CBF forPCD diagnosis were included for furtheranalysis (63, 64, 78). One article addressingciliary waveform analysis with standard-speed video recording was considered forfurther examination; yet, this additionalarticle did not employ currently recognized
PCD reference diagnostic standards anddid not use the reliable methods toperform ciliary waveform analysis (73).Thus, no articles addressing ciliarywaveform analysis with standard-speedvideo recording were included in the finalanalysis.
Summary of evidence. Three cross-sectional studies addressed this question. Allthree used TEM defects as the referencestandard, and none examined patients withPCD diagnosed by genetics. Two of thesewere cohort-type studies, but the onlyprospective cohort study, by Stannard andcolleagues, was a single-center study thatexamined diagnostic testing accuracy ofCBF in 371 consecutively referred patientswith symptoms of PCD (63). With use ofCBF alone, with a prespecified cutoff valueof 11 Hz to diagnose PCD, approximately13% of PCD cases were missed on the basisof TEM studies confirming the diagnosis,with sensitivity and specificity of 87% and77%, respectively. The authors offered otherwaveform analysis techniques and scoringsystems that perform superior to CBFmeasurement alone, but these are allperformed with HSVM and thus were notconsidered to answer this specific questionon standard-speed video recording. Theother cohort study, by Hirst and colleagues,was a retrospective, multicenter analysisof 73 patients referred for suspicion ofPCD (64). Only patients recruited at theLeicester site were included in our dataanalysis, because the other recruitingcenter commonly incorporated the indextest (CBF and ciliary motility assessment)within the reference standard andpossibly did not perform TEM testing ifciliary motility was normal. Analysis ofthe Leicester patients revealed that CBFvalues, at a prespecified cutoff of 10 Hz,provided 68% and 78% sensitivity andspecificity, respectively, compared withTEM studies. The third study included asmaller population and was conductedretrospectively (78). This showed a lowspecificity of CBF compared with TEMdiagnosis of PCD. Because genetic PCDtesting was not performed in any of theprevious studies, it is possible (if notlikely) that reported accuracy wasoverestimated (Figures E4.2 and E4.3 andTable E4.1).
Recommendation. We suggest notusing CBF measurement as a diagnostic testin patients with a high probability of havingPCD (conditional/weak recommendation,
AMERICAN THORACIC SOCIETY DOCUMENTS
e34 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

At least 2 of the 4 key clinical features for PCD: Unexplained neonatal respiratory distress in term infant Year-round daily cough beginning before 6 months of age Year-round daily nasal congestion beginning before 6 months of age Organ laterality defect
Access to nNO testing (with chemiluminescence device and standardized protocol) at specialty centerAND Cooperative patient 5 years old, capable of performing nNO testing maneuver
Nasal nitric oxide measurement* Extended genetic testing panel†
No to eitherYes to both
(preferred pathway)
Yes
No PCD Unlikely
Pursue additional corroborativePCD testing:¶
- Extended genetic panel testing (first line)-TEM of ciliary ultrastructure
Diagnosis of PCD,if CF is excluded.
- Advise repeat nNO toverify low value‡
Unlikely PCD diagnosisPursue genetic testing
if strong clinical features§
Biallellic pathogenicvariants in PCD-associated gene
Single pathogenicvariant in PCD-
associated gene#
No pathogenicvariants in PCD-
associated genes#
Low nNO level Normal nNO level
Diagnosis of PCD
Electron microscopy of ciliary ultrastructure
Inadequate sample orindeterminate
analysis
Normal ciliaryultrastructure
Recognized ciliaryultrastructural
defect||
UnknownConsider repeat TEM
or referral to PCDspecialty center
Diagnosis of PCD PCD Still Possible
Figure 1. Suggested diagnostic algorithm for evaluating the patient with suspected primary ciliary dyskinesia. *Cystic fibrosis should be ruled out beforeperforming nNO measurement, as roughly one-third of CF patients can have nNO values below PCD diagnostic cutoffs. nNO measurements should onlybe performed with chemiluminescence analyzers using standardized protocols at centers with specific expertise in nNO measurements. Some nNOanalyzers have not received approval from federal agencies worldwide (U.S. Food and Drug Administration and Health Canada have not approved allchemiluminescence devices for clinical use), which may have implications for clinical implementation. †Genetic panels testing for mutations in more than12 disease-associated PCD genes, including deletion/duplication analysis. ‡As nNO levels can be significantly decreased by viral respiratory tractinfections, a repeat nNO measurement, at least 2 weeks after the initial low value (expert opinion), is recommended to ensure that the initial low value is notsecondary to a viral process. A normal nNO value upon repeat testing suggests that the patient does not have PCD, as nNO values remain consistentlylow in PCD. xMost forms of PCD resulting in normal nNO levels have normal or nondiagnostic electron microscopy studies. Thus, genetic testing isrecommended in these cases. #Or presence of variants of unknown significance. For the purposes of this algorithm, “likely pathogenic” variants and“pathogenic” variants are grouped together as pathogenic. ¶Additional corroborative testing may provide information on clinical prognosis, furtherunderstanding of the disease, and suggest potential future therapeutic considerations. jjKnown disease-associated TEM ultrastructural defects includeouter dynein arm defects, outer dynein arm plus inner dynein arm (IDA) defects, IDA defects with microtubular disorganization, and absent central pair,identified using established criteria (1, 6, 13). Of note, the presence of IDA defects alone is rarely diagnostic for PCD. DUp to 30% of PCD cases can havenormal ciliary ultrastructure of electron microscopy (EM). Consider referral to PCD specialty center if there is a strong clinical phenotype but all EM andgenetic testing are negative. CF = cystic fibrosis; nNO = nasal nitric oxide; PCD = primary ciliary dyskinesia; TEM = transmission electron microscopy.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e35

low certainty in the diagnostic accuracy ofthe test but very low certainty in the overallevidence). No recommendation could bemade regarding the use of ciliarywaveform analysis without HSVM as adiagnostic test for PCD, because no studiesusing currently recognized referencestandards were identified by our systematicreview.
Justification and implementationconsiderations. This analysis shows that thediagnostic accuracy of CBF calculation ispoor in comparison with the referencestandard of TEM testing. Although notmeeting inclusion criteria for this analysis,another study of PCD cases using genetictesting as the diagnostic reference standarddemonstrated overlapping CBF valuesbetween patients with PCD, healthy controlsubjects, and disease control subjects (77).Furthermore, there are no significantdifferences in cost (compared with thereference standard, when CBF is performedas part of a larger ciliary motilityassessment with HSVM), direct benefits,or indirect benefits when using CBF as adiagnostic test (Table E4.2 [evidence-to-decision table]). The majority of studiesand recommendations supporting ciliarymotion analysis via CBF or standard-speedvideo microscopy were published over15 years ago (70–73, 79), and sincethen, no prospective validation studieshave proven this technique as diagnosticof PCD.
PCD stakeholders expressed verystrong agreement with this
recommendation because they appreciatethe benefits of early and accurate PCDdiagnosis may have for long-term clinicaland psychosocial outcomes. Stakeholdersalso believe it is critically important toproperly diagnose patients with PCD on thebasis of genetics and/or TEM defects inorder to identify criteria causing a continueddecline in this subgroup of patients withPCD, which may lead to targeted, noveltherapies for this subgroup.
The committee realizes that bright-fieldmicroscopy with CBF measurement is afeasible and inexpensive test that is sometimesused in centers lacking experience in PCD.The committee also realizes that prohibitingthis testing will require referral of potentialpatients with PCD to more specialized PCDcenters for definitive diagnosis using moreexpensive investigations, such as TEM andgenetic testing. However, with the high rateof false-negative results of CBF and lightmicroscopy without HSVM, potential patientswith PCD will continue to receive incorrectdiagnoses if these practices continue. Thus,centers relying on CBF measurement as theirsole PCD diagnostic tool should refer allpotential patients with PCD to specializedPCD centers for more reliable diagnostictesting (Table 4.2).
Future research opportunities. Furtherinvestigation of real-time ciliary waveformanalysis without HSVM, accompaniedby automated waveform and CBFinterpretation software, may provide a rolefor real-time light microscopy in the future.However, with the increasing use of HSVM
recording for ciliary waveform analysis, itseems doubtful that further research intonon-HSVM waveform analysis will occur.
Conclusions: ProposedDiagnostic Algorithm
On the basis of our review of availableevidence, we propose a diagnosticalgorithm for patients who have a clinicalphenotype consistent with PCD (Figure 1).The committee was unable to stronglyrecommend a single PCD diagnostic testand recommends that a panel of diagnostictests be applied to diagnose PCD, whichmay require referral to a PCD specialtycenter to provide comprehensiveevaluation and testing. In addition,whereas nNO measurements (whenmeasured correctly) may have diagnosticaccuracy equivalent to that of TEM andgenetic testing, it should not completelyreplace these tests in all cases. Rather,clinicians should appreciate the addeddiagnostic value of multiple positive tests,specifically nNO measurement withgenetics or TEM.
The proposed algorithm represents anidealized setting in which all diagnostic testsare accessible to a provider. The authorsrecognize, however, that there may beinternational differences, and providersmust consider diagnostic options based onavailability. Obviously, the algorithm willneed to be modified with the emergence ofnewer tests. n
This official clinical practice guideline was prepared by an ad hoc primary ciliary dyskinesia subcommittee of the ATS Assembly onPediatrics.
Members of the subcommittee are asfollows:
ADAM J. SHAPIRO, M.D. (Co-Chair)VALERY LAVERGNE, M.D. (Co-Chair,
Methodologist)STEPHANIE D. DAVIS, M.D. (Co–Vice Chair)MICHELE MANION (Co–Vice Chair)BILLY ANTON
MARK A. CHILVERS, M.D.MATTHEW L. COOPER, M.D.SAM J. DANIEL, M.D.M. LEIGH ANNE DANIELS, M.D.SHARON D. DELL, M.D.TORI EASTVOLD
LYNN EHRNE
THOMAS W. FERKOL, M.D.
ELENA GUADAGNO, M.L.I.S.IBRAHIM A. JANAHI, M.D.MARCUS HERBERT JONES, M.D.MAUREEN JOSEPHSON, M.D.MICHAEL R. KNOWLES, M.D.MARGARET W. LEIGH, M.D.CARLOS MILLA, M.D.LUCY MORGAN, M.D.LAWRENCE M. NOGEE, M.D.KENNETH N. OLIVIER, M.D.JESSICA E. PITTMAN, M.D.DEEPIKA POLINENI, M.D.MARGARET ROSENFELD, M.D.SCOTT D. SAGEL, M.D.STEPHANIE M. WARE, M.D., PH.D.
OZGE YILMAZ, M.D.MAIMOONA A. ZARIWALA, PH.D.
Author Disclosures: A.J.S. served as siteprincipal investigator for a Parion/Vertexclinical trial for VX-371: Clearing Lungswith ENaC Inhibition in Primary CiliaryDyskinesia (CLEAN-PCD), registrationnumber NCT02871778. S. D. Davis servedas a consultant for Eli Lilly and Vertex;received research support from Circassia(formerly Aerocrine), Parion/Vertex, andthe Cystic Fibrosis Foundation; servedas a speaker for ABcomm Inc. andParion/Vertex; received support from aneducational grant from Gilead; and servedon an advisory committee for Parion/Vertex.
AMERICAN THORACIC SOCIETY DOCUMENTS
e36 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018
S. D. Dell served as site principalinvestigator for a Parion/Vertex clinicaltrial for VX-371 (see above); served on anadvisory committee and as a consultant forVertex; and served as a consultant forNovartis. T.W.F. served as site principalinvestigator for a Parion/Vertex clinical trialfor VX-371 (see above); served as siteprincipal investigator for a device trial forCircassia (formerly Aerocrine); holds fiveUnited States and international patents; andreceived research support from the Children’sDiscovery Institute and the Cystic FibrosisFoundation. M.R.K. served on an advisorycommittee for Corus Pharma and ProteostasisTherapeutics; and served as a consultant for
Gilead and Vertex. M.W.L. served as siteprincipal investigator for the Parion/Vertexclinical trial for VX-371 (see above); served assite principal investigator for a device trial forCircassia (formerly Aerocrine); and served onan advisory committee for Vertex. C.M. servedas a consultant for AbbVie, Gilead,Proteostasis, and Vertex; served as a siteprincipal investigator for a Proteostasis clinicaltrial for PTI-428 (an investigational oraltreatment for cystic fibrosis); and served as siteprincipal investigator for a Parion/Vertex clinicaltrial for VX-371 (see above). L.M.N. receivedroyalties from UpToDate for coauthoring achapter on genetic surfactant dysfunctiondisorders. K.N.O. received research
support from Insmed and MatinasBioPharma; and served as a speaker forBayer HealthCare. D.P. served asconsultant for Vertex. S.D.S. receivedresearch support from the Cystic FibrosisFoundation. O.Y. received travel supportfor conferences from Abdi Ibrahim,Allergopharma–Merck Turkey, Bilim, andGlaxoSmithKline. M.A.Z. served as aconsultant for a Parion/Vertex clinical trialfor VX-371 (see above). V.L., M.M., B.A.,M.A.C., M.L.C., S.J.D., M.L.A.D., T.E.,L.E., E.G., I.A.J., M.H.J., M.J., L.M.,J.E.P., M.R., and S.M.W. reported norelationships with relevant commercialinterests.
References
1. Knowles MR, Zariwala M, Leigh M. Primary ciliary dyskinesia. Clin ChestMed 2016;37:449–461.
2. Bush A, Chodhari R, Collins N, Copeland F, Hall P, Harcourt J, et al. Primaryciliary dyskinesia: current state of the art. Arch Dis Child 2007;92:1136–1140.
3. Zariwala MA, Knowles MR, Omran H. Genetic defects in ciliary structureand function. Annu Rev Physiol 2007;69:423–450.
4. Noone PG, Leigh MW, Sannuti A, Minnix SL, Carson JL, Hazucha M,et al. Primary ciliary dyskinesia: diagnostic and phenotypic features.Am J Respir Crit Care Med 2004;169:459–467.
5. Kouis P, Yiallouros PK, Middleton N, Evans JS, Kyriacou K,Papatheodorou SI. Prevalence of primary ciliary dyskinesia inconsecutive referrals of suspect cases and the transmission electronmicroscopy detection rate: a systematic review and meta-analysis.Pediatr Res 2017;81:398–405.
6. Shapiro AJ, Zariwala MA, Ferkol T, Davis SD, Sagel SD, Dell SD, et al.;Genetic Disorders of Mucociliary Clearance Consortium. Diagnosis,monitoring, and treatment of primary ciliary dyskinesia: PCDFoundation consensus recommendations based on state of the artreview. Pediatr Pulmonol 2016;51:115–132.
7. Leigh MW, Ferkol TW, Davis SD, Lee HS, Rosenfeld M, Dell SD, et al.Clinical features and associated likelihood of primary ciliary dyskinesiain children and adolescents. Ann Am Thorac Soc 2016;13:1305–1313.
8. Davis SD, Ferkol TW, Rosenfeld M, Lee HS, Dell SD, Sagel SD, et al.Clinical features of childhood primary ciliary dyskinesia by genotype andultrastructural phenotype. Am J Respir Crit Care Med 2015;191:316–324.
9. Mullowney T, Manson D, Kim R, Stephens D, Shah V, Dell S. Primaryciliary dyskinesia and neonatal respiratory distress. Pediatrics 2014;134:1160–1166.
10. Shapiro AJ, Davis SD, Ferkol T, Dell SD, Rosenfeld M, Olivier KN, et al.;Genetic Disorders of Mucociliary Clearance Consortium. Lateralitydefects other than situs inversus totalis in primary ciliary dyskinesia:insights into situs ambiguus and heterotaxy. Chest 2014;146:1176–1186.
11. Brozek JL, Akl EA, Jaeschke R, Lang DM, Bossuyt P, Glasziou P, et al.;GRADE Working Group. Grading quality of evidence and strength ofrecommendations in clinical practice guidelines: Part 2 of 3. TheGRADE approach to grading quality of evidence about diagnostictests and strategies. Allergy 2009;64:1109–1116.
12. Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, et al.GRADE guidelines: 2. Framing the question and deciding onimportant outcomes. J Clin Epidemiol 2011;64:395–400.
13. Schunemann HJ, Oxman AD, Brozek J, Glasziou P, Bossuyt P, Chang S,et al. GRADE: assessing the quality of evidence for diagnosticrecommendations. Evid Based Med 2008;13:162–163.
14. Schunemann HJ, Jaeschke R, Cook DJ, Bria WF, El-Solh AA, Ernst A,et al.; ATS Documents Development and ImplementationCommittee. An official ATS statement: grading the quality ofevidence and strength of recommendations in ATS guidelines andrecommendations. Am J Respir Crit Care Med 2006;174:605–614.
15. Whiting PF, Rutjes AW,WestwoodME,Mallett S, Deeks JJ, Reitsma JB, et al.;QUADAS-2 Group. QUADAS-2: a revised tool for the quality assessmentof diagnostic accuracy studies. Ann Intern Med 2011;155:529–536.
16. Shapiro AJ, Josephson M, Rosenfeld M, Yilmaz O, Davis SD, Polineni D,et al. Accuracy of nasal nitric oxide measurement as a diagnostic testfor primary ciliary dyskinesia: a systematic review and meta-analysis.Ann Am Thorac Soc 2017;14:1184–1196.
17. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADEguidelines: 1. Introduction—GRADE evidence profiles and summaryof findings tables. J Clin Epidemiol 2011;64:383–394.
18. McMaster University and Evidence Prime Inc. GRADEpro GDT [accessed2017 May 28]. Available from: http://www.guidelinedevelopment.org.
19. Schunemann HJ, Mustafa R, Brozek J, Santesso N, Alonso-Coello P,Guyatt G, et al.; GRADE Working Group. GRADE guidelines: 16.GRADE evidence to decision frameworks for tests in clinical practiceand public health. J Clin Epidemiol 2016;76:89–98.
20. Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y,et al. GRADE guidelines: 14. Going from evidence to recommendations:the significance and presentation of recommendations. J Clin Epidemiol2013;66:719–725.
21. Andrews JC, Schunemann HJ, Oxman AD, Pottie K, Meerpohl JJ,Coello PA, et al. GRADE guidelines: 15. Going from evidence torecommendation-determinants of a recommendation’s direction andstrength. J Clin Epidemiol 2013;66:726–735.
22. Zariwala MA, Knowles MR, Leigh MW. Primary ciliary dyskinesia. In:Adam MP,Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K,et al. GeneReviews®. Seattle, WA: University of Washington, Seattle;2007 Jan 24 [updated 2015 Sep 3].
23. Djakow J, Kramna L, Dušatkova L, Uhlık J, Pursiheimo JP, Svobodova T,et al. An effective combination of Sanger and next generationsequencing in diagnostics of primary ciliary dyskinesia. PediatrPulmonol 2016;51:498–509.
24. Boaretto F, Snijders D, Salvoro C, Spalletta A, Mostacciuolo ML,Collura M, et al. Diagnosis of primary ciliary dyskinesia by a targetednext-generation sequencing panel: molecular and clinical findings inItalian patients. J Mol Diagn 2016;18:912–922.
25. Kim RH, A Hall D, Cutz E, Knowles MR, Nelligan KA, Nykamp K, et al.The role of molecular genetic analysis in the diagnosis of primaryciliary dyskinesia. Ann Am Thorac Soc 2014;11:351–359.
26. Marshall CR, Scherer SW, Zariwala MA, Lau L, Paton TA, Stockley T,et al.; FORGE Canada Consortium. Whole-exome sequencingand targeted copy number analysis in primary ciliary dyskinesia.G3 (Bethesda) 2015;5:1775–1781.
27. Olin JT, Burns K, Carson JL, Metjian H, Atkinson JJ, Davis SD, et al.;Genetic Disorders of Mucociliary Clearance Consortium. Diagnosticyield of nasal scrape biopsies in primary ciliary dyskinesia: amulticenter experience. Pediatr Pulmonol 2011;46:483–488.
28. Simoneau T, Zandieh SO, Rao DR, Vo P, Palm KE, McCown M, et al.Impact of cilia ultrastructural examination on the diagnosis of primaryciliary dyskinesia. Pediatr Dev Pathol 2013;16:321–326.
29. Shoemark A, Dixon M, Corrin B, Dewar A. Twenty-year review ofquantitative transmission electron microscopy for the diagnosis ofprimary ciliary dyskinesia. J Clin Pathol 2012;65:267–271.
30. Papon JF, Coste A, Roudot-Thoraval F, Boucherat M, Roger G, TamaletA, et al. A 20-year experience of electron microscopy in the diagnosisof primary ciliary dyskinesia. Eur Respir J 2010;35:1057–1063.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e37
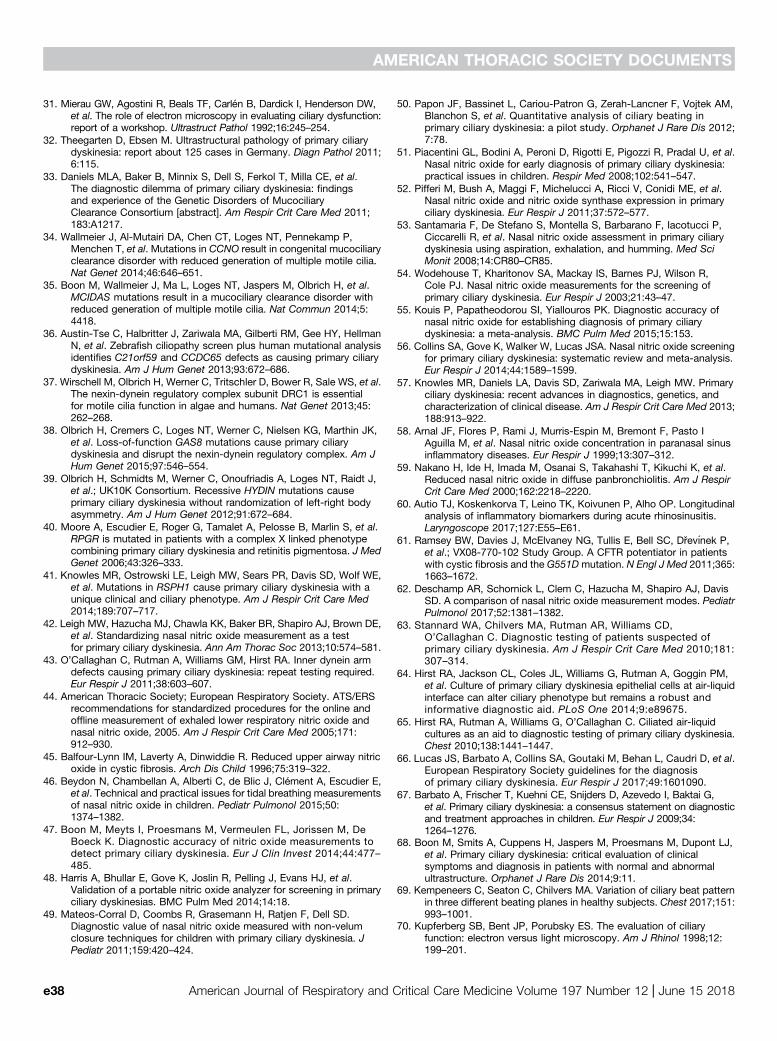
31. Mierau GW, Agostini R, Beals TF, Carlen B, Dardick I, Henderson DW,et al. The role of electron microscopy in evaluating ciliary dysfunction:report of a workshop. Ultrastruct Pathol 1992;16:245–254.
32. Theegarten D, Ebsen M. Ultrastructural pathology of primary ciliarydyskinesia: report about 125 cases in Germany. Diagn Pathol 2011;6:115.
33. Daniels MLA, Baker B, Minnix S, Dell S, Ferkol T, Milla CE, et al.The diagnostic dilemma of primary ciliary dyskinesia: findingsand experience of the Genetic Disorders of MucociliaryClearance Consortium [abstract]. Am Respir Crit Care Med 2011;183:A1217.
34. Wallmeier J, Al-Mutairi DA, Chen CT, Loges NT, Pennekamp P,Menchen T, et al. Mutations in CCNO result in congenital mucociliaryclearance disorder with reduced generation of multiple motile cilia.Nat Genet 2014;46:646–651.
35. Boon M, Wallmeier J, Ma L, Loges NT, Jaspers M, Olbrich H, et al.MCIDAS mutations result in a mucociliary clearance disorder withreduced generation of multiple motile cilia. Nat Commun 2014;5:4418.
36. Austin-Tse C, Halbritter J, Zariwala MA, Gilberti RM, Gee HY, HellmanN, et al. Zebrafish ciliopathy screen plus human mutational analysisidentifies C21orf59 and CCDC65 defects as causing primary ciliarydyskinesia. Am J Hum Genet 2013;93:672–686.
37. Wirschell M, Olbrich H, Werner C, Tritschler D, Bower R, Sale WS, et al.The nexin-dynein regulatory complex subunit DRC1 is essentialfor motile cilia function in algae and humans. Nat Genet 2013;45:262–268.
38. Olbrich H, Cremers C, Loges NT, Werner C, Nielsen KG, Marthin JK,et al. Loss-of-function GAS8 mutations cause primary ciliarydyskinesia and disrupt the nexin-dynein regulatory complex. Am JHum Genet 2015;97:546–554.
39. Olbrich H, Schmidts M, Werner C, Onoufriadis A, Loges NT, Raidt J,et al.; UK10K Consortium. Recessive HYDIN mutations causeprimary ciliary dyskinesia without randomization of left-right bodyasymmetry. Am J Hum Genet 2012;91:672–684.
40. Moore A, Escudier E, Roger G, Tamalet A, Pelosse B, Marlin S, et al.RPGR is mutated in patients with a complex X linked phenotypecombining primary ciliary dyskinesia and retinitis pigmentosa. J MedGenet 2006;43:326–333.
41. Knowles MR, Ostrowski LE, Leigh MW, Sears PR, Davis SD, Wolf WE,et al. Mutations in RSPH1 cause primary ciliary dyskinesia with aunique clinical and ciliary phenotype. Am J Respir Crit Care Med2014;189:707–717.
42. Leigh MW, Hazucha MJ, Chawla KK, Baker BR, Shapiro AJ, Brown DE,et al. Standardizing nasal nitric oxide measurement as a testfor primary ciliary dyskinesia. Ann Am Thorac Soc 2013;10:574–581.
43. O’Callaghan C, Rutman A, Williams GM, Hirst RA. Inner dynein armdefects causing primary ciliary dyskinesia: repeat testing required.Eur Respir J 2011;38:603–607.
44. American Thoracic Society; European Respiratory Society. ATS/ERSrecommendations for standardized procedures for the online andoffline measurement of exhaled lower respiratory nitric oxide andnasal nitric oxide, 2005. Am J Respir Crit Care Med 2005;171:912–930.
45. Balfour-Lynn IM, Laverty A, Dinwiddie R. Reduced upper airway nitricoxide in cystic fibrosis. Arch Dis Child 1996;75:319–322.
46. Beydon N, Chambellan A, Alberti C, de Blic J, Clement A, Escudier E,et al. Technical and practical issues for tidal breathing measurementsof nasal nitric oxide in children. Pediatr Pulmonol 2015;50:1374–1382.
47. Boon M, Meyts I, Proesmans M, Vermeulen FL, Jorissen M, DeBoeck K. Diagnostic accuracy of nitric oxide measurements todetect primary ciliary dyskinesia. Eur J Clin Invest 2014;44:477–485.
48. Harris A, Bhullar E, Gove K, Joslin R, Pelling J, Evans HJ, et al.Validation of a portable nitric oxide analyzer for screening in primaryciliary dyskinesias. BMC Pulm Med 2014;14:18.
49. Mateos-Corral D, Coombs R, Grasemann H, Ratjen F, Dell SD.Diagnostic value of nasal nitric oxide measured with non-velumclosure techniques for children with primary ciliary dyskinesia. JPediatr 2011;159:420–424.
50. Papon JF, Bassinet L, Cariou-Patron G, Zerah-Lancner F, Vojtek AM,Blanchon S, et al. Quantitative analysis of ciliary beating inprimary ciliary dyskinesia: a pilot study. Orphanet J Rare Dis 2012;7:78.
51. Piacentini GL, Bodini A, Peroni D, Rigotti E, Pigozzi R, Pradal U, et al.Nasal nitric oxide for early diagnosis of primary ciliary dyskinesia:practical issues in children. Respir Med 2008;102:541–547.
52. Pifferi M, Bush A, Maggi F, Michelucci A, Ricci V, Conidi ME, et al.Nasal nitric oxide and nitric oxide synthase expression in primaryciliary dyskinesia. Eur Respir J 2011;37:572–577.
53. Santamaria F, De Stefano S, Montella S, Barbarano F, Iacotucci P,Ciccarelli R, et al. Nasal nitric oxide assessment in primary ciliarydyskinesia using aspiration, exhalation, and humming. Med SciMonit 2008;14:CR80–CR85.
54. Wodehouse T, Kharitonov SA, Mackay IS, Barnes PJ, Wilson R,Cole PJ. Nasal nitric oxide measurements for the screening ofprimary ciliary dyskinesia. Eur Respir J 2003;21:43–47.
55. Kouis P, Papatheodorou SI, Yiallouros PK. Diagnostic accuracy ofnasal nitric oxide for establishing diagnosis of primary ciliarydyskinesia: a meta-analysis. BMC Pulm Med 2015;15:153.
56. Collins SA, Gove K, Walker W, Lucas JSA. Nasal nitric oxide screeningfor primary ciliary dyskinesia: systematic review and meta-analysis.Eur Respir J 2014;44:1589–1599.
57. Knowles MR, Daniels LA, Davis SD, Zariwala MA, Leigh MW. Primaryciliary dyskinesia: recent advances in diagnostics, genetics, andcharacterization of clinical disease. Am J Respir Crit Care Med 2013;188:913–922.
58. Arnal JF, Flores P, Rami J, Murris-Espin M, Bremont F, Pasto IAguilla M, et al. Nasal nitric oxide concentration in paranasal sinusinflammatory diseases. Eur Respir J 1999;13:307–312.
59. Nakano H, Ide H, Imada M, Osanai S, Takahashi T, Kikuchi K, et al.Reduced nasal nitric oxide in diffuse panbronchiolitis. Am J RespirCrit Care Med 2000;162:2218–2220.
60. Autio TJ, Koskenkorva T, Leino TK, Koivunen P, Alho OP. Longitudinalanalysis of inflammatory biomarkers during acute rhinosinusitis.Laryngoscope 2017;127:E55–E61.
61. Ramsey BW, Davies J, McElvaney NG, Tullis E, Bell SC, Drevınek P,et al.; VX08-770-102 Study Group. A CFTR potentiator in patientswith cystic fibrosis and the G551Dmutation. N Engl J Med 2011;365:1663–1672.
62. Deschamp AR, Schornick L, Clem C, Hazucha M, Shapiro AJ, DavisSD. A comparison of nasal nitric oxide measurement modes. PediatrPulmonol 2017;52:1381–1382.
63. Stannard WA, Chilvers MA, Rutman AR, Williams CD,O’Callaghan C. Diagnostic testing of patients suspected ofprimary ciliary dyskinesia. Am J Respir Crit Care Med 2010;181:307–314.
64. Hirst RA, Jackson CL, Coles JL, Williams G, Rutman A, Goggin PM,et al. Culture of primary ciliary dyskinesia epithelial cells at air-liquidinterface can alter ciliary phenotype but remains a robust andinformative diagnostic aid. PLoS One 2014;9:e89675.
65. Hirst RA, Rutman A, Williams G, O’Callaghan C. Ciliated air-liquidcultures as an aid to diagnostic testing of primary ciliary dyskinesia.Chest 2010;138:1441–1447.
66. Lucas JS, Barbato A, Collins SA, Goutaki M, Behan L, Caudri D, et al.European Respiratory Society guidelines for the diagnosisof primary ciliary dyskinesia. Eur Respir J 2017;49:1601090.
67. Barbato A, Frischer T, Kuehni CE, Snijders D, Azevedo I, Baktai G,et al. Primary ciliary dyskinesia: a consensus statement on diagnosticand treatment approaches in children. Eur Respir J 2009;34:1264–1276.
68. Boon M, Smits A, Cuppens H, Jaspers M, Proesmans M, Dupont LJ,et al. Primary ciliary dyskinesia: critical evaluation of clinicalsymptoms and diagnosis in patients with normal and abnormalultrastructure. Orphanet J Rare Dis 2014;9:11.
69. Kempeneers C, Seaton C, Chilvers MA. Variation of ciliary beat patternin three different beating planes in healthy subjects. Chest 2017;151:993–1001.
70. Kupferberg SB, Bent JP, Porubsky ES. The evaluation of ciliaryfunction: electron versus light microscopy. Am J Rhinol 1998;12:199–201.
AMERICAN THORACIC SOCIETY DOCUMENTS
e38 American Journal of Respiratory and Critical Care Medicine Volume 197 Number 12 | June 15 2018

71. Pedersen M. Specific types of abnormal ciliary motility in Kartagener’ssyndrome and analogous respiratory disorders: a quantified microphoto-oscillographic investigation of 27 patients. Eur J Respir Dis Suppl 1983;127:78–90.
72. Greenstone M, Rutman A, Dewar A, Mackay I, Cole PJ. Primary ciliarydyskinesia: cytological and clinical features. Q J Med 1988;67:405–423.
73. Santamaria F, de Santi MM, Grillo G, Sarnelli P, Caterino M, Greco L.Ciliary motility at light microscopy: a screening technique for ciliarydefects. Acta Paediatr 1999;88:853–857.
74. Friedman NR, Pachigolla R, Deskin RW, Hawkins HK. Optimal technique todiagnose primary ciliary dyskinesia. Laryngoscope 2000;110:1548–1551.
75. Josephson GD, Patel S, Duckworth L, Goldstein J. High yield techniqueto diagnose immotile cilia syndrome: a suggested algorithm.Laryngoscope 2010;120(Suppl 4):S240.
76. Welch JE, Hogan MB, Wilson NW. Ten-year experience using a plastic,disposable curette for the diagnosis of primary ciliary dyskinesia.Ann Allergy Asthma Immunol 2004;93:189–192.
77. Raidt J, Wallmeier J, Hjeij R, Onnebrink JG, Pennekamp P, Loges NT,et al. Ciliary beat pattern and frequency in genetic variants of primaryciliary dyskinesia. Eur Respir J 2014;44:1579–1588.
78. Olm MA, Kogler JE Jr, Macchione M, Shoemark A, Saldiva PH,Rodrigues JC. Primary ciliary dyskinesia: evaluation usingcilia beat frequency assessment via spectral analysis ofdigital microscopy images. J Appl Physiol (1985) 2011;111:295–302.
79. Bush A, Cole P, Hariri M, Mackay I, Phillips G, O’Callaghan C, et al.Primary ciliary dyskinesia: diagnosis and standards of care. EurRespir J 1998;12:982–988.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e39





























