Embed Size (px)
Citation preview
Gen CAT08 1/1/2009
AMERICAN HEALTH SOLUTIONS SERIES IIASSOCIATION GROUP CATASTROPHIC HOSPITAL INSURANCE
FOR MEMBERS OF THENATIONAL CONSUMER’S ADVANTAGE ASSOCIATION
AND THEIR FAMILIES
NOTE: These plans are marketed in multiple states so coverage, optionalbenefits and Policy provisions may vary depending on the state ofresidence. These variances are listed in the State Variance Section of theForms Package. These variances must be reviewed with the applicant.
Individually UnderwrittenAssociation Group Catastrophic Hospital Insurance
Underwritten By Standard Life and Accident Insurance CompanyAdministrative Offices at One Moody Plaza
Galveston, Texas
Catastrophic Hospital.pdf 12/2/08 3:52:47 PM
Gen CAT08 1/1/2009
The American Health Solutions Series Association Group Catastrophic Hospital Insurance plansare underwritten by Standard Life and Accident Insurance Company a member of theAmerican National Family of Companies, which have enjoyed financial strength and stability since1905. Administrative Offices are located in Galveston, TX.Standard Life and Accident Insurance Company (“Standard Life”) has been evaluated andassigned the following ratings by nationally recognized, independent rating agencies. The ratingsare current as of January 2009.
A.M. Best A (Excellent) 3rd highest of 13 active company ratings 1
“Standard & Poor’s A+ (Very Strong) 5th highest of 20 active company ratings 2
“Ratings reflect current independent opinions of the financial capacity of an insurance organizationto meet the obligations of its insurance policies and contracts in accordance with their terms.They are based on comprehensive quantitative and qualitative evaluations of the company and itsmanagement strategy. The rating agencies do not provide ratings as a recommendation topurchase insurance or annuities. The ratings are not a warranty of an insurer's current or futureability to meet its contractual obligations.
Ratings may be changed, suspended, or withdrawn at any time. For the most current ratings visitStandard Life’s Internet site at www.slaico.com.
1 A.M. Best’s active company rating scale is: A++ (Superior), A+ (Superior), A (Excellent), A-(Excellent), B++ (Very Good), B+ (Very Good), B (Adequate), B- (Adequate), C++ (Fair), C+(Fair), C (Marginal), C- (Marginal) and D (Poor).
2 Standard & Poor’s active company rating scale is: AAA (Extremely Strong), AA (Very Strong), A(Strong), BBB (Good), BB (Marginal), B (Weak), CCC (Very Weak) and CC (Extremely Weak).Plus (+) or Minus (-) modifiers show the relative standing within the categories from AA to CCC.
These ratings are provided to you so that you may make a comparison of Standard Lifeand Accident Insurance Company to other companies. They are not provided as arecommendation by the rating companies to purchase this coverage.
This brochure contains a brief description of the coverage under the Group Policy Form SLA-C08-P. Coverage may vary depending upon Your state of residence. Consult Your agent forspecific exceptions or changes. Should inconsistencies occur with the information provided in thisbrochure, the terms and conditions of the Group Contract, as amended per state law, will apply.The Group Policy is the contract of insurance. Your Certificate describes the rights andobligations of both You and the insurance company under the Group Policy. It is, therefore,important that You read Your Certificate carefully. A sample is available, please ask your agent.
Notice: The association group insurance policy described in this brochure is availableonly to members of the National Consumer’s Advantage Association and is not intendedto be an employer sponsored health insurance plan.
Gen CAT08 1/1/2009
NCAA members enjoy a number of health, travel, consumer and business related benefitsfor a nominal monthly membership fee.
National Consumer’s Advantage Association (NCAA) was formed in 1993 to educate and benefitmembers by providing information, resources and access to savings on products and services.Association membership rates and benefits are subject to change without notice. NCAA offerstwo levels if membership to fit the needs of prospective members. Membership Services Officecan be contacted at 1-800-992-8044; email @egroupmanager.com or writing to 16476Chesterfield Airport Road, Chesterfield, MO 63017
SILVER PLUS level membership dues are $4.00 per month and provides the following basicbenefit package.
• Med Script Discount Pharmacy Service-Managed Care mail order service providingup to 50% savings on prescriptions.
• Lens Crafters Vision Club-20% discount on purchases; 10% discount on eye examsand contact lenses at some stores.
• Hearing Services-Up to 60% discount on quality hearing aids.• Vitamin and Nutrition Supplement Discounts.• Car Rental Discounts-Special savings at Alamo, Avis, Hertz or National.• North American Van Lines Moving Discounts-Substantial discounts on relocation
services.• Penny Wise Office Supply Discounts- Up to 36% off already discounted prices on a
large selection of items.• Powernet Global-Long distance rate of 4.9 cents per minute state-to-state, 24/ 7 days
a week.• Customized Web Sites-20% discount on full-service web site development and
maintenance.• Internet Access Services-Discounts on unlimited dial-up access to the Internet.• Emergency Medical Card-provides personal medical profile in case of an emergency.• GlobalFit discounts up to 60% at national fitness centers.• GymAmerica interactive exercise and diet programs.• CarPerks discount on auto purchases.• Travel Club discounts.
GOLD PLUS level membership dues are $6.00 per month and provides Silver membershipbenefits plus access to the following additional privileges and services.
• Crisp Learning.• Pre-Employment Background Reports.• Payroll Processing Services.• Roadside Assistance.• Theme Park and Floral service Discounts.• Magazine Subscription.• AD&D Coverage.• HopTheShop.com-Cybermall featuring over 100 high quality e-tailers and stores with
special discounts and features.• Medical Air Transport Services.• Child ID Card Services• Hewlett-Packard discount on computer and digital equipment.• DHL Express discounts on most classes of delivery.• Pinnacle special rates and services on credit card processing.• ITC-50 Hotel discounts of 50% at over 4,000 hotels
Catastrophic Hospital.pdf 12/2/08 3:56:05 PM
Gen CAT08 1/1/2009
Design a plan that meets your insurance needs and budget.
Catastrophic Hospital Plans: Indemnity and PPO plans available with all options
Issue Ages: 0-63 1/2
Option A: Calendar Year Cash Deductible Amounts:
$750, $1,500, $2,000, $2,500, $5,000, $10,000, $15,000, $20,000 or $25,000
Rate of Payment: 100%, 80% or 50%
Stop-Loss Amounts: $5,000 or $10,000
Maximum Benefit per Covered Person per Injury or Sickness: $1,000,000 or $2,000,000(Refer to Restoration of benefits section)
Option B (Family coverage only):
Benefits similar to those provide by an H S A Plan with the flexibility of being able to add optionalriders to enhance the base plan. This plan does not qualify as an H S A Plan.
Calendar Year Cash Deductible Amounts: $3,000, $4,000, $5,000, $10,000
Rate of Payment: 100%, 80% or 50%
Maximum Benefit per Covered Person per Injury or Sickness: $1,000,000 or $2,000,000(Refer to Restoration of benefits section)
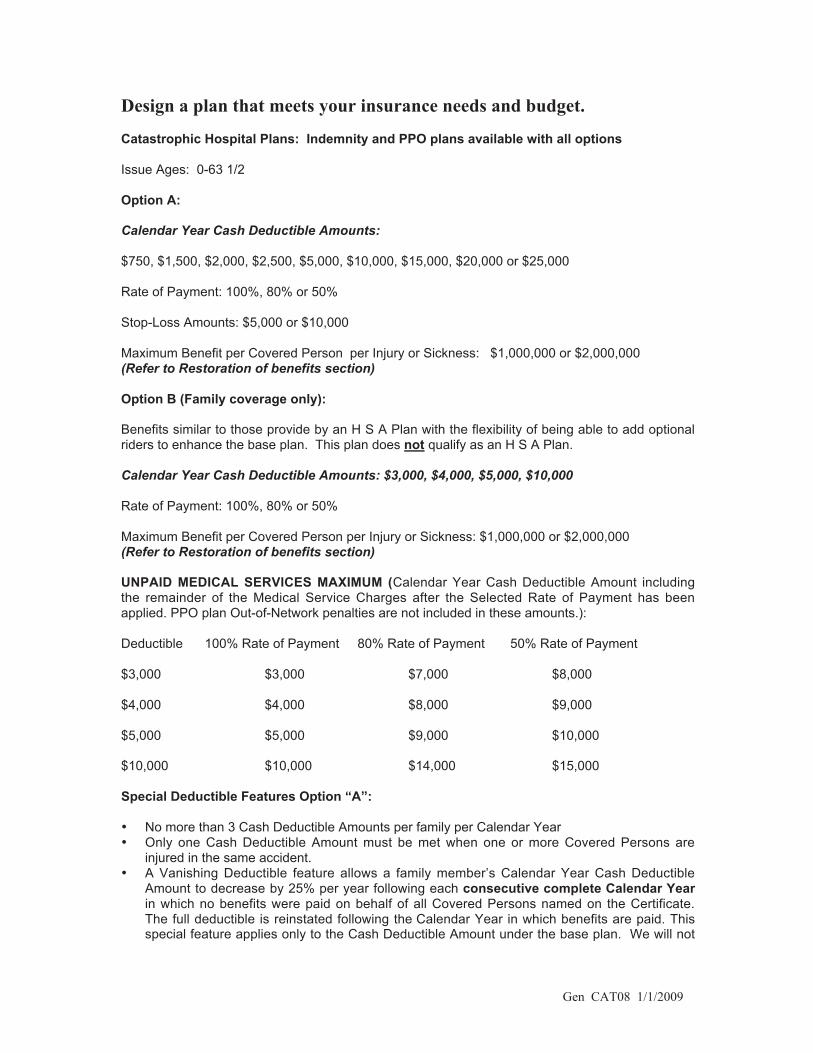
UNPAID MEDICAL SERVICES MAXIMUM (Calendar Year Cash Deductible Amount includingthe remainder of the Medical Service Charges after the Selected Rate of Payment has beenapplied. PPO plan Out-of-Network penalties are not included in these amounts.):
Deductible 100% Rate of Payment 80% Rate of Payment 50% Rate of Payment
$3,000 $3,000 $7,000 $8,000
$4,000 $4,000 $8,000 $9,000
$5,000 $5,000 $9,000 $10,000
$10,000 $10,000 $14,000 $15,000
Special Deductible Features Option “A”:
• No more than 3 Cash Deductible Amounts per family per Calendar Year• Only one Cash Deductible Amount must be met when one or more Covered Persons are
injured in the same accident.• A Vanishing Deductible feature allows a family member’s Calendar Year Cash Deductible
Amount to decrease by 25% per year following each consecutive complete Calendar Yearin which no benefits were paid on behalf of all Covered Persons named on the Certificate.The full deductible is reinstated following the Calendar Year in which benefits are paid. Thisspecial feature applies only to the Cash Deductible Amount under the base plan. We will not
Catastrophic Hospital.pdf 12/2/08 3:56:47 PM
Gen CAT08 1/1/2009
give any further reductions once the Cash Deductible Amount is reduced to zero. Thisprovision does not apply to a Deductible Amount in excess of $15,000.
Special Features Option “B”:
• The Calendar Year Deductible Amount can be satisfied by one or more Covered Persons.• If your selected Rate of Payment is less than 100%, once combined charges for Medical
Services incurred by one or more Covered Persons during the Calendar Year exceed theUnpaid Medical Service Charge Maximum, the rate of payment for the remainder of theCalendar Year will be 100%.
Option C (H S A Compatible Plans)
Maximum Benefit Per Covered Person per Covered Injury or Sickness: $1,000,000 or $2,000,000(Refer to Restoration of benefits section)
Rate of Payment Options: 100%, 80% or 50%
Calendar Year Cash Deductibles: *
Individual - ($1,500; $2,000; $2,500 or $5,000)
Family - ($3,000; $4,000; $5,000 or $10,000)
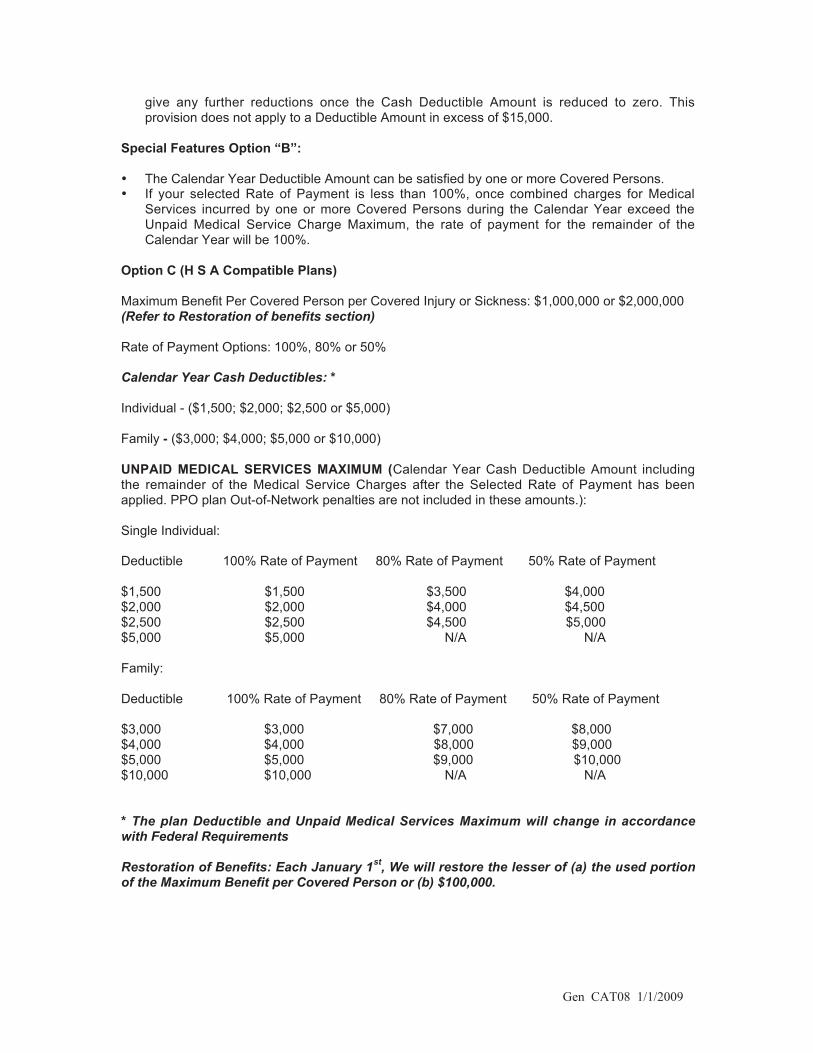
UNPAID MEDICAL SERVICES MAXIMUM (Calendar Year Cash Deductible Amount includingthe remainder of the Medical Service Charges after the Selected Rate of Payment has beenapplied. PPO plan Out-of-Network penalties are not included in these amounts.):
Single Individual:
Deductible 100% Rate of Payment 80% Rate of Payment 50% Rate of Payment
$1,500 $1,500 $3,500 $4,000$2,000 $2,000 $4,000 $4,500$2,500 $2,500 $4,500 $5,000$5,000 $5,000 N/A N/A
Family:
Deductible 100% Rate of Payment 80% Rate of Payment 50% Rate of Payment
$3,000 $3,000 $7,000 $8,000$4,000 $4,000 $8,000 $9,000$5,000 $5,000 $9,000 $10,000$10,000 $10,000 N/A N/A
* The plan Deductible and Unpaid Medical Services Maximum will change in accordancewith Federal Requirements
Restoration of Benefits: Each January 1st, We will restore the lesser of (a) the used portionof the Maximum Benefit per Covered Person or (b) $100,000.
Catastrophic Hospital.pdf 12/2/08 3:57:19 PM
Gen CAT08 1/1/2009
Covers a Wide Range of Care:
• slatipsoH • Same Day Surgery Facility• Home Health Care• In-Hospital Doctor Visits including consultations• Surgery• Assistant Surgeon• Organ Transplants including donor charges• Blood, Blood Plasma and Derivatives• Anesthesia• Hospice care• Mammograms• Second Surgical Opinion• Ambulance• Chemotherapy• Physiotherapy
Other Plan Features:
• You cannot be singled out for rate increase• No pre-admission certification required• 24/7 Coverage• Critical Illness benefit (Not available with H S A Plans)• Cash Confinement benefit (Not available with H S A Plans)
NOTE: THIS COVERAGE DOES NOT PROVIDE BENEFITS FOR THE TREATMENT OFALCOHOLISM OR DRUG USE.
This brochure contains a brief description of the coverage under the Group Policy Form SLA-C08-P. Coverage may vary depending upon Your state of residence. Consult Your agent forspecific exceptions or changes. Should inconsistencies occur with the information provided in thisbrochure, the terms and conditions of the Group Contract, as amended per state law, will apply.The Group Policy is the contract of insurance. Your Certificate describes the rights andobligations of both You and the insurance company under the Group Policy. It is, therefore,important that You read Your Certificate carefully. A sample is available, please ask your agent.
Notice: The association group insurance policy described in this brochure is availableonly to members of the National Consumer’s Advantage Association and is not intendedto be an employer sponsored health insurance plan.
Catastrophic Hospital.pdf 12/2/08 3:58:48 PM
Gen CAT08 1/1/2009
After You have met Your Cash Deductible and Your selected Rate of Payment is less than100%, the plan pays either 50% or 80% up to either the selected Stop Loss Amount (Option“A”) or the Option “B” and Option “C” Unpaid Services Maximum (maximum out-of-pocket). Once You have met this limit the plan pays 100% of additional eligible chargesduring the remainder of the Calendar Year.
Eligible Medical Service Charges while Hospital Confined or at a Same Day SurgicalFacility including the Reasonable and Customary Charges for:
• Daily average semi-private hospital room & board• Hospital charges for Intensive Care, Cardiac Care or Neonatal Intensive Care Unit• Miscellaneous In-hospital Expenses including operating room, recovery room, anesthesia,
central supplies, x-rays, lab, oxygen, medicines or drugs, splints or casts• In-hospital Doctor visits, other than Surgeon, including consultations• Blood, blood plasma or blood derivatives• Surgeon’s fees• Physiotherapy- physical therapy , speech therapy, or inhalation therapy• Pathology and Radiology• Breast Reconstruction• Chemotherapy and Radiation Therapy
Eligible Medical Service Charges for services provided outside a Hospital or AmbulatorySurgical Facility:
• Reasonable and Customary charges for professional ambulance services (ground or air) tothe nearest hospital qualified to treat the injuries or medical emergencies
• Home Health Care up to $7,500 per Calendar Year. Confinement must be within 7days of aprior Hospital stay of 3 days
• Reasonable and Customary charges for Hospice Care per Covered Person• Post Confinement Therapy
Human Organ Transplant: Up to the Group Policy’s Maximum Benefit per Covered Person perInjury and Sickness. This includes donor charges up to $15,000 in Medical Services if theCertificate Holder or a Covered Person is legally responsible for the charges.
Critical Illness Benefit– When You or a Covered Person is first Hospital Confined for treatmentof a diagnosed Critical Illness We will pay a $5,000 Critical Illness Benefit Amount. Critical Illnessmeans Cancer (other than skin, but including melanoma), Stroke (CVA) or Heart Attack (AcuteMyocardial Infarction) first diagnosed for a Covered Person more than 10 days after theCertificate Date. This benefit is payable only once for each Covered Person. In the event aCovered Person dies as the result of a Critical Illness without being Hospital Confined, ½ theCritical Illness Benefit will be paid to the Beneficiary named in the Enrollment Application on thebasis of post-mortem Critical Illness diagnosis. Not available with the H S A Plans.
Cash Confinement Benefit – Beginning on the third calendar day of a Covered Person’sHospital confinement for treatment of an Injury or Sickness for which benefits are otherwiseprovided under the Group Policy, we will pay a $100 Cash Confinement Benefit for each day aCovered Person remains Hospital confined. A Covered Person’s Hospital confinement beginningwithin three calendar days of his/her Hospital discharge will be considered a continuation ofhis/her previous Hospital confinement for purposes of this provision. Benefits payable under thisprovision may not be assigned. Not available with the H S A Plans.
Gen CAT08 1/1/2009
Preferred Provider Rider (SLA-PPO08) Option “A”
The rider reduces the cost of the base coverage.
When You or a Covered Person is admitted to a Preferred Provided Hospital or Same DaySurgery Facility and receive treatment from Preferred Provider Doctors in such facilities; anyresulting benefits payable under the Group Policy will be payable at the selected Rate ofPayment.
When You or a Covered Person is admitted to a Hospital that is not a Preferred Provider Hospital;use a Same Day Surgery Facility that is not part of Preferred Provider Same Day Surgery Facility;or receive treatment from a Doctor who is not a Preferred Provider Doctor; any benefits payableunder the Group Policy will be payable at a Rate of Payment that is 20% less than the selectedRate of Payment percentage, unless such admission, use or treatment is the result of anemergency.
Preferred Provider Rider (SLA-PPOB08) Option “B” and SLA-PPOH08 Option “C” (H S APlans)
The rider reduces the cost of the base coverage.
When You or a Covered Person is admitted to a Preferred Provided Hospital or Same DaySurgery Facility and receive treatment from Preferred Provider Doctors in such facilities; anyresulting benefits payable under the Group Policy will be payable at the selected Rate ofPayment.
When You or a Covered Person is admitted to a Hospital that is not a Preferred Provider Hospital;use a Same Day Surgery Facility that is not part of Preferred Provider Same Day Surgery Facility;or receive treatment from a Doctor who is not a Preferred Provider Doctor; any benefits payableunder the Group Policy will result in a 20% reduction of any otherwise eligible Medical ServicesCharges that We do not pay due to a Covered Person’s voluntary use of an Out-of-Networkprovider, unless such admission, use or treatment is the result of an emergency.
Optional Additional Benefit Riders for additional premium. Benefits are not subject to theGroup Policy’s Deductible Amount or Rate of Payment.(NOT AVAILABLE WITH H S A PLANS)
Outpatient Accident Expense Benefit Rider SLA-ACC608:
We will pay the Reasonable and Customary Charges in excess of this Rider’s Deductible Amountwhen such charges are incurred by a Covered Person for the Medically Necessary Outpatienttreatment of a covered Injury up to the Rider’s Maximum Benefit per Injury. Initial treatment by aDoctor must begin within forty-eight (48) hours of the Injury; and subsequent treatment must bereceived within thirty (30) days of the Injury.
Benefits are available in the following benefit and deductible combinations:
$500/$100; $1,000/$250; $1,500/$250; or $2,500/$500
Notice-The association group insurance policy described in this brochure is available onlyto members of the National Consumer’s Advantage Association and is not intended to bean employer sponsored health insurance plan.
Gen CAT08 1/1/2009
Outpatient Doctor Rider SLA-OPD608: (Not available with the Outpatient DiagnosticImaging Rider):
We will pay benefits for the Medically Necessary Outpatient treatment of a Covered Person whenthe Reasonable and Customary Charges for the Rider Services described below and provided asa part of such treatment exceed this Rider’s Calendar Year Deductible. Benefits will be paid at80% of the Reasonable and Customary Charges up to the selected Maximum Benefit for suchRider Services. The following deductibles and maximum benefit are available: Deductibles: $750;$1,000; or $1,500. Maximum Benefits: $25,000 or $100,000.
Rider Services are:
1. Hospital Emergency room or other Outpatient clinic;2. Doctor;3. Anesthesia, including administration charges, for a Covered Person undergoing
Outpatient surgery;4. Charges for Outpatient diagnostic tests;5. Miscellaneous supplies including casts, splints, braces, hypodermics, and crutches;6. Childhood immunizations, provided for children under the age of six. (Not subject to the
Rider’s Deductible.);7. Prescription drugs taken or administered within 30 days of a Covered Person being
Hospital Confined when administered for treatment of the same condition that caused theCovered Person to be Hospital Confined (including medication for the treatment ofdiabetes); and
8. Diabetes self-management training and patient management, including medical nutritiontherapy, not exceed $500 in a two-year period.
Limitations:
1. No benefits will be paid under this Rider for spinal manipulations, hot or cold packtreatment or ultra sound treatment; radiation therapy, including treatment planning;chemotherapy, including treatment planning; physical therapy; speech therapy;occupational therapy or for the rental or purchase of durable medical equipment; and
2. Benefits payable under this Rider for each Covered Person are subject to theOUTPATIENT DOCTOR RIDER MAXIMUM BENEFIT PER CALENDAR YEAR andOUTPATIENT DOCTOR RIDER CASH DEDUCTIBLE PER CALENDAR YEAR.
Outpatient Prescription Drug Rider SLA-OPRx08:
Once a Covered Person’s Prescription Drug charges exceed this Rider’s applicable DeductibleAmount in a Calendar Year and the appropriate Copayment Amount has been paid, We will payany additional Prescription Drug charges for the same Covered Person during the remainder ofthe Calendar Year at the applicable Rate of Payment Amount. The Covered Person must meetthe Deductible before benefits are payable under this Rider for the Covered Person. If more thanone Covered Person is covered under this Rider, then the maximum Deductible Amount thatmust be met in a Calendar Year is two times the Deductible Amount and may be met collectivelyby all Covered Persons.
When You obtain Prescriptions Drugs from a Non-Participating Pharmacy, You must pay theentire cost of the drugs to the Non-Participating Pharmacy at the time of purchase. You may thensend a claim to Standard life for reimbursement. Standard Life will deduct the applicableCopayment and applicable Rate of Payment Amount from the total charges and then pay theclaim at the negotiated rate it has with a Participating Pharmacy provider.
Gen CAT08 1/1/2009
Participating Pharmacy:
Prescription Drug Calendar Year Deductible:
Individual: $500 or $1,000 Family: $1,000 or$2,000
Copay:
Generic: $10, Mail Order Generic: $30
Brand Name: $25, Mail Order Brand Name: $75
Non-Participating Pharmacy:
Prescription Drug Calendar Year Deductible:
Individual: $1,000 or $2,000 Family: $2,000 or$4,000
Copay: Generic: $10 Brand Name: $25
Note: There is no mail order available when ordered through a non-participating pharmacy.
Rate of Payment Amount:
Generic: 100% after the Deductible and Copay
Brand Name when no generic equivalent available: 50% after the Deductible and Copay
Brand Name when Generic is available: After You meet the deductible and pay the $10Generic Copay, You are responsible for 100% of the difference between the cost of theGeneric and Brand Name drug.
We do not cover drugs that are associated with an Injury or Sickness that We haveexcluded by name or description. We will not pay benefits under this Rider for drugsexcluded by this rider.
Payment for a Prescription Drug does not mean We have any liability under Eligible Expenses.Prescription by a Doctor does not automatically make treatment Medically Necessary.
No benefit will be paid for:
1. Any Ancillary Drug Charge included in the cost of the Prescription Drug;2. The cost of any Prescription Drug dispensed in a quantity that exceeds a thirty-one (31) day
supply unless the packaging of the manufacturer or the prescription requires a greaterquantity, except 90 day Mail Order Drugs;
3. Prescription Drugs used in the treatment of primary nocturnal enuresis (bedwetting) for aCovered Person under the age of six;
4. Contraceptives, including any drugs or devices that are prophylactic or preventative in nature. We will not apply this Exception to a contraceptive Prescription Drug that is Medically
Necessary for the treatment of an existing Sickness that the Group Policy would otherwisecover;
5. Any drug which is taken to end pregnancy;6. Any drug that does not require a Doctor’s prescription, except prenatal vitamins a Doctor
prescribes for pregnancy;7. Prescription refills: (a) In excess of the number specified in the Doctor’s prescription; or (b) Dispensed more than one year after the initial prescription date;8. Prescription Drugs that a Doctor administers or dispenses while in his office or while a
Covered Person is in a facility that provides medical care, including unit dose Prescription Drugsand any supplies.
Catastrophic Hospital.pdf 12/2/08 4:01:51 PM
Gen CAT08 1/1/2009
9. Prescription Drugs that a Doctor prescribes or are otherwise used for:(a) Cosmetic purposes;(b) Treatment of hair loss;(c) Care, services or treatment that the Group Policy excludes;(d) Treatment of an Injury or Sickness that the Group Policy does not cover;(e) Losing weight;(f) Treating Acne (including Accutane);(g) Promoting growth (for example: growth hormone);(h) Treating sexual dysfunction or inadequacy; or(i) Facilitating smoking cessation (including any Prescription Drug containing
nicotine or its derivatives).10. Prescription Drugs that a Doctor prescribes for the treatment of mental illness, chronic fatigue syndrome or fibromyalgia.
11. Any Prescription Drug that is not consistent with the diagnosis and treatment of the Covered Person’s Injury or Sickness because:
(a) The Prescription Drug is excessive in terms of the scope, duration or intensity ofscope;
(b) The duration or intensity of Prescription Drug therapy is excessive in terms ofwhat is needed to provide safe, adequate and appropriate care; or
(c) The Prescription Drug is solely for the Covered Person’s, Covered Person’sfamily or Doctor’s convenience.
12. Prescription Drugs prescribed for the replacement of lost or stolen prescriptions.
Outpatient Diagnostic Imaging Rider SLA-DIR608: (Not available with the OutpatientDoctor Rider)
Benefits are payable under this Rider once the Reasonable and Customary Charges incurred bya Covered Person for Medically Necessary Diagnostic Imaging exceed this Rider’s Calendar YearCash Deductible Amount. We then pay [80%] of such remaining charge up to the Calendar YearRider Maximum. Diagnostic Imaging means Magnetic Resonance Imaging (MRI), MagneticResonance Angiography (MRA), Computed Axial Tomography (CAT Scans), Positron EmissionTomography (PET Scans), or Computed Tomography (CT scans). Benefits provided by this Riderwill not duplicate similar benefits provided under the Group Policy. Total benefits paid under theGroup Policy and this, or any other Rider will not be greater than the actual expense incurred.
The following deductibles and maximum benefit are available: Deductibles: $750; $1,000 or$1,500; Maximum Benefit: $25,000.
This brochure contains a brief description of the coverage under the Group Policy Form SLA-C08-P. Coverage may vary depending upon Your state of residence. Consult Your agent forspecific exceptions or changes. Should inconsistencies occur with the information provided in thisbrochure, the terms and conditions of the Group Contract, as amended per state law, will apply.The Group Policy is the contract of insurance. Your Certificate describes the rights andobligations of both You and the insurance company under the Group Policy. It is, therefore,important that You read Your Certificate carefully. A sample is available, please ask your agent.
Gen CAT08 1/1/2009
Information you should know:
When Coverage Begins-We require evidence of insurability before coverage is provided. Oncewe have approved Your Enrollment Application, and other conditions remain as described in theEnrollment Application, coverage for You and those dependents listed in the EnrollmentApplication and accepted by Us will begin on the Certificate Date shown in the CertificateSchedule.
Newborn and Adopted Children-A child born to You, adopted by You or a child placed foradoption with You is automatically covered from birth, date of adoption or date placed foradoption for 31 days.
To continue the child as a Covered Person, You must notify the company of the child’s birth, dateof adoption or date of placement for adoption and pay the additional premium for the child notlater than 62 days following the child’s date of birth, date of adoption or placement for adoption.
Pregnancy- Coverage for normal pregnancy is not provided. If a Covered Person hasComplications of Pregnancy while covered under the Policy, Medical Services incurred fortreatment of such Complications of Pregnancy will be considered for payment as if they hadresulted from Sickness. If an expense does not result solely from the treatment of theComplications of Pregnancy, then it will be deemed due to normal pregnancy and not coveredunder the Group Policy.
Foreign Emergency Treatment-Your coverage remains in effect for Emergency treatment whiletraveling outside of the United States. Benefits will be the lesser of: (1) the actual charges for theservices; or (2) the benefit for Medical Services that We would have paid if the Covered Personhad received the Emergency treatment in the location where the Covered Person resides.
Other Insurance Benefits-This Plan has a Coordination of Benefits provision which is a methodof coordinating benefits payable under more than one insurance plan so that benefits from allsources do not exceed 100% of a Covered Person’s Allowable Expense.
Premium Changes-We will not change Your premium prior to the first anniversary of theCertificate Date, unless Your coverage or residence changes. After the first anniversary ofcoverage, We may change premium as a result of a change in Your age or residence or anytime,and from time to time, that we decided to change rates for persons in your or a Covered Person’sclass. We will give You 30 days notice before any premium change. The new rates will apply ona class basis as determined by Standard Life.
Pre-Existing Conditions- Means a condition not otherwise excluded by name or specificdescription: (1) for which medical advice, testing, care, treatment or medication was given or wasrecommended by, or received from a Doctor within twelve months before the Certificate Date; or(2) that would have caused a reasonably prudent person to seek medical diagnosis or treatmentwithin twelve months before the Certificate Date. The Company does not cover Pre-ExistingConditions for the first twelve months of coverage.
The Pre-Existing Condition provision does not apply to a covered person who enrolled as aHIPAA Eligible individual.
Notice: The association group insurance policy described in this brochure is availableonly to members of the National Consumer’s Advantage Association and is not intendedto be an employer sponsored health insurance plan.
Gen CAT08 1/1/2009
Termination of Coverage- We can terminate or non-renew coverage under the Group Policy asof any premium due date under any of the following conditions:
(a) You failed to pay premiums or contributions in accordance with the terms of the Group Policyor We have not received timely premium payments;
(b) You or a Covered Person has performed an act or practice that constitutes fraud withrespect to activities under the Group Policy;
(c) You no longer reside, live or work in the PPO service area or in an area where We haveauthority to do business. We will only apply this provision if We end coverage uniformly andwithout regard to any health status related factor of a Covered Person; or
(d) We cease to offer coverage in the medical expense market in accordance with applicablestate law.
In the event of termination or non-renewal of coverage, the Company will give You notice asrequired by law.
EXCEPTIONS:
WE DO NOT COVER AN INJURY OR SICKNESS THAT IS EXCLUDED BY NAME ORDESCRIPTION.
THIS POLICY DOES NOT PROVIDE COVERAGE FOR LOSS CAUSED BY, CONTRIBUTEDTO, OR RESULTING FROM ANY OF THE FOLLOWING EXCEPTIONS.
1. Injury or Sickness if the loss is covered under these or similar laws:worker’s compensation,
ro ,ytilibail s’reyolpme occupational disease laws.
2. Injury or Sickness that results from war or an act of war, whether war is declared or not. 3. Care or supplies that a Covered Person receives in a Hospital or other facility that a
government agency runs; however, We will not apply this Exception if:(a) The Covered Person receives a charge that he has to pay by law, and(b) The Hospital or facility would have made the charge even if no insurance existed.
4. The diagnosis and/or treatment of the adenoids, tonsils, gallbladder, reproductive organs,and hernia for the first six months of coverage; however, if We have excluded any one ofthese conditions by rider, We do not pay any benefit for the condition, regardless of when thetreatment takes place; or if such condition is a Preexisting Condition, any benefitconsideration will be in accordance with the Preexisting Conditions provision; however, thisException does not apply to a HIPAA Eligible Individual.
5. Procedures or treatments that are Experimental or Investigational Medicine. 6. Pregnancy and childbirth, except for Complications of Pregnancy. 7. Mental Disorders. 8. Cosmetic surgery or reconstructive surgery, including breast reduction and surgery to repair, replace, or remove breast implants; however, this Exception does not apply when surgery is required:
a) To correct damage for a covered Injury or Sickness;b) To repair a birth defect of a child born to the Certificateholder and continuously covered
under this Policy from its birth; orc) For reconstructive surgery following a covered mastectomy.
9. Dental Treatment, unless due to Injury to a Covered Person’s natural teeth. 10. A Pre-Existing Condition as defined in this Policy. 11. Any attempt at suicide, while sane. 12. An intentionally self-inflicted Injury, while sane.
Gen CAT08 1/1/2009
13. A Covered Person’s commission of or attempt to commit a felony or being engaged in anillegal occupation.
14. A Covered Person being intoxicated, unless such intoxication is the result of a prescriptiondrug taken as prescribed by a Doctor.
15. A Covered Person with a blood alcohol concentration equal to or in excess of .08 gms/dloperating any motor vehicle, including any off-road vehicle, or watercraft.
16. Any procedure for refractive correction, eye refraction or the purchase or fitting of vision orhearing aids, Cochlear Implants and related devices.
17. Weight reduction or treatment of obesity, including exogenous, endogenous, or morbidobesity.
18. Mandibular or maxillofacial surgery to correct growth defects and jaw disproportions ormalocclusions; increase vertical dimension; or reconstruct occlusion after one year from achild’s date of birth or a child’s date of adoption, except where such surgery is for the repairof a congenital anomaly or birth defect of a child born to the Certificateholder or a child thathe/she adopts if the child is continuously covered from birth, adoption, or placement foradoption. This exception does not apply to the treatment of temporomandibular joint disorderor craniomandibular disorder.
19. Treatment provided outside the United States of America, its possessions and territories,except as otherwise provided under Foreign Emergency Treatment.
20. Diagnosis or treatment (including surgery) of sexual dysfunction disorder or inadequacy; ortranssexual surgery.
21. Sclerotherapy for veins of the extremities or laser surgery to minimize veins.22. Routine newborn care.23. Care in a nursing home or custodial institution; domiciliary care or rest cures.24. Charges for Medical Services that the Certificateholder or a Covered Person is not legally
obligated to pay.25. Any charges for or relating to: artificial insemination; in-vitro fertilization or any other
diagnosis or treatment for the control, promotion, or enhancement of fertility; treatment forimpotency; sterilization or reversal of prior sterilization; abortion, unless the life of the motherwould be endangered if the fetus were carried to term; or therapeutic abortion.
26. Drugs and supplies provided for home use.27. TREATMENT OF ALCOHOLISM OR DRUG USE.28. False labor; pre-term or premature labor; occasional spotting; prescribed rest while pregnant;
morning sickness; hyperemesis gravidarum; or pre-eclampsia. There may be otherconditions that relate to a difficult pregnancy that a Doctor can manage.
Catastrophic Hospital.pdf 12/2/08 4:04:44 PM






























